Embed Size (px)
Citation preview

Conferencia III: Dilemas en el tratamiento de Feocromocitomas y
Paragangliomas
Dilemmas in Management of Pheochromocytoma and Paraganglioma
William F. Young, Jr., MD, MScMayo Clinic
Rochester, MN, USA
© 2011 Mayo Foundation for Medical Education and Research. All rights reserved.

PheochromocytomaPheochromocytoma ——BackgroundBackground
�� CatecholamineCatecholamine--secreting tumor secreting tumor usually localized to the adrenal glandusually localized to the adrenal gland
�� Frequently soughtFrequently sought and and rarely foundrarely found
�� When correctly diagnosed and When correctly diagnosed and properly treated, it is properly treated, it is curablecurable
�� When undiagnosed or improperly When undiagnosed or improperly treated, it can betreated, it can be fatalfatal

Clinical PresentationClinical Presentation
�� PrevalencePrevalence ---- 0.01% to 0.1%0.01% to 0.1%
�� OccurrenceOccurrence ---- equally in men equally in men and women, primarily in the 3rd and women, primarily in the 3rd through 5th decadesthrough 5th decades
�� SymptomsSymptoms ---- present in 50% of present in 50% of patients & paroxysmalpatients & paroxysmal

When to Suspect:When to Suspect:�� Hyperadrenergic spells (eg, episodes of Hyperadrenergic spells (eg, episodes of
palpitations, diaphoresis, headache, tremor, pallor)palpitations, diaphoresis, headache, tremor, pallor)�� Resistant hypertensionResistant hypertension�� A familial syndrome that predisposes to pheo/PGL A familial syndrome that predisposes to pheo/PGL
(eg, MEN 2, NF1, VHL, SDH)(eg, MEN 2, NF1, VHL, SDH)�� A family history of pheochromocytomaA family history of pheochromocytoma�� An incidentally discovered adrenal massAn incidentally discovered adrenal mass�� Hypertension and atypical diabetes mellitus Hypertension and atypical diabetes mellitus �� Pressor response to anesthesia, surgery, or Pressor response to anesthesia, surgery, or
angiographyangiography�� Onset of hypertension at a young age (eg, <20 yrs)Onset of hypertension at a young age (eg, <20 yrs)�� Idiopathic dilated cardiomyopathyIdiopathic dilated cardiomyopathy

Case DetectionCase DetectionLaboratory Evaluation (1):Laboratory Evaluation (1):�� Fractionated cats (dopamine, Fractionated cats (dopamine,
norepinephrine, and epinephrine) & norepinephrine, and epinephrine) & fractionated mets (metanephrine and fractionated mets (metanephrine and normetanephrine) by HPLC or tandem mass normetanephrine) by HPLC or tandem mass spectrometryspectrometry
�� At Mayo Clinic, the most reliable caseAt Mayo Clinic, the most reliable case--detection strategy is measuring fractionated detection strategy is measuring fractionated mets and cats in a 24mets and cats in a 24--hr urine collection. If hr urine collection. If clinical suspicion is high, then plasma fx clinical suspicion is high, then plasma fx mets are also measuredmets are also measured

Case DetectionCase DetectionLaboratory Evaluation (2):Laboratory Evaluation (2):�� Although it is preferred that patients not receive any Although it is preferred that patients not receive any
meds during lab testing, Rx with most meds may be meds during lab testing, Rx with most meds may be continued (continued (all BPall BP --related meds are OK!!!related meds are OK!!! ))
�� Tricyclic antidepressants (TCAs) interfere most Tricyclic antidepressants (TCAs) interfere most frequently with the interpretation of 24frequently with the interpretation of 24--hr urinary fx hr urinary fx cats & mets cats & mets (TIP: cyclobenzaprine [Flexeril(TIP: cyclobenzaprine [Flexeril ] is a ] is a TCA)TCA)
�� Rx with TCAs & antipsychotic agents should be Rx with TCAs & antipsychotic agents should be tapered & D/C at least 2 wks before testing tapered & D/C at least 2 wks before testing
�� It is also important to recognize that catecholamine It is also important to recognize that catecholamine secretion may be appropriately secretion may be appropriately ↑↑ed in situations of ed in situations of physical stress or illness (eg, stroke, MI, CHF, OSA) physical stress or illness (eg, stroke, MI, CHF, OSA)

