Embed Size (px)
Citation preview
Réanimation (2008) 17, 74—97
Disponib le en l igne sur www.sc iencedi rec t .com
journa l homepage: ht tp : / / f rance .e lsev ier .com/di rec t /REAURG/
CONFÉRENCE DE CONSENSUS INTERNATIONALE
Weaning from mechanical ventilation�,��
Sevrage de la ventilation mécanique
J.-M. Bolesa,∗, J. Bionc, A. Connorsd, M. Herridgeh,B. Marsh i, C. Melot j, R. Pearle, H. Silvermanf,M. Stanchinag, A. Vieillard-Baronb, T. Weltek
a Department of Medical Intensive Care and Medical Emergencies, Hôpital de la Cavale-Blanche University Hospital,Université de Bretagne Occidentale, 29200 Brest cedex, Franceb Medical Intensive Care Unit, Ambroise-Paré University Hospital, Assistance publique—Hôpitaux de Paris, Boulogne, Francec Department of Anaesthesia and Intensive Care Medicine, Queen-Elizabeth Hospital, Birmingham, UKd Case Department of Medicine at MetroHealth Medical Center, Case Western Reserve University, Cleveland, OH, USAe Department of Anaesthesia, Stanford University School of Medicine, Stanford, CA, USAf Department of Medicine, University of Maryland Medical Center, Baltimore, MD, USAg Department of Pulmonary and Critical Care Medicine, Rhode Island Hospital, Providence, RI, USAh Department of Medicine, Toronto General Hospital, Toronto, ON, Canadai Department of Anaesthesia and Intensive Care Medicine, Trinity College, Dublin, Irelandj Department of Intensive Care, Erasme Hospital, Free University of Brussels, Brussels, Belgiumk Department of Pulmonary Medicine, University of Hannover Medical School, Hannover, Germany
Available online 26 Novembre 2007
KEYWORDSMechanicalventilation;Weaning frommechanicalventilation
Summary Weaning covers the entire process of liberating the patient from mechanical supportand from the endotracheal tube. Many controversial questions remain concerning the bestmethods for conducting this process. An International Consensus Conference was held in April2005 to provide recommendations regarding the management of this process. An 11-memberinternational jury answered five predefined questions. (1) What is known about the epidemiologyof weaning problems? (2) What is the pathophysiology of weaning failure? (3) What is the usualprocess of initial weaning from the ventilator? (4) Is there a role for different ventilator modesin more difficult weaning? (5) How should patients with prolonged weaning failure be managed?The main recommendations were as follows. (1) Patients should be categorised into three groupsbased on the difficulty and duration of the weaning process. (2) Weaning should be considered
as early as possible. (3) A spontaneous breathing trial is the major diagnostic test to determinewhether patients can be successfully extubated. (4) The initial trial should last 30 min and� Statement of the Seventh International Consensus Conference on Intensive Care Medicine, organised jointly by the European RespiratorySociety (ERS), the American Thoracic Society (ATS), the European Society of Intensive Care Medicine (ESICM), the Society of Critical CareMedicine (SCCM) and the ‘‘Société de réanimation de langue francaise’’ (SRLF), and approved by the ERS Executive Committee,February 2007.
�� Conférence de consensus publiée initialement dans EurRespir J 2007;29:1033—56.∗ Corresponding author.
E-mail address: [email protected] (J.-M. Boles).
1624-0693/$ — see front matterdoi:10.1016/j.reaurg.2007.10.001
Weaning from mechanical ventilation 75
consist of either T-tube breathing or low levels of pressure support. (5) Pressure support orodes should be favoured in patients failing an initial trial/trials. (6)hniqhoul
twtttcsitr
af
Tq
1bWtdw
Qe
W
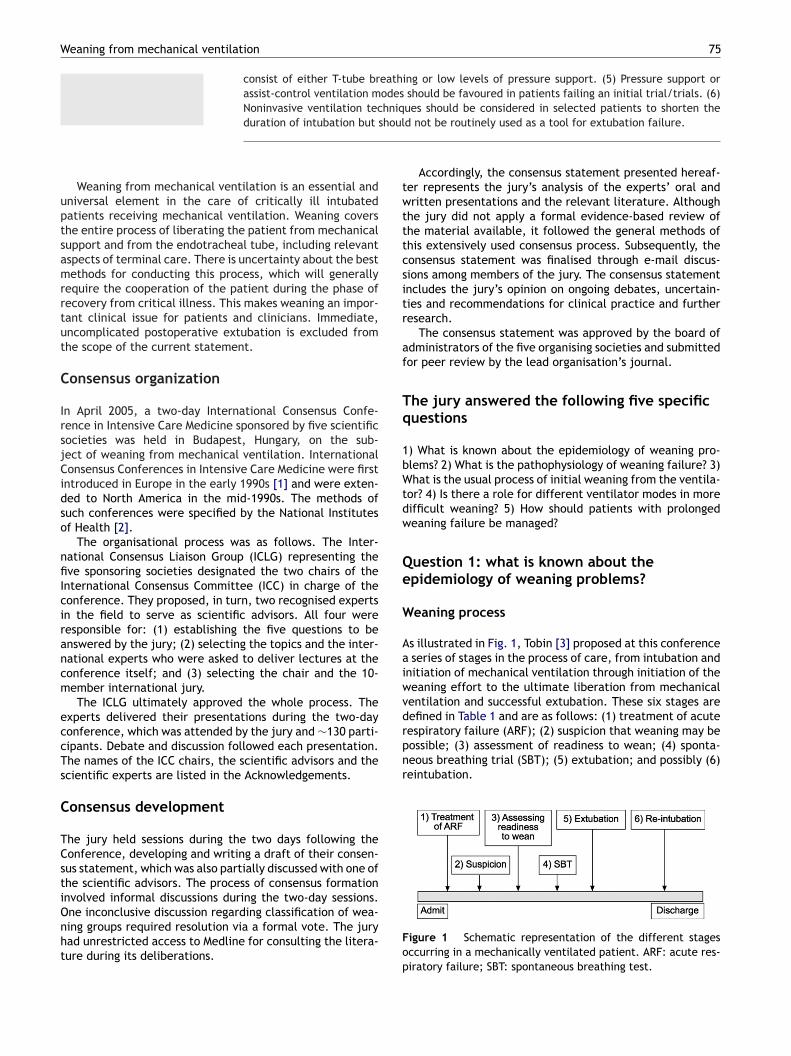
Aaiwventilation and successful extubation. These six stages aredefined in Table 1 and are as follows: (1) treatment of acuterespiratory failure (ARF); (2) suspicion that weaning may bepossible; (3) assessment of readiness to wean; (4) sponta-neous breathing trial (SBT); (5) extubation; and possibly (6)reintubation.
assist-control ventilation mNoninvasive ventilation tecduration of intubation but s
Weaning from mechanical ventilation is an essential anduniversal element in the care of critically ill intubatedpatients receiving mechanical ventilation. Weaning coversthe entire process of liberating the patient from mechanicalsupport and from the endotracheal tube, including relevantaspects of terminal care. There is uncertainty about the bestmethods for conducting this process, which will generallyrequire the cooperation of the patient during the phase ofrecovery from critical illness. This makes weaning an impor-tant clinical issue for patients and clinicians. Immediate,uncomplicated postoperative extubation is excluded fromthe scope of the current statement.
Consensus organization
In April 2005, a two-day International Consensus Confe-rence in Intensive Care Medicine sponsored by five scientificsocieties was held in Budapest, Hungary, on the sub-ject of weaning from mechanical ventilation. InternationalConsensus Conferences in Intensive Care Medicine were firstintroduced in Europe in the early 1990s [1] and were exten-ded to North America in the mid-1990s. The methods ofsuch conferences were specified by the National Institutesof Health [2].
The organisational process was as follows. The Inter-national Consensus Liaison Group (ICLG) representing thefive sponsoring societies designated the two chairs of theInternational Consensus Committee (ICC) in charge of theconference. They proposed, in turn, two recognised expertsin the field to serve as scientific advisors. All four wereresponsible for: (1) establishing the five questions to beanswered by the jury; (2) selecting the topics and the inter-national experts who were asked to deliver lectures at theconference itself; and (3) selecting the chair and the 10-member international jury.
The ICLG ultimately approved the whole process. Theexperts delivered their presentations during the two-dayconference, which was attended by the jury and ∼130 parti-cipants. Debate and discussion followed each presentation.The names of the ICC chairs, the scientific advisors and thescientific experts are listed in the Acknowledgements.
Consensus development
The jury held sessions during the two days following theConference, developing and writing a draft of their consen-sus statement, which was also partially discussed with one ofthe scientific advisors. The process of consensus formationinvolved informal discussions during the two-day sessions.
One inconclusive discussion regarding classification of wea-ning groups required resolution via a formal vote. The juryhad unrestricted access to Medline for consulting the litera-ture during its deliberations.Fop
ues should be considered in selected patients to shorten thed not be routinely used as a tool for extubation failure.
Accordingly, the consensus statement presented hereaf-er represents the jury’s analysis of the experts’ oral andritten presentations and the relevant literature. Although
he jury did not apply a formal evidence-based review ofhe material available, it followed the general methods ofhis extensively used consensus process. Subsequently, theonsensus statement was finalised through e-mail discus-ions among members of the jury. The consensus statementncludes the jury’s opinion on ongoing debates, uncertain-ies and recommendations for clinical practice and furtheresearch.
The consensus statement was approved by the board ofdministrators of the five organising societies and submittedor peer review by the lead organisation’s journal.
he jury answered the following five specificuestions
) What is known about the epidemiology of weaning pro-lems? 2) What is the pathophysiology of weaning failure? 3)hat is the usual process of initial weaning from the ventila-
or? 4) Is there a role for different ventilator modes in moreifficult weaning? 5) How should patients with prolongedeaning failure be managed?
uestion 1: what is known about thepidemiology of weaning problems?
eaning process
s illustrated in Fig. 1, Tobin [3] proposed at this conferenceseries of stages in the process of care, from intubation and
nitiation of mechanical ventilation through initiation of theeaning effort to the ultimate liberation from mechanical
igure 1 Schematic representation of the different stagesccurring in a mechanically ventilated patient. ARF: acute res-iratory failure; SBT: spontaneous breathing test.
76
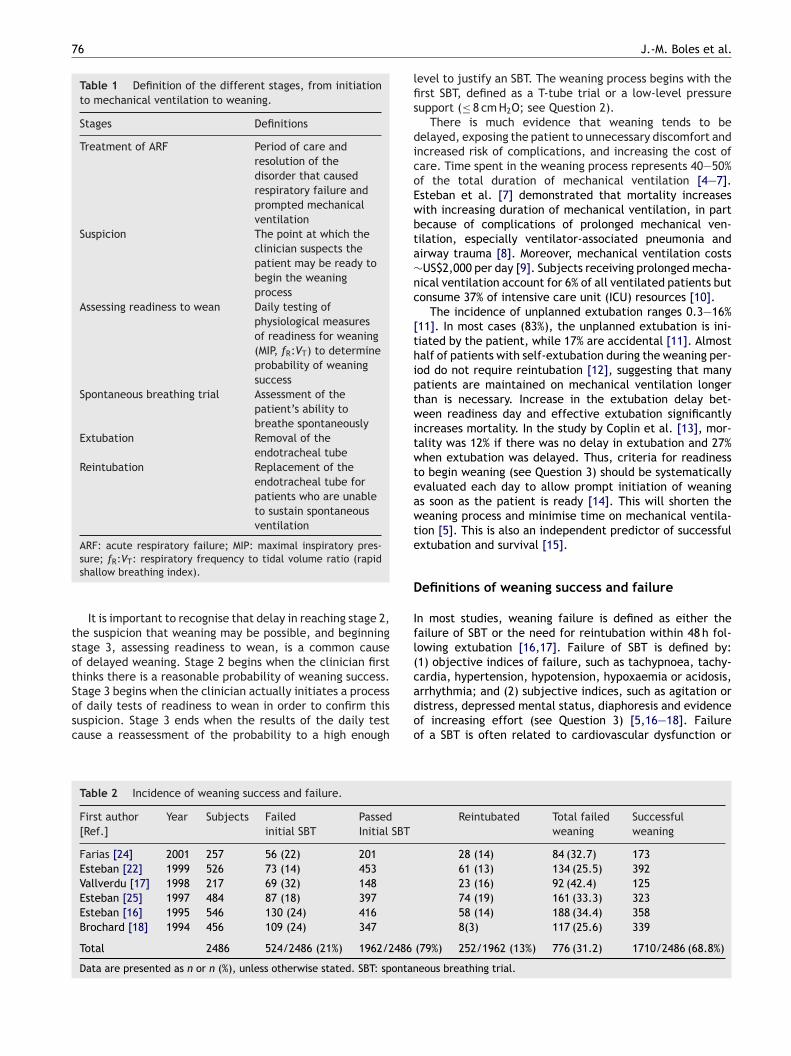
Table 1 Definition of the different stages, from initiationto mechanical ventilation to weaning.
Stages Definitions
Treatment of ARF Period of care andresolution of thedisorder that causedrespiratory failure andprompted mechanicalventilation
Suspicion The point at which theclinician suspects thepatient may be ready tobegin the weaningprocess
Assessing readiness to wean Daily testing ofphysiological measuresof readiness for weaning(MIP, fR:VT) to determineprobability of weaningsuccess
Spontaneous breathing trial Assessment of thepatient’s ability tobreathe spontaneously
Extubation Removal of theendotracheal tube
Reintubation Replacement of theendotracheal tube forpatients who are unableto sustain spontaneousventilation
ARF: acute respiratory failure; MIP: maximal inspiratory pres-
tsotSosc
lfis
dicoEwbta∼nc
[thiptwitwteawte
D
Ifl(cardia, hypertension, hypotension, hypoxaemia or acidosis,
sure; fR:VT: respiratory frequency to tidal volume ratio (rapidshallow breathing index).
It is important to recognise that delay in reaching stage 2,he suspicion that weaning may be possible, and beginningtage 3, assessing readiness to wean, is a common causef delayed weaning. Stage 2 begins when the clinician firsthinks there is a reasonable probability of weaning success.
tage 3 begins when the clinician actually initiates a processf daily tests of readiness to wean in order to confirm thisuspicion. Stage 3 ends when the results of the daily testause a reassessment of the probability to a high enoughadoo
Table 2 Incidence of weaning success and failure.
First author[Ref.]
Year Subjects Failedinitial SBT
PassedInitial SBT
Farias [24] 2001 257 56 (22) 201Esteban [22] 1999 526 73 (14) 453Vallverdu [17] 1998 217 69 (32) 148Esteban [25] 1997 484 87 (18) 397Esteban [16] 1995 546 130 (24) 416Brochard [18] 1994 456 109 (24) 347
Total 2486 524/2486 (21%) 1962/2486
Data are presented as n or n (%), unless otherwise stated. SBT: spontan
J.-M. Boles et al.
evel to justify an SBT. The weaning process begins with therst SBT, defined as a T-tube trial or a low-level pressureupport (≤ 8 cm H2O; see Question 2).
There is much evidence that weaning tends to beelayed, exposing the patient to unnecessary discomfort andncreased risk of complications, and increasing the cost ofare. Time spent in the weaning process represents 40—50%f the total duration of mechanical ventilation [4—7].steban et al. [7] demonstrated that mortality increasesith increasing duration of mechanical ventilation, in partecause of complications of prolonged mechanical ven-ilation, especially ventilator-associated pneumonia andirway trauma [8]. Moreover, mechanical ventilation costsUS$2,000 per day [9]. Subjects receiving prolonged mecha-ical ventilation account for 6% of all ventilated patients butonsume 37% of intensive care unit (ICU) resources [10].
The incidence of unplanned extubation ranges 0.3—16%11]. In most cases (83%), the unplanned extubation is ini-iated by the patient, while 17% are accidental [11]. Almostalf of patients with self-extubation during the weaning per-od do not require reintubation [12], suggesting that manyatients are maintained on mechanical ventilation longerhan is necessary. Increase in the extubation delay bet-een readiness day and effective extubation significantly
ncreases mortality. In the study by Coplin et al. [13], mor-ality was 12% if there was no delay in extubation and 27%hen extubation was delayed. Thus, criteria for readiness
o begin weaning (see Question 3) should be systematicallyvaluated each day to allow prompt initiation of weanings soon as the patient is ready [14]. This will shorten theeaning process and minimise time on mechanical ventila-
ion [5]. This is also an independent predictor of successfulxtubation and survival [15].
efinitions of weaning success and failure
n most studies, weaning failure is defined as either theailure of SBT or the need for reintubation within 48 h fol-owing extubation [16,17]. Failure of SBT is defined by:1) objective indices of failure, such as tachypnoea, tachy-
rrhythmia; and (2) subjective indices, such as agitation oristress, depressed mental status, diaphoresis and evidencef increasing effort (see Question 3) [5,16—18]. Failuref a SBT is often related to cardiovascular dysfunction or
Reintubated Total failedweaning
Successfulweaning
28 (14) 84 (32.7) 17361 (13) 134 (25.5) 39223 (16) 92 (42.4) 12574 (19) 161 (33.3) 32358 (14) 188 (34.4) 3588(3) 117 (25.6) 339
(79%) 252/1962 (13%) 776 (31.2) 1710/2486 (68.8%)
eous breathing trial.

77
Table 3 Classification of patients according to the weaningprocess.
Group/category Definition
Simple weaning Patients who proceed from initiationof weaning to successful extubationon the first attempt without difficulty
Difficult weaning Patients who fail initial weaning andrequire up to three SBT or as long asseven days from the first SBT toachieve successful weaning
Prolonged weaning Patients who fail at least threeweaning attempts or require > 7 days
S
ft∼ih(m
ut
rt7tsMdhr
p3
R
PoCwChpv
Weaning from mechanical ventilation
inability of the respiratory pump to support the load of brea-thing. Extubation failure may be related to the same causes[19,20], in addition to upper airway obstruction or excessivesecretions [11].
Failure of extubation is associated with high mortalityrate, either by selecting for high-risk patients or by indu-cing deleterious effects such as aspiration, atelectasis andpneumonia [21]. Interestingly, mortality is not especiallyincreased when failure of extubation is related to upperairway obstruction (one out of nine patients; 11%) but ismarkedly increased in the other cases (19 out of 52 patients;36%) [22]. Predictors of extubation failure have been repor-ted [23], such as excess secretions, arterial carbon dioxidetension (Pa, CO2) > 5.99 kPa (45 mm Hg), duration of mecha-nical ventilation > 72 h, upper airway disorders and a priorfailed weaning attempt.
