Embed Size (px)
Citation preview
DEVELOPMENTAL DYSPLASIA OF THE HIP
By UDENNAKA EMMANUEL IKECHUKWU (IPT)PEDIATRICS UNITPHYSIOTHERAPY DEPARTMENTUNIVERSITY OF CALABAR TEACHING HOSPITAL, CALABAR
OUTLINEINTRODUCTIONANATOMY OF THE HIP JOINT EPIDEMIOLOGYRISK FACTORSPATHOPHYSIOLOGYCLINICAL FEATURESDIAGNOSISMANAGEMENTCOMPLICATIONSCONCLUSION
INTRODUCTION• Developmental dysplasia of the hip (DDH) is a spectrum of
disorders of development of the hip that present in different forms at different ages
• It is used to refer to patients who were born with dislocation or instability of the hip, which may result in hip dysplasia.
• The condition may occur at any time, from conception to skeletal maturity.
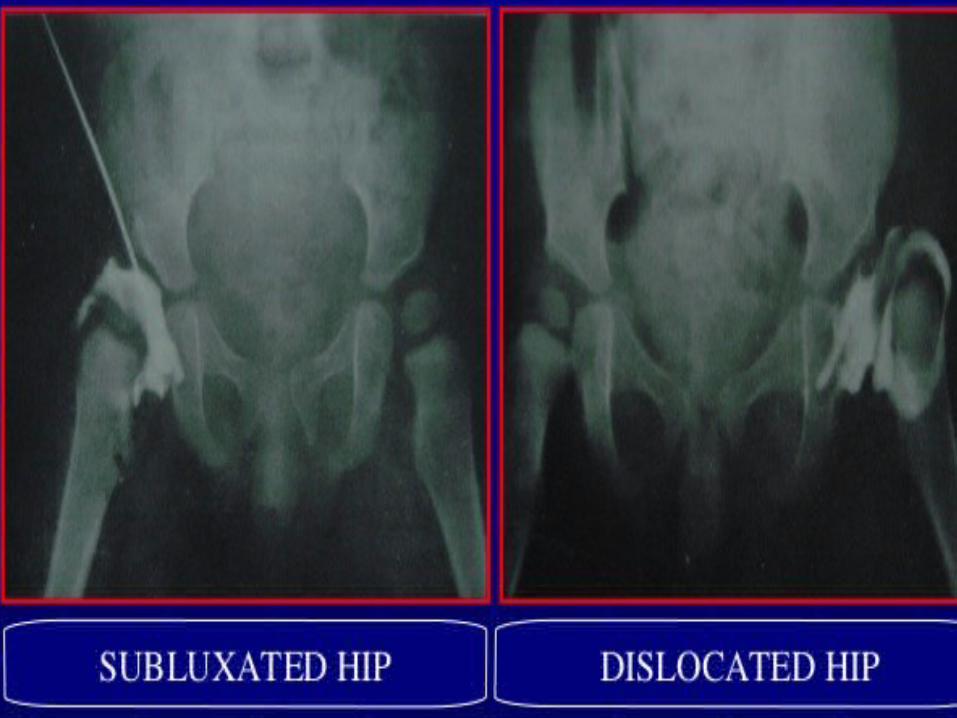
• Females are affected 7 times more• More specifically a group of terms are used to describe the
condition: Subluxation, Dislocation, Instability, Teratologic Dislocation.
