Embed Size (px)
Citation preview

CONGENITAL DEFECTS OF THE SKULL AND SCALP
By B. McC. O'BRIEN, B.Sc., M.S., F.R.C.S., and JEAN E. DRAKE, M.B., B.S., D.C.H.
Odswck Hospital, Salisbury
THIS condition has received little attention in this country. Eight previous cases of congenital skull and scalp defects have been reported by Campbell (I826), Priestley (I859), Greig (I93I), Yudkin (x947, I948), and Savage (i956). However, in the Continental and American literature more cases have been described, and altogether there have been I52 reported cases.
Campbell (I826) was the first writer to describe these lesions. His first case was an infant born with a deficiency of the skull and scalp over the bregma who died as a result of hmmorrhage from the superior sagittal sinus on the eighth day. Three years later a female infant from the same family presented with a similar defect 2 cm. long in the mid-occipital region. This defect healed over by the age of 3 months but the child died from hydrocephalus at 8 months.
Billard (I828) followed with a case of a skin defect in the left parietal region. Kehrer (IgIO) reviewed thirty-two previous cases and added two of his own. He listed twenty-two writers contributing to these cases. Then followed publications by Bonnaire and Durante (I913) , Abt (I917), and Heidler (I924) , who reviewed forty-two previous cases. Terruhn (I93O) mentions seventy-six cases and twenty-nine cases of skin defects elsewhere. Ingalls (I933) had the published series of sixty cases examined personally ; many of these were embryos or stillborn. Kehrer (I9IO) mentions fourteen cases published by Fredericks in I889.
We present five further examples of these lesions, seen in a two-year period, from patients referred to the Plastic Unit. These defects probably occur more frequently than one would gather from the literature. It is likely that small lesions have been noticed but not reported. Savage (I956) comments that he has seen a number of newborn infants with punched-out scalp ulcers, 0" 5 cm. in diameter, covered with a thin glistening membrane, which have healed in four days after birth. A bony defect is not always present.
CASE REPORTS
Case i.--Male infant, the first child in the family, was born with two defects in the skull and scalp (I.5 and o. 5 cm. in diameter) approximating one another in the midline of the vertex. Each defect had a punched-out appearance, was circular and the floor was formed by a transparent glistening membrane overlying the dura.
The pregnancy was normal and there was no relevant family history. The Wassermann reaction was negative. The skin had fully healed over at four weeks. The bony defect in the region of the posterior fontanelle (confirmed by X-ray) had closed by the age of 3 months. Two atrophic scars remained together with a small exostosis of the skull underneath. These scars were excised when the child was 3 years old.
Case 2.--Female infant, first-born, with two circular defects of skull and scalp at the vertex, each 2 era, in diameter and again covered with a fine glistening membrane;
$o~

CONGENITAL DEFECTS OF THE SKULL AND SCALP IO 3
In addition the infant had a superficial hmmangioma (o'5 cm. diameter) over the left upper arm.
The obstetric and family histories were normal. The Wassermann reaction was negative. An X-ray of the mother's pelvis in the puerperium showed no abnormality, but an X-ray of the infant's skull showed a widening of the posterior fontanelle at the site of the defects.
The skin cover was complete at 2 months, the bony defect closing at 6 months. At the age of 2 years the child had two bald areas at the vertex with a small tuft of hair in the middle of the larger one ; a small exostosis was present.
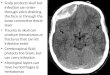
FIG. I
SkuU X-ray of Case 3 (anteroposterior).
A second child was born two years after this child but he showed no abnormalities other than a mild ear deformity.
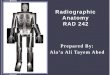
Case 3.--Female infant, first-born, with one very large scalp and skull defect 6"5 cm. in diameter at the vertex. The bony defect was easily palpable in the region of the posterior fontanelle and was well shown in the X-rays (Figs. r and 2). In addition, the infant had a cleft palate and was later found to be a spastic and an epileptic. The mother had toxmmia of pregnancy but there was no relevant family history. The Wassermann reaction was negative.
Examination of the child at 6 months showed a residual granulating area 2 cm. in diameter. A considerable part of her life was spent in hospital because of recurrent broncho-pneumonia. She died at the age of 6 months. Autopsy revealed broncho- pneumonia, congenital atelectasis of the lungs, and polycystic kidneys. The ulcer in the scalp was firmly adherent to the underlying dura~ but the rest of the skull was normal,