Rate of weaning failure after a single SBT is reported to be26—42% (Table 2) [17,22]. This variation in the rate of wea-ning failure among the studies may be due to differences inthe definition of weaning failure, especially differences inthe subjective indexes used to define failed SBT, or variationin the patients studied. For instance, chronic obstructivepulmonary disease (COPD) appears as an independent riskfactor for increased duration of weaning and weaning fai-lure [18]. Vallverdu et al. [17] reported that weaning failureoccurred in as many as 61% of COPD patients, in 41% ofneurological patients and in 38% of hypoxaemic patients.Contradictory results exist regarding the rate of weaningsuccess among neurological patients [13,17]. The study byCoplin et al. [13] of brain-injured patients demonstratedthat 80% of patients with a Glasgow coma score < 8 and 91%of patients with a Glasgow coma score < 4 were successfullyextubated. Finally, as shown in Table 2, in 2486 patients fromsix randomised studies, 524 patients failed SBT and 252 fai-led extubation after passing SBT, leading to a total weaningfailure rate of 31.2%. [16—18,22,24,25].
Several studies have recently proposed the use of nonin-vasive ventilation (NIV) for extubated patients in differentclinical situations, including prophylactic intervention inCOPD patients who failed SBT [26], patients with repea-ted SBT failure [27] and postsurgical patients. However, theeffectiveness of NIV remains to be determined.
The increased use of NIV raises the question of how todefine weaning success or failure. The current authors pro-pose the following definitions. Weaning success is defined asextubation and the absence of ventilatory support 48 h follo-wing the extubation. Weaning failure is defined as one of thefollowing: (1) failed SBT; (2) reintubation and/or resumptionof ventilatory support following successful extubation; or (3)death within 48 h following extubation.
Since NIV may allow extubation while mechanical ven-tilation is continued in the form of NIV, an intermediatecategory called ‘‘weaning in progress’’ is recommended forpatients who are extubated but remain supported by NIV.
Classification of patients
A new classification of patients into three groups is propo-sed, as suggested by Brochard [28] during the internationalconsensus conference, according to the difficulty and lengthof the weaning process (Table 3).
F
Ftd
of weaning after the first SBT
BT: spontaneous breathing trial.
The simple weaning group includes patients who success-ully pass the initial SBT and are successfully extubated onhe first attempt. This group, named group 1, represents69% of weaning patients (Table 2). Prognosis in this group
s good, with an ICU mortality of ∼5% [17,22] and an in-ospital mortality of ∼12% [22]. The remaining patients∼31%) represent groups 2 and 3. In this population, ICUortality is ∼25% [17,22].Group 2, difficult weaning, includes patients who require
p to three SBT or as long as seven days from the first SBTo achieve successful weaning.
Group 3, prolonged weaning, includes patients whoequire more than three SBT or > 7 days of weaning afterhe first SBT. Indeed, in the study by Esteban et al. [22], the5th percentile for duration of weaning for all patients, forhose with COPD and those with acute respiratory distressyndrome (ARDS) were four, five and six days, respectively.oreover, estimating from the survival curves from the stu-ies by Esteban et al. [16] and Brochard et al. [18], aboutalf of the patients who failed initial SBT (group 2) stillequired mechanical ventilation at day 7.
Therefore, the current authors estimate that ∼15% ofatients would be in the prolonged weaning group (group).
ecommendations
atients can be readily categorised into three groups basedn the difficulty and duration of the weaning process.lear definitions of the timing, stages and outcomes of theeaning process will support further research in weaning.linicians should evaluate readiness for weaning early in theospital course to allow prompt initiation of the weaningrocess. An efficient weaning process reduces time on theentilator and improves patient outcomes.
urther research
urther study is needed of the effectiveness of NIV inhe process and outcomes of weaning. The proposedefinitions of the weaning process and the groups of

7 J.-M. Boles et al.
pttn
Qw
Apfnimlrndilildbcir
R
Tvmtt(etgdtiv<pcwppiotstopr[
it
Table 4 Common pathophysiologies and their incidence,which may impact on the ability to wean a patient frommechanical ventilation.
Pathophysiology Consider
Respiratory load Increased work of breathing:inappropriate ventilator settingsReduced compliance: pneumonia(ventilator-acquired); cardiogenic ornoncardiogenic oedema; pulmonaryfibrosis; pulmonary haemorrhage;diffuse pulmonary infiltratesAirway bronchoconstrictionIncreased resistive load
During SBT: endotracheal tubePostextubation: glottic oedema;
increased airway secretions; sputumretention
Cardiac load Cardiac dysfunction prior to criticalillness increased cardiac workloadleading to myocardial dysfunction:dynamic hyperinflation; increasedmetabolic demand; unresolved sepsis
Neuromuscular Depressed central drive: metabolicalkalosis; mechanical ventilation;sedative/hynotic medicationsCentral ventilatory command: failure ofthe neuromuscular respiratory systemPeripheral dysfunction: primary causesof neuromuscular weakness; CINMA
NeuropsychologicalDeliriumAnxiety, depression
Metabolic Metabolic disturbancesRole of corticosteroidsHyperglycaemia
Nutrition OverweightMalnutritionVentilator-induced diaphragmdysfunction
dttostl
to
8
atients who undergo weaning need to receive careful tes-ing and scrutiny. Studies of the patients’ outcomes inhe difficult weaning and prolonged weaning groups areeeded.
uestion 2: what is the pathophysiology ofeaning failure?
thorough and systematic search for potentially reversibleathologies should be conducted in all patients who did notulfil simple weaning as previously defined. Using the defi-itions put forth in this statement, this places the patientn group 2, and reversible aetiologies for weaning failureay be categorised as follows: respiratory load, cardiac
oad, neuromuscular competence (central and periphe-al), critical illness neuromuscular abnormalities (CINMA),europsychological factors, and metabolic and endocrineisorders (Table 4). These same factors should be soughtn group 3 patients, who have required mechanical venti-ation for > 7 days. The pathophysiology of weaning failuren group 3 may be complex and multifactorial. Irreversibleesions may become apparent at this time point or clearlyelineated issues (e.g. cardiac dysfunction or CINMA) maye difficult to optimise or slow to resolve. In this group ofhronically critically ill patients it is imperative that theres a disciplined approach to ongoing surveillance for anyeversible or remediable factors.
espiratory load
he decision to attempt discontinuation of mechanicalentilation has largely been based on the clinician’s assess-ent that the patient is haemodynamically stable, awake,
he disease process has been treated adequately andhat indices of minimal ventilator dependency are presente.g. inspiratory oxygen fraction (FI,O2 ) ≤ 0.5, positivend-expiratory pressure (PEEP) ≤ 8 cm H2O, arterial oxygenension (Pa,O2)/FI,O2 > 20.0 kPa (150 mm Hg), arterial oxy-en saturation ≥ 90%). The success of weaning will beependent on the ability of the respiratory muscle pumpo tolerate the load placed upon it. This respiratory loads a function of the resistance and compliance of theentilator pump. Normal respiratory system resistance is5 cm H2O l−1 s−1. Normal respiratory system static com-liance is 0.06—0.1 l cm H2O−1. Improvement in static lungompliance may alert the clinician to the potential foreaning from mechanical ventilation and has been incor-orated into a computer-driven model [29] where a plateauressure of ≤ 30 cm H2O for a tidal volume (VT) ≥ 8 ml kg−1
s included in the algorithm prior to decreasing levelsf pressure support ventilation (PSV). Maximum inspira-ory pressure has been used to assess inspiratory muscletrength, measured either after negative pressure is main-ained for 1 s after a forceful expiration to residual volumer using a unidirectional expiratory valve. A maximum ins-iratory pressure value of ≤ −20 to −25 cm H2O has been
eferenced as a predictive index for successful weaning30,31].An excess work of breathing (WOB) may be imposed bynappropriate ventilator settings (e.g. inadequate inspira-ory flow rate or flow trigger setting) resulting in ventilator
ompav
Anaemia
SBT: spontaneous breathing trial; CINMA: critical illness neuro-muscular abnormalities.
ysynchrony [32]. Components of such dysynchrony includehe lead time between onset of inspiratory effort andhe onset of flow delivery, respiratory effort after onsetf flow, ineffective triggering, expiratory effort prior towitchover from mechanical inflation to exhalation, andhe effect of high intrinsic PEEP (representing a thresholdoad).
Reduced pulmonary compliance may be secondaryo pneumonia, cardiogenic or noncardiogenic pulmonaryedema, pulmonary fibrosis, pulmonary haemorrhage or
ther diseases causing diffuse pulmonary infiltrates. Pneu-onia is common in critically ill patients, either as therimary admission diagnosis or as a subsequent ventilator-cquired pneumonia. Ventilator-acquired pneumonia has aariable incidence of 9—67% [33] and an attributable mor-
N
Ltotaipaf
DWethlatdtpdb[
mmolall
CFtbptbom[
PAiiTbdaneuron disease are usually apparent before weaning diffi-
Weaning from mechanical ventilation
tality of up to 50%. Shortening the weaning process isan important goal in reducing the incidence of ventilator-acquired pneumonia [27,34]. However, adequate treatmentof the underlying disease process is a prerequisite to extuba-tion. The need for reintubation is associated with a 4.5-foldincreased risk of nosocomial pneumonia [21]. Therapeuticguidelines and recommendations for reducing the incidenceof ventilator-acquired pneumonia have been recently publi-shed [35]. Reduced pulmonary compliance attributable tocardiogenic or noncardiogenic pulmonary oedema shouldbe considered, with optimisation of cardiac function andclearance of lung water instituted as clinically indicated.Reduced pulmonary compliance secondary to pulmonaryfibrosis (acute or premorbid) or reduced chest wall com-pliance secondary to kyphoscoliosis may be less amenableto treatment (more likely to represent group 3 patient pro-file). The splinting effect of obesity, abdominal distensionor ascites may be further considerations.
Additional load may be related to reversible airway bron-choconstriction, which should be addressed prior to SBT.Patients with COPD may also manifest dynamic hyperinfla-tion and reduced compliance when forced to operate at theless efficient upper margin of the pressure—volume curve.
The process of weaning may impose an increased resistiveload on the ventilatory muscles, either from the endotra-cheal tube during an SBT or postextubation from glotticoedema or increased airway secretions and sputum reten-tion [36—38].
Cardiac load
Many patients will have identified ischaemic heart disease,valvular heart disease, systolic or diastolic dysfunction priorto, or identified during, their critical illness. More subtle andless easily recognised are those patients with myocardialdysfunction, which is only apparent when exposed to theworkload of weaning.
The transfer of a patient from positive pressure ventila-tion to spontaneous ventilation is associated with increasedvenous return and negative intra-thoracic pressure causingincreased left ventricular after load and increased myo-cardial oxygen consumption. Thus, latent or unrecognisedmyocardial dysfunction may become manifest at the com-mencement of the weaning attempts [39—41]. This is furtherreflected in the beneficial effects seen with the applicationof continuous positive airway pressure (CPAP) [42] or NIV incardiogenic pulmonary oedema [43].
There are several contributors to increased cardiac work-load. These include: dynamic hyperinflation (intrinsic PEEP),which increases pulmonary vascular resistance, reducesright ventricular filling and impairs cardiac output; theincreased metabolic demand of the weaning process; andunresolved systemic disease (e.g. sepsis). There is an obli-gatory increase in cardiac output to meet the metabolicdemand of a weaning trial. Measurable indices includeincreased serum lactate and decreased mixed venous oxy-
gen saturation (SV,O2 ). Weaning failure has been predictedthrough the use of SV,O2 during SBT [44] or measurement ofgastric mucosal pH [45]. Myocardial ischaemia may becomemanifest during SBT. This may result in reduced left ventri-cular compliance, pulmonary oedema and increased WOB.cdtts
79
euromuscular competence
iberation from mechanical ventilation requires the resump-ion of neuromuscular activity to overcome the impedancef the respiratory system, to meet metabolic demands ando maintain carbon dioxide homeostasis. This requires andequate signal generation in the central nervous system,ntact transmission to spinal respiratory motor neurons, res-iratory muscles and neuromuscular junctions. Disruption ofny portion of this transmission may contribute to weaningailure.
epressed central driveith complete absence of central drive, patients do not
xhibit any ventilatory activity upon discontinuation fromhe ventilator, and this persists despite hypercapnia andypoxaemia. Examples of this may include, but are notimited to, encephalitis, brainstem haemorrhage/ischaemiand neurosurgical complications. It is more challengingo identify a reduction in ventilatory drive. The carbonioxide responsiveness test may be used to assess this buthere are few studies evaluating its utility in critically illatients. The responsiveness of central drive to carbonioxide assessed from the 100 ms occlusion pressure haseen shown to predict weaning success in a small case series46].
Central drive may be impeded by metabolic alkalosis,echanical ventilation itself or the use of sedative/hypnoticedications. Of these three possible contributors, there are
nly data that link sedative/hypnotic medication use to pro-onged weaning. The importance of the contribution of dailywakening and heightened awareness over sedation to pro-onged weaning and ICU stay has been established in theiterature [47].
entral ventilatory commandailure of the neuromuscular respiratory system to main-ain homeostasis results in an increased central drive toreathe, which in turn may cause ventilatory failure. Thisattern may be observed in response to an increased resis-ive load from upper airway obstruction, an imbalanceetween mechanical load and respiratory muscle capacityr isolated muscle weakness. Abnormalities of upper airwayotor control are a potential cause of extubation failure
37].
eripheral dysfunctionfter respiratory or cardiac causes have been excluded
n the difficult-to-wean patient, the contribution of per-pheral neuromuscular abnormalities should be considered.hese neuromuscular disorders may be common and haveeen reported in up to 62% of patients in some stu-ies [48]. Primary causes of neuromuscular weakness suchs Guillain-Barré syndrome, myasthenia gravis and motor
ulties are encountered. However, occasionally these newiagnoses will be made in the course of investigatinghe difficult-to-wean patient. Most neuromuscular dysfunc-ion that complicates weaning is acquired during the ICUtay.

8
C
CdbcpaohnRpCsmiovptwpamom
plm[
wccArppnmtbisac[
t[bwrtmn
io[
P
DDlaos[phwurtrd
AMaTp[b[
osfreasI
aiPsnbmm
M
MHandcd
R
0
ritical illness neuromuscular abnormalities
INMA are the most common peripheral neuromuscularisorders encountered in the ICU setting and usually involveoth muscle and nerve [49]. These disorders were first des-ribed in Canada and France in 1984 [50,51]. The reportedrevalence of CINMA in the literature has varied 50—100%nd this has been associated with severity of illness, multiplergan dysfunction, exposure to corticosteroids, presence ofyper-glycaemia and prolonged ICU stay [52—56]. The diag-osis of CINMA may be made at the bedside using the Medicalesearch Council score [57] with confirmation by electro-hysiological testing and muscle biopsy when appropriate.linically significant weakness has been associated with acore < 48 [56]. CINMA presents as a motor deficit whereuscle weakness is bilateral, symmetrical and most marked
n the proximal muscles. Electroneuromyographic studiesf the limbs show sensorimotor axonopathy with preser-ed velocities and decreased amplitude of compound actionotentials. Neuromuscular transmission is normal except inhe case of prolonged neuromusuclar blocade. In patientsith severe muscle involvement, decreased motor actionotentials and fibrillation potentials may resemble a motorxonopathy and a true distinction between a nerve and/oruscle lesion may be difficult. Myopathy may be confirmed
n muscle biopsy and type II fibre drop-out with a loss ofyosin filaments is a consistent finding [58].Three studies have shown that diaphragmatic electro-
hysiological abnormalities are common in patients withocomotor electroneuromyographic abnormalities and wereore prevalent when the limb weakness was more severe
52,59,60].The bedside evaluation of respiratory neuromuscular
eakness is difficult. Maximum inspiratory pressure and vitalapacity (VC) are dependent on patient comprehension andooperation and are hindered by the endotracheal tube.s a result, many have questioned their ability to detectespiratory neuromuscular dysfunction that contributes torolonged weaning [61—63]. Twitch transdiaphragmaticressure in response to bilateral stimulation of the phrenicerves can give an effort-independent measure of diaphrag-atic contractility [64]. Clinical applicability is limited as
his requires placement of both an oesophageal and gastricalloon. The airway pressure at the end of the tracheal tuben response to phrenic nerve stimulation has been propo-ed to be a noninvasive alternative measure and may haverole in monitoring inspiratory muscle contractility as its
orrelation to twitch transdiaphragmatic pressure is weak64].
The contribution of CINMA to prolonged mechanical ven-ilation has been studied in 10 cohorts of ICU patients54,56,65—72]. Four studies have shown an associationetween CINMA and an increased duration of weaning oreaning failure [49,67,70,71]. Two of these used multiva-
iable analysis to control for confounding factors and showedhat CINMA was an independent risk factor for duration ofechanical ventilation and weaning failure, including the
eed for tracheostomy [49,71].Neuromuscular dysfunction related to CINMA usually
mproves over weeks [65] but some disability may persistver months and interfere with activities of daily living73,74].
Ttaio
J.-M. Boles et al.
sychological dysfunction
eliriumelirium, or acute brain dysfunction, is a disturbance of the
evel of cognition and arousal and, in ICU patients, has beenssociated with many modifiable risk factors, including: usef psychoactive drugs; untreated pain; prolonged immobili-ation; hypoxaemia; anaemia; sepsis; and sleep deprivation75]. Important literature regarding delirium in critically illatients has emerged since 2001. The prevalence of deliriumas been reported to range 22—80% [76,77]. It is associatedith prolonged ICU stay and is a predictor of higher mortalityp to six months after discharge from the ICU [77]. A deli-ium screening tool has been developed and validated buthere is no established consensus on treatment [75]. Deli-ium has not yet proven to be directly linked to weaningifficulties but studies are underway.
nxiety and depressionany patients suffer significant anxiety during their ICU staynd the process of weaning from mechanical ventilation.hese memories of distress may remain for years [78]. Therevalence of anxiety during ICU is reported to be 30—75%79,80]. Patients report the following as important contri-utors to anxiety: dyspnoea [81]; inability to communicate82]; and sleep disruption [78].
