Embed Size (px)
Citation preview
Conducting an Exposure Assessment Evaluation Issues Relevant to the Military and Veteran Population
Omowunmi (‘Wunmi) Osinubi, MD, MSc, MBA, FRCA, ABIHM Occupational & Environmental Health Physician War Related Illness and Injury Study Center
August 2013
VETERANS HEALTH ADMINISTRATION
Purpose of Exposure Evaluation
• Better understanding of Veteran’s exposure concerns
• Evaluate relationship between exposures and health conditions
• Opportunity for patient education
• Inform diagnostic assessment
1
VETERANS HEALTH ADMINISTRATION
Occupational and Environmental Exposures in the Context of Military Service
What does it mean to be a Veteran?
ASK ▪ LISTEN ▪ LEARN 2

VETERANS HEALTH ADMINISTRATION
Cultural Competency
What is the military?
• “Not just a job, a way of life.”
• Duty ▪ Honor ▪ Courage
• Service to Country
• A Vet is a Vet
• History and Purpose
• Organizations:
– Army
– Marine Corps
– Air Force
– Navy
– Coast Guard
3
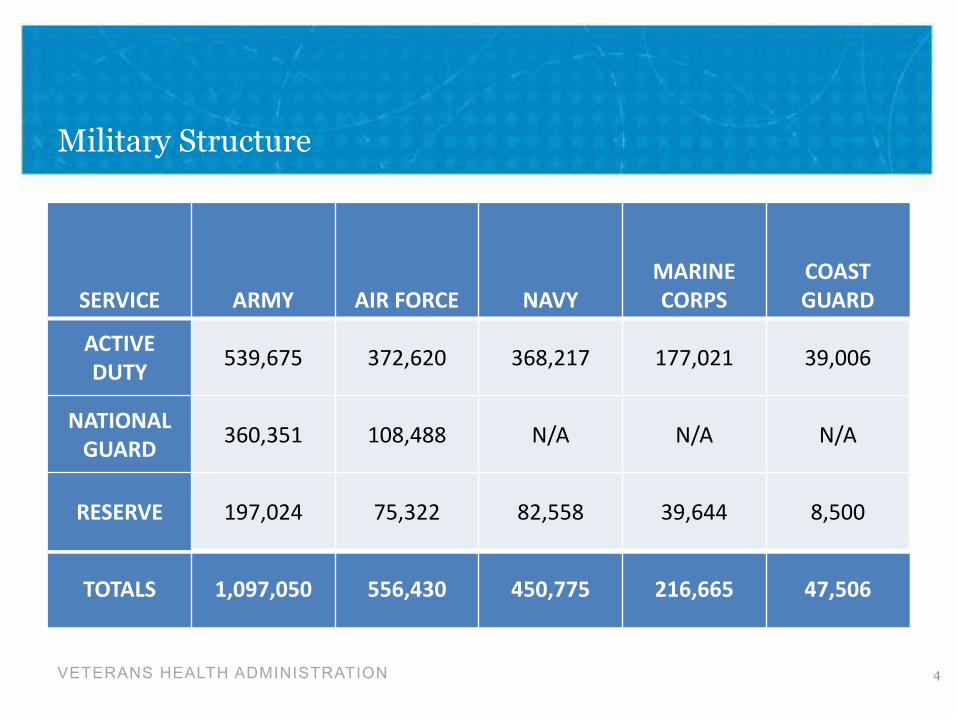
Military Structure
SERVICE ARMY AIR FORCE NAVY MARINE CORPS
COAST GUARD
ACTIVE DUTY 539,675 372,620 368,217 177,021 39,006
NATIONAL GUARD 360,351 108,488 N/A N/A N/A
RESERVE 197,024 75,322 82,558 39,644 8,500
TOTALS 1,097,050 556,430 450,775 216,665 47,506
4 VETERANS HEALTH ADMINISTRATION
VETERANS HEALTH ADMINISTRATION
Differences Between the Conflicts: Stressors
• Volunteer vs. Draft
• Lengthy or Multiple Deployments
• Technology
• Civilian Support
• Threats
• Media
• Casualties
5
VETERANS HEALTH ADMINISTRATION
Today’s Military Demographics in Comparison to the Draft Population
• Average age is older
• Educational backgrounds – higher percent college graduates,
high school/GED requirement
• Marital status (percent married higher)
• Heritage: Family history of military service that may span
multiple generations
6
VETERANS HEALTH ADMINISTRATION
Environmental Exposure Assessment Step by Step “How To”
• Introduction: Display empathy and care for the Veteran to
establish trust and credibility. Tell the Veteran upfront that you
will be honest - explaining what you do and don't know. Listen
actively and patiently.
• Explanation of plan: Describe how you'll conduct the
assessment to give the Veteran some "control" and make them
a partner in the assessment. Think about the fact that this is a
Veteran who is trained to listen to authority but may feel like
they have had that trust violated.
• Basic toxicology: Explain the need for a route of exposure and
for a temporal relationship between exposure and effect.
Explaining this in the generic sense may make discussions of
specific exposures much easier for the Veteran to understand.
7
VETERANS HEALTH ADMINISTRATION
Environmental Exposure Assessment Step by Step “How To” (cont’d.)
• Exposure history pre-enlistment/pre-deployment: Ask about location of birth,
residencies, environment, schooling, neighborhood exposures, hobbies, travel,
summer activities, and all jobs, etc.
• Exposure history during deployment: (Stay tuned)
• Exposure history post-deployment: Same issues as in pre-deployment exposure
history. Ask about multiple deployments. Include treatments for conditions which
began post-deployment.
• Exposure history post-separation: Again ask about residencies, hobbies, travel,
employment, etc. Many Veterans become government contractors with the same
types of exposures as when they were active duty.
8
VETERANS HEALTH ADMINISTRATION
Environmental Exposure Assessment Specific Concerns Related to Deployment
• This is what the Veteran came to talk about.
– Time, duration and location of deployment(s)
• In area of hostilities? (Under fire and/or fired weapon)
– Chemical weapons/alarms? (use of MOPP gear/gas mask – for how long?)
– Prophylactic medicines? (anti-malarials, nerve agent antidotes)
– Biological weapons
– Sanitation during deployment? (illness while in theater)
– Chemical exposures? (solvents/petrochemicals/pesticides/herbicides, etc.)
– Exposures to body fluids/dead bodies? (mass graves, etc.)
– Exposure to air pollution – general or a specific factory, e.g., cement/asbestos dust?;
burn pits smoke? sand/dust storms?
– Insects/arthropods/bugs, including flies?
9
VETERANS HEALTH ADMINISTRATION
I was exposed to DU
radiation, oil well fires,
sand/dust storms; there were
nerve gas alarms; I took
nerve pills, got the anthrax
shots and other unknown
hazards ……I think I have Gulf
War Illness.
Environmental Exposure Assessment Case #1: 55year old Gulf War Army Veteran (GW)
• What exposures are the
specific exposures that
the Veteran is concerned
about?
– Prioritize and rank
exposures of concern
• Address each specific
exposure related to his
deployment/military
service
• Ask about “other
exposures”
– Veteran is a partner in
the process
10
VETERANS HEALTH ADMINISTRATION
Addressing Specific Exposures of Concern: How to Elicit, Assess, and Find Information
11
Exposure Assessment Important Elements
Who Where When How What Why
VETERANS HEALTH ADMINISTRATION
Who?
• Who was exposed?
– Vietnam Veteran and Agent Orange exposure Boots on the ground in Vietnam
• Did others have similar exposures and outcomes?
Korean demilitarized zone
Thailand military bases
Brown Water Veterans
• Any pre-existing conditions/exposures that would place the exposed at greater risk
of disease development?
– Yes, he had exposures to solvents possibly contaminated with benzene
• Increased risk for leukemia with/or without Agent Orange exposure
12
VETERANS HEALTH ADMINISTRATION
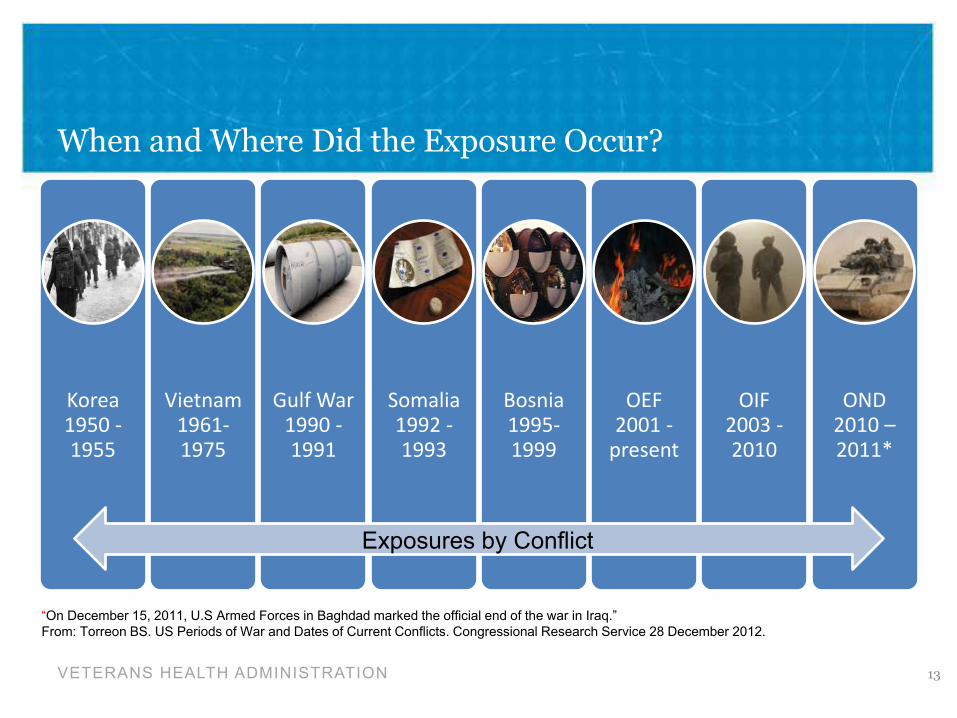
When and Where Did the Exposure Occur?
