-
Concurrent Session 09: Implementation of Cervical Cancer
Screening in Low-Resource Settings
Consortium of Universities for Global Health
6th Annual Meeting
March 16, 2018
Laura Rozek, Ph.D.
Associate Professor of Environmental Health, Nutrition and
Global Public HealthAssociate Director, Office of Global Public
Health
Director, Global Cancer Initiative
University of Michigan School of Public Health
-
The cancer burden is greatest in low and middleincome
countries
-
http://canceratlas.cancer.org/taking-action/cancer-registries/
Proportion (%) of the regional population covered by high
quality cancer registration and high quality complete vital
registration of
death low levels in many global areas
-
Globocan: http://globocan.iarc.fr
Unacceptably high global mortality from cervical cancer burden
in LMICs
-
Speakers Gloria Sanchez, Facultad de Medicina Universidad de
Antioquia,
Colombia: Evaluation of quality of healthcare delivery to
prevent cervical cancer in low-resource settings
Mesrach Ayalew Kebede, St. Pauls Hospital Millennium Medical
College, Addis Ababa: Efforts to address barriers to cervical
cancer screening in Ethiopia
Rafael Meza, University of Michigan School of Public Health: HPV
self-sampling for cervical cancer screening in indigenous and rural
communities in Guatemala
-
Evaluation of quality of healthcare delivery to prevent cervical
cancer
in low-resource settings
Implementation of Cervical Cancer Screening in Low Resource
SettingsGloria I. Sanchez MSc, PhD6th Annual CUGH ConferenceNew
York, NY, March 16, 2018
-
Regional disparities of cervical cancer mortality in LACs
Almonte M, Murillo R, Snchez GI, Jernimo J, Salmern J, Ferreccio
C, Lazcano-Ponce E, Herrero R. Salud Publica Mex. 2010
Nov-Dec;52(6):544-59.
-
Introduction
Clinically, or self-collected HPV test is more accurate and
detects high-grade cervical disease earlier than cytology
However, many HPV positive women will clear infection soon and
donot need immediate treatment
Adequate follow-up of HPV positive women in unorganized settings
oflow-middle income countries is challenging
Optimal referral avoids overtreatment and overuse of health
careservices
Focus in women with higher risk of disease
-
Introduction
Evidence of implementation of HPV testing mainly in studies
within organized screening settings (Dillner L et al, Int J Cancer
2011).
Scaling-up HPV-based screening in unorganized settings,
Low-middle income countries.
Pragmatic trials: High-quality evidence, outcomes relevant to
patients and decisions makers, real-life clinical practices.
Colombia: Guidelines for screening with hrHPV testing but not
programmatic use of it yet
Opportunity to evaluate the quality of health services for
follow-up of screen positive women
-
Aim To compare under routine clinical conditions of a
opportunistic screening setting the effectiveness to detect
CIN2+ and efficiency to reduce CIN2+ and health care utilization of
immediate colposcopy (IC), conventional cytology at 6/12 months
(RC) and hrHPV testing (HPV) after 2 years follow-up of women with
ASC-US cytology
-
ENROLMENTVISIT
STUDYPOPULATION
20-69 years old women, first time ASC-US cytology, residents of
the MetropolitanArea of Medellin, attended routine screening
services, of three Healthcare
Management Organizations (HMOs) of Medellin, Colombia
Recruitment by phone invitation (until 3 months after ASC-US
Pap)
Eligibility criteria, informed consent, pelvic examination,
questionnairessample collection (blood, cervical specimens in STM
and cytology)
Randomization
Repeat cytology at 6 and 12 months
Immediate routine colposcopy HC2-HPV triage
2 yearsFOLLOW-UP
Phone calls at 6 and 18 m
