Embed Size (px)
Citation preview
Connected Language in Early Mild Cognitive Impairment
by
Kimberly Diggle Mueller
A dissertation submitted in partial fulfillment of
the requirements for the degree of
Doctor of Philosophy
(Communication Sciences and Disorders)
at the
UNIVERSITY OF WISCONSIN-MADISON
2017
Date of final oral examination: 5/12/2017
This dissertation is approved by the following members of the Final Oral Committee:
Lyn S. Turkstra, Professor, Communication Sciences and Disorders
Cynthia Fowler, Professor, Communication Sciences and Disorders
Michelle R. Ciucci, Associate Professor, Communication Sciences and Disorders
Margarita Kaushanskaya, Professor, Communication Sciences and Disorders
Bruce P. Hermann, Professor, Neurology
Sterling C. Johnson, Professor, Medicine
Rebecca L. Koscik, Senior Scientist, Wisconsin Alzheimer’s Institute

i
Table of Contents
Dedication ....................................................................................................................................... ii
Acknowledgements ........................................................................................................................ iii
Abstract .......................................................................................................................................... vi
Chapter 1
Introduction ......................................................................................................................................1
Chapter 2
Manuscript 1: Review of Picture Description Tasks ....................................................................11
Chapter 3
Manuscript 2: Connected Language in Late Middle-Aged Adults at Risk for Alzheimer’s
Disease, a cross-sectional study .....................................................................................................67
Chapter 4
Manuscript 3: The Latent Structure and Test-Retest Stability of Connected Language Measures
in the Wisconsin Registry for Alzheimer’s Prevention .................................................................98
Chapter 5
Manuscript 4: A Longitudinal Study of Connected Language in Preclinical
Mild Cognitive Impairment .........................................................................................................132
Chapter 6
Conclusion and Future Directions ...............................................................................................163
References ...................................................................................................................................172
Appendix 1
Reasons to Participate in Alzheimer’s Research: Varying Perspectives of Participants
from The Wisconsin Registry for Alzheimer’s Prevention .........................................................189
Appendix 2
The Association Between Amyloid Burden and Language Outcomes in the
Wisconsin Registry for Alzheimer’s Prevention (WRAP) ..........................................................195
Appendix 3
Characteristics of Connected Language Subtypes in the Wisconsin Registry
for Alzheimer’s Prevention ..........................................................................................................204
ii
Dedication
To the memory of my grandmother, Rose Cababe
“Sitto”
iii
ACKNOWLEDGEMENTS
My sincere gratitude begins with Dr. Lyn S. Turkstra, whose brilliant guidance has accompanied
me on this journey since 2006. With good humor and patience, Dr. Turkstra has given me many
tools for success as a researcher, teacher and mentor. Lyn’s work with SLP students, and with
adolescents and adults with traumatic brain injury is beyond inspirational. Lyn, thank you for
your direction and advocacy for me and for all SLP students, and I know we will have much to
taco bout in the years to come.
To my mother and father, for your unconditional love and support: thank you for being
wonderful parents. To my brother Eddie, whose intelligence and focus, creative and otherwise,
has been a constant source of inspiration for me: thank you.
To Dr. Mark A. Sager, who founded the WRAP study in 2001, and who gave me encouragement
and support to accomplish this dissertation. Dr. Sager’s kind-hearted and generous spirit is a
constant source of inspiration for me: thank you, Mark, for believing in me, and for your vision
for WRAP.
To Dr. Asenath LaRue and Dr. Bruce Hermann, the designers of the WRAP neuropsychological
test battery, who took a chance and allowed me to collect speech samples from WRAP
participants since 2012. Thank you for these years of encouragement and guidance.
To Dr. Rebecca Koscik, for your unending patience and gentle guidance, you are brilliant
beyond words and I couldn’t have had a better stats guru in my corner. Thank you, Becca.
iv
To Dr. Sterling Johnson, for listening to my goals and giving me full support, mentorship, and
independence to learn. Your direction and leadership for the WRAP study is invaluable, and I
am grateful to be able to work with you.
To Dr. Cynthia Fowler, Dr. Michelle Ciucci, Dr. Margarita Kaushanskaya, and all of the
members of my committee: thank you for your support and for the time you spent to review my
work.
To Shawn Bolin, Nia Norris, Diane Wilkinson, Joanne Nordeen, Lisa Bluder and Ian Canovi, for
collecting these speech samples day in and day out. You are the unsung heroes of WRAP, you
help make this study the success that it is. To all of my WAI colleagues past and present, thank
you for supporting me and for being such wonderful co-workers and friends. To Sara Riedeman
and Kristina Fiscus, for transcribing hundreds of language samples, thank you!
To the selfless, passionate, and dedicated WRAP participants: I am grateful to you, the world
will be grateful to you, for all you give to the fight against Alzheimer’s disease. You are heroes,
and I am honored to have met many of you: thank you.
To Rosie Norman, my colleague, my partner in crime, my friend for life: I cannot imagine going
through this without you. This process has given me many gifts, but your friendship is one of the
greatest gifts of all. Thank you, Rosie.
To all of my friends and family, to Linda and Gary Simonetti, Donald Cababe, Catherine Diggle,
Mary Ann Mueller, to Cathy and Ron Rotter, Mike and Tracey Mueller, thank you for your
support and encouragement.
v
To my friend, Lisa Turso Kaufman: thank you, Lisel, for checking in, never giving up, and
always making me (and the world) laugh, you are so important to me.
To my friend, Parul Vakani, who has literally been by my side through every major milestone
since first grade: Bena, I am so grateful for you.
To my wonderful sons, Aidan and Daniel Mueller: you make me happy every day. I am (and will
always be) so proud of you and all of the great things you do. Thank you for being so patient
while I worked on this. I love you!
Finally, my deepest gratitude to my husband Tim: you quietly, lovingly supported me every step
of the way. Thank you for the hours you spent formatting and editing these pages, and for all of
the encouragement you gave me throughout this process. This would not have been possible
without you.
vi
ABSTRACT
Research evidence continues to accrue suggesting that pathological changes associated with
Alzheimer’s disease (AD) occur years or decades before the onset of cognitive and functional
symptoms. As a result, there is an urgent need for sensitive measures that can detect the earliest
functional and cognitive change. Connected language analysis, in which spoken language is
assessed within the context of discourse, is a promising tool for early diagnosis of functional
changes, because it more closely approximates everyday language use than traditional
standardized language tests and thus may be more sensitive to early changes. Although many
studies have documented changes in connected language in AD, little is known about when
language difficulties first emerge on the path to a clinical diagnosis. The goal of this work was to
investigate whether or not changes in connected language could be detected in a group of late-
middle-aged, asymptomatic adults at risk for AD. We first compared the connected language of
cognitively stable individuals to those identified as having early memory declines (“eMCI”), using
a cross-sectional, matched-pairs design. Results showed that the eMCI group produced less
informative language than the cognitively stable group. Next, we characterized the psychometric
properties of connected language measures. We identified four factors of connected language in a
group of cognitively stable adults: semantic, lexical, syntax, and fluency. These factors were
invariant across sex and parental history of AD, and stable at two time points. Finally, we used the
confirmed factor structure to evaluate connected language across two time points. We found that
adults with eMCI declined more rapidly in semantic and fluency measures than adults who were
cognitively stable. We also found that change in fluency and semantics, and lower baseline syntax
predicted eMCI diagnosis at the second visit. This work provides evidence that changes in
everyday language may be detected at very early preclinical stages of cognitive decline. Connected
vii
speech and language may be a useful performance-based tool for assessing and monitoring early
functional declines.
Keywords: Connected Language, Discourse, Connected Speech, Alzheimer’s disease, Mild
Cognitive Impairment, Preclinical Alzheimer’s disease, Language, Picture Description,
Longitudinal
1
CHAPTER 1
Introduction
2
INTRODUCTION AND SPECIFIC AIMS
Alzheimer’s disease (AD) is the leading cause of dementia in older adults, and is
currently the sixth leading cause of death in the United States (Xu, Murphy, Kochanek, & Arias,
2016). Unless interventions are developed to cure or prevent AD, the number of people
diagnosed with the disease could rise to 16 million by 2050, costing the nation up to $1.1 trillion
annually. Consequently, efforts are underway to identify methods to detect the earliest point at
which AD processes begin (i.e., the Mild Cognitive Impairment (MCI) stage or before) in order
to develop and test therapeutic interventions to prevent or slow disease progression. Although
major advances have been made in the early detection of pathological markers of AD (i.e.,
accumulation of beta-amyloid (Aβ) and neurofibrillary tangles) (Jack et al., 2013), there is still
an urgent need for sensitive measures that detect subtle declines in both cognition and activities
of daily living (ADL) (Snyder et al., 2014). While much of this effort has been directed toward
episodic memory declines, the hallmark cognitive symptom of AD, there has also been a steady
increase in research on speech and language changes in clinical AD. There is evidence
suggesting that language deterioration begins early in the AD trajectory, possibly decades before
the clinical presentation of dementia, and that such deterioration is evident in spoken language
(also referred to as “connected language,” “connected speech,” or “discourse”) (Cuetos, F.,
Arango-Lasprilla, J.C., Uribe, C. Valencia, & F. Lopera, 2007; Garrard, Maloney, Hodges, &
Patterson, 2005; Snowdon et al., 1996).
Discourse analysis is a compelling area of study for early detection and disease
monitoring for several reasons. First, word retrieval difficulties in conversation are one of the
first subjective complaints in MCI and AD. Word-finding problems are also common in normal
aging, but they are almost always temporary and are thought to be due to difficulty retrieving
3
phonological information, which has been associated with age-related atrophy of the left insula
of the brain (Shafto, Burke, Stamatakis, Tam, & Tyler, 2007). In the case of MCI, however,
word-retrieval problems are more frequent and severe, and are thought to be due to problems
with semantic memory. Specifically, during the preclinical phase of AD (Braak Stage 1),
neurofibrillary tangles begin in the mediotemporal complex, including the perirhinal and
entorhinal cortices, which are part of the language network involved in semantic memory (Braak
& Braak, 1991). This leads to the second reason why examining discourse deserves attention:
declines in episodic memory are a part of normal aging and MCI and AD, whereas semantic
memory remains stable in normal aging, and some semantic abilities even improve over time
(Nilsson, 2003). Thus semantic memory declines may be an important discriminating feature
between declines of normal aging and those of MCI and AD (Venneri, Mitolo, & De Marco,
2016). A third rationale for using discourse in assessment is related to participant burden: a
speech sample is relatively quick and effortless to provide, and is an inexpensive yet rich source
of information about conversational function, working memory, executive functions, and
language (Almor, Kempler, MacDonald, Andersen, & Tyler, 1999; Coelho, Liles, & Duffy,
1995; Henry, Crawford, & Phillips, 2004), whereas typical neuropsychological tests of these
functions can take up to several hours, are labor-intensive, and often stressful for the participant.
Finally, there are cognitive-communication interventions that have been shown to be effective in
adults with MCI and early AD (Mahendra, 2001); by better understanding how and when
discourse is affected on the trajectory of AD dementia, these interventions can be improved and
tailored to specific stages of disease.
Although there is substantial evidence for discourse changes in mild to severe stages of
AD, little is known about discourse in the preclinical phase. The goal of the work presented here
4
was to determine if discourse problems present concurrently with very early memory declines,
and to characterize discourse longitudinally, prior to the possible onset of clinical impairment.
The language samples are drawn from late-middle-age adults enrolled in the Wisconsin Registry
for Alzheimer’s Prevention (WRAP), a longitudinal study that was designed to identify
biological and lifestyle risk factors associated with cognitive decline due to AD.
The first step in the research process was to complete an extensive review of the literature
on connected language in MCI and AD, which is presented in Chapter 2. Three major findings
arose from the review: 1) there is substantial evidence of changes in connected language in the
mild to severe stages of AD, but a dearth of knowledge about change in preclinical AD; 2) use of
the “Cookie Theft” task from the Boston Diagnostic Aphasia Examination (Goodglass & Kaplan,
1983) is ubiquitous in studies of MCI and AD; and 3) researchers have used numerous measures
to examine aspects of connected language, including several measures of content, syntax,
morphology, and pragmatics; as well as measures of speech and voice, including pitch variations,
voice onset time, and speech fluency measures. The results of the review led to the specific aims
and hypotheses for the present study, which are listed below.
SPECIFIC AIMS
Specific Aim 1: To compare discourse between adults with and without psychometric MCI
(pMCI) in a late-middle-aged cohort enriched for family history of Alzheimer’s Disease.
Hypothesis 1. Adults with pMCI will perform worse on measures of semantic content, syntax
complexity, lexical diversity, and/or discourse fluency than those who are cognitively stable.
Specific Aim 2: To characterize the psychometric properties of discourse in a late-middle-
aged cohort enriched for family history of Alzheimer’s Disease.
5
Hypothesis 2a. A latent structure of discourse, as examined through exploratory and
confirmatory factor analyses, will reveal factors that correspond to the content, syntax, and
fluency of discourse.
Hypothesis 2b. If a latent structure is confirmed, the resulting factors will be invariant across sex
and family history status.
Hypothesis 2c. Temporal stability of resulting factors will be adequate for a two-year interval.
Specific Aim 3: To compare longitudinal discourse performance of participants with
preclinical cognitive declines (pMCI) to those who are cognitively stable.
Hypothesis 3. Participants with pMCI will show steeper declines of connected language
measures over time than those who are cognitively healthy.
The results of this work will be presented in the chapters that follow. First, I provide a
glossary of terms used throughout the paper. This is intended to clarify terminologies that may
carry different meanings across disciplines (e.g., speech-language pathology vs.
neuropsychology and medicine), as well as to define terms in the Alzheimer’s disease literature
or concepts specific to the WRAP study that have evolved over time. Next, Chapter 2 presents
the review paper that serves as the background and further introduction to the study of connected
language in MCI and AD. In Chapter 3, I describe a cross-sectional study showing that
participants with early memory declines expressed less content in the picture description task
than those who were cognitively healthy. Chapter 4 details a study of exploratory and
confirmatory factor analyses and shows that we identified four latent factors of connected
language which were invariant across sex and family history status, with adequately stability
over time. In Chapter 5, I describe a longitudinal study in which we used linear mixed effects
models and showed that participants with subclinical mild cognitive impairment declined faster
6
on semantic and fluency measures of connected language than cognitively stable individuals. In
Chapter 6, I discuss the implication of the collective findings and directions for future research.
The appendices are comprised of related studies that I completed during the course of this
process.
7
DEFINITIONS
Language: In the field of Speech-Language Pathology (SLP), the term “language” is
differentiated from “speech.” In this paper, “language” refers to a synergistic system comprised
of the following individual language domains: 1) phonology, the study of the rules of the speech
sound system of a language; 2) morphology, the study of the rules that govern how morphemes
(the smallest meaningful units of language) are used; 3) syntax, the rules of how words can be
combined to form sentences; 4) semantics, the meaning of words and combinations of words;
and 5) pragmatics, the rules associated with the use of language (both verbal and nonverbal) in
conversation and social situations. Taken together, these domains form a dynamic integrative
whole referred to as “language” (Gleason, 2005).
Speech: The SLP field refers to “speech” as the articulation of speech sounds, the fluency of
speaking (rate, rhythm, sound and word repetitions), and the production and quality of voice
(pitch, loudness, resonance, duration).
Connected Language: Spoken language that is used in a continuous sequence, as in everyday
conversation. Also referred to as “connected speech,” “spontaneous speech,” “spoken language,”
and “discourse.” Although the fields of neuropsychology and linguistics frequently use the term
“connected speech” in the AD literature, it is important to make clear the distinction between
speech (fluency, articulation, voice) and language (words, units of meaning, sentence structure,
etc.), especially since researchers are increasingly investigating both in AD.
Discourse Fluency: Refers to the flow of speaking in connected language, taking into account
filled and unfilled pauses, sound-, word-, and phrase-repetitions, circumlocutions, revisions, and
false starts.
8
Verbal Fluency: Refers to a neuropsychological task in which participants are required to
generate as many words as possible from a category (either semantic or phonemic) in a given
time. In this work, I make the distinction between “verbal fluency” and “discourse fluency,” with
the latter referring to the flow of speaking in a connected language task.
Mild Cognitive Impairment (MCI): The diagnosis of MCI requires that there is concern about
cognitive decline by the person or a significant other, impairment in one or more cognitive
domains, but there is preservation of independence in activities of daily living. In the WRAP
study, a participant is diagnosed with “clinical MCI” if there is a significant decline in cognitive
performance and if the participant and/or informant report substantial concern about cognitive
change.
Psychometric MCI (pMCI): Psychometric MCI in the WRAP study was determined by
examining individual performance at each wave relative to robust internal norms. Participants
classified as having pMCI had episodic memory factor scores that were greater than 1.5 standard
deviations below the robust norms. This method was published in 2014 (Koscik et al., 2014);
Manuscript 2 (Kimberly Diggle Mueller et al., 2016) uses the “pMCI” terminology.
Early MCI (eMCI): Since the pMCI construct, WRAP researchers have further refined the
criteria for diagnosis of preclinical MCI, or “eMCI.” One of the most notable changes was the
addition of a consensus conference review process. In brief, a panel of dementia experts
(neuropsychologists, physicians, nurse practitioners) review longitudinal cognitive performance,
informant reports of cognitive and functional status, and medical and psychosocial histories in
order to identify individuals in the cohort who exhibit lower than expected objective
performance on cognitive measures (based on robust internal norms), but may not yet report
subjective decline (Koscik et al., 2016). Manuscript 4 uses the “eMCI” terminology.
9
REFERENCES
Almor, A., Kempler, D., MacDonald, M. C., Andersen, E. S., & Tyler, L. K. (1999). Why do
Alzheimer patients have difficulty with pronouns? Working memory, semantics, and
reference in comprehension and production in Alzheimer's disease. Brain Lang, 67(3),
202-227. doi:10.1006/brln.1999.2055
Braak, H., & Braak, E. (1991). Neuropathological stageing of Alzheimer-related changes. Acta
neuropathologica, 82(4), 239-259.
Coelho, C. A., Liles, B. Z., & Duffy, R. J. (1995). Impairments of discourse abilities and
executive functions in traumatically brain-injured adults. Brain injury, 9(5), 471-477.
Cuetos, F., Arango-Lasprilla, J. C., Uribe, C., Valencia, C., & Lopera, F. (2007). Linguistic
changes in verbal expression: a preclinical marker of Alzheimer's disease. J Int
Neuropsychol Soc, 13(3), 433-439. doi:10.1017/S1355617707070609
Garrard, P., Maloney, L. M., Hodges, J. R., & Patterson, K. (2005). The effects of very early
Alzheimer's disease on the characteristics of writing by a renowned author. Brain, 128(Pt
2), 250-260. doi:10.1093/brain/awh341
Gleason, J. B. (2005). THE DEVELOPMENT OF LANGUAGE, 6/e.
Goodglass, H., & Kaplan, E. (1983). Boston diagnostic aphasia examination booklet: Lea &
Febiger.
Henry, J. D., Crawford, J. R., & Phillips, L. H. (2004). Verbal fluency performance in dementia
of the Alzheimer’s type: a meta-analysis. Neuropsychologia, 42(9), 1212-1222.
Jack, C. R., Jr., Knopman, D. S., Jagust, W. J., Petersen, R. C., Weiner, M. W., Aisen, P. S., . . .
Trojanowski, J. Q. (2013). Tracking pathophysiological processes in Alzheimer's disease:
an updated hypothetical model of dynamic biomarkers. Lancet Neurol, 12(2), 207-216.
doi:10.1016/S1474-4422(12)70291-0
Koscik, R. L., Berman, S. E., Clark, L. R., Mueller, K. D., Okonkwo, O. C., Gleason, C. E., . . .
Johnson, S. C. (2016). Intraindividual Cognitive Variability in Middle Age Predicts
Cognitive Impairment 8–10 Years Later: Results from the Wisconsin Registry for
Alzheimer’s Prevention. Journal of the International Neuropsychological Society,
22(10), 1016-1025.
Koscik, R. L., La Rue, A., Jonaitis, E. M., Okonkwo, O. C., Johnson, S. C., Bendlin, B. B., . . .
Sager, M. A. (2014). Emergence of mild cognitive impairment in late middle-aged adults
in the wisconsin registry for Alzheimer's prevention. Dement Geriatr Cogn Disord, 38(1-
2), 16-30. doi:10.1159/000355682
Mahendra, N. (2001). Direct interventions for improving the performance of individuals with
Alzheimer's disease. Paper presented at the Semin Speech Lang.
Mueller, K. D., Koscik, R. L., Turkstra, L. S., Riedeman, S. K., LaRue, A., Clark, L. R., . . .
Johnson, S. C. (2016). Connected Language in Late Middle-Aged Adults at Risk for
Alzheimer’s Disease. Journal of Alzheimer's Disease(Preprint), 1-12.
Nilsson, L. G. (2003). Memory function in normal aging. Acta Neurologica Scandinavica,
107(s179), 7-13.
Shafto, M. A., Burke, D. M., Stamatakis, E. A., Tam, P. P., & Tyler, L. K. (2007). On the tip-of-
the-tongue: neural correlates of increased word-finding failures in normal aging. J Cogn
Neurosci, 19(12), 2060-2070.
Snowdon, D. A., Kemper, S. J., Mortimer, J. A., Greiner, L. H., Wekstein, D. R., & Markesbery,
W. R. (1996). Linguistic ability in early life and cognitive function and Alzheimer's
disease in late life. Findings from the Nun Study. JAMA, 275(7), 528-532.

10
Snyder, P. J., Kahle-Wrobleski, K., Brannan, S., Miller, D. S., Schindler, R. J., DeSanti, S., . . .
Chandler, J. (2014). Assessing cognition and function in Alzheimer's disease clinical
trials: Do we have the right tools? Alzheimer's & Dementia, 10(6), 853-860.
Venneri, A., Mitolo, M., & De Marco, M. (2016). Paradigm shift: semantic memory decline as a
biomarker of preclinical Alzheimer's disease. Biomark Med, 10(1), 5-8.
doi:10.2217/bmm.15.53
Xu, J., Murphy, S. L., Kochanek, K. D., & Arias, E. (2016). Mortality in the United States, 2015.
NCHS data brief(267), 1.
11
CHAPTER 2
Manuscript 1: Review of Picture Description Tasks

12
Connected Speech and Language in Mild Cognitive Impairment and Alzheimer’s Disease:
A Review of Picture Description Tasks
K.D. Mueller, MSa,b*, B.P. Hermann, Ph.D.c, J. Mecollarib, and L.S. Turkstra, Ph.D.a,d,e
aDepartment of Communication Sciences and Disorders, University of Wisconsin - Madison,USA
bWisconsin Alzheimer’s Institute, University of Wisconsin-Madison, USA;, cDepartment of
Neurology, University of Wisconsin-Madison, USA;
dDepartment of Surgery, University of Wisconsin-Madison, USA;
eNeuroscience Training Program, University of Wisconsin-Madison, USA.
*Address correspondence to Kimberly D. Mueller, Wisconsin Alzheimer’s Institute, University
of Wisconsin-Madison, 610 Walnut Street, 9th Floor, Madison, WI 53726 (Email:

