Embed Size (px)
Citation preview

Eliane Pedra Dias, Ana Luisa Figueira Gouvêa,Claudia Carvalhal Eyer
Condyloma acuminatum: its histopathological patternRealized at Antônio Pedro University Hospital, Department of Pathology,
Universidade Federal Fluminense - Niterói, Brazil.
Condyloma acuminatum is one of the clinicai manifestations of papillomavirus infection. The classical histopathological features arealready known and do not constitute a diagnostic problem. Clinically, it has been classified into growth or proliferative, full-expression,and regressive or persistent phases, with the histopathological aspects of these distinct phases being well documented in ~quinecutaneous papillomas. We have designed a protocol of histopathological analysis in order to investigate the possibility of identifyingthe evolutional phases in human condylomata acuminata. Sixty condylomata acuminata from the files of the Department of Pathology,Universidade Federal Fluminense, were studied regarding koilocytosis, paraceratosis, acantosis, basal cell hyperplasia and mono-nuclear cell infiltrate. After an individual analysis and comparison of the cases, the main differential aspects of condyloma acuminatumwere: koi/ocytosis, transepithelial Iymphocytic infiltrate and basal cell hyperplasia. Thus, condylomatous lesions can be histopatho-logically differentiated in three major patterns: proliferative, viral replication activity and regressive.
UNITERMS: Condyloma acuminatum, koilocytosis, histopathologic pattern, regression.
INTRODUCTION
Condyloma aculninatum represents one of the manyclinicaI manifestations of the HumanPapilIomavirus infection (HPV); it is found more
frequently in the genital region and rarely in mucousmembranes. 1-3 Frequently associated with HPV 6 and 11,the incubation period ranges from 3 weeks to 8 monthsand occurs particularly in young i~dividuals.1.3 PrincipalclinicaI consequences are transmission to sexual partnersand to the fetus and newborn by infected mothers, and therisk of developing squamous cell carcinoma.3-5 Untreatedlesions can remain unchanged for 10 or more years, ormore rarely, lnay regress spontaneously.2
Address for correspondence:Eliane Pedra DiasRua Br. de Itapagipe, 401 BI. 2 Apt. 20Rio de Janeiro/RJ - Brasil- CEP 20261-000
Classical histopathological features of Condylomaacuminatum were recognized long ago, and arecharacterized by acantosis, papillomatosis, hyperceratosis,paraceratosis and koilocytosis.ó-x Many studies havedescribed its clinicaI aspects and a great variety of lesions.Different clinicaI classifications have already beenproposed by many authors, but none have been able tocorrelate the clinicaI with the histopathological aspects.3,9,IO
The analysis of several biopsies from outpatientclinics in gynecology and sexual transmitted diseases(STD) allowed us to observe the differences, bathquantitative and qualitative, in the various condylomataacuminata. The growth phase, the full-expression phase,and the regressive ar persistent phase have been wellcharacterized clinicallyY These phases were recognizedhistopatholagically in equine cutaneous papillomas byHAMADA et al.ll There have been no similar studies inhumans. Therefore, in order to identify their differencesand similarities and classify the histopathologicalevolutionary phases of condylomata acuminata, it isnecessary to conduct a histopathological study.
DIAS, E.P,; ANA LUISA FIGUEIRA GOUVÊA,A,L.F.; EYER, C.C - Condylomaacuminatum: its histopathological pattern
São Paulo Medicai Journal/RPM 115(2): 1383-1389, 1997

1384
Among the great number of clinicallesions associatedwith papillomavirus infection, only flat warts present thecharacteristics of spontaneous regression. Many reportshave attempted to explain this phenomenon, 12-16and mostof them concurthat cell-mediated immunity is responsiblefor the effective regression of this kind of lesion. Thisimmune response is expressed by an early infiltration ofmacrophages and T lymphocytes CD4+ in the dermis andlater transepitheliaI. The non-regressing warts have aninconspicuous infiltrate composed of T lymphocytesCD8+.17
In 1993, OKABAYASHI et aI.,18 using rabbits,classified the lesions as proliferative (marked cellularproliferation) and regres,sive (inflammatory mononuclearcell infiltrate dermal and transepithelial). In 1994,COLEMAN et aI. published their first study on theregression of genital warts in closely monitored patients.The main histopathological feature identified byCOLEMAN et aI. was a marked, continuous subepithelialinflammatory infiltrate, with prominent dermal infiltration.