Causes of False Positive Biochemical TestingCauses of False Positive Biochemical Testing
�� Tricyclic antidepressantsTricyclic antidepressants ---- including including cyclobenzaprine (Flexerilcyclobenzaprine (Flexeril®®))
�� LevodopaLevodopa (Sinemet(Sinemet®®))�� EthanolEthanol�� Withdrawal from clonidine (CatapresWithdrawal from clonidine (Catapres®®) & other ) & other
drugs (eg, illicit drugs)drugs (eg, illicit drugs)�� Antipsychotics (not SSRIs)Antipsychotics (not SSRIs)�� Major physical stress (eg, surgery, stroke, ICU)Major physical stress (eg, surgery, stroke, ICU)�� Obstructive sleep apnea syndromeObstructive sleep apnea syndrome�� Measurements are not affected by most Measurements are not affected by most
antihypertensivesantihypertensives

Dilemma: Diagnostic Issues Dilemma: Diagnostic Issues �� Suppression testing with clonidine or Suppression testing with clonidine or
provocative testing with glucagon, histamine, provocative testing with glucagon, histamine, or metoclopramide are NEVER neededor metoclopramide are NEVER needed
�� In a pt with In a pt with spellsspells , the degree of , the degree of ↑↑ of fx mets of fx mets & cats should be markedly abnormal& cats should be markedly abnormal——in other in other words, if a pheo is responsible for words, if a pheo is responsible for ““classic classic pheochromocytoma spellspheochromocytoma spells””, then the , then the biochemical tests are biochemical tests are ALWAYSALWAYS unequivocally unequivocally abnormal (eg, >5abnormal (eg, >5--fold increases above the fold increases above the upper limit of normal)upper limit of normal)
�� Just because a patient is being treated with a Just because a patient is being treated with a ββ--adrenergic inhibitor without problems does adrenergic inhibitor without problems does NOT mean they cannot have a pheo NOT mean they cannot have a pheo
There is a key link between clinical context and biochemical diagnosisthat most clinicians don ’t recognize

Dilemma: Diagnostic Issues Dilemma: Diagnostic Issues
Additional tips:Additional tips:�� ALL biochemical tests may be nl in an ALL biochemical tests may be nl in an
asx pheo pt with an adrenal asx pheo pt with an adrenal incidentaloma that is discovered in its incidentaloma that is discovered in its ““prepre--biochemical phasebiochemical phase””——the good the good news here is that the imaging news here is that the imaging phenotype will guide your management.phenotype will guide your management.
�� Imaging phenotype (dense, vascular, Imaging phenotype (dense, vascular, slow contrast washout) slow contrast washout) ““ trumpstrumps ””biochemical testing any daybiochemical testing any day
There is a key link between clinical context and biochemical diagnosisthat most clinicians don ’t recognize

Dilemma: Diagnostic Issues Dilemma: Diagnostic Issues Additional tips:Additional tips:�� Most reference labs in the USA have standardized Most reference labs in the USA have standardized
their 24their 24--hr fx mets & cats assays on nl laboratory hr fx mets & cats assays on nl laboratory volunteers that are drugvolunteers that are drug--free & have nl BPfree & have nl BP——I have I have NEVER tested such a patient for pheo!NEVER tested such a patient for pheo!
�� Appropriate 24Appropriate 24--hr urine cutoffs based on pts tested hr urine cutoffs based on pts tested for pheo, but proved to not have this rare tumor are:for pheo, but proved to not have this rare tumor are:
��Met <400 mcg; Normet <900 mcg; Total met Met <400 mcg; Normet <900 mcg; Total met <1000 mcg<1000 mcg
��NE <170 mcg; EPI <35 mcg; DA <700 mcgNE <170 mcg; EPI <35 mcg; DA <700 mcg
�� Pts with lab values > these cutoffs either have Pts with lab values > these cutoffs either have pheo, severely ill (eg, intensive care unit), or are pheo, severely ill (eg, intensive care unit), or are taking a drug that is causing false positive testingtaking a drug that is causing false positive testing