13
Connected Speech and Language in Mild Cognitive Impairment and Alzheimer’s Disease:
A Review of Picture Description Tasks
ABSTRACT
The neuropsychological profile of people with Mild Cognitive Impairment (MCI) and Alzheimer’s
Disease (AD) dementia includes a history of decline in memory and other cognitive domains,
including language. While language impairments have been well described in AD, language
features of MCI are less well understood. A potentially sensitive measure of language in MCI is
analysis of connected speech. Connected speech analysis is the study of an individual’s spoken
discourse, usually elicited by a target stimulus, and can help us understand how language deficits
typical of MCI and AD manifest in everyday communication. Among discourse genres, picture
description is a constrained task that relies less on episodic memory and more on semantic
knowledge and retrieval, within the cognitive demands of a communication context. Here we
review picture description task data from adults with MCI and AD, identify speech and language
parameters assessed, discuss the potential value of this task for MCI diagnosis, and provide
recommendations for future research.
KEYWORDS: Mild Cognitive Impairment, Alzheimer’s Disease, connected speech,
language, discourse
14
BACKGROUND
Alzheimer’s Disease (AD) is a neurodegenerative disease that is most often diagnosed
based on clinical symptoms, most notably gradual worsening of problems with learning and
memory that affect activities of daily living (McKhann et al., 2011). Accumulating evidence
(Albert et al., 2011; Sperling et al., 2011) suggests that the neuropathology of AD begins decades
before the onset of clinical symptoms. Determining the most sensitive assessment tools for
detecting cognitive change is crucial not only for early identification, but also for disease
monitoring in clinical trials. Considerable research has focused on assessment of memory and
executive functions (Buckner, 2004; Small, Perera, DeLaPaz, Mayeux, & Stern, 1999), which
are the typical hallmarks of both AD and Mild Cognitive Impairment (MCI) (Albert et al., 2011),
but language assessment also may be sensitive to early cognitive change (Taler & Phillips,
2008). Analysis of connected language may be particularly revealing. Connected language
analysis is the study of self-generated discourse, and has been an intriguing area of AD research
for several reasons: 1) connected language involves ongoing interactions among cognitive
processes including semantic storage and retrieval, executive functions, and working memory,
which contrasts with isolated tasks such as picture-naming or word-list-learning; 2) connected
language more closely approximates language production in everyday contexts than do
standardized tests; and 3) connected language can be a quick means of assessment with relatively
low burden for the participant. Most connected language research has used subjects with mild to
moderate AD, but some retrospective analyses of connected language (Ahmed, Haigh, de Jager,
& Garrard, 2013b; Berisha, Wang, LaCross, & Liss, 2015; Garrard et al., 2005) have revealed
changes at the MCI phase or earlier. In this paper, we provide a comprehensive review of studies
15
of connected language in AD, to determine its diagnostic utility at the MCI or even pre-MCI
phases of disease.
Language deficits in AD dementia have been well documented (Price et al., 1993; Taler
& Phillips, 2008) and the language profile of adults with AD typically is characterized by “empty
speech” (Nicholas, Obler, Albert, & Helm-Estabrooks, 1985), referring to word retrieval deficits
that result in the use of circumlocutions, nonspecific language, and an overabundance of words
conveying limited ideas. In the moderate to severe stages of disease, communication skills
degrade further with deficits in both production (Kemper, Thompson, & Marquis, 2001) and
comprehension of language, (Bickel, Pantel, Eysenbach, & Schröder, 2000; Grossman et al.,
1996; MacDonald, Almor, Henderson, Kempler, & Andersen, 2001; Martin & Fedio, 1983)
associated with communication breakdowns in everyday interactions (Savundranayagam &
Orange, 2014), and increased frustration that may result in challenging behaviors (Woodward,
2013). Often the end stage of AD is characterized by a complete lack of verbal communication,
and the person with AD becomes socially disengaged (Blair, Marczinski, Davis-Faroque, &
Kertesz, 2007; Chung & Cummings, 2000; Frisoni, Fratiglioni, Fastbom, Viitanen, & Winblad,
1999; Hart et al., 2003; Ripich & Terrell, 1988).
The assessment of language in AD typically includes tasks of verbal fluency (Clark et al.,
2009), confrontation naming (Bayles & Tomoeda, 1983), and comprehension of syntax (e.g., the
Token Test (De Renzi & Vignolo, 1962)), all of which have been useful in discriminating among
mild, moderate, and severe stages of AD. Characterizations of language functions in MCI are
much less clear in the literature. For instance, verbal fluency tasks, particularly semantic fluency,
have been shown to differentiate MCI from control groups (Clark et al., 2009; Mueller et al.,
2015; Nutter-Upham et al., 2008), but confrontation-naming tasks have been less effective in
16
characterizing word retrieval problems in MCI (Testa et al., 2004). Subtle, preclinical changes in
language have been particularly problematic to document, because memory impairment is often
the primary symptom of AD, and although language abilities and memory are necessarily
intertwined, there is no standardized approach to differentiating language from memory
impairments. Further, it has been difficult to differentiate between the language changes in MCI
and those associated with normal aging. Thus, quantifying memory difficulties and language
problems simultaneously may increase diagnostic sensitivity, as well as provide important
prognostic indicators. For example, De Jager et al. (De Jager, Blackwell, Budge, & Sahakian,
2005; De Jager & Budge, 2005) found that a subgroup of participants who evidenced both
associative learning and naming deficits showed steeper cognitive decline over four years than
those with deficits in only one of these two domains. As communication problems have been
shown to be directly correlated with challenging behaviors in AD (Gitlin, Winter, Dennis,
Hodgson, & Hauck, 2010; Rao, Anderson, Inui, & Frankel, 2007) as well as with increases in
caregiver burden (Savundranayagam, Hummert, & Montgomery, 2005), it also is critical to
identify communication difficulties early in the disease so non-pharmacological communication
interventions can be implemented for both the patient and caregiver.
The analysis of connected language more closely approximates functional
communication skill than performance on isolated, single-word language tasks, and has therefore
received increased attention over the last two decades. The seminal study of retrospective
language analysis in AD was the Nun Study (Snowdon et al., 1996), in which Snowdon and
colleagues examined early life writing samples of cloistered nuns and were able to predict
cognitive decline based on density of ideas in early writing. The authors theorized that low idea
density reflected suboptimal “neurocognitive development” and thus increased risk for cognitive
17
decline or AD neuropathology. Kemper et al. (2001) further examined the Nuns’ writing
samples, and found that rates of decline in both idea density and grammatical complexity were
similar for those nuns who developed dementia and those who did not, but that those who
developed dementia had lower baseline levels on both measures, supporting the theory of
developmental disadvantage. Other retrospective studies have examined language of public
figures, such novels of the British writer Iris Murdoch, in which decreases in language abilities
were apparent years before her formal diagnosis of AD (Garrard et al., 2005). Berisha et al.
(2015) examined the unscripted speeches of former president Ronald Reagan, and found
decreases in the proportion of unique words and increases in use of fillers over time prior to his
diagnosis of AD.
Other studies of connected speech and language have used language samples obtained
from more constrained tasks such as picture description. While open-ended elicitation methods
may provide a larger quantity of output, they can be highly variable within and across individuals
and contexts, and thus cannot be easily standardized for between- and within-group comparisons.
By contrast, picture description tasks can be easily evaluated with standardized measures, and if
the picture is visible throughout the task they rely less on episodic memory. Picture stimuli most
frequently cited in the literature are Norman Rockwell prints such as “Easter Morning”
(Tomoeda, Bayles, Trosset, Azuma, & McGeagh, 1996), and the “Cookie Theft” picture from
the Boston Diagnostic Aphasia Examination (BDAE) (Goodglass & Kaplan, 1983). The “Cookie
Theft” picture is the most widely used overall, and was designed to include aspects of person,
time, place, and actions, and depicts key vocabulary which is acquired early in life (Giles,
Patterson, & Hodges, 1996).
18
As the language deficits in Alzheimer’s Disease are typically semantically-based,
measures of informational content of language are particularly important. Picture description
readily lends itself to these measures and has the added benefit of minimizing demands on
episodic and autobiographical memory. There is a large literature on picture description in AD,
making it difficult to identify themes and variables across studies. The literature on picture
description or any other aspect of language in MCI is comparatively small, although
retrospective studies do suggest that declines in language may evolve in prodromal phases.
Picture description tasks could be informative at the MCI and pre-MCI phase, not only to help
inform diagnosis, but also to reveal the earliest point at which cognitive-communication
intervention could be most useful. In this review, we set out to examine picture description tasks
and explore the ways in which the literature reports on their utility in MCI and AD. Our aim was
to answer the following research questions:
1. What measures of speech and language are assessed in picture description
tasks?
2. What psychometric properties of connected speech analysis have been reported?
3. What are the limitations of the reported studies, and needs for future research?
4. What is the evidence to support using connected language analysis as a means
to detect and describe how cognitive problems may manifest in everyday speech
and language at the MCI stage?
19
METHODS
Inclusion Criteria for the Review
Study Design Criteria
We included only English-language experimentally-based peer reviewed journal articles that
focused on diagnostic testing with both quantitative and qualitative data results. All studies were
required to have included a picture description task such as “Cookie Theft” from the Boston
Diagnostic Aphasia Examination (BDAE; Goodglass & Kaplan, 1980), the “picnic scene” from
the Western Aphasia Battery (WAB; Kertesz, 1982), or Norman Rockwell prints.
Participant Criteria
Additional criteria included that study participants were diagnosed with probable or confirmed
Alzheimer’s Disease, Mild Cognitive Impairment, or preclinical MCI. Studies that included other
types of dementia (e.g., Vascular dementia) or other neurodegenerative disorder (e.g.,
Parkinson’s) were included, provided that there was also an AD or MCI group. We included
participants who spoke languages other than English, and studies were not excluded based on
age or sex characteristics of participants.
Exclusion Criteria
Studies that met one or more of the following seven criteria were excluded: 1) studies published
in a language other than English for which translations were not available; 2) studies not
published as a peer-reviewed journal article (i.e. poster abstracts, conventions, etc.); 3) studies
that did not include quantitative analyses; 4) studies that did not use picture descriptions as an
assessment tool, but rather for other purposes such as intervention targets or as a means of
monitoring a particular therapeutic intervention; 5) studies in which the picture description task
20
was limited to written descriptions rather than verbal; 6) studies where picture description
consisted of sequential action descriptions only (e.g. listing events in a sequence of pictures,
picture naming, or story re-telling); 7) studies in which picture description was part of a larger
language-test battery, but where scores for picture description alone were not available.
Method for Searching and Identifying Studies
We conducted an electronic literature search for articles reported up to December 2016 using the
PubMed, PsychINFO and CINAHL databases. A librarian verified indices and search terms used
to identify records, and suggested additional terms that were used to search WEB OF SCIENCE
and SCOPUS. We randomized and divided relevant search terms into eleven different groups,
each containing at least seven words or more of the relevant search terms that were entered into
the database. For example, “Dementia OR Alzheimer’s disease AND Connected Speech OR
Spontaneous Language AND Cookie Theft OR Picture description OR Norman Rockwell Prints”
was one group of search terms that fit our criteria. For randomization, we put each of the terms
listed into a random name generator and examined results until it was evident to the reviewers
that a cohesive group of search terms was established. Each group of terms was then entered into
a database, resulting articles were collected, and duplicates were removed. We tracked the
number of articles retrieved during each screening process using the PRISMA (Moher, Liberati,
Tetzlaff, Altman, & and the, 2009) Flow Diagram
The review process was as follows: two authors (KDM, JM) first independently screened
titles for potentially eligible studies following the inclusion criteria. Next, abstracts and/or full
text versions of those articles were reviewed, and articles that did not meet the inclusion criteria
were removed. The final set of articles was then scanned for additional references that were not
21
returned in the electronic search. Any disagreements between the two reviewers were resolved
by discussion.
RESULTS
The search initially returned 871 results. After exclusion criteria were applied, the final
selection was 34 papers. The most common exclusions included studies that only examined
Primary Progressive Aphasia or other dementia variants without an AD group, tasks that did not
include a single picture description component, or articles that examined written picture
descriptions only. Remaining articles were scanned for additional references and 2 more were
added, bringing the total to 36.
Of the 36 studies included in the review, 25 studies used the “Cookie Theft” picture from
the BDAE, 4 of which used the Cookie Theft combined with other pictures. One study used the
picture from the Dutch version of the Comprehensive Aphasia Test (Swinburn, Porter, &
Howard, 2004), 5 studies used Norman Rockwell prints, and one study used the Picnic Scene
from the Western Aphasia Battery (Kertesz, 1982). 31 studies examined patients with AD
dementia, and 5 studies included an MCI or pre-MCI group. Across all 36 studies, there was a
total of 1,127 patients with AD dementia and 274 with MCI or pre-MCI. The average number of
participants with AD or MCI per study was 35, with age ranges of 65.1 – 82.5 years for AD, and
43.2 – 73.5 years for MCI or pre-MCI. Participant characteristics and major study findings are
summarized in Table 1.
22
Language Measures Examined in Picture Description Tasks
The studies we reviewed examined a variety of measures across several domains of expressive
language. The following is a summary of the measures grouped by semantic content, syntax and
pragmatic language.
Semantic Content
Picture-related Content Thematic Elements. Several studies examined the amount of thematic
elements expressed that were directly relevant to the picture stimulus. Nicholas et al (1985)
identified 8 thematic elements of the Cookie Theft picture and used the number of elements
expressed as the outcome measure in four groups: AD, Wernike’s aphasia, anomic aphasia and
normal controls. The AD group consisted of 19 people with AD ranging from mild to moderately
severe (mean age=67). Patients with AD expressed significantly fewer content elements than the
controls; differences between the AD group and the groups with aphasia were not significant.
Hier, Hagenlocker, & Shindler (1985) assessed content using a similar list of 8 actions
and objects in the Cookie Theft picture, which they referred to as “relevant observations”, and
divided their AD group into “early” and “late” stage. The late-stage AD group produced
significantly fewer relevant observations than the early-stage group, and the AD group combined
produced fewer relevant observations than controls. Findings were replicated by Vuorinen et al.
(2000). Cuetos et al. (2007) used a similar set of 8 themes (“semantic units”), to analyze Cookie
Theft picture descriptions by a group of 19 carriers of the E280A mutation in the Presenilin1
gene, and found that, prior to the onset of clinical symptoms, carriers produced fewer semantic
units than non-carriers. Conversely, Smith et al. (Smith, Chenery, & Murdoch, 1989) applied
Hier’s pictorial “theme” construct with the Picnic Scene from the Western Aphasia Battery with
a control group and participants with moderate to moderately severe AD. The authors found that
23
the two groups produced an equal number of semantic elements, but the group with AD required
more time and more syllables to communicate these elements.
Forbes-McKay and Venneri (2005) performed a normative study of discourse variables
from Cookie Theft descriptions (as well as “complex” pictures with more elements) using 240
healthy individuals, ages 20 to 90 years, with varying years of education. The authors developed
cut scores for a modified “Rating Scale Profile of Speech Characteristics” from the Boston
Diagnostic Aphasia Examination (Goodglass & Kaplan, 1983). They then used these cut scores
to determine the sensitivity of the measures in a group of 30 adults with probable AD (mean age
75) across “minimal,” mild and moderate severity (based on Mini Mental State Examination
(MMSE) (Cockrell & Folstein, 1987)). The scores that displayed the best discriminant power
between controls and AD were information content (proportion of phrases containing indefinite
terms, inappropriate phrases and redundant words), 7 pictorial themes, word finding delays, and
the response to word finding delays (70% correct classification rate). Sajjadi et al.(2012) looked
at 10 pictorial themes in pictures descriptions from the Comprehensive Aphasia Test (Swinburn
et al., 2004), and found that the group of 20 adults with mild AD produced significantly fewer
themes than controls. Bschor et al. (2001) examined Cookie Theft picture descriptions at 4 stages
of AD, defined by the Global Deterioration Scale. The authors identified 12 elements of the
Cookie Theft picture, including persons, objects, localizations, actions and features, and found
that while each AD group differed significantly from the others and from controls, the measures
did not distinguish between MCI and normal controls. The authors concluded that there was no
advantage to using the Cookie Theft picture task over standardized language tests such as verbal
fluency or the Boston Naming Test in distinguishing among severities of AD.
24
Beginning with Croisile et al. (1996), several studies (Ahmed, de Jager, Haigh, &
Garrard, 2012a; Ahmed et al., 2013a; Ahmed et al., 2013b; Carlomagno, Santoro, Menditti,
Pandolfi, & Marini, 2005; Fraser et al., 2014; Kavé & Levy, 2003; Lira, Minett, Bertolucci, &
Ortiz, 2014; Shimada et al., 1998) used measures combining thematic elements and unspecified
information units, resulting in a list of 23 possible information units of the Cookie Theft picture.
The authors claimed that analysis of information units provided a more liberal (yet still
constrained) tally of relevant content produced by the speaker, including objects, actions/facts,
places and subjects, and that by having this wider range of criteria, more subtle deficits could be
observed. Studies using the 23-information-unit system found differences between adults with
AD and controls, and some studies found differences among stages of AD (Ahmed et al., 2013b;
Forbes, Venneri, & Shanks, 2001).
General Information Units. Other studies (Arkin & Mahendra, 2001; Giles et al., 1996; C. K.
Tomoeda & K. A. Bayles, 1993; Tomoeda et al., 1996) have used a more general concept of
content, defining “information units” as “the smallest non-redundant meaningful fact or
inference,” whether or not the information conveyed was specific to the picture stimulus. Giles et
al. (1996), for example, studied 48 adults with “minimal,” mild, or moderate AD and found that
adults with AD produced fewer overall information units than controls.
Conciseness of Information. Conciseness has been operationalized as the number of words the
speaker uses to express ideas. The theory is that people with AD will need more words to convey
ideas because of word-finding-related behaviors such as circumlocutions and repetitions.
Conciseness is calculated by dividing the number of ideas expressed by the total number of
words, a measure commonly referred to as “idea density.” Sixteen studies examined some form
of idea density (Ahmed et al., 2012a; Ahmed et al., 2013a; Ahmed et al., 2013b; Bayles et al.,
25
1999; Croisile et al., 1996; Duong, Giroux, Tardif, & Ska, 2005; Forbes-McKay, Shanks, &
Venneri, 2013; Forbes-McKay & Venneri, 2005; Groves-Wright, Neils-Strunjas, Burnett, &
O'Neill, 2004; Hier et al., 1985; McNamara, Obler, Au, Durso, & Albert, 1992; Murray, 2010;
Sajjadi et al., 2012; Shimada et al., 1998; C. K. Tomoeda & K. A. Bayles, 1993; Tomoeda et al.,
1996), denoted by a variety of names, including “lexical index,” “information content,” and
“information unit conciseness index.” For example, Snowdon et al. (1996) examined written
discourse from the Nun Study and found that low idea density in early life was associated with
reduced cognitive performance later in life. Riley et al. (Riley, Snowdon, Desrosiers, &
Markesbery, 2005) extended these findings by concluding that early life idea density was
associated with lower brain weight, higher degree of cerebral atrophy, and increased
neurofibrillary pathology in later life. Ahmed et al. (2013a) examined idea density in 18 patients
with autopsy confirmed AD at the mild stage (MMSE mean = 21) and found that they produced
fewer total semantic units than controls, but differences in idea density between the two groups
did not reach significance. The study of “empty speech” by Nicholas et al. (1995) examined
conciseness with measures thought to contribute to the “non-specificity” of discourse in AD,
such as empty phrases (common idioms contributing no relevant information), deictic terms
(e.g., “this,” “that” without referents), indefinite terms (e.g., “thing” or “stuff”), pronouns
without proper noun antecedents, and repetitions. AD patients produced more of most of these
behaviors than did controls.
Efficiency. Efficiency is the rate at which meaningful information is conveyed over time,
calculated by dividing the total number of information units by the duration of the speech
sample. Smith et al. (1989) found that 18 adults with moderately severe AD produced 21 fewer
content units per minute than controls, due to increased circumlocutions and repetitions. Murray
26
(2010) used an analogous measure referred to as “performance deviations per minute,” in which
fillers, irrelevant words, revisions or false starts, vague or nonspecific vocabulary and inaccurate
output (e.g., paraphasias) were divided by the total number of minutes in the speech sample; this
measure was lower for adults with AD (n=17) than for those with depression (n=18) or normal
aging (n=14). The authors suggested that discourse information measures may help disentangle
the similarities in symptoms of early AD versus depression in older adults.
Lexical Richness/Diversity. Eleven studies (Ahmed et al., 2012a; Ahmed et al., 2013b; Croisile et
al., 1996; F. Cuetos et al., 2007; Fraser et al., 2014; Hier et al., 1985; Kavé & Levy, 2003; Lira et
al., 2014; Murray, 2010; Sajjadi et al., 2012; Sitek et al., 2015) measured some aspect of lexical
richness or lexical diversity, by inspecting word types and totals. Measures included total
number of words, total unique words, and the ratio of unique words to total words, referred to as
“type-token ratio.” More recently, studies have used the Moving Average Type Token Ratio
(MATTR) (Covington & McFall, 2010) to identify lexical diversity, because unlike type-token
ratio, it is independent of text length. Only two studies (Kathleen C Fraser, Jed A Meltzer, &
Frank Rudzicz, 2015; V. Rentoumi, L. Raoufian, S. Ahmed, C. A. de Jager, & P. Garrard, 2014)
used MATTR and other computational measures such as Brunet’s index and Honore’s statistic.
Fraser et al. (2015), using cookie theft samples from a corpus of 167 adults with AD, found that
Honore’s statistic was lower for adults with AD than controls, and Rentoumi’s et al. (2014)
machine classifier results showed lower Honore’s statistic for 18 patients with mixed pathology
versus those 18 participants with AD pathology alone. Other studies investigated lexical content
through ratios of open class/closed class words (Ahmed et al., 2012; Ahmed et al., 2013a;
Ahmed et al., 2013b), measuring different parts of speech such as verbs and pronouns, (Ahmed
et al., 2013b; Fraser et al., 2014) proportions of pronouns, nouns, adjectives and verbs, ratio of
27
nouns to verbs, pronouns to nouns plus pronouns, and verbs to nouns plus verbs. For example, in
Ahmed et al.’s (Ahmed et al., 2013b) study of 9 adults with autopsy-confirmed AD, the
proportion of pronouns were significantly different between MCI and moderate AD groups, and
Fraser et al. (2015) found that proportion of pronouns and proportion of nouns and verbs
classified language samples of participants with AD versus healthy controls.
Quantity. Several studies (Croisile et al., 1996; Giles et al., 1996; Cheryl K Tomoeda & Kathryn
A Bayles, 1993) reported that adults with moderate AD produced fewer words than controls on
picture-description tasks, whereas others (Bschor et al., 2001; Smith et al., 1989; Tomoeda et al.,
1996) found no differences in total words among groups of controls and patients with MCI, mild
AD, and moderately severe AD. Murray (2010) investigated normal controls, AD patients, and
older adults with depression, and found no group differences in total words; and Nicholas et al.
(1985) found no differences in total words among groups of patients with anomic aphasia,
Wernike’s aphasia, AD, or normal controls. Conversely, DeLira et al (2014) found controls
produced more total words than patients with AD, but there was no difference in quantity
between mild and moderate AD groups.
Syntax and Morphology (Language Form)
“Syntax” refers to the rules that govern how words can be combined to form sentences, while
“morphology” is the system that governs the structure of words and the construction of word
forms. Multiple studies included at least one measure of syntactic complexity. Common
constructs included words per clause (Kave & Levy, 2003); grammatical form (measures of an
“appropriate use” of syntactic conjunctions, tenses, conditionals, subordinate clauses and passive
constructions) (Forbes-McKay & Venneri, 2005; Lai, Pai, & Lin, 2009); measures of “phrase
length” (also called t-unit length (Fraser et al., 2015; Sajjadi et al., 2012), and proportion of
28
words in sentences (Ahmed et al., 2012b); number and type of clauses in a sentence (e.g.,
dependent vs. subordinate clauses); clause types that differ in complexity (e.g., passive vs.
infinitive vs. coordinate clauses (Hier et al., 1985; Kavé & Levy, 2003); the proportion of verbs
to nouns plus verbs (based on the premise that syntactic simplification is indexed by number of
verbs used in an utterance) (Kavé & Levy, 2003); pronoun/referent ratio (Chapman, Ulatowska,
King, Johnson, & McIntire, 1995); and errors in sentences, referred to either as grammatical
errors, syntactic errors (Kavé & Levy, 2003), or verb-agreement errors (Sajjadi et al., 2012).
One study used a syntactic complexity index, consisting of complex clauses divided by total
number of clauses (Duong et al., 2005). Several studies examined mean length of utterance
(MLU), defined as the number of morphemes (smallest unit of meaning) divided by the total
number of utterances (Ahmed et al., 2012a; Ahmed et al., 2013b; Hier et al., 1985; Murray,
2010; Ripich, Fritsch, Ziol, & Durand, 2000). The general hypothesis motivating these studies is
that either working memory limitations or semantic memory limitations in AD affect one’s
ability to use complex grammatical constructions. Findings regarding syntax differences were
mixed; for example, Murray’s (2010) selected construct of syntactic complexity, MLU, was not a
distinguishing factor among healthy adults, adults with depression and adults with AD. Kave &
Levy (2003), in a study of 14 adults with AD and 48 controls, found that reduced information,
not syntax or morphology, was the distinguishing factor between the groups. Ripich et al.
(2000) found a decrease in MLU in adults with severe AD over time, but not for those with mild
or moderate AD. Conversely, Ahmed et al. (2012a, 2013b) found differences in syntactic
complexity between adults with MCI and controls, and between MCI and moderate AD stages.
The differences in syntactic complexity were not significant when individual measures were
29
tested, but were apparent using a composite score consisting of MLU, words in sentences,
syntactic errors, nouns with determiners, and verbs with inflections.
Pragmatic Language
The following section outlines measures that fall under the pragmatic language domain, which
refers to the social rules of language for the purpose of communication, including: 1) using
language to achieve goals (Ciccia & Turkstra, 2002); 2) using information from the context to
achieve these goals; and 3) using the interaction between people to initiate, maintain, and
terminate conversations (Ciccia, 2011).
One study (Ripich et al., 2000) examined several pragmatic abilities among patients at
different stages of AD (early (n=10; MMSE=23); middle (n=10; MMSE=16.2) late (n=10;
MMSE=10.3), with measures including questions, turns, unsure statements, judgments, giving
names, and egocentric comments. The only significant difference across stages was in questions,
in that the severe AD group asked more questions over time. The authors argued that question-
asking was a compensatory strategy, and as a result, adults in late-stage AD may have had
insight into their communication problems. The authors acknowledged, however, that the study
had a number of possible confounds. First, a caregiver was asked to administer the picture
description task in order to mirror a more typical communicative interaction. While this method
achieved the ecological goal of the study, caregiver interactions were varied and uncontrolled.
Some caregivers asked questions, and provided prompts and encouragement while others did not.
Second, due to the constrained nature of the picture description task, it is unlikely that it captured
pragmatic skills that are typical of conversations in everyday life.
Coherence. Coherence refers to the appropriate maintenance of topic in discourse (Halliday &
Hasan, 2014), measured by how closely an utterance is thematically related to the immediately
30
preceding utterance (local coherence) and by how closely an utterance relates to the general topic
at hand (global coherence) (Laine, Laakso, Vuorinen, & Rinne, 1998). One study examined
coherence: Chapman et al. (1995) used picture descriptions of Norman Rockwell prints within a
frame analysis, with “frames” being defined as internalized knowledge structures. The authors
identified aspects of content, including typical frames of interpretation, atypical, incorrect, or no
frames, propositions supporting frames, and propositions disrupting frames as measures of
coherence. They examined these variables in three groups: early stage AD (n=12), “old-elderly”
(n=12) and normal controls (n=12). The old-elderly and normal controls produced significantly
more typical frames, and more frame-supporting information than the AD group. The authors
attributed AD patients’ difficulties to memory deficits, attentional deficits, visual perceptual
problems, disruption of internalized frame representation, or failure to access frame knowledge.
Perseveration. One study (Bayles, Tomoeda, Kaszniak, Stern, & Eagans, 1985) examined verbal
perseveration in the description of Norman Rockwell prints, dividing total number of words
within perseverations by total number of words in the speech sample. The authors also calculated
rate of perseveration on two other language tasks: confrontation naming and generative naming.
Across all tasks, the AD group produced significantly more perseverations than controls;
however, on the picture description task alone, there were no significant differences between the
two groups. The authors postulated that this was because picture description was an easier task
due to the visual stimulus, similar to the argument made by Bschor et al. (2001).
Speech Intonation/Prosody. Three studies (Forbes-McKay et al., 2013; Forbes-McKay &
Venneri, 2005; Forbes, Venneri, & Shanks, 2002) examined “melodic line”, a subjective
measure of speech prosody defined as “the appropriate use of intonational contour, including
alterations in pitch, volume and duration” (Goodglass & Kaplan, 1983). For instance, Forbes-
31
McKay et al. compared melodic line using a “simple” picture (Cookie Theft or “The Tripping
Woman,” (Semenza & Cipolotti, 1989)) versus a “complex” picture (“Bus Stop” or “Chaos”,
unpublished, designed by the researchers). The number of pictorial themes differentiated the
simple tasks from the complex. Results showed no group differences on simple picture tasks
(Cookie Theft and Tripping Woman) but there were differences in melodic line for the complex
picture tasks. Fraser et al. (2015) examined several acoustic features of speech in patients with
AD using machine learning methods that captured both rate and phonation patterns, and found
acoustic abnormalities to be a significant factor. Konig et al.(2015) also used an automated
feature analysis examining vocal and temporal aspects of speech among controls, and patients
with MCI or AD, and reported a classification accuracy of 81%.
Discourse Fluency
“Verbal fluency” is a term used in neuropsychological contexts generally referring to timed,
word-generation tasks, while in Speech-Language Pathology contexts, “fluency disorders” are
defined as interruptions in the flow of speaking characterized by atypical rate, rhythm and
repetitions in sounds, syllables, words and phrases. “Fluency,” in the literature of discourse of
adults with AD, typically refers to the smoothness or flow of spoken language. Abnormalities of
fluency in this population are typically characterized by filled and unfilled pauses, word
repetitions, circumlocutions, and revisions. In contrast with fluency disorders (i.e., stuttering),
abnormalities in the fluency of adults with MCI or AD are rarely characterized at the
phonological level.
Ten studies reported on some aspect of discourse fluency. The study of “empty speech”
by Nicholas et al. (1985) was one of the first to examine aspects of fluency in the connected
speech of persons with AD. The authors found that adults with AD (n=19) had significantly
32
more repetitions than controls (n=30) in Cookie Theft descriptions. Similarly, Tomoeda et al.
(1986) found more aborted phrases, revisions, and ideational repetitions in the AD group than the
controls. Several other studies showed a greater number of repetitions (Fraser et al., 2015; Hier et
al., 1985) and revisions (Hier et al., 1985; Sajjadi et al., 2012) in AD groups versus controls.
These findings contrast with studies examining fluency earlier on the disease continuum, which
did not find differences between adults with vs. without AD (Ahmed et al., 2012a; 2013b). From
these findings, it appears that disfluent behavior is a reflection of moderate to severe stages of
disease when semantic processing is overtly compromised.
Speech Rate
Speech rate typically is calculated as syllables per minute. Of the six studies that have evaluated
speech rate (Ahmed et al., 2012a; Ahmed et al., 2013a; Ahmed et al., 2013b; Giles et al., 1996;
Murray, 2010; Smith et al., 1989), none found significant differences among groups.
Speech Monitoring
Speech monitoring is related not only to word retrieval deficits and to pragmatic language skill,
but also to “anosognosia,” the awareness of one’s own deficits. McNamara et al. (1992)
investigated word error monitoring skills by comparing uncorrected and repaired errors in adults
with AD (n=15) or Parkinson Disease (PD) (n=22) vs. normally aging adults (n=141). AD and
PD groups were equally impaired in error monitoring as compared to the controls. Severity of
naming deficits correlated negatively to the amount of uncorrected errors (r=-.37). The authors
suggested that this impairment was related to executive function difficulties in the clinical
groups. The authors did not report correlations between error monitoring and executive function
test scores, however, which could have strengthened that hypothesis.
33
Another measure of speech monitoring used in the picture description literature is
“response to word finding delays,” defined as “whether patients appear unaware of their
problem, produce an approximation of the target word, or actively search and produce the target
word.” (Forbes-McKay & Venneri, 2005) Response to word finding delays differed significantly
between minimal AD and normal controls (Forbes-McKay & Venneri, 2005; Forbes et al.,
2002). The measure was based on the Goodglass & Kaplan (1983) scale for rating discourse on
the Boston Diagnostic Aphasia Examination, and is comprised of clinical judgment of behavior
that is rated on a Likert-type scale ranging from 1 to 7 (7 being no abnormality).
Summary of Language Measures Results. In general, semantic content of picture descriptions is
the most frequently cited measure of language degradation, followed by some measure of idea
density. A major limitation of the studies reviewed here was lack of age-matching of healthy
controls to subjects with AD, as several studies included AD groups that were older than the
controls. Variables such as voice onset time, syntactic complexity, and fluency can be affected
by aging, so age difference between groups is a potential confounding factor. In some studies,
AD groups were not adequately described in terms of severity, which may lead to an
oversimplification of results. In addition, studies used multiple names for the same construct
(e.g., ‘content units’, ‘thematic units’, ‘semantic units’), which adds to difficulty in aggregating
and interpreting results across studies. Additionally, measures such as “melodic line”,
“unspecified content units”, and “response to word finding” are subjective, and thus would be
difficult to reproduce in other studies. Finally, some studies reported either limited information
on inter- and intra-reliability of transcriptions/scoring or no information at all.
Psychometric Properties of Connected Speech Analysis in Picture Description Tasks
Test-Retest Reliability
34
As part of a normative study of simple and complex picture description tasks, Forbes-McKay &
Venneri (2005) examined test-retest reliability in a randomly selected group of 40 healthy adults,
ages 23-84 (mean age=60) who were retested after a one-week delay. There were low test-retest
correlations for measures that distinguished AD groups from controls, including information
content (.56), pictorial themes (.50), word finding delays (.50), and semantic paraphasias (-.10).
This can be explained by practice effects (particularly following the short one-week interval),
and ceiling effects in this healthy and relatively young cohort. We were unable to identify any
other study reporting test-retest reliability for measures specifically designed for the MCI/AD
population.
Inter-Rater Reliability
The majority of studies examined in this review reported on some form of inter-rater reliability,
with coefficients ranging between .78 and .99 for coding of language variables (most notably
content units), although some studies did not report actual correlation coefficients. Very few
studies reported on inter-rater reliability of the transcription process itself, which may also add
unnecessary variability to results (Garrard, Haigh, & de Jager, 2011; Macwhinney, Fromm,
Forbes, & Holland, 2011).
Comparison of Picture Description to Standardized Language Measures
Kave et al. (2016) compared language performance across picture naming, semantic verbal
fluency, and Cookie Theft picture description tasks in adults with AD (n=20) versus controls
(n=20). Some measures of connected speech correlated with the picture-naming scores (e.g.,
percent content words, nouns, and pronouns; mean frequency of words; mean word length), but
only one dimension of connected speech (percent nouns) correlated with semantic fluency. The
authors suggested that the lack of significant correlation between measures of connected speech