Visit to primary site at 12 m
Refer to Colposcopy in any cytology ASCUS
Routine management by health care management and provider
organizations
EXIT VISIT (24 months)
All women tested by HC2-HPV/Pap smear. if any positive referred
to research colposcopy (One or two biopsies from observed lesions
and one at random , If no lesions two random biopsies)
Routine management
Both negative Any ASC-US Positive Negative
Routine colposcopy
CIN2 CIN1
Follow-up with Pap smear
6/12m
Routine screening
Treatment
Study Design
-
Total ASC-US referred
7,866
Assessed for eligibility
4,509
Ineligible for invitation (3,357): Age not 20 to 69 years: 856
Residence outside the study area: 513 ASC-US cytology more than 3 m
old: 1,988
Randomized2,661
Excluded (1,845): No meeting inclusion criteria: 1,134 (407
reported, previous abnormal cytology, 271 had a clinical,
condition, 172 had colposcopy appointment , 123 were pregnant and
161 other reasons)
Declined to participate: 702 Deferred: 12
Immediate colposcopy (IC)882
Repeat cytology at 6/12 m (RC)890
hrHPV triage (HPV)889
100% to routine colposcopy Routine colposcopy if routine
cytology ASC-US Routine colposcopy if hrHPV+
had at least one ASC-US cytology (n=125)
NILM only (n=410) without retrieved records (n= 350)
unknown result (n=4) hrHPV+ rate (361/887): 41%
At least one ASC-US cytology (n=217)
NILM only (n=485) without retrieved records (n=178) unknown
result (n=10) ASC-US rate (217/702): 31%
FOLLOW-UP
Median (IR) time: 23 (22-25) months
ALLOCATION
had 1 colposcopy 772/882 (88%) had 1 histology 492/772 (64%)
889890882ANALYZEDITT analysis
ENROLLMENT Jan 2011-2014
had 1 colposcopy (372/890): 42% had 1 histology 271/372):
73%
had 1 colposcopy (462/889):52% had 1 histology: (313/462):
68%
At least one ASC-US cytology (n=128)
NILM only (n= 455) without retrieved records (n=291) unknown
result (n= 8)
Consort
-
Data Collection for community-based Diagnoses
1,726 pathology reports 898 biopsies, 697 other specimens and
131 both 1.320 of follow-up and 406 of exit visit
2,301 slides corresponding to 1,017 (59%) reports reviewed by 2
expert pathologists
Only 646 cervical biopsies with unique specimens were included
in the final analysis
-
Cumulative detection of Reviewed CIN2+ in different Health
Management Organizations
Logrank test P= 0.26
Logrank test P= 0.12
-
HPV (n=889)
IC (n=882)
RC (n=890)
ASC-US (n=217)
NLIM (n=485)
hrHPV+ (n=361)
hrHPV- (n=526)
A B
C
Use of Colposcoy by arm and triage test resultdurin 24 months of
women with ASCUS cytology
-
Comparison of total Use of Colposcoy by armand triage test
result
Arm / Test # Womenby test result
# Womenattending
Colposcopy%
RC Arm (N= 890)ASCUS 217 183 84,33*ASCUS 485 199 41,03**W/o
cytology 188 70 37,23
HPV arm (N=889)Positive 361 334 92,52*Negative 526 127
24,14**W/o Test 2 0
*Chi-squared test P = 0,0019 ASCUS vs. HPV positive**Chi-squared
test P < 0,0001 ASCUS vs. HPV Negative
-
Interpretations of community and Experts histology diagnosis of
cervical biopsies
Bhapkar test p-value < 0.001 , Unweighted Kappa= 0.320, 95%
confidence interval: 0.275-to 0.365N= 646 diagnostic reports with
diagnosis obtained in unique cervical specimens
Negative CIN1 CIN2 CIN3 Cancer TotalNegative 206 20 27 1 0
254Row% 81 8 11 0 0 100CIN1 72 91 104 36 1 304Row% 24 30 34 12 0
100CIN2 5 6 22 38 1 72Row% 7 8 31 53 1 100CIN3 0 0 2 14 0 16Row% 0
0 13 88 0 100Cancer 0 0 0 0 0 0Row% --- --- --- --- --- ---Total
283 117 155 89 2 646
Community Experts
Tabla original
CommunityExperts
NegativeCIN1CIN2CIN3CancerTotalNegativeCIN1CIN2CIN3Cancer
Negative20620271025420620271
Row%81811001007291104361
CIN172911043613045622381
Row%243034120100214