Korea 1950 -1955
Vietnam 1961-1975
Gulf War 1990 -1991
Somalia 1992 -1993
Bosnia 1995-1999
OEF 2001 -
present
OIF 2003 -2010
OND 2010 – 2011*
13
Exposures by Conflict
“On December 15, 2011, U.S Armed Forces in Baghdad marked the official end of the war in Iraq.” From: Torreon BS. US Periods of War and Dates of Current Conflicts. Congressional Research Service 28 December 2012.
VETERANS HEALTH ADMINISTRATION
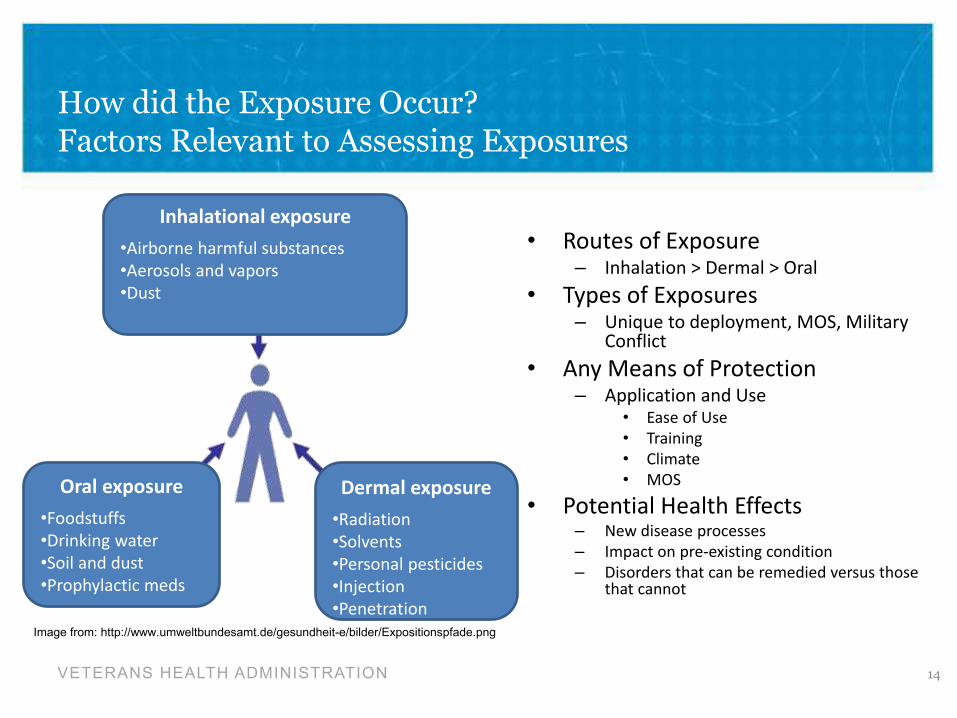
How did the Exposure Occur? Factors Relevant to Assessing Exposures
Inhalational exposure
•Airborne harmful substances
•Aerosols and vapors
•Dust
Oral exposure •Foodstuffs
•Drinking water
•Soil and dust
•Prophylactic meds
Dermal exposure •Radiation
•Solvents
•Personal pesticides
•Injection
•Penetration
Image from: http://www.umweltbundesamt.de/gesundheit-e/bilder/Expositionspfade.png
• Routes of Exposure – Inhalation > Dermal > Oral
• Types of Exposures – Unique to deployment, MOS, Military
Conflict
• Any Means of Protection – Application and Use
• Ease of Use
• Training
• Climate
• MOS
• Potential Health Effects – New disease processes
– Impact on pre-existing condition
– Disorders that can be remedied versus those that cannot
14
What Was the Exposure? Case Study #2: OEF/OIF Veteran
• What is respirable dust and was our OEF/OIF Veteran exposed?
• What sizes should be of concern when considering the upper airways, lower airways?
15
I’m in limbo….My breathing problems
are changing my life…I don’t understand
what’s going on……I’m going through a
tough time….But that doesn’t mean that
I’m crazy.
VETERANS HEALTH ADMINISTRATION
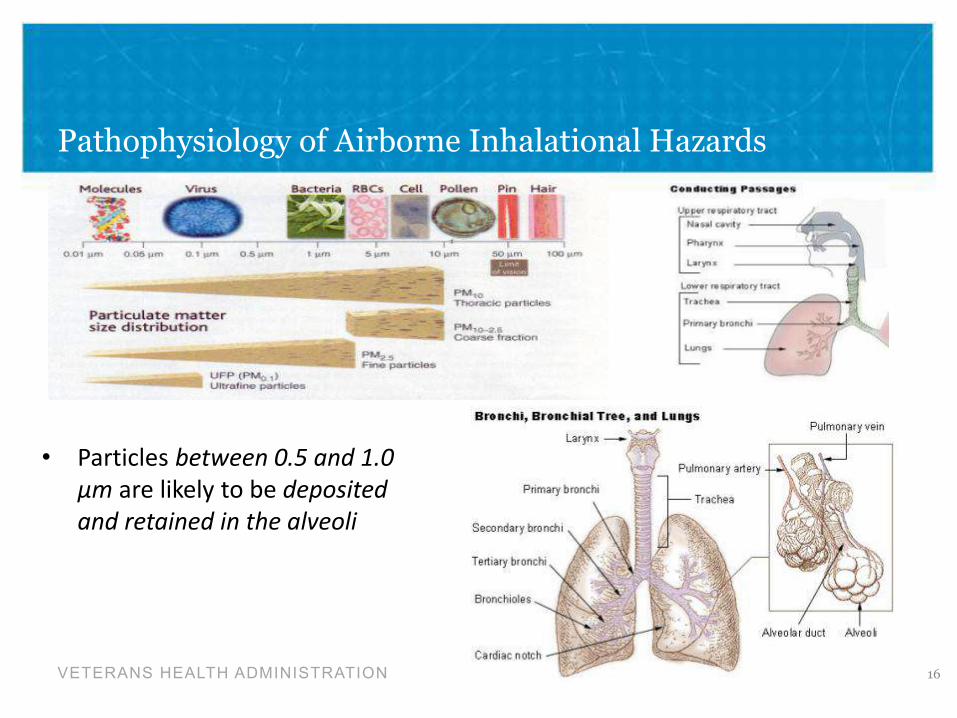
Pathophysiology of Airborne Inhalational Hazards
• Particles between 0.5 and 1.0
µm are likely to be deposited
and retained in the alveoli
VETERANS HEALTH ADMINISTRATION 16
VETERANS HEALTH ADMINISTRATION
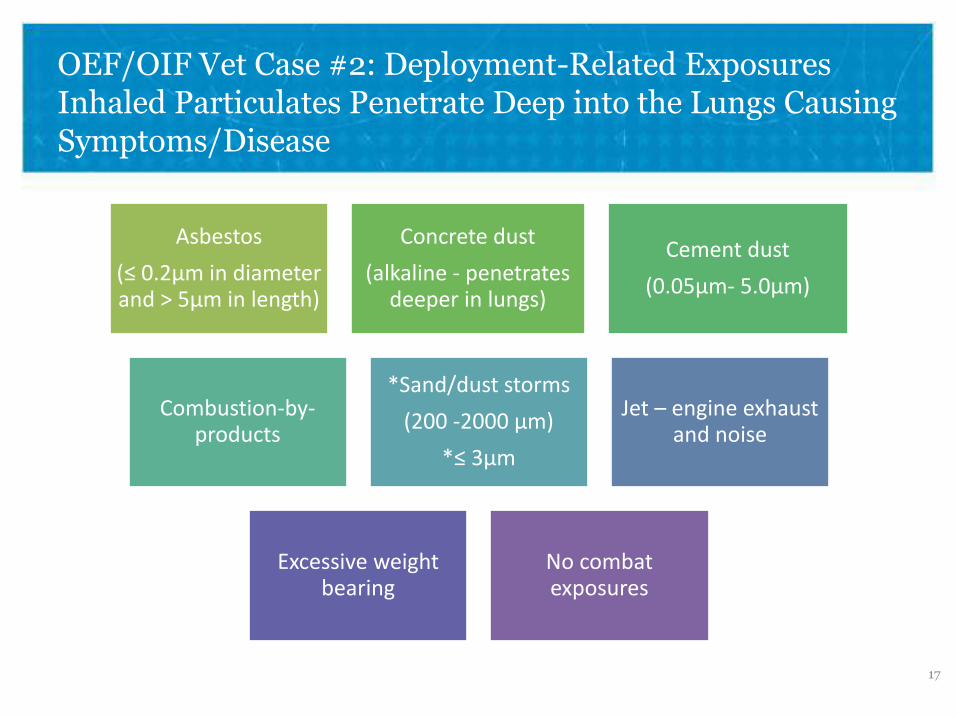
OEF/OIF Vet Case #2: Deployment-Related Exposures Inhaled Particulates Penetrate Deep into the Lungs Causing Symptoms/Disease
Asbestos
(≤ 0.2μm in diameter and > 5μm in length)
Concrete dust
(alkaline - penetrates deeper in lungs)
Cement dust
(0.05μm- 5.0μm)
Combustion-by-products
*Sand/dust storms
(200 -2000 μm)
*≤ 3μm
Jet – engine exhaust and noise
Excessive weight bearing
No combat exposures
17
VETERANS HEALTH ADMINISTRATION
Why Did Exposure Occur? Rationale for Military Vaccinations
• Important for military force health
protection in peacetime and in war
• Protect troops from:
– Infectious diseases that are common
to US populations
– Serious/deadly infectious diseases in