Sleep studies have shown that patients are unable to restr sleep, and 25% report nightmares [78]. Furthermore, poly-omnographic studies show that ICU patients suffer fromrequent arousals and sleep fragmentation [83]. Sleep dis-uption may be related to ventilatory mode [84] and recentvidence suggests that ambient noise in the ICU may not bes significant a contributor as initially thought [85]. Depres-ion may occur as a discrete disorder or in association withCU delirium [86].
Several strategies have been reported to minimisenxiety during mechanical ventilation. These include:mprovement of speech by increasing inspiratory time andEEP, or ventilating with bi-level PSV [87]; improvement ofleep by minimising noise, light and nursing interventions atight; and the use of relaxation techniques, such as biofeed-ack. The combination of biofeedback with VT techniqueay reduce anxiety and decrease the time to wean fromechanical ventilation [88].
etabolic and endocrine
etabolic disturbancesypophosphataemia, hypomagnesaemia and hypokalaemiall cause muscle weakness. Hypothyroidism and hypoadre-alism may also contribute to difficulty weaning. However,ata are not available that specifically evaluate the relativeontribution of each of these metabolic derangements touration of mechanical ventilation weaning failure.
ole of corticosteroids
he importance of corticosteroids in weaning failure, eitherheir relative deficiency or supplementation, needs furthernalysis. Physiological replacement of steroids is commonn current clinical practice as clinicians target an absoluter relative cortisol deficiency [89]. Data from the corticus
lsStvpdo
A
Tgfhptndilatpn
R
Rsverc
F
Fotww
Qw
A
PccvtrS
Weaning from mechanical ventilation
study may help further define the role of steroids for the cri-tically ill patient. In one outcome study of survivors of ARDS[74], the absence of corticosteroids was associated with abetter functional outcome. The effect of drug dosage needsfurther elucidation, with higher doses than those recommen-ded for physiological replacement therapy being associatedwith severe myopathy [72]. Any exposure to exogenous corti-costeroids during the ICU stay might cause muscle weaknessand possibly contribute to the duration of mechanical ven-tilation.
Corticosteroid therapy impairs glycaemic control. Signi-ficant reduction in the mean duration of mechanicalventilation has been reported in a population of surgicalpatients in whom a tight glycaemic control regimen was ins-tituted [90]. Whether this effect is translated to a broadergroup of medical intensive care patients awaits analysis.
Nutrition
OverweightThe mechanical effects of obesity (overweight is definedas body mass index > 25 kg m−2) with decreased respira-tory compliance, high closing volume/functional residualcapacity ratio and elevated WOB might be expected toimpact on the duration of mechanical ventilation. In a secon-dary analysis of the data for the ARDS Network trials ofmechanical ventilation (6 versus 12 ml kg−1 VT), the dura-tion of mechanical ventilation was similar for overweightand obese patients compared with the normal body weightgroup (18.5—24.9 kg m−2) [91]. Another study looked at theeffect of obesity on length of ICU stay, which was increased,but the duration of mechanical ventilation was not [92].
MalnutritionAlthough malnutrition has been reported in as high as 40%of critically ill patients, data linking it to weaning dif-ficulty are limited. For instance, in the ARDS Networktrials, 4.7% of patients were defined as underweight. Under-weight patients, defined as those with a body mass index< 20 kg m−2, may suffer depressed ventilatory drive [93],limited muscle mass and weaning difficulty.
Ventilator-induced diaphragm dysfunction andcritical illness oxidative stress
Ventilator-induced diaphragm dysfunction and critical ill-ness oxidative stress is defined as loss of diaphragmforce-generating capacity that is specifically related touse of controlled mechanical ventilation [94]. The patho-physiology comprises muscle atrophy, structural injury,fibre-type transformation and remodelling. In rabbit dia-phragm models, after 72 h of controlled mechanicalventilation mitochondrial swelling, myofibril damage andincreased lipid vacuoles are noted [95]. Oxidative stressmay play an important role in this process, with oxidativemodifications noted within 6 h of commencing controlled
mechanical ventilation [96].The role of trace element and vitamin supplementationsthat support antioxidant function in the critically ill patientis evolving. One prospective randomised trial [97] found that�-tocopherol and ascorbic acid supplementation reduced
ceprt
81
ength of ICU stay and duration of mechanical ventilation in aurgical ICU, when compared with unsupplemented controls.uch supplementation, particularly selenium, would appearo be safe in critically ill patients [98], though route (enteralersus parenteral) and dosage require further analysis. It isroposed that this may help attenuate ventilator-inducediaphragmatic dysfunction [94]. Genetic susceptibility toxidative stress remains unconfirmed.
naemia
here remains considerable debate as to the desired haemo-lobin level when considering whether a patient is suitableor weaning. Previous weaning guidelines referenced aaemoglobin target of ≥ to 8—10 g dL−1. In a large pros-ective randomised study, Hebert et al. [99] have reportedhat a liberal red blood cell transfusion strategy maintai-ing haemoglobin concentration at 10—12 g dL−1 does notecrease the duration of mechanical ventilation in criticallyll patients. In a smaller group of COPD patients, transfusioned to a significant decrease of both the minute ventilationnd the WOB [100]. Randomised controlled trials are neededo help define the appropriate target for different patientopulations. The role of erythropoietin in selected patientseeds further study.
ecommendations
eversible pathology should be aggressively and repeatedlyought in all patients in groups 2 and 3. Ongoing sur-eillance for load, neuromuscular competence, metabolic,ndocrine and nutrition issues are important. Emerging lite-ature supports a search for CINMA and neuropsychologicalontributors to weaning failure.
urther research
urther research should include epidemiological evaluationf the pathophysiological contributors to weaning failure ashe patient moves from acute critical illness with difficulteaning (group 2) to chronic critical illness with prolongedeaning (group 3).
uestion 3: what is the usual process of initialeaning from the ventilator?
ssessing readiness to wean
rolonged mechanical ventilation is associated with signifi-ant morbidity and mortality. Therefore, weaning should beonsidered as early as possible in the course of mechanicalentilation. The process of initial weaning from the ventila-or involves a two-step strategy. It begins with an assessmentegarding readiness for weaning, which is then followed byBT as a diagnostic test to determine the likelihood of suc-
essful extubation. In fact, for the majority of patients, thentire weaning process simply involves confirmation that theatient is ready for extubation. Patients who meet the crite-ia reported in Table 5 should be considered as being readyo wean from mechanical ventilation. Failing to extubate
82
Table 5 Considerations for assessing readiness to wean.
Clinical assessment Adequate coughAbsence of excessivetracheobronchial secretionResolution of disease acutephase for which the patientwas intubated
Objective measurements Clinical stabilityStable cardiovascular status
(i.e. fC ≤140 beats min−1,systolic BP 90—160 mm Hg, noor minimal vasopressors)
Stable metabolic statusAdequate oxygenation
Sa,O2 > 90% on ≤ FI,O2 0.4 (orPa,O2/FI,O2 ≥ 150 mm Hg)
PEEP ≤8 cm H2OAdequate pulmonary function
fR ≤ 35 breaths min−1
MIP ≤ −20 to −25 cm H2OVT > 5 ml kg−1
VC > 10 ml kg−1
fR:VT, 105 breaths min−1 L−1
No significant respiratoryacidosisAdequate mentationNo sedation or adequatementation on sedation (orstable neurologic patient)
Data taken from [5,6,13,16—18,22]. fC: cardiac frequency; BP:blood pressure; Sa,O2: arterial oxygen saturation; FI,O2 : inspi-ratory oxygen fraction; Pa,O2: arterial oxygen tension; PEEP:
pimfva
ncglptteotaatltvs
bnbaivw[f
T
Mmttcs[uflPpTossttopafisitwsaDi[phwim
qctaptpeAlthough depressed mentation is frequently considered a
positive end-expiratory pressure; fR: respiratory frequency; MIP:maximal inspiratory pressure; VT: tidal volume; VC: vital capa-city. 1 mm Hg = 0.133 kPa.
atients who can in fact be successfully weaned is morenjurious than a failed SBT. Since many patients who do noteet all the criteria in Table 5 are able to wean success-
ully from mechanical ventilation, these criteria should beiewed as considerations for probable weaning rather thans strict criteria that must all be met simultaneously.
The initial assessment of the readiness for disconti-uation of mechanical ventilation support often involvesalculation of the rapid shallow breathing index (RSBI). Ineneral, patients should be considered for an RSBI calcu-ation and subsequent SBT earlier rather than later, sincehysicians frequently underestimate the ability of patientso be successfully weaned. For many patients, discontinua-ion of sedation is a critical step that can be achieved byither daily interruption of sedation or continuous titrationf sedation to a level that allows the patient to be adequa-ely responsive [47]. An SBT should be considered as soons possible once the patient meets the criteria in Table 5;gain, these criteria are to be taken as considerations ratherhan as rigid requirements. An initial assessment of the like-
ihood of a successful SBT is appropriate in order to avoidrials in patients with a high probability of failure. Howe-er, the predictive value of indices that attempt to predictuccessful SBT may be low in clinical practice. But it mustcdi[
J.-M. Boles et al.
e considered that pre-test probability of successful wea-ing, upon which predictive value of indices is based, maye very high because of the late measure of these indices inmajority of patients’ course. The most commonly used test
s calculation of the RSBI (respiratory frequency [fR]:VT). Aalue < 100—105 breaths min−1 l−1 predicts a successful SBTith a reported sensitivity of 0.97 and specificity of 0.65
62]. In patients in whom the clinical probability of success-ul weaning is high, the RSBI might be omitted.
he spontaneous breathing trial
ultiple studies have examined the methodology for perfor-ing an SBT. There appears to be no difference in either
he percentage of patients who pass the SBT or the percen-age of patients successfully extubated when a T-tube trial isompared with the use of low levels of pressure support (PS),uch as 7 cm H2O [6] or 8 cm H2O [101] in adults or 10 cm H2O24] in paediatric patients, or the use of CPAP [102]. These of automatic tube compensation (ATC), which adjustsor the assumed resistance of the endotracheal tube, is ateast as successful as the use of simple T-tube or low-levelS [103]. PS has been used in previous studies with the pur-ose of overcoming the resistance of the endotracheal tube.hese studies failed to account for the increased resistancef the inflamed natural upper airways following extubation,o that postextubation WOB is best approximated withoutuch compensation [38,104]. Thus, it does not make senseo use PS for the purpose of overcoming the resistance ofhe endotracheal tube. The same line of reasoning applies tother modes of ventilation that have been proposed for thisurpose, such as ATC. In the case of SBT failure because ofparticularly narrow endotracheal tube, ATC may be bene-cial. Studies demonstrate that patients who fail an SBT doo within the first ∼20 min [22,62], so the success rate for annitial SBT is similar for a 30-min compared with a 120-minrial [22,105]. The need for a longer duration trial in patientsho have previously failed weaning has not been adequately
tudied. The impact of low levels (≤5 cm H2O) of PEEP duringn SBT has not been formally studied but is likely to be small.ue to dynamic hyperinflation, patients with COPD may have
mproved pulmonary function with CPAP. Reissmann et al.106] found that patients with COPD were more likely toass a 30-min SBT when 5—7.5 cm H2O CPAP was supplied;owever, the likelihood of successful extubation in patientsho require CPAP during an SBT has not been studied. The
ncreasing use of NIV (see Question 4) following extubationay make extubation more appropriate for such patients.Criteria for passing SBT include respiratory pattern, ade-
uate gas exchange, haemodynamic stability and subjectomfort. Six large studies [16—18,22,24,25] demonstratedhat only 13% of patients who successfully passed the SBTnd were extubated required reintubation (Table 2). Inatients who do not receive an SBT and are extubated,he failure rate is ∼40% [107]. Patients who successfullyass the SBT should be extubated if neurological status,xcessive secretions and airway obstruction are not issues.
ontra-indication to extubation [108], Coplin et al. [13]emonstrated a low reintubation rate (9%) in stable brain-njured patients with a Glasgow coma score ≤4. Koh et al.109] found that Glasgow coma score did not predict extuba-
Weaning from mechanical ventilation
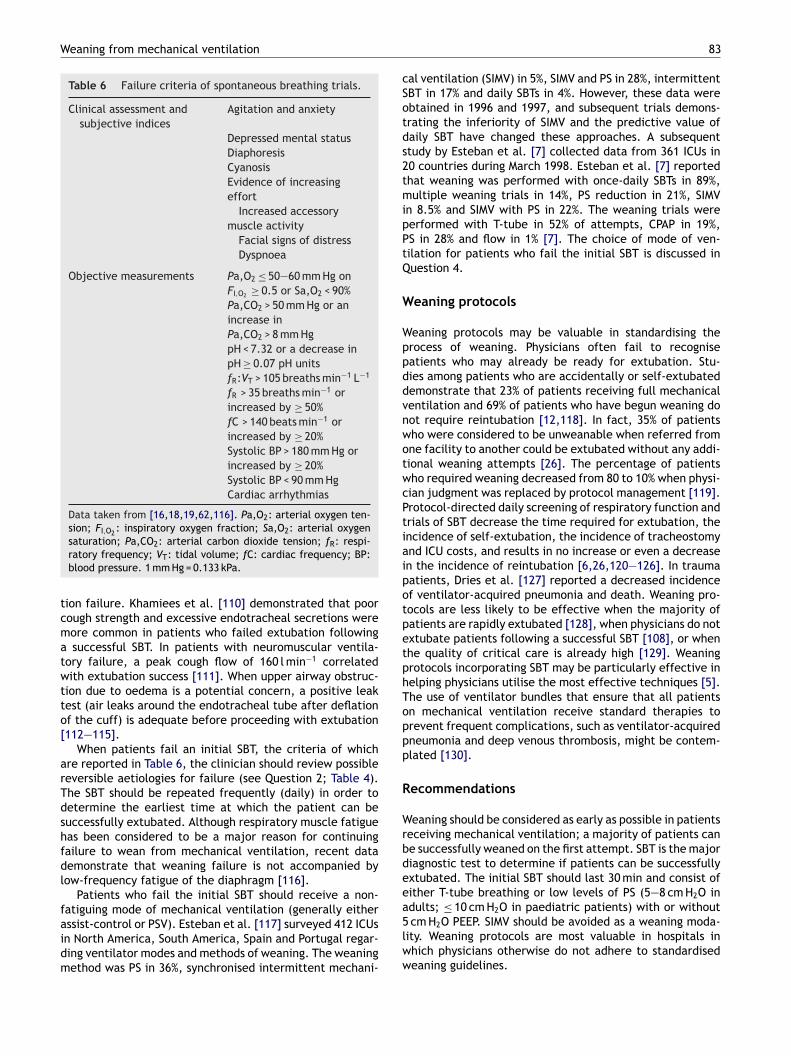
Table 6 Failure criteria of spontaneous breathing trials.
Clinical assessment andsubjective indices
Agitation and anxiety
Depressed mental statusDiaphoresisCyanosisEvidence of increasingeffort
Increased accessorymuscle activity
Facial signs of distressDyspnoea
Objective measurements Pa,O2 ≤ 50—60 mm Hg onFI,O2 ≥ 0.5 or Sa,O2 < 90%Pa,CO2 > 50 mm Hg or anincrease inPa,CO2 > 8 mm HgpH < 7.32 or a decrease inpH ≥ 0.07 pH unitsfR:VT > 105 breaths min−1 L−1
fR > 35 breaths min−1 orincreased by ≥ 50%fC > 140 beats min−1 orincreased by ≥ 20%Systolic BP > 180 mm Hg orincreased by ≥ 20%Systolic BP < 90 mm HgCardiac arrhythmias
Data taken from [16,18,19,62,116]. Pa,O2: arterial oxygen ten-sion; FI,O2 : inspiratory oxygen fraction; Sa,O2: arterial oxygen
cSotds2tmipPtQ
W
WppddvnwotwcPtiaipotpetphToppp
R
Wrbdeeadults; ≤ 10 cm H O in paediatric patients) with or without
saturation; Pa,CO2: arterial carbon dioxide tension; fR: respi-ratory frequency; VT: tidal volume; fC: cardiac frequency; BP:blood pressure. 1 mm Hg = 0.133 kPa.
tion failure. Khamiees et al. [110] demonstrated that poorcough strength and excessive endotracheal secretions weremore common in patients who failed extubation followinga successful SBT. In patients with neuromuscular ventila-tory failure, a peak cough flow of 160 l min−1 correlatedwith extubation success [111]. When upper airway obstruc-tion due to oedema is a potential concern, a positive leaktest (air leaks around the endotracheal tube after deflationof the cuff) is adequate before proceeding with extubation[112—115].
When patients fail an initial SBT, the criteria of whichare reported in Table 6, the clinician should review possiblereversible aetiologies for failure (see Question 2; Table 4).The SBT should be repeated frequently (daily) in order todetermine the earliest time at which the patient can besuccessfully extubated. Although respiratory muscle fatiguehas been considered to be a major reason for continuingfailure to wean from mechanical ventilation, recent datademonstrate that weaning failure is not accompanied bylow-frequency fatigue of the diaphragm [116].
