Embed Size (px)
Citation preview

Indian Journal of Experimental Biology Vol. 4 1, July 2003. pp. 70 1-709
Congenital adrenal hyperplasia: Biochemical and molecular perspecti yes
Anll rllpa Maitra* & Heena Sh irwalkar
ational lnstilUte for Research in Reproductive Hea lth ( ICMR), Jehang ir M erwanji Street. Parel, Mumbai 4000 12. India
Congenital adrenal hyperplasia is a disorder occurring in both scxes and is the commonest cau se of ambiguou~ genitali a. It is a group of autosomal recessi vc di sorders in which. on the basis of an enzy me defect the bulk of steroid hormone producti on by adrena l cortex shift s from corti cos teroids to androgens. Autosomal recess ive mutations in the CY P2 1. CYP 17. CYP I I B I and 3~HSD genes that encode stero idogenic enzymes. in 'Idd i ton to mutations in the gene cncodi ng the intrace llular cholestcrol transport protcin steroidogeni c acute rcgulatory protein StA R can cause CA H. Each of the defects causes different biochemical consequences and clinica l features. Deficienc ies in 2 1 hydroxy lase (2 1-0H) and II ~- H yd roxy la se ( II ~-OH) are the two most frcquent causes of CAl-I. Allthc biochemica l defcc ts impair corti sol sec retion. resul ting. into compensatory hypcrsee rct ion of ACTH and consequent hyperpl as ia of the ad rena l cortex. Research in recent years has clarified clinical, bi ochemica l and geneti c problems in diagnosis and treatmcnt of the di sorders. Expanding knowledge of the gene mutations associated with each of thesc disordcrs is providing va luab le diagnostic tools in additi on to
the biochcmical profile and phcnotypc. Gcnotyping is uscful in se lecting instances to providc gcnctic counsc ling and to clarify ambiguous cases.
Keywords: Androgen. Au tosomal rccessi ve di sorder. Congcnital adrenal hyperpl asia. Corti costeroid
Congenital Adrenal Hyperp lasia (CA H) is a group of di sorders caused by inborn errors of stero id metaboli sm. It is a generic term to descri be a fami ly of ad renal di sorders characteri zed by defi ciency of enzymes crucial for sY llthesis of the adrena l steroid , cort isol. Depending on the pos ition of enzyme block, the di sease has been class i fied into various forms. In all these forms, low plasma corti so l from abnormall y 10\." rates of synthesis causes secondary elevati on of' ACTH and subsequent hyperplasia. Congenital adrenal hyperplasia is thus a coll ective term for a number of autosomal recess i ve di sorders affecting ad renal cortex and its development, lead ing to
defecti ve corti sol biosynthesi s. Symptoms due to CAH can vary from mild to
severe depending on the degree o f enzymatic defec t. In the classi c form, defects in the cy tochrome P450s,
21-hydroxylase (2 1-0H) or II~- h ydroxylase ( II ~OH) cause varying degrees of gen ital ambiguity in fema les reflecting re- routing of excess corti so l precursors to androgen sy nthes is pathway during fetal deve lopment. Prenatal androgen excess causes virilization of female genitalia and post-natall y results in advanced bone age and puberty in both females and
* For correspondence: E-mail: anuru pamaitra@hotm ail.com Fax : 9 1-022-41 394 12
males. Defects in androgen synthes is due to defects in
W-hydroxysteroid dehydrogenase C3B HSD)/65-64 isomerase, in 17cx-hydroxy lase/l7 ,20 lyase and in the steroidogenic acute regulatory protein result In inadeq uate prenatal virili zat ion of males and depressed puberty in both sexes. Less severe, nonclass ica l forms of CAH present pos tnatall y as signs of androgen excess.
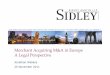
Over the las t decades. genes caus ing various fo rms of the disorder have been identified. Emerg ing informati on is helping in reshap ing thinking about their pathophys iology and supplementing their clini ca l and biochemical diagnosi s. Rev iew presented here provides the current state o f know ledge on these aspects of CAH in the order of genes involved in the adrena l stero idogenesis, from the mitochondrial entry of cholestero l to corti sol sy nthes is (Fig. I ) . The latest syndrome to be molecularly in vesti gated, congen ital lipoid adrenal hyperplasia (CL AH) is descri bed f irst fo llowed by the other more frequentl y seen syndromes VIZ. 3~-h yd roxystero id dehydrogenase (3~HSD), I7cx hydroxy lase (P450c 17), II B hydroxylase (P450c II ) and 2 1 hydroxylase (P450c2 1) deficiencies.
COl/gellitaL Lipoid adrenal hyperplasia alld steroidogenic acute regulatory (star) protein
Congenital Lipoid Adrenal Hyperplasia (CLAH ) is a rare autosomal recess ive disorder that severely

702 IND IAN J EXP BIOL. JULY 2003
disrupt the sy nthesis of all adrenal and gonadal stero ids resultin g in severe salt wasting and a fema le phenotype. It is the most severe form of CAH caused by mutations in the Steroidogenic Acute Regul ato ry (StAR) protein. The central ro le of StAR protein in ca using CLAH was first described by Lin el al. in 1995 when he reported that mutat ion in StAR gene caused congenital lipoid adrenal hyperp lasia I . Key role of the protein in tri ggering ac ute stero idogenic response was evident from the find ing that it promoted steroidogenesis in non stero idogeni c COS I cells co-transfected with StAR and side chain cleavage enzy me and that mutati ons in the gene caused CLAH. It is now well understood th at in adrenals, the chroni c regulation of stero idogenesis by ACTH is at the level of gene transcripti on, but acute regu lation, such as in response to LH surge or to infusion of ACTH is at the level of choles terol access
Cholesl. Trafficker
CHOLESTEROL Cytosol
StAR Depdt Cholesterol transfer
to P450 scc2. The protei n that triggers thi s process of
acute steroidogenes is was identified as StAR and cloned and characterized by Clark et at .) in 1994.
