Embed Size (px)
Citation preview

5/31/18
1
Funded by ARTIC – CAHO and HQO
Dr. Andriy V. Samokhvalov, MD, PhDPsychiatrist and Clinician-Scientist with Addictions Division
and Institute for Mental Health Policy Research, CAMHAssistant Professor, Department of Psychiatry, CAMH
Principal Investigator, DA VINCI
The DA VINCI Project: Developing, Implementing and Scaling Up an
Integrated Care Pathway for Depression and Alcoholism.
10th Annual Addiction Day and Networking FairJune 1st, 2018
MacEwan Hall, University of Calgary, Alberta
* None* The DA VINCI project was supported by the Adopting
Research to Improve Care (ARTIC) Program, a proven model that accelerates the spread and implementation of evidence-based health care interventions across Ontario. ARTIC is co-led by the Council of Academic Hospitals of Ontario (CAHO) and Health Quality Ontario, and is funded by the Ministry of Health and Long-term Care.
Conflict of Interest
Objectives
1. To introduce the concept of an Integrated Care Pathway (ICP)
2. To outline the epidemiology and current challenges in treatment of concurrent depression and alcohol use disorder
3. To describe the DA VINCI project rationale, goals and methodology4. To review the treatment outcomes in patients who received treatment via DA VINCI in a variety of settings

5/31/18
2
DEFINITION: What is an INTEGRATED CARE PATHWAY (ICP)
“A Clinical Pathway is a multidisciplinary outline of anticipated care, placed in an appropriate timeframe, to help a patient with a specific condition or set of symptoms move progressively through a clinical experience to positive outcomes”.
Middleton, Barnett & Reeves (2001)
Benefits of ICP include:
Evidence-based careImproved collaboration, communication, teamwork and care between professionals(efficient use of all resources)Reduce unnecessary variations in patient careOutcome-based, measuring improvements in care and outcomesImprove the patient and family experience of care
5
CAMH Integrated care pathways include:
Pharmacological Interventions (Medication
Algorithms/Titration Schedules)
Non-Pharmacological
Interventions (Psychosocial /
Behavioural interventions)
Clinical Team Intervention (High Performing Teams / Inter-professional
Collaboration)
ICP Implementation, Evaluation and Sustainability
support (Dedicated ICP Program at
CAMH)
* Started in 2013* Establish the Method
• Project leadership team• NHS GOSH Pathways Methodology• Clinical quality improvement focus• Engagement of clinical teams• Pharmacologic and non-pharmacologic Interventions• Who, What, When, Where?
ICP Strategy at CAMH

5/31/18
3
Development and implementation of ICPs at CAMH
Adapted from: Great Ormond Street Hospital for Children. NHS Trust. “How to produce and evaluate an ICP”.
ICPs at CAMH:1. Dementia with agitation (inpatient)2. Treatment-resistant Schizophrenia (inpatient)3. Major Depression and Alcohol Dependence / AUD (outpatient)4. Emergency Department agitation5. Early Episode Schizophrenia (inpatient and outpatient)6. Bipolar Depression (outpatient)7. Late life Schizophrenia (outpatient)8. Memory Clinic (outpatient)9. The two newest additions
1. Major Depressive Disorder (outpatient)2. Alcohol Use Disorder (outpatient)
Expanding the ICP reach
9
Epidemiology
2012 Canadian Community Health Survey prevalence:Alcohol Use Disorder
Lifetime prevalence: 18.1%12-month prevalence: 3.2%
Major Depressive EpisodeLifetime prevalence: 11.5%12-month prevalence: 4.8%
Statistics Canada, Canadian Community Health Survey - Mental Health (CCHS), 2012;

5/31/18
4
Comorbidity Data
Currie et al., 2005
* 12-month prevalence, %:* Individual disorders:* Alcohol dependence (AD): 2.6%* Major depressive disorder (MDD): 4.0%
* Comorbid disorders:* Alcohol dependence / MDD: 5.8%* Major depressive disorder / AD: 8.8%
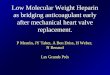
Clinical observationsDistribution of alcohol-dependent patients by severity of depressive symptoms (n=155)
15%
14%
10%
26%
21%
14%
0%
5%
10%
15%
20%
25%
30%
Normal Mild Bord. Moder. Severe Extreme
n Majority (85%) of alcohol-dependent patients have depressive symptomsn Severity of depressive symptoms in 61% of alcohol-dependent patients is
moderate or higher
Clinical considerations
* High prevalence of both disorders* High comorbidity between the two conditions* Hypothesized causal links between MDD and AUD* Undertreatment of MDD in patients with AUD
and AUD in patients with MDD * Low treatment retention and poor treatment
outсomes* Evidence of effectiveness of combined use of
anti-craving medications and antidepressants* Evidence of effectiveness of combined
psychotherapy and pharmacotherapy