CIN256223817200000
Row%7831531100
CIN300214016
Row%0013880100
Cancer000000
Row%------------------
Total283117155892646
Bhapkar test p-value < 0.001
Agreement
Para 3 categoras: 0, 1 y 2+
By record (n=646)02
AgreementKappa indexAgreementKappa
%(95% CI)k(95% CI)agreeliagrelsagrekliklsk
Global58(54-62)0.39(0.34-0.44)57.8947454.0517361.644410.39035040.34235140.4383493
IC54(48-61)0.35(0.27-0.42)54.2986447.7134760.736930.34699550.26915040.4248406
RC59(53-66)0.41(0.33-0.49)59.3301452.5603665.763140.41089670.32680840.4949849
ASC-US55(45-65)0.38(0.26-0.50)55.4347845.2637165.170190.3806240.26020090.501047
HPV60(54-66)0.41(0.33-0.50)60.1851953.5339366.48050.41363640.3275810.4996917
hrHPV+57(49-64)0.39(0.29-0.48)57.0552149.3799964.405550.38540260.28710980.4836954
By case (n=565)
AgreementKappa indexAgreementKappa
%(95% CI)k(95% CI)agreeliagrelsagrekliklsk
Global58(54-62)0.40(0.35-0.45)58.4070854.2995462.401080.40143450.35003860.4528303
IC53(46-60)0.33(0.25-0.41)52.7363245.8479359.522070.33401930.25350620.4145323
RC61(49-71)0.44(0.30-0.58)60.8108149.4195271.135080.44114580.30150640.5807853
ASC-US63(56-69)0.45(0.36-0.54)62.702755.5421369.346470.45160460.36042690.5427823
HPV60(53-67)0.43(0.33-0.52)60.335253.0238767.212240.42532220.33088720.5197571
hrHPV+56(48-65)0.38(0.27-0.49)56.2547.598164.537690.37858690.26663290.4905409
-
Reproducibility between Community and Expert Pathologists
histological Diagnosis
N= 646 diagnostic reports with diagnosis obtained in unique
specimens. IC = immediate colposcopy, RC= repeat cytology, HPV:
Human Papillomavirus. *Unweighted Kappa estimated using 3
categories (Negative, CIN1 and CIN2+).ASC-US: Atypical Squamous
Cells of Undetermined Significance
% (95% CI) k (95% CI)Global 58 (54-62) 0,39 (0,34-0,44)IC arm 54
(48-61) 0,35 (0,27-0,42)RC arm 59 (53-66) 0,41 (0,33-0,49)
ASC-US 55 (45-65) 0,38 (0,26-0,50)HPV 60 (54-66) 0,41
(0,33-0,50)
hrHPV+ arm 57 (49-64) 0,39 (0,29-0,48)
Agreement Kappa index*
Tabla original
LocalReviewed
NegativeCIN1CIN2CIN3CancerTotalNegativeCIN1CIN2CIN3Cancer
Negative20620271025420620271
Row%81811001007291104361
CIN172911043613045622381
Row%243034120100214
CIN256223817200000
Row%7831531100
CIN300214016
Row%0013880100
Cancer000000
Row%------------------
Total283117155892646
Bhapkar test p-value < 0.001
Agreement
Para 3 categoras: 0, 1 y 2+
By record (n=646)02
AgreementKappa index*AgreementKappa
%(95% CI)k(95% CI)agreeliagrelsagrekliklsk
Global58(54-62)0.39(0.34-0.44)57.8947454.0517361.644410.39035040.34235140.4383493
IC
arm54(48-61)0.35(0.27-0.42)54.2986447.7134760.736930.34699550.26915040.4248406
RC
arm59(53-66)0.41(0.33-0.49)59.3301452.5603665.763140.41089670.32680840.4949849
ASC-US55(45-65)0.38(0.26-0.50)55.4347845.2637165.170190.3806240.26020090.501047
HPV60(54-66)0.41(0.33-0.50)60.1851953.5339366.48050.41363640.3275810.4996917
hrHPV+
arm57(49-64)0.39(0.29-0.48)57.0552149.3799964.405550.38540260.28710980.4836954
By case (n=565)
AgreementKappa indexAgreementKappa
%(95% CI)k(95% CI)agreeliagrelsagrekliklsk
Global58(54-62)0.40(0.35-0.45)58.4070854.2995462.401080.40143450.35003860.4528303
IC53(46-60)0.33(0.25-0.41)52.7363245.8479359.522070.33401930.25350620.4145323
RC61(49-71)0.44(0.30-0.58)60.8108149.4195271.135080.44114580.30150640.5807853
ASC-US63(56-69)0.45(0.36-0.54)62.702755.5421369.346470.45160460.36042690.5427823
HPV60(53-67)0.43(0.33-0.52)60.335253.0238767.212240.42532220.33088720.5197571
hrHPV+56(48-65)0.38(0.27-0.49)56.2547.598164.537690.37858690.26663290.4905409
-
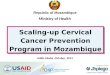
Cumulative detection of CIN2+ by Community and Expert
Pathologists diagnosis by period and arm
1.47 1.46
2.590.11
1.35
0.22
0.79