35
and semantic fluency tasks could be due to two factors: 1) the picture description task, like the
picture naming task, had visual support which the fluency task did not; 2) verbal fluency tasks
are highly dependent on executive functions, whereas picture description may be more reliant
upon semantic stores. The authors support their hypothesis by noting that the control group
showed a lack of correlation between the naming scores, verbal fluency scores, and the
connected speech variables, implying that each task is dependent upon different retrieval
demands.
Parallel Test Form Reliability
Forbes-McKay et al. (2005) collected normative data for two simple picture stimuli (Cookie
Theft and Tripping Woman) and two complex pictures (Chaos Traffic Scene and Bus Stop
Scene). Responses to the two simple pictures showed high correlations for grammatical form,
information content, and error monitoring, but low correlations for pictorial themes and word-
finding delays, most likely due to ceiling effects of these measures in a healthy, young group.
Results were similar for the complex pictures – i.e., high correlations on most measures. Another
study compared descriptions of two pictures differing in content level (high vs. low) in an AD
group and a normal control group. Interestingly, there was a significant group by content
interaction, as the AD group produced more content units in the low content picture than in the
high content picture relative to controls (Ehrlich, Obler, & Clark, 1997). March et al. (2006)
compared the Cookie Theft to other elicitation tasks (cartoon, describing a map) and found that
the Cookie Theft was more sensitive to reduced noun use than the other more complex methods.
(March, Wales, & Pattison, 2006)
36
Discriminant Validity
Several studies compared picture description task data among clinical groups, such as vascular or
mixed dementia vs. pure AD, early- vs. late-stage AD, or AD vs. fronto-temporal variants.
Theese studies aimed to determine if picture description tasks were sensitive to between-groups
differences.
Normal aging and early AD. Forbes-McKay et al. (2005) provided a normative study with cut-
off scores for normal individuals up to age 90 years. Specifically, the cut off scores were for the
measures included in the BDAE discourse coding scheme (Goodglass & Kaplan, 1983), as well
as some additional measures specifically for AD (response to word finding delays, information
content, speech monitoring, and information content specific to the picture). They performed
multiple regressions adjusting for age, sex and education, and obtained cut-off scores based on
tolerance limits, and found that with these cut-off scores, individuals with “minimal” AD were
able to be correctly identified with 70% accuracy. The study by Chapman et al. (1995) included a
group of “older-elderly” adults (>80 years), and the early AD group performed significantly
worse than the old-elderly group on a range of discourse cohesion measures. Conversely, Bschor
et al. (2001) found no significant differences between controls and adults with MCI, with
significant differences only between controls and adults with moderately-severe AD. Duong et
al. (2005) submitted nine measures of discourse processing to cluster analysis and found that the
clusters failed to distinguish .between normal aging (n=53) and mild-to-moderate AD (n=46)
50% of the time.
Stages of Alzheimer’s Disease. There is mixed evidence that discourse measures discriminate
among stages of disease. In the study by Forbes et al. (2002) adults with “minimal” AD (n=10;
MMSE=24-30) had significantly more word-finding delays and produced more semantic

37
paraphasias than controls, and those measures also differentiated patients in the mild AD stage
(n=10; MMSE = 19-23) from controls. Alternatively, Bschor et al. (2001) found that
standardized tasks such as Boston Naming Test and category/letter fluency tasks were more
sensitive to stages of disease than the picture description task. However, this study examined
only four content aspects of the sample (objects, locations, actions, features) according to the
authors’ internally developed protocol, thus aspects of conciseness, efficiency, fluency, or syntax
were not examined. Similarly, Carlomango et al. (2005) calculated total words, information
units, information units per minute, words per minute and percent correct information units in
discourse samples, all of which distinguished between controls and adults with AD, but not
between mild and moderate AD. More recently, Ahmed compared retrospective data from adults
at different stages of disease, who had autopsy-confirmed AD to data from controls, and found
that measures of semantic and lexical content and syntactic complexity captured the progression
of impairment through stages of disease. (Ahmed et al., 2013a)
Primary Progressive Aphasia and AD. The examination of spontaneous speech for primary
progressive aphasia has become part of routine diagnostic examination (Gorno-Tempini et al.,
2011). Sajjadi et al. (2012) compared data among Semantic Dementia (SD), AD, and normal
controls groups, and found that the AD and SD groups were similar in speaking rate, proportions
of closed-class words, and number of redundant words and phrases, and both produced fewer
pictorial themes than controls. The SD group differed from the AD group on a separate
spontaneous speech task (a semi-structured interview), in which the SD group produced
significantly more semantic and morpho-syntactic errors than the AD and control groups. Ahmed
et al. (2012) asked if a group of autopsy-confirmed AD patients showed similar language
patterns to those seen in logopenic Primary Progressive Aphasia (lvPPA), and found that only
38
one patient with AD out of 18 showed a similar pattern to lvPPA. The authors concluded that
lvPPA is a true clinical variant of PPA and not a clinical feature of Alzheimer’s Disease.
Alzheimer’s Disease and Parkinson Disease. One study compared speech monitoring between
persons with AD and PD and normal controls (McNamara et al., 1992). Both the AD and PD
groups corrected significantly fewer speech errors than controls. While AD patients tended to use
single-word repairs, PD patients were more like to use both single-word and sentence-level
reformulations.
Alzheimer’s Disease and Vascular Dementia. Nicholas et al. (1985) used the Cookie Theft task
to describe empty speech in four groups: AD, Wernike’s aphasia, anomic aphasia and normal
controls. The AD group consisted of 19 people with AD ranging from mild to moderately severe.
The group with AD produced significantly fewer content elements than control subjects, and
adults with Wernike’s aphasia had the least informative samples of all 4 groups. The
distinguishing factor between Wernike’s aphasia and AD was that the Wernike’s group produced
more neologisms than the AD group, and the authors concluded that neologistic speech can serve
as a diagnostic marker. The AD group was heterogeneous in severity of AD, which potentially
confounded interpretation of results, as lexical deficits increase in severity as the disease
progresses. Vuorinen (2000) and Carlomango (2005) examined semantic measures in vascular
dementia/aphasia and AD and found that the two groups performed similarly and worse than
control subjects, and that semantic measures did not distinguish between the two dementia
groups.
Alzheimer’s Disease and Depression. Elderly patients with depression are sometimes
misdiagnosed with dementia, due to the similarities in clinical presentation, such as deficits in
memory, attention, and processing speed; social withdrawal; anxiety; and apathy (Dobie, 2002).
39
Murray (Murray, 2010) found that picture description task measures helped differentiate AD
from depression, as the depressed group performed similarly to controls on all measures of
discourse. Therefore, while cognitive screening and assessment may not accurately distinguish
depression due to potentially reversible cognitive deficits, narrative analysis may be of clinical
use.
Sex Differences in Picture Description Abilities
Bayles et al. (1999) examined sex differences in idea density (information units/total words) in a
group of men and women with probable AD with similar dementia severity. Within both cross-
sectional and longitudinal designs, the authors found no significant differences between men and
women on any measure.
Longitudinal Analyses using Picture Description
Four studies examined picture description results longitudinally. Forbes-McKay et al.(2013)
found that phonological paraphasias (speech sound errors) were significantly increased at a 12-
month follow up, but that other deficits noted at baseline (word finding delays, semantic
paraphasias, and fewer repaired errors) had not changed significantly at 12 months. Ahmed
found increasing deficits in semantic and lexical content and syntactic complexity across three
stages of disease in subjects with pathologically confirmed AD (Ahmed et al., 2013b). Bayles et
al. (1999) found no significant differences in idea density between men and women at a two-year
follow-up.
Brain Imaging and Picture Description Tasks
Shimada et al. (1998) studied regional cerebral blood flow (rCBF) during the Picture Description
Task (Ulatowska, 1985), and found significant correlations between number of information units
and blood flow changes in the occipital lobe and left thalamus, suggesting “thalamo-coritcal
40
functional circuits.” Due to the small sample size and the single-time point measurement, these
results need replication.
DISCUSSION
Without question, Alzheimer’s Disease degrades the language system, and more broadly,
the communication system, at some point on the continuum of disease. These results show that a
task as simple and non-invasive as describing a picture can yield rich information about language
content, syntax, and pragmatics at several points in the course of disease. Results are more robust
at later stages of AD, but are inconclusive at the MCI stage. Certainly, the retrospective studies
of earlier life writings indicate that a process of change may be occurring pre-clinically;
however, writing and speaking engage different cognitive processes. The relatively few studies
of the spoken language of adults with MCI showed promise that detectable differences in
connected speech are evident early on the AD continuum, but clearly more research is needed.
Perhaps the earliest evidence of change in connected language comes from the
prospective study by Cuetos et al. (2007) that examined preclinical disease in carriers of the
E280A mutation of the PSN-1 gene, and these results were promising: a reduction in information
units at a young age and at a truly preclinical state with no evidence of clinical impairment. This
finding was replicated in a pre-clinical population showing sub-clinical declines in memory by
Mueller et al. (2016), although the sample was an at-risk cohort; whether or not these individuals
represent a true preclinical AD group is unknown. Longitudinal designs that study connected
language in preclinical or at-risk groups prospectively are needed to determine when connected
language can be a sensitive and informative measure of early cognitive decline.
The study by Kave et al. (2016) delineates the probable underlying differences between
speech and language in discourse versus in isolation: while picture description measures
41
accurately distinguished controls from AD patients, the authors found weak or minimal
correlations of several connected speech measures with focal tasks such as picture naming and
verbal fluency. This indicates that connected speech may be able to tap into additional processes
not accessed by way of standardized measures, and may serve as an important marker for early
diagnosis and for clinically meaningful change.
Review of discourse studies revealed that the notion that syntax is preserved at least until
the moderate stages of AD is an oversimplification. While many of the rules of grammar are
maintained until late in the disease, likely because they are governed by procedural memory
systems, there is accruing evidence that syntax becomes simplified even in early stages of
disease.(Ahmed et al., 2013b; Ripich et al., 2000) Automated methods, larger sample sizes, and
longitudinal analyses are necessary to understand when and to what degree syntax is affected.
An additional rationale for using connected speech analysis is intervention: cognitive-
communication interventions, much like pharmacological interventions, will likely be more
effective earlier in the disease course before neuropathological changes become diffuse (Jack et
al., 2011; Oren, Willerton, & Small, 2014). Using connected speech as a diagnostic measure will
also help to describe the problems that affect everyday communication, and in so doing, allow us
to develop targeted communication interventions that help minimize communication partner
stress and burden. Connected speech also can be a functional marker for disease progression and
response to pharmacological interventions, as it may be a more objective measure than self- or
caregiver-report of functional activities of daily living. A 2015 report on “Innovative Diagnostic
Tools for Early Detection of Alzheimer’s Disease” (Laske et al., 2015) listed analysis of
spontaneous speech and voice (rate, voice onset time, variations in pitch and amplitude) and
42
spontaneous language (content, syntax, pragmatics) as one of the innovative tools that deserves
further research.
Many of the studies here presented with common limitations. First, the sample sizes
were often small (mean across the 38 studies = 35) and lacking in diverse ethnic and cultural
backgrounds, or did not report on racial background at all. The majority of studies did not report
on hearing status, which may have confounded results (particularly with respect to concurrent
neuropsychological tests). Some studies did not clearly define stages of disease. For example,
Chapman et al. (Chapman et al., 1995) classified the AD group as “mild AD,” however the
group’s mean Logical Memory score was 3.7(SD=2.2), which is significantly lower than the
scores reported in the literature for mild AD (Petersen et al., 1999). Finally, many studies did
not match controls according to age, gender and education, which would have strengthened
results.
The general conclusions of this review highlight the importance of longitudinal analysis
of connected speech and language, to better and more accurately describe the progression of
language changes beginning in MCI or before. Five of the studies reviewed were longitudinal
designs (Ahmed et al., 2013b; Bayles et al., 1999; Bayles, Tomoeda, & Trosset, 1993; Forbes-
McKay & Venneri, 2005; Ripich et al., 2000), and each showed that some aspect of connected
language showed change at follow-up. These studies’ sample sizes ranged from 9 to 31
(mean=16), and the samples’ mean age ranged from 71 to 80 (mean=74.9). Larger-scale studies,
beginning at younger ages and with more points of follow-up may not only better characterize
language change, but also the test-retest stability of these measures in people who are not
declining in language and memory.
43
Only one study examined sex differences in picture description and AD (Bayles et al.,
1999) and found no differences; however, other findings suggest that AD pathology is
differentially manifested clinically between sexes (Barnes et al., 2005). For instance, findings
suggest that the association between AD pathology and clinical AD is substantially stronger in
women than in men (Barnes et al., 2005), while sex differences favor women in verbal learning
and memory (Lewin, Wolgers, & Herlitz, 2001). However, potential confounds exist in studying
sex-based differences in cognitive outcomes for MCI and AD, such as: differences in hormonal
history; history of depression, anxiety or substance abuse; and differences in education, lifestyle
and occupational history. Therefore, an area of need for future research is to examine sex
differences in connected speech using longitudinal analyses with larger sample sizes, detailed
personal, health and lifestyle histories, and across various stages of AD. Using multi-modal
imaging biomarkers as a concurrent means of assessing AD pathology while studying sex-based
differences in connected speech over time may reveal further information about AD risk.
Much of the research reported here required arduous, labor-intensive hand transcription,
counting, and coding. Other promising research methods are automatic feature classification
systems, machine learning techniques, and natural language processing, which have now been
applied to the study of speech and language in AD (Fraser et al., 2015; König et al., 2015;
Rentoumi et al., 2014). Automated methods also may assist with analysis of “melodic line” or
other aspects of speech prosody that to date have been analyzed using subjective judgments.
Despite good training methods and inter-rater reliability, subjective judgements are prone to
human error, and machine classification removes some of the human error in obtaining these
measures. Technology also allows faster and easier analysis of rate, prosody, pitch, and loudness,
and may detect patterns not perceptible to humans. For example, acoustic analyses accurately
44
identified MCI, mild AD and moderate AD with up to 89% accuracy, using vocal features that
were not detectable to the human ear (König et al., 2015).
One conclusion of this review is that the studies reviewed here showed varied if not
limited cohesiveness in the terms used to describe identical language constructs. A factor
contributing to this heterogeneity of terms may be the varied disciplines approaching the
problem (e.g., linguistics, neuropsychology, speech-language pathology). A more cohesive
approach by standardizing terms across disciplines may help to aggregate future results, and to
better understand the systematic effects of studying connected language for the diagnosis and
monitoring of language in AD.
The narrow focus of our review, in terms of both tasks and populations, can be
considered a limitation. In particular, much information can be garnered from the Primary
Progressive Aphasia research about progressive and specific language decline. Several of the
PPA studies included picture description tasks, and by excluding those studies without an AD
component, we may have missed valuable comparisons among progressive disorders. Because
we excluded other connected language elicitation methods, such as personal event narratives and
conversations, we were unable to assess strengths and weaknesses of different methods that
attempt to achieve the same goal. Future reviews should include task comparisons, to identify the
most sensitive, specific, effective, and efficient tasks for eliciting and analyzing connected
speech and language.
In addition to the research limitations discussed above, picture description tasks have
inherent limitations. First, while these tasks elicit spontaneous, unrehearsed speech and language,
they by no means reflect conversational speech, where the breakdowns in patient-caregiver
communication actually occur. Picture description is essentially a monologue: the needs of the
45
listener are limited as opposed to the demands in less concrete, natural conversations.
Conversational tasks, in which there is a back-and-forth exchange between two or more people,
also require a good deal of executive function, metacognitive and pragmatic skill, and language
comprehension, and thus may be more useful in understanding communication challenges in
activities of daily living. Conversational speech and language, and its relation to picture
description, in an area of research that needs further investigation in MCI and AD.
Second, one of the strengths of picture description tasks can also be considered a
limitation; that is, while the task allows for standardization, and thus lends itself to longitudinal
assessment and comparison across studies, the picture used should be one that is culturally and
socially representative of patients’ experiences to best capture that individual’s semantic
knowledge. Pictures such as the “Cookie Theft” can become dated and irrelevant to future
cohorts, and may not be an adequate stimulus across cultures. Future research using picture
description tasks should aim to address cultural and generational relevance as the population
demographics change, by developing and investigating new and diverse stimuli.
CONCLUSION
Our review shows that picture description tasks, as an elicitation method for obtaining connected
language samples, are useful in detecting differences in semantic processing, syntactic
complexity, pragmatic language use, and speech and voice parameters between persons with
Alzheimer’s disease and those who are aging typically, and across stages of disease. While
evidence for the tool’s sensitivity at the MCI phase or before is limited, there is still indication
that subtle changes in speech and language can be detected, particularly longitudinally.
Clinically, providing spontaneous speech in this context may present a quick and efficient means
of gaining information about language, while posing less burden to the adults with MCI and AD.