In the di sease, the affected 46 XY genetic males are born with wholly female ex ternal genitali a, reflect ing absence of testosterone synthes is between 6 and 12 weeks of ges tation. Adrenals at birth are engorged with cholestero l es ter deposits . Affected newborns have low but measurable levels of steroid hormones, but they soo n die from glucocort icoid or mineralocorticoid deficiency if hormona l replacement therapy is no t initiated. However surv ival till adulthood in some of the treated cases have been reported4 Reports suggest a wide variability in the prevalence of the disease. The disease is reported ro be co mmon in Japanese, Korean and Palestini an Arab population, but is rare elsewhere5
. Studies on the Indian popu lati on are not avai lab le. Wi th the
~ ...................... . ...... ~ : P45Oc l 7
PREGNELONONE ----t.~ I 7-0H PREGN ELONON E DHEA · · ·
3~-HSD ~ 3~-HSD I P450c l7 1r : P45Oc17
~ 3~ HSD
PROGESTERONE • 17-0H PROGESTERONE : • Androstenedione
: ......... ~~:~2.1 .. ~ ........................ :~5~:~t .......... ~ 17~ Hs"j· P450arom\
DEOXYCORTICOSTERON E II -DEOXYCORTISOL
I I ~~ P450C I I 1r P450C II .. Testosterone ~ Estrone
CORTICOSTERONE CORTISOL 'P450 arom 1 7~ HSD I P450cII ~ +
ALDOSTERONE Adrenal I Gonads I Estradiol
Cortex . .: , ..............................•..............................••.........•... ••..••. ... .......
Fig. I - Schcm:ll ic pathway from mitochondrial entry of cholestero l to synthesis or adrenal and gonadal steroids.

MAITRA & SHIRWALKAR : CONGENITAL ADRENAL HYPERPLASIA 703
knowledge on the central role of StAR protein in regulating acute steroidogenesis , there has been a growing interest regarding mutat ions in the gene and it s association with CA l-I. The gene is located on chromosomc 8 and is 8kb in size w ith scven exons and six introns. A large number of mutations have been reported in six of the seven exons w ith majority of them ly ing in exons 5-7 . Fig. 2 prov ides a schematic diagram of the gene and some of the major mutations observed . The mutations reported are ei ther missense. nonsense or splice site vari ati ons causing ab lat ion or inactivation of the protein6 A pre liminary attempt has been undertaken by us with this background, to amp li fy and analyse the cod ing sequences of StAR gene in a normal Indian population vis-ii-v is confirmed cases of CA I-l. Fig. 3 demonstrates PCR amplifi cati on of the variou s exons of the gene from DN A ex tracted from peri pheral blood. An inserti on variant in the exon 7 w ithin untranslated reg ion of the gene, which has not been reported so far is indicated through our stud / .
Pathophysiology of Lipoid CAH has been explained through a two hit model4. As per thi s model , although mutations in the gene ab lates StAR dependent steroidogenes is, a low leve l of StA R independent stero idogenes is persists. This permits normal placental steroidogenesis and term gestation and also accounts for the low but detectable leve ls of steroid hormones in the sera of li poid CAH patients in the first momh of li fe. However, these concentrations are too low to suppress secretion of ACTH and other gonadotropins. These tropic hormones stimul ate cellular uptake of LDL cholesterol and increased production of cholesterol from aceta te. The stimulati on results in the accumulation of cho lesterol esters. which eventuall y di srupts the ce ll, either throu gh ph ys ica l engorgement of the cell w ith droplets of choles terol es ters or by a chemica l action of cholestero l ox idation products or both. Thi s second hit thu s destroys the low level of StAR independent steroidogeneis, leading to the unmeasurable levels of steroid in the serum o f older children with lipoid CA H
A21 8V
Q258X 6R272 947 illsA L27SP
5'>JdclTT M22ST
1 189deiG 26 1 dell 246 illS G
56-1del 13 bp 838deiA 54~ insTT Q2 12X
~ f 65()d CIC
A Ins
T-1\ (iV-II EI69k [ 169 G RI93X RI82L
Fig. 2 - Schcll1 :.t ti c diagram or si eroid acute regulatory gene and major Illulations reported IAdapted rrom - Miller and Slrau ~s, ./ Sreroid /Jiocil l' lII Mol Bioi. 69.( 19l)l)) 13 11
1.,,,,,'1 1:'0111 -I3 7hp I.ane :'i I .alle 2.C) -\ '(' c( tlll fni I .:t llc 6 La ne 3. 10 1) ' ,\ i.ad der I .alle 7 i." "C -I Fxu Il3 17·1 hI'
" , \;004
","\;( H1"'
Fxonn
2110 hI' 23 ·thp 1.; 7 hp
r'UIl 7 ~ .\ .l.1hl\
Fig. :I - PCR JmpliriC<l liOIl or va ri ou. exo lls or sicroidogenic aCllie regulalory gene

704 INDIAN J EXP SIOL. JULY 200]
;]nd the absence o f circulating tes tos terone in affected 46 X Y fetuses.