0.67 0.341.13
2.36
1.24
0
2
4
6
8
10
12
IC(N=882)
RC(N=890)
HPV(N=889)
2 ye
ar C
umul
ativ
e De
tect
ion
of C
IN2+
by
Com
mun
ity P
atho
logi
sts (
%)
6.92
3.03
6.52
0.23
2.47
0.56
1.13
1.46
0.56
3.51
4.492.59
0
2
4
6
8
10
12
IC(N=882)
RC(N=890)
HPV(N=889)
2 ye
ar C
umul
ativ
e De
tect
ion
of C
IN2+
by
Exp
ert P
atho
logi
sts (
%)
4.6 x 2.0x
2 p value = 0.004
2 p value = < 0.001
2.5x
-
Expertpathology
result
TotalN
With No LEEP (%)
With LEEP (%)
Negative 971 960 (98.9) 11 (1.1)
CIN1 172 163 (94.8) 9 (5.2)
CIN2 160 111 (69.4) 49 (30.6)
CIN3/AIS 48 18 (37.5) 30 (62.5)
Treatment among women of the ASCUS-COL trial with biopsies given
the diagnosis
of expert pathologists
-
Period on LEEP/LLETZ tissue specimens during the 24 months
follow-up of 2.661 women of the ASCUS Trial
PERIODIC arm RC arm HPV arm Total by
periodN % N % N %
Enrollment 14 (28,5) 17 (34,6) 18 (36,7) 49
Follow-up 6 (25,0) 6 (25,0) 12 (50,0) 24
Exit 14 (50,0) 10 (35,7) 4 (14,2) 28
Total by arm 34 33 34 101
FET P= 0.03 Enrollment vs exit of IC vs HPV arm
Enrollment period (first six months for IC and HPV, and first 12
months for RC).
-
Worst histopathology result of biopsy by local and expert
pathologists
Julia C. Gage Juan Felix, Mario Morales, Mauricio Maza, Karla
Alfaro, Philip E. Castle, Jane Kim, Rachel Masch, Proma Paul,
Miriam Cremer. Accuracy of Histopathology in a Regional Cervical
Cancer Screening Program in El Salvador
-
Conclusions
Under routine conditions of health care services serving women
with ASC-US cytology of Medellin, compared with strategies that
include colposcopy or repeat cytology, the strategy that included
HPV testing:Detected more cases of CIN2+ at enrolmentSignificantly
reduced more health care utilization
The strategy of immediate colposcopy presented the highest
underdiagnosed of CIN2+
The underdiagnosed pathology had impact on the proper treatment
of women with CIN2+
-
Final considerations
Quality and delivery of services in unorganized screening
settings are heterogeneous
Assessment of quality of services for follow-up of screening
positives should be a requirement for implementation of new
screening technologies
Need for external assessment of Quality of Pathology Education
and enforcement for the adequate use of guidelines is also
highlighted
-
Comparison of immediate colposcopy, repeat conventional cytology
and hrHPV testing for the management of ASC-US cytology in routine
health services of
Medellin, Colombia:
The ASCUS-COL Trial: A randomized pragmatic trial
Sponsor
Primary research site
Secondary Research sitesUnidad Video Diagnstica De La Mujer
S.A.S
Competing interests: The HC2-hrHPV DNA test was donated by
QIAGEN.
Gloria I. Sanchez, MSc, PhDPrincipal Investigator
Research TeamMark Stoler, MD Phil Castle, PhD Peter Sasieni, PhD
Maribel Almonte, PhD
Rolando Herero, MD, PhD
Maria Cecilia , MD,PhD candidate
Armando Baena , MSc, PhD, current postdoct at IARC
-
Maria C Agudelo* MD, Armando Baena, PhD* Tatiana Ramirez*,
Melisa Castaeda. Infection and Cancer Group School of Medicine,
University of Antioquia, Medellin, Colombia.
David SuescunLaboratory of Pathology Suescun
Carlos BuitragoClinica Soma, Medellin, Colombia
Juan C. OchoaVideodiagnostica de la Mujer, Medellin,
Colombia
Marcela Riveros, MDDepartment of Pathology, Hospital Pablo Tobon
Uribe, Medellin, Colombia
Guadalupe Posada, MD, Luis Jaime Gomez, MDDinamica IPS,
Medellin, Colombia,
*Recipients of Fellowships for doctoral training from
COLCIENCIAS
Carolina Lopez MD, Jorge Castao MD, Miguel Roldan. MD, Mauricio
BorreroDepartments of Pathology, and Ginecology and Obstetrics,
School of Medicine, University of Antioquia, Medellin,
Colombia.