Patients who fail the initial SBT should receive a non-
fatiguing mode of mechanical ventilation (generally eitherassist-control or PSV). Esteban et al. [117] surveyed 412 ICUsin North America, South America, Spain and Portugal regar-ding ventilator modes and methods of weaning. The weaningmethod was PS in 36%, synchronised intermittent mechani-5lww
83
al ventilation (SIMV) in 5%, SIMV and PS in 28%, intermittentBT in 17% and daily SBTs in 4%. However, these data werebtained in 1996 and 1997, and subsequent trials demons-rating the inferiority of SIMV and the predictive value ofaily SBT have changed these approaches. A subsequenttudy by Esteban et al. [7] collected data from 361 ICUs in0 countries during March 1998. Esteban et al. [7] reportedhat weaning was performed with once-daily SBTs in 89%,ultiple weaning trials in 14%, PS reduction in 21%, SIMV
n 8.5% and SIMV with PS in 22%. The weaning trials wereerformed with T-tube in 52% of attempts, CPAP in 19%,S in 28% and flow in 1% [7]. The choice of mode of ven-ilation for patients who fail the initial SBT is discussed inuestion 4.
eaning protocols
eaning protocols may be valuable in standardising therocess of weaning. Physicians often fail to recogniseatients who may already be ready for extubation. Stu-ies among patients who are accidentally or self-extubatedemonstrate that 23% of patients receiving full mechanicalentilation and 69% of patients who have begun weaning doot require reintubation [12,118]. In fact, 35% of patientsho were considered to be unweanable when referred fromne facility to another could be extubated without any addi-ional weaning attempts [26]. The percentage of patientsho required weaning decreased from 80 to 10% when physi-ian judgment was replaced by protocol management [119].rotocol-directed daily screening of respiratory function andrials of SBT decrease the time required for extubation, thencidence of self-extubation, the incidence of tracheostomynd ICU costs, and results in no increase or even a decreasen the incidence of reintubation [6,26,120—126]. In traumaatients, Dries et al. [127] reported a decreased incidencef ventilator-acquired pneumonia and death. Weaning pro-ocols are less likely to be effective when the majority ofatients are rapidly extubated [128], when physicians do notxtubate patients following a successful SBT [108], or whenhe quality of critical care is already high [129]. Weaningrotocols incorporating SBT may be particularly effective inelping physicians utilise the most effective techniques [5].he use of ventilator bundles that ensure that all patientsn mechanical ventilation receive standard therapies torevent frequent complications, such as ventilator-acquiredneumonia and deep venous thrombosis, might be contem-lated [130].
ecommendations
eaning should be considered as early as possible in patientseceiving mechanical ventilation; a majority of patients cane successfully weaned on the first attempt. SBT is the majoriagnostic test to determine if patients can be successfullyxtubated. The initial SBT should last 30 min and consist ofither T-tube breathing or low levels of PS (5—8 cm H2O in
2
cm H2O PEEP. SIMV should be avoided as a weaning moda-ity. Weaning protocols are most valuable in hospitals inhich physicians otherwise do not adhere to standardisedeaning guidelines.

8
F
FfeRSppw
Qv
Iiasfpaaa
P
PnodaohTsStSohestd4
tav
(sagm
snPc
bou
N
Icbwhbhfd
AcPlibgwb[
hptvswefibNtamstctcfpftbl
NrPt
4
urther research
uture studies should define the minimal criteria requiredor assessment of readiness for weaning (in order to allowarlier weaning), the need for a screening test such as theSBI prior to the SBT, identification of patients who pass anBT but fail extubation, the role of CPAP/PEEP in the COPDatient undergoing SBT, the required duration of the SBT inatients who fail the initial trial, and the specific aspects ofeaning protocols which improve weaning outcome.
uestion 4: is there a role for differententilator modes in more difficult weaning?
n patients requiring mechanical ventilation, weaning failures relatively common, with an estimated prevalence of 31%nd a range 26—42% [5,16,18,22]. When initial attempts atpontaneous breathing fail to achieve the goal of liberationrom mechanical ventilation, clinicians must choose appro-riate mode(s) of ventilatory support which: (1) maintainfavourable balance between respiratory system capacity
nd load; (2) attempt to avoid diaphragm muscle atrophy;nd (3) aid in the weaning process.
ressure support ventilation
SV is commonly utilised and is the sole mode of mecha-ical ventilation used during the weaning process in ∼21%f patients [7]. PSV can be used during a SBT (not furtheriscussed here) and as a weaning mode in both groups 2nd 3 (previously described). PSV used as the sole modef mechanical ventilation during initial weaning attemptsas been tested in two large randomised controlled trials.he study by Brochard et al. [18] involving 456 randomi-ed patients determined that the use of PSV compared withIMV and intermittent T-piece trials resulted in shorter dura-ion of weaning (5.7 ± 3.7 days PSV versus 9.9 ± 8.2 daysIMV). During this protocol PSV was decreased from a meanf 19 cm H2O by 2 or 4 cm H2O per day. In 130 patients whoad failed the initial SBT, Esteban et al. [16] reported thatither one daily trial or multiple daily trials of unassisted,pontaneous breathing (T-piece) more substantially reducedhe duration of weaning than either SIMV or PSV, the medianuration of weaning with each technique being 3, 3, 5 anddays, respectively.For those patients who have repeated difficulty tolera-
ing weaning, i.e. group 3 as previously defined, PSV haslso been observed to reduce the duration of mechanicalentilation (see Question 5) [26].
Lastly, it should be emphasised that in several trialsincluding those mentioned previously) intermittent use ofpontaneous breathing via a T-tube was comparable to PSVs a weaning mode. Thus, after failed SBT, the use of pro-ressively increased time on a T-piece is also an effectiveeans of liberating patients from the ventilator.
Overall, there is consensus from the group and strongupport from the literature for the use of PSV as a wea-ing mode after initial failed SBT (for group 2). The use ofSV may also be helpful in liberating patients from mechani-al ventilation after several failed attempts at spontaneous
(aa(r
J.-M. Boles et al.
reathing (group 3). The literature does not support the usef SIMV alone as a weaning mode and little data exist for these of SIMV and PSV combined.
oninvasive ventilation
n weaning, NIV has been studied for three different indi-ations, which should be strictly separated. First, NIV haseen used as an alternative weaning modality for patientsho are intolerant of the initial weaning trial. Secondly, NIVas been used as a treatment option for patients who haveeen extubated but developed ARF within 48 h. Thirdly, NIVas been used as a prophylactic measure after extubationor patients who are at high risk for reintubation but whoid not develop ARF.
lternative weaning technique for patients who failedonventional weaninghysiological studies suggest that similar levels of venti-atory support can be delivered by NIV compared to PSVn stable COPD patients who cannot tolerate spontaneousreathing. It has thus been hypothesised that in this selectroup of patients NIV might be useful as a bridge to totalithdrawal of ventilatory support; and would lower ICU mor-idity. Four studies have been published in such a setting27,34,131,132].
In the majority of studied individuals, patients developedypercapnia during initial attempts at weaning, and mostatients had evidence of COPD. Despite failure of the SBTs,he intervention groups were extubated and placed on NIVia face mask with PSV set to a minimum inspiratory pres-ure of 15 cm H2O. The control groups were conventionallyeaned with PSV (via standard mechanical ventilation) andxtubated, but the details of this procedure are not speci-ed in any of the four published papers. All trials were notlinded and the performing departments had expertise withIV. Based on these trials the use of NIV for weaning shor-ened the total duration of invasive mechanical ventilationnd ICU stay, and substantially reduced the rate of nosoco-ial infection. In two studies [27,34], a significantly higher
urvival rate could also be found in the NIV group. However,wo points need emphasis. First, although early extubationan avoid all of the complications of mechanical ventila-ion, the patients who fail SBTs may be sick with substantialomorbidities and at risk for extubation failure (discussedurther later). Thus, although NIV is useful in very selectedopulations, its use cannot be recommended for all patientsailing a SBT. Secondly, based on the definitions outlined inhis statement, patients who are extubated to NIV should note considered a weaning success until they are completelyiberated from NIV as a form of therapy for ARF.
IV as a prophylactic measure for patients with a highisk for reintubationrophylactic use of NIV has been studied in two popula-ions of surgical patients. In two studies [133,134] CPAP
5—10 cm H2O) was used to prevent reintubation in patientsfter major abdominal or vascular surgery. Compared withcontrol group (postoperative oxygen insufflation), CPAPmean 7.5 cm H2O) improved oxygenation and reduced theate of both reintubation and infection. In the study by

Weaning from mechanical ventilation
Table 7 Criteria for extubation failure.
fR > 25 breaths min−1 for 2 hfC > 140 beats min−1 or sustained increase or decrease of
> 20%Clinical signs of respiratory muscle fatigue or increased
work of breathingSa,O2 < 90%; Pa,O2, < 80 mm Hg on FI,O2 ≥ 0.50
Hypercapnia (Pa, CO2 > 45 mm Hg or ≥ 20% frompreextubation), pH < 7.33
fR: respiratory frequency; fC: cardiac frequency; Sa,O2: arterial
itahit
atpbfofc
C
Caplrasdctwcwtostpccpdct
niamoCTv
A
Tting for the nonlinear pressure drop across the endotracheal
oxygen saturation; Pa,O2: arterial oxygen tension; FI,O2 : inspi-ratory oxygen fraction; Pa,CO2: arterial carbon dioxide tension.1 mm Hg = 0.133 kPa.
Bohner et al. [133] reintubation rate was not significantlyreduced with CPAP. In both studies there was a trend towardsa shorter stay in the hospital and a better survival. Lastly,studies are underway for patients from groups 2 and 3who are at high risk for extubation failure. However, nofirm recommendations can be made for this select groupof patients.
NIV for the treatment of respiratory insufficiency afterextubation (postextubation failure)Postextubation failure is defined mainly by clinical crite-ria (Table 7). It has a mean prevalence of 6.3—17.7% andis associated with increased ICU mortality. Two small single-centre trials [135,136] studied organ transplant patients whodeveloped respiratory insufficiency after extubation. NIVimproved oxygenation and reduced the fR significantly, com-pared with oxygen insufflation alone. PSV was also superiorto PEEP [135]. In the study by Antonelli et al. [136], thereintubation rate and the duration of ICU stay were lower inthe control group, but neither study revealed an advantagein terms of mortality.
In two large randomised, multicentre studies [137,138],NIV was evaluated for treatment of acute respiratory insuf-ficiency occurring in the first 48 h after extubation and wascompared with standard oxygen therapy. Neither study sho-wed advantages for the use of NIV. In the study by Estebanet al. [138], the NIV group had worse survival comparedwith the oxygen group. The authors hypothesised that a 10-hdelay in reintubation was the cause of the increased mor-tality in the NIV group [138]. However, both studies haveimportant limitations: in the study by Keenan et al. [137],it is probable that both the inspiratory and expiratory pres-sures set on the ventilator (10 and 5 cm H2O, respectively)were too low, and, as the authors point out, the experienceof the ICU staff with NIV was limited. The trial conduc-ted by Esteban et al. [138] focused mostly on patients withmild respiratory failure (mean fR 29 breaths min−1, pH 7.39,Pa,CO2 46 mm Hg, Pa,O2 79 mm Hg, at the time of randomi-sation) and the different modes, ventilator type or settingsfor mechanical ventilation were not clear. In addition, thecriteria for the discontinuation of NIV and the crossover ofcontrol patients to NIV were unclear. Lastly, a post hoc ana-
lysis of this data revealed a lower reintubation rate for thesmall number (10%) of patients with COPD included in thetrial [138]. Overall, the literature does not support the useof NIV as a treatment for extubation failure.tamp
85
One important issue to emphasise in all of the NIV trialss patient mix and aetiology of the respiratory failure beingreated. The evidence for use of NIV in COPD patientsnd those with hypoxic respiratory failure with concomitantypercapnic respiratory failure is substantially stronger thann other groups. Careful patient selection is imperative forhe use of NIV and for future study design.
In conclusion, NIV cannot generally be recommended forny of the specific topics mentioned previously. However,here is promise that for some subgroups (hypercapnic res-iratory insufficiency, especially in COPD patients) NIV maye helpful in expediting the weaning process. Clear criteriaor discontinuation of NIV must be defined. Positive effectsf a prophylactic CPAP or NIV treatment in patients at riskor reintubation seem likely, but larger studies have yet toonfirm this observation.
ontinuous positive airway pressure
PAP applied during spontaneous breathing in patients withcute respiratory insufficiency reduces mean intrathoracicressure, has beneficial effects on right and left ventricu-ar performance [40,139], improves oxygenation [134] andeduces the WOB [140]. From a physiological point of view,dditional application of PEEP either alone or with PSVeems logical for weaning. However, few prospective stu-ies are available. Feeley et al. [141], in a randomisedontrolled trial, concluded that PEEP in spontaneously brea-hing patients may be helpful during weaning of patientsith primarily hypoxic respiratory failure. In cardiac surgi-al patients, typically included in the previously discussedeaning group 1, Bailey et al. [142] randomised patients
o receive CPAP or T-piece trials prior to extubation andbserved no significant difference in oxygenation or timepent on mechanical ventilation. Others have hypothesisedhat the use of CPAP during weaning may be helpful torevent immediate postextubation hypoxaemia; however,ompared to T-piece trials no clear improvement in out-omes has been observed. Lastly, CPAP has been used forrophylaxis against postoperative extubation failure. Squa-rone et al. [134] observed, in a multicentre randomisedontrolled trial, that CPAP compared to oxygen supplemen-ation substantially reduced the reintubation rate.
In summary, for group 1 patients, CPAP may be an alter-ative to standard weaning modes, although its applicationn groups 2 and 3 patients has not been clearly evaluated. Inddition, although combinations of CPAP and PSV are com-only applied during the weaning period, there is also a lack
f prospective randomised controlled trials to suggest thatPAP is superior to other techniques such as PSV alone or-tube in the process of weaning from invasive mechanicalentilation.
utomatic tube compensation
he use of ATC, a ventilatory method aimed at compensa-
ube during spontaneous breathing, is at least as successfuls the use of simple T-tube or low-level PS for weaning fromechanical ventilation [103]. If an SBT fails because of aarticularly narrow endotracheal tube, ATC may be bene-

8
fitr
P
T(Ctownbh
S
RgdIdtlmbil
AAttsmbtimcbccdAcPrArt
tseahvww
pg
KTItrTatfimob(tsammtd
C
Offlwdalinstwmmhiptoptdttv2
R
6
cial. For more difficult weaning patients (groups 2 and 3)here is a lack of controlled trials to make any meaningfulecommendations about the use of ATC.
roportional assist ventilation
he physiological response to proportional assist ventilationPAV) has been studied in ventilator-dependent patients withOPD. In comparison to PSV and CPAP, there was no substan-ial difference in oxygenation, pressure time product andther physiological variables. Only when CPAP was combinedith PAV was a more substantial change in these parametersotable [143—145]. PAV is available with some respiratorsut its application is sometimes regarded as difficult andas not been investigated thoroughly in weaning trials.
ervocontrolled ventilation
apid adaptation of the ventilatory support to the chan-ing situations of a patient is one of the major factorsetermining the length of the weaning process. However,CU staff resources are often too limited to allow imme-iate response. Automatic ventilatory modes provide a toolo achieve optimal ventilatory support and an individualevel of PS with the aim of rapid extubation. Two suchodes, adaptive support ventilation (ASV) and a knowledge-ased expert system (Smartcare1), have been integratednto conventional intensive care ventilators and are avai-able on the market.
daptive support ventilationSV is based on a computer-driven closed-loop regula-ion system of the ventilator settings, which is responsiveo changes in both respiratory system mechanics andpontaneous breathing efforts [146]. At the beginning ofechanical ventilation, the clinician enters the patient’sody weight and sets the desired percentage of minute ven-ilation (100% being equal to 100 ml kg−1 body weight min−1
n adult patients), as well as the FI,O2 , level of PEEP andaximal inspiratory pressure (MIP). Thereafter, mechani-
al ventilation starts with closed-loop regulation algorithmsased on real-time determination of the expiratory timeonstant [147]. Adjustment of inspiratory pressure, dutyycle and fR (to ensure an fR and minute ventilation withinefined limits) may improve patient-ventilator interactions.ny spontaneous breathing efforts trigger either a pressure-ontrolled breath or a spontaneous breath with inspiratoryS, the level of which is adjusted to meet the target respi-atory frequency to tidal volume ratio (fR:VT) combination.SV can thus manage the spectrum of ventilatory supportanging from controlled mechanical ventilation to PS, up tohe preextubation weaning trial.
Two nonrandomised trials [148,149] and one randomisedrial [150] evaluating ASV during weaning have been publi-hed, all focused on postcardiac surgery patients. Earlierxtubation and fewer ventilator adjustments, as well as
reduced need for arterial blood gas measurements andigh-pressure alarms have been documented [150]. Howe-er, these results should be interpreted with caution, as ASVas compared with SIMV, which has been shown to be theorst weaning mode [16]. Therefore, further studies com-
Iars
J.-M. Boles et al.
aring ASV with other weaning techniques are necessary toain insights of the utility of this mode.
nowledge-based expert systemhis system, which is presently integrated in a standard
CU ventilator (Evita XL; Dräger, Lübeck, Germany) underhe brand name Smartcare®, has been developed over seve-al years and is based on fuzzy logic algorithms [151,152].he system follows two main goals. The first is a real-timedaptation of the level of pressure support to maintainhe patient within a ‘‘comfort’’ zone. This is defined as aR of 15—30 breaths min−1 (ranging up to 34 breaths min−1
n patients with neurological disease), a VT above mini-um threshold (250 ml if body weight is < 55 kg and 300 ml
therwise) and an end-tidal expiratory carbon dioxideelow maximum threshold (7.3 kPa (55 mm Hg) or 8.6 kPa65 mm Hg) in patients with COPD). To reach these targets,he level of PS is periodically adapted by the system inteps of 2—4 cm H2O. Secondly, the device also includes anlgorithm of a stepwise decrease of PS with the aim of auto-atically performing an SBT. The system has been shown toaintain a patient in the comfort zone more successfully
han clinician-directed adjustments [153]. Additional stu-ies are needed to evaluate its efficacy in difficult weaning.
ontrolled mechanical ventilation
lder studies have suggested that in patients weaningrom mechanical ventilation there is evidence of diaphragmatigue and possibly injury. This may occur because theoad on the respiratory muscles of patients who fail toean is increased to levels that would predictably pro-uce fatigue in the respiratory muscles if patients werellowed to continue spontaneous breathing without venti-ator assistance (i.e. the tension-time index is substantiallyncreased). Thus, by this logic, the use of controlled mecha-ical ventilation (CMV) to rest the fatiguing diaphragmeems reasonable. However, Laghi et al. [116] demonstra-ed that, despite greater load and diaphragmatic effort,eaning failure patients do not develop low-frequencyuscle fatigue, although these patients displayed diaphrag-atic weakness. Furthermore, a number of animal studies
ave demonstrated that CMV induces diaphragm musclenjury (ventilator-induced diaphragm dysfunction) [94]. Thishenomenon occurs in animals and is evident after short-erm application of CMV. The aetiology is unknown but thebserved decrease in diaphragm compound action muscleotentials has been attributed to oxidative stress withinhe muscle and muscle atrophy. Whether the diaphragmamage attributed to controlled ventilation is indeed largerhan during assist-control or PSV remains unclear. Therefore,here is no clear advantage of CMV compared with otherentilatory modes in patients with difficult weaning (group).
ecommendations
n groups 2 and 3 patients (patients failing prior attemptst SBT), PSV or assist-control ventilation should be favou-ed. NIV techniques to shorten the duration of intubationhould be considered in selected patients, especially those

mod
PTttfApb
TTltTotoacics
TAsafflr[rsstsE3epvt[vbost
Weaning from mechanical ventilation
with hypercapnic respiratory failure. NIV should not be rou-tinely used as in the event of extubation failure and shouldbe used with caution in those patients with hypoxic respi-ratory failure. CPAP may be effective in preventing hypoxicrespiratory failure in patients after major surgery; otherwisethere is no clear advantage over other modes of mechanicalventilation used during weaning. Servocontrolled ventilationmay be an additional tool for reducing time on mechanicalventilation; however, the numbers of studies are too limitedto make firm recommendations.