With regard to females, fetal ovaries do not express the genes for steroidogenic enzymes and the 46 XX fema les affected w ith CLAH do not recei ve the second hit until the onset of puberty , when LH stimulates low levels of StAR-independent stero idogenes is. Each month another folli cle IS recruite and stimulated by gonadotrop ins, producing spont:lI1eous age-apprupriate breast deve lopment in affected girl s. Ilowevt.:r. gonadutorpin stimu lati on quick ly resu lts in cholesterol engorgement in these ce ll s (the second hit in lipoid CAH), so that the later phase or ovarian steroidogenesis, the sec reti on of large amounts of progesterone, does not occur. Foil icles that art.: not rec rui ted remai n unsti mul ated and constitute a reservoir of steroidogenic cell s undamaged by the second hit of lipoid CAH. Thus with each monrhly cycle, a new undamaged fo lli cle is recruited and est rogen is produced, leading to cyc li c uterine es trogen withdrawal bleeding that resembles normal menses, but as there is no progesterone, these cyc les are anovulatory.
The two-hit model has been further substant iated through generation of StAR knock-out mice by Caron (' I a/. ~ in 1997 and Hasegawa e l u / .<) in 2000.
3/3-hydroxysteroid dehydrogenase deJiciellcy alld CAH 3f3-Hydroxystcroid dehydrogenase/,15-tA isomerase
( 3~H SD) cata lyses the 3B-hydroxys teroid dehydrogenation and ,15 to ,14 isomeri zation of the ,15 stero ids pregnenolone, 17-hydroxypregnenolone, dehydroepiandrosterone and androstenediol into their respective ,14-ketostero iods, namely progesterone,
17a hydroxy progesterone, ,14-androstened ionc and tes tosterone. Thus as w ill be ev ident from Fig. I this hi func tional dimerie enzyme is required for the biosynthesis of all classes of steroid hormones, namely glucoconico ids, mineral ocorti co ids, proges
terone, androgens and estrogens. Isozmyes of the 3BHSD family have been characteri zed during the past decade .and their criti ca l ro le in the steroidogenic reaction s in the ad renal cortex, gonads, placenta and a vari ety of per ipheral target ti ssues have been elucidated. It is a mcmbrane bound enzyme located in the endoplasmic reti culum and mitochondri a. The
type 1 3~-HSD gene was firs t cloned by Luu and his co-workers 10 in 1989 followed by Typell 3BHSD gene by Rheaume el a/." in 199 1. The type I gene encodes an enzyme of 372 amino acids and is predominantly
expressed in the placenta an ; periphera l ti ssues. T ype II gene, sharing 93% homology w ith Type I encodes a protein o f 37 1 amino acids " nd is almost exc lusive ly ex pressed in the adrenals, th e ovary and tes ti sl2. The genes are 7.'8. kb in size consisting of four exons and are ass igned to chromosome I . A ll known mutations
depleting 3B HSD acti v ity arc in the 3BHSDlI gene11.
CAH due to 3fjHSD de frc ieney is relati ve ly rare and is known to ex ist in two distinct classe. viz. class ica l and nonc lass ical forms. Class ica l form. accounting for about 1% to 10% of CA H cases. has been shown to result from mutations in the typc II
3 (~HSD 14 15 I . .. hi ' I-' gene ' ' . t can eX lsl In elt er sa t·· wastlng or
non sa lt-wasting forms. The non class ica l 3~HSD deficiency, also referred to as late onset deficiency has becn more diffi cult to di agnose and has not been
associated w ith any mu tat i ns in the 3BH SD gene. The salt los ing form is usuall y diagnosed during the f irst few Illonths of l i fe and is associated with i nsu ffi cient biosynthesis of aldosterone and consequcnt salt Juss which may be ratal i f not di agnosed and treated earl y . In contra:; t in non salt
los ing form of 3BIISD defi ciency may be diagnosed later, often delayed until adrenarche. In class ica l
3~HSD deficiency, the basal plasma levels of ,15 steroids such as pregnenolone, 17-0H preg nenolonc and DHEA arc elcva ted in affected indi viduals. o f which the elevated pla ~ma level of 17-0 1-1 pregnenolone after stimul ation with ACTH appears to be the best indicator. Over-all an elevated rat io o f ,15/,14 steroids is considered to be the best biologica l parameter for diagnosis o f 3f511 SD deficiency l(,.
As regards molecular dlagnosis, a total o f 34
mutati ons in the type ll 3 ~HSD gene have been reported so fa r (Fig. 4). Thi s includes 5 frameshift , 4 nonsense, I in -frame deletion, 1 splicing and 23 missense mutations. The heterogeneous clinical presentation seen in the disorder has been attributed to thi s w ide distributi on of the gene Illutati ons. Funct ional charac teri za tion of most of the mutan t genes has also been calTied out by transient express ion of the mutant proteins using intact human 293 ce ll s. The studi es have prov ided valuab le information on the genotype phenotype relati onship o f the mutant prote ins wi th severity of the disease l7.
l7a-hydroxylase deficiency aild CAH 17a Hydroxy lase (P450 c 17) is the enzyme that
brings abollt 17-hyd roxy lati on of pregnenolone and progesterone to 17a-hydroxypregnenolonc and 17a-

MAITRA & SH IR WALKAR: CONGENITAL ADRENAL HYPERPLASIA 70S
hydroxy progesterone respectively. This 17-a-hydroxypregnenolone may further undergo sc iss ion of the C 17, 20 carbon bond to yield dehydroepiandrosterone.