-
EFFORTS TO ADDRESS BARRIERS TO CERVICAL CANCER SCREENING IN
ETHIOPIA
Mesrach Ayalew, MPHResearch Investigator and Lecturer
St. Pauls Hospital Millennium Medical College (SPHMMC)Addis
Ababa, Ethiopia
28
-
Outline
Cervical cancer; incidence and mortality rates CC Screening in
Ethiopia, SPHMMC Findings from VIA screening- SPHMMC Why
self-collected samples?
Pilot in Addis Ababa; Self collected CC screeningData collection
device, Results
Challenges and Opportunities Future directions
Findings from a focus group discussion Potential impact
29
-
30
-
The ProblemHigh incidence of cervical cancer
high mortality from cervical cancer
Globocan: http://globocan.iarc.fr
-
32
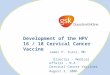
Cervical Cancer Incidence and Mortality Rates
0
5
10
15
20
25
30
Incidence Mortality
Per 1
00,0
00 w
omen
EthiopiaGuatemalaUSUKCanada
Globocan: http://globocan.iarc.fr
-
33
In a large number of countries, the majority of women have never
had a pelvic exam. This proportion is largest in Malawi, Ethiopia
and Bangladesh, where more than 90% of women report that they have
never had a pelvic exam.
PLOS Medicine, 2008
-
CC screening
34
Single visit approach (VIA), cytology Health facilities, NGO,
target groups (30-45), community mobilization (HEW)
>90% of cervical cancer is caused by HPV High-risk HPV types
16 (55.7%), 18 (8.2%), 56 (8.2%), 45 (4.1%), 39 (2.5%), 52 (1.6%),
31 (1.6%), 35 (1.6%), 58 (0.8%),
33 (0.8%), 59 (0.8%) were observed as single multiple infection
in south western Ethiopia (A. Bekele et al, 2010)
In rural parts of Ethiopia the most common genotypes of HPV are
16 (24.4%), followed by 52 (11.6%), 56 (10.5%) and 31 (10.5%)
(Sami-Ramzi et al, 2014)
-
35
Screening protocol - SPHMMC
Cervical cancer
screeningSCJ
PAP smear
Negative
Re-test in 5 years
Positive
LEEP cryotherapy
Follow-up after one yearRe-screening
-
36
191 (12 %) of the women screened for VIA had positive results
and 10 (0.6%) women with lesions suspicious for cancer. No
information on HPV rates Limited information on follow-up care
through VIA screening
VIA screening at SPHMMC
Based on logistic regression models:
women with lower education status, higher parity, and living
outside Addis Ababa have higher odds of a positive VIA result ;
adjusting for all other variables.
Odds of positive VIA result decrease by 6% for one year increase
in age at first intercourse; adjusting for all other variables.
Kebede et al (in progress)
-
Barriers to screening
37
Lack of knowledge about the need for cervical screening,
fatalistic attitudes about cervical cancer
Availability and convenience
Embarrassment or shame about having a pelvic exam, as well as
fear of the screening procedure
Previous bad experience
-
Why study self-collection?
Self-collection has never been tested in Ethiopia, effective in
other locations
Screening services may not be available or, when available, are
inaccessible, underused, or unreliable. (informal FGD)
Supplements the static approach (VIA) and hence increases the
screening coverage
Skepticism about acceptability, stigma
High rates of interest and participation (results from a pilot
study), privacy Evidence to inform policy making
-
Why..Pilot in Addis Ababa Cross sectional design, women sampled
from 3 kebeles in Addis Ababa
Women ages 20-60 recruited by health workers
Structured, quantitative interview Understanding of HPV/cervical
cancer Health beliefs Limited health history
Interviews conducted in Amharic by nurses
-
Data Collection Devices
Interview data collected through Qualtrics app
HPV samples collected using HerSwab kits Will be used to test
for HPV (14 high risk types: 16, 18, 31,
33, 35, 39, 45, 51, 52, 56, 58, 59, 66, 68)
Samples to be tested at SPHMMC
Women will be called to receive results
All women with positive results will be encouraged to attend VIA
screening clinic
-
Preliminary Results 206 women, 206 samples (July 2017); Average
age: 39.8 years (range 18
65)
16% Muslim, 73% Orthodox, 11% Protestant
11% had a previous Pap/VIA, 4% told they had an abnormal test
(40% dont remember)
Of those who did not have a Pap/VIA or did not remember: 53% of
the women reported no reason/never thought about it 34% said they
did not know or did not think they needed the test
-
Preliminary Results Majority (81%) of women believe cervical
cancer is very or extremely
serious, 78% think cervical cancer is curable with early
detection and treatment (14% did not know)
Only 40% of the women preferred to do the test at home prior to
the self swab
POST test Majority (80.6%) reported the self-test comfortable
and very comfortable,
and 90.3 % said it was easy and very easy to do the swab.