46
Finally, technological advances in machine learning, automatic speech recognition, and natural
language processing offer exciting opportunities for expansion in knowledge about subtle
changes, while affording more efficient and expedient means to analyze speech and language.
47
REFERENCES
Ahmed, S., de Jager, C. A., Haigh, A.-M. F., & Garrard, P. (2012). Logopenic aphasia in
Alzheimer's disease: clinical variant or clinical feature? Journal of Neurology,
Neurosurgery & Psychiatry, jnnp-2012-302798.
Ahmed, S., de Jager, C. A., Haigh, A. M., & Garrard, P. (2012a). Logopenic aphasia in
Alzheimer's disease: clinical variant or clinical feature? J Neurol Neurosurg Psychiatry,
83(11), 1056-1062. doi:10.1136/jnnp-2012-302798
Ahmed, S., de Jager, C. A., Haigh, A. M., & Garrard, P. (2013a). Semantic processing in
connected speech at a uniformly early stage of autopsy-confirmed Alzheimer's disease.
Neuropsychology, 27(1), 79-85. doi:10.1037/a0031288
Ahmed, S., de Jager, C. A., Haigh, A. M. F., & Garrard, P. (2012b). Logopenic aphasia in
Alzheimer's disease: clinical variant or clinical feature? Journal of Neurology
Neurosurgery and Psychiatry, 83(11), 1056-1062. doi:10.1136/jnnp-2012-302798
Ahmed, S., Haigh, A. M., de Jager, C. A., & Garrard, P. (2013b). Connected speech as a marker
of disease progression in autopsy-proven Alzheimer's disease. Brain, 136(Pt 12), 3727-
3737. doi:10.1093/brain/awt269
Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., . . . Phelps,
C. H. (2011). The diagnosis of mild cognitive impairment due to Alzheimer's disease:
recommendations from the National Institute on Aging-Alzheimer's Association
workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement, 7(3),
270-279. doi:10.1016/j.jalz.2011.03.008
Arkin, S., & Mahendra, N. (2001). Discourse analysis of Alzheimer's patients before and after
intervention: Methodology and outcomes. Aphasiology, 15(6), 533-569.
Barnes, L. L., Wilson, R. S., Bienias, J. L., Schneider, J. A., Evans, D. A., & Bennett, D. A.
(2005). Sex differences in the clinical manifestations of alzheimer disease pathology.
Archives of General Psychiatry, 62(6), 685-691. doi:10.1001/archpsyc.62.6.685
Bayles, K. A., Azuma, T., Cruz, R. F., Tomoeda, C. K., Wood, J. A., & Montgomery Jr, E. B.
(1999). Gender differences in language of Alzheimer disease patients revisited. Alzheimer
Disease and Associated Disorders, 13(3), 138-146.
Bayles, K. A., & Tomoeda, C. K. (1983). Confrontation naming impairment in dementia. Brain
Lang, 19(1), 98-114.
Bayles, K. A., Tomoeda, C. K., Kaszniak, A. W., Stern, L. Z., & Eagans, K. K. (1985). Verbal
perseveration of dementia patients. Brain Lang, 25(1), 102-116.
Bayles, K. A., Tomoeda, C. K., & Trosset, M. W. (1993). Alzheimer's disease: Effects on
language. Developmental Neuropsychology, 9(2), 131-160.
Berisha, V., Wang, S., LaCross, A., & Liss, J. (2015). Tracking discourse complexity preceding
Alzheimer's disease diagnosis: a case study comparing the press conferences of
Presidents Ronald Reagan and George Herbert Walker Bush. J Alzheimers Dis, 45(3),
959-963. doi:10.3233/JAD-142763
48
Bickel, C., Pantel, J., Eysenbach, K., & Schröder, J. (2000). Syntactic comprehension deficits in
Alzheimer's disease. Brain Lang, 71(3), 432-448.
Blair, M., Marczinski, C. A., Davis-Faroque, N., & Kertesz, A. (2007). A longitudinal study of
language decline in Alzheimer's disease and frontotemporal dementia. Journal of the
International Neuropsychological Society, 13(02), 237-245.
Bschor, T., Kuhl, K. P., & Reischies, F. M. (2001). Spontaneous speech of patients with
dementia of the Alzheimer type and mild cognitive impairment. Int Psychogeriatr, 13(3),
289-298.
Buckner, R. L. (2004). Memory and executive function in aging and AD: multiple factors that
cause decline and reserve factors that compensate. Neuron, 44(1), 195-208.
Carlomagno, S., Santoro, A., Menditti, A., Pandolfi, M., & Marini, A. (2005). Referential
communication in Alzheimer's type dementia. Cortex, 41(4), 520-534.
Chapman, S. B., Ulatowska, H. K., King, K., Johnson, J. K., & McIntire, D. D. (1995).
Discourse in early Alzheimer's disease versus normal advanced aging. American Journal
of Speech-Language Pathology, 4(4), 124-129.
Chung, J. A., & Cummings, J. L. (2000). Neurobehavioral and neuropsychiatric symptoms in
Alzheimer's disease. Neurologic clinics, 18(4), 829-846.
Ciccia, A. (2011). Pragmatic Communication. In J. S. Kreutzer, J. DeLuca, & B. Caplan (Eds.),
Encyclopedia of Clinical Neuropsychology (pp. 1994-1995). New York, NY: Springer
New York.
Ciccia, A. H., & Turkstra, L. S. (2002). Cohesion, communication burden, and response
adequacy in adolescent conversations. Advances in Speech Language Pathology, 4(1), 1-
8.
Clark, L. J., Gatz, M., Zheng, L., Chen, Y. L., McCleary, C., & Mack, W. J. (2009). Longitudinal
verbal fluency in normal aging, preclinical, and prevalent Alzheimer's disease. Am J
Alzheimers Dis Other Demen, 24(6), 461-468. doi:10.1177/1533317509345154
Cockrell, J., & Folstein, M. F. (1987). Mini-Mental State Examination (MMSE).
Psychopharmacology bulletin, 24(4), 689-692.
Covington, M. A., & McFall, J. D. (2010). Cutting the Gordian knot: The moving-average type–
token ratio (MATTR). Journal of Quantitative Linguistics, 17(2), 94-100.
Croisile, B., Ska, B., Brabant, M. J., Duchene, A., Lepage, Y., Aimard, G., & Trillet, M. (1996).
Comparative study of oral and written picture description in patients with Alzheimer's
disease. Brain Lang, 53(1), 1-19. doi:10.1006/brln.1996.0033
Cuetos, F., Arango-Lasprilla, J. C., Uribe, C., Valencia, C., & Lopera, F. (2007). Linguistic
changes in verbal expression: a preclinical marker of Alzheimer's disease. J Int
Neuropsychol Soc, 13(3), 433-439. doi:10.1017/S1355617707070609
49
De Jager, C., Blackwell, A. D., Budge, M. M., & Sahakian, B. J. (2005). Predicting cognitive
decline in healthy older adults. The American Journal of Geriatric Psychiatry, 13(8),
735-740.
De Jager, C. A., & Budge, M. M. (2005). Stability and predictability of the classification of mild
cognitive impairment as assessed by episodic memory test performance over time.
Neurocase, 11(1), 72-79.
De Renzi, A., & Vignolo, L. A. (1962). Token test: A sensitive test to detect receptive
disturbances in aphasics. Brain: a journal of neurology.
Dobie, D. (2002). Depression, dementia, and pseudodementia. Paper presented at the Seminars
in clinical neuropsychiatry.
Duong, A., Giroux, F., Tardif, A., & Ska, B. (2005). The heterogeneity of picture-supported
narratives in Alzheimer's disease. Brain Lang, 93(2), 173-184.
doi:10.1016/j.bandl.2004.10.007
Ehrlich, J. S., Obler, L. K., & Clark, L. (1997). Ideational and semantic contributions to narrative
production in adults with dementia of the Alzheimer's type. J Commun Disord, 30(2), 79-
98; quiz 98-79.
Forbes-McKay, K., Shanks, M. F., & Venneri, A. (2013). Profiling spontaneous speech decline
in Alzheimer's disease: a longitudinal study. Acta neuropsychiatrica, 25(06), 320-327.
Forbes-McKay, K. E., & Venneri, A. (2005). Detecting subtle spontaneous language decline in
early Alzheimer's disease with a picture description task. Neurol Sci, 26(4), 243-254.
doi:10.1007/s10072-005-0467-9
Forbes, K. E., Venneri, A., & Shanks, M. F. (2001). Distinct patterns of spontaneous speech
deterioration: an early predictor of Alzheimer's disease. Brain Cogn, 48(2-3), 356-361.
Forbes, K. E., Venneri, A., & Shanks, M. F. (2002). Distinct patterns of spontaneous speech
deterioration: an early predictor of Alzheimer's disease. Brain Cogn, 48(2-3), 356-361.
Fraser, K. C., Meltzer, J. A., Graham, N. L., Leonard, C., Hirst, G., Black, S. E., & Rochon, E.
(2014). Automated classification of primary progressive aphasia subtypes from narrative
speech transcripts. Cortex, 55, 43-60. doi:10.1016/j.cortex.2012.12.006
Fraser, K. C., Meltzer, J. A., & Rudzicz, F. (2015). Linguistic features identify Alzheimer's
disease in narrative speech. Journal of Alzheimer's Disease, 49(2), 407-422.
Frisoni, G. B., Fratiglioni, L., Fastbom, J., Viitanen, M., & Winblad, B. (1999). Mortality in
nondemented subjects with cognitive impairment: the influence of health-related factors.
American journal of epidemiology, 150(10), 1031-1044.
Garrard, P., Haigh, A.-M., & de Jager, C. (2011). Techniques for transcribers: assessing and
improving consistency in transcripts of spoken language. Literary and Linguistic
Computing, fqr018.
50
Garrard, P., Maloney, L. M., Hodges, J. R., & Patterson, K. (2005). The effects of very early
Alzheimer's disease on the characteristics of writing by a renowned author. Brain, 128(Pt
2), 250-260. doi:10.1093/brain/awh341
Giles, E., Patterson, K., & Hodges, J. R. (1996). Performance on the Boston Cookie Theft picture
description task in patients with early dementia of the Alzheimer's type: Missing
information. Aphasiology, 10(4), 395-408.
Gitlin, L. N., Winter, L., Dennis, M. P., Hodgson, N., & Hauck, W. W. (2010). Targeting and
managing behavioral symptoms in individuals with dementia: A randomized trial of a
nonpharmacological intervention. Journal of the American Geriatrics Society, 58(8),
1465-1474.
Goodglass, H., & Kaplan, E. (1983). Boston diagnostic aphasia examination booklet: Lea &
Febiger.
Gorno-Tempini, M., Hillis, A., Weintraub, S., Kertesz, A., Mendez, M., Cappa, S. e., . . . Boeve,
B. (2011). Classification of primary progressive aphasia and its variants. Neurology,
76(11), 1006-1014.
Grossman, M., D'Esposito, M., Hughes, E., Onishi, K., Biassou, N., White-Devine, T., &
Robinson, K. (1996). Language comprehension profiles in Alzheimer's disease, multi-
infarct dementia, and frontotemporal degeneration. Neurology, 47(1), 183-189.
Groves-Wright, K., Neils-Strunjas, J., Burnett, R., & O'Neill, M. J. (2004). A comparison of
verbal and written language in Alzheimer's disease. J Commun Disord, 37(2), 109-130.
doi:10.1016/j.jcomdis.2003.08.004
Halliday, M. A. K., & Hasan, R. (2014). Cohesion in english: Routledge.
Hart, D., Craig, D., Compton, S., Critchlow, S., Kerrigan, B., McIlroy, S., & Passmore, A.
(2003). A retrospective study of the behavioural and psychological symptoms of mid and
late phase Alzheimer's disease. Int J Geriatr Psychiatry, 18(11), 1037-1042.
Hier, D. B., Hagenlocker, K., & Shindler, A. G. (1985). Language disintegration in dementia:
effects of etiology and severity. Brain Lang, 25(1), 117-133.
Jack, C. R., Jr., Albert, M. S., Knopman, D. S., McKhann, G. M., Sperling, R. A., Carrillo, M.
C., . . . Phelps, C. H. (2011). Introduction to the recommendations from the National
Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for
Alzheimer's disease. Alzheimers Dement, 7(3), 257-262. doi:10.1016/j.jalz.2011.03.004
Kave, G., & Goral, M. (2016). Word retrieval in picture descriptions produced by individuals
with Alzheimer's disease. Journal of Clinical and Experimental Neuropsychology, 38(9),
958-966. doi:10.1080/13803395.2016.1179266
Kavé, G., & Goral, M. (2016). Word retrieval in picture descriptions produced by individuals
with Alzheimer’s disease. Journal of Clinical and Experimental Neuropsychology, 38(9),
958-966.
Kave, G., & Levy, Y. (2003). Morphology in picture descriptions provided by persons with
Alzheimer's disease. J Speech Lang Hear Res, 46(2), 341-352.
51
Kavé, G., & Levy, Y. (2003). Morphology in picture descriptions provided by persons with
Alzheimer's disease. Journal of Speech, Language, and Hearing Research, 46(2), 341-
352.
Kemper, S., Thompson, M., & Marquis, J. (2001). Longitudinal change in language production:
effects of aging and dementia on grammatical complexity and propositional content.
Psychology and aging, 16(4), 600.
Kertesz, A. (1982). Western aphasia battery test manual: Psychological Corp.
König, A., Satt, A., Sorin, A., Hoory, R., Toledo-Ronen, O., Derreumaux, A., . . . Robert, P. H.
(2015). Automatic speech analysis for the assessment of patients with predementia and
Alzheimer's disease. Alzheimer's & Dementia: Diagnosis, Assessment & Disease
Monitoring, 1(1), 112-124.
Lai, Y. H., Pai, H. H., & Lin, Y. T. (2009). To be semantically-impaired or to be syntactically-
impaired: Linguistic patterns in Chinese-speaking persons with or without dementia.
Journal of Neurolinguistics, 22(5), 465-475. doi:10.1016/j.jneuroling.2009.03.004
Laine, M., Laakso, M., Vuorinen, E., & Rinne, J. (1998). Coherence and informativeness of
discourse in two dementia types. Journal of Neurolinguistics, 11(1), 79-87.
Laske, C., Sohrabi, H. R., Frost, S. M., López-de-Ipiña, K., Garrard, P., Buscema, M., . . .
O'Bryant, S. E. (2015). Innovative diagnostic tools for early detection of Alzheimer's
disease. Alzheimer's & Dementia, 11(5), 561-578.
doi:http://dx.doi.org/10.1016/j.jalz.2014.06.004
Lewin, C., Wolgers, G., & Herlitz, A. (2001). Sex differences favoring women in verbal but not
in visuospatial episodic memory. Neuropsychology, 15(2), 165.
Lira, J. O. d., Minett, T. S. C., Bertolucci, P. H. F., & Ortiz, K. Z. (2014). Analysis of word
number and content in discourse of patients with mild to moderate Alzheimer's disease.
Dementia & Neuropsychologia, 8(3), 260-265.
MacDonald, M. C., Almor, A., Henderson, V. W., Kempler, D., & Andersen, E. S. (2001).
Assessing working memory and language comprehension in Alzheimer's disease. Brain
Lang, 78(1), 17-42.
Macwhinney, B., Fromm, D., Forbes, M., & Holland, A. (2011). AphasiaBank: Methods for
Studying Discourse. Aphasiology, 25(11), 1286-1307.
doi:10.1080/02687038.2011.589893
March, E. G., Wales, R., & Pattison, P. (2006). The uses of nouns and deixis in discourse
production in Alzheimer's disease. Journal of Neurolinguistics, 19(4).
Martin, A., & Fedio, P. (1983). Word production and comprehension in Alzheimer's disease: The
breakdown of semantic knowledge. Brain Lang, 19(1), 124-141.
McKhann, G. M., Knopman, D. S., Chertkow, H., Hyman, B. T., Jack, C. R., Jr., Kawas, C. H., .
. . Phelps, C. H. (2011). The diagnosis of dementia due to Alzheimer's disease:
recommendations from the National Institute on Aging-Alzheimer's Association

52
workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement, 7(3),
263-269. doi:10.1016/j.jalz.2011.03.005
McNamara, P., Obler, L. K., Au, R., Durso, R., & Albert, M. L. (1992). Speech monitoring skills
in Alzheimer's disease, Parkinson's disease, and normal aging. Brain Lang, 42(1), 38-51.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & and the, P. G. (2009). Preferred reporting
items for systematic reviews and meta-analyses: The prisma statement. Annals of Internal
Medicine, 151(4), 264-269. doi:10.7326/0003-4819-151-4-200908180-00135
Mueller, K. D., Koscik, R. L., LaRue, A., Clark, L. R., Hermann, B., Johnson, S. C., & Sager, M.
A. (2015). Verbal Fluency and Early Memory Decline: Results from the Wisconsin
Registry for Alzheimer's Prevention. Arch Clin Neuropsychol, 30(5), 448-457.
doi:10.1093/arclin/acv030
Mueller, K. D., Koscik, R. L., Turkstra, L. S., Riedeman, S. K., Larue, A., Clark, L. R., . . .
Johnson, S. C. (2016). Connected Language in Late Middle-Aged Adults at Risk for
Alzheimer's Disease. Journal of Alzheimers Disease, 54(4), 1539-1550. doi:10.3233/jad-
160252
Murray, L. L. (2010). Distinguishing clinical depression from early Alzheimer's disease in
elderly people: Can narrative analysis help? Aphasiology, 24(6-8), 928-939.
Nicholas, M., Obler, L. K., Albert, M. L., & Helm-Estabrooks, N. (1985). Empty speech in
Alzheimer's disease and fluent aphasia. J Speech Hear Res, 28(3), 405-410.
Nutter-Upham, K. E., Saykin, A. J., Rabin, L. A., Roth, R. M., Wishart, H. A., Pare, N., &
Flashman, L. A. (2008). Verbal fluency performance in amnestic MCI and older adults
with cognitive complaints. Arch Clin Neuropsychol, 23(3), 229-241.
doi:10.1016/j.acn.2008.01.005
Oren, S., Willerton, C., & Small, J. (2014). Effects of Spaced Retrieval Training on Semantic
Memory in Alzheimer's Disease: A Systematic Review. Journal of Speech, Language,
and Hearing Research, 57(1), 247-270.
Petersen, R. C., Smith, G. E., Waring, S. C., Ivnik, R. J., Tangalos, E. G., & Kokmen, E. (1999).
Mild cognitive impairment: clinical characterization and outcome. Archives of
Neurology, 56(3), 303-308.
Price, B. H., Gurvit, H., Weintraub, S., Geula, C., Leimkuhler, E., & Mesulam, M. (1993).
Neuropsychological patterns and language deficits in 20 consecutive cases of autopsy-
confirmed Alzheimer's disease. Archives of Neurology, 50(9), 931-937.
Rao, J. K., Anderson, L. A., Inui, T. S., & Frankel, R. M. (2007). Communication interventions
make a difference in conversations between physicians and patients: a systematic review
of the evidence. Medical care, 45(4), 340-349.
Rentoumi, V., Raoufian, L., Ahmed, S., de Jager, C. A., & Garrard, P. (2014). Features and
machine learning classification of connected speech samples from patients with autopsy
proven Alzheimer's disease with and without additional vascular pathology. J Alzheimers
Dis, 42 Suppl 3, S3-17. doi:10.3233/JAD-140555
53
Riley, K. P., Snowdon, D. A., Desrosiers, M. F., & Markesbery, W. R. (2005). Early life
linguistic ability, late life cognitive function, and neuropathology: findings from the Nun
Study. Neurobiology of aging, 26(3), 341-347.
Ripich, D. N., Fritsch, T., Ziol, E., & Durand, E. (2000). Compensatory strategies in picture
description across severity levels in Alzheimer's disease: A longitudinal study. Am J
Alzheimers Dis Other Demen, 15(4), 217-228.
Ripich, D. N., & Terrell, B. Y. (1988). Patterns of discourse cohesion and coherence in
Alzheimer's disease. J Speech Hear Disord, 53(1), 8-15.
Sajjadi, S. A., Patterson, K., Tomek, M., & Nestor, P. J. (2012). Abnormalities of connected
speech in semantic dementia vs Alzheimer's disease. Aphasiology, 26(6), 847-866.
doi:10.1080/02687038.2012.654933
Savundranayagam, M. Y., Hummert, M. L., & Montgomery, R. J. (2005). Investigating the
effects of communication problems on caregiver burden. The Journals of Gerontology
Series B: Psychological Sciences and Social Sciences, 60(1), S48-S55.
Savundranayagam, M. Y., & Orange, J. (2014). Matched and mismatched appraisals of the
effectiveness of communication strategies by family caregivers of persons with
Alzheimer's disease. International Journal of Language & Communication Disorders,
49(1), 49-59.
Semenza, C., & Cipolotti, L. (1989). Neuropsicologia con carta e matita. Padova: Cleup Editrice
Padova.
Shimada, M., Meguro, K., Yamazaki, H., Horikawa, A., Hayasaka, C., Yamaguchi, S., . . .
Yamadori, A. (1998). Impaired verbal description ability assessed by the Picture
Description Task in Alzheimer's disease. Archives of Gerontology and Geriatrics, 27(1),
57-65.
Sitek, E. J., Kluj-Kozłowska, K., Barczak, A., Kozłowski, M., Wieczorek, D., Przewłócka, A., . .
. Sławek, J. (2015). Overlapping and distinguishing features of descriptive speech in
Richardson variant of progressive supranuclear palsy and non-fluent progressive aphasia.
Postępy Psychiatrii i Neurologii, 24(2), 62-67.
Small, S. A., Perera, G. M., DeLaPaz, R., Mayeux, R., & Stern, Y. (1999). Differential regional
dysfunction of the hippocampal formation among elderly with memory decline and
Alzheimer's disease. Annals of neurology, 45(4), 466-472.
Smith, S. R., Chenery, H. J., & Murdoch, B. E. (1989). Semantic abilities in dementia of the
Alzheimer type. II. Grammatical semantics. Brain Lang, 36(4), 533-542.
Snowdon, D. A., Kemper, S. J., Mortimer, J. A., Greiner, L. H., Wekstein, D. R., & Markesbery,
W. R. (1996). Linguistic ability in early life and cognitive function and Alzheimer's
disease in late life. Findings from the Nun Study. JAMA, 275(7), 528-532.
Sperling, R. A., Aisen, P. S., Beckett, L. A., Bennett, D. A., Craft, S., Fagan, A. M., . . . Montine,
T. J. (2011). Toward defining the preclinical stages of Alzheimer’s disease:
Recommendations from the National Institute on Aging-Alzheimer's Association