Localization (1)Localization (1)�� We usually do not proceed with localization We usually do not proceed with localization
studies until biochemical studies have studies until biochemical studies have confirmed the dx of a catecholamineconfirmed the dx of a catecholamine--secreting tumorsecreting tumor
�� ComputerComputer--assisted imaging of the adrenal assisted imaging of the adrenal glands abdomen with contrastglands abdomen with contrast--enhanced CT enhanced CT should be the first localization test (sensitivity, should be the first localization test (sensitivity, >95%; specificity, >65%)>95%; specificity, >65%)
�� Approximately 85% of these tumors are found Approximately 85% of these tumors are found in the adrenal glands, and 95% are found in in the adrenal glands, and 95% are found in the abdomen and pelvisthe abdomen and pelvis

Average size = 4.5 cmAverage size = 4.5 cm

T-2T-1

Dilemma: Localization IssuesDilemma: Localization Issues��
123123II--Metaiodobenzylguanidine (MIBG) Metaiodobenzylguanidine (MIBG) scintigraphy is indicated if abdominal imaging is scintigraphy is indicated if abdominal imaging is negativenegative
��123123II--MIBG is superior to MIBG is superior to 131131II--MIBG because the MIBG because the photon energy allows single photon emission photon energy allows single photon emission computed tomographic (SPECT) imagescomputed tomographic (SPECT) images
�� If a typical (<10 cm) unilateral adrenal pheo is If a typical (<10 cm) unilateral adrenal pheo is found on CT or MRI, found on CT or MRI, 123123II--MIBG scintigraphy is MIBG scintigraphy is superfluous and may even confuse the cliniciansuperfluous and may even confuse the clinician
�� If the adrenal pheo is >10If the adrenal pheo is >10--cm in diameter or if a cm in diameter or if a PGL is found, then PGL is found, then 123123II--MIBG scintigraphy is MIBG scintigraphy is indicated because the pt has increased risk of indicated because the pt has increased risk of malignant disease & additional PGLsmalignant disease & additional PGLs

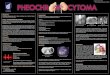
68-yr-old woman with labile hypertensionMarkedly increased 24-hr urine NE and normet

123I-MIBG Scan


��123123II--MIBG is taken up in normal adrenal MIBG is taken up in normal adrenal glands & it is usually asymmetric. glands & it is usually asymmetric. Inexperienced radiologists will typically call Inexperienced radiologists will typically call the LT adrenal suspicious on the LT adrenal suspicious on 123123II--MIBG MIBG scintigraphy because it is much more easily scintigraphy because it is much more easily seenseen
�� Never remove an adrenal gland based on Never remove an adrenal gland based on 123123II--MIBG without CT/MRI corroboration. MIBG without CT/MRI corroboration. Again, a symptomatic pheo typically >4.5 cm Again, a symptomatic pheo typically >4.5 cm in diameterin diameter
Dilemmas with MIBGDilemmas with MIBG

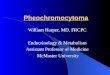
““ MIBG TrapsMIBG Traps ””4444--yryr --old manold man
New onset New onset ↑↑↑↑↑↑↑↑BP & spellsBP & spells
2424--hr urine:hr urine:nmet = 687 mcgnmet = 687 mcgmet = 143 mcgmet = 143 mcg
123123--II--MIBG: MIBG: ““ + LT+ LT””
CT: CT: ““ + LT adrenal+ LT adrenal ””
Lap LT adx: normalLap LT adx: normalcortex & medullacortex & medulla
MIBG Pearls:MIBG Pearls:
There is a normalThere is a normalasymmetry in asymmetry in adrenal uptakeadrenal uptakeLT > RTLT > RT
Symptomatic pheo Symptomatic pheo must have a sizable must have a sizable factory (eg, > 3 cm)factory (eg, > 3 cm)

Localization IssuesLocalization Issues�� It is important to recognize the meds that may It is important to recognize the meds that may
interfere with interfere with 123123II--MIBG uptake (eg, tricyclic MIBG uptake (eg, tricyclic antidepressants, labetalol, CCBs) because antidepressants, labetalol, CCBs) because they should be D/C before imaging they should be D/C before imaging
�� Localizing procedures that also can be used, Localizing procedures that also can be used, but are rarely required, include computerbut are rarely required, include computer--assisted imaging of the chest, neck, and headassisted imaging of the chest, neck, and head
�� Other localizing studies, such as somatostatin Other localizing studies, such as somatostatin receptor imaging with receptor imaging with 111111InIn--DTPADTPA--pentetreotide, may also be considered; but pentetreotide, may also be considered; but the sensitivity of somatostatin receptor the sensitivity of somatostatin receptor imaging with imaging with 111111InIn--DTPADTPA--pentetreotide is lowpentetreotide is low