deployment situations
– Biological warfare agents
18
VETERANS HEALTH ADMINISTRATION
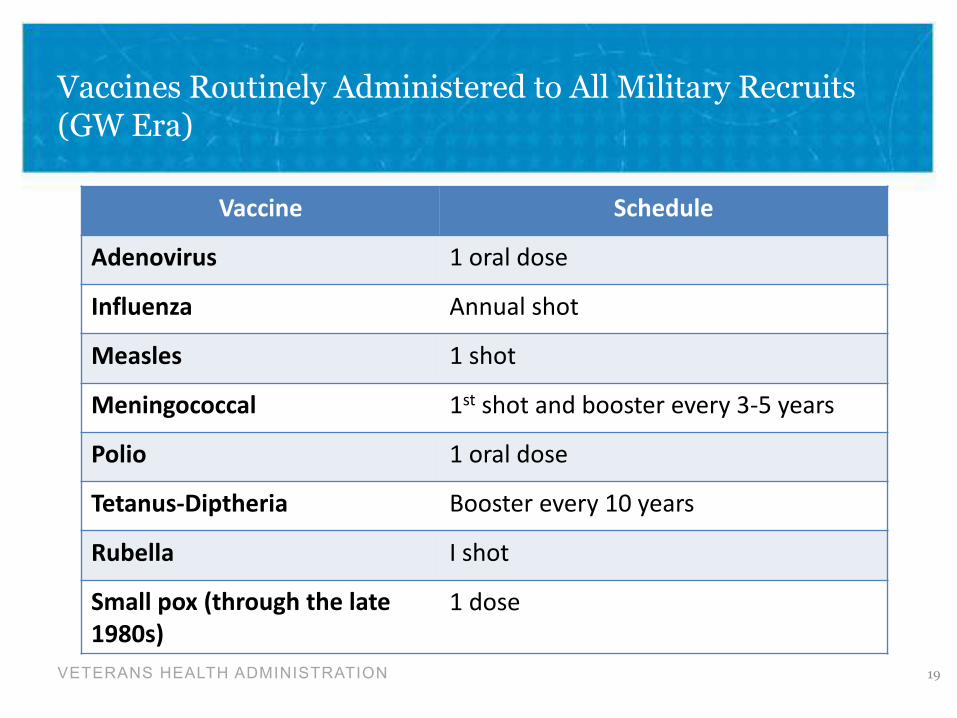
Vaccines Routinely Administered to All Military Recruits (GW Era)
Vaccine Schedule
Adenovirus 1 oral dose
Influenza Annual shot
Measles 1 shot
Meningococcal 1st shot and booster every 3-5 years
Polio 1 oral dose
Tetanus-Diptheria Booster every 10 years
Rubella I shot
Small pox (through the late 1980s)
1 dose
19
VETERANS HEALTH ADMINISTRATION
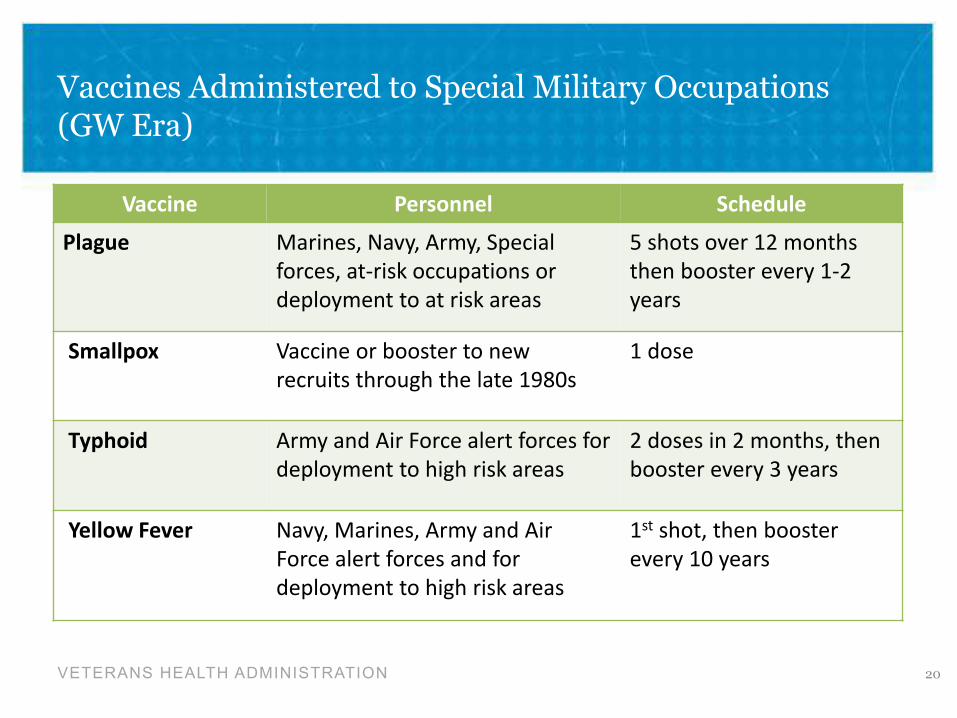
Vaccines Administered to Special Military Occupations (GW Era)
Vaccine Personnel Schedule
Plague Marines, Navy, Army, Special
forces, at-risk occupations or
deployment to at risk areas
5 shots over 12 months
then booster every 1-2
years
Smallpox Vaccine or booster to new
recruits through the late 1980s
1 dose
Typhoid Army and Air Force alert forces for
deployment to high risk areas
2 doses in 2 months, then
booster every 3 years
Yellow Fever Navy, Marines, Army and Air
Force alert forces and for
deployment to high risk areas
1st shot, then booster
every 10 years
20
VETERANS HEALTH ADMINISTRATION
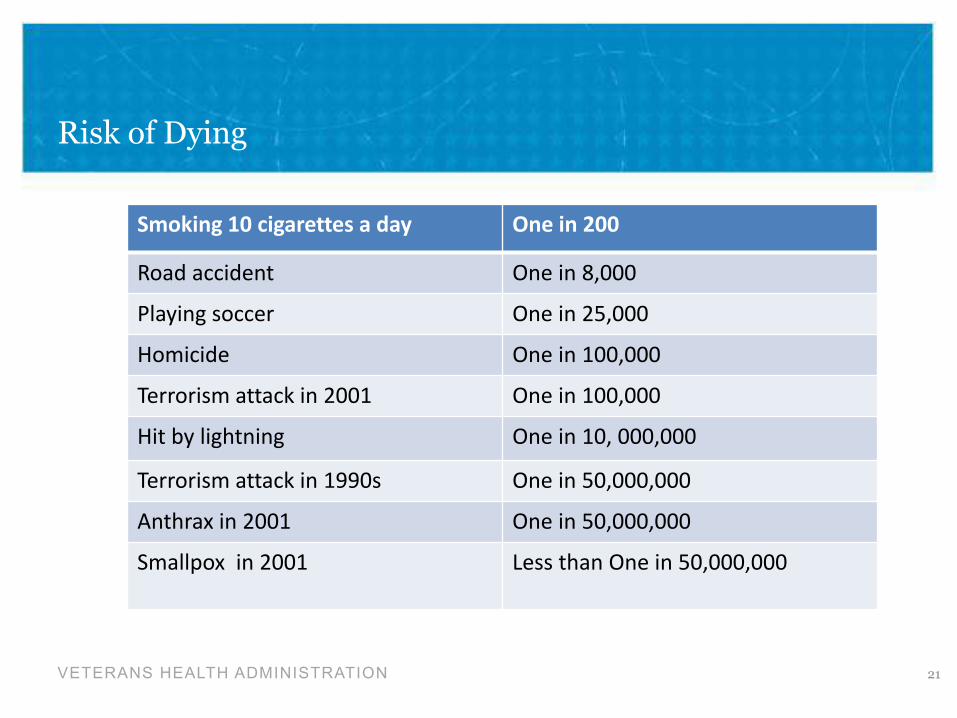
Risk of Dying
21
Smoking 10 cigarettes a day One in 200
Road accident One in 8,000
Playing soccer One in 25,000
Homicide One in 100,000
Terrorism attack in 2001 One in 100,000
Hit by lightning One in 10, 000,000
Terrorism attack in 1990s One in 50,000,000
Anthrax in 2001 One in 50,000,000
Smallpox in 2001 Less than One in 50,000,000
VETERANS HEALTH ADMINISTRATION
Biological Weapons (BWs)
• Biological warfare
– Dispersal of biological agents including microbes and/or their
toxins to cause widespread illness, death and/or terror.
• Characteristics of BWs
– Low visibility and high potency
– Substantial accessibility and easy delivery
• Since 1980s terrorist organizations have become users of biological
agents
• Iraq began an offensive BWs program in 1985
– After the Persian Gulf War, Iraq disclosed that it had bombs, Scud
missiles, 122-mm rockets, and artillery shells armed with
botulinum toxin, anthrax and aflatoxin.
– Spray tanks fitted aircrafts that could distribute 2000 L of BWs
over a target
22
VETERANS HEALTH ADMINISTRATION
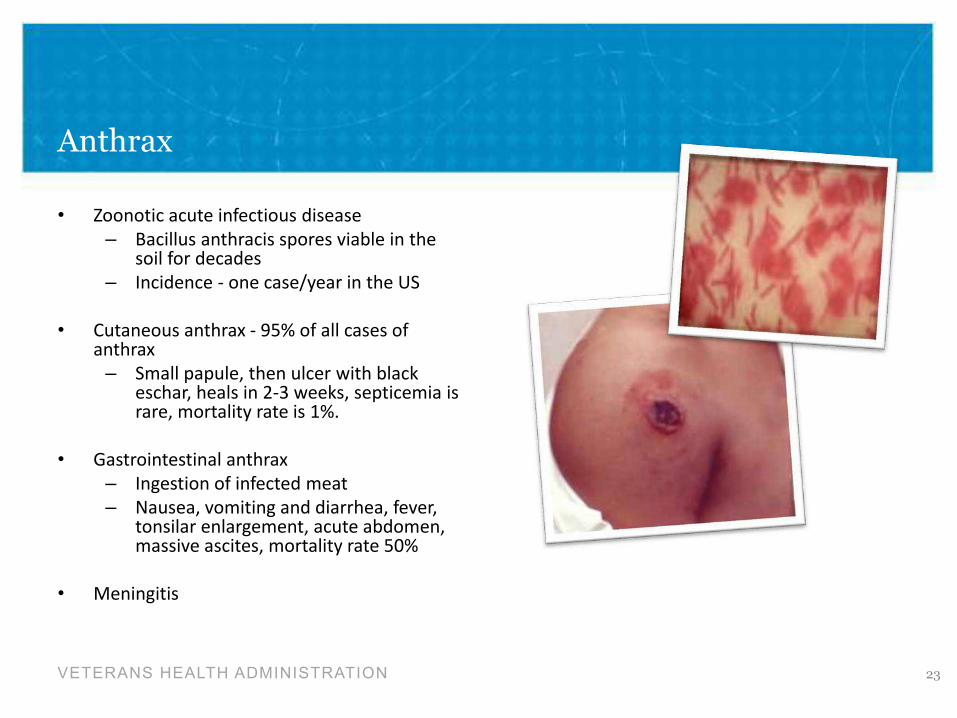
Anthrax
• Zoonotic acute infectious disease
– Bacillus anthracis spores viable in thesoil for decades
– Incidence - one case/year in the US
• Cutaneous anthrax - 95% of all cases of anthrax
– Small papule, then ulcer with blackeschar, heals in 2-3 weeks, septicemia is rare, mortality rate is 1%.