Defects in P450c 17 lead to male pseudohermaphroditism with various degrees of ambiguous genitalia. Patients with the deticiency have decreased cOl1isol synthesis, overproduct ion of ACTH and stimulation of steps proximal to P4S0c 17 (Fig. I ). These pat ients may have mild symptoms of glucoconicoid deticiency, but this is not life-threatening as the lack of P450c 17 resu lts in the overproduction of corti costerone, wh ich also has glucocorti co id activity . Affected females are phenotyp ica lly normal but fail to undergo adrenarche and puberty .
Gene encodi ng the enzyme complex CYP 17 is located on chromosome 10 that is structurally related to the gene for P450c2 1 (2 I -hydroxy lase) . Several
A
different mutat ions in the gene have been reported lead ing to either a complete or partial form of the di se;\se I 8
.
1 J fJ-hydroxylase deficiellcy alld CAJ-J I I ~- hydroxy l ase (P450c I J) is the enzy me that
cata lyses the terminal step in biosynthes is of cortisol viz. II ~ hydroxy lation of II-deoxycorti sol to cortisol. Deficiency of the enzy me is the second most common cause of CAH, nex t to 2 1-hydroxy lase deficiency. It is encoded by the gene CYP JIB I , wh ich is induced by ACTH and is suppressed by glucoconicoids 'uch as dexamethasone. Mut ations in the gene lead to deficient adrenal II p-hydroxylase acti vity and inefficient convers ion of II-deoxycortisol to cort iso l. Decreased corti sol product ion leads via poor feedback control to increased ACTH secretion. Thi s leads to
\ 1(1 - \
\ ~1 1 C;1 ~~ ll ' ·itbhli
8
\111\
C III' . ; '1
I'lftJ .• ISm. ,
j
\S2 I
10,,- 1 c; r. F 1.\ .' \
\\1 - 1\
( ; ~I' ..J \ .
'-/. '
~lu \I:-Il i2:'11 - ~-3 f lS.J ':W,'\ ) 11- J - I x<
I _ .:!II~ "
1'1 <:'1.
, ~:' "} ilgi'S' !'PAt ..
, .1 11 .\ \
i8:iZHi'A fC!.J ') \ Sh - dj ·j ( ,
~ I.~ d.-l \ \
Fig. 4 - Scheillali c rcprcscntaLion of thc lIlutations idcnLified in the IiSD382 gene in indi viduals suffering from classica l W- HSD deficiency . (A ) The lIli sscnse lIlutatioll s Ih ~tl have heen shown 10 relai n a certain amoulll of 3~- HSD aCliviLy. A lso highlighLed arc Lhe co faclor hinding domain (C BD). Lhe two putative subSLrate binding dOlllains (S BD). and the Iwo membrane-spanning domains (MSD). (8) The missense mutalions IhaL have been shown La abolish enzY llle activ it y (top), and the nonsense, frallleshif'L and in-frame deleti on mUlations (bollom). Mutant recombinant proteins with apparent instabitity an: shown in bold btack hoxes_ (Adaplcd from Simard . Moisan and Morel. Sel1l /<eprod Med, 2002)

overproduct ion by ad renal ce ll s of the steroid precursors prior to the block. The precursors are thus shunted into androgen pathway resulting in rn ~lrk ed
androgen excess and virili za ti on. li p-hydroxy lase deficiency is an autosomal recess ive di sorder and is estimated to be prevalent in about 5% of pati ents with CA l-I. Overall prevalence in the genera l population is es timated to be approx imately I in 250000 19 Females with class ic I JP-hydroxylase deficiency are born w ith masculini zation of their ex ternal genitalia, cau sed by secret ion of adrenal androgens during embyronic and fetal developmen t. In non-classic li P- hydroxy lase deficiency, the patients arc born with normal genitalia and present with signs of androgen excess as children. Adu lt women may present w ith hirsuiti sm and amenorrhoea. However on ly a sma ll percentage of women with hirsuiti sm and amenorrhoea have nonclassic I I P-hydroxy lase deficienc/(I· 2 1.
The gene encodi ng P4.')Oc II , CYP II B 1 is 7 kb in size located in chromosome X and conrains 9 exons. In class ic I I p-hydroxy lase deficiency more than 30 different mutations in the functional regions o f the gene have been reported so far (Fig. 5). The Illutations reported are missense, nonsense and sp li ce site Illutations. Functional ana lys is of these mutations show an abolition of the enzyme ac ti vi t/~ .
With regard to non-class ic form of the disease, reports are scarce. The study by Joehrer e l 0/. 2.1 in these cases. reported nonsense as we ll as missense Illutations that caused reducti on In the enzyme
Exon I
P32~ I nI
1'42S
W l1 6X
2
A
KI74X
I OS-~28bp- 11 4
120-insAGACA· 121 G1 24~ 1 1ll
V I 29M
3 4
splice si te mutation G to T + 16 III in the splice donor site
5
acti vity. A wide variability in the phenotype w ith regard to mutat ions has also been reported in both class ic and non-class ic forms of the disease. Based on these mutational ana lys is of DNA obtained by amniocentes is or chori onic villus biopsies, attempts have been made for pre-natal diagnosis of the di sease. However, it has been of limited val ue so fa r, mainl y due to the wide di stributi on of mutations with in the gene.