Further research
In groups 2 and 3 patients, well-designed randomisedcontrolled trials comparing different modes of mechanicalventilation and the physiological impact on weaning are nee-ded. Investigating the impact of ventilator-induced muscleinjury and fatigue in humans is necessary.
Question 5: how should patients withprolonged weaning failure be managed?
A significant number of patients will experience prolon-ged weaning failure despite multiple weaning attemptsfollowing SBTs. Although specific epidemiological data donot exist, one study showed that this population repre-sents ∼10% of ICU admissions and consumes a significantamount of the overall ICU patient-days and ∼50% of finan-cial resources [154]. Two other studies demonstrated thatup to 20% of medical ICU patients remained dependent onventilatory support after 21 days [155,156].
Assuming that reversible factors have been optimised(e.g. cardiac, metabolic, etc.), the eventual clinical out-come of patients with prolonged weaning failure will dependon the long-term trajectory of the underlying disease. Stu-dies have shown that patients with neuromuscular and chestwall disorders are less likely to be weaned completelycompared with patients with COPD. However, the formerpatients have decreased mortality compared with patientswith COPD, who have the highest mortality [157].
The role of tracheostomy
Tracheostomy has become an increasingly common interven-tion in ICUs [158] with the introduction of percutaneoustechniques performed by the intensivist at the bedside[159]. It would now be unusual for clinicians to persistwith orotracheal intubation in patients perceived as beingdifficult to wean, in the absence of contra-indications totracheostomy.
Proposed advantages for tracheostomy include easierairway management, improved patient comfort and com-munication, reduction in sedative use, earlier weaningfrom respiratory support, improved respiratory mechanics,earlier transition to oral feeding, reduced oropharyngeal
trauma and prevention of ventilator-acquired pneumonia[156,160]. Adverse effects include misplacement, haemor-rhage, obstruction, displacement, impairment of swallowingreflexes and late tracheal stenosis. Conversely, cliniciansshould also consider the possibility that tracheostomy pro-aeas
87
otes only short-term survival and increases the proportionf dependent survivors suffering a heavy burden of chronicisease [158].
atient comfort and sedationhe benefits of minimising sedation [47,161] might be easiero achieve with a tracheostomy rather than an orotrachealube. Also, nurses consider that tracheostomy is more com-ortable for patients undergoing prolonged weaning [162].
small prospective survey found that only four out of 20atients shared this view [163]. Such research is complicatedy problems with patient recall and communication.
echnical, mechanical and safety aspectsracheostomy may offer a more secure airway than a trans-aryngeal tube [160] with fewer accidental extubations,hough this will also reflect issues of staffing and expertise.racheostomy may reduce WOB by improving some aspectsf pulmonary mechanics [164,165], but there is no evidencehat this is linked to reductions in weaning time or lengthf stay. Although several studies report reduced ventilator-cquired pneumonia rates in patients with a tracheostomyompared with orotracheal tubes [166—169], this effect isnconsistent [170,171] and most studies are methodologi-ally weak. The issue requires further examination linked totudies examining timing of tracheostomy.
iming of tracheostomylthough prolonged translaryngeal intubation causes tis-ue trauma, promotes bacterial translocation and infection,nd usually requires sedation to reduce patient discom-ort, there is little evidence to guide optimal timingor a tracheostomy, in part because of the methodo-ogical diversity in the 15 studies and one systematiceview which have been conducted in this area (Table 8)109,160,166—169,172—181]. Only eight of these studies areandomised controlled trials, four of which have been publi-hed since 1997 [168,169,172,173]. Rumbak et al. [169]creened 135 medical ICU patients to perform a prospec-ive randomised study of 120 patients, with weaning andedation protocols used to standardise care between groups.arly tracheostomy (within two days of admission) halved0-day mortality rate and reduced pneumonia, accidentalxtubation and ICU length of stay. However, 10 out of 60atients randomised to deferred tracheostomy weaned fromentilation without requiring this intervention, emphasisinghe need for better predictors of ventilator dependence182—184]. Such predictors will need to take into accountariable weaning techniques and their generalisability wille affected by case-mix variation and prior probabilitiesf weaning in different populations. A smaller randomisedtudy in 44 patients with burns showed no advantage toracheostomy performed on average at day 4 postburn [173].
Prospective randomised trials to determine the mostppropriate timing for tracheostomy will need to: ensurequipoise between participating centres; define ‘‘early’’;nd consider the impact of case-mix variation. Evaluationhould include patient-centred outcomes.
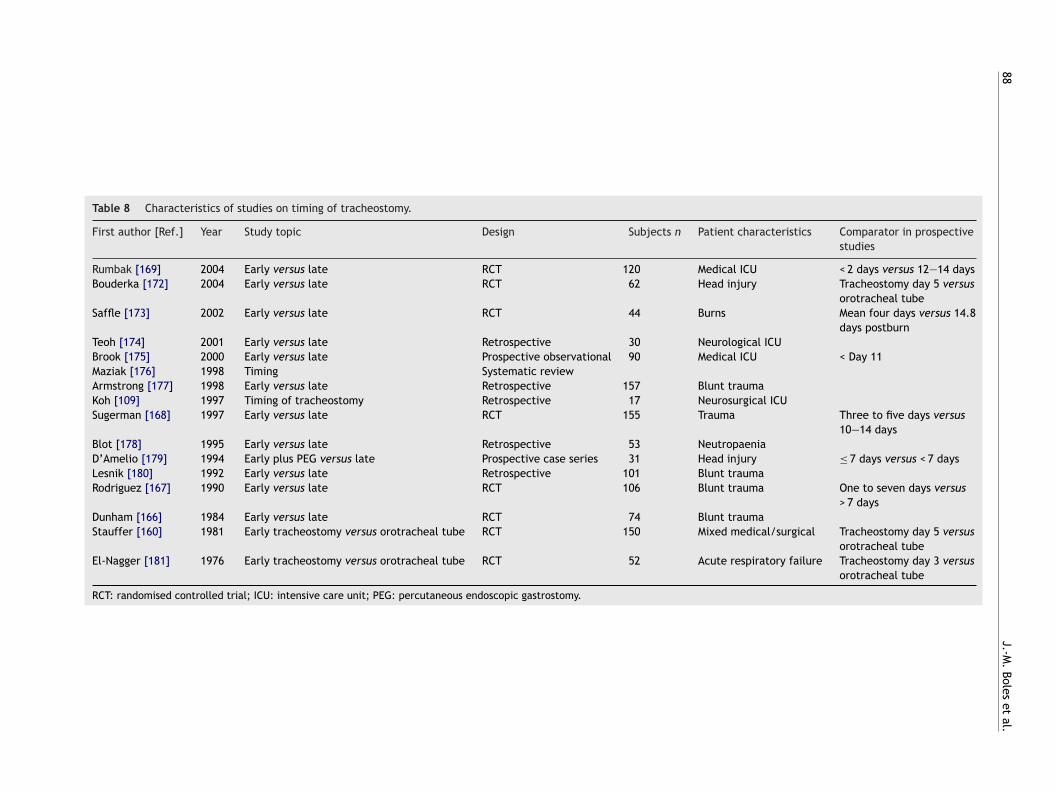
88J.-M
.Boles
etal.
Table 8 Characteristics of studies on timing of tracheostomy.
First author [Ref.] Year Study topic Design Subjects n Patient characteristics Comparator in prospectivestudies
Rumbak [169] 2004 Early versus late RCT 120 Medical ICU < 2 days versus 12—14 daysBouderka [172] 2004 Early versus late RCT 62 Head injury Tracheostomy day 5 versus
orotracheal tubeSaffle [173] 2002 Early versus late RCT 44 Burns Mean four days versus 14.8
days postburnTeoh [174] 2001 Early versus late Retrospective 30 Neurological ICUBrook [175] 2000 Early versus late Prospective observational 90 Medical ICU < Day 11Maziak [176] 1998 Timing Systematic reviewArmstrong [177] 1998 Early versus late Retrospective 157 Blunt traumaKoh [109] 1997 Timing of tracheostomy Retrospective 17 Neurosurgical ICUSugerman [168] 1997 Early versus late RCT 155 Trauma Three to five days versus
10—14 daysBlot [178] 1995 Early versus late Retrospective 53 NeutropaeniaD’Amelio [179] 1994 Early plus PEG versus late Prospective case series 31 Head injury ≤ 7 days versus < 7 daysLesnik [180] 1992 Early versus late Retrospective 101 Blunt traumaRodriguez [167] 1990 Early versus late RCT 106 Blunt trauma One to seven days versus
> 7 daysDunham [166] 1984 Early versus late RCT 74 Blunt traumaStauffer [160] 1981 Early tracheostomy versus orotracheal tube RCT 150 Mixed medical/surgical Tracheostomy day 5 versus
orotracheal tubeEl-Nagger [181] 1976 Early tracheostomy versus orotracheal tube RCT 52 Acute respiratory failure Tracheostomy day 3 versus
orotracheal tube
RCT: randomised controlled trial; ICU: intensive care unit; PEG: percutaneous endoscopic gastrostomy.

pmssmaoc
rcodbmpicidd
S
Aswwpaplr
ntapfi
STuia
5s5la[
md
Weaning from mechanical ventilation
OutcomeCohort studies report longer duration of mechanical ven-tilation and ICU and hospital stay in tracheostomisedpatients [156,185—187]. Effects on mortality are incon-sistent [185,188]. A retrospective 3-yr review of 549 patientswith tracheostomy reported poor survival and functionaloutcomes [186]. The rate of tracheostomy in the NorthCarolina Medicare database [158] has increased over a 10-year period from 8.3 to 24.2 cases per 100,000; 25% ofpatients died in hospital, 23% were discharged to a skilled-nursing facility, 35% were discharged to rehabilitation orlong-term care units, and only 8% were discharged home.There are few prospective randomised controlled studiesthat have evaluated these factors objectively from thepatients’ perspective and in terms of longer-term outcomes.The absence of such studies may reflect lack of equipoiseamongst clinicians or a feeling that tracheostomy is a prag-matic approach to patient care which does not requireevaluation. Research methodologies will need to adjust forlocal circumstances such as existence of long-term weaningfacilities.
Percutaneous tracheostomyPercutaneous dilational tracheostomy is increasingly utili-sed as an alternative to conventional surgical tracheostomy.A recent meta-analysis demonstrated this technique to beassociated with fewer complications compared with surgicaltracheostomy [189]. No difference was observed betweenthe two techniques regarding overall procedure-relatedcomplications or death. A recent prospective, randomisedstudy comparing percutaneous dilational tracheostomy withsurgical tracheostomy in critically ill patients demonstra-ted the former to be a cost-effective alternative to surgicaltracheostomy with no difference in ICU or hospital lengthof stay. The reduction of costs resulted from the procedurebeing performed in the ICU rather than consuming operatingroom facilities and personnel [190].
Rehabilitation
Rehabilitation is the process of restoring health or normallife by training and therapy after illness, but it would seempreferable to do this proactively by optimising and preser-ving physiological reserve at the earliest possible stage inacute disease, as well as trying to restore it during the laterphases of chronic critical illness.
Patients who survive the acute phase of critical ill-ness experience a wide range of physical disabilities [74],including: neuromyopathies; muscle wasting, weakness andfatigability; joint deformities and contractures; and theadditional residual disease-related damage to specific organsystems. Patients who remain ventilator-dependent in theICU may suffer the additional burden of continued systemicinflammation and catabolism combined with limited mobi-lity and suboptimal nutrition, and this particularly affectsthe neuromuscular system. One study showed that 62% of
difficult-to-wean patients had neuromuscular disease suffi-ciently severe enough to account for ventilator dependency[48]. These observations suggest that efforts to prevent ortreat respiratory muscle weakness might have a role in redu-cing weaning failure.cwCsw
89
Rehabilitation efforts have focused on improving muscleower and endurance through passive and active move-ents, posture and different forms of exercise. Many studies
how effects of modest magnitude on various surrogate mea-ures, such as respiratory physiology, oxygen consumption,uscle fibre atrophy and protein loss. There is, however,lack of studies demonstrating an impact of rehabilitation
n the prevention or reversal of weaning failure or otherlinically important outcomes.
In addition to neuromuscular disorders, patients expe-ience other physical and psychosocial effects, such as:hanges to skin and hair; endocrine impairment; disordersf sleep, mood and libido; and pain. The high symptom bur-en of survivors of chronic critical illness is accompaniedy mortality rates of ∼50% at 3 months [191]. Close familyembers are also affected by what is in effect a form ofost-traumatic stress syndrome [192]. Since multifacetednterventions such as self-help rehabilitation programmesan improve physical function after critical illness [193],t is possible that improvements in clinical outcomes forifficult-to-wean patients might be achieved using a metho-ology similar to that of ventilator bundles.
pecialised weaning units
cute care units probably lack the necessary focus, per-onnel and organisational structure to care for patientsith prolonged weaning failure. In contrast, specialisedeaning units (SWUs) offer specialised teams (e.g. nurses,hysiologists, respiratory therapists, nutritionists, etc.) andn appropriate ‘‘bridge to home’’ environment for suchatients and their families (e.g. privacy, daytime activity,onger visiting hours and undisturbed sleep). They alsoelieve pressure on scarce ICU beds.
These units can be of two types: (1) step-down units oroninvasive respiratory care units within acute care hospi-als; and (2) regional weaning centres that serve severalcute care hospitals within the region.The type of unitreferable will depend on the healthcare structure andnancing system of each individual region or country.
Observational studies indicate that 34—60% of patients inWUs can be weaned successfully from ventilatory support.hese studies also suggest that successful weaning can occurp to three months after admission to these units. Moremportantly, the long-term mortality rate is not adverselyffected by the transfer to an SWU [194,195].
Of the successfully weaned patients, ∼70% (range0—94%) are discharged home alive; however, the one-yearurvival rate for these patients ranged 38—53%. Hence, only—25% of patients admitted to a specialised weaning faci-ity can be expected to be ventilator independent and alivet home 1 yr after their initial respiratory failure (Fig. 2)196—201].
The clinical outcome of patients requiring prolongedechanical ventilation is largely driven by the underlyingisease. For example, one study showed that weaning suc-
ess was highest in postoperative patients (58%) and thoseith acute lung injury (57%), and lowest in patients withOPD or neuromus-cular disease (22%) [202]. The long-termurvival rate after successful weaning is worse in patientsith severe COPD compared with non-COPD patients [201].
90
Fl
Sacisc
Ic[rtd
m[pwfi(tpcdco
aqdtotmtdo
rcsett
H
Aprp(cduvihsfw
T
SapWfibteoanmdlahr
opscaTbObf[c
Several recent studies suggest that routine palliative
igure 2 Mortality and weaning process in patients with pro-onged weaning failure. SBT: spontaneous breathing trial.
Few studies have compared outcomes of care betweenWUs and ICUs. A controlled historical study by Gracey etl. [198] showed that the mortality rate decreased signifi-antly after a dedicated ventilator unit had been openednside an acute care hospital. However, given service pres-ures and financial constraints, it is unlikely that randomisedontrolled comparisons will be performed.
SWUs may be cost-effective alternatives to acuteCUs. Several observational studies estimate lower dailyosts of care for ventilator-dependent patients in SWUs157,203—205], primarily through lower salaries, andeduced building charges, monitoring (e.g. noninvasive),echnical equipment (e.g. portable ventilators), cost ofiagnostics and therapeutics.
Weaning strategies used in SWUs have included inter-ittent mandatory ventilation/PS, PSV, and T-tube trials
26,202,203,206,207]. Vitacca et al. [26] studied 75 COPDatients randomised to PSV or T-tube SBT, both of whichere delivered via the use of protocols. No significant dif-
erence was found in weaning success rate (73 versus 77%n the PSV and SBT group, respectively) and mortality rate11.5 versus 7.6%). However, when the outcomes of applyinghese defined protocols were retrospectively compared withrior uncontrolled clinical practice, the 30-day weaning suc-ess rate was significantly greater (87 versus 70%). Thus, inifficult-to-wean patients, the use of clearly defined proto-ols, independent of the mode used, may result in betterutcomes than uncontrolled clinical practice.
Many issues remain unresolved for SWUs. These includedmission criteria, minimum operating standards and staffualifications. Although some SWUs accept every ventilator-ependent patient, most apply admission criteria, such aswo documented failed weaning trials [198], the presencef a tracheostomy tube, clinical stability and the poten-ial to benefit from rehabilitation [208,209]. These criteria
ay (appropriately) select patients who are more likelyo benefit but may also favourably influence the outcomeata of individual SWUs. Standards for the establishmentf SWUs might include acceptable nurse/patient ratios, the
csic
J.-M. Boles et al.
equirement for a supervising pulmonary physician, qualifi-ations of respiratory therapists and the presence of certainpecialised staff members (e.g. nutritionists, psychologists,tc.). Without such benchmarking, the possibility exists ofransferring patients from a well-functioning ICU to a less-han-optimal SWU.
ome ventilation
s previously noticed, a significant number of patients withrolonged weaning failure remain ventilator dependent,equiring long-term ventilatory support, which may now berovided as NIV in the home setting. A study from ClevelandOH, USA) [208] in patients following ARDS, cardiothora-ic surgery or with COPD showed that 9% of patients wereischarged home with partial ventilatory support, with 1%sing NIV and 8% requiring partial mechanical ventilationia the tracheostomy. Schönhofer et al. [201] showed thatn a predominantly COPD population, 75% were dischargedome from an SWU, of whom 31.5% required home NIV. A UKtudy [157] reported that of surviving patients, 38% wereully weaned and 35% required further home ventilation,ith the majority using NIV.
erminal care for the ventilator-dependent patient
tudies have measured the quality of life of patientsfter prolonged mechanical support [210—212] and of thoseatients receiving home mechanical ventilation [213—217].hile these studies report varying results, there are a signi-cant number of patients who rate their quality of life aseing low. Patients with COPD rate their quality of life lowerhan those patients with neuromuscular disorders [216]. Thexistence of a poor quality of life coupled with the prospectf low survival rates might prompt autonomous patients whore ventilator dependent to consider withdrawal of mecha-ical ventilation or those who are not ventilator dependentay decide to forgo future ventilatory attempts. Sharedecision making is the most appropriate model for forgoingife-sustaining support, and clinicians will need to provideccurate prognostic information because such informationas been shown to influence patients’ preferences regardingesuscitation [218].