• Gastrointestinal anthrax
– Ingestion of infected meat
– Nausea, vomiting and diarrhea, fever,tonsilar enlargement, acute abdomen,massive ascites, mortality rate 50%
• Meningitis
23
VETERANS HEALTH ADMINISTRATION
Pulmonary Anthrax -“Woolsorter’s Disease”
– Inhalational anthrax is the most likely form of disease to
follow military or terrorist attack
• Such an attack likely will involve aerosolized delivery of
anthrax spores
– Fever, malaise, fatigue, myalgia, respiratory distress which
may be followed by onset of shock and death within 24-36
hours
– Mortality rate is 80-90%, but may approach 100% if septic
shock
– Of the 11 cases of inhalational anthrax in the 2001
bioterrorism attacks in the US, only 6 patients survived (65%
survival rate)
24
VETERANS HEALTH ADMINISTRATION
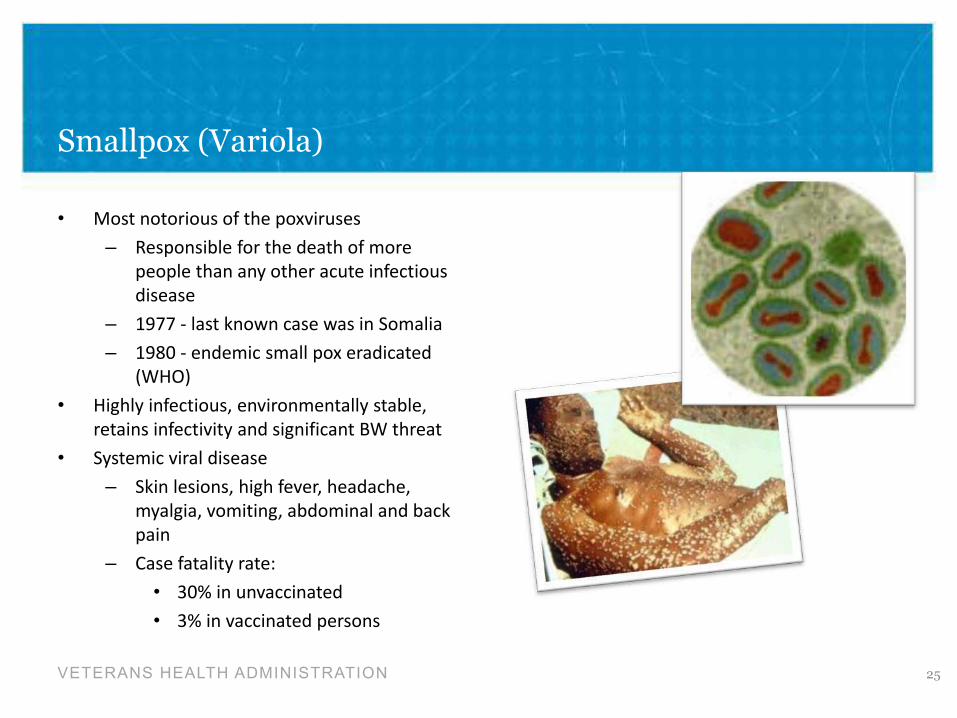
Smallpox (Variola)
• Most notorious of the poxviruses
– Responsible for the death of more
people than any other acute infectious
disease
– 1977 - last known case was in Somalia
– 1980 - endemic small pox eradicated
(WHO)
• Highly infectious, environmentally stable,
retains infectivity and significant BW threat
• Systemic viral disease
– Skin lesions, high fever, headache,
myalgia, vomiting, abdominal and back
pain
– Case fatality rate:
• 30% in unvaccinated
• 3% in vaccinated persons
25
VETERANS HEALTH ADMINISTRATION
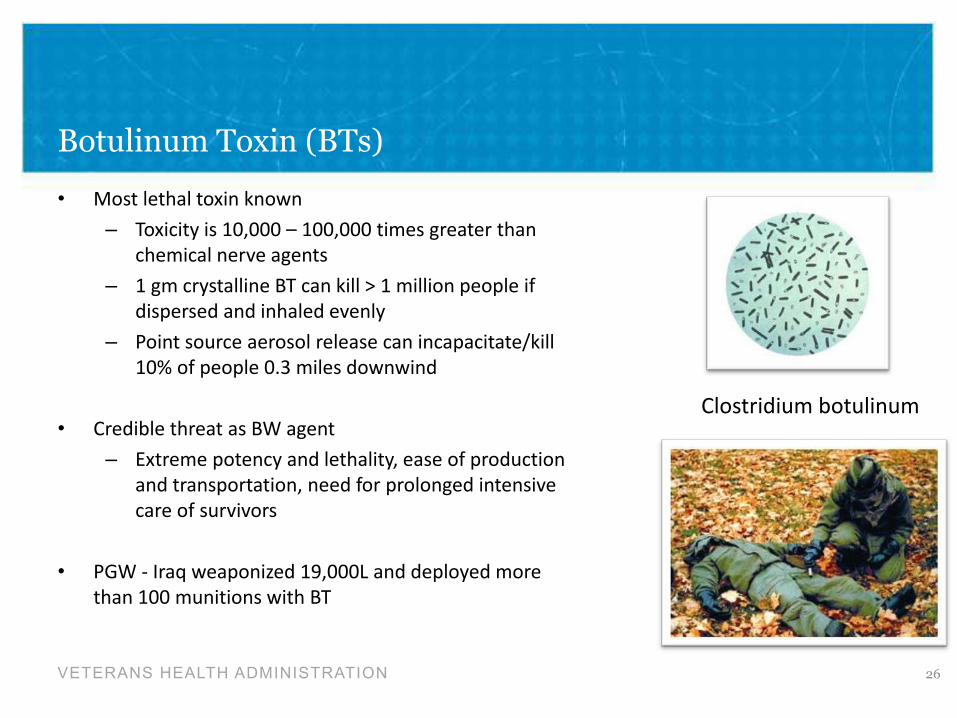
Botulinum Toxin (BTs)
• Most lethal toxin known
– Toxicity is 10,000 – 100,000 times greater than
chemical nerve agents
– 1 gm crystalline BT can kill > 1 million people if
dispersed and inhaled evenly
– Point source aerosol release can incapacitate/kill
10% of people 0.3 miles downwind
• Credible threat as BW agent
– Extreme potency and lethality, ease of production
and transportation, need for prolonged intensive
care of survivors
• PGW - Iraq weaponized 19,000L and deployed more
than 100 munitions with BT
Clostridium botulinum
26
VETERANS HEALTH ADMINISTRATION
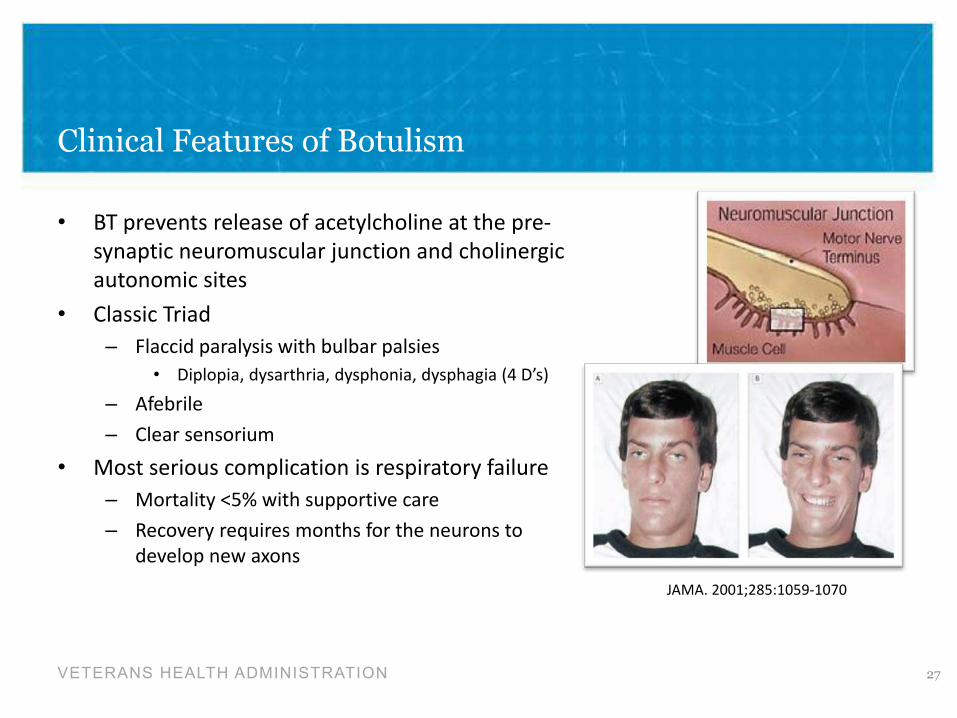
Clinical Features of Botulism
• BT prevents release of acetylcholine at the pre-
synaptic neuromuscular junction and cholinergic
autonomic sites
• Classic Triad
– Flaccid paralysis with bulbar palsies
• Diplopia, dysarthria, dysphonia, dysphagia (4 D’s)
– Afebrile
– Clear sensorium
• Most serious complication is respiratory failure
– Mortality <5% with supportive care
– Recovery requires months for the neurons to
develop new axons
JAMA. 2001;285:1059-1070
27
VETERANS HEALTH ADMINISTRATION
Mandatory Bio-warfare Military Vaccines: So Why Did the Exposure Occur?
