Embed Size (px)
Citation preview

248
CLINICO-PATHOLOGICAL CONFERENCE-No. 22
The borderline of lupus erythematosus disseminatus
Clinical History (Dr. M. D. Milne)The patient was a native of Nigeria, who
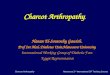
arrived in this country in good health in 1939.In i944 he developed a right basal pneumoniacomplicated by a pleural effusion, and was treatedwith sulphonamides. Soon afterwards he had aprofuse epistaxis requiring treatment by cauteriza-tion, and also severe haematuria. He was foundto have thrombocytopenia and a splenectomy wasperformed. Section of the spleen showed non-specific changes with hyperplasia of the Malphigiancorpuscles and proliferation of reticulum cells(Fig. I).
In 1945, he had pneumonia of the right upperzone and there were further attacks of pneumoniain 1946, I947 and 1948. In 1950, he was firstseen at the Hammersmith Hospital as an out-patient. He had had symptoms suggestive of apyrexia for the previous three weeks, the illnesshaving commenced with a rigor. There had beenconsiderable cough and sputum, but on examina-tion no abnormal physical signs were found.There was no albuminuria and no lymphadeno-pathy, and X-ray of the chest was normal.
In 195i he developed a pyrexia up to I050,followed by a right pleural effusion. He com-plained of joint pains, which were 'fleeting' incharacter, clinically similar to those of acuterheumatic fever. Pleural tap gave a clear straw-coloured fluid, sterile on culture and containinglymphocytes. He developed enlarged glands inthe axillae and posterior triangles of the neck.A biopsy showed non-specific changes with folli-cular and sinus hyperplasia. A white cell countof 3900/cu. mm. was recorded. There was noalbuminuria.
In February I952 he was first admitted toHammersmith Hospital complaining of generalizedaches and pains of six weeks' duration and painful
Held at the Postgraduate Medical School (Hammer-smith Hospital) on November I8, I953. The reportwas assembled by Dr. Bernard Lennox. The sectionswere prepared under the direction of Mr. J. Griffinand the photomicrographs taken by Mr. C. A. P.Graham,
: r·- ~-:~gq~?'~... ~"~~'¥.,'; :~.-' ,
ii
ac'i _WE. ... . ~
9 -" '
Al #:
,~*** *· ~ ..~:.
j·.~.,~, ~.. ~ . ,,.-.
FIG. I.--A section of the spleen removed in I944. Thearteriole in this Malpighian body shows no traceof concentric fibrosis. The pale halo round thegerm centre, described (Leffler, 1952) as charac-teristic of' hypersplenism' is seen indistinctly; itwas not a very marked feature in this case.H. & E. x 75.
swellings of the right foot and left knee for fivedays.On examination, he was found to be pyrexial.
There was a generalized arthropathy, but the leftknee and right ankle were the most severelyaffected joints. These two joints were very hot,red, swollen and tender. There was a generalizedlymphadenopathy, the glands being discrete, firmand not tender. There was an albuminuriaamounting to 2 g. per litre. The erythrocytesedimentation rate varied from 37 to 85 mm. perhour. Chest X-ray showed small basal effusions.X-ray of the joints was normal. The white cellcount was Io,ooo/cu. mm., 95 per cent. beingpolymorphonuclear leucocytes. Repeated bloodcultures proved to be sterile. Serum albuminwas 2.1 g./Ioo ml. and serum globulin 5.6 g./Ioo ml. On aspiration of the left knee, io ml. ofa very viscous fluid containing 5600 cells/cu. mm.was obtained. The joint pains responded well tosalicylate therapy. A clinical diagnosis of sub-
by copyright. on D
ecember 20, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.343.248 on 1 May 1954. D
ownloaded from

May 1954 Clinico-Pathological Conference 251
acute disseminated lupus erythematosus was made.Lupus erythematosus cells were not demonstratedin the blood and a synovial biopsy of the left kneewas not contributory.
In March 1953 he was admitted to anotherhospital, complaining of pain in the chest, togetherwith cough and haemoptysis. There were signsof pneumonia at the right lung base. There wasa white cell count of 26,ooo/cu. mm. of which78 per cent. were polymorphonuclear leucocytes.There was considerable albuminuria, with granularcasts and red blood cells present. X-ray of thechest showed consolidation of the whole of theright upper lobe with a small right pleural effusion.A rash followed initial penicillin therapy, afterwhich he was successfully treated with chloro-mycetin.