When patients lack decision-making capacity, the lawsf individual regions and countries will determine the legalermissibility of surrogates’ (medical or nonmedical) deci-ions to forgo life-sustaining support. These laws, and theircumstances in which they may be applied, vary widely,nd in some European countries are currently under review.here are also substantial personal, religious and culturaliases which affect the behaviour of care givers [219,220].f concern are studies demonstrating poor communicationetween the physicians of critically ill patients and theiramilies [221] or termination of support without family input222]. SWUs should ensure that these issues are openly dis-ussed and incorporated in management policies.
are or ethics consultation can improve the quality of deci-ion making regarding withdrawing mechanical ventilationn the acute ICU setting [223—225]. Input from palliativeare specialists and ethicists in the chronic setting would

(MRmA(
R
Weaning from mechanical ventilation
seem appropriate as well. Several commentators offer gui-dance for clinicians in the practical aspects of withdrawingmechanical ventilation, including the development of astandardised order form for the withdrawal of life supportin the ICU [226,227].
Recommendations
Studies of rehabilitation should examine multifaceted inter-ventions focused on improving patient-centred outcomes.Care bundles might be a relevant research methodology forthis purpose. SWUs may be cost-effective for certain groupsof patients with prolonged weaning failure but guidelines areneeded for admission criteria, minimum structural and ope-rating standards, and risk-adjusted benchmarks that permitassessment of efficacy and safety. NIV in the home settingmight be considered an option for patients with prolongedweaning failure after careful attention to home dischargeplanning. Decisions to withhold or withdraw mechanicalventilatory support should reflect a shared decision-makingmodel that is informed by a full disclosure of prognostic dataand should be based on patient-centred interests and values.
Further research
Adequately powered clinical studies of tracheostomy shouldevaluate optimal timing and longer-term patient-centredoutcomes. Controlled studies are needed to assess theimpact of mechanical ventilatory support after hospitali-sation, especially in chronic obstructive pulmonary diseasepatients, addressing outcomes such as exacerbation fre-quency, health status and costs. Further studies are requiredto delineate the process of terminal discontinuation of ven-tilatory support in specialised weaning units.
Conflict of interest
Statement of interest for J. Bion, A. Connors, M. Herridge,R. Pearl, H. Silverman, M. Stanchina and T. Welte can befound at www.erj.ersjournals.com/misc/statements.shtml.
Acknowledgements
International Consensus Committee members: M. Levy (Bos-ton, MA, USA) and M. Zelter (Paris, France). Scientificadvisors: M. Elliott (Leeds, UK) and M. Tobin (Hines, IL, USA).Experts who wrote reports and delivered presentations:J. Mancebo (Barcelona, Spain), P. Navalesi (Pavia, Italy),S. Epstein (Boston), S. Carson (Chapel Hill, NC, USA), M.Polkey (London, UK), T. Similowski (Paris), M.R. Pinsky (Pitts-burgh, PA, USA), M.W. Elliott (Leeds), F. Laghi (Hines), A.Torres (Barcelona), B. de Jonghe (Poissy, France), A. Jubran(Hines), M. Tobin (Hines), L. Brochard (Créteil, France),C. Sassoon (Long Beach, CA, USA), M. Vitacca (Gussago,Italy), T. Vassilakopoulos (Athens, Greece), A. Rossi (Ber-
gamo, Italy), S. Nava (Pavia, Italy), N. Hill (Boston), P.Jolliett (Geneva, Switzerland), B. Schönhofer (Hannover,Germany), E. L’Her (Brest, France), R. Gosselink (Leuven,Belgium), J.R. Curtis (Seattle, WA, USA). Jury: J-M. Boles(chairman; Brest), J. Bion (Birmingham, UK), A. Connors91
Cleveland, OH, USA), M. Herridge (Toronto, Canada), Brianarsh (Dublin, Ireland), Christian Melot (Brussels, Belgium),onald Pearl (Stanford, CA, USA), Henry Silverman (Balti-ore, MD, USA), Michael Stanchina (Providence, RI, USA),ntoine Vieillard-Baron (Boulogne, France), Tobias WelteHannover, Germany).
eferences
[1] Carlet J, Artigas A, Bihari D, et al. The first Europeanconsensus conference in intensive care medicine: introduc-tory remarks. Intensive Care Med 1992;18:180—1.
[2] National Institutes of Health, Office of Medical Applicationof Research. Guidelines for the planning and management ofconsensus development conferences. Washington, US govern-ment Printing Office, 1995.
[3] Tobin MJ. Role and interpretation of weaning predictors.As presented at the 5th international consensus Confe-rence in intensive care medicine: Weaning from mechanicalventilation. Hosted by ERS, ATS, ESICM, SCCM and SRLF; Buda-pest, April 28—29,2005. Available at www.ersnet.org/ers/lr/browse/default.aspx?id52814.
[4] Esteban A, Alia I, Ibanez J, Benito S, Tobin MJ, The SpanishLung Failure Collaborative Group. Modes of mechanical ven-tilation and weaning. A national survey of Spanish hospitals.Chest 1994;106:1188—93.
[5] Ely EW, Baker AM, Dunagan DP, et al. Effect on the durationof mechanical ventilation of identifying patients capable ofbreathing spontaneously. N Engl J Med 1996;335:1864—9.
[6] Kollef MH, Shapiro SD, Silver P, et al. A randomized, controlledtrial of protocol-directed versus physician-directed weaningfrom mechanical ventilation. Crit Care Med 1997;25:567—74.
[7] Esteban A, Anzueto A, Frutos F, et al., Mechanical Ventila-tion International Study Group. Characteristics and outcomesin adult patients receiving mechanical ventilation: a 28-dayinternational study. JAMA 2002;287:345—55.
[8] Tobin MJ. Mechanical ventilation. N Engl J Med1994;330:1056—61.
[9] Cooper LM, Linde-Zwirble WT. Medicare intensive care unituse: analysis of incidence, cost, and payment. Crit Care Med2004;32:2247—53.
[10] Wagner DP. Economics of prolonged mechanical ventilation.Am Rev Respir Dis 1989;140:S14—8.
[11] Epstein SK. Decision to extubate. Intensive Care Med2002;28:535—46.
[12] Epstein SK, Nevins ML, Chung J. Effect of unplanned extuba-tion on outcome of mechanical ventilation. Am J Respir CritCare Med 2000;161:1912—6.
[13] Coplin WM, Pierson DJ, Cooley KD, Newell DW, RubenfeldGD. Implications of extubation delay in brain-injured patientsmeeting standard weaning criteria. Am J Respir Crit Care Med2000;161:1530—6.
[14] Hall JB, Wood LD. Liberation of the patient from mechanicalventilation. JAMA 1987;257:1621—8.
[15] Ely EW, Baker AM, Evans GW, Haponik EF. The prognosticsignificance of passing a daily screen of weaning parameters.Intensive Care Med 1999;25:581—7.
[16] Spanish Lung Failure Collaborative GroupEsteban A, FrutosF, Tobin MJ, et al. A comparison of four methods of wea-ning patients from mechanical ventilation. N Engl J Med1995;332:345—50.
[17] Vallverdu I, Calaf N, Subirana M, Net A, Benito S, ManceboJ. Clinical characteristics, respiratory functional parameters,and outcome of a two-hour T-piece trial in patients wea-ning from mechanical ventilation. Am J Respir Crit Care Med1998;158:1855—62.
9
2[18] Brochard L, Rauss A, Benito S, et al. Comparison of threemethods of gradual withdrawal from ventilatory supportduring weaning from mechanical ventilation. Am J Respir CritCare Med 1994;150:896—903.
[19] Jubran A, Tobin MJ. Pathophysiologic basis of acute res-piratory distress in patients who fail a trial of weaningfrom mechanical ventilation. Am J Respir Crit Care Med1997;155:906—15.
[20] Capdevila XMD, Perrigault P-F, Ramonatxo M, et al.Changes in breathing pattern and respiratory muscle perfor-mance parameters during difficult weaning. Crit Care Med1998;26:79—87.
[21] Torres A, Gatell JM, Aznar E, et al. Re-intubation increases therisk of nosocomial pneumonia in patients needing mechanicalventilation. Am J Respir Crit Care Med 1995;152:137—41.
[22] Spanish Lung Failure Collaborative GroupEsteban A, Alia I,Tobin MJ, et al. Effect of spontaneous breathing trial durationon outcome of attempts to discontinue mechanical ventila-tion. Am J Respir Crit Care Med 1999;159:512—8.
[23] Carlucci A, Richard JC, Wysocki M, Brochard L. Noninvasiveversus conventional mechanical ventilation. An epidemiologicsurvey. Am J Respir Crit Care Med 2001;163:874—80.
[24] Farias JA, Retta A, Alia I, et al. A comparison of two methodsto perform a breathing trial before extubation in paedia-tric intensive care patients. Intensive Care Med 2001;27:1649—54.
[25] The Spanish Lung Failure Collaborative GroupEsteban A, AliaI, Gordo F, et al. Extubation outcome after spontaneous brea-thing trials with T-tube or pressure support ventilation. Am JRespir Crit Care Med 1997;156:459—65.
[26] Vitacca M, Vianello A, Colombo D, et al. Comparison oftwo methods for weaning patients with chronic obstruc-tive pulmonary disease requiring mechanical ventilation formore than 15 days. Am J Respir Crit Care Med 2001;164:225—30.
[27] Ferrer M, Esqinas A, Arancibia F, et al. Noninvasive ventilationduring persistent weaning failure. Am J Respir Crit Care Med2003;168:70—6.
[28] Brochard L. Pressure support is the preferred weaningmethod. As presented at the 5th international consen-sus conference in intensive care medicine: weaningfrom mechanical ventilation. Hosted by ERS, ATS, ESICM,SCCM and SRLF; Budapest, April 28—29,2005. Available atwww.ersnet.org/ers/lr/browse/default.aspx?id52814.
[29] Bouadma L, Lellouche F, Cabello B, et al. Computer-drivenmanagement of prolonged mechanical ventilation and wea-ning: a pilot study. Intensive Care Med 2005;31:1446—50.
[30] Marini J, Smith T, Lamb V. Estimation of inspiratory musclestrength in mechanically ventilated patients: the mea-surement of maximal inspiratory pressure. J Crit Care1986;1:32—8.
[31] Caruso P, Friedrich C, Denari S, Ruiz S, Deheinzelin D.The unidirectional valve is the best method to deter-mine maximal inspiratory pressure during weaning. Chest1999;115:1096—101.
[32] Leung P, Jubran A, Tobin M. comparison of assisted ventilatormodes on triggering, patient effort and dyspnoea. Am J RespirCrit Care Med 1997;155:1940—8.
[33] Chastre J, Fagon JY. Ventilator-associated pneumonia. Am JRespir Crit Care Med 2002;165:867—903.
[34] Nava S, Ambrosino N, Clini E, et al. Noninvasive mechanicalventilation in the weaning of patients with respiratory failuredue to chronic obstructive pulmonary disease. A randomized,
controlled trial. Ann Intern Med 1998;128:721—8.[35] American Thoracic Society. Guidelines for the managementof adults with hospital-acquired, ventilator-associated, andhealthcare-associated pneumonia. Am J Respir Crit Care Med2005;171:388—416.
J.-M. Boles et al.
[36] Salam A, Tilluckdharry L, Amoateng-Adjepong Y, ManthousCA. Neurologic status, cough, secretions and extubation out-comes. Intensive Care Med 2004;30:1334—9.
[37] Epstein SK, Ciubotaru RL. Independent effects of etiology offailure and time to reintubation on outcome for patients fai-ling extubation. Am J Respir Crit Care Med 1998;158:489093.
[38] Straus C, Louis B, Isabey D, Lemaire F, Harf A, BrochardL. Contribution of the endotracheal tube and the upperairway to breathing workload. Am J Respir Crit Care Med1998;157:23—30.
[39] Lemaire F, Teboul JL, Cinotti L, et al. Acute left ventricu-lar dysfunction during unsuccessful weaning from mechanicalventilation. Anesthesiology 1988;69:171—9.
[40] Pinsky MR, Summer WR, Wise RA, et al. Augmentation ofcardiac function by elevation of intrathoracic pressure. ApplPhysiol 1983;54:950—5.
[41] Pinsky MR. Breathing as exercise: the cardiovascular responseto weaning from mechanical ventilation. Intensive Care Med2000;26:1164—6.
[42] Naughton MT, Rahman MA, Hara K, et al. Effect of continuouspositive airway pressure on intrathoracic and left ventriculartransmural pressure in patients with congestive heart failure.Circulation 1995;91:1725—31.
[43] Nava S, Carbone G, Di Battista N, et al. Noninvasive ventila-tion in cardiogenic pulmonary oedema: a multi-centre trial.Am J Respir Crit Care Med 2003;168:1432—7.
[44] Jubran A, Mathru M, Dries D, et al. Continuous recordings ofmixed venous oxygen saturation during weaning from mecha-nical ventilation and the ramifications thereof. Am J RespirCrit Care Med 1998;158:1763—9.
[45] Mohsenifar Z, Hay A, Hay J, et al. Gastric intraluminal pHas a predictor of success or failure in weaning patients frommechanical ventilation. Ann Intern Med 1993;119:794—8.
[46] Montgomery AB, Holle RH, Neagley SR, Pierson DJ, SchoeneRB. Prediction of successful ventilator weaning using air-way occlusion pressure and hypercapnic challenge. Chest1987;91:496—9.
[47] Kress JP, Pohlman AS, O’Connor MF, Hall JB. Daily interrup-tion of sedative infusions in critically ill patients undergoingmechanical ventilation. N Engl J Med 2000;342:1471—7.
[48] Spitzer AR, Giancarlo T, Maher L, Awerbuch G, Bowles A.Neuromuscular causes of prolonged ventilator dependency.Muscle Nerve 1992;15:682—6.
[49] De Jonghe B, Bastuji-Garin S, Sharshar T, Outin H, Brochard L.Does ICU-acquired paresis lengthen weaning from mechanicalventilation? Intensive Care Med 2004;30:1117—21.
[50] Bolton CF, Gilbert JJ, Hahn AF, Sibbald WJ. Polyneuropa-thy in critically ill patients. J Neurol Neurosurg Psychiatry1984;47:1223—31.
[51] Couturier JC, Robert D, Monier P. Polynevrites compliquantdes séjours prolonges en réanimation. [Idiopathic polyneuro-pathy in 11 patients under prolonged intensive care]. LyonMed 1984;252:247—9.
[52] Witt NJ, Zochodne DW, Bolton CF, et al. Peripheralnerve function in sepsis and multiple organ failure. Chest1991;99:176—84.
[53] Campellone JV, Lacomis D, Kramer DJ, et al. Acute myopathyafter liver transplantation. Neurology 1998;50:46—53.
[54] Garnacho-Montero J, Madrazo-Osuna J, Garcia-Garmendia JL,et al. Critical illness polyneuropathy: risk factors and clini-cal consequences. A cohort study in septic patients. IntensiveCare Med 2001;27:1288—96.
[55] Bercker S, Weber-Carstens S, Maria D, et al. Critical illness
polyneuropathy and myopathy in patients with acute respira-tory distress syndrome. Crit Care Med 2005;33:711—5.[56] De Jonghe B, Sharshar T, Lefaucheur JP, et al. Paresis acquiredin the intensive care unit: a prospective multicenter study.JAMA 2002;288:2859—67.
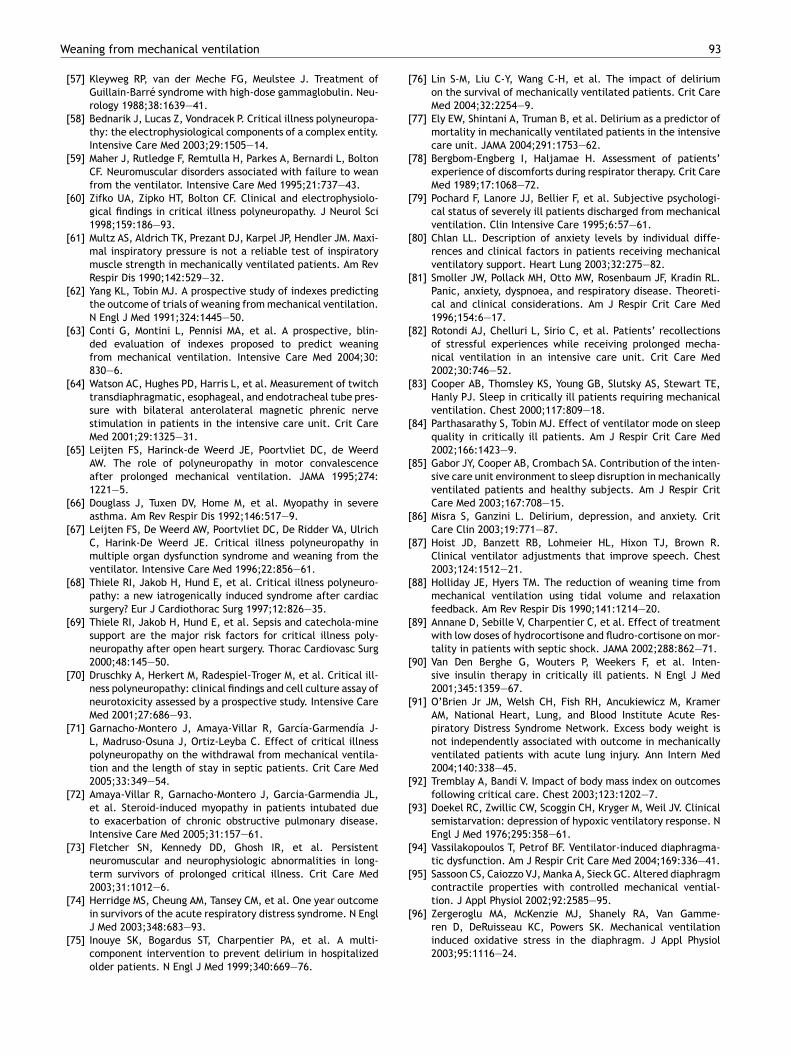
Weaning from mechanical ventilation
[57] Kleyweg RP, van der Meche FG, Meulstee J. Treatment ofGuillain-Barré syndrome with high-dose gammaglobulin. Neu-rology 1988;38:1639—41.