Majority (82%) preferred to test at home after the self-swab
-
Why study.self collection
FGD (CHW, Women in the community both urban and rural)
Focused on Knowledge about cervical cancer Knowledge source
Cervical cancer screening
experience Screening barriers Future self screening Screening
motivation Support system and etc.
Urban / Rural Previous experience Availability of VIA Having
children/not
having children Younger / older
43
-
Challenges for CC Screening in Ethiopia
Issues with the processing of samples/tests
Infrastructure, expertise, organization
Challenges with returning results, and follow-up of positive
tests
Complicated landscape with many small NGOs
No screening modality will be effective unless these issues are
addressed
-
Opportunities
HEP ;Deeply rooted in communities, providing primary level
preventive activities to household members
15 packages
Key players : HEW, Model families, HDA (30 HH), women focused
HDA
45
-
Future directions
46
Identify the individual stakeholders in the community (HDA)
Laboratory support
Large scale promotional activities
Phased approach (Mobile service then move to integrated
services)
Conduct both HPV and VIA screening to validate results for
community
stakeholders
-
Maintaining effective links
47
Counseling (HEW, trained HDA) and provision of Her Swab kit
(weekly HDA meet ups-Home)
Transport of self collected samples and reports (scheduled once
a week) (Laboratory to HC)
Women collect report and get treatment when indicated at the
HC
Tracking system for client who do not attend treatment or didnt
collect results (HEW-Home visit or HDA network meet ups)
Collection of screening data (HIS) and feedback from clients
-
Potential Impact Generating evidence to inform local and
regional cervical cancer prevention
and control planning
Enabling cervical cancer screening in all Ethiopian women Make
HPV self-collection a reality Set up community programs to help
facilitate self-swab HPV screening
Empowering women in Ethiopia to take care of their health and
understand risk
Further characterize HPV infection types in Addis
-
49
Thank you
-
HPV self-sampling for cervical cancer screening in indigenous
and rural
communities in Guatemala
Rafael MezaAssociate Professor
Department of EpidemiologyGlobal Public Health
University of Michigan
[email protected]; @meza_rafa
50
mailto:[email protected]
-
Cervical Cancer Incidence and Mortality Rates
0
5
10
15
20
25
Incidence Mortality
Per 1
00,0
00 w
omen
*
Guatemala
US
UK
Canada
30-35% of annual female cancers at the National Cancerology
Hospital (INCAN) in 2013
Source: INCAN cancer registry
* Luciani et al 2013
Chart1
22.35.78.87.5
12.53.132.4
Guatemala
US
UK
Canada
Per 100,000 women*
Sheet1
GuatemalaUSUKCanada
Incidence22.35.78.87.5
Mortality12.53.132.4
To update the chart, enter data into this table. The data is
automatically saved in the chart.
-
Globocan 2012
-
Cervical Cancer Screening in Guatemala
*
* American Cancer Society 2011
-
Cervical Cancer Screening in Guatemala
DHS 2014-2015, women ages 15-49 Ever Pap - 49.8 %
Ethnicity Non-indigenous women - 54.2% Indigenous women -
43.5%
Urbanicity Urban 52.8% Rural 46.9%
-
Access is only part of the equation
Quality
Follow-up
Treatment
Cervical Cancer Screening in Guatemala
-
HPV self-sampling Pap smears and VIA may not be the
most effective method for preventing cervical cancer in
indigenous and rural populations in Guatemala
Is HPV self-collection an acceptable, and perhaps more
effective, alternative to universal Pap or VIA screening in this
setting?