Xo4 BRITISH JOURNAL OF PLASTIC SURGERY-
Case 4.--Female infant, first-born, with two small circular scalp and bone defects in the superior auricular regions. These were each i cm. in diameter and covered with a glistening membrane.
The obstetric history was normal and there were no similar defects in the family. The scalp lesions healed rapidly in a few weeks. When the child was seen at the age of 6 months, bony union was complete and two brown pigmented bald patches remained.
Case 5.--This female infant was born with a single scalp and bone defect in the midline of the vertex in the region of the posterior fontanelle. The defect was circular and 2 cm. in diameter. Obstetric and family histories were normal. The rate at which healing took place was not recorded. As in the other cases, a bald area on the scalp resulted, but there was no exostosis.
FIG. 2 Skull X-ray of Case 3 (lateral).
DESCRIPTION OF DEFECTS (Tables I and II)
These five patients revealed the same characteristics in their lesions as have been described by other writers.
The defects may involve either scalp alone or scalp and skull. Vertex, occipital, and post-auricular areas are the commonest sites in that order.
Eighty per cent. are either midline or nearly midline. In one of our patients (Case 4) the defects were situated in the superior auricular region and were bilateral. According to Ingalls, 7o per cent. are single, 2o per cent. double, and 8 per cent. triple. Occasionally, more than three lesions are encountered as Ingalls (I933) and Yudkin (I947) both reported a case with four scalp defects,

C O N G E N I T A L D E F E C T S O F T H E S K U L L A N D S C A L P 10 5
These defects are found more commonly in females and are usually seen in the first-born.
In our cases there were three double lesions and two single ones, occurring in four female infants and one male of whom four were definitely known to be first-born.
The size of the defects is variable. The smallest that we encountered was 0'5 cm. in diameter and the largest 6"5 cm. in diameter. Heidler (1924) reported a lesion of 9 cm. in diameter.
TABLE I
Site
N u m b e r Size
Type . Shape Sex
D e p t h o f Defect
Case I .
Vertex midline
2
(a) I "5 c m . diam. (b) o '5 c m . d i a m .
Membranous Circular
Male first-born
Case 2.
Vertex midline
2
(a) I "5 c m . × 3 cm. (b) 2 c m . diam.
Membranous Circular Female
first-born
C a s e 3.
Vertex midline
I
6 '5 c m . diam.
Membranous Circular Female
first-born
S k i n + bone
Case 4.
Superior auricular bilateral
e i c m . d i a m .
each Membranous
Circular F e m a l e
first-born
S k i n + bone
Case 5.
V e r t e x midline
I e c m . diam.
Membranous Circular Female
S k i n + b o n e S k i n + b o n e S k i n + bone
TABLE II
C a s e 3. C a s e 4. C a s e 5.
F a m i l y h i s t o r y . Obstetric history Rate of healing :
(a) S k i n
(b) Bone
Complications of defect Other skin defects Final result
Case I. Case 2.
Normal Normal Normal Normal
I m o n t h 2 months
2 m o n t h s 5 months
None None None None Scar Scar
Normal Pre-eclampsia
Partly healed at 6 months
Little progress at 6 months
None None
Incomplete healing. Death
Normal Normal
3 weeks
4 months
None None Scar
Normal Normal
Not known
Not known
None None Scar
The lesions in our patients at birth presented a similar picture of circular punched-out ulcers. At the base of the ulcer the dnra could be seen covered by a transparent glistening membrane. In all our cases there were underlying bony defects corresponding in size to the scalp deficiency. The surrounding skin edge was well defined with a thin margin devoid of hairs. Anderson and N o w (1942), Calloway et al. (I946), and Savage (1956) stated that the circular type of lesion was confined to skin alone but this is not confirmed by our experience. Ingalls (1933) believed that the bony defects were present in the majority of cases. Occasionally, double lesions involving skin and bone and skin only can be seen in the one case (Yudkin, 1947). No abnormality of the meninges was observed by us and none recorded elsewhere.
The defects may occur in several forms,

106 BRITISH ]'OURNAL OF PLASTIC SURGERY
I. Membranous.--(a) Circular, the commonest; (b) linear, seen occasionally, are usually single and nearly always overlie the sagittal suture (Kehrer, 191o; Pincherle, 1938 ; Savage, 1956).
2.. Bullous (Ingalls, Yudkin).--Ingalls noticed this form in the foetus. He
Fig. 3.--Case 3, showing partial skin healing of a large defect at the age of
3 months.
Fig. 4 .--Case I at the age of 3 years showing resultant bald areas.
Fig. 5.--Case 2 at the age of 2 years showing resultant bald areas.
FIG. 3
FIG. 4 FIG. 5
considered that the bulla~ later ruptured and formed clear-cut ulcers in the newborn infant. Greig (1931) suggested that the bullous form is more likely in the stillborn and the ulcerated in those that survive.
Course of Heal ing. - - In our patients the defects covered by their thin membranes soon become true ulcers with granulating surfaces. Epithelialisation steadily occurred from the edges~ followed more slowly by underlying bone growth,

