Embed Size (px)
Citation preview

Confronting the Myth of the
“Non-Adherent” Patient:
How Overcoming Victim Blaming in Healthcare
Can Lead to Better Patient Outcomes
Kathleen Trujillo, LMSW

2
Introduction: A little about me…

Learning Objective 1: Understand the issues associated with the “non-compliant” label.
Learning Objective 2: Use specific assessment strategies to improve assessment.
Learning Objective 3: Understand how integrated healthcare teams can overcome victim-blaming in healthcare.
Learning Objective 4: Provide BETTER CARE for all patients.
At the conclusion
of this session, the
participant will be
able to:
3
LEARNING OBJECTIVES

4
Non-Compliance vs.
Non-Adherence
• Evolution of the terms over the years1
• Resulted from an intention to avoid value judgments of patients1
• Belief that term “non-adherence” = patient understanding and
participation in their own treatment process, while “non-
compliance” = patient submission to the will of medical
professionals.1
• Does the distinction matter?

The Myth of the “Non-adherent” Patient
How is non-adherence defined?
•Taking prescribed agents at doses & times recommended by providers2
•Different classifications2:
• Discontinuation, skipping, altering dosages.
• Forgetfulness, careless missing of doses.
What do medical professionals often mean when they use
the term?
Why is it problematic?
•Leads to healthcare “victim blaming.”
•Allows healthcare professionals and healthcare systems to avoid taking
responsibility for patient outcomes.

What Does “Non-Adherence”
Really Mean?3
Lack of Access to Care
Lack of Supports to Address Social
Challenges
Lack of Education & Understanding

Causes of “Non-Adherence”?
Causes of Non-Adherence3
Forgetfulness (32%) Cost Issues (23%)
Perceived Side Effects (27%) Don't feel it would help (19%)
According to Kaiser
Permanente study of
approximately 9,000
patients.
Note:
46% would fall under
the “better
education” category
Study says nothing
about social issues.

Why does non-
adherence matter?
Expensive
Shorter Lifespan
Quality of Life

The Expense of Healthcare
Healthcare Expense in General:4
•In 2010 the costs of U.S. healthcare exceeded $2.7T, 17.9% of GDP.
•By 2020, projections 20% of GDP.
•20%-30% of U.S. healthcare spending identified as wasteful.
Non-adherence = $100-$300 billion of avoidable healthcare costs.4
•Medical non-adherence account for 33%-69% of drug-related adverse
events that result in hospital admissions.5
Non-adherence to medical treatment is a major concern in chronic
disease management.6
•Almost half of all American adults---117 million people—suffer from
chronic disease.
•1 in 4 Americans has multiple chronic diseases.

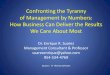
Non-Adherence &
Patient Lifespan
• According to the CDC & DHS,
chronic diseases are responsible for
7 out of 10 deaths each year, and
treating people with chronic
diseases accounts for 86% of our
nation’s health care costs.7
• Individuals with mental health and
substance abuse disorders die
decades before the average
person—largely from untreated and
preventable chronic illnesses like
hypertension, diabetes, obesity, and
cardiovascular disease.8
Infographic: The University of Michigan, Center for Managing Chronic Disease.15

Non-Adherence &
Qualify of Life
• Cost is not only financial, it’s
emotional: chronic disease is
strongly correlated with
depression9. Addressing non-
adherence not only leads to
healthier patients, but HAPPIER
patients.
• Depressed patients are 76% more
likely to be non-adherent to
treatment than non-depressed
patients.1

Challenges to Addressing
Adherence
Challenges to Overcome:
• Not typically seen as a “social issue” akin to IV drug use, DV,
homelessness, etc. by medical professionals OR social workers.
• Social workers don’t widely receive formal training on basic
medical issues, meds, treatment regimens, side effects, etc.
• Disciplines remain in their “box”: Physicians and nurses aren’t
trained to understand social issues, social workers aren’t
trained to understand medical issues.10

Challenges to Addressing
Adherence
Physicians & nurses: understand
implications of non-adherence,
but don’t understand their role in
addressing it 11.
Role of Physicians and Nurses in
patient education & understanding of
their own medical treatment.
•Undermined by TIME pressures.
•Average physician spends 13-16 min
w/ patients.12

Evolution of
Healthcare14
Fee for Service
Focus:
Addressing Medical Acuity Per Visit.
- Little incentive to address overall health issues.
Quality Based Pmnts
Focus: High Quality Healthcare Delivery
- Measured by readmission statistics
Integrated Healthcare
Focus: Integration of healthcare disciplines
-Intended to provide more holistic care.
-Requires improved collaboration & understanding between disciplines.