[58] Bednarik J, Lucas Z, Vondracek P. Critical illness polyneuropa-thy: the electrophysiological components of a complex entity.Intensive Care Med 2003;29:1505—14.
[59] Maher J, Rutledge F, Remtulla H, Parkes A, Bernardi L, BoltonCF. Neuromuscular disorders associated with failure to weanfrom the ventilator. Intensive Care Med 1995;21:737—43.
[60] Zifko UA, Zipko HT, Bolton CF. Clinical and electrophysiolo-gical findings in critical illness polyneuropathy. J Neurol Sci1998;159:186—93.
[61] Multz AS, Aldrich TK, Prezant DJ, Karpel JP, Hendler JM. Maxi-mal inspiratory pressure is not a reliable test of inspiratorymuscle strength in mechanically ventilated patients. Am RevRespir Dis 1990;142:529—32.
[62] Yang KL, Tobin MJ. A prospective study of indexes predictingthe outcome of trials of weaning from mechanical ventilation.N Engl J Med 1991;324:1445—50.
[63] Conti G, Montini L, Pennisi MA, et al. A prospective, blin-ded evaluation of indexes proposed to predict weaningfrom mechanical ventilation. Intensive Care Med 2004;30:830—6.
[64] Watson AC, Hughes PD, Harris L, et al. Measurement of twitchtransdiaphragmatic, esophageal, and endotracheal tube pres-sure with bilateral anterolateral magnetic phrenic nervestimulation in patients in the intensive care unit. Crit CareMed 2001;29:1325—31.
[65] Leijten FS, Harinck-de Weerd JE, Poortvliet DC, de WeerdAW. The role of polyneuropathy in motor convalescenceafter prolonged mechanical ventilation. JAMA 1995;274:1221—5.
[66] Douglass J, Tuxen DV, Home M, et al. Myopathy in severeasthma. Am Rev Respir Dis 1992;146:517—9.
[67] Leijten FS, De Weerd AW, Poortvliet DC, De Ridder VA, UlrichC, Harink-De Weerd JE. Critical illness polyneuropathy inmultiple organ dysfunction syndrome and weaning from theventilator. Intensive Care Med 1996;22:856—61.
[68] Thiele RI, Jakob H, Hund E, et al. Critical illness polyneuro-pathy: a new iatrogenically induced syndrome after cardiacsurgery? Eur J Cardiothorac Surg 1997;12:826—35.
[69] Thiele RI, Jakob H, Hund E, et al. Sepsis and catechola-minesupport are the major risk factors for critical illness poly-neuropathy after open heart surgery. Thorac Cardiovasc Surg2000;48:145—50.
[70] Druschky A, Herkert M, Radespiel-Troger M, et al. Critical ill-ness polyneuropathy: clinical findings and cell culture assay ofneurotoxicity assessed by a prospective study. Intensive CareMed 2001;27:686—93.
[71] Garnacho-Montero J, Amaya-Villar R, García-Garmendía J-L, Madruso-Osuna J, Ortiz-Leyba C. Effect of critical illnesspolyneuropathy on the withdrawal from mechanical ventila-tion and the length of stay in septic patients. Crit Care Med2005;33:349—54.
[72] Amaya-Villar R, Garnacho-Montero J, Garcia-Garmendia JL,et al. Steroid-induced myopathy in patients intubated dueto exacerbation of chronic obstructive pulmonary disease.Intensive Care Med 2005;31:157—61.
[73] Fletcher SN, Kennedy DD, Ghosh IR, et al. Persistentneuromuscular and neurophysiologic abnormalities in long-term survivors of prolonged critical illness. Crit Care Med2003;31:1012—6.
[74] Herridge MS, Cheung AM, Tansey CM, et al. One year outcome
in survivors of the acute respiratory distress syndrome. N EnglJ Med 2003;348:683—93.[75] Inouye SK, Bogardus ST, Charpentier PA, et al. A multi-component intervention to prevent delirium in hospitalizedolder patients. N Engl J Med 1999;340:669—76.
93
[76] Lin S-M, Liu C-Y, Wang C-H, et al. The impact of deliriumon the survival of mechanically ventilated patients. Crit CareMed 2004;32:2254—9.
[77] Ely EW, Shintani A, Truman B, et al. Delirium as a predictor ofmortality in mechanically ventilated patients in the intensivecare unit. JAMA 2004;291:1753—62.
[78] Bergbom-Engberg I, Haljamae H. Assessment of patients’experience of discomforts during respirator therapy. Crit CareMed 1989;17:1068—72.
[79] Pochard F, Lanore JJ, Bellier F, et al. Subjective psychologi-cal status of severely ill patients discharged from mechanicalventilation. Clin Intensive Care 1995;6:57—61.
[80] Chlan LL. Description of anxiety levels by individual diffe-rences and clinical factors in patients receiving mechanicalventilatory support. Heart Lung 2003;32:275—82.
[81] Smoller JW, Pollack MH, Otto MW, Rosenbaum JF, Kradin RL.Panic, anxiety, dyspnoea, and respiratory disease. Theoreti-cal and clinical considerations. Am J Respir Crit Care Med1996;154:6—17.
[82] Rotondi AJ, Chelluri L, Sirio C, et al. Patients’ recollectionsof stressful experiences while receiving prolonged mecha-nical ventilation in an intensive care unit. Crit Care Med2002;30:746—52.
[83] Cooper AB, Thomsley KS, Young GB, Slutsky AS, Stewart TE,Hanly PJ. Sleep in critically ill patients requiring mechanicalventilation. Chest 2000;117:809—18.
[84] Parthasarathy S, Tobin MJ. Effect of ventilator mode on sleepquality in critically ill patients. Am J Respir Crit Care Med2002;166:1423—9.
[85] Gabor JY, Cooper AB, Crombach SA. Contribution of the inten-sive care unit environment to sleep disruption in mechanicallyventilated patients and healthy subjects. Am J Respir CritCare Med 2003;167:708—15.
[86] Misra S, Ganzini L. Delirium, depression, and anxiety. CritCare Clin 2003;19:771—87.
[87] Hoist JD, Banzett RB, Lohmeier HL, Hixon TJ, Brown R.Clinical ventilator adjustments that improve speech. Chest2003;124:1512—21.
[88] Holliday JE, Hyers TM. The reduction of weaning time frommechanical ventilation using tidal volume and relaxationfeedback. Am Rev Respir Dis 1990;141:1214—20.
[89] Annane D, Sebille V, Charpentier C, et al. Effect of treatmentwith low doses of hydrocortisone and fludro-cortisone on mor-tality in patients with septic shock. JAMA 2002;288:862—71.
[90] Van Den Berghe G, Wouters P, Weekers F, et al. Inten-sive insulin therapy in critically ill patients. N Engl J Med2001;345:1359—67.
[91] O’Brien Jr JM, Welsh CH, Fish RH, Ancukiewicz M, KramerAM, National Heart, Lung, and Blood Institute Acute Res-piratory Distress Syndrome Network. Excess body weight isnot independently associated with outcome in mechanicallyventilated patients with acute lung injury. Ann Intern Med2004;140:338—45.
[92] Tremblay A, Bandi V. Impact of body mass index on outcomesfollowing critical care. Chest 2003;123:1202—7.
[93] Doekel RC, Zwillic CW, Scoggin CH, Kryger M, Weil JV. Clinicalsemistarvation: depression of hypoxic ventilatory response. NEngl J Med 1976;295:358—61.
[94] Vassilakopoulos T, Petrof BF. Ventilator-induced diaphragma-tic dysfunction. Am J Respir Crit Care Med 2004;169:336—41.
[95] Sassoon CS, Caiozzo VJ, Manka A, Sieck GC. Altered diaphragmcontractile properties with controlled mechanical vential-tion. J Appl Physiol 2002;92:2585—95.
[96] Zergeroglu MA, McKenzie MJ, Shanely RA, Van Gamme-ren D, DeRuisseau KC, Powers SK. Mechanical ventilationinduced oxidative stress in the diaphragm. J Appl Physiol2003;95:1116—24.
9
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
4
[97] Nathens AB, Neff MJ, Jurkovich GJ, et al. Randomised, pros-pective trial of antioxidant supplementation in critically illsurgical patients. Ann Surg 2002;236:814—22.
[98] Heyland DK, Dhaliwal R, Suchner U, Berger MM. Antioxi-dant nutrients: a systematic review of trace elements andvitamins in the critically ill patient. Intensive Care Med2005;31:327—37.
[99] Hebert PC, Blajchman MA, Cook DJ, et al. Transfusion requi-rements in critical care investigators, Canadian critical caretrials group. Do blood transfusions improve outcomes relatedto mechanical ventilation? Chest 2001;119:1850—7.
100] Schonhofer B, Wenzel M, Geibel M, Kohler D. Blood trans-fusion and lung function in chronically anemic patients withsevere chronic obstructive pulmonary disease. Crit Care Med1998;26:1824—8.
101] Matic I, Majeric-Kogler V. Comparison of pressure supportand T-tube weaning from mechanical ventilation: randomizedprospective study. Croat Med J 2004;45:162—6.
102] Jones DP, Byrne P, Morgan C, Fraser I, Hyland R. Posi-tive end-expiratory pressure versus T-piece. Extubation aftermechanical ventilation. Chest 1991;100:1655—9.
103] Haberthur C, Mols G, Elsasser S, Bingisser R, Stocker R, Gutt-mann J. Extubation after breathing trials with automatic tubecompensation, T-tube, or pressure support ventilation. ActaAnaesthesiol Scand 2002;46:973—9.
104] Mehta S, Nelson DL, Klinger JR, Buczko GB, Levy MM. Pre-diction of postextubation work of breathing. Crit Care Med2000;28:1341—6.
105] Perren A, Domenighetti G, Mauri S, Genini F, Vizzardi N.Protocol-directed weaning from mechanical ventilation: clini-cal outcome in patients randomized for a 30-min or 120-mintrial with pressure support ventilation. Intensive Care Med2002;28:1058—63.
106] Reissmann HK, Ranieri VM, Goldberg P, Gottfried SB.Continuous positive airway pressure facilitates spontaneousbreathing in weaning chronic obstructive pulmonary diseasepatients by improving breathing pattern and gas exchange.Intensive Care Med 2000;26:1764—72.
107] Zeggwagh AA, Abouqal R, Madani N, Zekraoui A, Kerkeb O.Weaning from mechanical ventilation: a model for extuba-tion. Intensive Care Med 1999;25:1077—83.
108] Namen AM, Ely EW, Tatter SB, et al. Predictors of successfulextubation in neurosurgical patients. Am J Respir Crit CareMed 2001;163:658—64.
109] Koh WY, Lew TW, Chin NM, Wong MF. Tracheostomy in aneuro-intensive care setting: indications and timing. AnaesthIntensive Care 1997;25:365—8.
110] Khamiees M, Raju P, DeGirolamo A, Amoateng-Adjepong Y,Manthous CA. Predictors of extubation outcome in patientswho have successfully completed a spontaneous breathingtrial. Chest 2001;120:1262—670.
111] Bach JR, Saporito LR. Criteria for extubation and tra-cheostomy tube removal for patients with ventilatoryfailure. A different approach to weaning. Chest 1996;110:1566—71.
112] Fisher MM, Raper RF. The ‘‘cuff -leak’’ test for extubation.Anaesthesia 1992;47:10—2.
113] Sandhu RS, Pasquale MD, Miller K, Wasser TE. Measurement ofendotracheal tube cuff leak to predict postextubation stridorand need for reintubation. J Am Coll Surg 2000;190:682—7.
114] Jaber S, Chanques G, Matecki S, et al. Postextubation stri-dor in intensive care unit patients. Risk factors evaluationand importance of the cuff-leak test. Intensive Care Med
2003;29:69—74.115] DeBast Y, De Backer D, Moraine JJ, Lemaire M, VandenborghtC, Vincent JL. The cuff leak test to predict failure of tra-cheal extubation for laryngeal oedema. Intensive Care Med2002;28:1267—72.
J.-M. Boles et al.
[116] Laghi F, Cattapan SE, Jubran A, et al. Is weaning failure causedby low-frequency fatigue of the diaphragm? Am J Respir CritCare Med 2003;167:120—7.
[117] Esteban A, Anzueto A, Alia I, et al. How is mechanicalventilation employed in the intensive care unit? An inter-national utilization review. Am J Respir Crit Care Med2000;161:1450—8.
[118] Betbese AJ, Perez M, Bak E, Rialp G, Mancebo J. A prospectivestudy of unplanned endotracheal extubation in intensive careunit patients. Crit Care Med 1998;26:1180—6.
[119] Saura P, Blanch L, Mestre J, Valles J, Artigas A, FernandezR. Clinical consequences of the implementation of a weaningprotocol. Intensive Care Med 1996;22:1052—6.
[120] Horst HM, Mouro D, Hall-Jenssens RA, Pamukov N. Decreasein ventilation time with a standardized weaning process. ArchSurg 1998;133:483—8.
[121] Henneman E, Dracup K, Ganz T, Molayeme O, Cooper C. Effectof a collaborative weaning plan on patient outcome in thecritical care setting. Crit Care Med 2001;29:297—303.
[122] Smyrnios NA, Connolly A, Wilson MM, et al. Effects of amultifaceted, multidisciplinary, hospital-wide quality impro-vement program on weaning from mechanical ventilation.Crit Care Med 2002;30:1224—30.
[123] Scheinhorn DJ, Chao DC, Stearn-Hassenpflug M, Wallace WA.Outcomes in post-ICU mechanical ventilation: a therapist-implemented weaning protocol. Chest 2001;119:236—42.
[124] Marelich GP, Murin S, Battistella F, Inciardi J, Vierra T, RobyM. Protocol weaning of mechanical ventilation in medical andsurgical patients by respiratory care practitioners and nurses:effect on weaning time and incidence of ventilator-associatedpneumonia. Chest 2000;118:459—67.
[125] Grap MJ, Strickland D, Tormey L, et al. Collaborative practice:development, implementation, and evaluation of a weaningprotocol for patients receiving mechanical ventilation. Am JCrit Care 2003;12:454—60.
[126] Tonnelier JM, Prat G, Le Gal G, et al. Impact of a nurses’protocol-directed weaning procedure on outcomes in patientsundergoing mechanical ventilation for longer than 48 hours:a prospective cohort study with a matched historical controlgroup. Crit Care 2005;9:R83—9.
[127] Dries DJ, McGonigal MD, Malian MS, Bor BJ, Sullivan C.Protocol-driven ventilator weaning reduces use of mechanicalventilation, rate of early reintubation, and ventilator-associated pneumonia. J Trauma 2004;56:943—51.
[128] Randolph AG, Wypij D, Venkataraman ST, et al. Effect ofmechanical ventilator weaning protocols on respiratory out-comes in infants and children: a randomized controlled trial.JAMA 2002;288:2561—8.
[129] Krishnan JA, Moore D, Robeson C, Rand CS, Fessler HE. Aprospective, controlled trial of a protocol-based strategy todiscontinue mechanical ventilation. Am J Respir Crit Care Med2004;169:673—8.
[130] Berenholtz SM, Milanovich S, Faircloth A, et al. Impro-ving care for the ventilated patient. Jt Comm J Qual Saf2004;30:195—204.
[131] Girault C, Daudenthun I, Chevron V, Tamion F, Leroy J,Bonmarchand G. Noninvasive ventilation as a systematic extu-bation and weaning technique in acute-on-chronic respiratoryfailure. A prospective, randomized controlled study. Am JRespir Crit Care Med 1999;160:86—92.
[132] Chen J, Qiu D, Tao D. Time for extubation and sequentialnoninvasive mechanical ventilation in COPD patients withexacerbated respiratory failure who receive invasive venti-
lation. Zhonghua Jie He He Hu Xi Za Zhi 2001;24:99—100.[133] Bohner H, Kindgen-Milles D, Grust A, et al. Prophylactic nasalcontinuous positive airway pressure after major vascular sur-gery: results of a prospective randomized trial. LangenbecksArch Surg 2002;387:21—6.
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
Weaning from mechanical ventilation
[134] Squadrone V, Coha M, Cerutti E, et al. Piedmont intensivecare units network (PICUN). Continuous positive airway pres-sure for treatment of postoperative hypoxemia: a randomizedcontrolled trial. JAMA 2005;293:589—95.
[135] Kilger E, Briegel J, Haller M, et al. Effects of noninvasivepositive pressure ventilatory support in non-COPD patientswith acute respiratory insufficiency after early extubation.Intensive Care Med 1999;25:1374—80.
[136] Antonelli M, Conti G, Bufi M, et al. Noninvasive ventilationfor treatment of acute respiratory failure in patients under-going solid organ transplantation: a randomized trial. JAMA2000;283:235—41.
[137] Keenan SP, Powers C, McCormack DG, Block G. Noninva-sive positive-pressure ventilation for postextubation res-piratory distress: a randomized controlled trial. JAMA2002;287:3238—44.
[138] Esteban A, Frutos-Vivar F, Ferguson ND, et al. Noninva-sive positive-pressure ventilation for respiratory failure afterextubation. N Engl J Med 2004;350:2452—60.
[139] Jardin F, Farcot JC, Boisante L, et al. Influence of positiveend-expiratory pressure on left ventricular performance. NEngl J Med 1981;304:387—92.
[140] Petrof BJ, Legare M, Goldberg P, Milic-Emili J, GottfriedSB. Continuous positive airway pressure reduces work ofbreathing and dyspnoea during weaning from mechanical ven-tilation in severe chronic obstructive pulmonary disease. AmRev Respir Dis 1990;141:281—9.