• It is not restricted to congenital abnormalities of the hip, and includes some hips that were normal at birth and subsequently became abnormal.
ANATOMY OF THE HIP JOINT • One of the most stable joints in the body .• Hip joint is a multi axial ball and socket synovial joint designed
for stability and weight bearing.• Movements at the joint include flexion, extension, abduction,
adduction , medial and lateral rotation and circumduction.
ARTICULAR SURFACES:• Head of femur articulates with acetabulum of hip bone to
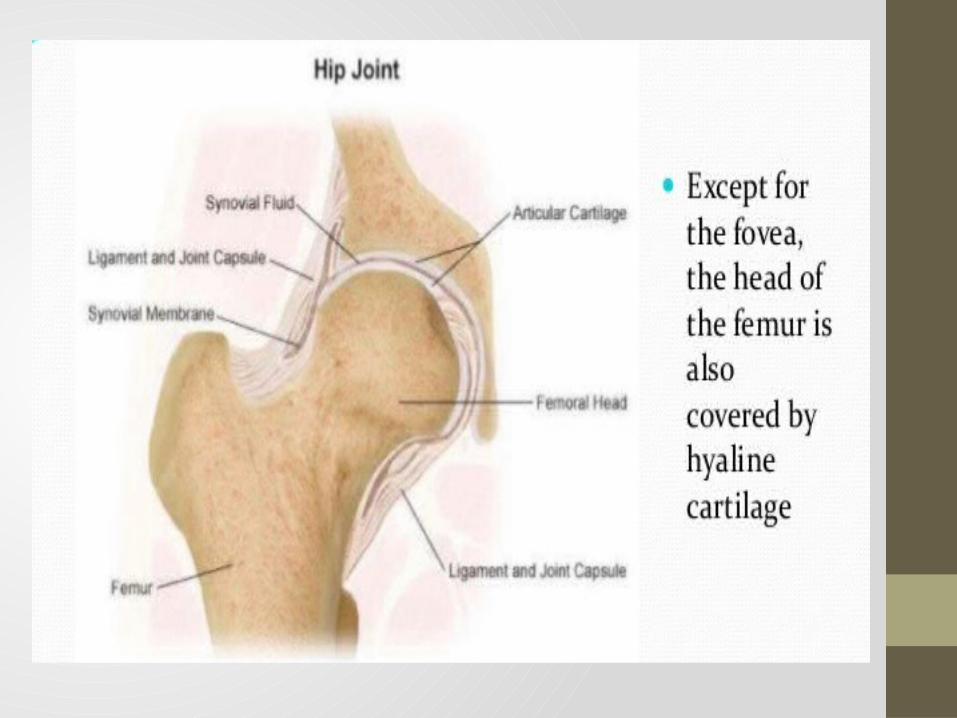
form hip joint.• Head of femur- more than half of a sphere, covered with a
hyaline cartilage• Acetabulum- lunate shape with a notch & fossa
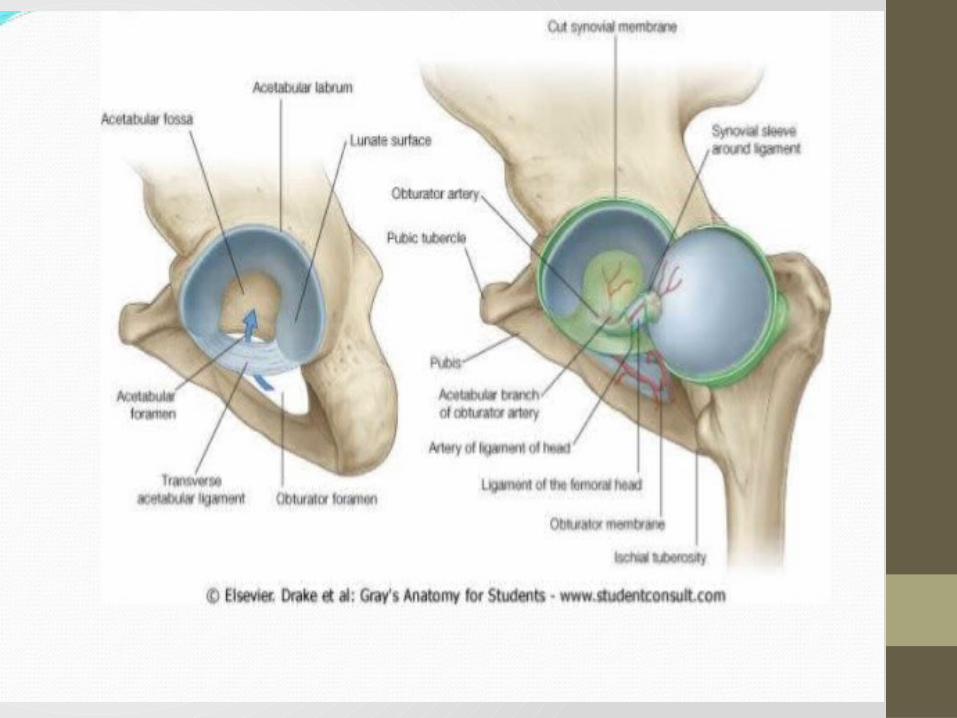
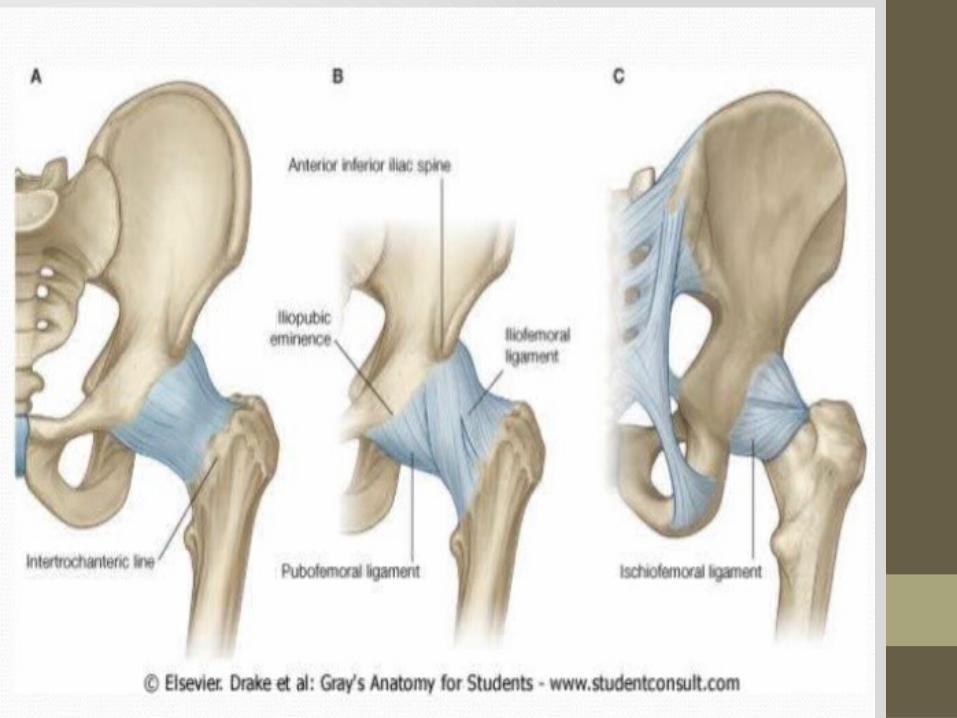
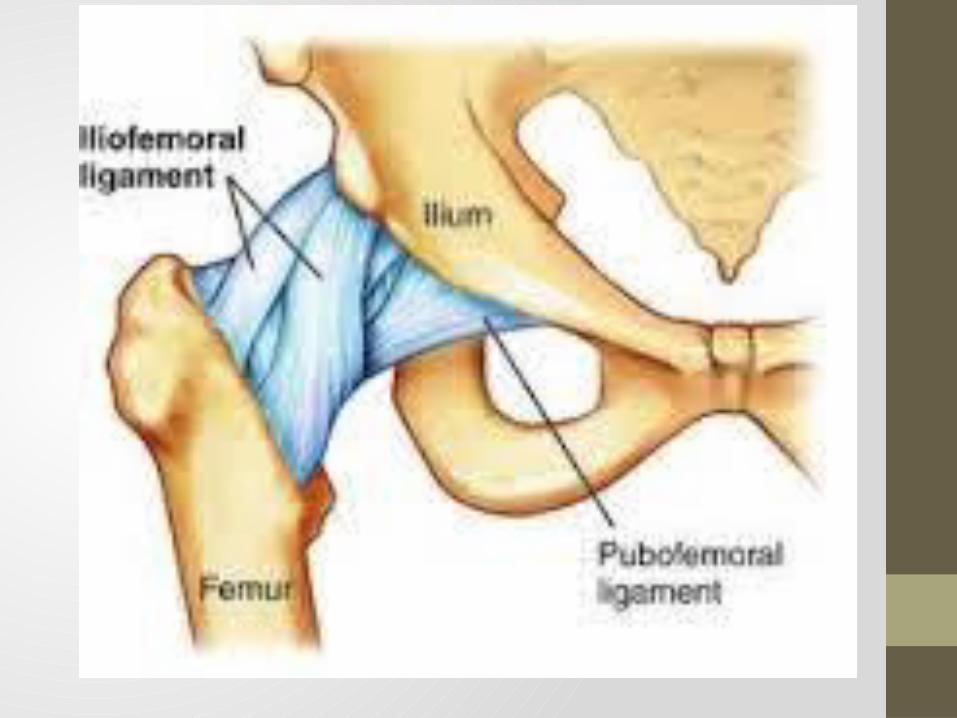
LIGAMENTS OF THE HIP JOINTEXTRASCAPULAR:• Iliofemoral• Pubofemoral• IschiofemoralINTRASCAPULAR• Ligamentum teres• Transverse ligament of the acetabulum.