Based on random observations and studies on theregression phenomenon causing papillomavirus lesions, wehave designed a protocol to histopathologically analyze thecondylomata acuminata, aiming to identify its evolutionaryphases.
MATERIALS AND METHODS
The parameters investigated in the epithelium were:koilocytosis (according to MEISELS6), basal cellhyperplasia (four or more layers of basal cells), acantosis,hyperceratosis, and paraceratosis. Histological evaIuationof the dermis included the presence and localization(dermal, basal epithelial, transepitheliaI) of mononucIearcell infiltrate. The investigation reveaIed extremely highleveIs of variation in paraceratosis and mononuclear cellinfiltrate, and this resuIted in further classificationaccording to intensity, being low, medium and high asfollows:
Paraceratosis low: condyloma with few areas ofparaceratosis in the epithelium.
Paraceratosis medium: condyloma with some areasof paraceratosis in the epitheIium.
Paraceratosis high: condyloma with paraceratosisthroughout the epithelium.
Mononuclear cell infiltrate low: condyloma withfew Iymphocytes and histiocytes in few areas.
Mononuclear cell infiltrate. medium:condyloma with Iymphocytes and histiocytes, withmoderate distribution, sometimes in foci or in a band-Iike pattern.
Mononuclear cell infiltrate high: condyloma withintense lymphocytes and histiocytes infiltrate, many timesin a band-like pattern.
After individual analysis, the cases were groupedaccording to their differences and similarities in an attemptto establish an evolutionary cIassification.
We retrospectivelystudied 60 condylomataacuminata from the files ofthe Department of Patho-logy (UFF) from January1994 through April 1996.The selected 60 casesfulfilled the followingrequirements: a) specimensmeasuring not less than 0.5em in length and withsufficient dermis; and b)specimens not displayingacute inflammation.
The specimens werestained by the H.E. techni-que and analyzed as to theclassical histopathologicaIaspects considered cha-racteristic of condylomaacuminatuTÍ1.
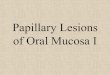
Figure 1 - KOILOCYTOSIS (@) criteria for the c1assification of condylomata acuminatum as VI RALREPLICATION ACTIVITY PHASE (Hematoxilina & Eosina Objective 100 x Ocular 10 x).
São Paulo Medicai Journal/RPM 115(2): 1383-1389, 1997 DIAS, E.P.; ANA LUISA FIGUEIRA GOUVÊA,A.L.F.; EYER, C.C - Condylomaacuminatum: its histopathological pattern

1385
GROUP A (n=16)
The detailed histo-pathological analysis of thecases (Fig. 4) showedacantosis, hyperceratosis andparaceratosis in all cases, andbasal cell hyperplasia in 4 (25percent). Paraceratosis wasconsidered mild or moderatein 25 percent of the cases andintense in 50 percent. 'Thelymphocytic inflammatoryinfiltrate was seen in all cases(mild in 69 and moderate in31 percent). Dermis and thebase of the epithelium were
to the dermis and the koilocytosis; when present, it wasin a concentration of five or less (Fig. 3).
Thus, according to the predominant characteristics,such as koilocytosis, transepithelial mononuclear cellinflammatory infiltrate or transepithelial inflammatoryinfiltrate and the absence of koilocytosis, the cases werefurther separated in groups A, B and C respectively. Theremaining 13 lesions did not meet any of the criteria and
therefore were considered asbelonging to an intermediateevolutionary phase andexcluded from the study.
Figura 3: ABSENCE of KOILOCYTOSIS and TRANSEPITHELIAL LYMPHOCYTIC INFILTRATE(@), criteria for the classification of condylomata acuminatum as PROLIFERATIVE PHASE.(Hematoxilina & Eosina Objetiva 40 x Ocular 10 x).