54
workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's & Dementia,
7(3), 280-292.
Swinburn, K., Porter, G., & Howard, D. (2004). CAT: comprehensive aphasia test: Psychology
Press.
Taler, V., & Phillips, N. A. (2008). Language performance in Alzheimer's disease and mild
cognitive impairment: a comparative review. J Clin Exp Neuropsychol, 30(5), 501-556.
doi:10.1080/13803390701550128
Testa, J. A., Ivnik, R. J., Boeve, B., Petersen, R. C., Pankratz, V. S., Knopman, D., . . . Smith, G.
E. (2004). Confrontation naming does not add incremental diagnostic utility in MCI and
Alzheimer's disease. J Int Neuropsychol Soc, 10(4), 504-512.
doi:10.1017/S1355617704104177
Tomoeda, C. K., & Bayles, K. A. (1993). Longitudinal effects of Alzheimer disease on discourse
production. Alzheimer Dis Assoc Disord.
Tomoeda, C. K., & Bayles, K. A. (1993). Longitudinal effects of Alzheimer disease on discourse
production. Alzheimer Dis Assoc Disord, 7(4), 223-236.
Tomoeda, C. K., Bayles, K. A., Trosset, M. W., Azuma, T., & McGeagh, A. (1996). Cross-
sectional analysis of Alzheimer disease effects on oral discourse in a picture description
task. Alzheimer Dis Assoc Disord, 10(4), 204-215.
Ulatowska, H. K. (1985). The aging brain: Communication in the elderly: College-Hill.
Vuorinen, E., Laine, M., & Rinne, J. (2000). Common pattern of language impairment in
vascular dementia and in Alzheimer disease. Alzheimer Dis Assoc Disord, 14(2), 81-86.
Woodward, M. (2013). Aspects of communication in Alzheimer's disease: clinical features and
treatment options. International Psychogeriatrics, 25(06), 877-885.
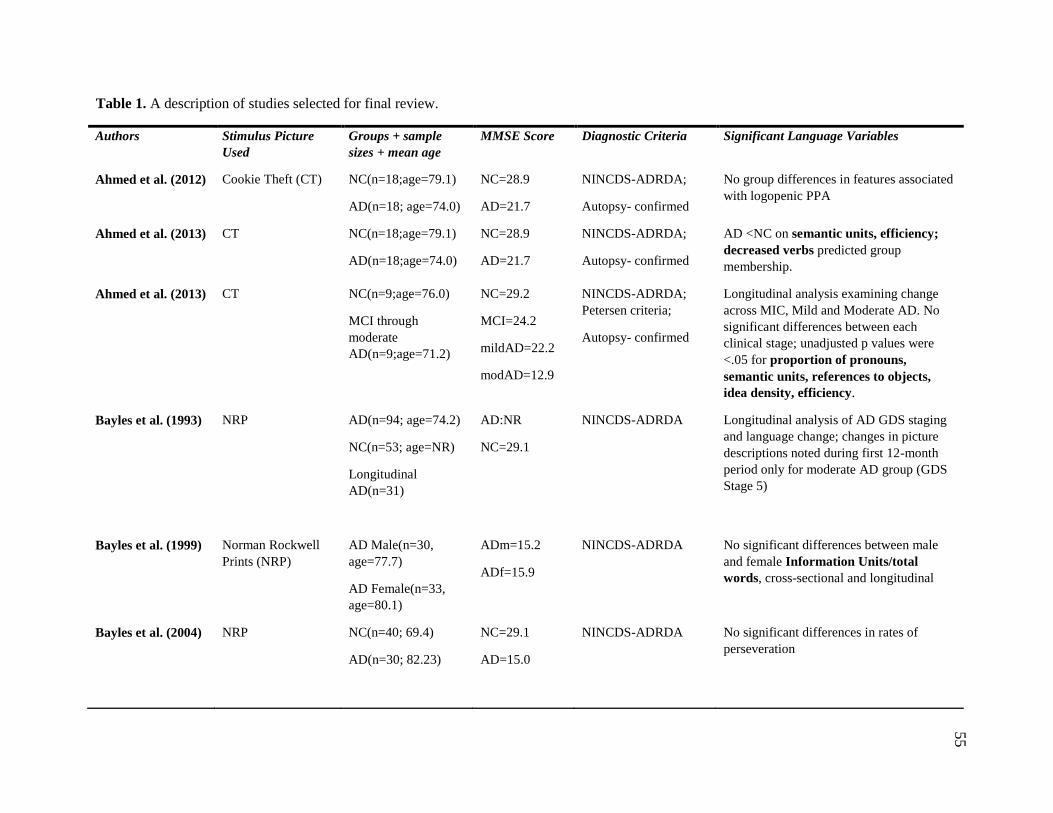
55
Table 1. A description of studies selected for final review.
Authors Stimulus Picture
Used Groups + sample
sizes + mean age MMSE Score Diagnostic Criteria Significant Language Variables
Ahmed et al. (2012) Cookie Theft (CT) NC(n=18;age=79.1)
AD(n=18; age=74.0)
NC=28.9
AD=21.7
NINCDS-ADRDA;
Autopsy- confirmed
No group differences in features associated
with logopenic PPA
Ahmed et al. (2013) CT NC(n=18;age=79.1)
AD(n=18;age=74.0)
NC=28.9
AD=21.7
NINCDS-ADRDA;
Autopsy- confirmed
AD <NC on semantic units, efficiency;
decreased verbs predicted group
membership.
Ahmed et al. (2013) CT NC(n=9;age=76.0)
MCI through
moderate
AD(n=9;age=71.2)
NC=29.2
MCI=24.2
mildAD=22.2
modAD=12.9
NINCDS-ADRDA;
Petersen criteria;
Autopsy- confirmed
Longitudinal analysis examining change
across MIC, Mild and Moderate AD. No
significant differences between each
clinical stage; unadjusted p values were
<.05 for proportion of pronouns,
semantic units, references to objects,
idea density, efficiency.
Bayles et al. (1993) NRP AD(n=94; age=74.2)
NC(n=53; age=NR)
Longitudinal
AD(n=31)
AD:NR
NC=29.1
NINCDS-ADRDA Longitudinal analysis of AD GDS staging
and language change; changes in picture
descriptions noted during first 12-month
period only for moderate AD group (GDS
Stage 5)
Bayles et al. (1999) Norman Rockwell
Prints (NRP)
AD Male(n=30,
age=77.7)
AD Female(n=33,
age=80.1)
ADm=15.2
ADf=15.9
NINCDS-ADRDA No significant differences between male
and female Information Units/total
words, cross-sectional and longitudinal
Bayles et al. (2004) NRP NC(n=40; 69.4)
AD(n=30; 82.23)
NC=29.1
AD=15.0
NINCDS-ADRDA No significant differences in rates of
perseveration
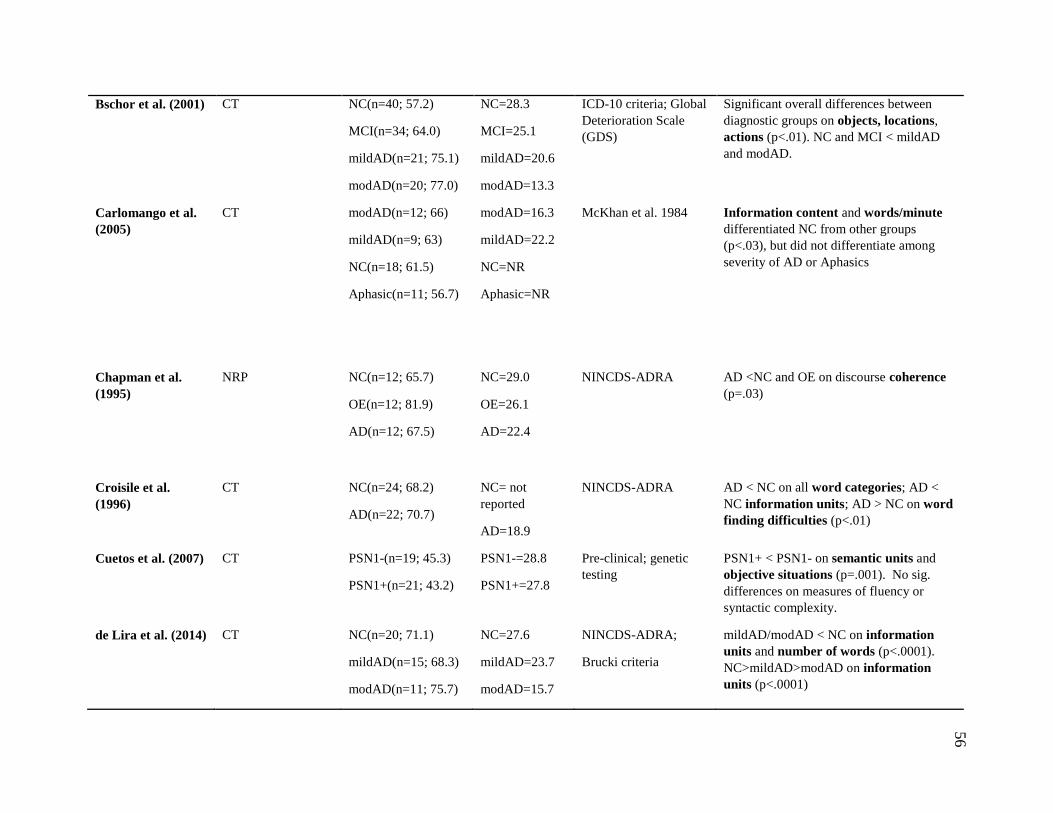
56
Bschor et al. (2001) CT NC(n=40; 57.2)
MCI(n=34; 64.0)
mildAD(n=21; 75.1)
modAD(n=20; 77.0)
NC=28.3
MCI=25.1
mildAD=20.6
modAD=13.3
ICD-10 criteria; Global
Deterioration Scale
(GDS)
Significant overall differences between
diagnostic groups on objects, locations,
actions (p<.01). NC and MCI < mildAD
and modAD.
Carlomango et al.
(2005)
CT modAD(n=12; 66)
mildAD(n=9; 63)
NC(n=18; 61.5)
Aphasic(n=11; 56.7)
modAD=16.3
mildAD=22.2
NC=NR
Aphasic=NR
McKhan et al. 1984 Information content and words/minute
differentiated NC from other groups
(p<.03), but did not differentiate among
severity of AD or Aphasics
Chapman et al.
(1995)
NRP NC(n=12; 65.7)
OE(n=12; 81.9)
AD(n=12; 67.5)
NC=29.0
OE=26.1
AD=22.4
NINCDS-ADRA AD <NC and OE on discourse coherence
(p=.03)
Croisile et al.
(1996)
CT NC(n=24; 68.2)
AD(n=22; 70.7)
NC= not
reported
AD=18.9
NINCDS-ADRA AD < NC on all word categories; AD <
NC information units; AD > NC on word
finding difficulties (p<.01)
Cuetos et al. (2007) CT PSN1-(n=19; 45.3)
PSN1+(n=21; 43.2)
PSN1-=28.8
PSN1+=27.8
Pre-clinical; genetic
testing PSN1+ < PSN1- on semantic units and
objective situations (p=.001). No sig.
differences on measures of fluency or
syntactic complexity.
de Lira et al. (2014) CT NC(n=20; 71.1)
mildAD(n=15; 68.3)
modAD(n=11; 75.7)
NC=27.6
mildAD=23.7
modAD=15.7
NINCDS-ADRA;
Brucki criteria
mildAD/modAD < NC on information
units and number of words (p<.0001).
NC>mildAD>modAD on information
units (p<.0001)
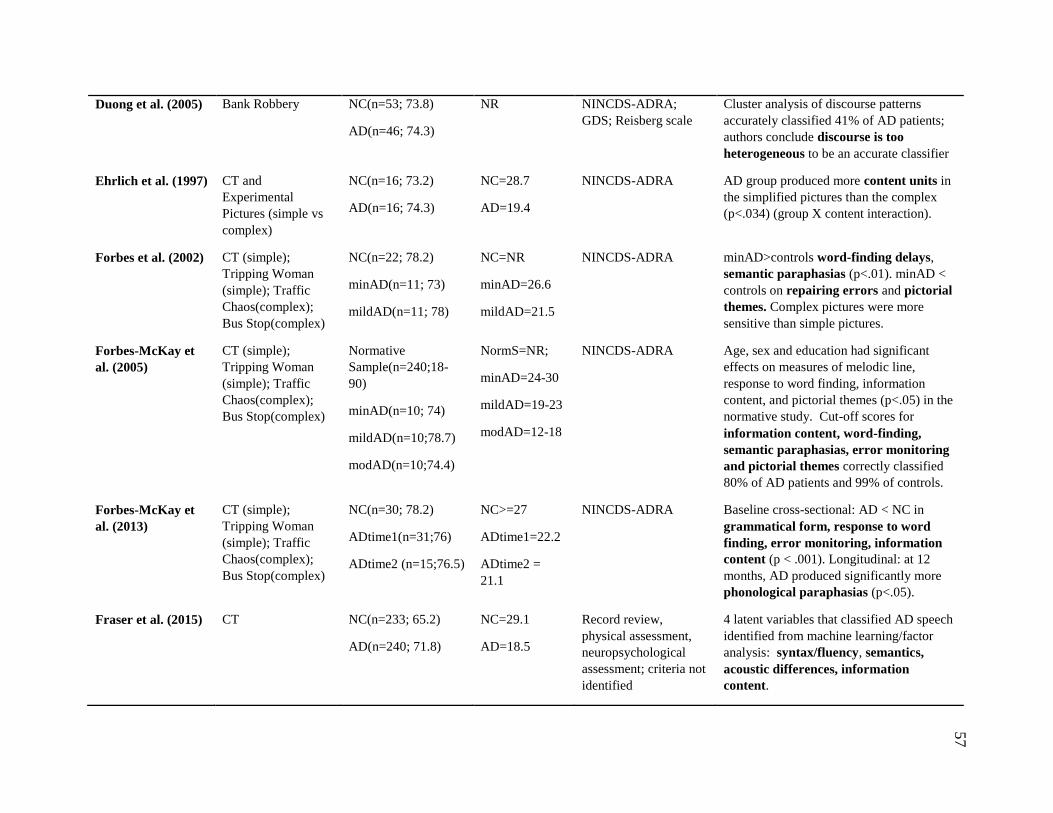
57
Duong et al. (2005) Bank Robbery NC(n=53; 73.8)
AD(n=46; 74.3)
NR NINCDS-ADRA;
GDS; Reisberg scale Cluster analysis of discourse patterns
accurately classified 41% of AD patients;
authors conclude discourse is too
heterogeneous to be an accurate classifier
Ehrlich et al. (1997) CT and
Experimental
Pictures (simple vs
complex)
NC(n=16; 73.2)
AD(n=16; 74.3)
NC=28.7
AD=19.4
NINCDS-ADRA AD group produced more content units in
the simplified pictures than the complex
(p<.034) (group X content interaction).
Forbes et al. (2002) CT (simple);
Tripping Woman
(simple); Traffic
Chaos(complex);
Bus Stop(complex)
NC(n=22; 78.2)
minAD(n=11; 73)
mildAD(n=11; 78)
NC=NR
minAD=26.6
mildAD=21.5
NINCDS-ADRA minAD>controls word-finding delays,
semantic paraphasias (p<.01). minAD <
controls on repairing errors and pictorial
themes. Complex pictures were more
sensitive than simple pictures.
Forbes-McKay et
al. (2005)
CT (simple);
Tripping Woman
(simple); Traffic
Chaos(complex);
Bus Stop(complex)
Normative
Sample(n=240;18-
90)
minAD(n=10; 74)
mildAD(n=10;78.7)
modAD(n=10;74.4)
NormS=NR;
minAD=24-30
mildAD=19-23
modAD=12-18
NINCDS-ADRA Age, sex and education had significant
effects on measures of melodic line,
response to word finding, information
content, and pictorial themes (p<.05) in the
normative study. Cut-off scores for
information content, word-finding,
semantic paraphasias, error monitoring
and pictorial themes correctly classified
80% of AD patients and 99% of controls.
Forbes-McKay et
al. (2013)
CT (simple);
Tripping Woman
(simple); Traffic
Chaos(complex);
Bus Stop(complex)
NC(n=30; 78.2)
ADtime1(n=31;76)
ADtime2 (n=15;76.5)
NC>=27
ADtime1=22.2
ADtime2 =
21.1
NINCDS-ADRA Baseline cross-sectional: AD < NC in
grammatical form, response to word
finding, error monitoring, information
content (p < .001). Longitudinal: at 12
months, AD produced significantly more
phonological paraphasias (p<.05).
Fraser et al. (2015) CT NC(n=233; 65.2)
AD(n=240; 71.8)
NC=29.1
AD=18.5
Record review,
physical assessment,
neuropsychological
assessment; criteria not
identified
4 latent variables that classified AD speech
identified from machine learning/factor
analysis: syntax/fluency, semantics,
acoustic differences, information
content.
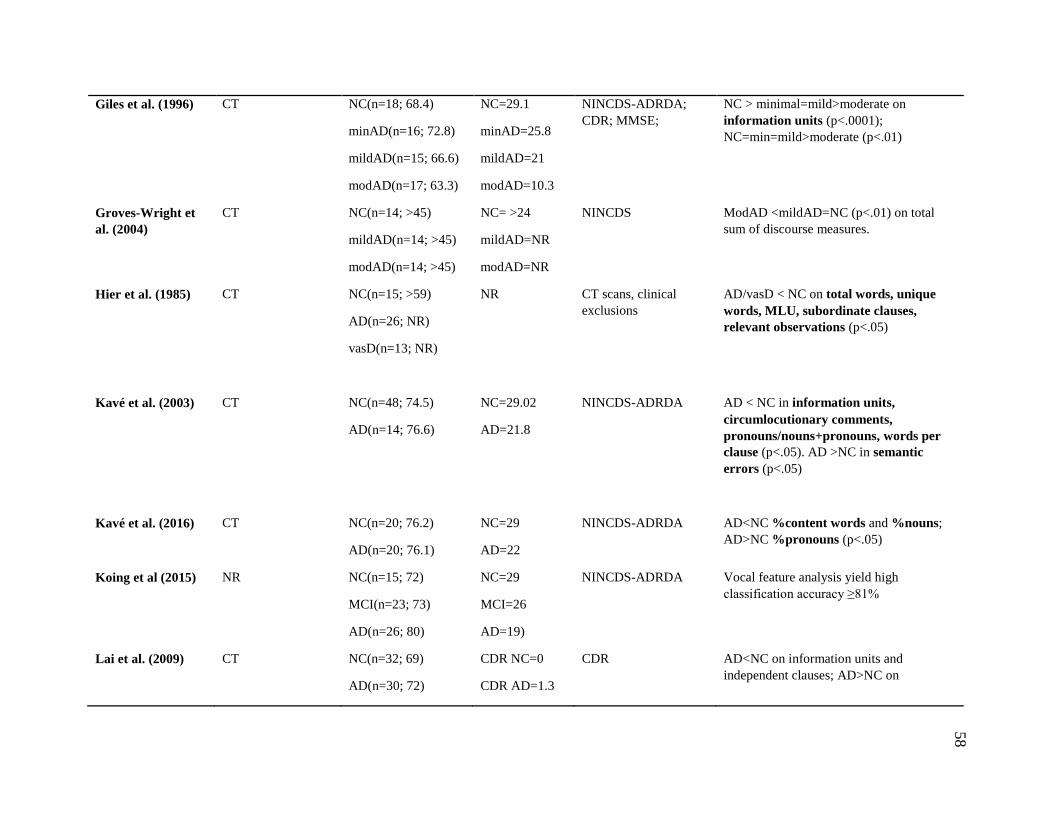
58
Giles et al. (1996) CT NC(n=18; 68.4)
minAD(n=16; 72.8)
mildAD(n=15; 66.6)
modAD(n=17; 63.3)
NC=29.1
minAD=25.8
mildAD=21
modAD=10.3
NINCDS-ADRDA;
CDR; MMSE; NC > minimal=mild>moderate on
information units (p<.0001);
NC=min=mild>moderate (p<.01)
Groves-Wright et
al. (2004)
CT NC(n=14; >45)
mildAD(n=14; >45)
modAD(n=14; >45)
NC= >24
mildAD=NR
modAD=NR
NINCDS ModAD <mildAD=NC (p<.01) on total
sum of discourse measures.
Hier et al. (1985) CT NC(n=15; >59)
AD(n=26; NR)
vasD(n=13; NR)
NR CT scans, clinical
exclusions AD/vasD < NC on total words, unique
words, MLU, subordinate clauses,
relevant observations (p<.05)
Kavé et al. (2003) CT NC(n=48; 74.5)
AD(n=14; 76.6)
NC=29.02
AD=21.8
NINCDS-ADRDA AD < NC in information units,
circumlocutionary comments,
pronouns/nouns+pronouns, words per
clause (p<.05). AD >NC in semantic
errors (p<.05)
Kavé et al. (2016) CT NC(n=20; 76.2)
AD(n=20; 76.1)
NC=29
AD=22
NINCDS-ADRDA AD<NC %content words and %nouns;
AD>NC %pronouns (p<.05)
Koing et al (2015) NR NC(n=15; 72)
MCI(n=23; 73)
AD(n=26; 80)
NC=29
MCI=26
AD=19)
NINCDS-ADRDA Vocal feature analysis yield high
classification accuracy ≥81%
Lai et al. (2009) CT NC(n=32; 69)
AD(n=30; 72)
CDR NC=0
CDR AD=1.3
CDR AD<NC on information units and
independent clauses; AD>NC on
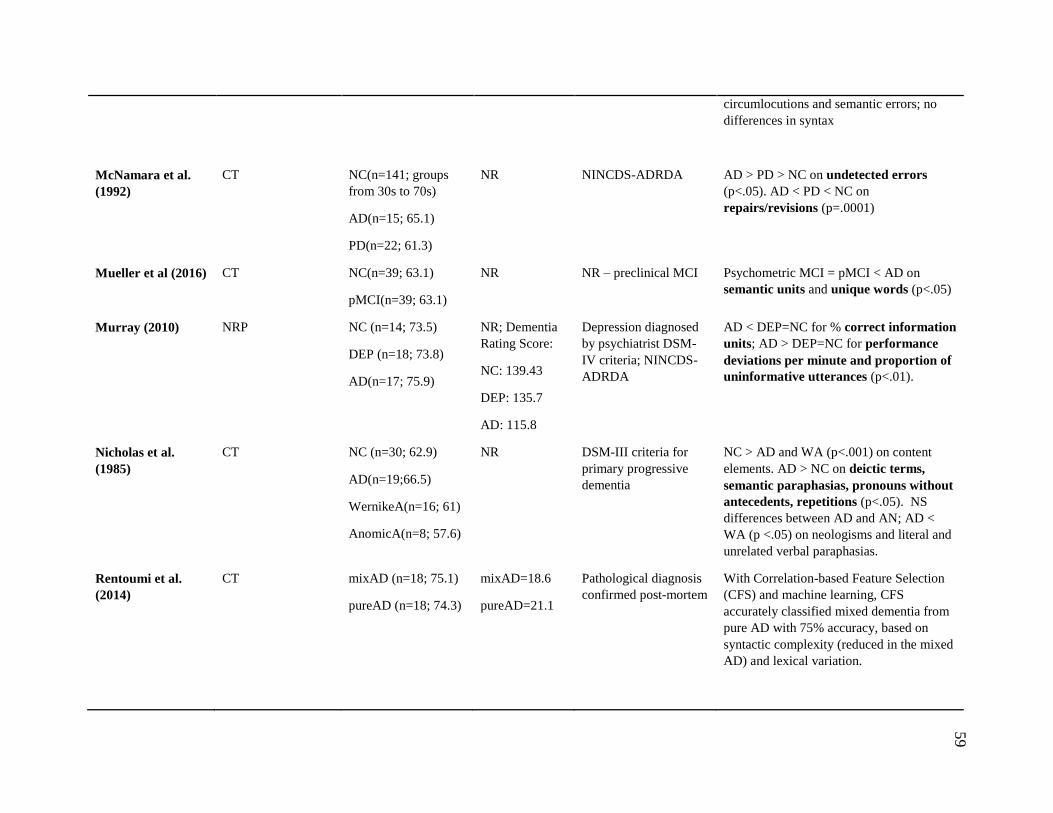
59
circumlocutions and semantic errors; no
differences in syntax
McNamara et al.
(1992)
CT NC(n=141; groups
from 30s to 70s)
AD(n=15; 65.1)
PD(n=22; 61.3)
NR NINCDS-ADRDA AD > PD > NC on undetected errors
(p<.05). AD < PD < NC on
repairs/revisions (p=.0001)
Mueller et al (2016) CT NC(n=39; 63.1)
pMCI(n=39; 63.1)
NR NR – preclinical MCI Psychometric MCI = pMCI < AD on
semantic units and unique words (p<.05)
Murray (2010) NRP NC (n=14; 73.5)
DEP (n=18; 73.8)
AD(n=17; 75.9)
NR; Dementia
Rating Score:
NC: 139.43
DEP: 135.7
AD: 115.8
Depression diagnosed
by psychiatrist DSM-
IV criteria; NINCDS-
ADRDA
AD < DEP=NC for % correct information
units; AD > DEP=NC for performance
deviations per minute and proportion of
uninformative utterances (p<.01).
Nicholas et al.
(1985)
CT NC (n=30; 62.9)
AD(n=19;66.5)
WernikeA(n=16; 61)
AnomicA(n=8; 57.6)
NR DSM-III criteria for
primary progressive
dementia
NC > AD and WA (p<.001) on content
elements. AD > NC on deictic terms,
semantic paraphasias, pronouns without
antecedents, repetitions (p<.05). NS
differences between AD and AN; AD <
WA (p <.05) on neologisms and literal and
unrelated verbal paraphasias.
Rentoumi et al.
(2014)
CT mixAD (n=18; 75.1)
pureAD (n=18; 74.3)
mixAD=18.6
pureAD=21.1
Pathological diagnosis
confirmed post-mortem With Correlation-based Feature Selection
(CFS) and machine learning, CFS
accurately classified mixed dementia from
pure AD with 75% accuracy, based on
syntactic complexity (reduced in the mixed
AD) and lexical variation.
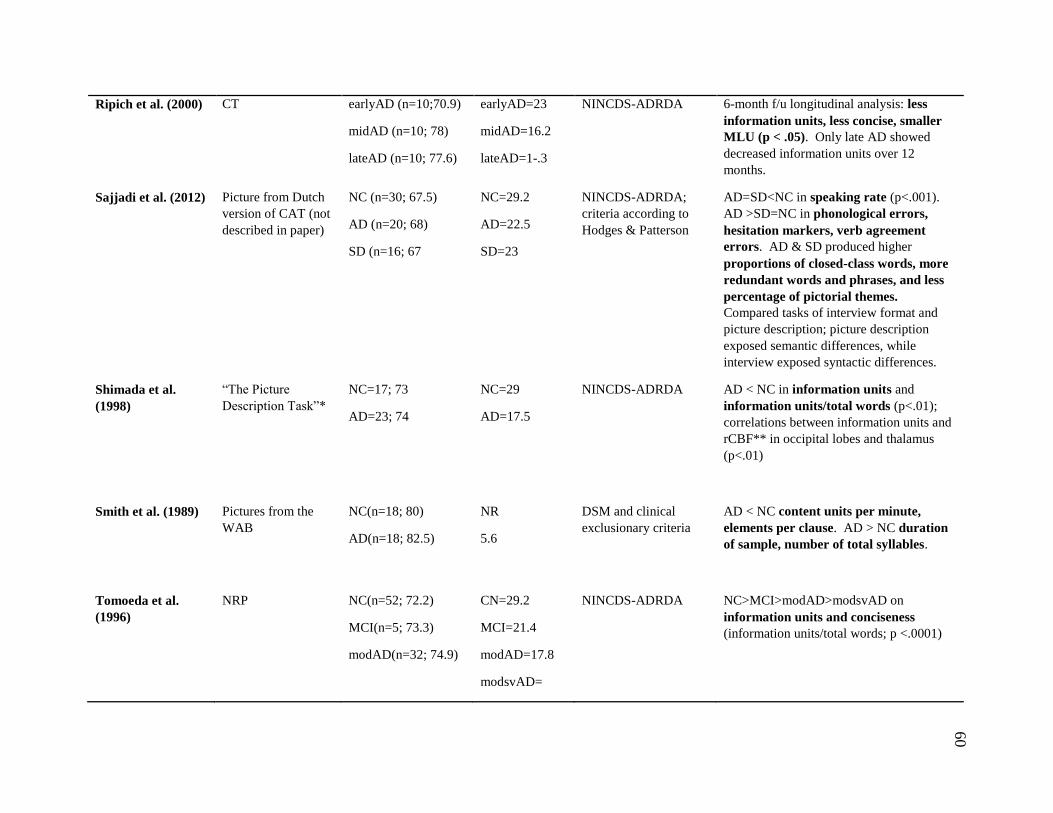
60
Ripich et al. (2000) CT earlyAD (n=10;70.9)
midAD (n=10; 78)
lateAD (n=10; 77.6)
earlyAD=23
midAD=16.2
lateAD=1-.3
NINCDS-ADRDA 6-month f/u longitudinal analysis: less
information units, less concise, smaller
MLU (p < .05). Only late AD showed
decreased information units over 12
months.
Sajjadi et al. (2012) Picture from Dutch
version of CAT (not
described in paper)
NC (n=30; 67.5)
AD (n=20; 68)
SD (n=16; 67
NC=29.2
AD=22.5
SD=23
NINCDS-ADRDA;
criteria according to
Hodges & Patterson
AD=SD<NC in speaking rate (p<.001).
AD >SD=NC in phonological errors,
hesitation markers, verb agreement
errors. AD & SD produced higher
proportions of closed-class words, more
redundant words and phrases, and less
percentage of pictorial themes.
Compared tasks of interview format and
picture description; picture description
exposed semantic differences, while
interview exposed syntactic differences.
Shimada et al.
(1998)
“The Picture
Description Task”*
NC=17; 73
AD=23; 74
NC=29
AD=17.5
NINCDS-ADRDA AD < NC in information units and
information units/total words (p<.01);
correlations between information units and
rCBF** in occipital lobes and thalamus
(p<.01)
Smith et al. (1989) Pictures from the
WAB NC(n=18; 80)
AD(n=18; 82.5)
NR
5.6
DSM and clinical
exclusionary criteria AD < NC content units per minute,
elements per clause. AD > NC duration
of sample, number of total syllables.
Tomoeda et al.
(1996)
NRP NC(n=52; 72.2)
MCI(n=5; 73.3)
modAD(n=32; 74.9)
CN=29.2
MCI=21.4
modAD=17.8
modsvAD=
NINCDS-ADRDA NC>MCI>modAD>modsvAD on
information units and conciseness
(information units/total words; p <.0001)
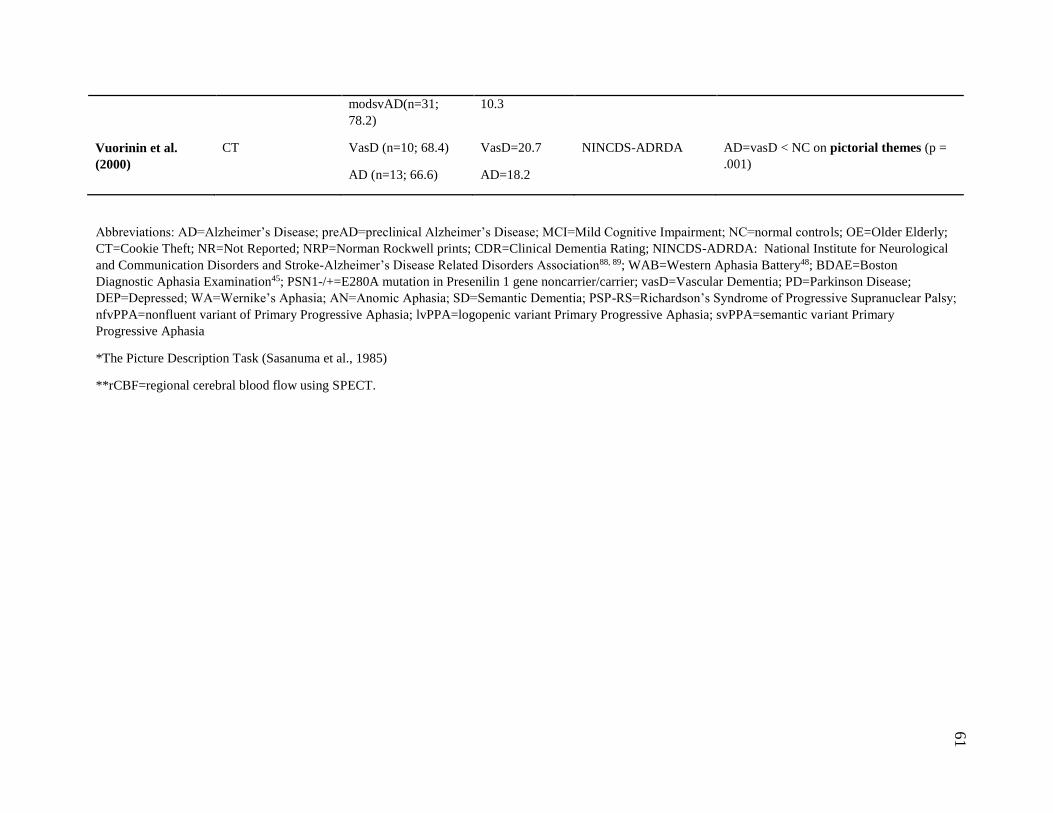
61
modsvAD(n=31;
78.2) 10.3
Vuorinin et al.
(2000)
CT VasD (n=10; 68.4)
AD (n=13; 66.6)
VasD=20.7
AD=18.2
NINCDS-ADRDA AD=vasD < NC on pictorial themes (p =
.001)
Abbreviations: AD=Alzheimer’s Disease; preAD=preclinical Alzheimer’s Disease; MCI=Mild Cognitive Impairment; NC=normal controls; OE=Older Elderly;
CT=Cookie Theft; NR=Not Reported; NRP=Norman Rockwell prints; CDR=Clinical Dementia Rating; NINCDS-ADRDA: National Institute for Neurological
and Communication Disorders and Stroke-Alzheimer’s Disease Related Disorders Association88, 89; WAB=Western Aphasia Battery48; BDAE=Boston
Diagnostic Aphasia Examination45; PSN1-/+=E280A mutation in Presenilin 1 gene noncarrier/carrier; vasD=Vascular Dementia; PD=Parkinson Disease;
DEP=Depressed; WA=Wernike’s Aphasia; AN=Anomic Aphasia; SD=Semantic Dementia; PSP-RS=Richardson’s Syndrome of Progressive Supranuclear Palsy;
nfvPPA=nonfluent variant of Primary Progressive Aphasia; lvPPA=logopenic variant Primary Progressive Aphasia; svPPA=semantic variant Primary
Progressive Aphasia
*The Picture Description Task (Sasanuma et al., 1985)
**rCBF=regional cerebral blood flow using SPECT.
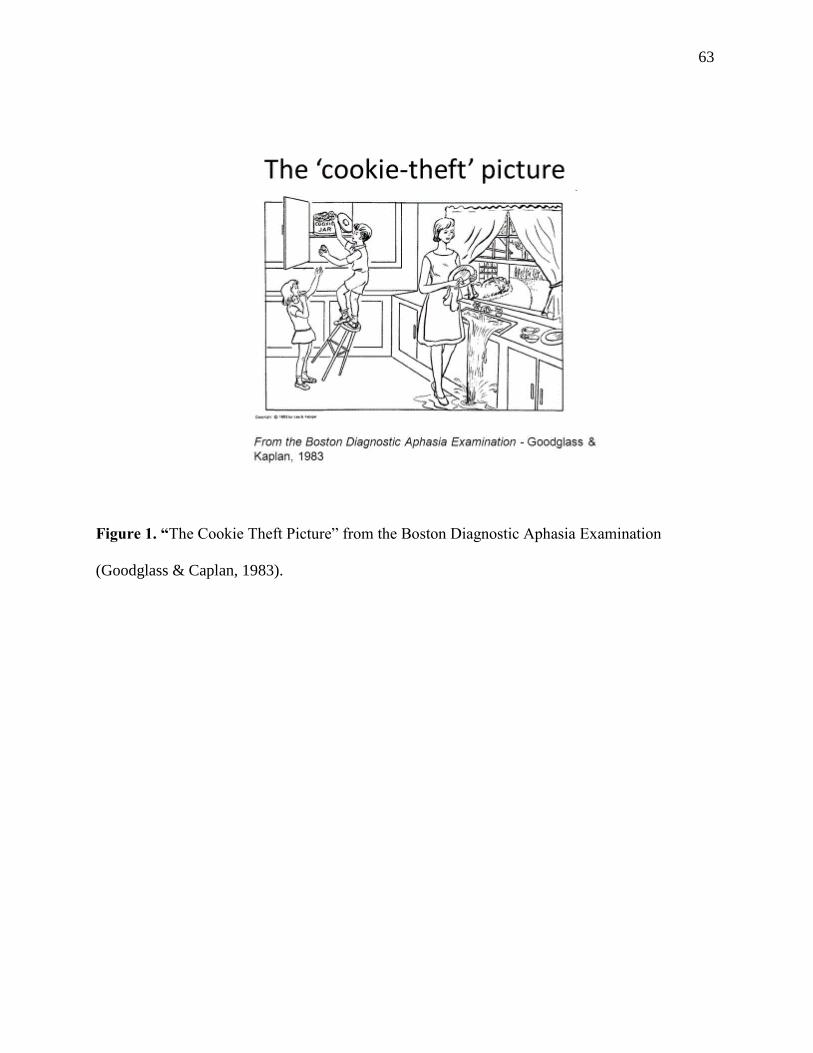
63
Figure 1. “The Cookie Theft Picture” from the Boston Diagnostic Aphasia Examination
(Goodglass & Caplan, 1983).
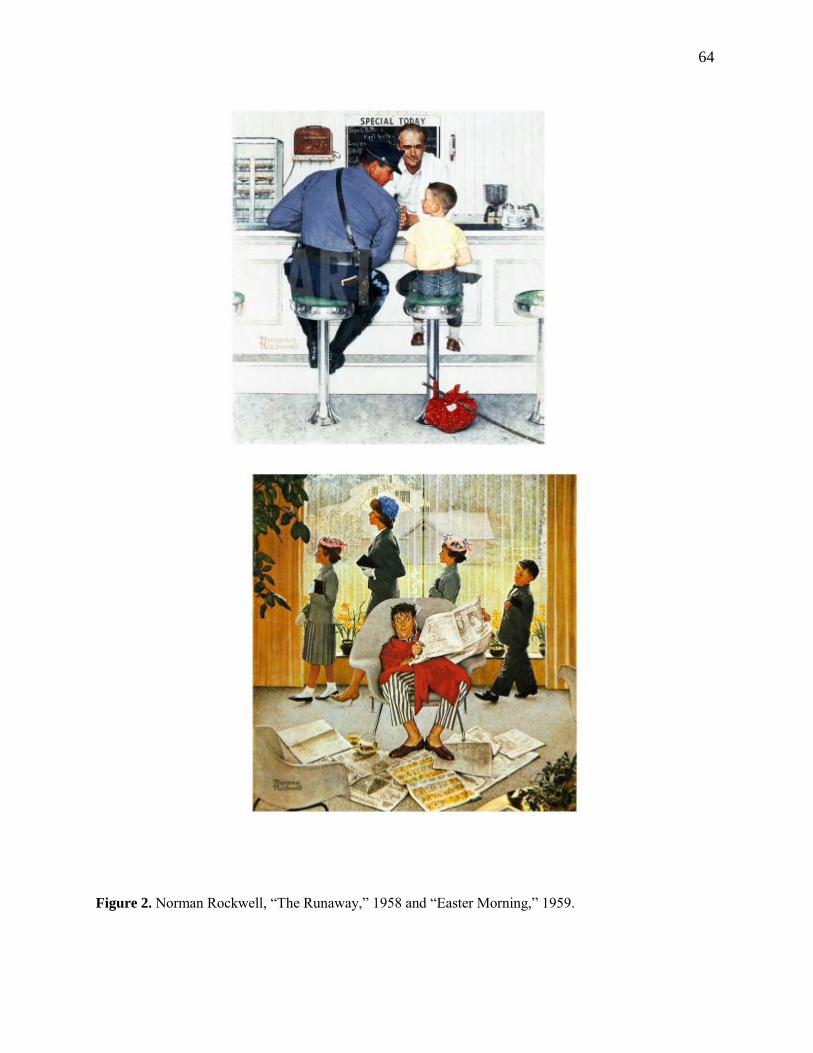
64
Figure 2. Norman Rockwell, “The Runaway,” 1958 and “Easter Morning,” 1959.