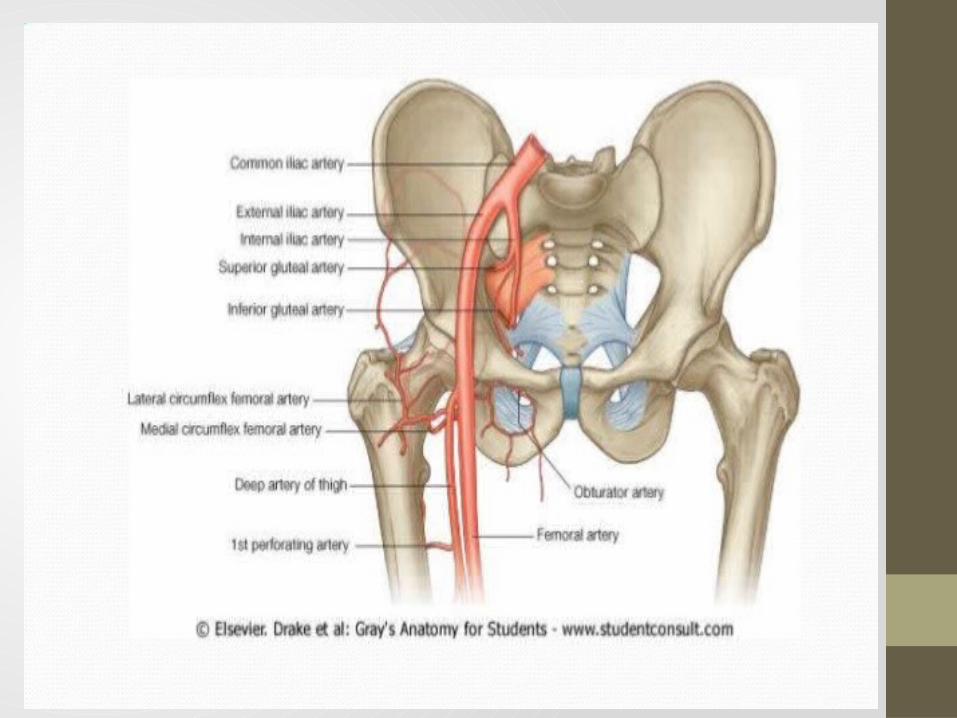
BLOOD SUPPLY • Two circumflex femoral arteries (medial and lateral)• They anastomoses at the base of the femoral neck to form a
ring, from which smaller arteries arise to the supply the joint itself.
• Foveal artery ( branch of the obturator artery)
NERVE SUPPLY• Femoral nerve• Obturator nerve• Nerve to quadratus femoris• Superior gluteal nerve
Movement and muscles• Flexion: Iliosoas, rectus femoris, Sartorius• Extension: Gluteus Maximus,
semimembranous,semitendinosus and biceps femoris• Abduction: Gluteus medius, gluteus minimus and the deep
gluteals (piriformis, gemelli etc.)• Adduction: Adductors longus, brevis and magnus,pectineus
and gracillis• Lateral rotation: Biceps femoris, gluteus Maximus, and the
deep gluteals (piriformis, gemelli etc.)• Medial rotation: Gluteus medius and minimus,
semitendinosus and semimembranosus
Embryonic dev.• 4-6weeks – the hip joint develops from the cartilaginous
anlage• 7-8th week – acetabulum and head of femur are formed from
the same primitive mesenchymal cells• 11th week - complete development of the hip• At late gestation, femoral head grows more rapidly than the
acetabular cartilage.• At birth, acetabulum is at its most shallow and most lax in
order to maximize hip ROM which facilitates delivery process• After several weeks, acetabular cartilage develops faster than
the femoral head, which allows progressively more coverage.
EPIDEMIOLOGY• The overall frequency of developmental dysplasia of the hip
(DDH) is usually reported as approximately 1 case per 1000 individuals, though Barlow believed that the incidence of hip instability during newborn examination was as high as 1 case per 60 newborns. According to the study more than 60% newborns with instability became stable by the age of 1week and 88% became stable by age 2 months leaving only 12% with residual hip instability.
• An estimated 80% of persons with DDH are female and the rate of breech positioning in children with DDH is approximately 20% ( compared to 2-4% in normal positioning) the prevalence of DDH in females born in breech position has been estimated to be as high as 1 case in 15 person in studies.
EPIDEMIOLOGY CONTD.• In native American's and Laplanders, the prevalence of
prevalence of hip dysplasia is much higher (nearly 25-50 cases per 1000 persons) than in other races, the prevalence is very low in southern Chinese and black populations. An underlying genetic disposition also appears to exist, in that the frequency of hip dysplasia is 10 times higher in children whose parents had developmental dysplasia of hip (DDH) than in those whose parents did not.