28
VETERANS HEALTH ADMINISTRATION
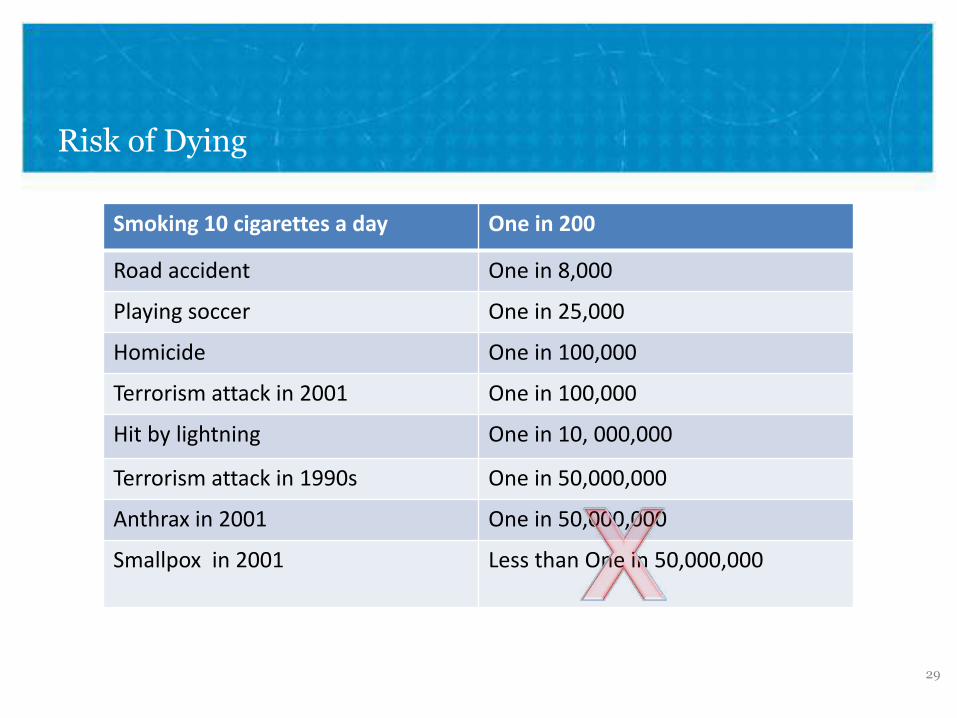
Risk of Dying
Smoking 10 cigarettes a day One in 200
Road accident One in 8,000
Playing soccer One in 25,000
Homicide One in 100,000
Terrorism attack in 2001 One in 100,000
Hit by lightning One in 10, 000,000
Terrorism attack in 1990s One in 50,000,000
Anthrax in 2001 One in 50,000,000
Smallpox in 2001 Less than One in 50,000,000
29
VETERANS HEALTH ADMINISTRATION
Vaccination Adverse Effects
• No immunization is completely safe
• Some Servicemembers who received these vaccines have developed medical
conditions which they are attributing to vaccines
– Migraines, heart problems, diabetes
– Multiple sclerosis, neuropathies, medically unexplained gastrointestinal, neuromuscular
and musculoskeletal problems
• Questions have been raised about effects of receiving multiple vaccinations over a
short period of time versus reaction to any single vaccine
• Case reports of similar health problems in soldiers who received the vaccines but
did not actually deploy
30
VETERANS HEALTH ADMINISTRATION
Smallpox Vaccine
• Vaccination is safe and effective for most people
– Mild symptoms
• Local soreness and redness
• Enlarged regional lymph nodes
• Low fever
– 1 out of 3 people may feel unwell enough to miss work
• Serious reactions
– Vaccinia rash - localized or widespread (generalized vaccinia)
– Toxic allergic rash to the vaccine (erythema multiforme)
– 1 in 1000 recipients
31
VETERANS HEALTH ADMINISTRATION
Smallpox Vaccine (cont’d.)
• Life-threatening reactions
– Eczema vaccinatum
• Widespread severe skin infection in persons with eczema or atopic dermatitis
– Vaccinia necrosum
• Extensive tissue destruction leading to death
– Post-vaccinal encephalitis
• More recent developments
– Causal association between vaccination and myocarditis
– Angina and heart attack have been reported post-vaccination
– Persons with post-vaccination chest pain, shortness of breath or cardiac disease must
seek medical attention ASAP
32
VETERANS HEALTH ADMINISTRATION
Anthrax Vaccine (Gulf War)
• AVA was licensed in 1970
– Alumnium hydroxide-adsorbed preparation
• Vaccination series comprised 6 subcutaneous injections over 18 months
– 0, 2 and 4 weeks; 6, 12 and 18 months; annual boosters
• There was not enough time or adequate AVA supplies to vaccinate all the troops in
time for deployment
– 41% of all US vets; 30% of Navy Seabees reported receiving AVA
33
VETERANS HEALTH ADMINISTRATION
AVA – Public Perception
• Media controversy and public debate fueled by several factors
– ? Efficacy against inhalational anthrax
– ? Manufacturing quality control problems
– ? Short and long-term side effects
– ? Vaccine components and adjuvants
• “Squalene” vs Aluminium hydroxide hypotheses
– ? Military policies that first mandated vaccinations, punished refusals for vaccinations
and later retracted mandatory vaccination
– ? Indications for vaccinations was not uniformly applied
– ? Vaccinations performed in “secrecy”, inadequate informed consent, and incomplete
documentation of anthrax vaccinations
– ? Variability in vaccines used
• Differences in vaccines used prior to the 1970s versus Gulf war vaccines
• Differences in US versus UK military vaccines
• Differences in reactions/adverse effects associated with different lots of the AVAs
34
With Permission -http://www.johnlund.com/page.asp?ID=2154
35
VETERANS HEALTH ADMINISTRATION
Questions About Military Vaccinations?
• Vaccine HealthCare Centers Network
– Walter Reed Regional Vaccine Healthcare Center (Bethesda/Ft. Belvoir).
– Fort Bragg Regional Vaccine Healthcare Center, NC
– Wilford Hall Regional Vaccine Healthcare Center, Lackland AFB, TX
– Naval Medical Center Portsmouth Richard E. Shope Regional Vaccine Healthcare Center, Portsmouth, VA
• DoD Vaccine Clinical Call Center 24/7 at:
– 1-866-210-6469
– VHC Physicians with expertise in vaccinology are on-call to assist the nurses in answering patient and provider inquiries.
– http://www.vhcinfo.org
36
VETERANS HEALTH ADMINISTRATION
Other Exposures of Concern? Pesticides and Gulf War
• “On a nightly basis, we would spray our uniforms with
pesticides…. We had to hang them outside so that the excess
spray would dissipate in the air….