2 I-hydroxylase deficiency alld CAH The deficiency of enzyme 2 1-hyd roxy lase (2 1-
OHD) is the most common ca use of CA i-1 w ith a frequency of about I per l 4000 li ve bi nhs in the general population14
. In an Ind ian study among cases of ambi guous genitali a, 2 1-hyd roxy lase deficiency was found to be the cause of CA H in more th an 900/(' of cases detec!ed25
.16
. It is the key enzyme in ad renal cortex bringing about conversion of progesterone and 17 -hydrox yprogesteronc to deox ycorticos terone and II -deoxycortisol respecti ve ly (Fig I ). Di sorders in th e gene encod ing the enzyme viz. CYP2 1 cause about 95 % of all cases of CAH 27 . 2~ . Both classica l and nonclass ica l fo rms of CAH due to 2 1-hydroxy lase deficiency havc been recogni sed . The classical disorder, occu rring in about I : J 3.0nO to I : 15, oon births world \.v ide~Y, has two forms, si mple virili zing and sa lt was ting. Pat ients with simple vir ili zing 2 1-hydrox y lase deficiency man i fest viril iza ti on ow i ng to excess androgen secreti on. Sa lt was tin g 2 1-0HD (in
6
splice site mutation G to A + I I1t in the splice donor si te
7 8
R4 27H V44 1G R448H R448C L4641ns3nt
')
3'
splice site mutation A to G + 4 n1 in the splice donor site
7 kb
Fig. 5 - Schemati c represental ion of Ihe genomic sl nlClu rc of Ihe human CYP Il ll I gene and posil ions of lllul,J[ions rcporled. Exons are
represcnted by hoxes: black hoxes demarcale Ihe coding regions. and open boxes represent the non-coding re~ions (t., deletion: ins, inserti on; nt. nLicleoti de).(Adapteci fro lll Pt'[er M . Sell/ Reprod Mcd. 2002)

add iti on to hyperandrogcneni sm), which in vo lves a deficiency in aldosteronc producti on as well as in corti sol, occurs in ahout three -fourths o f class ica l cases. The non-c lass ica l form , which in vo lves a milder enzy matic defect, occurs in about I : 100 births in the general populati on.
As has been described ea rli er, thc defi cient corti so l product ion in these cases 1<; fo ll owed by overproducti on of ACTH by th~ pituitary due to poor negative feedback, resulting In ad renocorti ca l hypcrplasia. Precursor steroids prox imal to the 2 1-hydroxy lase cnzyme block and/or those for which 2 1-hydroxy lation is not requireci (progesterone, 17-hyd roxyprogesterone, L':A-andros tened ione) are oversecreted and shunted into pathway of androgen synthes is. Classica ll y affec ted females who do not undergo trea tment are thu s v irili zed " in utero" and are born w ith ambiguous genitali a. Post natall y in both class ica l and non classica l forms. ma les and females can present at any time w ith signs of and rogen excess.
Most patients wi th class ic CA H-2 10HD al so have inadequate aldosterone and therc!'ore cannot maintain sodium balance. Abou t 25 % have sufficient aldosterone levels and no salt was ting, yet show prenatal virili 7.ation <lI1d/or marked ly increased producti on of hormonal precursors of 2 I -hyrdoxy lase (e.g. 17 OHP). These indi viduals are referred to as "S imple viriti zers". Patients w ith the mild , non-class ic form of 2 I -hydroxy lase deficiency Illay have any of the signs of post natal androgen excess but affected females may have varying degrees of ambiguous ex ternal genitali a. Adrenal steroid precursors of 2 I -hydroxy lase are only mildl y elevated. 17-0H progesterone levels are rai sed. parti cularly in response to an intravenous bo lus of ACTH . The severity o f signs and symptoms of mild androgen excess vari es w idely. and prohab ly many affected indi viduals are asymptomati c. Severe cystic acne, hirsuti sm and oligomenorrhoea in young women are cOlllmonl y presenting symptoms. M ale patients are large ly asymptomatic, but may present w ith acne or in fertilit y.
New born males w ith 2 I -h ydroxy lase deficiency usuall y show increased phallus size, pi gmented scrotum and bil ateral testes. Newborn fema les wi th class ic virili zing CAH, manifest variabl e degrees o f genital ambigu ity ca used by high systemic leve ls of ad renal androgens beg inning at abou t 71h week o f gestati on. Females w ith the milder non-class ic form of the di sorder are di stin gui shed by little v irili za ti on at birth 'O
Class ic 2 1-hyd roxy lase dcficiency is di agnosed
based on a marke Il y elevatc:d serum level of 17 OHP. the main substrate for the enzy me. The d iagnllsis can be further refined by perfo rming ACTH stimul at ion. And rostenedione leve ls along w ith 17 OH P prov ides the method for monitoring effi cacy of therapy in fema les and tes tos terone al ong w ith 17-0HP in case of males.
Reproducti ve prob lems for women w ith the di sease usuall y become apparent in ado lescence. The average age at which menarche occurs in in:ldcquaLely trea ted girl s is late compared w ith hea lthy peers .. l . Such pati ents often have a cl ini ca l pic ture similar tn polycysti c ovary sy ndrome w ith sonographi c ev idence of mUltiple cys ts, anovulati on. irregular bl eed ing and hype randrogenic sy mptoms. In non-classic CA H. a signifi cant reducti on in insu lin sensiti v ity is also seen among non-obese young women as compared w ith control s of simil ar age and we ight. However a review carri ed out in 1992, found that up to about 80o/c of simple virili zers and 60% of sa lt -wasters can hc:a r chiILiren'2 . In m:lI es w ith class ic fo rm of th e di sease. impaired gonadal functi on i · less frequen t compared to fema les. M ost males arc ab le to father children. or at least ha ve adequate sperm counts" . Among simple v irili zers, tes ti cu lar integrity may be normal even in the absence of trea tment.