65
Figure 3. “The Picnic Scene” from the Western Aphasia Battery (Kertesz, 2006).
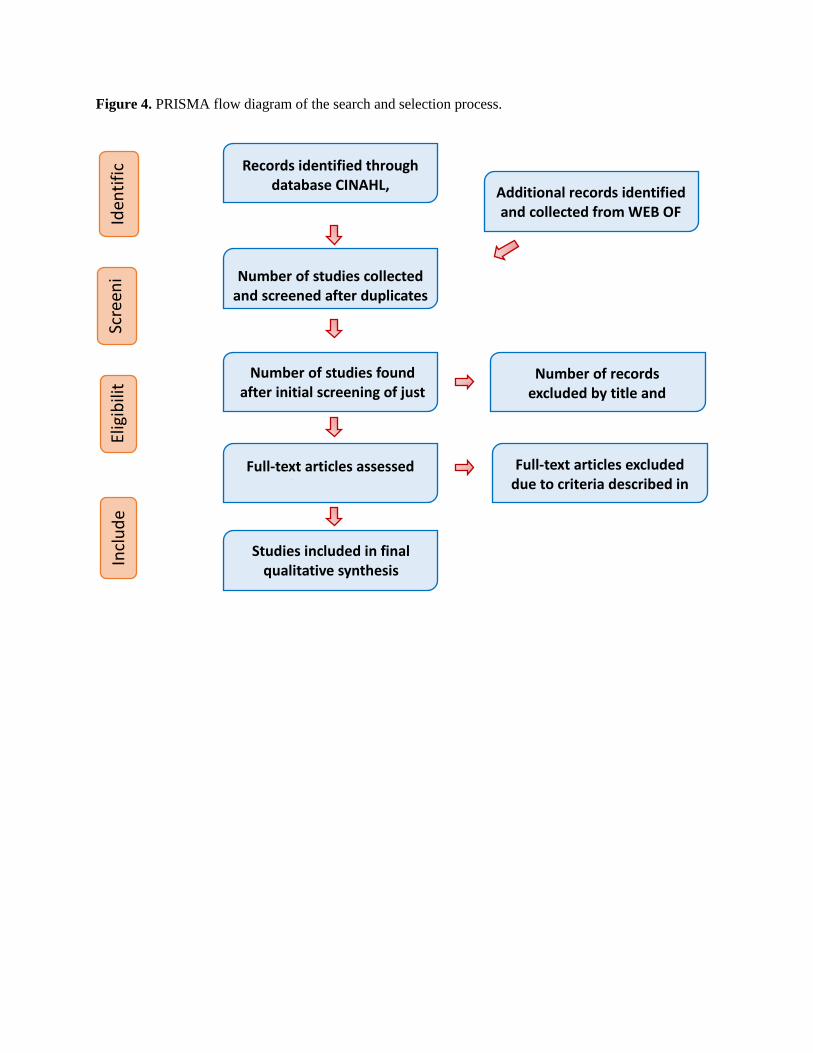
Figure 4. PRISMA flow diagram of the search and selection process.
Iden
tifi
cat
ion
Scre
eni
ng
Elig
ibili
ty
Incl
ud
ed
Records identified through database CINAHL,
PSYCHINFO, PUBMED search Additional records identified and collected from WEB OF
SCIENCE and SCOPUS
Number of studies collected and screened after duplicates
were removed
Number of studies found after initial screening of just
title and abstract
Number of records excluded by title and
abstract
Full-text articles assessed for eligibility
Full-text articles excluded due to criteria described in
the methods section.
Studies included in final qualitative synthesis
(n= 36)
67
CHAPTER 3
Manuscript 2: Connected Language in Late Middle-Aged
Adults at Risk for Alzheimer’s Disease
A cross-sectional study

68
Connected Language in Late Middle-Aged Adults at Risk for Alzheimer’s Disease
Published in final edited form as: J Alzheimers Dis. 2016 Oct18; 54(4): 1539-1550;
doi: 10.3233/JAD-160252
Kimberly Diggle Mueller1,5; Rebecca L. Koscik1; Lyn S. Turkstra5; Sarah K. Riedeman5;
Asenath LaRue1; Lindsay R. Clark1,3, Bruce Hermann1,4; Mark A. Sager1; Sterling C. Johnson2,1,3
1Wisconsin Alzheimer’s Institute, University of Wisconsin School of Medicine and Public
Health, Madison, WI
2Geriatric Research Education and Clinical Center, William S. Middleton Memorial VA
Hospital, Madison WI 53705
3Wisconsin Alzheimer’s Disease Research Center, University of Wisconsin School of Medicine
and Public Health, Madison, WI
4Department of Neurology, University of Wisconsin School of Medicine and Public Health,
Madison, WI
5Department of Communication Sciences & Disorders, University of Wisconsin, Madison, WI
Corresponding author:
Kimberly D Mueller, MS, Wisconsin Alzheimer’s Institute, Wisconsin Alumni Research
Foundation – 9th Floor, University of Wisconsin School of Medicine and Public Health, Madison,
Wisconsin 53792, USA. Phone: 608-829-3300; fax: 608-829-3315 Email: [email protected]

69
ABSTRACT
Connected language is often impaired among people with Alzheimer’s Disease (AD), yet little is
known about when language difficulties first emerge on the path to a clinical diagnosis. The
objective of this study was to determine whether individuals with psychometric (preclinical)
evidence of amnestic Mild Cognitive Impairment (MCI) (pMCI) showed deficits in connected
language measures. Participants were 39 pMCI and 39 cognitively healthy (CH) adults drawn from
the Wisconsin Registry for Alzheimer’s Prevention, who were matched for age, literacy, and sex.
Participants completed a connected language task in which they described the Cookie Theft picture
from the Boston Diagnostic Aphasia Examination. Language samples were analyzed across 3
language domains: content, syntactic complexity, and speech fluency. Paired t-tests were used to
compare CH and pMCI groups on all variables, and Cohen’s d effect sizes were calculated for
each comparison. The CH and pMCI groups differed significantly on measures of content (e.g.,
CH group produced more semantic units, more unique words and had larger idea density, on
average, than the pMCI group). The picture description findings are consistent with previous
retrospective studies showing semantic language differences in adults with autopsy-confirmed
AD. Given that these comparisons are between cognitively healthy and pMCI individuals (before
a clinical MCI diagnosis), these findings may represent subtle language difficulty in spontaneous
speech, and may be predictive of larger language changes over time.
Key Words: Speech; Mild Cognitive Impairment; Alzheimer’s Disease; Semantics; Dementia;
Discourse; Linguistics; Language Disorders
70
INTRODUCTION
A major goal of neuropsychological research in Alzheimer’s Disease (AD) is early
detection of cognitive decline. To date much of this research has focused on identifying
individuals who meet criteria for mild cognitive impairment (MCI), because of the high risk of
converting to dementia in this group (Albert et al., 2011; Fischer et al., 2007). MCI diagnostic
criteria established by a joint National Institute on Aging and Alzheimer’s Association consensus
panel include the following: concern about cognitive decline by the person or significant other,
preservation of independence in functional abilities, and impairment in one or more cognitive
domains (Albert et al., 2011). Although episodic memory impairment is often the main cognitive
symptom of Alzheimer’s Disease, considerable research evidence suggests that the
neuropathological changes of Alzheimer’s Disease develop years or decades before the onset of
such cognitive symptoms (Alcolea et al., 2014; Jack et al., 2013; Zimmer et al., 2014).
Therefore the quest to find sensitive neuropsychological measures that are effective in detecting
very early decline, that can be differentiated from typical changes associated with aging, has
been ongoing.
In addition to episodic memory decline, declines in semantic memory have also been
described early on the continuum of Alzheimer’s Disease. Semantic memory refers to
knowledge of concepts, objects, people and words. Barbeau et al., 2012 (Barbeau et al., 2012)
found that a group with MCI performed significantly worse than controls on several semantic
memory tasks, including naming famous faces, cultural knowledge, and famous public events.
The authors argue that the semantic deficits exist without temporal gradient (i.e., deficits exist no
matter how old or recent the learning occurred), and thus may not be caused by episodic memory
deficits. The authors also found that the semantic impairments were correlated with anterior,
71
extra-hippocampal, temporal lobe brain structures as well as to the hippocampus. Didic et al.,
2011 (Didic et al., 2011) describe semantic memory as being “context-free”; that is, the recall of
previously learned facts, words or names is dissociable from the original context in which it was
learned, and is less dependent upon the hippocampus and more dependent upon anterior medial
temporal structures which appear to be affected earlier in Alzheimer’s disease. Didic et al., 2011
argue that even the more sensitive tests designed to assess episodic memory function, such as
word list learning and recall, are “context-free” by nature and difficulties may be reflective of
semantic, as well as episodic memory problems. Venneri et al., 2016 theorize that assessments
targeted toward semantic memory may be more sensitive in distinguishing normal aging
processes from preclinical AD; that is, normal aging typically results in a gradual decline in
episodic memory, while semantic memory is usually spared, if not improved, in normal aging
(Venneri et al., 2016).
Semantic memory difficulties, within the context of everyday functioning, may be
manifest by word retrieval difficulties and naming impairments, which are common complaints
in both MCI and AD. Faber-Langendoen et al. (Faber-Langendoen et al., 1988) found that 36%
of mild AD patients and 100% of severe AD patients had aphasia (i.e., impairment in some
aspect of language function) concurrent with memory impairments.
To characterize word finding problems, clinicians and researchers often use confrontation
naming tasks as a means of quantifying this difficulty. While declining performance on typical
confrontation naming tasks is evident in Alzheimer’s Disease (Taler & Phillips, 2008), and
confrontation naming tasks have been useful in staging more moderate to severe AD (Welsh,
Butters, Hughes, Mohs, & Heyman, 1992), such tests have not been useful in reliably detecting
differences in preclinical AD or MCI(Testa et al., 2004; Willers, Feldman, & Allegri, 2008) .
72
Word finding may also be evaluated by using verbal fluency tasks, in which patients are
asked to name words of a category or words beginning with a specified letter, and are often used
to assess problems with both executive function and language in Alzheimer’s Disease (Taler &
Phillips, 2008). Specifically, studies of verbal fluency in MCI have shown lower scores in those
with MCI and AD compared to age-matched controls (Clark et al., 2009; Nutter-Upham et al.,
2008; Price et al., 2012). Recently, our group found differences in verbal fluency abilities
between persons identified as “cognitively healthy” and those identified as ‘psychometric MCI’,
a construct using robust norms across three longitudinal visits and analogous to early or
‘preclinical’ MCI, which may possibly identify very subtle cognitive dysfunction (Mueller et al.,
2015).
Assessment of isolated language functions, however, might not capture the magnitude of
problems experienced in everyday communication contexts. For evaluation that more closely
approximates language demands of everyday life, researchers have turned to assessment of
spontaneous, connected speech, both as a diagnostic resource as well as a research tool toward
understanding the subtle deficits reported by patients in their natural settings. Connected
language is elicited by having an individual produce spoken or written language in response to a
particular question or stimulus, including picture description tasks(S. Ahmed et al., 2012a;
Ahmed et al., 2013b; F. Cuetos et al., 2007; Forbes-McKay & Venneri, 2005), familiar story re-
telling (Thompson & Mack, 2014) (e.g., “Cinderella” story) , wordless picture book descriptions
(Fergadiotis, Wright, & Capilouto, 2011), and general autobiographical interviews (Irish et al.,
2015). Language is then analyzed using measures such as efficiency (e.g., idea density),
conciseness (e.g., how many words required to express an idea), complexity (e.g. syntax
complexity), and speech fluency (e.g., the number of repetitions, circumlocutions, filled pauses).
73
Analysis of connected language has revealed subtle differences years or decades before diagnosis
of AD (F. Cuetos et al., 2007; Forbes-McKay & Venneri, 2005; Garrard et al., 2005; Snowdon et
al., 1996) . These language differences were a salient finding in the Nun Study(Snowdon et al.,
1996), in which idea density in early life writing samples was an accurate predictor of later-life
progression to AD. Links between content of language samples and preclinical AD also were
reported by Cuetos (F. Cuetos et al., 2007), who examined spontaneous language in a group of
19 carriers of the E280A mutation in the Presenilin 1 gene at the preclinical stage of AD (mean
age = 43.2). Carriers showed deficits in the production of semantic categories in a picture
description task during the pre-clinical phase of disease. There were no differences between
carriers and non-carriers in average sentence length or total number of sentences, which implies
that clinical examination of language productivity would not necessarily detect group
differences. More recently, Ahmed (Ahmed et al., 2013a) examined longitudinal profiles of 15
adults (mean age 71.2) with autopsy-confirmed AD and found decreasing linear trends in
syntactic complexity and semantic and lexical content across stages of disease, including the
MCI stage of disease. Given evidence of subtle language changes in MCI, it was of interest to
see if connected language differences could be a cognitive marker in very early declines that are
prior to a diagnosis of MCI. Specifically, we hypothesized that participants who were
cognitively healthy would differ on connected language outcomes from a subset with
psychometric evidence of aMCI (i.e., the subset did not have a clinical diagnosis of MCI, but did
meet statistical criteria for early decline as described in the methods). While evidence for early
language change exists based on retrospective analysis (Berisha et al., 2015; Garrard et al.,
2005), to our knowledge no studies have examined connected speech and language prospectively
in an at-risk cohort.
74
In the current study, we examined connected language samples in a group of adults (ages
40-65 years at baseline) who were at risk for AD, defined as “psychometric MCI (pMCI).” The
psychometric MCI construct refers to the presence of memory declines across at least two of
three longitudinal study visits based on internal norms (described further in the methods section).
We hypothesized that adults who were clinically cognitively intact but met psychometric criteria
of MCI (Koscik et al., 2014) would have lower scores on measures of content, syntactic
complexity, and speech fluency than age- and education-matched adults defined as cognitively
healthy.
MATERIALS AND METHODS
Participants
Participants were recruited from the Wisconsin Registry for Alzheimer’s Prevention (WRAP)
study (N>1500), an ongoing longitudinal cohort study enriched for positive parental history of
AD. WRAP study design and assessment protocols are described in detail elsewhere (La Rue et
al., 2008; Sager, Hermann, & La Rue, 2005). In brief, participants in the positive parental history
group have at least one biological parent with either autopsy-confirmed or probable AD as
defined by NINCDS-ADRDA (National Institute of Neurological and Communicative Disorders
and Stroke - Alzheimer’s Disease and Related Disorders Association) research criteria
(McKhann et al., 2011). At baseline, WRAP participants are cognitively intact and in early to
late middle-age (M=54 years), and return for follow-up assessments 4 years after baseline and
every 2 years thereafter. Participants complete extensive neuropsychological testing at each
study visit. Collection of speech samples was added to the third visit protocol and collection has
been ongoing across all visits since that time. All study procedures were approved by the
University of Wisconsin-Madison’s Institutional Review Board, and procedures were done in
75
accord with the ethical standards of the Human Research Protection Program of the UW-
Madison and the 1975 Declaration of Helsinki.
Selection of Cases and Controls for the Present Analyses
Psychometric MCI (pMCI).The primary predictor in our analysis was the psychometric MCI
(pMCI) status group (i.e., cognitively healthy (CH) versus pMCI). The construct of pMCI,
described in detail elsewhere (Koscik et al., 2014), requires a participant to have episodic
memory scores more than 1.5 SD below robust norms on at least 2 of 3 study visits; robust
norms were developed by using a reference group’s baseline scores to develop more sensitive
prediction limits based on age, gender, and WRAT-3 reading scores(Koscik et al., 2014).
Inclusion criteria. For this study, individuals with neurological diagnoses including meningitis,
stroke, epilepsy, multiple sclerosis and Parkinson’s disease, as well as individuals who were non-
native English speakers, were not eligible. After those exclusions were applied, we identified 40
participants who had speech samples and who also met psychometric MCI (pMCI) criteria. Once
eligible cases were identified, one cognitively healthy participant (“CH”; no episodic memory or
executive function scores more than 1.5 SD below robust norms across 3 visits) was randomly
selected for each pMCI case from the subset of CH in the same age range (no difference greater
than 3 years), gender, and literacy level (CH were from the same decile, using age- and sex-
adjusted Wide Range Achievement Test -3 (WRAT-3) scores (Wilkinson, 1993)) as the pMCI
case.
The sample size of 40 for each of two study groups was targeted initially based on feasibility of
analyzing speech samples and sensitivity analyses that suggested power of .8 to detect effect
sizes of ~.40 to .50 (assuming a correlation between the pMCI and CH groups of .10-.15). One
speech sample was unusable, so the final sample size was 39 per group.
76
Additional predictors and covariates. Other variables examined included depressive symptoms as
measured by the Centers for Epidemiologic Studies Depression scale (CES-D,(Johnson et al.,
2011; Radloff, 1991)), parental family history of AD (FH+), the presence of one or more APOE
ɛ4 allele, obtained as described elsewhere (Johnson et al., 2011), standardized language measures
(Boston Naming Test(Goodglass & Kaplan, 1983); Verbal Fluency tasks), and measures of
episodic memory and executive function (Table 1).
Language Sample Procedure
Participants provided informed consent to have speech samples recorded. Participants were
provided with the “Cookie Theft” picture from the Boston Diagnostic Aphasia Examination
(Goodglass & Kaplan, 1983) , and were instructed to “Tell me everything you see going on in
this picture.” The test administrators were instructed to provide minimal feedback, but were
instructed to give the scripted prompt, “do you see anything else going on?” if responses were
unusually brief. Duration of the picture description speech sample ranged from approximately
one to three minutes in total length (including examiner prompts). All responses were recorded
using an Olympus VN-6200PC digital audio recorder.
Transcriptions
Transcriptions of the speech samples for this study were performed by a trained speech-language
pathology graduate student (SKR) using Codes for Human Analysis of Transcripts
(CHAT;(Macwhinney et al., 2011)). Utterance boundaries were determined by the “T-unit”
classification system, defined as a main clause and all of its modifiers (Hunt, 1965). We coded
the samples for automatic analyses by the Computer Language Analysis (CLAN) program
(Macwhinney et al., 2011). Common codes included those for fillers, revisions, repetitions,
pauses, semantic units (for description of these measures, see below in “language measures”), as
77
well as for various non-verbal behaviors (e.g., laughing). Semantic units, parts of speech, total
words, total utterances, and other quantifiers were automatically extracted by the CLAN
program.
Ten percent of samples were re-transcribed and coded by a second rater, a trained speech-
language pathologist (KDM), and inter-rater agreement was 98.9% for transcriptions and 82.5%
for semantic unit coding. Disagreements for semantic unit coding were discussed, a manual was
developed based on consensus, and semantic units were re-coded. Both the examiners and coders
were blinded to the group status (CH or pMCI) of participants at the time of data collection and
transcription.
Language Measures
The measures used for analysis and illustrative examples are summarized in Tables 1a and 1b.
Language measures were chosen based on previous literature that focused on discourse analysis
in MCI or preclinical AD (S. Ahmed et al., 2012a; Ahmed et al., 2013a; Ahmed et al., 2013b;
Berisha et al., 2015; F. Cuetos et al., 2007).
Semantic Content and Lexical Richness
Total semantic units. The total number of semantic units for the “Cookie Theft” picture
description task was obtained using the semantic unit classification described by Croisile
(Croisile et al., 1996) and Ahmed (Ahmed et al., 2013b), that included 23 semantic units,
consisting of people, objects, actions and attitudes.
Semantic unit idea density. Semantic Unit Idea Density was calculated by dividing the total
number of semantic units by the number of words.
78
Propositional idea density. An additional form of propositional idea density was automatically
extracted from the CLAN program, adapted from the Computerized Propositional Idea Density
Rater (CPIDER3) (Brown, Snodgrass, Kemper, Herman, & Covington, 2008; Covington &
McFall, 2010; Macwhinney et al., 2011). In brief, propositions correspond to verbs, adjectives,
adverbs, prepositions and conjunctions divided by the total number of words (excluding
repetitions and fillers).
Unique words and total words. The number of unique words and total words were calculated.
Moving Average Type-Token Ratio (MATTR). For a measure of lexical diversity we used the
Moving-average type-token ratio (MATTR), which is an index based on a moving window that
computes an average of type-token ratios for each successive window of a fixed length
(Covington & McFall, 2010) (we used fixed length of 10).
Proportion of pronouns. This measure was calculated by dividing the number of pronouns by the
total number of nouns plus pronouns.
Proportion of verbs. This ratio was defined as number of verbs divided by total verbs plus nouns.
Syntactic Complexity
Mean length of utterance. As a measure of syntactic complexity for both tasks, we calculated
Mean Length of Utterance (MLU), the number of morphemes (units of linguistic meaning)
divided by number of utterances.
Verb index. Verb index was defined as the ratio of number of verbs to total number of utterances.
We calculated this measure as a way to capture the number of clauses per utterance, and because
verb deficits have been shown to coincide with disruptions in discourse (Kim & Thompson,
2004).
79
Speech Fluency
Maze Index. In order to measure speech fluency, we defined mazes as repetitions, revisions, false
starts and fillers (e.g., “uh, um”). Maze index was calculated by dividing the total number of
mazes by the number of utterances (Bird, Lambon Ralph, Patterson, & Hodges, 2000; Nicholas
et al., 1985; Wilson et al., 2010).
Filled pauses. Filled pauses was the proportion of fillers (e.g., “um,” “uh”) to number of
utterances, and was examined based on previous findings showing an increase in filled pauses
(Wilson et al., 2010).
Analyses
Prior to testing our hypotheses, all language variables were transformed to normally-distributed
z-scores (i.e., ~N (0,1)), except for Boston Naming Test. Due to high ceiling effects of BNT in
our sample, no transformations yielded a normal distribution. Paired sample t-tests or Chi-Square
Tests of Independence were used to compare CH and PMCI groups on all variables. For the
Semantic Units measure, two outliers were identified so we applied Winsor adjustments to these
values. For the Boston Naming Test (BNT) (Goodglass & Kaplan, 1983), we used a Mann-
Whitney Wilcoxon test due to the high ceiling effects of the BNT in the WRAP sample. Effect
sizes were calculated for each comparison using Cohen’s d: (mean group 1 – mean group
2)/pooled sd. All tests were two-tailed using an alpha of .05. For the discourse measures that
differed significantly by pMCI status, we also examined the Pearson correlation coefficients
among discourse, verbal fluency, and verbal memory (using the combined sample of n=78).
Analyses were performed using SAS v9.3, R version 3.2.2, and SPSS version 22.