…The sand fleas were a problem. We used to put flea collars
around the legs of our cots, or we would put flea powder on
the floor around our cots to try to keep the sand fleas away
from us while we were sleeping…
…We slept with nets over us to keep the flies off….The flies
were ungodly” – --SSgt TS, Gulf War Veteran (GRAC Report, 2008)
37
VETERANS HEALTH ADMINISTRATION
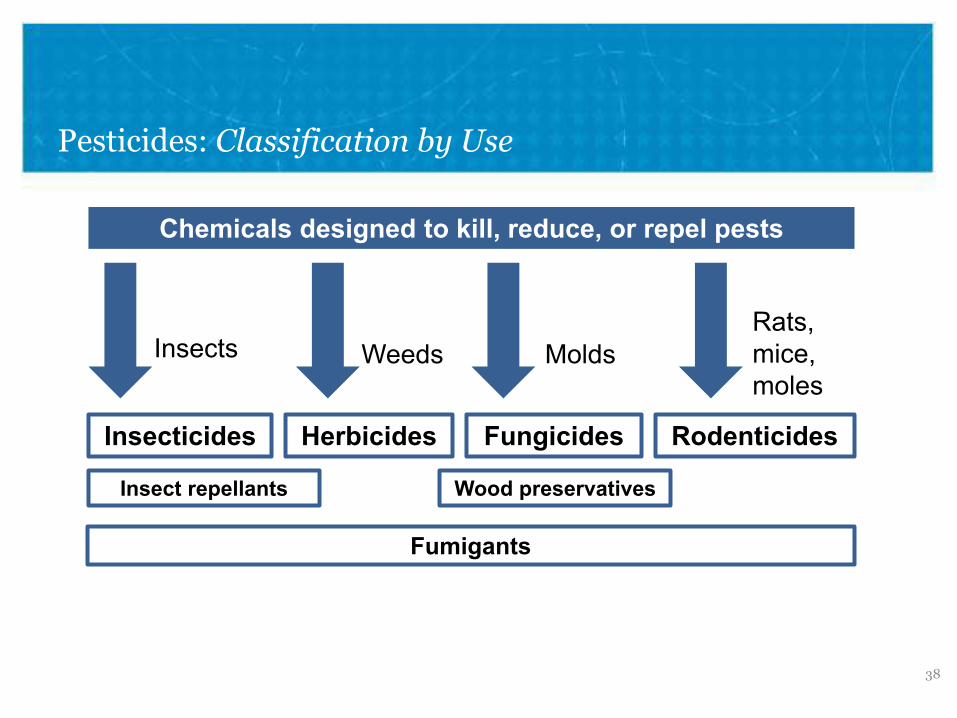
Pesticides: Classification by Use
Chemicals designed to kill, reduce, or repel pests
Insects
Insecticides
Weeds
Herbicides
Insect repellants
Molds
Fungicides
Rats, mice, moles
Rodenticides
Wood preservatives
38
Fumigants
VETERANS HEALTH ADMINISTRATION
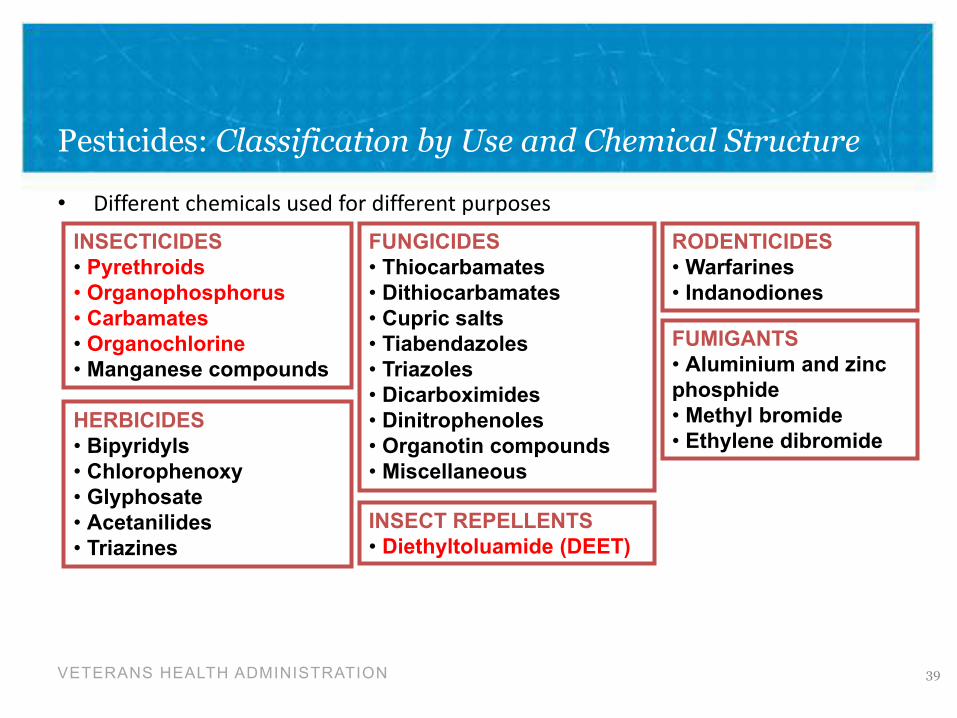
Pesticides: Classification by Use and Chemical Structure
• Different chemicals used for different purposes
INSECTICIDES
• Pyrethroids
• Organophosphorus
• Carbamates
• Organochlorine
• Manganese compounds
FUNGICIDES
• Thiocarbamates
• Dithiocarbamates
• Cupric salts
• Tiabendazoles
• Triazoles
• Dicarboximides
• Dinitrophenoles
• Organotin compounds
• Miscellaneous
RODENTICIDES
• Warfarines
• Indanodiones
HERBICIDES
• Bipyridyls
• Chlorophenoxy
• Glyphosate
• Acetanilides
• Triazines
INSECT REPELLENTS
• Diethyltoluamide (DEET)
FUMIGANTS
39
• Aluminium and zinc
phosphide
• Methyl bromide
• Ethylene dibromide
VETERANS HEALTH ADMINISTRATION
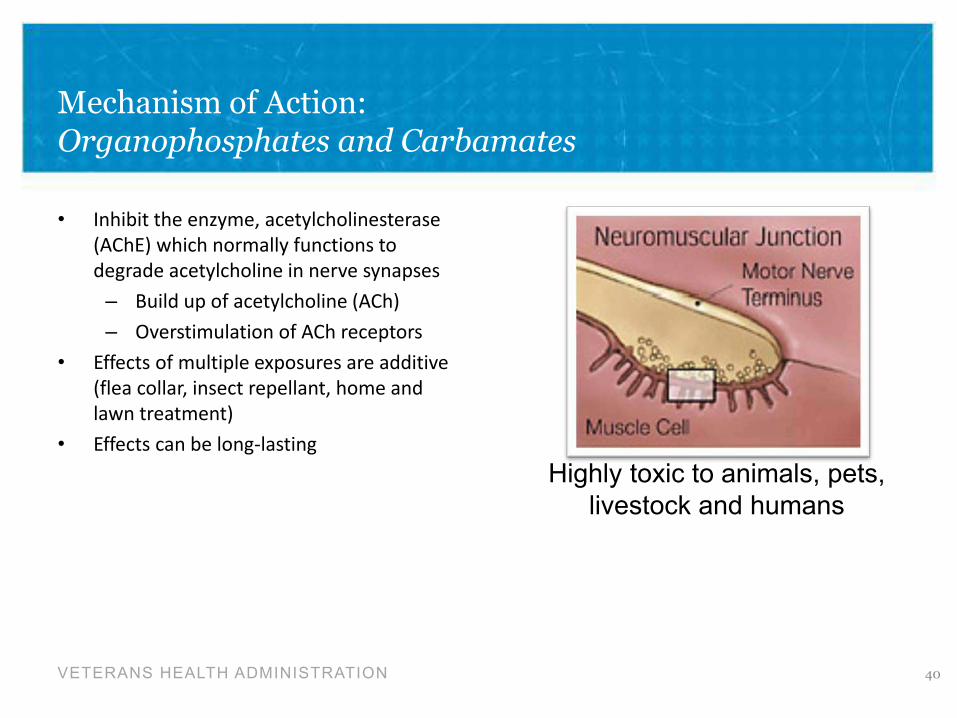
Mechanism of Action: Organophosphates and Carbamates
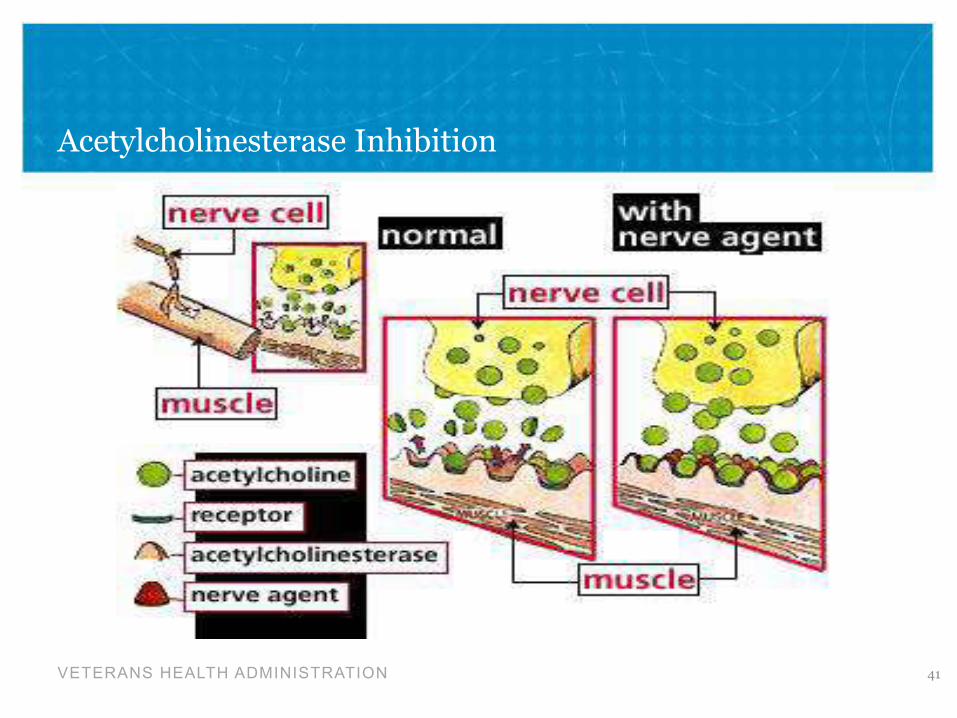
• Inhibit the enzyme, acetylcholinesterase
(AChE) which normally functions to
degrade acetylcholine in nerve synapses
– Build up of acetylcholine (ACh)
– Overstimulation of ACh receptors
• Effects of multiple exposures are additive
(flea collar, insect repellant, home and
lawn treatment)
• Effects can be long-lasting
40
Highly toxic to animals, pets, livestock and humans
VETERANS HEALTH ADMINISTRATION
Acetylcholinesterase Inhibition
41
VETERANS HEALTH ADMINISTRATION
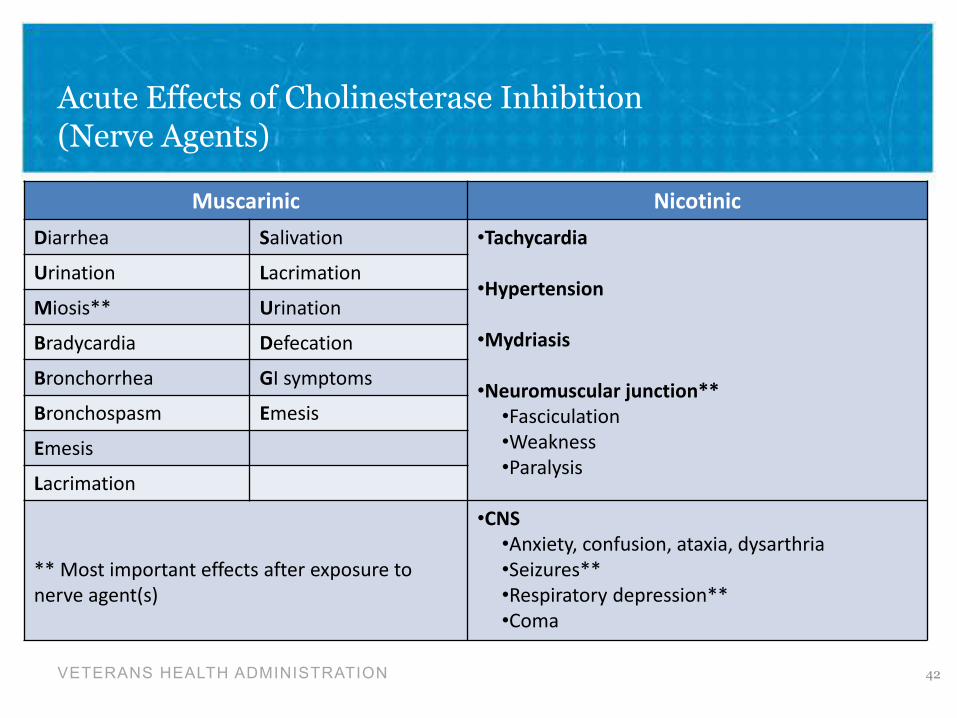
Acute Effects of Cholinesterase Inhibition (Nerve Agents)
42
Muscarinic Nicotinic Diarrhea
Urination
Miosis**
Bradycardia
Bronchorrhea
Bronchospasm
Emesis
Lacrimation
Salivation
Lacrimation
Urination
Defecation
GI symptoms
Emesis
•Tachycardia
•Hypertension
•Mydriasis
•Neuromuscular junction** •Fasciculation
•Weakness
•Paralysis
** Most important effects after exposure to
nerve agent(s)
•CNS •Anxiety, confusion, ataxia, dysarthria
•Seizures**
•Respiratory depression**
•Coma
VETERANS HEALTH ADMINISTRATION
Chronic Health Effects of Cholinesterase Inhibitors
• Organophosphate-induced delayed polyneuropathy (OPIDN)
– Occurs 2-3 weeks after exposure to large doses of OPs
– Due to inhibition of neuropathy target esterase
– Distal muscle weakness with relative sparing of the neck muscles, cranial nerves, and
proximal muscle groups
– Pathology shows dying back neuropathy of distal peripheral nerves
– Recovery can take up to 12 months
• Long term (years) work exposures (dippers/sprayers)
– Deficits in cognitive/neurobehavioral tests (memory, abstraction, sustained attention
and/or speed of information processing)
– Decreased vibrotactile sensitivity
– Normal EMGs/NCVs and neurological examination
43
VETERANS HEALTH ADMINISTRATION
Use of Pesticides in 1st Gulf War: At Least 64 Pesticides/Related Products
• Large numbers of flying and biting insects and other pests
– Environmental fogging and spraying
• Pest control important part of force protection and readiness
• Military issued pesticide creams, liquids, sprays for skin, uniforms and beddings
– Personal repellants – 33% cream or 75% liquid DEET on the skin,
– 0.5% Permathrin sprayed on uniforms
– Troops self-acquired pesticides – flea collars, citronella products, OFF, etc.