CONGENITAL DEFECTS OF THE SKULL AND SCALP IO 7
Fig. 3 illustrates a large skull and scalp deficiency where granulation has occurred and neighbouring epithelium has partly covered the area at three months. In smaller lesions skin closure is usually completed within two months ; bony union is obtained some months later. In Case 3 where the original defect was extensive (see Figs. I and 2), there was still a large gap in the skull when the child died at the age of 6 months. Savage (I956) reported one case with a longitudinal bony defect that did not close until six months. Apart from Case 3, bony defects in our patients closed spontaneously. A small exostosis remained in Cases I and 2, a feature also noticed by Pincherle (I938) in his case report. When healing was complete the patients were left with bald patches of varying sizes (Figs. 4 and 5).
HISTOLOGY
The nature of the thin membrane overlying the dura at the base of the scalp defect has been a source of speculation in the past. Bonnaire and Durante (1913) found this membrane to consist of fiat nucleated cells and came to the conclusion that it was a continuation of the pericranium. However, Kahn and Olmedo (195 o) reported that it was composed of a thin epidermis fading out to an atrophic corium. The collagen in the area was compact with relatively little adipose tissue and no sebaceous or sweat glands; some calcified hair follicles were present. No microscopic evidence of inflammation has been observed (Abt, I917).
There was no histology performed on the lesions in our patients except in Case I where the scar was excised. This histology report was " a fiat, rather thin, keratinising epidermis resting on a fibrous dermis and subcutaneous tissue in which there are no epidermal appendages, fat cells, or inflammatory cells."
COMPLICATIONS
There were no complications resulting from the defects in our patients. This, however, has not been the experience of some writers. In Campbell's first case (I826) death followed from superior sagittal sinus hssmorrhage. This occurred also with cases reported by Heidler (i924), Pincherle (I938), Peer and Van Duyn (I948). Warning hmmorrhages may precede the fatal bleeding.
There were no skin defects, other than those on the head, in our patients. Ingalls (I933) reported that they occurred elsewhere in 8 per cent. of cases and were usually multiple and extensive. He did not observe any secondary complications such as hsemorrhage or infections in these skin lesions, and healing usually occurred rapidly within a few weeks. There were no associated bony defects. Abt (I917) described a case with symmetrical defects on the knees which healed in six weeks, and he listed other sites--bridge of nose, buttocks, abdominal wall, and elbows--where they may occur.
However, skin defects are more common on the scalp than other sites, for Terruhn (i93 o) reviewed seventy-six scalp lesions and only twenty-nine elsewhere on the body.
In only one of our patients (Case 3) were other congenital abnormalities found (cleft palate, pulmonary atelectasis, polycystic kidneys), and these resulted in the death of the child. Coexistent abnormalities have been reported by Kehrer (igio), Ingalls (I933), Pincherle (i938), Kahn and Olmedo (I95O), and include hydrocephalus, meningocele, microphthalmos, syndactyly, and other limb deformities.

lO8 BRITISH JOURNAL OF PLASTIC SURGERY
MORTALITY
Most of the defects are small and heal quickly. Case 3 had a large defect, but death was not due to this lesion.
Hmmorrhage from the larger central defects is a possible cause of death. Ingalls found that the mortality in sixty cases was about 20 per cent., but this included stillbirths.
He states that most of the deaths were more or less directly referable to the lesions present on the scalp, and due to hmmorrhage or infection followed by meningitis.
z~TIOLOGY
An inherited tendency for these defects to occur has been noticed by some writers. Among these are Campbell (1826), who reported two cases in one family, and Tisserand-Perrier (I953), who found multiple defects over the vertex in three generations. This writer also quotes Goldsmith (1922) as recording sixteen cases in five generations. In none of Goldsmith's cases were the defects situated in the more common midline position.
A recessive gene was implicated by Kahn and Olmedo (I95O), whereas Tisserand-Perrier believed it to be a dominant gene. This hereditary trait exists only in a small number of recorded cases.
Earlier writers stressed the fact that amniotic adhesions were the cause of these defects, but this theory has long been discarded. Syphilis has been ruled out as syphilitic ulcers do not appear until three to four weeks after birth and spirochmtes have not been demonstrated (Anderson and Novy, 1942). The Wassermann reactions of the mothers of our patients were negative.
When first seen, the punched-out, clear-cut appearance of these defects suggests a traumatic cause, but in neither our patients nor in those of others has a difficult labour or obstetrical operation been found to be responsible.
The fact that these lesions occur over the fontanelles, sagittal sutures, or inferior angles of the parietal bones can be explained on the basis of delayed bony union at these sites. However, scalp defects, particularly without a lesion in the skull, are not so easily understood. Likewise, it is difficult to explain skin defects elsewhere which are usually unassociated with a bony deficiency, e.g., abdominal wall (Dowler, 1932 ). Abt (1917) thought that the defects were formed in the second month of foetal life before hairbuds, sebaceous or sweat glands appeared. Ingalls found thin-walled blebs in the midline of the head of several embryos as early as ten weeks. He considers that these blebs later ulcerated and produced the characteristic defect seen in the full-term infant.
Failure of closure of midline structures during development have been thought to be the cause. However, 20 per cent. of scalp defects do not lie in the midline, nor do those skin defects found elsewhere in the body.
It is now generally accepted that the growth and differentiation of the bones of the vault of the skull are dependent on the growth of the underlying brain. Snell (1958) considers that some defect in the underlying brain development was the cause of the lack of development of the skull bones and that the brain malformation may take the form of a local overgrowth of the walls of the neural tube. This abnormality in the formation of the underlying brain could be connected with the failure of the development of the overlying skin as both are formed from the neighbouring ectoderm (Snell).