In May 1953 he was admitted for the secondand last time to Hammersmith Hospital. He wasthen an extremely apathetic and chronically illman without any specific complaints. Themucous membranes were pale. The heart wasnormal and the blood pressure I40/90. Therewas diminution of breath sounds and dullness topercussion at both lung bases. Rubbery, discretelymph glands were felt in both axillae. Theliver was just palpable; no abnormality was foundin the central nervous system. The haemoglobinwas I2.2 g./ico ml. and the white cell count was7000/cu. mm. The blood urea was Ioo mg./Ioo ml.and the plasma proteins 7.5 g./Ioo ml. withreduction of the albumin and increase of they-globulin fraction. Lupus erythematosus cellswere now demonstrated in the peripheral blood.Sternal marrow was reported as showing earlymegaloblastic changes. X-ray of the chest showedthickening of the pleura in the right costo-phrenicangle with mottling of the right upper zone.Serum electrolytes were: sodium I30 meq./L.,potassium 7.4 meq./L., chloride Io07 meq./L.,bicarbonate 8 meq./L., inorganic phosphorusI2.5 mg./Ioo ml., calcium 6.9 mg./ioo ml. Theblood urea slowly rose to 332 mg./Ioo ml., thepatient developed oedema of the face and died ina state of coma with occasional uraemic convulsions.Final Diagnosis:
Disseminated lupus erythematosus withoutskin rash.
Terminal ureamia. Evidence that the diseasehad involved the lungs and pleura, thejoints, the lymph glands, spleen andhaemopoietic tissue.
The accepted clinical features of disseminatedlupus ervythematosus are:
(a) Erythematous skin lesions.*(b) Constitutional symptoms of cachexia, fever
and weight loss.*(c) Arthralgia and arthritis.
*(d) Leucopenia, secondary anaemia and throm-bocytopenia.
*(e) Lymphadenopathy.(f) Abacterial endocarditis (Libman- Sacks
syndrome).*(g) Polyserositis with pleurisy, pericarditis and
occasionally ascites.*(h) Renal disease.*(i) Hyperglobulinaemia and presence of lupus
erythematosus cells.This patient showed seven out of nine of these
(starred in the list), and since any one patientcannot be expected to show Ioo per cent. of themanifestations of this protean disease, a confidentclinical diagnosis of the condition could be made.
Pathology (Professor J. H. Dible)Sections from the spleen which had been
removed nine years previously failed to show thecharacteristic lesion of generalized lupus erythe-matosus.At post-mortem there were old adhesions
involving both pleural spaces and pericardium.The left lung was oedematous and congested. Theright lung shows, in addition, visible fibrous bandsin the parenchyma of the middle and lower lobes.The liver showed no noteworthy changes, exceptfor some increased cellular infiltration of theportal tracts and siderosis of the Kupffer cells.The peritoneal cavity contained about 200 cc. ofclear fluid.The kidneys weighed 275 gm. each, and pre-
sented the appearance of 'large white kidneys'with some petechiae of the sub-capsular surface.There was generalized enlargement of the lymphglands which were discrete, white, rubbery andlacking. in follicular pattern. The colon wasmoderately oedematous with a good deal ofadherent mucus. The vertebral and sternalmarrow-were rather brownish and the- upper thirdof the left femur contained brownish-red marrow.The left knee and hip joints were examined andshowed no abnormalities.On microscopical examination the evidence for
lupus erythematosus was minimal, but consideredsignificant. The lack of characteristic changes inthe spleen, it was thought, might coincide withthe early stage at which this organ was removed.The histological lesion in the kidneys was that ofa glomerulo-nephritis (Figs. 2 and 3), withcrescent formation, capsule lobulation, tuft adhe-sions, capsular thickening, and eventual glome-rular hyalinization (Fig. 4). The large size of thekidneys was mainly due to an extreme distensionof the tubules with dense colloid-like proteinmaterial, in the absence of which there wouldhave been considerable reduction in the size ofthese organs (Fig. 5). No characteristic glome-
D
by copyright. on D
ecember 20, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.343.248 on 1 May 1954. D
ownloaded from

252 POSTGRADUATE MEDICAL JOURNAL May 1954
'':' 4' '
~··::4
FIG. 2.-Glomerulo-nephritis : a relatively acute lesionwith early capsular proliferation. H. & E. x I6o.