80
RESULTS
The average age of the participants included in these analyses was 63.1 years (SD=6.3);
22% were female; and the average WRAT reading standard score was 110.6(7.4). The
cognitively healthy (CH) and pMCI (psychometric MCI) groups differed significantly in terms of
APOE-4, in that the CH group had a higher percentage of participants with at least one E4 allele;
family history status was not significantly different. Table 2 shows that the demographic
characteristics of the pMCI groups were very similar, as would be expected based on the
matched sampling strategy that was used. Table 2 also describes the two samples regarding
neuropsychological performance, and is reflective of the defining nature of the psychometric
aMCI criteria (Koscik et al., 2014; Taler & Phillips, 2008). Specifically, the verbal and learning
scores were significantly different between the two groups, but the executive function scores
were not. Both letter fluency and category fluency, which were not part of the psychometric
aMCI diagnostic criteria, yielded worse scores for the PMCI group than the CH group (p = .0005
and p<.0001, respectively); the Boston Naming Test was not significantly different between
groups.
Connected language results are presented in Table 3. To facilitate review of all language
outcomes in a single graph, the mean(se) of the corresponding z-scores across several language
outcome measures are shown in Figure 1 by cognitive status groups. The CH and PMCI groups
differed significantly on two content measures: pMCI subjects produced fewer unique words (p
= .028) and fewer semantic units (p = .018) than the CH group. Marginal differences were found
in Propositional Idea Density (p = .09) and in the Moving Average Type-Token Ratio (MATTR)
(p = .06). The CH and PMCI groups did not differ significantly on Maze Index or filled
pauses/utterance, nor on any of the syntactic complexity measures.
81
Secondary Analyses. Since the Cognitively Healthy group had significantly more APOE-4
carriers, we ran secondary analyses using ANCOVAs with APOE-4 as a covariate (Table 4). The
pMCI group continued to show significantly lower Semantic Units (p = .008) than the CH group
(adjusted means(se): CH=14.5(.44); pMCI=12.7(.44)). In addition, when adjusting for APOE-4
status, the pMCI group showed significantly lower propositional idea density than the CH group
(p = .028) (adjusted means(se): CH=.46(.01); pMCI=.44(.01)), and fewer unique words (p = .03)
(adjusted means(se): CH=71.6(3.3); pMCI=61.1(3.3)). No other differences were statistically
significant. To further remove the confounding risk factor of APOE-4, we re-ran the analysis for
each APOE subset (i.e., APOE-4 non-carriers and carriers). In the APOE-4 non-carrier subset,
the pMCI group (n=31) continued to show reduced semantic units (p=.05), fewer unique words
(p=.05), and increased use of filled pauses (p=.028) compared to the CH group (n=20). In the
APOE-4 carrier subset, non-significant differences were observed for comparisons of pMCI
(n=8 ) and CH (n= 19) in all measures; power to detect significant differences was limited in this
subset.
We also examined the relationship between the connected language variables and the
more standard verbal fluency measures and the R-AVLT in the neuropsychological test battery
(Fig 2). Bivariate Pearson correlations for the set of 78 participants were moderate for unique
words and letter fluency (r=.41), unique words and AVLT (r=.39); idea density was moderately
correlated with letter fluency (r=.40); Semantic Units was moderately correlated with AVLT
(r=.34), but not with the verbal fluency tasks.
DISCUSSION
In this study, spontaneous language samples were examined from two groups of late-
middle-aged participants drawn from a cohort enriched for family history of AD: those who were
82
evidencing psychometric memory decline based on internal robust norms (pMCI) and those who
were classified as cognitively healthy. Psychometric memory decline was identified in
participants who showed episodic memory scores that were more than 1.5 SD below robust
norms on at least 2 of 3 study visits. We hypothesized that the pMCI group would perform worse
on language variables characterizing semantic content, syntactic complexity, and speech fluency,
than those who were cognitively healthy.
The pMCI group performed worse on both phonemic (letter) and semantic (category)
fluency, two measures that were not included in the psychometric criteria for determining the
groups. The confrontation naming task (Boston Naming Test) was not significantly different
between groups, consistent with previous MCI literature (Taler & Phillips, 2008).
Our results suggested that the pMCI group expressed fewer semantic units and fewer
unique words than the cognitively healthy group, which is a similar finding to that seen in studies
with persons with MCI and AD (Ahmed et al., 2013a; Berisha et al., 2015; F. Cuetos et al., 2007;
Forbes-McKay & Venneri, 2005). Recently, Berisha (Berisha et al., 2015) found that former
President Ronald Reagan’s use of unique words declined over time, prior to his diagnosis of
Alzheimer’s Disease. Similarly, while the pMCI group in our sample exhibited verbal learning
and memory declines across longitudinal visits that were significant according to robust norms,
they were not diagnosed with clinical MCI because they were not sufficiently impaired
according to general test norms. Therefore, the pMCI group did not meet formal diagnostic
criteria for MCI and are categorized as having a psychometric condition; these findings may
suggest and reinforce the idea that language symptoms may be present antecedent to meeting
formal diagnostic criteria for the clinical condition (aMCI). The semantic unit findings may
represent subtle differences in semantic processing, particularly within the context of the
83
demands of producing spontaneous speech, and may be predictive of larger language changes
over time. That the Semantic Units measure was not significantly correlated with either verbal
fluency tasks, but was correlated with the Rey Auditory Verbal Learning Test, suggests that it
may tap into additional language or other cognitive processes, and may contribute unique
knowledge regarding preclinical language changes.
The differences in semantic units between the two groups could support the hypothesis
that semantic memory declines may be reflective of the underlying early neuropathology in the
transentorhinal, mediotemporal networks, while the hippocampus may still be spared (Venneri et
al., 2016). Further, when the task is embedded within spontaneous speech, a more qualitative
analysis affords an informative characterization of problems within a functional context. The
task itself is relatively quick and noninvasive for patients to complete, and may be informative
not only for very early diagnosis, but also for disease course monitoring in both pharmacological
and nonpharmacological clinical trials.
Secondary analyses were conducted to adjust for the higher percentage of participants
with APOE-4 in the cognitively healthy group. Since APOE E-4 is considered to be a risk factor
for cognitive decline even in normally aging populations (Bretsky, Guralnik, Launer, Albert, &
Seeman, 2003), we were interested in adjusting for this possible confound in our control group.
This adjustment of controlling for APOE-4 strengthened the results of the Semantic Units and
unique words findings, and also revealed that the pMCI group’s language samples had lower
propositional idea density than the CH group. While several studies have shown that lower
propositional density in early life predicted future AD risk (Engelman, Agree, Meoni, & Klag,
2010; Snowdon et al., 1996), and one small study found that young APOE-4 carriers had lower
propositional density than noncarriers (Medina et al., 2011), the effect of APOE4 status on
84
language abilities in aging and in AD risk is not well understood. Whether APOE4 status exerts
an effect on future language declines will be addressed in longitudinal follow-up studies on this
cohort.
No differences were detected in syntactic complexity; this may be due to the possibility
that syntactic complexity remains preserved at preclinical or early phases, as evidenced
previously (Kemper et al., 1993). However, Le et al. (Le, Lancashire, Hirst, & Jokel, 2011)
analyzed several novels of British writers over time and found some decreases in the use of
passive voice, consistent with other previous findings (Bates, Harris, Marchman, Wulfeck, &
Kritchevsky, 1995). Therefore it is possible that our samples of the picture description task are
simply too short to detect syntactic differences. The same can be said for the lack of findings
with respect to fillers, revisions, and repetitions in this group. It is also possible that syntactic
differences will be more detectable upon longitudinal analysis of change within individuals.
The greatest limitations of this study include the small sample size and not adjusting for
multiple comparisons. We powered our study to detect plausible effect sizes using an alpha of
.05; adjustments for multiple comparisons would have greatly reduced our statistical power, and
increasing the sample size was beyond our resources at the time of analysis. An additional
limitation includes the fact that several measures that have been shown to identify impairment in
Alzheimer’s Disease (e.g., error monitoring (the proportion of revised errors to total errors),
timing aspects such as performance deviations per minute or response-time to word-finding
delays) were not analyzed, as we based our measures on those that have been examined in MCI
or preclinical AD. Nonetheless, the addition of such measures would add clarity to the limited
research available in this population. Future studies will include factor analyses of the many
85
discourse measures examined in previous AD literature in order to more concisely characterize
aspects of language and to reduce the amount of multiple comparisons.
The strengths of this study include utilizing connected language analysis measures in a
unique population: a cohort of clinically healthy individuals who are at-risk for Alzheimer’s
Disease. Thus far, connected language analysis has proven to be useful in detecting deficits at
early stages of autopsy-confirmed AD(Ahmed et al., 2013b) and in preclinical stages of disease
in carriers of the E280A mutation (F. Cuetos et al., 2007). An additional strength of this study is
examining groups that are based upon internally-derived norms (Koscik et al., 2014) which
allowed us to identify a “preclinical” MCI group. Further examination of connected language
using larger sample sizes of the pMCI and CH groups longitudinally may yield important
findings regarding improving the ability to detect early language deficits, aiding in differential
diagnosis, and providing direction for non-pharmacological communication interventions.
In conclusion, these results suggest that subtle yet detectable changes in connected
language may be present during preclinical stages of cognitive decline. For relatively little
investment of patient time and effort, language tasks can yield rich information not only about
semantic storage and retrieval, but also about the complex cognitive processes involved in
producing spontaneous, connected language. Further, these analyses may help to provide tools
for differential diagnosis among variants of cognitive decline, such as AD versus Primary
Progressive Aphasia (S. Ahmed et al., 2012a), or between dementia and other co-morbid
conditions such as depression (Murray, 2010). Future research will examine changes over time,
to better understand how such changes correspond to or predict clinical outcomes, document
disease progression, and aid in determining strategies and interventions for improved
communication between patients and caregivers.
86
ACKNOWLEDGMENTS
We would like to thank WRAP participants and WAI staff for their contributions to the WRAP
study. Without their efforts this research would not be possible. Gratitude also to Sarah
Riedeman for language transcription and to Davida Fromm for consultation on CHAT/CLAN.
WRAP is supported by NIA grant R01AG27161 (Wisconsin Registry for Alzheimer Prevention:
Biomarkers of Preclinical AD), Louis Holland Research Sr. Research Fund, Helen Bader
Foundation, Northwestern Mutual Foundation, Extendicare Foundation and State of Wisconsin.
WRAP is also supported by the Clinical and Translational Science Award (CTSA) program,
through the NIH National Center for Advancing Translational Sciences (NCATS), grant
UL1TR000427. The content is solely the responsibility of the authors and does not necessarily
represent the official views of the NIH. The authors state that there are no conflicts of interest.
Kimberly Diggle Mueller, MS CCC-SLP, Wisconsin Alzheimer’s Institute, University of
Wisconsin School of Medicine & Public Health, Madison, Wisconsin USA
Phone: 608-829-3300 Email: [email protected] Web: www.wai.wisc.edu
87
REFERENCES
[1] Fischer P, Jungwirth S, Zehetmayer S, Weissgram S, Hoenigschnabl S, Gelpi E, Krampla
W, Tragl KH (2007) Conversion from subtypes of mild cognitive impairment to
Alzheimer dementia. Neurology 68, 288-291.
[2] Albert MS, DeKosky ST, Dickson D, Dubois B, Feldman HH, Fox NC, Gamst A,
Holtzman DM, Jagust WJ, Petersen RC, Snyder PJ, Carrillo MC, Thies B, Phelps CH
(2011) The diagnosis of mild cognitive impairment due to Alzheimer's disease:
recommendations from the National Institute on Aging-Alzheimer's Association
workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement 7, 270-
279.
[3] Jack CR, Jr., Knopman DS, Jagust WJ, Petersen RC, Weiner MW, Aisen PS, Shaw LM,
Vemuri P, Wiste HJ, Weigand SD, Lesnick TG, Pankratz VS, Donohue MC, Trojanowski
JQ (2013) Tracking pathophysiological processes in Alzheimer's disease: an updated
hypothetical model of dynamic biomarkers. Lancet Neurol 12, 207-216.
[4] Zimmer ER, Leuzy A, Benedet AL, Breitner J, Gauthier S, Rosa-Neto P (2014) Tracking
neuroinflammation in Alzheimer's disease: the role of positron emission tomography
imaging. J Neuroinflammation 11, 120.
[5] Alcolea D, Carmona-Iragui M, Suarez-Calvet M, Sanchez-Saudinos MB, Sala I, Anton-
Aguirre S, Blesa R, Clarimon J, Fortea J, Lleo A (2014) Relationship between beta-
Secretase, inflammation and core cerebrospinal fluid biomarkers for Alzheimer's disease.
J Alzheimers Dis 42, 157-167.
[6] Barbeau EJ, Didic M, Joubert S, Guedj E, Koric L, Felician O, Ranjeva JP, Cozzone P,
Ceccaldi M (2012) Extent and neural basis of semantic memory impairment in mild
cognitive impairment. J Alzheimers Dis 28, 823-837.
[7] Didic M, Barbeau EJ, Felician O, Tramoni E, Guedj E, Poncet M, Ceccaldi M (2011)
Which memory system is impaired first in Alzheimer's disease? J Alzheimers Dis 27, 11-
22.
[8] Venneri A, Mitolo M, De Marco M (2016) Paradigm shift: semantic memory decline as a
biomarker of preclinical Alzheimer's disease. Biomark Med 10, 5-8.
[9] Faber-Langendoen K, Morris JC, Knesevich JW, LaBarge E, Miller JP, Berg L (1988)
Aphasia in senile dementia of the Alzheimer type. Ann Neurol 23, 365-370.
[10] Taler V, Phillips NA (2008) Language performance in Alzheimer's disease and mild
cognitive impairment: a comparative review. J Clin Exp Neuropsychol 30, 501-556.
[11] Welsh KA, Butters N, Hughes JP, Mohs RC, Heyman A (1992) Detection and staging of
dementia in Alzheimer's disease: Use of the neuropsychological measures developed for
the Consortium to Establish a Registry for Alzheimer's Disease. Archives of neurology
49, 448-452.
88
[12] Testa JA, Ivnik RJ, Boeve B, Petersen RC, Pankratz VS, Knopman D, Tangalos E, Smith
GE (2004) Confrontation naming does not add incremental diagnostic utility in MCI and
Alzheimer's disease. J Int Neuropsychol Soc 10, 504-512.
[13] Willers IF, Feldman ML, Allegri RF (2008) Subclinical naming errors in mild cognitive
impairment. Demant Neuropsychol 2, 217-222.
[14] Nutter-Upham KE, Saykin AJ, Rabin LA, Roth RM, Wishart HA, Pare N, Flashman LA
(2008) Verbal fluency performance in amnestic MCI and older adults with cognitive
complaints. Arch Clin Neuropsychol 23, 229-241.
[15] Clark LJ, Gatz M, Zheng L, Chen YL, McCleary C, Mack WJ (2009) Longitudinal verbal
fluency in normal aging, preclinical, and prevalent Alzheimer's disease. Am J Alzheimers
Dis Other Demen 24, 461-468.
[16] Price SE, Kinsella GJ, Ong B, Storey E, Mullaly E, Phillips M, Pangnadasa-Fox L, Perre
D (2012) Semantic verbal fluency strategies in amnestic mild cognitive impairment.
Neuropsychology 26, 490-497.
[17] Mueller KD, Koscik RL, LaRue A, Clark LR, Hermann B, Johnson SC, Sager MA
(2015) Verbal Fluency and Early Memory Decline: Results from the Wisconsin Registry
for Alzheimer's Prevention. Arch Clin Neuropsychol 30, 448-457.
[18] Ahmed S, de Jager CA, Haigh AM, Garrard P (2012) Logopenic aphasia in Alzheimer's
disease: clinical variant or clinical feature? J Neurol Neurosurg Psychiatry 83, 1056-
1062.
[19] Ahmed S, Haigh AM, de Jager CA, Garrard P (2013) Connected speech as a marker of
disease progression in autopsy-proven Alzheimer's disease. Brain 136, 3727-3737.
[20] Cuetos F, Arango-Lasprilla JC, Uribe C, Valencia C, Lopera F (2007) Linguistic changes
in verbal expression: a preclinical marker of Alzheimer's disease. J Int Neuropsychol Soc
13, 433-439.
[21] Forbes-McKay KE, Venneri A (2005) Detecting subtle spontaneous language decline in
early Alzheimer's disease with a picture description task. Neurol Sci 26, 243-254.
[22] Thompson CK, Mack JE (2014) Grammatical impairments in PPA. Aphasiology 28,
1018-1037.
[23] Fergadiotis G, Wright HH, Capilouto GJ (2011) Productive vocabulary across discourse
types. Aphasiology 25, 1261-1278.
[24] Irish M, Kamminga J, Addis DR, Crain S, Thornton R, Hodges JR, Piguet O (2015)
‘Language of the past’–Exploring past tense disruption during autobiographical narration
in neurodegenerative disorders. Journal of neuropsychology.
[25] Snowdon DA, Kemper SJ, Mortimer JA, Greiner LH, Wekstein DR, Markesbery WR
(1996) Linguistic ability in early life and cognitive function and Alzheimer's disease in
late life. Findings from the Nun Study. JAMA 275, 528-532.
89
[26] Garrard P, Maloney LM, Hodges JR, Patterson K (2005) The effects of very early
Alzheimer's disease on the characteristics of writing by a renowned author. Brain 128,
250-260.
[27] Ahmed S, de Jager CA, Haigh AM, Garrard P (2013) Semantic processing in connected
speech at a uniformly early stage of autopsy-confirmed Alzheimer's disease.
Neuropsychology 27, 79-85.
[28] Berisha V, Wang S, LaCross A, Liss J (2015) Tracking discourse complexity preceding
Alzheimer's disease diagnosis: a case study comparing the press conferences of
Presidents Ronald Reagan and George Herbert Walker Bush. J Alzheimers Dis 45, 959-
963.
[29] Koscik RL, La Rue A, Jonaitis EM, Okonkwo OC, Johnson SC, Bendlin BB, Hermann
BP, Sager MA (2014) Emergence of mild cognitive impairment in late middle-aged
adults in the wisconsin registry for Alzheimer's prevention. Dement Geriatr Cogn Disord
38, 16-30.
[30] La Rue A, Hermann B, Jones JE, Johnson S, Asthana S, Sager MA (2008) Effect of
parental family history of Alzheimer's disease on serial position profiles. Alzheimers
Dement 4, 285-290.
[31] Sager MA, Hermann B, La Rue A (2005) Middle-aged children of persons with
Alzheimer's disease: APOE genotypes and cognitive function in the Wisconsin Registry
for Alzheimer's Prevention. J Geriatr Psychiatry Neurol 18, 245-249.
[32] McKhann GM, Knopman DS, Chertkow H, Hyman BT, Jack CR, Jr., Kawas CH, Klunk
WE, Koroshetz WJ, Manly JJ, Mayeux R, Mohs RC, Morris JC, Rossor MN, Scheltens P,
Carrillo MC, Thies B, Weintraub S, Phelps CH (2011) The diagnosis of dementia due to
Alzheimer's disease: recommendations from the National Institute on Aging-Alzheimer's
Association workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers
Dement 7, 263-269.
[33] Wilkinson GS (1993) WRAT-3: Wide range achievement test, Wide Range.
[34] Radloff LS (1991) The use of the Center for Epidemiologic Studies Depression Scale in
adolescents and young adults. Journal of youth and adolescence 20, 149-166.
[35] Johnson SC, La Rue A, Hermann BP, Xu G, Koscik RL, Jonaitis EM, Bendlin BB,
Hogan KJ, Roses AD, Saunders AM, Lutz MW, Asthana S, Green RC, Sager MA (2011)
The effect of TOMM40 poly-T length on gray matter volume and cognition in middle-
aged persons with APOE epsilon3/epsilon3 genotype. Alzheimers Dement 7, 456-465.
[36] Goodglass H, Kaplan E (1983) Boston diagnostic aphasia examination booklet, Lea &
Febiger.
[37] Macwhinney B, Fromm D, Forbes M, Holland A (2011) AphasiaBank: Methods for
Studying Discourse. Aphasiology 25, 1286-1307.
[38] Hunt KW (1965) Grammatical Structures Written at Three Grade Levels. NCTE
Research Report No. 3.
90
[39] Croisile B, Ska B, Brabant MJ, Duchene A, Lepage Y, Aimard G, Trillet M (1996)
Comparative study of oral and written picture description in patients with Alzheimer's
disease. Brain Lang 53, 1-19.
[40] Covington MA, McFall JD (2010) Cutting the Gordian knot: The moving-average type–
token ratio (MATTR). Journal of Quantitative Linguistics 17, 94-100.
[41] Brown C, Snodgrass T, Kemper SJ, Herman R, Covington MA (2008) Automatic
Measurement of Propositional Idea Density from Part-of-Speech Tagging. Behavior
research methods 40, 540-545.
[42] Kim M, Thompson CK (2004) Verb deficits in Alzheimer’s disease and agrammatism:
Implications for lexical organization. Brain and language 88, 1-20.
[43] Nicholas M, Obler LK, Albert ML, Helm-Estabrooks N (1985) Empty speech in
Alzheimer's disease and fluent aphasia. J Speech Hear Res 28, 405-410.
[44] Bird H, Lambon Ralph MA, Patterson K, Hodges JR (2000) The rise and fall of
frequency and imageability: noun and verb production in semantic dementia. Brain Lang
73, 17-49.
[45] Wilson SM, Henry ML, Besbris M, Ogar JM, Dronkers NF, Jarrold W, Miller BL,
Gorno-Tempini ML (2010) Connected speech production in three variants of primary
progressive aphasia. Brain 133, 2069-2088.
[46] Bretsky P, Guralnik J, Launer L, Albert M, Seeman TE (2003) The role of APOE-ε4 in
longitudinal cognitive decline MacArthur Studies of Successful Aging. Neurology 60,
1077-1081.
[47] Engelman M, Agree EM, Meoni LA, Klag MJ (2010) Propositional density and cognitive
function in later life: Findings from the Precursors Study. The Journals of Gerontology
Series B: Psychological Sciences and Social Sciences 65, 706-711.
[48] Medina LD, Rodriguez-Agudelo Y, Geschwind DH, Gilbert PE, Liang L-J, Cummings
JL, Ringman JM (2011) Propositional density and apolipoprotein e genotype among
persons at risk for familial Alzheimer’s disease. Dementia and geriatric cognitive
disorders 32, 188-192.
[49] Kemper S, LaBarge E, Ferraro FR, Cheung H, Cheung H, Storandt M (1993) On the
preservation of syntax in Alzheimer's disease: Evidence from written sentences. Archives
of Neurology 50, 81-86.
[50] Le X, Lancashire I, Hirst G, Jokel R (2011) Longitudinal detection of dementia through
lexical and syntactic changes in writing: a case study of three British novelists. Literary
and Linguistic Computing, fqr013.
[51] Bates E, Harris C, Marchman V, Wulfeck B, Kritchevsky M (1995) Production of
complex syntax in normal ageing and Alzheimer's disease. Language and Cognitive
Processes 10, 487-539.
[52] Murray LL (2010) Distinguishing clinical depression from early Alzheimer's disease in
elderly people: Can narrative analysis help? Aphasiology 24, 928-939.
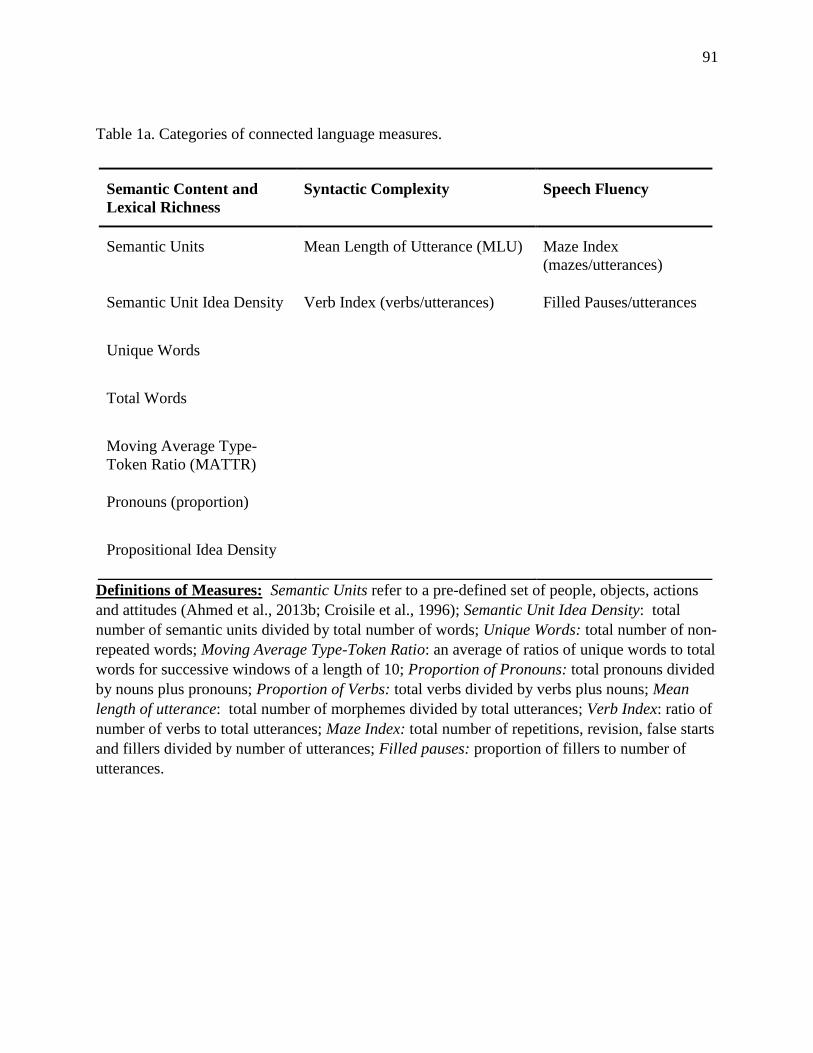
91
Table 1a. Categories of connected language measures.
Definitions of Measures: Semantic Units refer to a pre-defined set of people, objects, actions
and attitudes (Ahmed et al., 2013b; Croisile et al., 1996); Semantic Unit Idea Density: total
number of semantic units divided by total number of words; Unique Words: total number of non-
repeated words; Moving Average Type-Token Ratio: an average of ratios of unique words to total
words for successive windows of a length of 10; Proportion of Pronouns: total pronouns divided
by nouns plus pronouns; Proportion of Verbs: total verbs divided by verbs plus nouns; Mean
length of utterance: total number of morphemes divided by total utterances; Verb Index: ratio of
number of verbs to total utterances; Maze Index: total number of repetitions, revision, false starts
and fillers divided by number of utterances; Filled pauses: proportion of fillers to number of
utterances.
Semantic Content and
Lexical Richness
Syntactic Complexity Speech Fluency
Semantic Units Mean Length of Utterance (MLU) Maze Index
(mazes/utterances)
Semantic Unit Idea Density Verb Index (verbs/utterances) Filled Pauses/utterances
Unique Words
Total Words
Moving Average Type-
Token Ratio (MATTR)
Pronouns (proportion)
Propositional Idea Density
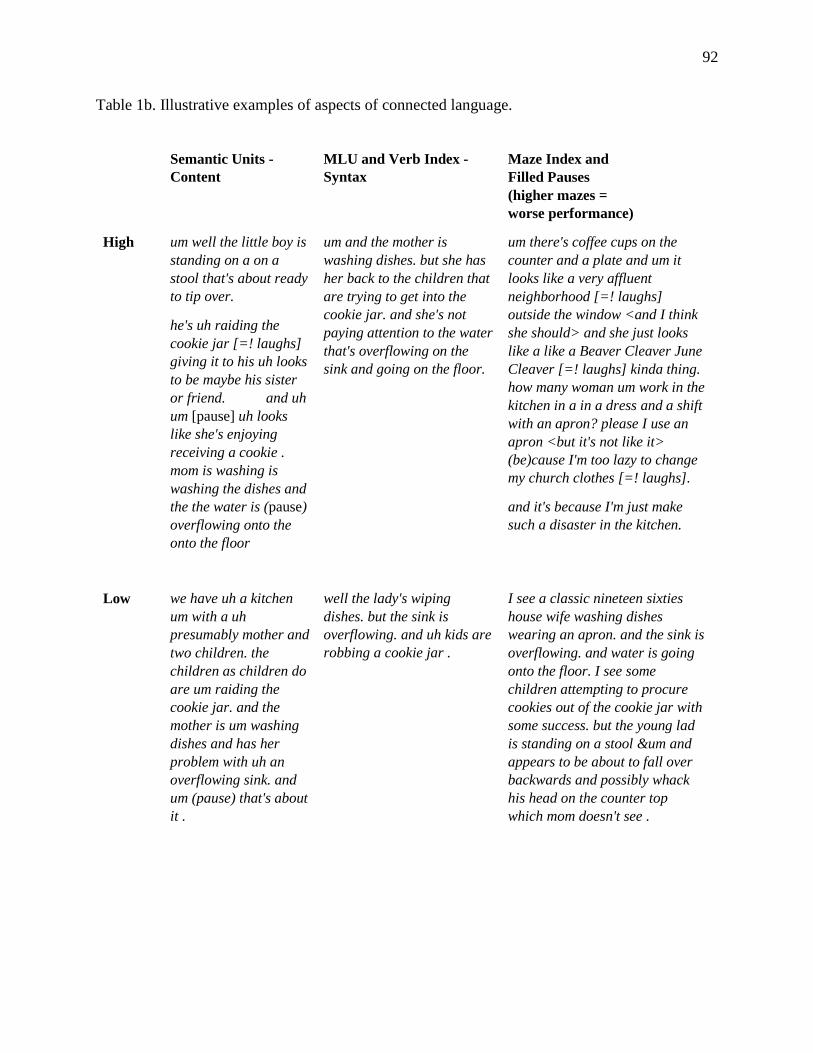
92
Table 1b. Illustrative examples of aspects of connected language.
Semantic Units -
Content
MLU and Verb Index -
Syntax
Maze Index and
Filled Pauses
(higher mazes =
worse performance)
High um well the little boy is
standing on a on a
stool that's about ready
to tip over.
he's uh raiding the
cookie jar [=! laughs]
giving it to his uh looks
to be maybe his sister
or friend. and uh
um [pause] uh looks
like she's enjoying
receiving a cookie .
mom is washing is
washing the dishes and
the the water is (pause)
overflowing onto the
onto the floor
um and the mother is
washing dishes. but she has
her back to the children that
are trying to get into the
cookie jar. and she's not
paying attention to the water
that's overflowing on the
sink and going on the floor.
um there's coffee cups on the
counter and a plate and um it
looks like a very affluent
neighborhood [=! laughs]
outside the window <and I think
she should> and she just looks
like a like a Beaver Cleaver June
Cleaver [=! laughs] kinda thing.
how many woman um work in the
kitchen in a in a dress and a shift
with an apron? please I use an
apron <but it's not like it>
(be)cause I'm too lazy to change
my church clothes [=! laughs].
and it's because I'm just make
such a disaster in the kitchen.
Low we have uh a kitchen
um with a uh
presumably mother and
two children. the
children as children do
are um raiding the
cookie jar. and the
mother is um washing
dishes and has her
problem with uh an
overflowing sink. and
um (pause) that's about
it .
well the lady's wiping
dishes. but the sink is
overflowing. and uh kids are
robbing a cookie jar .
I see a classic nineteen sixties
house wife washing dishes
wearing an apron. and the sink is
overflowing. and water is going
onto the floor. I see some
children attempting to procure
cookies out of the cookie jar with
some success. but the young lad
is standing on a stool &um and
appears to be about to fall over
backwards and possibly whack
his head on the counter top
which mom doesn't see .
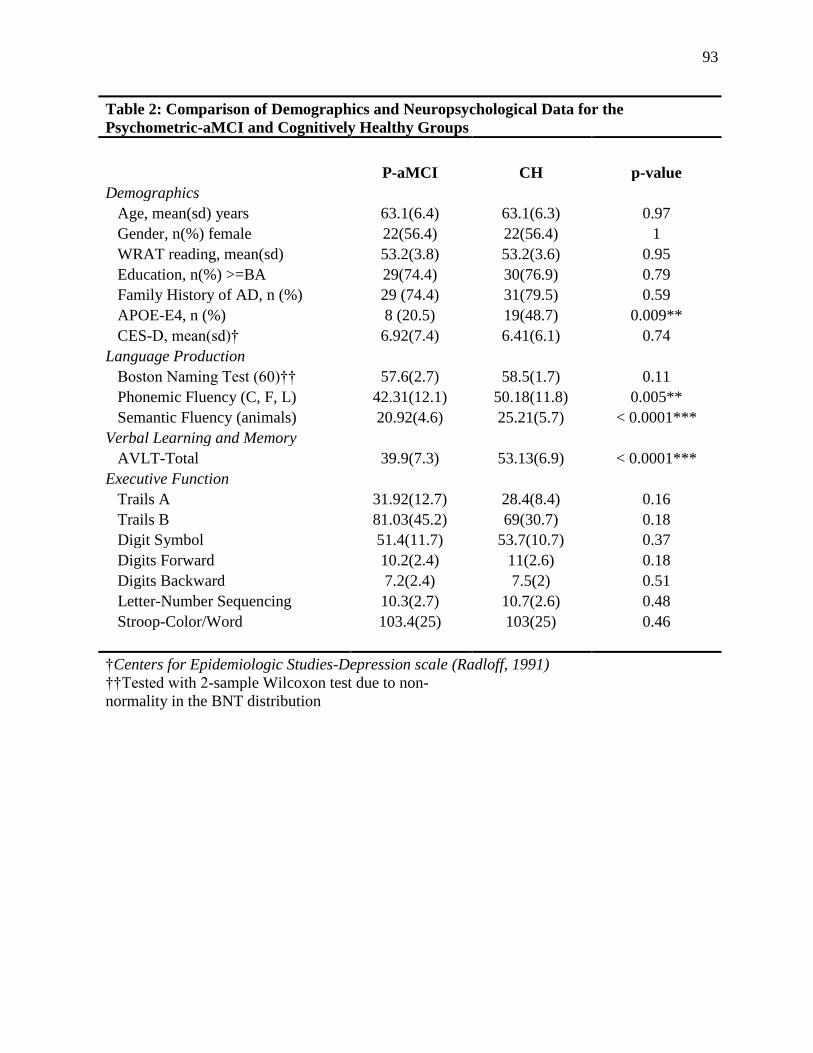
93
Table 2: Comparison of Demographics and Neuropsychological Data for the
Psychometric-aMCI and Cognitively Healthy Groups
P-aMCI CH p-value
Demographics Age, mean(sd) years 63.1(6.4) 63.1(6.3) 0.97
Gender, n(%) female 22(56.4) 22(56.4) 1
WRAT reading, mean(sd) 53.2(3.8) 53.2(3.6) 0.95
Education, n(%) >=BA 29(74.4) 30(76.9) 0.79
Family History of AD, n (%) 29 (74.4) 31(79.5) 0.59
APOE-E4, n (%) 8 (20.5) 19(48.7) 0.009**
CES-D, mean(sd)† 6.92(7.4) 6.41(6.1) 0.74
Language Production Boston Naming Test (60)†† 57.6(2.7) 58.5(1.7) 0.11
Phonemic Fluency (C, F, L) 42.31(12.1) 50.18(11.8) 0.005**
Semantic Fluency (animals) 20.92(4.6) 25.21(5.7) < 0.0001***
Verbal Learning and Memory AVLT-Total 39.9(7.3) 53.13(6.9) < 0.0001***
Executive Function Trails A 31.92(12.7) 28.4(8.4) 0.16
Trails B 81.03(45.2) 69(30.7) 0.18
Digit Symbol 51.4(11.7) 53.7(10.7) 0.37
Digits Forward 10.2(2.4) 11(2.6) 0.18
Digits Backward 7.2(2.4) 7.5(2) 0.51
Letter-Number Sequencing 10.3(2.7) 10.7(2.6) 0.48
Stroop-Color/Word 103.4(25) 103(25) 0.46
†Centers for Epidemiologic Studies-Depression scale (Radloff, 1991) ††Tested with 2-sample Wilcoxon test due to non-
normality in the BNT distribution
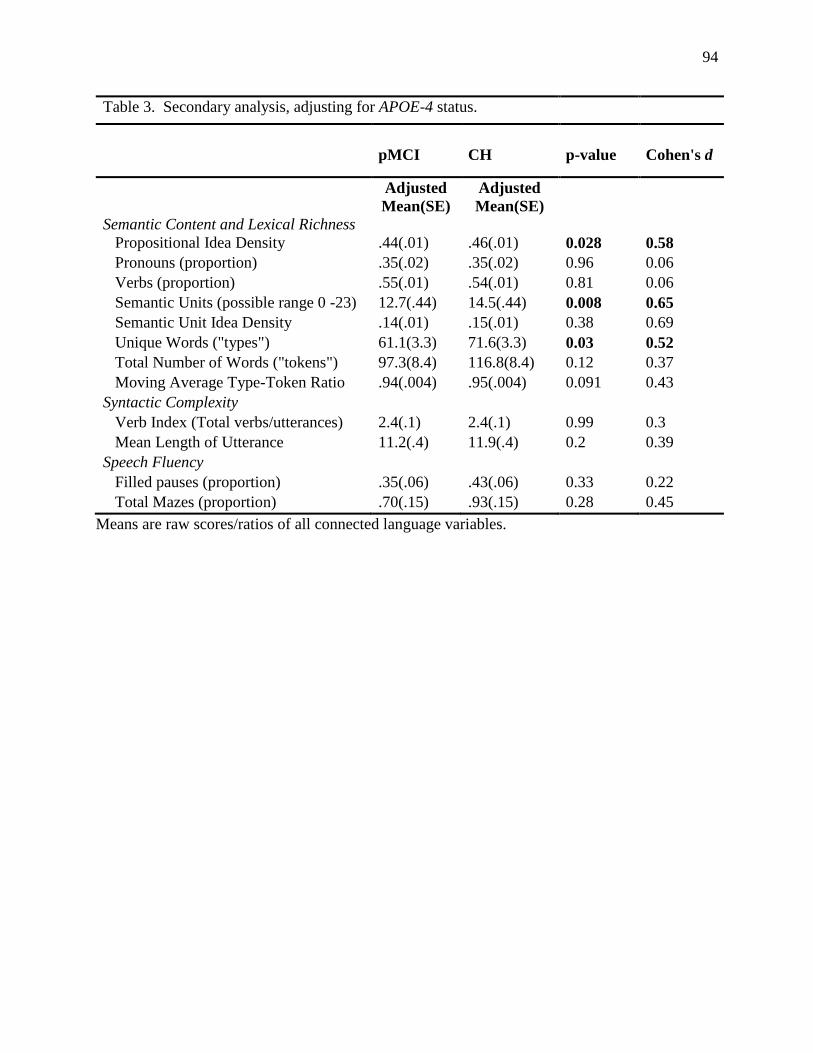
94
Table 3. Secondary analysis, adjusting for APOE-4 status.
pMCI CH p-value Cohen's d
Semantic Content and Lexical Richness
Adjusted
Mean(SE)
Adjusted
Mean(SE)
Propositional Idea Density .44(.01) .46(.01) 0.028 0.58
Pronouns (proportion) .35(.02) .35(.02) 0.96 0.06
Verbs (proportion) .55(.01) .54(.01) 0.81 0.06
Semantic Units (possible range 0 -23) 12.7(.44) 14.5(.44) 0.008 0.65
Semantic Unit Idea Density .14(.01) .15(.01) 0.38 0.69
Unique Words ("types") 61.1(3.3) 71.6(3.3) 0.03 0.52
Total Number of Words ("tokens") 97.3(8.4) 116.8(8.4) 0.12 0.37
Moving Average Type-Token Ratio .94(.004) .95(.004) 0.091 0.43
Syntactic Complexity
Verb Index (Total verbs/utterances) 2.4(.1) 2.4(.1) 0.99 0.3
Mean Length of Utterance 11.2(.4) 11.9(.4) 0.2 0.39
Speech Fluency
Filled pauses (proportion) .35(.06) .43(.06) 0.33 0.22
Total Mazes (proportion) .70(.15) .93(.15) 0.28 0.45
Means are raw scores/ratios of all connected language variables.
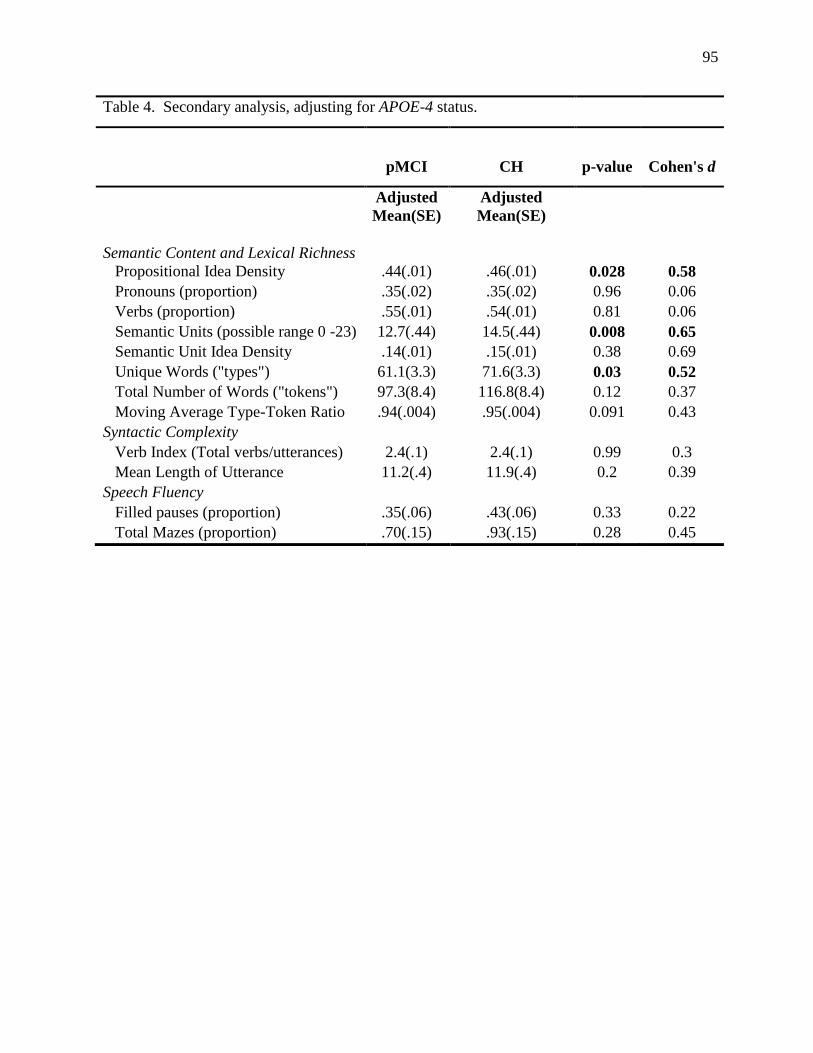
95
Table 4. Secondary analysis, adjusting for APOE-4 status.
pMCI CH p-value Cohen's d
Semantic Content and Lexical Richness
Adjusted
Mean(SE)
Adjusted
Mean(SE)
Propositional Idea Density .44(.01) .46(.01) 0.028 0.58
Pronouns (proportion) .35(.02) .35(.02) 0.96 0.06
Verbs (proportion) .55(.01) .54(.01) 0.81 0.06
Semantic Units (possible range 0 -23) 12.7(.44) 14.5(.44) 0.008 0.65
Semantic Unit Idea Density .14(.01) .15(.01) 0.38 0.69
Unique Words ("types") 61.1(3.3) 71.6(3.3) 0.03 0.52
Total Number of Words ("tokens") 97.3(8.4) 116.8(8.4) 0.12 0.37
Moving Average Type-Token Ratio .94(.004) .95(.004) 0.091 0.43
Syntactic Complexity
Verb Index (Total verbs/utterances) 2.4(.1) 2.4(.1) 0.99 0.3
Mean Length of Utterance 11.2(.4) 11.9(.4) 0.2 0.39
Speech Fluency
Filled pauses (proportion) .35(.06) .43(.06) 0.33 0.22
Total Mazes (proportion) .70(.15) .93(.15) 0.28 0.45