RESULTS
The histopathologicalanalysis of the 60condylomata acuminatashowed that koilocytosisand the mononuclearinflammatory infiltrationpresented the mostprominent quantitativedifferences.
First, we selected thecases where koilocytosis - thehistopathological marker ofthe cytopathic effect ofHPVreplication - was present. Thekoilocyfosis "intensity varies
from rare to very numerous Figure 2 - TRANSEPITHELIAL LYMPHOCYTIC INFILTRATE (@) criteria for the classificationand this variation was consi- of condylomata acuminatum as REGRESSIVE PHASE (Hematoxilina & Eosina Objective 40xdered as an evolutionary Ocular 10x).variation.
Group A was formed by 16 condylomata in whichmore than five koilocytosis (Fig.1) per section were visible.
From the other 44 cases, for our purposes Group B,we selected 19 condylomas in which the transepithelialinflammatory infiltrate (Fig. 2) - histopathological markerof regression phenomenon - was the most prominent feature.
Group C was formed by 12 condylomas in whichthe inflammatory infiltrate was absent or lnild and confined
DIAS, E.P.; ANA LUISA FIGUEIRA GOUVÊA,A.L.F.; EYER, C.C - Condyloma\
acuminatum: its histopathological pattern '
São Paulo Medicai Journal/RPM 115(2): 1383-1389, 1997

1386
100%
80%
60%
40%
20%
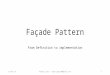
0%BH AC HC PC-L PC-M PC-A K lI-L II-M lI-A II-D II-B II-T II-AbsBH = Basal Hyperplasia AC = Acantosis HC HyperceratosisPC = Paraceratosis K Koilocytosis 11 Inflammatory Infiltrate-L = Light -M Moderate -A Accentuated-B = Basal -T Transepithelial -Abs = Absent
-D Dermal
GROUPS:
Figure 4 - Percentages relative to the various histopathological aspects identified in:
Figure 5 - Condylomata acuminatum with various koilocytosis, representative of the VIRALREPLICATION ACTIVITY PHASE. (Hematoxilina & Eosina Objective 10x Ocular 10x).
the most frequent localization (88 percent). This groupwas considered as having the viral replication activity(VRA) pattern (Fig. 5).
GROUP B (n=19)
In this group, (Fig. 4)basal cell hyperplasia wasdetected in 32 percent.Acantosis, hyperceratosisand paraceratosis wereobserved in all cases.Paraceratosis was mild in16 percent, moderate in 68percent and intense in 16percent. Koilocytosis wasrarely seen (6 cases/32percent). The mononuclearcell inflammatory infiltratewas localized in the dermisand epidermis, and con-sidered mild in 32 percent,moderate in 26 percent andintense in .42 percent. Thiswas classified as Regressive(R) pattern (Fig. 6).
GROUPC(n=22)
In this group, both transepithelial inflammatoryinfiltrate and koilocytosis were rarely seen or were absent.The histopathological analysis of this group (Fig. 4) hasdisplayed basal cell hyperplasia, acantosis, hyperceratosis
São Paulo Medicai Journal/RPM 115(2): 1383-1389, 1997 DIAS, EP.; ANA LUISA FIGUEIRA GOUVÊA,A.L.F.; EYER, C.C - Condylomaacuminatum: its histopathological pattern

1387
Figure 6 - Condylomata acuminatum with accentuated transepithe.liallymphocytic infiltrate withoutkoilocytosis (H), REGRESSIVE PHASE. (Hematoxilina & Eosina Objective 4 x Ocular 10 x).
and paraceratosis in all cases. The paraceratosis was lTIildin 80 percent and moderate in 20 percent. Koilocytosiswas less frequent (17 percent). Mononuclear cell infiltratewas absent in 33 percent, but in the remaining 8 patientslTIononuclear cell infiltrate was localized in the dermis andclassified as mild. This group was considered asProliferative (P) pattern (Fig.7).
koilocytosis in some lesionsmay expIai n the negati veresults observed in studiesutilizing procedures such asimlTIUnohistochemistry and/or in situ hybridization withthe aim of virus identi-fication. Koilocytosis wasdiagnosed in accordancewith MEISELSó criteria.The presence of aperinuclear halo, even thoseassociated with nuclearalterations, must becarefully interpreted. In ouropinion, this can not beregarded as anhistopathological criterionof compatibility with HPVinfection. Our results havealso demonstrated the
importance of koilocytosis in defining a pattern. In 31 casesclassified as proliferative or regressive, it was identifiedin only 8 cases (26 percent - Fig. 4).