1ov
FIG. 3.-Glomerulo-nephritis : a later stage, with muchperiglandular fibrosis. H. & E. x i6o.
......'4... ...''"]~~:*e': ....i~;:~~ ::;..,.;~- ~,z, :. ..
.../·..~f,~¥.~:~r'~ ~"~ i~lq~_..~
FIG. 4.-Glomerulo-nephritis: two late stages, one withcomplete hyalinization. The surrounding paren-chyma shows gross tubular atrophy and moderatecellular infiltration. H. & E. x I6o.
·:'
p. P
I·
FIG. 5.-A more general view of the renal cortex, show-ing the striking tubular dilatation and cast forma-tion. Note the scarcity of recognizable glomeruli.H. & E. x 55.
.i."?*l-.f*b.·.:*CYt`..a. -I~"31 ·E. .3.
I
.,··. .t.g.. .sli.~ 1 ..rr. .d.hTo,.r fr .CiEiC.·i;i:· ;·: Rlilr. jf.ll
·t'
Fl)i* **'.J.'.II· ··.·."
a.l ·tir..*Ii
. ..
iJI··.".t're, .a.i.4L. .;Z r
.".a.41·lcl.".3."...t.;aca.c.a.-1..FIG. 6.-Lymph node, showing both an " exhausted "
germinal centre, and a nodule formed by perica-pillary fibrosis which except for its small sizemimics very exactly the better-known splenicvascular lesions of L.E.D. H. & E. x I6o.
ruler lesions of lupus erythematosus were dis-cerned. The renal lesions found were typicallynephritic and it was not possible to relate them toan earlier lupus lesion.The condition of a lymph gland removed two
years earlier was contrasted with that found atpost-mortem. The first showed normal corticalgerm centres and supporting tissue, the lattershowed a striking condition of exhaustion of thegerm centres with disappearance of the specificcells and their replacement by granular eosino-philic tissue with numbers of histiocytes (Fig. 6).In addition, the vessels of the glands showed a
by copyright. on D
ecember 20, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.343.248 on 1 May 1954. D
ownloaded from

May I954 Clinico-Pathological Conference 253
periarterial fibrosis very like that seen in thespleen in generalized lupus erythematosus, whichtended to spread through the framework of thegland, involving the vessels in a thick layer ofloose collagenous tissue.The lungs showed evidence of old inflammatory
changes with bands of thick fibrous tissue, emphy-sema and organized pneumonia, with the develop-ment of intra-alveolar fibrous masses.The pericardium showed a layer of old fibrosis,
in which was incorporated a good deal of haemo-siderin, which it was thought represented ahaemorrhagic lesion at the time of the originalpurpuric manifestations. Deeper to this was alayer of recent fibrosis, with young blood vesselsand lymphocytic infiltration. There was in theolder fibrous tissue a single area of fibrin exudation.The colon showed complete denudation of the
mucus membrance, the lumen being lined withinactive-looking, thickened, sub-mucous fibroustissue. The lineal extent of this lesion was notdetermined. The bone marrow showed a mixtureof activity and exhaustion, there being many areasdevoid of haemopoietic cells.
SummaryDeath from uraemia with lesions of sub-acute
glomerulo-nephritis.Some evidence of chronic generalized lupus
erythematosus.Discussion
Dr. Milne: I think that one lesson that thiscase teaches is the great value of collaborationbetween clinicians and pathologists. If this casehad merely been reported as showing death fromuraemia, I think it might have been quite on thecards that many pathologists would have reportedthat kidney as a chronic pyelonephritis. Thatappearance of colloidal casts looking like thyroidtissue is usually attributed to pyelonephritis, butcareful search showed typical features whichfavour the clinical story of disseminated lupuserythematosus. Now this man died of renalfailure and I would just like to say a few words onthe renal side of lupus erythematosus, beforeother physicians discuss their own particularinterests.