T est icular tumors 01· ad renogenital sy ndrome may occur in CA l I males, espec iall y if thc:y arc inadequately trea tcd sa lt -wasters. A ll pati ents with class ic 2 1-hyd roxy lase deficiency and sy mptomat ic pati ents w ith non class ic di sease requ lf\~
glucocorti co id treatment. In fants w ith the sedt washing form o f 2 I -OP.D req uire mineralocorti co id and sodium chloride supplements In addition to glucocorti co id treatment.
The molecular genetic bas is of 2 1-0HD has been studi ed ex tensi ve ly and has important impli ca ti ons fo r prenata l diagnos is and counse ling. As dep icted ill Fi g. 6 the gene for C YP2 I encodill g the 2 1-hydroxy lase enzy me is located on chromosome 6 and li es in the middle of the major hi stocompati bi lity locus,·u5. Thus, di sorders o f adrena l 2 1-hydroxy lation are linked to spec ific hUlllan leukocyte antigen (HLA) types .The gene contains 10 exons spaced over 1.1 kb and bea rs close resemblance to the inacri ve pseudogene C YP2 I P. It is also repoled to have the highes t rates of single nucleotide pol Ylllorphi sms among over 100 human genes tes tecl36 Studies ha ve also revc;li ed as many as 56 Illu tati ons In the geneJ7
Approximately 40-50°;(, of these are either deletions or a si ngle poi nt Illutation alleri ng spl ici Ilg bet ween

708 INDIAN J EXP B IOL, JULY 2003
liLA Class I (1200 bpI
liLA Class III (1100 bpI
liLA Class II (9{)0 bpI
A DR DQ UP
C2 Ilf C YP21P CYI'2 1
Fig. 6 - Schcmat ic of CYP2 1 gcnc. CYP21 P is an inact ivc pscudogcnc; A.B,C.D arc HLA antigens; C4A and C4 B encodc comp lcment
component 4. (Adaptcd from Hughes LA . Selll Reprod Med. 2002)
second and third exons. The mu tati ons ha ve been largely shown to correlate with one of three main clinical categories: class ica l salt-washing, class ica l simple virili zing and non class ical or late onset form ofCAH3x
.
Deleterious mutations in the gene include an A -7 G substi tution, 13 nucleotides before the end of inn'on 2 that res ults in aberrant splicing of pre-mRNA, an 8-nt del etion in ex on 3 and a I nt inserti on in exon 7, each of which shifts the readi ng frame of translation, and a nonsense mutati on in codon 318 of ex on 8. Seven additional missense mutations ha ve also been reported in pati ents wi th 2 1-hydroxy lase deficiency . Functional effects of these mi ssense mutat ions have been assessed "i n- vitro" using different ex pression
d I bl " . . 171R systems an s lOW an a atlon tn enzyme actlvlly' ... With the gain in knowledge regard ing the DNA
mutations, tools have been es tab lished fo r pre-natal molecular di agnos is of the disease. Laboratories have developed strategies for rapid detection of the CYP2 1 gene mutations that account for large majority of cases39 Direct analys is of DN A extracted from chorionic villus sa mples has led to strengthening of pre-natal diagnosis of the di sease, th at has been based on second trimester amniotic tluid 17-0H progesterone measurements-lO.4t and HLA hap lotyping. However, a limi ting factor in this app li cation is the variability in the genotype phenoty pe associat ion reported with these mutations.
CA H being an inherited metabolic defect, attempts have been made to explore the prospects of gene therapy for amelioration of the disease. Sporadic reports have been ava il able in recen t years suggesting feasib ility of the approach-l 2. ln a recent report, mi ce with 21 -hydroxy lase deficiency have been rescued by transgenesis with a murine CYP21 gene-l3. However, the prospect of using the approach in humans is still not promising. Adequate suppression of adrenal
androgens along with norma l biosynthesis of corti so l. are seen to be major di ffi cu lt goals to achieve~x . Also. maintaining the levels of expression indefinitely seems unlikely to be achieved in foreseeable future and med ical therapy , al!hough n t perfect, wi II con tinue to be therapeutic options for the di seasc.
Acknowledgement Authors gratefu ll y acknowledge Dr. Zareen Palel,
Deputy Director NIRRH for hcr construct ive suggest ions. Help and support received from Dr. C P Puri Director IRRH is also acknow ledged. The publication is supported by [CMR, New Delhi.
References Lin D. Sugawara T, Str" uss III J r 1'1 al., Role of stcroiodgenenic acute rcgulatory protein in adrenal and gonadal stcroidogcncsis, Scicl1ce. 267 ( 1995) 1828.
2 Stocco D M & Clark B J. Regulation of thc acutc product ion of stcro ids in stcroidogenic cel ls. Elldocr Rei'. 17 ( 1996) 221.
3 Clark B J. Wcl ls J, K ing S R, SIOCCO D M Thc purifi catio n. cloning and cxprcss ion of a nove l lutcini /.ing horJl1 ()neinduced mitochondri al protcin in MA-I 0 llHl USC Icydig tumor cc ll s Characteri zation of the stcroidogenic acute rcgu latory protcin (S tAR). J Bioi Chelll , 269 ( 1994) ~X3 14.