Our study has delTIOnstrated the existence of a groupof lesions that show histopathological characteristics thatdenote a lymphocyte-mediated immunological responseby the patient.
The morphological regression phenomena in wartsis aIready weIl d?cumented not onIy in animaIs but aIso in
Figure 7 - Condylomata acuminatum with rare dermis Iymphocytes (@), without koilocytosis.PROLIFERATIVE PHASE. (Hematoxilina & Eosina Objective 10x Ocular 10x).
DISCUSSION
The analyses of speci-mens from 60 patients withcondylomata acuminatashows that there are quan-titative histopathologicaldifferences among them.
The relatively lowincidence observed forkoilocytosis (40 percent)was expected as koilo-cytosis represents the histo-pathological expression ofthe cytopathic effect ofHPV, and this is evidentonly in lesions with greatviral replication activity.The absence or rarity of
DIAS, E.P.; ANA LUISA FIGUEIRA GOUVÊA,A.L.F.; EYER, C.C - Condylomaacuminatum: its histopathological pattern
São Paulo Medicai Journal/RPM 115(2): 1383-1389, 1997

1388
humans.12-190ur results are in agreement with the literature,contributing to the histopathological characterization ofthe regression pattern of condylomata acuminata.However, this quantitative study based only in thehistopathological analysis is subjective, and its efficacy isquestionable.
On the other hand, the distribution of the IYlnphocyticinfiltrate is a lnore precise criteria which considers onlytwo possibilities: its presence or absence in different sites.We believe that the best histopathological regressionmarker for condylomata acuminata is the transepitheliallocalization of the lymphocytic infiltrate.
OKABAYASHI et aI., IX studying rabbit papillolnas,characterized a proliferative phase by a marked epithelialproliferation when compared with the other phases. In ourstudy, we characterized a group of lesions by the absenceof koilocytosis and transepithelial lymphocytic infiltrate(Group C). Employing the basal cell hyperplasia criterion- the histopathological expression of proliferation insquamous cell epitheliuln - we were able to verify itspresence in all Group C cases (Fig. 4), and in 25 and 32percent of group A and B cases, respectively. Thisexpressed difference was a major criteria for classifyingGroup C as representative ofthe proliferative pattern whichprobably corresponds to the early phase ofHPV infection.
Acantosis and hyperceratosis were present in all casesand for this reason they were not considered as particularcriteria for a,ny group. Paraceratosis was also observed inalI cases. However, it was inconspicuous in the
proliferative pattern and marked in the activity pattern,showing a clear relationship between the cytopathic effectof HPV and the disturbance in squamous celIdifferentiation (Fig. 4).
Prior studies have primarily emphasized the clinicaIvariations of condylomata acuminata, and secondarily theidentification of the virus by different technologicalmethods based on immunopathology and lnolecularbiology.2J.7.x
Our study resulted in three distinct patterns ofcondyloma cUlninatuln: proliferative, viraI replicationacti vity and regressi ve. These patterns probably retlect thebiological phase of the HPV infection: one phase ofinterference in the control of epithelium proliferation,another phase of an intense viraI replication with cytopathiceffects expression and finally, a phase characterized bythe regression ofthe action ofthe HPV, possibly in answerto the host defense.
These biological phases are probably linked to theclinicaI expression phases. However, it is possible that theduration of each phase depends on an efficient ilnmuneresponse. An accurate histopathologic study of condylolnaacuminatulTI, besides improving the precise diagnosis oflesions not presenting koilocytosis, permits theidentification of the histopathologicaI pattern. Thecorrelation of this pattern with the evolution tilne of thelesion and the recurrence history could give the physiciana prognostic evaluation based on the patient's own currentdefenses.