• The left hip is more affected than the right, bilateral involvement in 1 in 5 cases.
RISK FACTORS• GENETIC: hereditary predisposition, generalized joint laxity
and shallow acetabula• HORMONAL: common in females, maternal relaxin, high
estrogen and progesterone aggravate laxity• INTRAUTERINE MALPOSITION: breech position or
oligohydramnios favor‘s dislocation • First born child (primigravida)
PATHOPHYSIOLOGY • Dislocated at birth (classic DDH) or dislocation after birth
(underlying laxity)• Femoral head is dislocated upwards and laterally, epiphysis is
small and ossifies late.• Femoral neck is excessively anteverted• Acetabulum shallow,• Labrum may be folded into the cavity• Capsule is stretched, hip muscles undergo adaptive
shortening.
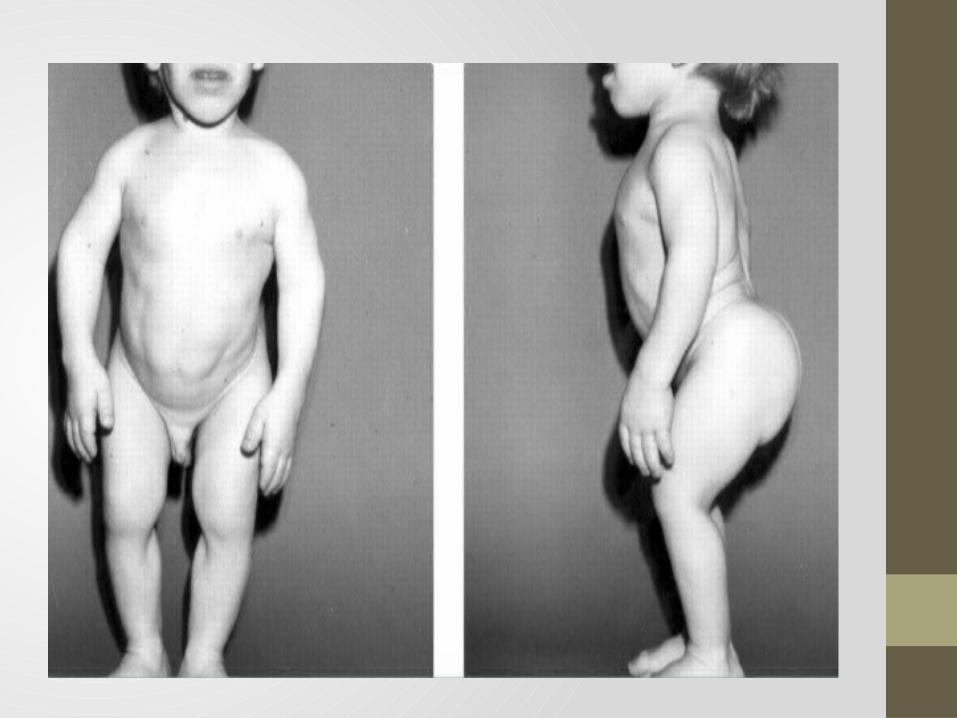
CLINICAL FEATURES• Detected at birth or soon after child starts walkingBirth – routine screening or suggestive signs in every newborns especially those at high riskEarly childhood – asymmetry of groin fold, click, limitation of movementOlder child – peculiar gait, no pain• Limitation of hip abduction, limb short and externally rotated• High buttock fold, asymmetric thigh fold, lordosis of lumbar
spine