5/31/18
5
ICP Major Depression and Alcohol Dependence
* Pilot project
Outpatient treatment:
12 to 16 weeks with an inter-professional team
Admission Criteria
Inclusion criteria:* AUD is the primary substance use disorder of concern i.e. the disorder that causes most distress.* MDD is the primary mental disorder of concern. Same principles as for AUD apply.
Exclusion criteria:* Bipolar disorder. The treatment of bipolar disorder is significantly different from the
pharmacotherapy for MDD. * Alcohol-induced mood disorder. When it’s possible to establish the diagnosis of alcohol-induced
mood disorder, treatment for AUD should be sufficient.* Inability to receive 16 weeks of treatment due to any reason, including, but not limited to:
* Strong active suicidal ideation / Imminent risk of suicide* Medical comorbidities warranting inpatient treatment* Need for alcohol withdrawal management (patients should be provided with medical withdrawal
services and then re-evaluated)* Non-fluent in spoken and written English
14
Standardized Assessments
Pre- and Post-Treatment only• Alcohol Use Disorders Identification Test (AUDIT)• Quality of Life Scales (WHODAS 2.0, EQoL)
Bi-weekly• Penn Alcohol Craving Scale (PACS)• Quick Inventory of Depressive Symptomatology (QIDS)
Pre and as needed• Suicide Risk Assessment
Part of Psychotherapy• Beck Depression Inventory (BDI)• Timeline Follow Back (TLFB)

5/31/18
6
Measurement-Based Care vs. Standard Treatment While Controlling for
Antidepressants
Guo et al (2015) Am J Psych; 172: 1004-1013
• Teaching hospital• Adult outpatients
with moderate to severe major depression
• Pharmacotherapy restricted to paroxetine or mirtazapine in both groups
Pharmacotherapy Manual: Evidence-based

5/31/18
7
Psychotherapy manual

5/31/18
8
* Physician: Assessment, pharmacotherapy* Psychologist (therapist): Psychotherapy according to the
manual* Nurse: Psychoeducation / Administration of clinical scales /
Case work* Pharmacist: Medication compliance / Psychoeducation* Administration: Scheduling, Communications* Team huddle: Weekly case reviews and coordination of
efforts
The ICP Team
Dec 2013

5/31/18
9
* ICP patients at various stages of program completion* N=37* Prospective data collection* Data on controls (HC) were obtained through
retrospective chart review of the patients who received treatment for alcohol use disorder at CAMH Addiction Medicine service and had baseline data on depressive symptoms severity
* Patients with moderate or higher depression scores were selected
* N=92
2014-2015: Early Outcomes
Early Outcomes: Retention rates
Early Outcomes: Drinking patterns, Cravings and Depressive Symptoms

5/31/18
10
The Client Experience* Many patients get to feel that they are part of something special
* The team reinforces this and encourages clients to make the “most of it”* The team feel the same way!
* The team forms an alliance with the patient* We create sense that we are working together to optimize outcomes
* We know the patient and the patient knows us* E.g. we interact with the patient even if they are not seeing us on that day* Occasionally the patient will advise the team members that they have
certain issues that are to be addressed by the team.* Information is shared during weekly team huddles* Patients usually do attend the sessions because they feel that they are
part of a team
Client Satisfaction Questionnaire
* Every patient was satisfied with the care overall: * 47.1% - satisfied, * 52.9% - very satisfied
* Symptoms improvement in 94.1% of pts for both MDD and AUD* Significant improvement of MDD symptoms in 64.7%* Significant improvement in drinking patterns in 82.3%
* All patients stated that the ICP changed their life in a positive way
* All patients would recommend the ICP to a friend
Early impressions* The ICP is a feasible approach to treatment of
concurrent Major Depressive Disorder and Alcohol Dependence with significantly higher retention rates than treatment as usual.
* Patients demonstrate improvements on several levels including depressive symptoms, and changes in alcohol drinking patterns.
* The pilot project achieved its objectives and demonstrated that the ICP model represents a promising treatment approach that can be recommended for broader implementation.