A priori answer: Yes, but we need to demonstrate it
-
HPV testing and self-collection >90% of cervical cancer is
caused by HPV -70% by
types 16 and 18
Sensitivity: >90% for HPV Higher sensitivity than Pap smears
(improved w/ positive HPV test) If HPV test is done first, will
miss lesions not related to HPV HPV tests have been shown to have
higher sensitivity than Pap for CIN II,
III, and cancerous lesions (relative detection rate of
1.3-2)
Specificity: Negative results signify minimal risk of disease in
next 10 years
Self-collection as effective and clinician collection
Limitations: cost and infrastructure requirements CareHPV,
Hibribio, Genexpert
-
Why more studies of self-collection? Self-testing works!
Widely
acceptable. But,
Few studies among rural/indigenous communities in Latin America
context matters
Skepticism about acceptability STD, stigma, privacy
-
Pilot Summer 2015Santiago Atitlan, Guatemala
Approximately 40,000 residents Primary language: Tzutujil
Average daily income: 4 USD Over 80% have at most primary
education
-
Methods Cross sectional design,
women proportionately sampled from 6 urban and 3 rural
neighborhoods
Women ages 18-60 recruited by community health workers
87% of interviews conducted in Tzutujil, 13% in Spanish
-
Data Collection Devices Interview data collected through
Qualtrics app
HPV samples collected using HerSwabkits
Samples shipped to Guatemala City bi-weekly for testing
Women called 10 days after collection to receive results
All women encouraged to attend local VIA screening clinic
-
HPV Testing Testing done at independent, non-profit lab
Asociacion de Salud Integral
Tested for 28 types of HPV 13 high risk types (known cervical
cancer risk factors): 16, 18,
31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68 15 low risk types
Expensive
-
Results: Self-Collection
202 women completed survey 95% of women who began the survey
completed the survey (no
major issues answering sensitive questions)
93% of women surveyed wanted to take self-swab test 88% eligible
(179 women)
100% of the women who took the test were willing to take it
again
91% of women tested called to get their results
Gotschlich et al, JGO 2017
-
Results: HPV Testing
21% tested positive for HPV17% tested positive for high-risk
HPV
Gotschlich et al, JGO 2017
-
Discussion/Conclusions < 15% of women had previously heard of
HPV
The self-swab test was found to be highly acceptable: -78% of
women found it comfortable-90% found it easy-100% were willing to
use as CC screening method
Over 80% of women said that they preferred to be screened in
their home with a self-swab kit over being screened at a doctors
office
-
Multi-Ethnic Longitudinal Study 2016-2017
Does HPV test result affect follow-up rates?
Two communities: Santiago Atitlan and Livingston Izabal
Implemented low-cost test at local lab
Follow women
-
Livingston Izabal, Guatemala
Approximately 60,000 residentsMix of Garifuna, Ladino and Qeqchi
ethnicitiesAverage income: 10 USD50% have completed at least some
secondary school
-
Recruitment
Santiago Atitlan 500 women 10 semi-structured surveys
Surveys/interviews in
Spanish and Tzutujil
Livingston Izabal 449 women
40% Indigenous, 30% Garifuna, 30% Ladino
11 semi-structured surveys
Surveys/interviews conducted in Spanish, Garifuna, and
Qeqchi
Murchland et al, under review
-
Results: Self-sampling
Santiago 2015 Santiago 2016 LivingstonWilling to self-collect*
93% 94% 53%
Collected sample 179 497 169Comfortable 78% 81% 87%Easy 90% 85%
87%Would prefer self-sampling over pap**
91% 97% 91%
Willingness to self-collect as regular screening
100% 99% 100%
* Age eligible women; ** among women who collected sample
Murchland et al, under review
-
Results
Lower willingness to self-collect in Livingtson
Literacy was significantly higher in women willing to
self-collect adjusted prevalence ratio, 1.45 [1.07-1.95]
Neither ethnicity, history of screening, nor reproductive
history were associated with the willingness to self-collect
-
Results HPV testing
Hybribio 13 (low-cost test) 19% positive samples for high-risk
HPV* No significant differences between the two
communities Women were called to return their results Provided
free access to follow-up pap/VIA to all
* Genotyping pending
-
Discussion
Generating evidence to inform local and regional cervical cancer
prevention and control planning
Enabling cervical cancer screening for indigenous/rural