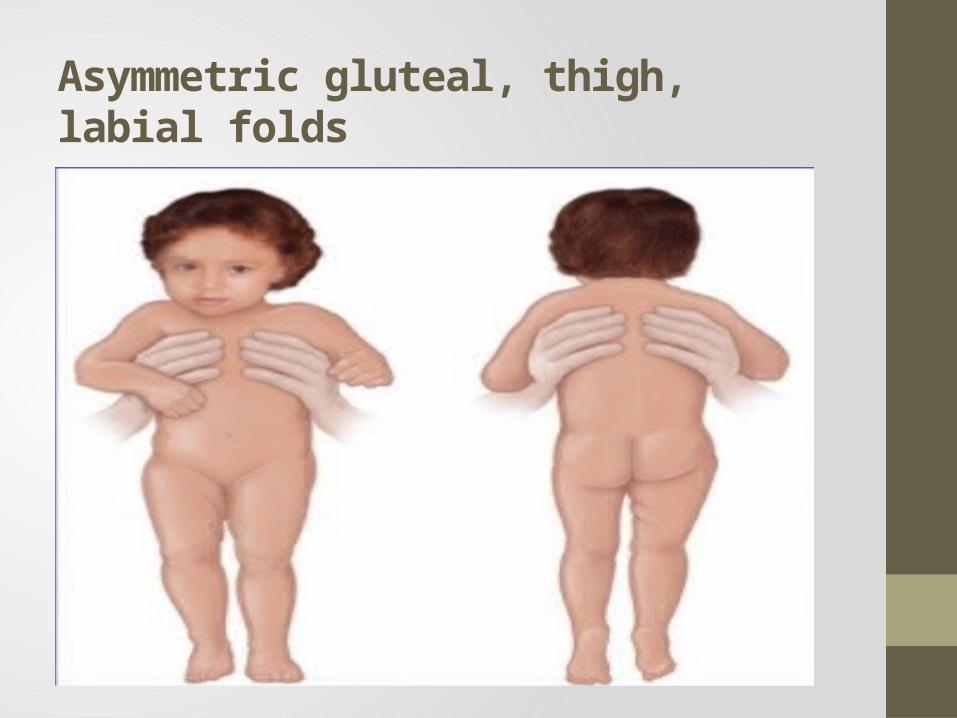
Asymmetric gluteal, thigh, labial folds
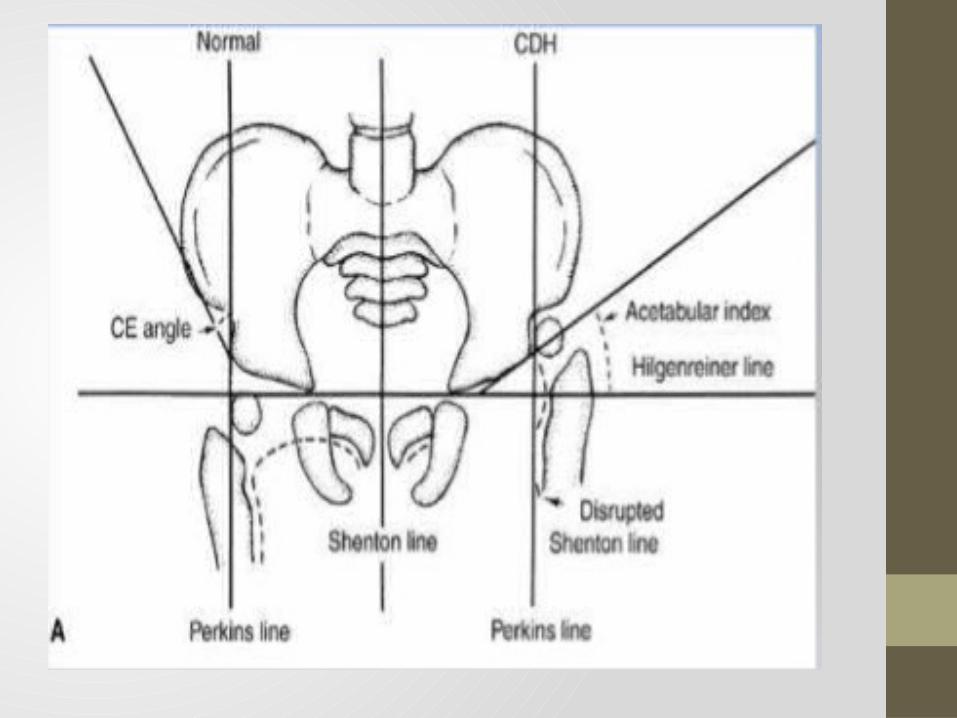
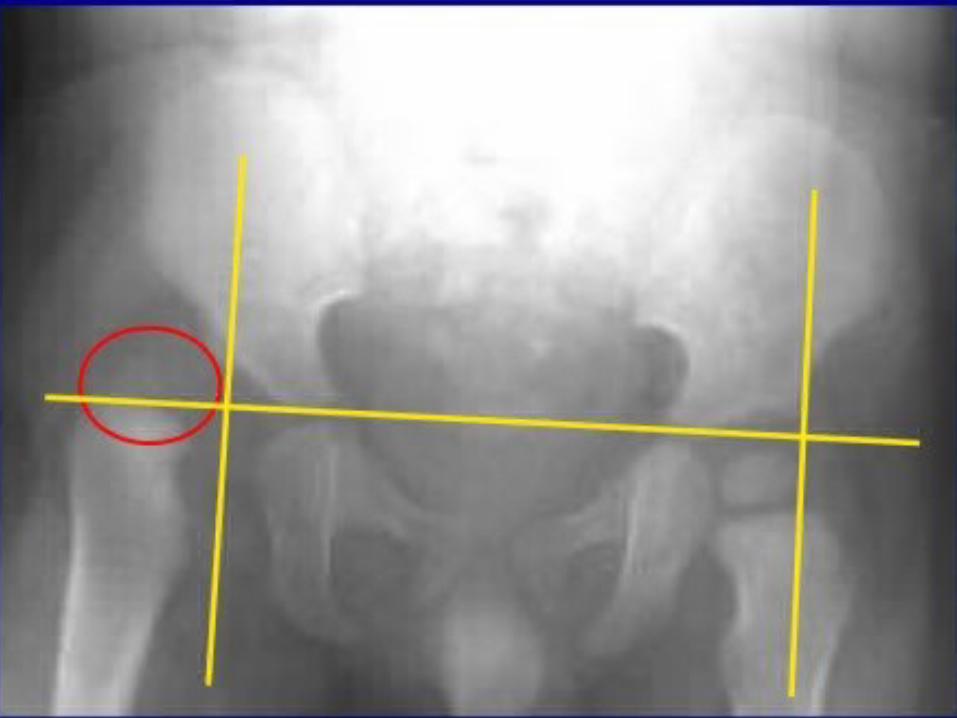
DIAGNOSIS• Clinical tests• Natural history• Radiological images
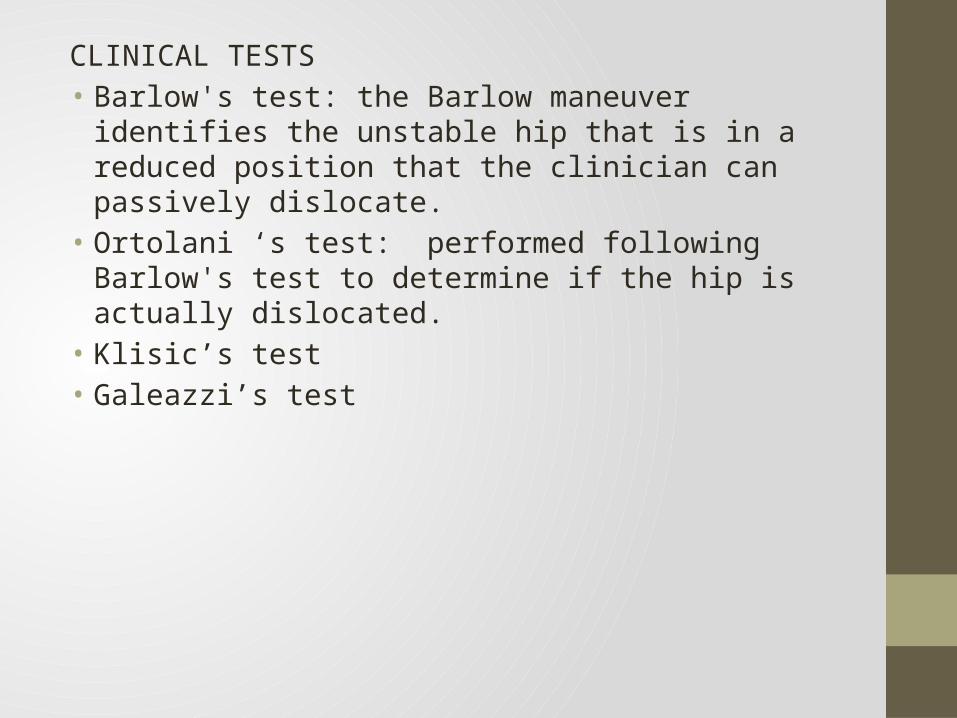
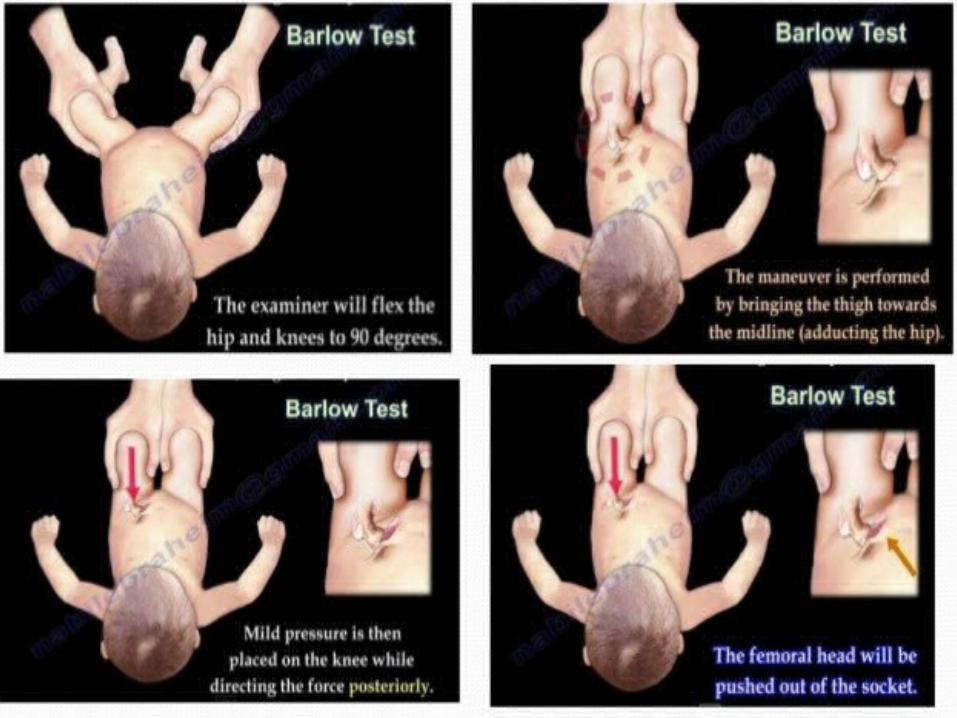
CLINICAL TESTS • Barlow's test: the Barlow maneuver identifies the unstable hip
that is in a reduced position that the clinician can passively dislocate.
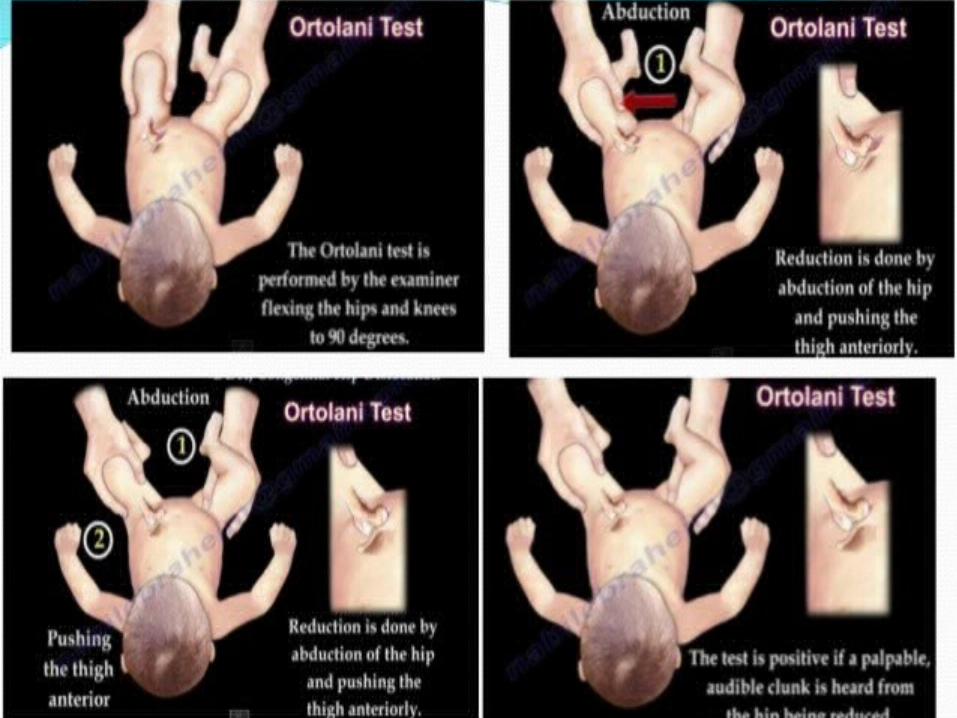
• Ortolani ‘s test: performed following Barlow's test to determine if the hip is actually dislocated.