Localization IssuesLocalization Issues��Although positron emission tomography Although positron emission tomography
(PET) scanning with (PET) scanning with 1818FF--fluorodeoxyglucose (FDG) or fluorodeoxyglucose (FDG) or 1111CC--hydroxyephedrine or 6hydroxyephedrine or 6--[[1818F]fluorodopamine can identify PGLs, F]fluorodopamine can identify PGLs, these expensive techniques probably these expensive techniques probably should be reserved for identifying sites should be reserved for identifying sites of metastatic disease and in patients of metastatic disease and in patients with negative with negative 123123II--MIBG scintigraphyMIBG scintigraphy

Localization IssuesLocalization Issues��� Although positron emission tomography Although positron emission tomography Although positron emission tomography
(PET) scanning with (PET) scanning with (PET) scanning with 181818FFF---fluorodeoxyglucose (FDG) or fluorodeoxyglucose (FDG) or fluorodeoxyglucose (FDG) or 111111CCC---hydroxyephedrine or 6hydroxyephedrine or 6hydroxyephedrine or 6---[[[181818F]fluorodopamine can identify PGLs, F]fluorodopamine can identify PGLs, F]fluorodopamine can identify PGLs, these expensive techniques probably these expensive techniques probably these expensive techniques probably should be reserved for identifying sites of should be reserved for identifying sites of should be reserved for identifying sites of metastatic disease and in patients with metastatic disease and in patients with metastatic disease and in patients with negative negative negative 123123123III---MIBG scintigraphyMIBG scintigraphyMIBG scintigraphy
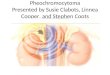
�� Selective venous sampling for Selective venous sampling for catecholamines is usually misleading catecholamines is usually misleading and should be avoidedand should be avoided

J Clin Endocrinol Metab. 2010 Mar;95(3):1328J Clin Endocrinol Metab. 2010 Mar;95(3):1328--32.32.

18 non-pheo pts:RT AV-to-LT AV EPIgradient was as high as 83:1 (median, 2.1:1; P<.02)Although less striking, similar findings were also seen for NE
J Clin Endocrinol Metab. 2010 Mar;95(3):1328-32.

0.1
1
10
100R
ight
AV
/Lef
t AV
Epinephrine Norepinephrine Dopamine
Freel EM et al. JCEM, 2010 95:1328-32

Dilemmas on LocalizationDilemmas on Localization�� The tumor can always be found in the sx pt with The tumor can always be found in the sx pt with
pheopheo——the avg diameter is 4.5 cm. the avg diameter is 4.5 cm. If you are If you are having trouble localizing a pheo, it is usually having trouble localizing a pheo, it is usually because your pt does not have a pheo & you because your pt does not have a pheo & you have ignored some of the biochemical dx tipshave ignored some of the biochemical dx tips
�� MRI is overMRI is over--ratedrated�� EPI/metanephrineEPI/metanephrine--predominant tumors will predominant tumors will
always be localized to the adrenal medulla or always be localized to the adrenal medulla or Organ of ZuckerkandlOrgan of Zuckerkandl
�� NE/normetanephrineNE/normetanephrine--predominant tumors may predominant tumors may arise from the adrenal medulla or from arise from the adrenal medulla or from sympathetic paraganglioma in the abd, pelvis, sympathetic paraganglioma in the abd, pelvis, chest, or neckchest, or neck