I have been impressed by the great diversity ofthe clinical picture of the renal lesion of lupuserythematosus and I am beginning to be equallyimpressed by the great diversity of the pathologicalpicture in the kidneys in this disease. The usualstory in the literature is that this is one of the causesof the nephrotic syndrome. It is one of thediagnoses you think of if you have a patient withgross oedema, gross albuminuria, anasarca andhypercholesterolaemia, with low serum albumen
and maybe high globulin. It is true that that isthe most common clinical manifestation of therenal lesion of lupus erythematosus, but I haveseen a case in which it presented almost indistin-guishably from acute Type I glomerulo-nephritis,with hypertension, haematuria and oedema. Thediagnosis was given away in that case by the factthat the patient had at about the same time apericardial friction rub and pleural effusions, andfive days later he developed a florid disseminatedrash typical of the disease. The case you havejust been shown had another type of renal lesion.This man never had nephrotic symptoms, henever had an acute glomerulo-nephritis, he merelyshowed a picture of moderately rapid progressiverenal failure. We know that the renal damagestarted in 1952, as shown by his albuminuria,but it had not gone far then-there was noisosthenuria, there was no nitrogen retention. Ayear later the glomeruli had been almost destroyed,as was shown clinically by the very high bloodurea and reduction of glomerular filtration rate,and shown much more clearly by Professor Dible'smicroscope; this was then the picture of terminalrenal failure. So this gives three examples of theways in which the clinical side of lupus erythema-tosus can differ.You can only diagnose this disease by being a
general physician, looking everywhere, seeking apeculiar combination of symptoms and signs,cleaving across all specialities. This applies tothe clinical manifestations of all the diseaseswhich we frankly do not understand, but whichwe speak of as belonging to the group of thecollagenoses.
Dr. Bywaters: There are one or two points Iwanted to raise. Despite a great deal of endeavourit doesn't seem to me that everyone is entirelycertain about the diagnosis of lupus erythema-tosus in this case. We don't know how long therehad been uraemia, except perhaps that in 1951there was no albuminuria or fixation of specificgravity. Could it possibly be that the originalepisode following after sulphonamides might havebeen an episode of nitrogen retention or pyelone-phritis ? Admittedly, the kidneys are not con-tracted, but this is, I think, the only such kidneyI have ever seen in a case reputed to have beenone of lupus erythematosus. I think the largenumber of colloid casts are most unusual and Idon't think, from what Professor Dible showedgrossly, that we could match it with other recordedcases (and there have been quite a number ofcases now recorded). The other point I wantedto emphasize was how extraordinarily useful wehave found these serological abnormalities indiagnosis. The lupus cell factor of the serumpoes sometimes appear in other conditions. It has
by copyright. on D
ecember 20, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.343.248 on 1 May 1954. D
ownloaded from

254 POSTGRADUATE MEDICAL JOURNAL May 1954
been recorded in penicillin sensitivity. I noticethat this chap had a penicillin rash sometimes.We have occasionally found a very few L.E. cellsin patients with rheumatoid arthritis without otherevidence of L.E., and in this patient one cell wasfound on only one occasion-I think one couldhave hoped for a little more than that. Otherquite useful reactions include a false positiveW.R., a Coombs' test, and finally (one thing wehave found very useful indeed) the differentialagglutination for sheep's cells, which is positivein about 6o per cent. of rheumatoids, but in aboutIoo per cent. of recent cases of lupus, a muchhigher positivity than the L.E. cell factor. It isvery simple to do and it is being done regularlyhere. Is there any information on this point inthis patient ?
Dr. Dacie: It was negative.Dr. Bywaters: Again, I think that is a point
against this diagnosis. I admit that when wefirst saw the patient I thought that on clinicalgrounds there was a fair-reason for suspecting thediagnosis of L.E. and it is still difficult to getaway from it. There is very little else one canthink of that would account for the long coursestarting with purpura, followed by severe albu-minuria, arthritis, serositis, and so on. But the-proof is not perhaps as complete as it might be.
Professor Dible: May I say that my attitude tothe kidney lesions was that I thought they were,from my point of view, a nephritis, but that thatdoesn't exclude the possibility that the causativetactor of lupus erythematosus, whatever it may be,might have had something to do with the presenceof nephritis.
Dr. Lennox: I think it is worth rememberinga case that Professor Dible showed us which hadboth wire loop lesions and quite definite nephriticlesions together in the kidney. That was in otherrespects an extremely typical case-lesions in thespleen and a highly typical skin eruption, on whichthe diagnosis was made in the first place.