women-Make HPV self-collection a reality-Set up community programs
to help facilitate self-swab HPV screening
Follow-up and access to treatment remain a challenge
independently of screening modality
-
Challenges for CC Screening in Guatemala
Access for indigenous and rural communities remains limited
Issues with the processing of samples/tests
Infrastructure, expertise, organization Need for a low-cost
widely available test Challenges with returning results, and
follow-up of positive tests
Complicated landscape with many small NGOs, plus a few large
ones and the government providing care
No screening modality will be effective unless these issues are
addressed
-
Status of CC Prevention in Guatemala
National Cervical Cancer Prevention Plan - 2014 CareHPV
Guatemala Scale-Up trial
MSPAS, Instancia por la Salud, PATH ~80K HPV tests in four urban
districts
HPV -> VIA -> Thermocoagulation MSPAS will continue, but
no major plans for expansion yet
HPV vaccination Starting Challenge of implementation
-
Other settings
Southern Thailand (preliminary data) Buddhist and Muslim
women
High acceptability: >95%
Even higher among Muslim women, who have lower screening rates
(ever pap 92% vs 73%)
100% preference over papCollaboration with Laura Rozek, Hutcha
Sriplung (PSU)
-
Acknowledgments Anna Gottschlich Audrey Murchland and Kristin
Bevilacqua Carlos Mendoza & Alvaro Rivera, INCAP Michael Dean,
NCI Gina Ogilvie, UBC Research Team:
Edwin Grajeda Andres Pineda Andree Sandoval Christian Alvarez
Regina Garca / Amanda Agustn
Community Health Workers Our participants and their communities
UM Office of Global Public Health, MCubed, CIHR CUGH, Laura Rozek,
panelists
-
Concurrent Session 09: Implementation of Cervical Cancer
Screening in Low-Resource SettingsSlide Number 2Proportion (%) of
the regional population covered by high quality cancer registration
and high quality complete vital registration of death low levels in
many global areasUnacceptably high global mortality from cervical
cancer burden in LMICsSpeakersEvaluation of quality of healthcare
delivery to prevent cervical cancer in low-resource
settingsRegional disparities of cervical cancer mortality in
LACsIntroductionIntroductionAimStudy DesignConsortData Collection
for community-based DiagnosesCumulative detection of Reviewed CIN2+
in different Health Management Organizations Use of Colposcoy by
arm and triage test result durin 24 months of women with ASCUS
cytologyComparison of total Use of Colposcoy by arm and triage test
resultInterpretations of community and Experts histology diagnosis
of cervical biopsiesReproducibility between Community and Expert
Pathologists histological Diagnosis Cumulative detection of CIN2+
by Community and Expert Pathologists diagnosis by period and arm
Treatment among women of the ASCUS-COL trial with biopsies given
the diagnosis of expert pathologistsPeriod on LEEP/LLETZ tissue
specimens during the 24 months follow-up of 2.661 women of the
ASCUS TrialWorst histopathology result of biopsy by local and
expert pathologists ConclusionsFinal considerationsComparison of
immediate colposcopy, repeat conventional cytology and hrHPV
testing for the management of ASC-US cytology in routine health
services of Medellin, Colombia:Slide Number 26EFFORTS TO ADDRESS
BARRIERS TO CERVICAL CANCER SCREENING IN ETHIOPIAOutline Slide
Number 30The ProblemSlide Number 32Slide Number 33CC screening
Slide Number 35VIA screening at SPHMMCBarriers to screening Why
study self-collection?Why..Pilot in Addis AbabaData Collection
DevicesPreliminary ResultsPreliminary ResultsWhy study.self
collection Challenges for CC Screening in EthiopiaOpportunities
Future directions Maintaining effective links Potential ImpactSlide
Number 49HPV self-sampling for cervical cancer screening in
indigenous and rural communities in GuatemalaSlide Number 51Slide
Number 52Cervical Cancer Screening in GuatemalaCervical Cancer
Screening in GuatemalaCervical Cancer Screening in GuatemalaHPV
self-sampling HPV testing and self-collectionWhy more studies of
self-collection?Pilot Summer 2015MethodsData Collection DevicesHPV
TestingResults: Self-CollectionResults: HPV
TestingDiscussion/ConclusionsMulti-Ethnic Longitudinal Study
2016-2017Livingston Izabal, GuatemalaSlide Number
68RecruitmentResults:
Self-samplingResultsResultsDiscussionChallenges for CC Screening in
GuatemalaStatus of CC Prevention in GuatemalaOther
settingsAcknowledgments Slide Number 78Slide Number 79