São Paulo Medicai Journal/RPM 115(2): 1383-1389, 1997 DIAS, E.P.; ANA LUISA FIGUEIRA GOUVÊA,A.LF.; EYER, C.C - Condylomaacuminatum: its histopathological pattern

REFERENCES
I. Ferenczy A. Epidemiology and clinicaI pathophysiology ofcondylomata acuminata. Am J Obstet Gynecol1995~ 172: 1331-39.
2. Oriel JD. Natural history of genital warts. Brit J Vener Dis1971~47:1-13.
3. Sykes NL. Condyloma acuminatum. Int J Dermtol1995~34:297-302.
4. Schneider A. Pathogenesis of genital HPV infection.Genitourin Med 1993~69: 165-73.
5. Dias EP, Barcelos JMP, Fonseca MEF, Basso NGS.Congenital papillomas and papillomatosis associated withthe HPV - Report on 5 cases. São Paulo Med J 1995~113:957-63. .
6. Meisels A, Fortin R, Roy M. Condylomatous Lesions oftheCervix 11: a cytologic, colposcopic and histopathologic study.Acta Cytologica 1977~21 :379-89.
7. Dias EP. Papilomavírus humano - Aspectos biológicos,clínicos e morfológicos. JBM 1993~64:206-17.
8. Myint SH, Shaw AV. Laboratory identification of humanpapillomavirus infection. In: Eds., Mindel A, Arnold E.Genital Warts human papillomavirus infection. London,1995:35-52.
9. Rock B, Shah K, Farmer E. A morphologic, pathologic, andvirologic study of anogenital warts in men. Arch Dennatol1992~ 127:495-500.
10. Gross G, Ikenberg H, Gissmann L, Hasedorn M.Papillomavirus infection ofthe anogenital region: Correlation
DIAS, E.P.; ANA LUISA FIGUEIRA GOUVÊA,A.L.F.; EYER, C.C - Condylomaacuminatum: its histopathological pattern
1389
between histology, clinicai picture and virus type - Proposalof a new nomenclature. J Invest Dermatol 1985~85: 147-52.
li. Hamada M, Oyamada T, Yoshikawa H, Yoshikawa T, ItakuraC. Histopathological development of equine cutaneouspapillomas. J Comp Pathol 1990~ I02(4:393-403.
12. Tagami H, Ogino A, Takigawa M, et aI. Regression of planewarts following spontaneous inflamation: Ahistopathological study. Br J Dermatol 1974~90: 147-54.
13. Tagarni H, Takigawa M, Ogino A, Imamura S, Ofugi S.Spontaneous regression of plane warts after inflammation.Arch Dermatol 1977~ 113: 1209-13.
14. Tagarni H, Oguchi M, Ofuji S. The phenomenon ofspontaneous regression of numerous flat warts:Imrnunological studies. Cancer 1980~45:2557-63.
15. Aiba S, Rokugo M, Tagami H. ImmunohistQlogic analysisof the phenonlenon of spontaneous regression of numerousflat warts. Cancer 1986~58: 1246-51.
16. Bishop PE, Millan AMc, Fletcher S. An immunohistologicalstudy of spontaneous regression of condylomata acuminata.Genitourin Med 1990~66:79-81.
17. Stanley MA, Chambers MA, Coleman N. Immunology ofhuman papilomavirus infection. In: Eds., Mindel A, ArnoldE. Genital Warts human papillomavirus infection. London,1995:259.
18. Okabayashi M, Angell MG, Budgeon LR, Kreider JW. Shopepapilloma cell and leukocyte proliferation in regressing andprogressing lesions. Am J Pathol 1993~ 142:489-95.
19. Colernan N, BirIey HDL, et aI. Immunological events inregressing genital warts. Am J Clin Pathol 1994~102:768-74.
São Paulo Medicai JournallRPM 115(2): 1383-1389, 1997