• Klisic’s test• Galeazzi’s test
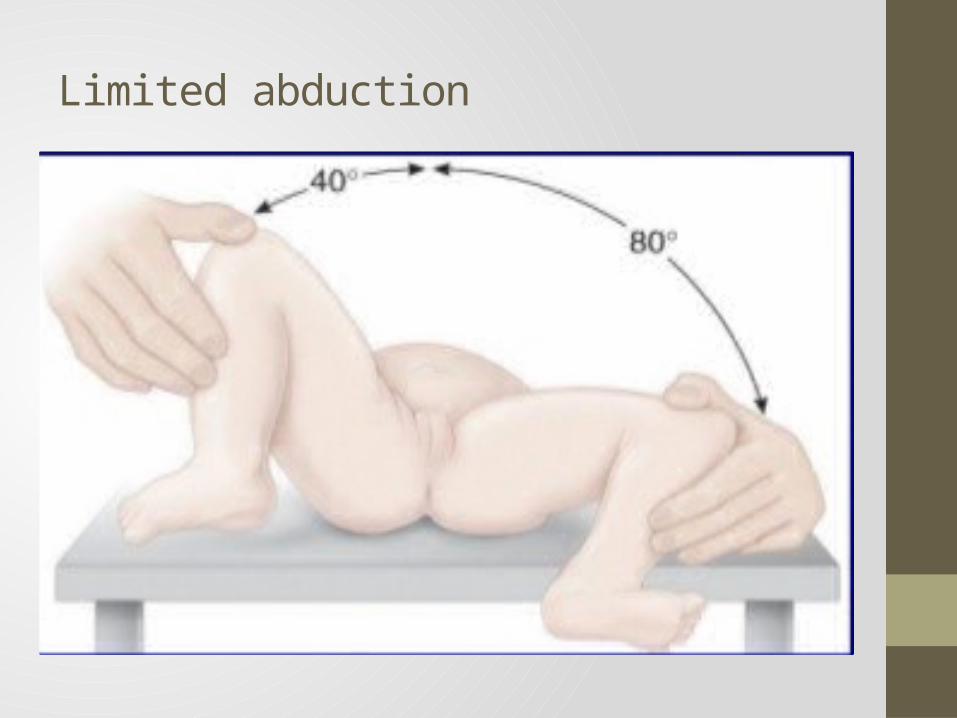
Limited abduction

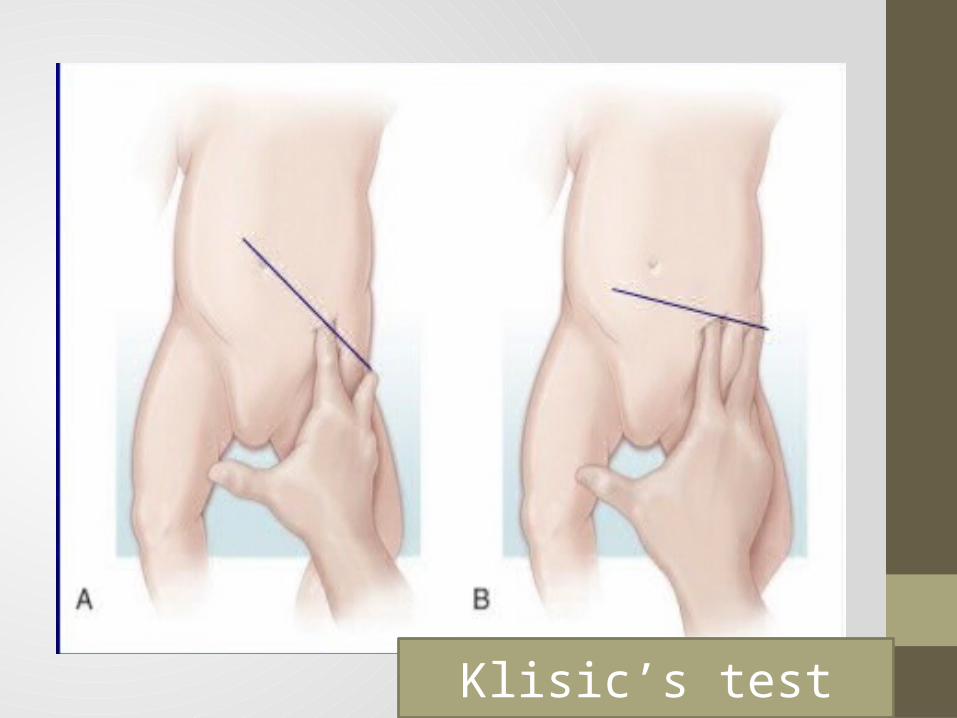
Klisic’s test
Radiological imaging• Ultrasound• MRI• CT• X-rays
DIFFERENTIAL DIAGNOSIS
• Proximal femoral focal deficiency • Fracture of the femoral neck• Coxa vara
MANAGEMENT • Aim is to achieve reduction of the head into the acetabulum
and maintain it until the hip becomes clinically stable and a round acetabulum covers the head.
• Most cases closed reduction is possible, else open reduction is done.
Birth to 6months:
Where facilities for ultrasound scanning are available, all new born infants at risk are examined by ultrasonography.
• If hip is reduced and has a normal cartilaginous outline, no treatment is required, observe for 3-6m
• If acetabular dysplasia or hip instability, the hip is splinted in a position of flexion and abduction and ultrasonography done at intervals to monitor the hip.
• If ultrasound is not available the infants are nursed in double napkins or an abduction pillow for the first 6 weeks and observe for first 6m for development of acetabular roof.