4 Mi l ler W L. Disorders of anurogcn biosynthcsis. Sem ReJirod Med. 20(3) (2002) 205.
S Bose H S. SalO S. A iscnbcrg J el al .. MI.lt::llioIlS in the stcroidogenic acutc rcgulatory protein (StAR ) in six patients with congenital lipoid adrcnal hypcrpla, ia. J Clill Elldocr Meta/). 8S( 10) (2000) 3636.
6 Millcr W L & Strauss III J F, Molccular pathology and mechanism or action or the stcroiodgcnic aCLIte regu latory protein. StAR. J Sleroid Biochem Mol Bioi. 69 ( 1999) 13 1.
7 M aitra A, Shirwa lkar H. Mukhopadhyay R 1'1 al. Mutation analysis of steroid acute .cgulatory genc in congenital adrcnal hyperplasia Abstrac t no. 4, National Confcrcncc on Reccnt Advanccs in Rcprcduct i vc Hea lth February 6-8, 2003, Jaipur, India.
8 Caron K, Sao S C, Wctsct W el al Targcted di sru pt ion or thc mousc gcne encodi ng stcroi dogenic aCllIe regulatory protcin prov idcs insight into congenital lipoid adrenal hypcrplas ia, Proc NaIl Acad Sci USII. 94 ( 1997) 11540.

M A ITRA & SH IRWALKAR : COl GE ITAL ADRENAL HY PERPLAS IA 709
9 Hasegawa T . Zhao L P. Caron K M 1'1 (/1. Deve lopmenlal rol es of thc slcroidogenic .ICUtC regulati on protei n (StA R) as rcvealed by StAR knockout Illi ce. Mol Elldoerill ol, 14 (2000) 1462.
10 Luu-The V. Lachance Y. Labrie C cl "I Full lellgth eDNA structurc and deduced 'lmino ac id sequence of human 31)hydroxy 5-ene steroid dchydrogcnasc. Mol Elldoerill ol. 3 ( 19X9) I3ID.
II Rhcaumc E. Lachanec Y. Zhao H F 1'1 al . Structurc and exprcssion or a ncw complcmcntary DN A coding thc almost exc lw,ive 3~- hydroxy steroid dehydrogcnase/dclta 5-dclta4-isomcrasc in human adrenals and gun.lds. Mol EIlr/IJcrinol . 5 ( 199 1) 1147.
12 Silllard J. Moisan A M & M nrci Y. Congenilal Adrenal Il ypcrplasia duc to 3IJ- Hydrnxy, teroid dchydrogcnase/L\5-L\4 isolllera,e deficicncy. Selll RetJmd /lIl ed, 20: 3 (2000) 255.
13 Sultan C S. Pari s F. Jcandel C el (II Aill biguous genitali a in the newborn . Selll Neprodl/c M erl . 2() : 3 (2002) 18 1.
14 Bois E. Mornet E. Champret A 1'1 al Congenital adrenal hyperp lasia (2 1-0H) in France : Popul at ion gcneti cs. A reI! Pedililr. 42 ( 1985) 175.
15 Thi len A. L.u·seon A COllgellital adrenal hypcrplasia in Swedcn 1969- 1986 prevalcnce. symptoms and age al diagnosis. lI ela Pediarr SC{l lld. 79 ( 1990) 168.
16 Cara J F, Mo,hang T Jr. Bengiovanni A M el III .. Elev:llcd 17-hydroxy progcsterone and testosterone in ncw born with 3 ~- hydrox y ~tero i d dehydrogenase dcl'ic iency . N Engl'/ M ed, 3 13 ( 1998) 6 18.
17 Moisan A M . Rickells M L. Tardy V el 01 .. Ncw insight into
the molecular basis of 3 ~- h yd roxysteroid dehydrogenase deficicncy : Identificati on of cight mutations in the HSD 3 ~2 gcne elevcn pati ents from seven new famil ies and compari son of the functi onal properti es or tweill y fi vc IllUlant ell /.ymcs, ./ elill ElI£loerillol M elli " , 84 ( 1999) 4410.
18 Auchus R J. M iller W L , Molecul ar mode lin~ of human P450 c 17 ( 17a-hydroxy laseIl 7. 20 Iyasc): Insights into reac ti on 1l1L'c hani s lll ~ and ef fcc ts of mutati ons, Mol Eli riocrill lJ l . 13 ( 1999) 11 69.
19 Rostcr A, Lciberman E ('{ lI l . . High frequency of congenital adrenal hyperplasi a (c lass ic I I P-hydroxy lasc deficiency) umong Jews rrom Morocco. 11 111./ Med Gellel. 42 ( 1992) 827.
20 Carmi na E, Mali zia G, Pagano M 1'1 al ., Prevalencc of latconsct 1 ifJ-hydroxy lase dcl'i c iency in hi rsute patieills. J Elidocr i ll ol l lll 'I'SI. I I ( 1988) 595.
21 Azziz R, Boot. L R. Parker C R 1'1 al I I P hydroxy lase dcfi cicncy in hypcrandrogeni slll Ferril Sleril 55 ( 1991 ) 733.
22 Peter M , Congcnital ad rcnal hyperpl nsia: II ~- h ydroxy l asc dcfi cicncy 5 1'111 RefJrod M erl. 20 : 3 (2002) 249.