[141] Feeley TW, Saumarez R, Klick JM, McNabb TG, Skillman JJ.Positive end-expiratory pressure in weaning patients fromcontrolled ventilation. A prospective randomised trial. Lancet1975;2:725—9.
[142] Bailey CR, Jones RM, Kelleher AA. The role of continuouspositive airway pressure during weaning from mechani-cal ventilation in cardiac surgical patients. Anaesthesia1995;50:677—81.
[143] Appendini L, Purro A, Gudjonsdottir M, et al. Responseof ventilator-dependent patients with chronic obstructivepulmonary disease to proportional assist ventilation andcontinuous positive airway pressure. Am J Respir Crit CareMed 1999;159:1510—7.
[144] Gay PC, Hess DR, Hill NS. Noninvasive proportional assistventilation for acute respiratory insufficiency. Comparisonwith pressure support ventilation. Am J Respir Crit Care Med2001;164:1606—11.
[145] Delaere S, Roeseler J, D’hoore W, et al. Respiratory muscleworkload in intubated, spontaneously breathing patientswithout COPD: pressure support versus proportional assistventilation. Intensive Care Med 2003;29:949—54.
[146] Tassaux D, Dalmas E, Gratadour P, Jolliet P. Patient-ventilatorinteractions during partial ventilatory support: a preliminarystudy comparing the effects of adaptive support ventila-tion with synchronized intermittent mandatory ventilationplus inspiratory pressure support. Crit Care Med 2002;30:801—7.
[147] Lourens MS, van den Berg B, Aerts JG, Verbraak AF,Hoogsteden HC, Bogaard JM. Expiratory time constants inmechanically ventilated patients with and without COPD.Intensive Care Med 2000;26:1612—8.
[148] Cassina T, Chiolero R, Mauri R, Revelly JP. Clinical experiencewith adaptive support ventilation for fast-track cardiac sur-gery. J Cardiothorac Vasc Anesth 2003;17:571—5.
[149] Petter AH, Chiolero RL, Cassina T, Chassot PG, Muller XM,Revelly JP. Automatic ‘‘respirator/weaning’’ with adaptive
support ventilation: the effect on duration of endotra-cheal intubation and patient management. Anesth Analg2003;97:1743—50.[150] Sulzer CF, Chiolero R, Chassot PG, Mueller XM, Revelly JP.Adaptive support ventilation for fast tracheal extubation
[
95
after cardiac surgery: a randomized controlled study. Anes-thesiology 2001;95:1339—45.
151] Dojat M, Brochard L, Lemaire F, Harf A. A knowledge basedsystem for assisted ventilation of patients in intensive careunits. Int J Clin Monit Comput 1992;9:239—50.
152] Dojat M, Harf A, Touchard D, Laforest M, Lemaire F, BrochardL. Evaluation of a knowledge-based system providing venti-latory management and decision for extubation. Am J RespirCrit Care Med 1996;153:997—1004.
153] Dojat M, Harf A, Touchard D, Lemaire F, Brochard L. Clinicalevaluation of a computer-controlled pressure support mode.Am J Respir Crit Care Med 2000;161:1161—6.
154] Cohen IL, Booth FV. Cost containment and mechanical venti-lation in the United States. New Horiz 1994;2:283—90.
155] Seneff MG, Zimmerman JE, Knaus WA, Wagner DP, DraperEA. Predicting the duration of mechanical ventilation. Theimportance of disease and patient characteristics. Chest1996;110:469—79.
156] Kurek CJ, Cohen IL, Lambrinos J, Minatoya K, Booth FV, ChalfinDB. Clinical and economic outcome of patients undergoingtracheostomy for prolonged mechanical ventilation in NewYork state during 1993: analysis of 6353 cases under diagnosis-related group 483. Crit Care Med 1997;25:983—8.
157] Pilcher DV, Bailey MJ, Treacher DF, Hamid S, Williams AJ,Davidson AC. Outcomes, cost and long-term survival ofpatients referred to a regional weaning centre. Thorax2005;60:187—90.
158] Cox CE, Carson SS, Holmes GM, Howard ABS, Carey TS.Increase in tracheostomy for prolonged mechanical ven-tilation in North Carolina, 1993—2002. Crit Care Med2004;32:2219—26.
159] Simpson TP, Day CJ, Jewkes CF, Manara AR. The impact ofpercutaneous tracheostomy on intensive care unit practiceand training. Anaesthesia 1999;54:186.
160] Stauffer JL, Olson DE, Petty TL. Complications and conse-quences of endotracheal intubation and tracheotomy. Aprospective study of 150 critically ill adult patients. Am JMed 1981;70:65—76.
161] Kress JP, Gehlbach B, Lacy M, Pliskin N, Pohlman AS, Hall JB.The long-term psychological effects of daily sedative inter-ruption on critically ill patients. Am J Respir Crit Care Med2003;168:1457—61.
162] Astrachan DI, Kirchner JC, Goodwin Jr WJ. Prolongedintubation versus tracheotomy: complications, practicaland psychological considerations. Laryngoscope 1988;98:1165—9.
163] L’Her E, Lellouche F, Ferrand E, Prat G, Brochard L. Is tra-cheostomy less comfortable than translaryngeal intubation?Am J Respir Crit Care Med 2003;167:A302.
164] Diehl J-L, El Atrous S, Touchard D, Lemaire F, Brochard L.Changes in the work of breathing induced by tracheotomyin ventilator-dependent patients. Am J Respir Crit Care Med1999;159:383—8.
165] Davis Jr K, Campbell RS, Johannigman JA, Valente JF, Bran-son RD. Changes in respiratory mechanics after tracheostomy.Arch Surg 1999;134:59—62.
166] Dunham CM, LaMonica C. Prolonged tracheal intubation in thetrauma patient. J Trauma 1984;24:120—4.
167] Rodriguez JL, Steinberg SM, Luchetti FA, Gibbons KJ,Taheri PA, Flint LM. Early tracheostomy for primary airwaymanagement in the surgical critical care setting. Surgery1990;108:655—9.
168] Sugerman HJ, Wolfe L, Pasquale MD, et al. Multicenter, ran-
domized, prospective trial of early tracheostomy. J Trauma1997;43:741—7.169] Rumbak MJ, Newton M, Truncale T, Schwartz SW, Adams JW,Hazard PB. A prospective, randomized, study comparing earlypercutaneous dilational tracheotomy to prolonged translaryn-
9
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
6
geal intubation (delayed tracheotomy) in critically ill medicalpatients. Crit Care Med 2004;32:1689—1694. Erratum in CritCare Med 2004;32:2566.
170] Jacobs S, Al Rasheed AM, Abdulsamat W, et al. Effects of asimple protocol on infective complications in intensive careunit patients undergoing percutaneous dilatational tracheo-stomy. Respir Care 2003;48:29—37.
171] Rello J, Lorente C, Diaz E, et al. Incidence, etiology, andoutcome of nosocomial pneumonia in ICU patients requiringpercutaneous tracheotomy for mechanical ventilation. Chest2003;124:2239—43.
172] Bouderka MA, Fakhir B, Bouaggad A, Hmamouchi B, HamoudiD, Harti A. Early tracheostomy versus prolonged endotrachealintubation in severe head injury. J Trauma 2004;57:251—4.
173] Saffle JR, Morris SE, Edelman L. Early tracheostomy doesnot improve outcome in burns patients. J Burn Care Rehabil2002;23:431—8.
174] Teoh WH, Goh KY, Chan C. The role of early tracheostomy incritically ill neurosurgical patients. Ann Acad Med Singapore2001;30:234—8.
175] Brook AD, Sherman G, Malen J, Kollef MH. Early versus latetracheostomy in patients who require mechanical ventilation.Am J Crit Care 2000;9:352—9.
176] Maziak DE, Meade MO, Todd TR. The timing of tracheotomy:a systematic review. Chest 1998;114:605—9.
177] Armstrong PA, McCarthy MC, Peoples JB. Reduced use ofresources by early tracheostomy in ventilator-dependentpatients with blunt trauma. Surgery 1998;124:763—6.
178] Blot F, Guiguet M, Antoun S, Leclercq B, Nitenberg G, EscudierB. Early tracheotomy in neutropenic, mechanically ventilatedpatients: rationale and results of a pilot study. Support CareCancer 1995;3:291—6.
179] D’Amelio LF, Hammond JS, Spain DA, Sutyak JP. Tracheo-stomy and percutaneous endoscopic gastrostomy in themanagement of the head-injured trauma patient. Am Surg1994;60:180—5.
180] Lesnik I, Rappaport W, Fulginiti J, Witzke D. The role ofearly tracheostomy in blunt, multiple organ trauma. Am Surg1992;58:346—9.
181] El-Naggar M, Sadagopan S, Levine H, Kantor H, Collins VJ.Factors influencing choice between tracheostomy and pro-longed translaryngeal intubation in acute respiratory failure:a prospective study. Anesth Analg 1976;55:195—201.
182] Heffner JE, Zamora CA. Clinical predictors of prolonged trans-laryngeal intubation in patients with the adult respiratorydistress syndrome. Chest 1990;97:447—52.
183] Troche G, Moine P. Is the duration of mechanical ventilationpredictable? Chest 1997;112:745—51.
184] Sellers BJ, Davis BL, Larkin PW, Morris SE, Saffle JR. Earlyprediction of prolonged ventilator dependence in thermallyinjured patients. J Trauma 1997;43:899—903.
185] Kollef MH, Ahrens TS, Shannon W. Clinical predictors and out-comes for patients requiring tracheostomy in the intensivecare unit. Crit Care Med 1999;27:1714—20.
186] Engoren M, Arslaninan-Engoren C, Fenn-Buderer N. Hospitaland long-term outcome after tracheostomy for respiratoryfailure. Chest 2004;125:220—7.
187] LoCicero J, McCann B, Massad M, Joob AW. Prolonged ven-tilatory support after open-heart surgery. Crit Care Med1992;20:990—2.
188] Frutos-Vivar F, Esteban A, Apezteguia C, et al. Outcome ofmechanically ventilated patients who require a tracheostomy.Crit Care Med 2005;33:290—8.
189] Freeman BD, Isabella K, Lin N, Buchman TG. A meta-analysisof prospective trials comparing percutaneous and surgical tra-cheostomy in critically ill patients. Chest 2000;118:1412—8.
190] Freeman BD, Isabella K, Cobb JP, et al. A prospective,randomized study comparing percutaneous with surgical
J.-M. Boles et al.
tracheostomy in critically ill patients. Crit Care Med2001;29:926—30.
[191] Nelson JE, Meier DE, Litke A, Natale DA, Siegel RE, MorrisonRS. The symptom burden of chronic critical illness. Crit CareMed 2004;32:1527—34.
[192] Azoulay E, Pochard F, Kentish-Barnes N, et al. Risk ofpost-traumatic stress symptoms in family members ofintensive care unit patients. Am J Respir Crit Care Med2005;171:987—94.
[193] Jones C, Skirrow P, Griffiths RD, et al. Rehabilitation aftercritical illness: a randomized, controlled trial. Crit Care Med2003;31:2456—61.
[194] Rudy EB, Daly BJ, Douglas S, Montenegro HD, Song R, Dyer MA.Patient outcome for the chronically critically ill: special careunit versus intensive care unit. Nurs Res 1995;44:324—31.
[195] Seneff MG, Wagner D, Thompson D, Honeycutt C, Silver MR.The impact of long-term acute-care facilities on the outcomeand cost of care for patients undergoing prolonged mechani-cal ventilation. Crit Care Med 2000;28:342—50.
[196] Elpern EH, Larson R, Douglass P, et al. Long-term outcomesfor elderly survivors of prolonged ventilator assistance. Chest1989;96:1120—4.
[197] Robson V, Poynter J, Lawler PG, et al. The need for a regionalweaning centre, a one-year survey of intensive care wea-ning delay in the Northern region of England. Anaesthesia2003;58:161—5.
[198] Gracey DR, Hardy D, Naessens JM, Silverstein MD, HubmayrRD. The mayo ventilator-dependent rehabilitation unit: a 5-year experience. Mayo Clin Proc 1997;72:13—9.
[199] Carson SS, Bach PB, Brzozowski L, et al. Outcomes after long-term acute care. An analysis of 133 mechanically ventilatedpatients. Am J Respir Crit Care Med 1999;159:1568—73.
[200] De Vivo MJ, Ivie CS. Life expectancy of ventilator dependentpersons with spinal cord injuries. Chest 1995;108:226—32.
[201] Schönhofer B, Euteneuer S, Nava S, Suchi S, Kohler D. Survivalof mechanically ventilated patients admitted to a specialisedweaning centre. Intensive Care Med 2002;28:908—16.
[202] Bagley PH, Cooney E. A community-based regional ventilatorweaning unit. Chest 1997;111:1024—9.
[203] Gracey DR, Hardy DC, Koenig GE. The chronic ventilator-dependent unit: a lower-cost alternative to intensive unitcare. Mayo Clin Proc 2000;75:445—9.
[204] Douglas SL, Daly BJ, Gordon N, Brennan PF. Survival and qua-lity of life: short-term versus long-term ventilator patients.Crit Care Med 2002;30:2655—62.
[205] Medicare payment advisory cCommission. Defining long-termcare hospitals. Chapter 5; June 2004 report. www.med-pac.gov/publications. Date last accessed November 2004.
[206] Latriano B, McCauley P, Astiz ME, Greenbaum D, Rackow EC.Non-ICU care of hemodynamically stable mechanically venti-lated patients. Chest 1996;109:1591—6.
[207] Scheinhorn DJ, Chao DC, Stearn-Hassenpflug M, LaBreeLD, Heltsley DJ. Post-ICU mechanical ventilation: treat-ment of 1123 patients at a regional weaning center. Chest1997;111:1654—9.
[208] Dasgupta A, Rice R, Mascha E, et al. Four-year experience witha unit for long-term ventilation (respiratory special care unit)at the Cleveland clinic foundation. Chest 1999;116:447—55.
[209] Gracey DR, Viggiano RW, Naessens JM, Hubmayr RD, Silver-stein MD, Koenig GE. Outcomes of patients admitted to achronic ventilator-dependent unit in an acute-care hospital.Mayo Clin Proc 1992;67:131—6.
[210] Chatila W, Kreimer DT, Criner GJ. Quality of life in survivors
of prolonged mechanical ventilatory support. Crit Care Med2001;29:737—42.[211] Ambrosino N, Bruletti G, Scala V, Porta R, Vitacca M. Cog-nitive and perceived health status in patient with chronicobstructive pulmonary disease surviving acute on chronic
[
[
[
[
[
[
[
Weaning from mechanical ventilation
respiratory failure: a controlled study. Intensive Care Med2002;28:170—7.
[212] Chelluri L, Im MPH, Kyung AMS, Belle SH. Long-term mortalityand quality of life after prolonged mechanical ventilation.Crit Care Med 2004;32:61—9.
[213] Pehrsson K, Olofson J, Larsson S, Sullivan M. Quality of lifeof patients treated by home mechanical ventilation due torestrictive ventilatory disorders. Respir Med 1994;88:21—6.
[214] Janssens JP, Penalosa B, Degive C, Rabeus M, Rochat T. Qua-lity of life of patients under home mechanical ventilation forrestrictive lung diseases: a comparative evaluation with COPDpatients. Monaldi Arch Chest Dis 1996;51:178—84.
[215] Markstrom A, Sundell K, Lysdahl M, Andersson G, Sche-din U, Klang B. Quality-of-life evaluation of patients withneuromuscular and skeletal diseases treated with nonin-vasive and invasive home mechanical ventilation. Chest2002;122:1695—700.
[216] Windisch W, Freidel K, Schucher B, et al. Evaluation ofhealth-related quality of life using the MOS 36-Item Short-Form Health Status Survey in patients receiving noninvasivepositive pressure ventilation. Intensive Care Med 2003;29:615—21.
[217] Windisch W, Freidel K, Schucher B, et al. The severe respi-ratory insufficiency (SRI) questionnaire: a specific measureof health-related quality of life in patients receiving homemechanical ventilation. J Clin Epidemiol 2003;56:752—9.
[218] Murphy DJ, Burrows D, Santilli S, et al. The influence of theprobability of survival on patients’ preferences regarding car-diopulmonary resuscitation. N Engl J Med 1994;330:545—9.
[219] Curtis JR, Bennett CL, Horner RD, Rubenfeld GD, DeHo-vitz JA, Weinstein RA. Variations in intensive care unit
[
97
utilization for patients with human immunodeficiency virus-related Pneumocystis carinii pneumonia: importance ofhospital characteristics and geographic location. Crit CareMed 1998;26:668—75.
220] Sprung CL, Cohen SL, Sjokvist P. End-of-life practices inEuropean intensive care units: the ethicus study. JAMA2003;290:790—7.
221] Azoulay E, Chevret S, Leleu G, et al. Half the families of inten-sive care unit patients experience inadequate communicationwith physicians. Crit Care Med 2000;28:3044—9.
222] Prendergast TJ, Luce JM. Increasing incidence of with holdingand withdrawal of life support from the critically ill. Am JRespir Crit Care Med 1997;155:15—20.
223] Dowdy MD, Robertson C, Bander JA. A study of proactiveethics consultation for critically and terminally ill patientswith extended lengths of stay. Crit Care Med 1998;26:252—9.
224] Campbell SG, Marrie TJ, Anstey R, Dickinson G, Ackroyd-Stolarz S. The contribution of blood cultures to the clinicalmanagement of adult patients admitted to the hospital withcommunity-acquired pneumonia: a prospective observationalstudy. Chest 2003;123:1142—50.
225] Schneiderman LJ, Gilmer T, Teetzel HD, et al. Effect of ethicsconsultations on nonbeneficial life-sustaining treatments inthe intensive care setting: a randomized controlled trial.JAMA 2003;290:1166—72.
226] Crawley LM, Marshall PA, Lo B, Koenig BA. End-of-life care
consensus panel. Strategies for culturally effective end-of-life care. Ann Intern Med 2002;136:673—9.227] Treece PD, Engelberg RA, Crowley L, et al. Evaluation of astandardized order form for the withdrawal of life support inthe intensive care unit. Crit Care Med 2004;32:1141—8.