CONGENITAL DEFECTS OF THE SKULL AND SCALP 109
The multiplicity of these lesions, the occasional familial occurrence, the absence of trauma and inflammation, and the presence of other congenital abnormalities all point to a developmental origin, but the cause of the real- development remains obscure.
TREATMENT
In the newborn the management of these cases is conservative and consists in covering the defect by a protective dressing and avoiding secondary infection. Later, when scars have been formed, these may be excised. This was done in Case I, and excision will follow shortly in Cases 2 and 4. This excision may be com- plete or undertaken in stages. For still larger scars rotation flaps may be necessary.
The necessity for operation on the large lesions overlying the superior sagittal sinus has been stressed (Peer and Van Duyn, 1948). In Kahn and Olmedo's case no bony defect was present, but large venous sinusoids were present beneath the membranous cover and they advise early skin cover by flaps sometimes preceded by ligation of the superior sagittal sinus (Peer and Van Duyn). The latter two writers have suggested that if the lesion is more than I to 2 cm. in width and lies over a suture line, it may become necrotic and they recommend early skin cover to prevent this. In the larger lesions the bony defect does not close spontaneously and grafting with bone or cartilage is necessary at a later stage to provide adequate protection for the brain.
SUMMARY
Five cases of congenital defects of the skull and scalp are presented. The main features, life history, and treatment of these deficiencies are described. The historical aspect of the subject is reviewed and the mtiology is discussed.
We wish to thank Mr J. E. Laing for permission to publish these cases and Jbr his helpful advice ; and Dr G. Ormiston, Dr N. R. Butler, and Dr L. Firman Edwards for referring Cases I, 2 and 3 respectively. Mr R. Conroy has been responsible for most of the photography.
REFERENCES
ABT, I. (1917). Amer. J. Dis. Child., 14, 113. ANDERSON, N. P., and NovY, F. G. (1942). Arch. Derm. Syph., N . Y . , 46, 251. BILLARD (I828). Quoted by Kehrer (191o). BONNAIRE, E., and DURANTE, G. (I913). Pr. todd., 21, 185. CALLOWAY, J. L., NOOJIN, R. O., RILEY, K. A., and KUHN, B. H. (1946). J. Pedlar.,
28, 2I 4. CAMPBELL, W. (1826). Edinb. J. reed. Sci., 2, 82. DOWLER, V. B. (I932). Amer. ~. Dis. Child., 44, I279. FREDERICKS (1889). Quoted by Kehrer (191o). GOLDSMITH (I922). Quoted by Tisserand-Perrier (I953). GREIG, D. M. (I931). Edinb. reed. J., 38, 341. HEIDLER, H. (I924). Wien. klin. Wschr., 37, II4. INGALLS, N. W. (I933). Amer. J. Obstet. Gynec., 25, 861. KAHN, E. A., and OLMEDO, L. (195o). Plast. reconstr. Surg., 6, 435. KEHRER, E. (I9IO). Mschr. Geburtsh. Gyndk., 3 r, 183. PEER, L. A., and VAN DUYN, J. (1948). Plast. reconstr. Surg., 3, 722. PINCHERLE, B. (I938). Arch. Mdd. Enf., 4I, 96. PRIESTLEY (I859). Trans. Obstet. Soc. Lond., I, 60. SAVA6E~ D. (I956). J. Obstet. Gynaec., Brit. Emp., 63, 351. SNELL, R. S. (I958). Personal communication. TERRUHN, E. (I93O). Arch. Gyndk., 40, 428. TISSERAND-PERRIER, M. (I953). Bull. Soc. frang. Derm. Syph., 60, 77. YUDKIN, S. (1947). Proc. R. Soc. Med., 40, 533.
(I948). Arch. Dis. Childh., 23, 6I.