5/31/18
11
ARTIC Opportunity
31
In April 2015, the Centre for Addiction and Mental Health (CAMH) was awarded ARTIC (AdvancingResearch To Improve Care) funding to disseminate the Integrated Care Pathway for the treatment of Major Depressive Disorder (MDD) and Alcohol Use Disorder (AUD). This initiative is known as the DA VINCI (Depression and Alcoholism: Validation of an INtegrated Care Initiative) project across Ontario.
The goal of the DA VINCI project was to support and accelerate the implementation of a standardized treatment protocol across a variety of health care settings and to ensure that patients with MDD and AUD have improved access to evidence-based treatment for these concurrent disorders. In addition to this, the project aimed to improve clinical process integration and to ensure high-quality, sustainable, patient-centered care.
DA VINCI Implementation Strategy
2015-2016 2-Year Outcomes
* Data from patients who started ICP between December 2013 and December 2015 (2 years)
* CAMH only
* N = 81
* Controls were matched by age, sex, severity of depression, and number of standard drinks consumed on weekly basis
* More comprehensive data set

5/31/18
12
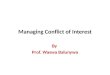
New analysis: December 2013 to December 2015
Base 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16ICP 100.0 100.0 100.0 98.8% 98.8% 98.8% 97.5% 96.3% 92.6% 88.9% 85.2% 85.2% 82.7% 82.7% 82.7% 82.7% 81.5%Controls 100.0 85.2% 79.0% 77.8% 72.8% 69.1% 65.4% 61.7% 56.8% 56.8% 53.1% 48.1% 42.0% 40.7% 38.3% 34.6% 30.9%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%
90.0%
100.0%
Retention rates in ICP patients and Controls
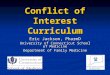
New analysis: December 2013 to December 2015
Legend: SD: Standard drink; DD: Drinking day; SD/DD: Standard drinks/drinking day; SD/w: SD per week, HDD/w: Heavy Drinking Days per week; DD/w: Drinking days per week; PACS: Cravings Scale; BDI: Beck Depression Inventory; QIDS: Quick Inventory of Depressive Symptoms
BDI QIDS PACS SD/w DD/w SD/DD HDD/w
ICP Base 26.3 14.6 17.6 44.6 4.5 7.7 4.2
ICP End 16.2 10.0 12.0 12.6 1.9 3.0 1.2
HC Base 28.3 56.9 5.5 9.5 4.8
HC End 25.2 2.8 5.7 2.0
0.0
10.0
20.0
30.0
40.0
50.0
60.0
Main clinical outcomes
New analysis: December 2013 to January 2016
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
neut
ral
sati
sfie
d
very
sat
isfie
d
diss
atis
fied
neut
ral
sati
sfie
d
v sa
tisfie
d
sati
sfie
d
v sa
tisfie
d
neut
ral
sati
sfie
d
v sa
tisfie
d
sati
sfie
d
v sa
tisfie
d
diss
atis
fied
sati
sfie
d
v sa
tisfie
d
sati
sfie
d
v sa
tisfie
d
atmosp here staff courtesy address concerns exp lanations abt Tx care free ofdiscrimination
protection of confidentiality Overal l care and Tx
Overall Satisfaction

5/31/18
13
New analysis: December 2013 to January 2016
0%
10%
20%
30%
40%
50%
60%
did not change Improved a l ittle bit Improvedmoderately
Improved quite abit
Improvedextremely
did not change Improved a l ittle bit Improvedmoderately
Improved quite abit
Improvedextremely
Mood Drinking patterns
Self-Reported Condition Improvement
* 8 ICP teams created
* 40-50 physicians trained
* 40-50 therapists trained* Many other health professionals
trained
* Over 400 patients treated (396 by the end of the project term)
* We had our Canadian Pathways Conference in 2015
DA VINCI results today
Site EnrolledCAMH 198Trillium 72North Bay 15UHN 28Royal Ottawa 10William Osler 31Hamilton 27Village Family 7Inner City 8
TOTAL: 396
End-of-Project Enrollment