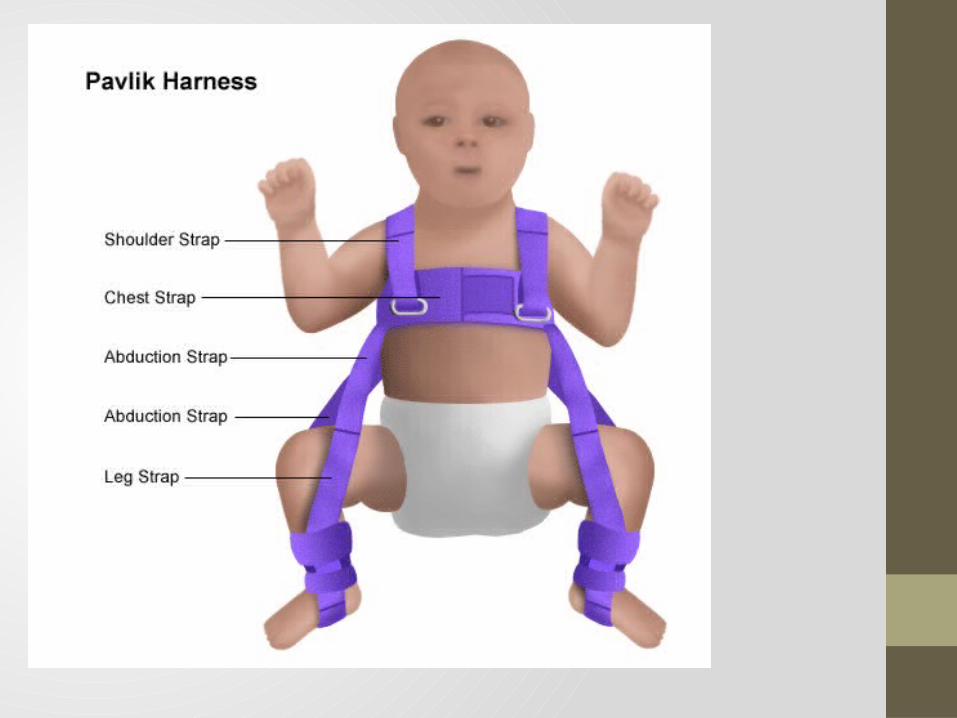
Splintage • The objective of splintage is to hold the hips somewhat flexed,
abducted and to maintain reduction.• Von Rosen's splint is a H-shaped splint• The Pavlik harness is more difficult to apply but gives the child
more freedom while still maintaining position.

Persistent dislocation: 6-18months• The hip must be reduced, preferably by closed methods but if
necessary by operation , and held reduced until acetabular development is satisfactory.
• Closed reduction: suitable after 3m and is performed with an arthrogram to confirm a concentric reduction.
• Failure to achieve concentric reduction should lead to abandoning this method in favor of an operative approach at approximately 1 year of age.
Splintage • Held in a plaster Spica at 60 degrees of flexion, 40 degrees of
abduction and 20 degrees of internal rotation.• After 6 weeks the Spica is changed and stability assessed • If satisfactory, Spica retained for 6weeks, then abduction splint
for 6months• If concentric reduction is not achieved, open reduction is
done.

Persistent dislocation from 18m to 4yrs:• In older children, arthrography and open reduction preferred
over closed reduction.• Traction – to loosen the tissues and bring the femoral had
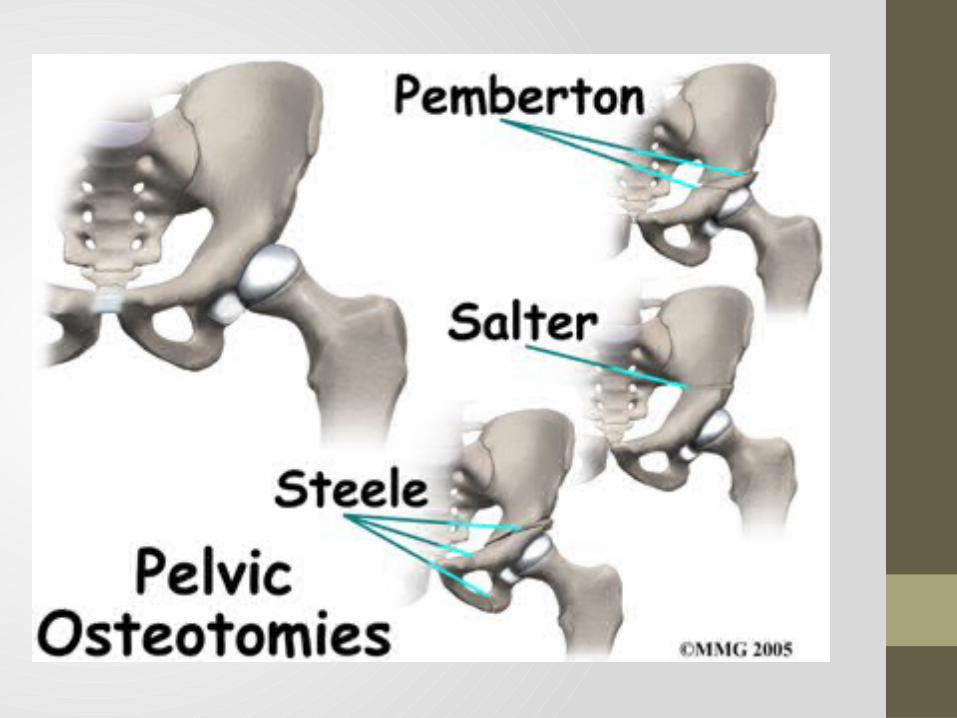
down opposite the acetabulum.• Acetabular reconstruction procedures are done • pericapsular reconstruction of the acetabular roof
(pembertons’s operation) or an innominate (salter) osteotomy
SPLINTAGE • After operation, the hip is held in a plaster Spica for 3 months
and then left unsupported
Dislocation in children >4 yrs.• Unilateral dislocation in children over 4yrs often leaves the
child with a mobile hip and little pain. though the child must accept the fact that his/her gait will be distinctly abnormal
• Bilateral dislocation leaves the child with a waddling gait which is symmetrical and therefore not so noticeable
• Avoid operation unless the hip is painful or deformity unusually severe.
Persistent dislocation in adults – if disability is severe enough total joint replacement is done.
Complications
The complications can arise if untreated or those that arise after treatment• A persistent limp on the affected side• A premature osteoarthritis of the hip which may require a
total hip replacement• Lower back or hip pain• Limb length discrepancy• Recurrent subluxation/dislocation• Failed reduction• Avascular necrosis
Conclusion • The left hip is dislocated more often than the right and 20% of
cases are bilateral.• normal occurrence of hip shallowness and capsular laxity in
the neonatal period are initial factors factors involved in DDH• It is more common in cultures that use swaddling of babies,
forcing the hips into extension and adduction• Affects females more than males.• The most reliable sign is limited abduction• CT is more helpful for pre operative evaluation in older
children or to document reduction, MRI is helpful for difficult cases and treatment complications.
Thanks for listening…