23 Jochrcr K. Gcley S. St rasser-Wozak E M C 1'1 lIl., CYP I I B I mutations cau sing non class ic adrenal hyperplusia due to 11 ~- hydroxy lase deficiency . /-1 /1111 Mol Gellel. 6 ( 1997) R29.
24 Pang S y, Wallace M A , Hofman L 1'1 al., World wide ex perience in ncw born sc reening for classical congcnital adrcnal hyprplasia duc to 2 1-hydroxy lasc deficicncy . Pedilllries. 81 ( 1988) 866.
25 Desa i M 1', Patcl Z M & Alilhani L M . Congenital adrenal hyperpl asia. In M edical gellel ies ill Illdia, Vol. 3. editcd by I C Vcrllla (Aroma Press. India) 1980 .
26 Patel Z M. Amhani L M . Dalal S J 1'1 al., Ambi guous genitali a ' lldiall Pt'dial , 2() ( 1983) 278.
27 Morel Y & Miller W L. Clin ica l and molccular gencti c" of congenita l ad renal hyperp lasia duc to 2 1-hydroxylase deficiency, l Id\' /-11/1/1 Gell l'l , 20 ( 199 1) I .
28 White PC & Spciser P W , Congeni ta l adrenal hyperpl as ia due to 2 I -hydroxylase defi ciency. Elldoer Rev, 2 1 (2000) 245.
29 Pang S & Clark A . Congenital ad renal hyperp lasia duc to 2 1-hydroxy lase ddic iency: New born sc reening and i ts relationship to thc diagnosis and treatment of the disorder. Sen 'ellillg, 2 ( 1993) 105.
30 Speiscr P W. Congenital adrenal hyperplasia: Transition from childhood to adu lthood . ./ Elidocrillol l lll 'esl . 24 (200 1) 61') I .
I I Helleday J. Si wers B. Ril/.en E 1 "l lIl., Subnorillal androgcn and elevated progesterone levels in women trealed for congenita l virili zing 2 1-Hydroxy lase defi ciency . .I Ciill Elldocrillol Me/ab , 76 ( 1993) 933.
32 Feldman S, Bill and L. Thalahard J C el al .. Fertilit y in womcn with latc onsct adrenal hyperpl as ia duc to 2 1-hydroxy lase deric iency , .I Ciill Elldocrill ol Merabol. 74 ( 1992) 635.
33 Urhan M D. Lce P A & Migeon C J, Adu lt hc i ~ ht and rertilit y in mcn with congenital virili zing adrcnal hypcrplas ia. N Ellgi .I Nl ed. 299 ( 1978) 1392.
34 Hi gashi Y. Yoshioka H. Yamane M 1'1 a/., Compictc nuclcotide sequence of two steroid 2 1-hydroxy lase gcnes t<1 ndcmly arrangcd in human chromosomc: A pscudogenc and gcnuinc genc f'roc NaIl Acad Sci US/I . 83 ( 1986) 284 1.
35 Whit e P C. cw M I & Dupont B. Structure of thc human steroid 2 I -hydroxy lase gcncs. Proc NaIl ll ead Sci USA, ( 3 ( 1986) 5 1 II.
36 Cargill M. Altschuler D. Ireland J 1'1 al .. Characteri zat ion of singlc nucleotidc polymorphi sms in cqding rcg ions of hU lllan genes. NIII Gellel , 22 ( 1999) 23 1.
37 Lee H H. CYP21 Illutati ons and congenital adrenal hypcrpl as ia, Clill Gellel . 59 (200 I ) 293.
]8 Ilughes I A . Con}?c nital adrenal hy perp la ~ ia : 2 1 - h yd roxyla~c
defi ciency in the new born and during in fancy. S1'1I1 Rellmd Med, 20 : 3 (2002) 229.
39 Yokoyama Y. TcraoKa M . Tsuiji K 1'1 0 1., Rapid sc rccning Illethod to detec t mutalions in C YP2 1. the gene ror 21 hydroxy lase, AliI ./ Ma l Gellel. 9~ (2000) 28 .
40 Stlchak R H & Patel Z M , Antc-natal diagnosis of congenita l ad renal hyperpl as ia ./ Clill Gellel Tribal Res. 12 ( 1996) 110.
4 1 Patel Z M. Sridhara S, Aillbani L M 1'1 al., Ant e-nata l diagnosis or congenital adrenal hypcrplasia. India II Pediar. 17 ( 1980) 833.
42 Stratakis C A & Rennert 0 M. Congen ital adrcnal hypcrpl asia: Moiccular genelics and alternative approaehe, to trcatmcnt. Cril Rev Ciill Lob Sci , 36 ( 1999) 329.
43 Gotoh H. Kusakabe M. Shiroshi T el 0 1. Survival of steroid 21-hydroxylase defic ient lIlice without cndogenous cort icosteroids artcr neonatal treatmcnt and genetic rcseue by transgencsis as a model systcm for treatment or congenital adrcnal hyperplasia in humans. EI/{Iouillulogv, 13 ( 1994) 1470.













![ElevatedEvolutionaryRatesamongFunctionallyDiverged ...downloads.hindawi.com/journals/ijeb/2011/274975.pdf · vertebrate genitalia [3]. Both Darwin and Eberhard explain this higher](https://img.pdfslide.net/doc/110x75/5fb951a42cfc9c0d1c1a37bc/elevatedevolutionaryratesamongfunctionallydiverged-vertebrate-genitalia-3.jpg)