• Pest strips, baits and sprays used in living quarters
• Lindane (organochlorine) used for delousing in processing > 87,000
enemy/prisoners, distributed to US Army personnel for their use
44
VETERANS HEALTH ADMINISTRATION
Personal Repellants
• DEET (N,N-Diethyl-3-methylbenzamide)
– Developed by the US Army after WW II
• Originally tested as a pesticide on farm fields
• Entered military use in 1946, civilian use in 1957
– Protects against mosquito and tick bites
• True repellant- mosquitoes intensely dislike odor
– Prevents Lyme dx, malaria, dengue fever, etc.
– Inhibits acetylcholinesterase and potentiates carbamates
– Excessive DEET and/or concurrent pesticide exposures
• Insomnia, mood disturbance, impaired cognitive function
45
VETERANS HEALTH ADMINISTRATION
GW Pesticide Overexposures
• Pesticide overuse was common and at times extreme, particularly among ground
troops
– 62% used some form of pesticides
– 50% used DEET a median of 30X/month
– Permathrin used on uniform average almost 30X/month
• Label states spray on uniform once every 6 weeks
– 13% used pesticide sprays 50X/month
– 5% used pesticides >100X/month (>3X/day)
46
47
“It also seems reasonable that people in
environments with large numbers of insects
such as the Persian Gulf, would be tempted to
use whatever means was available to remove
pests, including using products in ways that
were not recommended.”
-RAND National Defense Research Institute, Pesticide Use During the Gulf War
VETERANS HEALTH ADMINISTRATION
Gulf War and Chemical Weapons
• “My unit arrived in the Gulf the day before the air war started. We spent about 1
month in Saudi Arabia. Our chemical alarms went off several times during that
month…we had to go to MOPP – level four...
…While in Saudi Arabia, we started taking PB pills…about 3 days after, my eyes
were jittery, my vision was jumping, I was seeing double, and I was
nauseated…
….By the 4th day, I was vomiting a little blood, so I went to sick call, they told me
to cut the dose in half…nothing to worry about…others in the unit had similar
vision problems… “
» SSgt TS, Gulf War Veteran (GRAC Report, 2008)
48
VETERANS HEALTH ADMINISTRATION
Chemical Warfare - Nerve Agents
• Acetylcholinesterases (AChE) similar to organophosphate pesticides
• Readily absorbed by inhalation, ingestion and dermal contact
• Rapidly fatal systemic effects may occur
• Most toxic chemical warfare agents
– G-Type Nerve Agents
• Clear colorless liquids, volatile at ambient temp
• Tabun (GA); Sarin (GB); Soman (GD)
– V-Type Nerve Agents
• Amber liquid, low volatility unless high temp
• VX
M190 Honest John chemical warhead section containing demonstration M134 GB (Sarin) bomblets.
49
VETERANS HEALTH ADMINISTRATION
Symptoms of Nerve Agent Exposure
• Dose dependent
• Those potentially exposed typically recall certain symptoms
associated with low to moderate level exposures.
• Symptoms secondary to mild to moderate exposure typically
resolve within weeks after exposure
• Body of literature that suggests possible long term damage
to receptors
50
VETERANS HEALTH ADMINISTRATION
Protecting Troops from Nerve Agents
51
• Chemical agent detection, alarm monitoring systems
– Detect nerve agents at levels high enough to cause symptoms
– False alarm triggers - smoke, engine exhaust, rocket/missile propellant smokes, and
electromagnetic pulse (EMP).
– Repeated false alarms →ignoring and/or disabling the systems • Personal protective equipment (MOPP)
• Nerve agent prophylaxis (PB)
• Post-exposure treatment (antidotes)
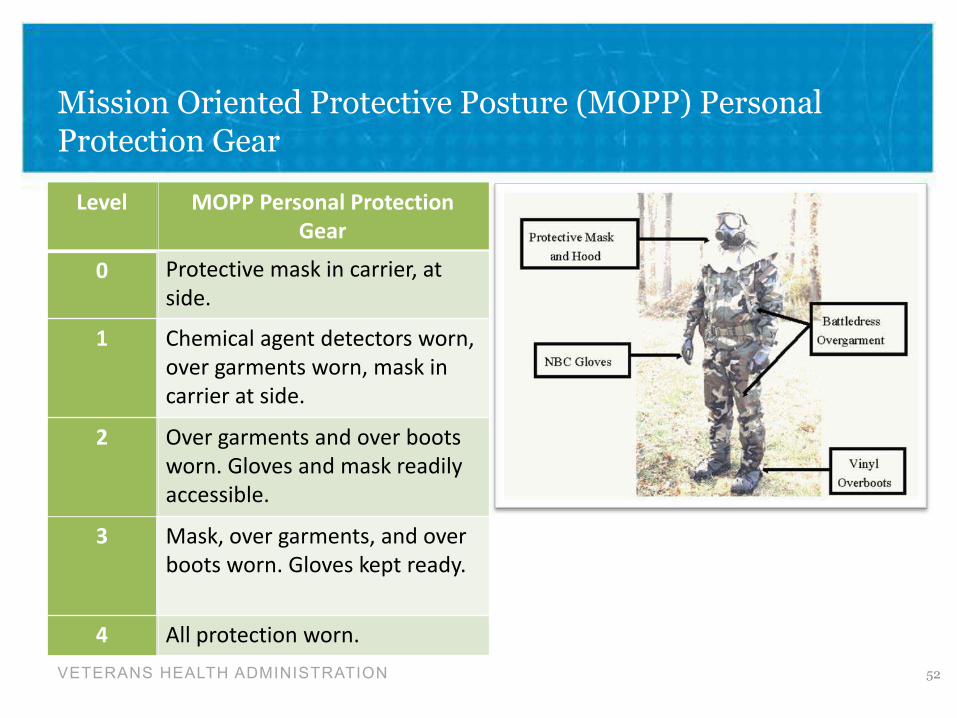
Mission Oriented Protective Posture (MOPP) Personal Protection Gear
52
Level MOPP Personal Protection Gear
0 Protective mask in carrier, at
side.
1 Chemical agent detectors worn,
over garments worn, mask in
carrier at side.
2 Over garments and over boots
worn. Gloves and mask readily
accessible.
3 Mask, over garments, and over
boots worn. Gloves kept ready.
4 All protection worn.
VETERANS HEALTH ADMINISTRATION
VETERANS HEALTH ADMINISTRATION
Nerve Agent Pyridostigmine Pretreatment (NAPP) Pills
• Active agent - Pyridostigmine bromide (“PB”)
• Distributed in 1st GW as part of 3-drug regimen to protect troops from nerve
agent poisoning
– PB - “small white pills” intended for use before nerve gas attack.
– If exposed to nerve agents, self-inject with antidotes pre-packed auto-injectors (post-exposure treatment).