Genetic TestingGenetic Testing�� 15% to 20% of pts with pheo/PGL have disease15% to 20% of pts with pheo/PGL have disease--
causing germline mutationscausing germline mutations
�� Hereditary pheo/PGL tumors typically present at Hereditary pheo/PGL tumors typically present at a younger age than sporadic neoplasmsa younger age than sporadic neoplasms
�� Genetic testing should be considered if a patient Genetic testing should be considered if a patient has one or more of the following: has one or more of the following: 1) PGL1) PGL2) bilateral adrenal pheo2) bilateral adrenal pheo3) unilateral adrenal pheo & + FHx of pheo/PGL3) unilateral adrenal pheo & + FHx of pheo/PGL4) unilateral adrenal pheo & young age (<30 y)4) unilateral adrenal pheo & young age (<30 y)5) other clinical findings suggestive of one of the 5) other clinical findings suggestive of one of the
syndromic disorderssyndromic disorders

Genetic Testing TipsGenetic Testing Tips1)1) Involve a genetic counselorInvolve a genetic counselor
2)2) Bilateral pheoBilateral pheo——alwaysalways has a genetic has a genetic causecause——MEN 2, VHL, NFMEN 2, VHL, NF--1, SDH1, SDH
3)3) Unilateral pheoUnilateral pheo——only do genetic testing only do genetic testing if you have a good reason (eg, age <30 if you have a good reason (eg, age <30 yr or +FHx)yr or +FHx)
4)4) ParagangliomaParaganglioma——they they allall should have should have sitesite--directed SDH testing directed SDH testing (Abd/pelvis/chest:(Abd/pelvis/chest:SDHBSDHB>>SDHD>SDHCSDHD>SDHC;;Head/neck: Head/neck: SDHDSDHD>>SDHCSDHC>>SDHBSDHB))
There are genetic forms of pheo &PGL that have not yet beendiscovered.
Thus, whether you dogermline mutation testing or not . . all first degree family relativesshould complete a 24 -hr urine formets & cats!

Treatment (1)Treatment (1)�� Combined Combined αα-- and and ββ--adrenergic blockade is adrenergic blockade is
one approach to control BP & prevent intraop one approach to control BP & prevent intraop hypertensive criseshypertensive crises
�� We start We start αα--adrenergic blockade with adrenergic blockade with phenoxybenzamine 7 to 10 days preop to phenoxybenzamine 7 to 10 days preop to normalize BP & expand contracted blood normalize BP & expand contracted blood volumevolume
�� BP should be monitored 2x/d. Target BP is BP should be monitored 2x/d. Target BP is <120/80 mm Hg (seated), with SBP >90 mm <120/80 mm Hg (seated), with SBP >90 mm Hg (standing); both targets should be Hg (standing); both targets should be modified on the basis of the patientmodified on the basis of the patient’’s age and s age and comorbid diseasecomorbid disease

Treatment (2)Treatment (2)�� On the second or third day of On the second or third day of αα--adrenergic adrenergic
blockade, pts are encouraged to start a diet blockade, pts are encouraged to start a diet high in sodium content (high in sodium content (≥≥5,000 mg daily)5,000 mg daily)
�� This degree of volume expansion may be This degree of volume expansion may be contraindicated in patients with CHF or renal contraindicated in patients with CHF or renal insufficiencyinsufficiency
�� After adequate After adequate αα--adrenergic blockade has adrenergic blockade has been achieved, been achieved, ββ--adrenergic blockade is adrenergic blockade is initiated, which typically occurs 2 to 3 days initiated, which typically occurs 2 to 3 days preoperativelypreoperatively
�� The last oral doses of The last oral doses of αα-- & & ββ--adrenergic adrenergic blockers are given early in the morning on the blockers are given early in the morning on the day of surgday of surg

LongLong --Term Postop F/UTerm Postop F/U��1 to 2 wks postop we measure fx cats 1 to 2 wks postop we measure fx cats
& mets in a 24& mets in a 24--h urine or plasma fx h urine or plasma fx metsmets
�� If levels are normal, the resection of If levels are normal, the resection of the pheo should be considered the pheo should be considered completecomplete
��↑↑eded levels of cats & mets detected levels of cats & mets detected postop are consistent with residual postop are consistent with residual tumor due to either a 2nd primary tumor due to either a 2nd primary lesion or occult metastaseslesion or occult metastases