5/31/18
14
Guidelines Concordance
AHC CH FHT OverallUse of scales 96.1% 91.9% 87.5% 94.6%Antidepressants 91.0% 91.9% 87.5% 91.0%Anti-craving meds 89.0% 83.8% 75.0% 86.9%All three components 84.5% 81.1% 75.0% 83.0%
0.0%
20.0%
40.0%
60.0%
80.0%
100.0%
* High concordance rates* Clinical scales use: 100% mark – almost all sites:
* Hamilton, North Bay, Royal, Village, William Osler!
* Anti-Craving Medications Use:* William Osler – 100%!* Hamilton FHT – 93.3%* CAMH – 91.9%
* Antidepressants use – 100% mark:* Hamilton, Village, Royal Ottawa, William Osler
* Overall:* William Osler – 100%!* Hamilton FHT – 93.3%* CAMH – 88.2%
Fidelity Data Highlights
Treatment Completion
AHC CH FHT OverallCompletion rates 74.2% 65.1% 54.2% 70.3%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
80.0%

5/31/18
15
* Overall completion rate is exceptionally high!
* Overall completion rate is slightly lower than in the pilot
study and in the 2-year outcomes analyses
* Predictably: AHC > CH > FHT
* Overall, the difference between different settings is not
very large given the resources available
* CAMH completion rate reduced to 74.1%
* There are TWO sites with ZERO dropouts:
* Royal Ottawa
* William Osler
Completion Data Highlights
Changes in Drinking Patterns
AHC CH FHT OverallBaseline SDW 38.43 21.04 38.68 35.1EoT SDW 12.13 6.03 23.91 11.88
05
1015202530354045
* Highest baseline alcohol consumption level: Hamilton (47.18
SD/w)
* Lowest: UHN, William Osler, Royal Ottawa (13.40-15.33
SD/w)
* Lowest End-Of-Treatment drinking patterns: UHN, Royal Ottawa, Trillium (3.80-5.00 SD/w)
* Highest: Still Hamilton (but they started high too)
* The biggest reduction:
* CAMH – 28.04
* Hamilton – 18.00
* Trillium – 17.05
Drinking Patterns Highlights

5/31/18
16
Changes is Depression Severity
AHC CH FHT OverallBaseline QIDS 15.13 14.81 16.70 15.21EoT QIDS 10.73 10.09 12.95 10.81
02468
1012141618
* The baseline and end-of-treatment data are very similar between the academic health centres, community hospitals and family health teams
* Variation between sites is insignificant in terms of baseline depression scores
* The EoT data suggests that the lowest EoT QIDS scores were in Royal Ottawa - over 50% reduction in depression severity!
Depression Data Highlights
Clinical Improvement
AHC CH FHT OverallQIDS 65.8% 76.7% 75.0% 68.8%Drinking Patterns 63.3% 56.4% 75.0% 62.9%
0.0%10.0%
20.0%30.0%40.0%
50.0%60.0%
70.0%80.0%90.0%

5/31/18
17
* Family Health Teams showed the highest level of symptom reduction
* The highest level of reduction – 81.8% - Hamilton* The highest levels of reduction in drinking patterns:* Royal Ottawa – 100%* William Osler – 83.3%* Hamilton – 80.0%
Improvement Data Highlights
Subjective Measures of Improvement
Patient Satisfaction Questionnaires

5/31/18
18
* DA VINCI showed that the ICP model is feasible in a variety of settings
* Academic Health Centres seem to be the best setting for ICP, as the outcome correlate with the resources invested
* Community hospitals were very close to the AHC in terms of their performance and exceeded them on some levels
* Overall high guidelines concordance and model fidelity* Provided care to a large number of patients and
improvement was achieved in the majority of patients
Lessons learnt
* Establish good partnerships based on realistic expectations* Consistency is the key* Model must be flexible enough to be adopted in a variety of
settings without sacrificing core features and elements* Some elements still might not be implementable at some
settings* Some elements might be redundant* Good, clinically effective, models might turn out to be not
the most cost-effective
Things to remember
* Thank you!
* Kudos to the amazing clinical teams all over the province!
* Questions are more than welcome!
Q&A Session