• Atropine
• 2-pralidoxime chloride (2-PAM)
53
VETERANS HEALTH ADMINISTRATION
Pyridostigmine Bromide (PB) Mechanism of Action
• PB is a carbamate compound, temporarily and reversibly binds
acetylcholinesterase (AChE)
– PB pre-treatment established blood levels adequate to temporarily bind about 30% of
circulating AChE
• Protect cholinergic receptors from excess AChE build up and “rescue” AChE in order to re-
stabilize cholinergic nerve transmission after nerve agent attack
• Orders for initiating PB pretreatment issued by unit commanders
• NAPP blister packs had 21 pills
– 30 mg q8h X 7d
54
VETERANS HEALTH ADMINISTRATION
PB and GW-related Symptoms
• ACh is key regulator of muscle action, pain, mood, memory and sleep → prominent symptoms in ill GW Vets
• PB may alter regulation of ACh
– There is large individual variation in enzyme inhibition for same PB dose (15 to 25 fold
differences)
– Widespread differences in the time course of clinical and/or toxic effects of PB
• Animal studies demonstrate some long lasting/permanent effects after stopping PB
– PB toxicity may be enhanced by stress, heat, and exposures to pesticides and/or nerve
agents
• Use of PB in 1st GW associated with higher rates of side effects than commonly observed in
clinical settings
55
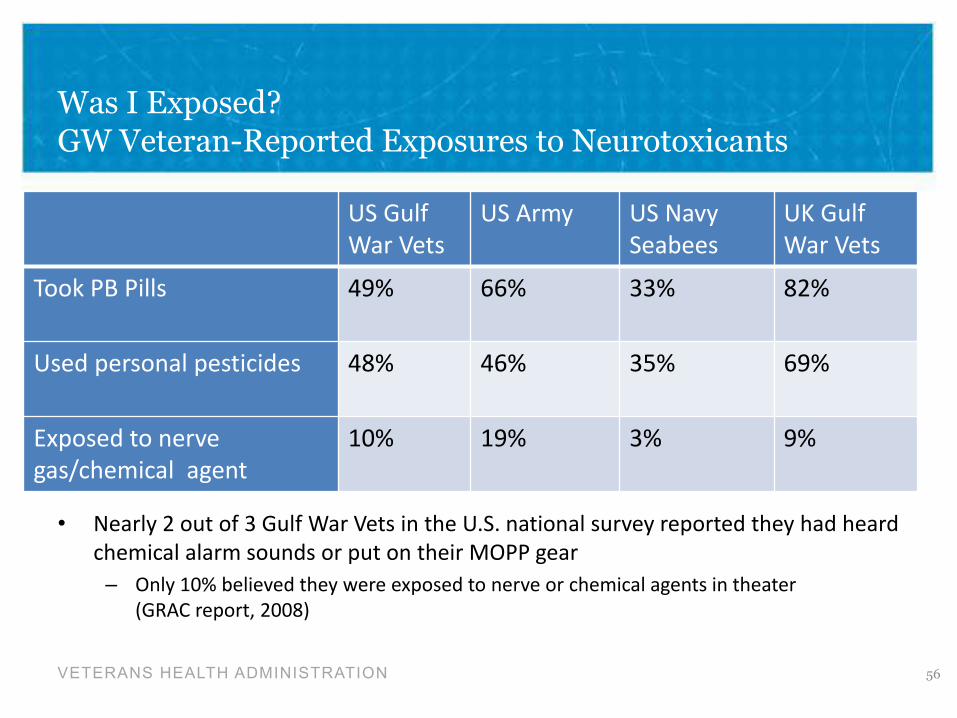
Was I Exposed? GW Veteran-Reported Exposures to Neurotoxicants
VETERANS HEALTH ADMINISTRATION
US Gulf
War Vets
US Army US Navy
Seabees
UK Gulf
War Vets
Took PB Pills 49% 66% 33% 82%
Used personal pesticides 48% 46% 35% 69%
Exposed to nerve
gas/chemical agent
10% 19% 3% 9%
56
• Nearly 2 out of 3 Gulf War Vets in the U.S. national survey reported they had heard
chemical alarm sounds or put on their MOPP gear
– Only 10% believed they were exposed to nerve or chemical agents in theater (GRAC report, 2008)
57
“We cannot rule out pyridostigmine
bromide as a possible contributor to
the increased health symptoms in
some Gulf War Veterans.”
-Golomb & Anthony RAND National Defense Research Institute
http://www.rand.org/pubs/testimonies/2005/CT164.pdf
VETERANS HEALTH ADMINISTRATION
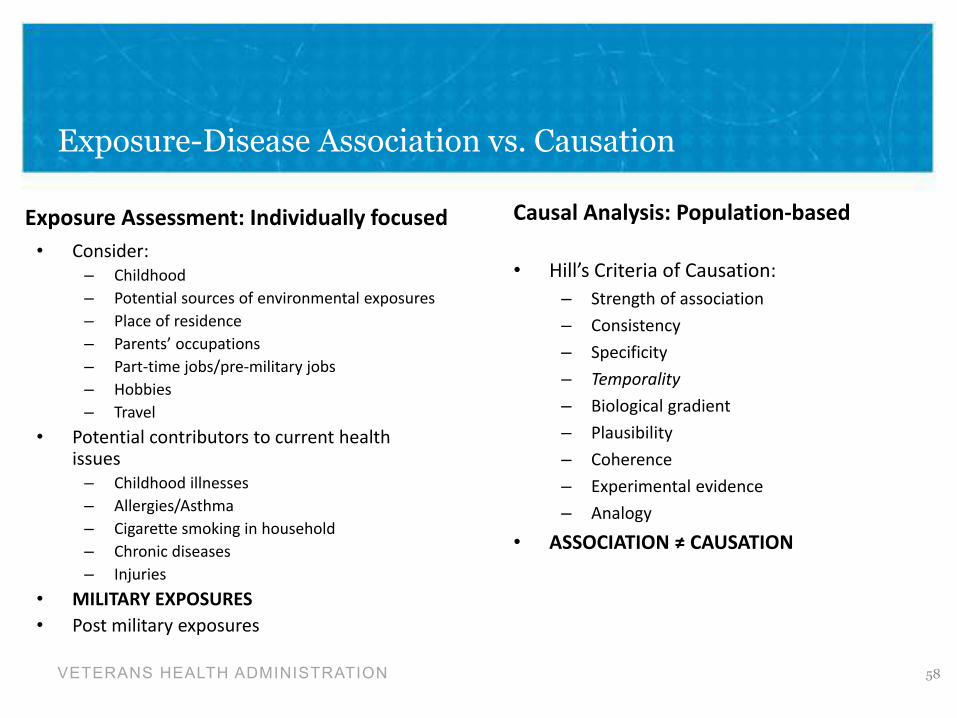
Exposure-Disease Association vs. Causation
Exposure Assessment: Individually focused • Consider:
– Childhood
– Potential sources of environmental exposures
– Place of residence
– Parents’ occupations
– Part-time jobs/pre-military jobs
– Hobbies
– Travel
• Potential contributors to current health issues
– Childhood illnesses
– Allergies/Asthma
– Cigarette smoking in household
– Chronic diseases
– Injuries
• MILITARY EXPOSURES • Post military exposures
Causal Analysis: Population-based
58
• Hill’s Criteria of Causation:
– Strength of association
– Consistency
– Specificity
– Temporality
– Biological gradient
– Plausibility
– Coherence
– Experimental evidence
– Analogy
• ASSOCIATION ≠ CAUSATION
VETERANS HEALTH ADMINISTRATION
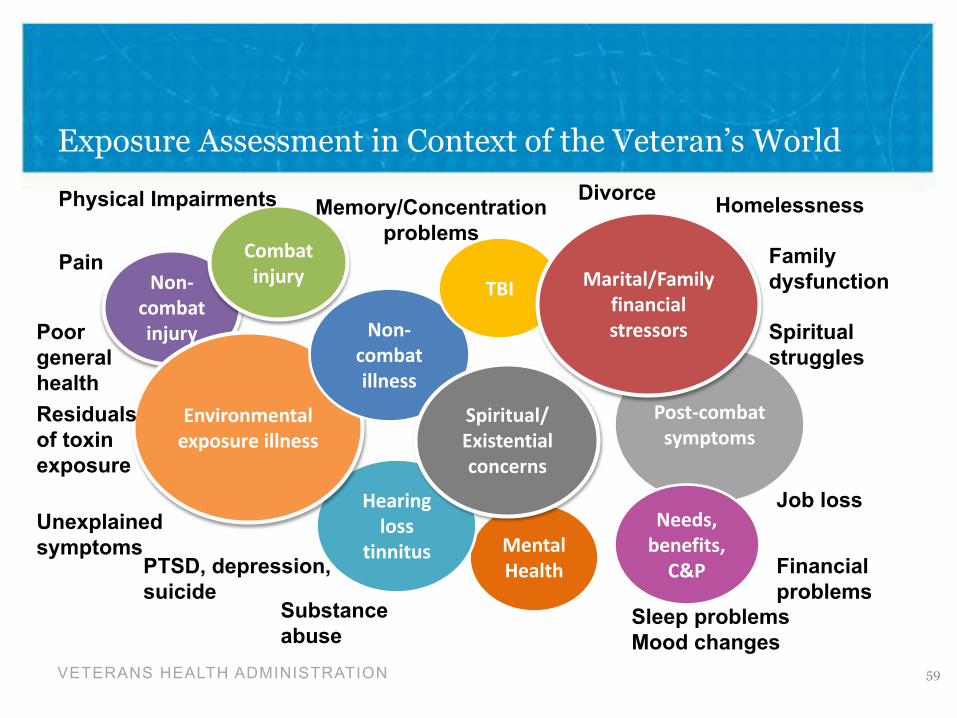
Exposure Assessment in Context of the Veteran’s World
Physical Impairments Memory/Concentration
problems
Divorce Homelessness
Pain Non-
combat injury
Combat injury TBI Marital/Family
financial stressors
Family
dysfunction
Poor
general
health
Non-combat illness
Spiritual
struggles
Residuals
of toxin
exposure
Environmental exposure illness
Spiritual/ Existential concerns
Post-combat symptoms
Unexplained
symptoms
Hearing loss
tinnitus
Job loss
PTSD, depression,
suicide
Mental Health
Needs, benefits,
C&P Financial
problems Substance
abuse Sleep problems
Mood changes
59
VETERANS HEALTH ADMINISTRATION
Addressing the (Frustrated) Veteran Goal: Impact Quality of Life
Veteran • Hostility
• Frustration
• Fear
• Unhappiness
• Pessimism
• Mistrust
• Misinformation
Clinician
60
• Empathy
• More Empathy - Let them talk
• Impact Expectations
• Hope
• Optimism
• Truth
• Educate
• Serenity Prayer Attitude
Why Should We Care About Veterans’ Exposure Concerns?
Because they cared for us.
SO WHY SHOULD WE CARE ABOUT
VETERANS’ EXPOSURE CONCERNS?
61 VETERANS HEALTH ADMINISTRATION