Dr. Bywaters: I was not quite clear whetherProfessor Dible thought this was a chronicglomerulo-nephritis; it seemed to me a littleatypical. Admittedly ordinary chronic or evenacute glomerulo-nephritis is one of the commonertypes of renal involvement in lupus.
Dr. Milne: I feel that from the point of viewof clinical medicine any consideration of this renallesion being a glomerulo-nephritis is really out ofthe question. There is no history of the verytypical clinical syndrome, either of Type I orType II glomerulo-nephritis. The renal diseaseis quite unlike typical glomerulo-nephritis as weknow it.
Dr. Cope: There is one other point in whichthe case is rather atypical, now we are collecting
points against the diagnosis. This was a man,and the disease is appreciably less common inmen than in women-not that that rules it out.I wonder whether the whole ambiguity isn'tbound up with the question of nomenclature, andwhether we oughtn't to recognize that this clinicalsyndrome which everyone these days would calldisseminated lupus erythematosus may haveseveral manifestations and several pathologicalpictures and be due to various causes.
Dr. Harrison: Can anybody offer any sugges-tion for the relationship between the repetitivepneumonias and this final picture of L.E.D.?
Dr. Bywaters: We have seen a number of casesof lupus with pneumonia and pneumonia-likepictures, but they were seldom as definite or aslocalized as these episodes appear to have been.I didn't really gather whether Professor Diblethought there was enough in the lungs finallyto correspond with a series of repetitive infectivepneumonias ?
Professor Dible: Yes.Dr. Fearnly: I notice this patient has never
had a leukopenia, and he has responded verywell with a leucocytosis to his various pneumonias.It is commonly believed that patients with lupusdon't show a leucocytosis when they get an infec-tion, but I think this is inaccurate, and that theyvery frequently do. It is also stated if I rememberrightly in French's Index of Differential Diag-nosis that pneumonia in negroes does not cause aleucocytosis; this patient appears to give the lieto that statement.
Dr. Milne: With regard to the lung changes,there is an excellent article in the current AmericanJournal of Medical Science, which states that re-current pneumonias are extremely frequent incases of proved lupus erythematosus; they aredue to secondary bacterial infection and many ofthe cases completely disprove the widely heldview that leucocytosis does not occur. The typicalwhite cell count of lupus is a leukopenia whennot infected, a leucocytosis when infected. Butthey make the point that I think is shown herethat the histology of the lungs is very atypical,and one can very rarely indeed diagnose lupuswith certainty from the lungs at autopsy. Withregard to the pericarditis, I would have thoughtpersonally that this was a mixture of lupus peri-carditis (as shown by the chronicity of some ofthe lesions) with uraemic pericarditis. I wouldemphasize the patient had no clinical manifesta-tions of pericarditis either clinically or by ECGuntil the end. We actually did hear a pericardialfriction rub right at the end, though I failed tomention that rather important fact in giving theclinical history.
Dr. Fraser: Talking of the lung manifestations,
by copyright. on D
ecember 20, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.343.248 on 1 May 1954. D
ownloaded from

May I954 Clinico-Pathological Conference
we had a patient here who died of pneumonia andwas postmortemed here about two years ago.She started like this with a basal pneumonia, andwas liable to frequent severe recurrences. Sheshowed the typical lupus changes in many respectsfinally. But she was somewhat like this-in havingbeen treated with penicillin and developing hyper-sensitivity to it as the first manifestation of anydisease. I wonder if anyone would like to com-ment on the likelihood that the sulphonamidesmight have started the disease off in the presentcase ?Dr. Bywaters: Dr. Gold, I believe, thinks that
sulphonamides can start this thing off as well asa number of other substances. Of course, foryears the current drug being used for discoidlupus (and for various other things) has beenblamed for the exacerbations and for the dissemi-nation of lesions. This is a matter of opinion;I personally do not believe that the sulphonamidesare primarily responsible.
Er. Cope: Perhaps we can add to that pointthe fact that as far as one can gather diseasesidentical with this and indeed the whole group ofsuch cases were described over 50 years ago byOsler at a time when there really were no syntheticdrugs at all. Incidentally, it is of interest thatOsler quite emphatically said 50 years ago thatthe disease occurs without a rash.