LongLong --Term Postop F/UTerm Postop F/U
�� 2424--h urine fx cats & mets or plasma fx h urine fx cats & mets or plasma fx mets should be checked annually for lifemets should be checked annually for life
�� Annual biochemical testing assesses for Annual biochemical testing assesses for metastatic disease, tumor recurrence in metastatic disease, tumor recurrence in the adrenal bed, or delayed appearance of the adrenal bed, or delayed appearance of multiple primary tumorsmultiple primary tumors
�� FollowFollow--up CT or MRI are not needed up CT or MRI are not needed unless the mets/cats become elevated or if unless the mets/cats become elevated or if a) the original tumor was associated with a) the original tumor was associated with minimal catecholamine excessminimal catecholamine excessb) the patient has a b) the patient has a SDHSDH mutationmutation

Malignant Pheo and PGL DilemmasMalignant Pheo and PGL Dilemmas�� Distinguishing between benign & malignant Distinguishing between benign & malignant
pheo/PGL is difficult on the basis of clinical, pheo/PGL is difficult on the basis of clinical, biochemical, or histopathologic characteristicsbiochemical, or histopathologic characteristics
�� Malignancy is rare in patients with MEN 2 or Malignancy is rare in patients with MEN 2 or VHL, but is common in those with familial PGL VHL, but is common in those with familial PGL caused by mutations in caused by mutations in SDHBSDHB
�� Although the 5Although the 5--y survival rate for pts with y survival rate for pts with malignant pheo is less than 50%, the prognosis malignant pheo is less than 50%, the prognosis is variable: is variable: ≈≈50% of pts have an indolent form of 50% of pts have an indolent form of the disease, with a life expectancy of >20 y, and the disease, with a life expectancy of >20 y, and the other 50% of pts have rapidly progressive the other 50% of pts have rapidly progressive disease, with death occurring within 1 to 3 y after disease, with death occurring within 1 to 3 y after diagnosisdiagnosis

Malignant Pheo and PGL DilemmasMalignant Pheo and PGL Dilemmas�� The clinician should first assess the pace of the The clinician should first assess the pace of the
malignant disease & target the level of therapy malignant disease & target the level of therapy to the aggressiveness of the tumor behaviorto the aggressiveness of the tumor behavior
�� ““ The penalty should match the crime!The penalty should match the crime! ””�� A multimodality multidisciplinary individualized A multimodality multidisciplinary individualized
approach is indicated to control catecholamineapproach is indicated to control catecholamine--dependent symptoms, local mass effect dependent symptoms, local mass effect symptoms from the tumor, and overall tumor symptoms from the tumor, and overall tumor burdenburden
�� Long term pharmacologic therapy for the patient Long term pharmacologic therapy for the patient with metastatic pheo is similar to that outlined for with metastatic pheo is similar to that outlined for the preoperative preparation of the patient with a the preoperative preparation of the patient with a catecholaminecatecholamine--secreting tumorsecreting tumor

SummarySummary�� ½½ of all pheos in USA are detected as incidental of all pheos in USA are detected as incidental
adrenal masses and these patients are adrenal masses and these patients are asymptomatic (asymptomatic (““imaging phenotype is key)!imaging phenotype is key)!
�� Case detection: fractionated metanphrines and Case detection: fractionated metanphrines and catecholamines; all antihypertensive meds OK; catecholamines; all antihypertensive meds OK; tricyclic antidepressants are the big problemtricyclic antidepressants are the big problem
�� If a pheo is causing dramatic symptoms, the degree If a pheo is causing dramatic symptoms, the degree of elevation in mets & cats should be similarly of elevation in mets & cats should be similarly dramaticdramatic
�� CT>MRI; Consider MIBG scintigraphy if PGL; never CT>MRI; Consider MIBG scintigraphy if PGL; never remove a remove a ““pheopheo”” based on MIBG alonebased on MIBG alone
�� You can always find the tumor in a symptomatic You can always find the tumor in a symptomatic patient (AVS is never needed)patient (AVS is never needed)
�� Consider genetic testing; all need lifelong followConsider genetic testing; all need lifelong follow--upup

Conferencia III: Dilemas en el tratamiento de Feocromocitomas y
Paragangliomas
Dilemmas in Management of Pheochromocytoma and Paraganglioma
William F. Young, Jr., MD, MScMayo Clinic
Rochester, MN, USA
© 2011 Mayo Foundation for Medical Education and Research. All rights reserved.