Integrated Healthcare Model
Movement toward integrated healthcare models in major
healthcare systems
•Healthcare systems responding to changing fee-for-service model
quality-based reimbursement by encouraging inter-disciplinary models
in acute care settings.13
• Focus on readmissions due to penalties imposed by CMS/HRRP = over
$400 million for healthcare organizations in 2015 and 2016.13
•Behavioral health programs:
• Incorporating NP’s and pharmacy access.
• Social services providers are beginning to understand that addressing
medical issues must be addressed with mental health issues.8

IHC Success…
Depends on Better…
•Collaboration & Understanding
• Between disciplines working together to address
medical and social issues.
• Gaining better understanding of each other’s
diagnostic terms, treatment, and prognosis.
• To fully participate in an interdisciplinary team we
must understand each other’s language.
•Advocacy
• Must encourage all professionals in medical settings to
see non-adherence as a social issue.
• Must stand against healthcare “victim blaming”
•Patient Assessment: Today’s Primary
Focus

Assessment…
Must:
• Be open-ended
• Take both medical AND social
acuity into consideration.
• Addresses the 3 main barriers:
• Patient understanding/education
on disease management.
• Access to medical treatment &
prescribed regimen
• Social Challenges

Assessment Math
Diagnosis + Social Issues – Mitigating Factors = Sociomedical Acuity
Sociomedical Acuity: The combination of medical factors and social
factors which determine a patient’s overall risk
(low/moderate/high).
•Risk for readmission
•Risk for “non-adherence”
•Risk of long-term illness, significant harm, and/or
death.
•Higher sociomedical acuity = higher need for integrated services

Group Assessment
Activity:Patient Poker
Playing The Hand You’re Dealt
•Review case scenarios & apply the “Assessment Math” sequence to determine risks
vs. mitigating factors.
•Assign a level of sociomedical acuity (low/moderate/high).
•Identify services and/or plan of action for your patient.

Today’s Takeaways
How we can do better….
•Better initial assessment.
• Consideration of sociomedical acuity.
• Avoiding victim blaming & the “non-adherent” label
•Better discharge & community planning
• Increased advocacy for patients.
•Better financial outcomes for healthcare entities.
Above all: Better CARE for patients.

QUESTIONS?
Contact:
Kathleen Trujillo, LMSW
(602) 710-0553

References (Slide 1 of 2)
1) Kleinsinger, F. (2010). Working with the noncompliant patient. The Permanent Journal, 14, 54-60.
2) Iihara, N., Nishio, T., Okura, M., Anzai, H., Kagawa, M., Houchi, H., and Kirino, Y. (2014). Comparing
patient dissatisfaction and rational judgment in intentional medical non-adherence versus
unintentional non-adherence. Journal of Clinical Pharmacy and Therapeutics, 39, 45-52.
3) Oyekan, E., Nimalasuriya, A., Martin, J., Scott, R., Dudl, R.J., and Greek, K. (2009). The B-SMART
Appropriate Medication-Use Process: A Guide for Clinicians to Help Patients. The Permanente
Journal, 13, 62-69.
4) Luga, A. & McGuire (2014). Adherence and health care costs. Risk Management Healthcare Policy, 7, 35-
44.
5) Blaschke, T. & Osterberg, L. (2005) Adherence to Medication. The New England Journal of Medicine, 353,
487-97.
6) Rafii, F., Fatemi, N.S., Danielson, E., Johansson, C.M., & Mondanloo, M. (2014). Iranian Journal of Nursing
and Midwifery Research. 19, 159-167.
7) The Centers for Disease Control and Prevention (2010). Multiple chronic conditions: A strategic
framework. Retrieved from:
https://www.hhs.gov/sites/default/files/ash/initiatives/mcc/mcc_framework.pdf

References (Slide 2/2)
8) U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services. (2010) Can we live longer? Integrated Healthcare’s Promise. Retrieved from: http://www.integration.samhsa.gov/about-us/what-is-integrated-care
9) Lorden, L. (2003). National Fibromyalgia & Chronic Pain Association. Chronic illness and happiness: Finding meaning in everyday life. Retrieved from: http://www.fmcpaware.org/fundraising/181-positive-attitude/951-chronic-illness-and-happiness-finding-meaning-in-everyday-life.html
10) Basu, G. & McCormick, D. (2017). Future doctors should be trained to promote social change. STAT. Retrieved from: https://www.statnews.com/2017/02/09/doctors-training-social-change/
11) Emsley, R., Alptekin, K., Azorin, J.M., Canas, F., Dubois, V., Gorwood, P., …Schreiner, A. (2015). Nurses’ perceptions of medication adherence in schizophrenia: results of the ADHES cross-sectional questionnaire survey. Therapeutic Advances in Psychopharmacology, 5, 339-350.
12) Medscape (2017). Medscape Physician Compensation Report. Retrieved from: http://www.medscape.com/features/slideshow/compensation/2016/public/overview?src=wnl_physrep_160401_mscpedit&uac=232148CZ&impID=1045700&faf=1
13) Centers for Medicare & Medicaid Services (2015). What’s the CMS Quality Strategy? Retrieved from: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/Value-Based-Programs/CMS-Quality-Strategy.html
14) Centers for Medicare & Medicaid Services (2016). Readmissions reduction program (HRRP). Retrieved from: https://www.cms.gov/medicare/medicare-fee-for-service-payment/acuteinpatientpps/readmissions-reduction-program.html
15) The University of Michigan, Center for Managing Chronic Disease. Retrieved from: https://cmcd.sph.umich.edu/
NOTE: Any photos without citation obtained without charge from: www.pixabay.com