Dr. Fearnly: One other point: Dr. Milneraised the question of liver damage on the basis ofthe liver function tests. You get an elevation ofthe serum globulin of this order not only in lupusbut to a lesser degree in rheumatoid arthritis.The thymol turbidity and the colloidal gold testare usually positive in rheumatoid arthritis, andin fact have been used for diagnosis, and they donot necessarily represent any liver damage.
Dr. Lennox: There is one small point I wouldlike to make. A lesion has been described recentlyin the spleen in thrombocytopoenic purpura, orto be more accurate in hypersplenism generally, asa pale band round the hyperplastic lymph follicles.As far as one can tell with the microprojector,I thought the spleen in this case showed it. Itmakes the position of this spleen queerer thanever. The patient had what was presumably theearly stages of lupus erythematosus, and yet thiswas manifesting itself as a splenic lesion of throm-bocytopoenic purpura and the characteristiclesions of lupus erythematosus disseminatus weretotally absent.
Dr. Dacie: May I ask one question ? ProfessorDible demonstrated lymphoid atrophy in thiscase ? Was this due to treatment with cortisoneor ACTH ?
Dr. Milne: He never had cortisone or ACTH.Dr. Doniach: This change was described some
years ago by Klemperer as typical in the lymphnodes, and that was before the time of treatmentwith ACTH.
Dr. Bywaters: I think Tracy Mallory firstnoticed it about I938 or so, but he never, so faras I know, published this, primarily because hewasn't entirely certain that this condition of a sortof emptiness of the germ centres was not seen inother conditions such as diphtheria. He was notsure that it was a specific change.
Dr. Lennox: It would be interesting to havepeople's opinion as to whether this disease hasreally increased or whether we are merely diag-nosing it more often. It certainly appears in listsof diagnoses at least twenty times as often as itdid 20 years ago.
Professor Dible: I looked up the discussion onone of our previous conferences and there Dr.Gold then said that most dermatologists thoughtit had increased-both that it had increased andthat it was more accurately diagnosed.
Dr. Bywaters: I think the impression in theStates, where they seem to see a lot more, is thatit has increased. But we, for instance, since 1939have had regularly about one case every twoyears here, seven or eight in all.
Dr. Fraser: Postmortemed ?Dr. Bywaters: Yes, they have all come to post-
mortem, except one who was started on ACTHhere two or three years ago and is still beingtreated by Sir Henry Cohen.
Dr. Fearnly: Part of the increase may be dueto the fact illustrated by this patient that thedisease is now recognized more commonly, andcertainly in such a patient 15 years ago it isunlikely that the diagnosis would have -beenrelated to the thrombocytopenic purpura of hisoriginal attack.
Dr. Cope: Can I just add one personal pointin that regard. That is, I had a case ten yearsago which in retrospect was undoubtedly one otdisseminated lupus. I could not diagnose it, twoprofessors of medicine were invited to try andboth of them failed to diagnose it also.
Dr. Fraser: We'd better close on that, I think!
BIBLIOGRAPHYROBINSON, W. D., et al. (I953), Ann. Int. Med., 39, 759, (General
Review).CAREY, R. A., et al. (i950), Bull. Johns Hopkins Hosp., 87, 425,
(' Thrombocytopenic Purpura as Presenting Manifestation. )KLEMPERER, P. (x948), Ann. Int. Med., 28, I, (Pathology.)ISRAEL, H. L. (I953), Amer. J. Med. Sci., 226, 387, (' Recurring
Attacks of Pneumonia.')OSLER, W. (I895), Ibid., 10o, 629, (Historical.)OSLER, W. (I903), Trans. Ass. Amer. Physicians, I8, 599,
(Historical.)LEFFLER, R. J. (1952), Amer. J. Path., 28, 303, (Hypersplenism
(splenic lesion)).
by copyright. on D
ecember 20, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.343.248 on 1 May 1954. D
ownloaded from










![Neck Swellings [Compatibility Mode]](https://img.pdfslide.net/doc/110x75/577d2fb61a28ab4e1eb27124/neck-swellings-compatibility-mode.jpg)




![Inflammatory Bowel Disease Arthropathy[1]](https://img.pdfslide.net/doc/110x75/577d21e21a28ab4e1e9619b3/inflammatory-bowel-disease-arthropathy1.jpg)