96
-0.6
-0.3
0
0.3
0.6Z-
Sco
res
Figure 1: Language Outcome Z-Scores by Cognitive Status
Cog. Healthy pMCI
* indicates scores were multipled by-1 so that higher values =better scores† indicates statistically significant
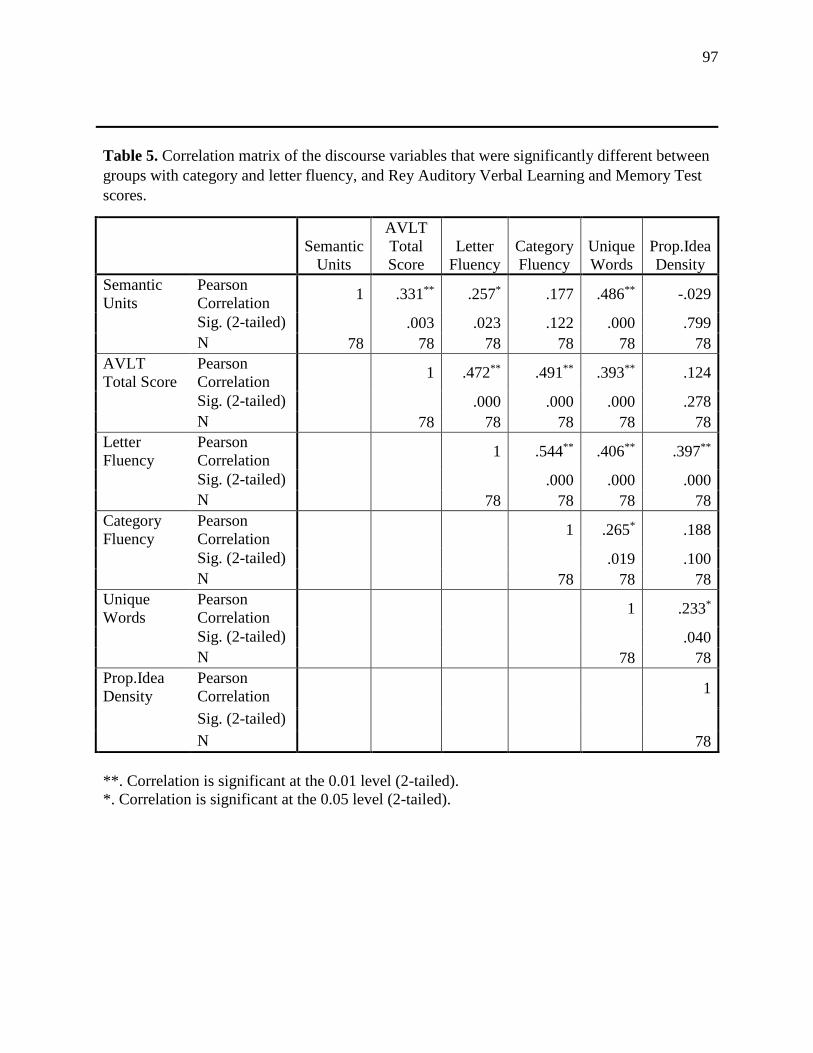
97
Table 5. Correlation matrix of the discourse variables that were significantly different between
groups with category and letter fluency, and Rey Auditory Verbal Learning and Memory Test
scores.
Semantic
Units
AVLT
Total
Score
Letter
Fluency
Category
Fluency
Unique
Words
Prop.Idea
Density
Semantic
Units
Pearson
Correlation 1 .331** .257* .177 .486** -.029
Sig. (2-tailed) .003 .023 .122 .000 .799
N 78 78 78 78 78 78
AVLT
Total Score
Pearson
Correlation 1 .472** .491** .393** .124
Sig. (2-tailed) .000 .000 .000 .278
N 78 78 78 78 78
Letter
Fluency
Pearson
Correlation 1 .544** .406** .397**
Sig. (2-tailed) .000 .000 .000
N 78 78 78 78
Category
Fluency
Pearson
Correlation 1 .265* .188
Sig. (2-tailed) .019 .100
N 78 78 78
Unique
Words
Pearson
Correlation 1 .233*
Sig. (2-tailed) .040
N 78 78
Prop.Idea
Density
Pearson
Correlation 1
Sig. (2-tailed)
N 78
**. Correlation is significant at the 0.01 level (2-tailed).
*. Correlation is significant at the 0.05 level (2-tailed).
98
CHAPTER 4
Manuscript 3: The Latent Structure and Test-Retest Stability of
Connected Language Measures in the Wisconsin Registry for
Alzheimer’s Prevention

99
The latent structure and test-retest stability of connected language measures in the Wisconsin
Registry for Alzheimer’s Prevention (WRAP)
Kimberly D. Mueller, MS a,b*; Rebecca Koscik, Ph.D.a, Bruce P. Hermann, Ph.D.c, Sterling C.
Johnson, Ph.D.a,d,e,f & Lyn S. Turkstra, Ph.Db,f,g.
aWisconsin Alzheimer’s Institute, University of Wisconsin School of Medicine and Public
Health, Madison, WI, USA
bDepartment of Communication Sciences and Disorders, University of Wisconsin – Madison,
Madison, WI, USA
cDepartment of Neurology, University of Wisconsin – Madison, Madison, WI, USA
dAlzheimer’s Disease Research Center, University of Wisconsin School of Medicine and Public
Health, Madison, WI, USA
eGeriatric Research Education and Clinical Center, Wm.S. Middleton Veterans Hospital,
Madison, WI, USA
fNeuroscience Training Program, University of Wisconsin-Madison, Madison, WI, USA
gDepartment of Surgery, University of Wisconsin-Madison, Madison, WI, USA
*Corresponding author. Tel.: 608-263-2860; Fax: 608-265-9122; E-mail address:
100
ABSTRACT
Introduction: This study investigates the latent structure, validity, and test-retest stability of
discourse measures in a late middle-aged cohort at risk for Alzheimer’s disease (AD).
Methods: Using a normative sample of three hundred ninety-nine participants (mean age = 61;
62% parental history of AD), exploratory factor analyses (EFA) and confirmatory factor analyses
(CFA) were conducted on 18 measures of connected language. Factor invariance across sex and
family history and longitudinal test-retest stability measures were calculated.
Results: The EFA revealed a 4-factor solution, consisting of semantic, syntax, fluency, and
lexical constructs. The CFA model substantiated the structure, and factors were invariant across
sex and family history. Test-retest stability measures were within acceptable ranges.
Conclusions: Results confirm a psychometrically sound factor structure that is invariant across
sex and family history. The factor structure could be useful in similar cohorts designed to detect
early cognitive decline or as outcome measures in clinical prevention trials.
101
The Latent Structure and Test-Retest Stability of Connected Language Measures in the
Wisconsin Registry for Alzheimer’s Prevention (WRAP)
INTRODUCTION
Alzheimer’s Disease (AD), the most common form of dementia, is neurodegenerative
disease that will affect more than 5 million Americans in 2017 (Association, 2014). Unless
scientists discover ways to prevent or delay the onset of AD, projected costs for the disease will
be over $1 trillion by 2050 (Association, 2014). Advances in imaging and biotechnology have
revealed that the neuropathological processes of AD begin years or decades before the onset of
clinical symptoms; therefore, researchers have been working to discover the most sensitive
measures for detecting cognitive change at the earliest point possible, i.e., in the Mild Cognitive
Impairment (MCI) stage or before. To this end, there has been an increasing number of
longitudinal studies of asymptomatic people who are at risk for AD (Beeri & Sonnen, 2016;
Coats & Morris, 2005; Ellis et al., 2009; Sager et al., 2005; Soldan et al., 2013). Studies of AD
risk groups allow for monitoring of both biomarker and cognitive profiles over time, and profiles
of biomarker positive groups may be informative in making predictions about future cognitive
decline (Racine et al., 2016).
The diagnosis of probable Alzheimer’s Disease (AD) requires that an individual show a
gradual and progressive change in memory function and at least one other cognitive domain,
causing interference with social and functional activities of daily living (Dubois et al., 2007;
McKhann et al., 2011). One of the other cognitive domains frequently affected is language, with
the most common complaint being word-retrieval problems (Clarnette, Almeida, Forstl, Paton, &
Martins, 2001). While typical assessment of language includes standardized testing of word
finding, over the last two decades researchers have been interested in moving beyond
102
standardized tests to examine speech and language in contexts that more closely approximate
everyday communication. Analysis of “connected language,” also referred to as “discourse,”
“connected speech,” or “spontaneous speech,” is the examination of spoken language produced
in a continuous sequence, as in everyday conversations. Because connected language analysis
can assess multiple cognitive-communication processes, it may be more sensitive to language
problems in the early stages of AD than are standardized language tests. Researchers elicit
connected language using a variety of methods, such as picture description tasks,
autobiographical narratives, and story-telling (e.g., “Tell me the story of Cinderella.”).
Connected language analysis may yield rich information about cognition, as tasks require a
complex interplay of not only retrieval from semantic and episodic memory stores, but also
executive functions for search and retrieval, planning, and shaping language to meet the
characteristics of the listener (Turkstra, 2001).
Studies of connected language in AD have used a multitude of measures due to the multi-
faceted nature of discourse. Specifically, researchers have analyzed semantic knowledge and
retrieval, syntactic complexity, speech fluency, pragmatic aspects of language (e.g., efficiency
and coherence), and narrative structure. Each of these connected language domains has been
linked to several underlying cognitive processes. For example, the semantic aspect of language is
purported to reflect the ability to access semantic and episodic memory systems, while complex
syntax and fluency may involve executive functions for the coordination of planning, search, and
retrieval. Pragmatic and social language functions may require self-monitoring and awareness of
the perspective or mental state of others, or “theory of mind” (Byom & Turkstra, 2012).
Although discourse measures have been well studied in AD, they are largely under-
investigated in the MCI literature. Also, most studies analyze multiple measures at once, which
103
may increase the risk of Type I error. Several researchers have grouped measures based on
theories linking measures to underlying linguistic constructs (e.g.,(Ahmed et al., 2013a; Ahmed
et al., 2013b; Vassiliki Rentoumi, Ladan Raoufian, Samrah Ahmed, Celeste A de Jager, & Peter
Garrard, 2014; Sajjadi et al., 2012; Sherratt, 2007; Wilson et al., 2010)), but few studies have
examined these constructs statistically. “Latent variables” refer to underlying constructs of
observable variables inferred from a statistical model, usually Exploratory Factor Analysis
(EFA) and/or Confirmatory Factor Analysis (CFA). By identifying a latent structure using
clusters of measures for each domain rather than each individual measure, redundancy and risk
of Type I error are minimized and the characteristics of everyday speech and language become
easier to interpret. This may be especially important for MCI groups, as language impairments in
these individuals will be less pronounced, and adjusting for multiple comparisons in a less
impaired group may place additional unnecessary constraints on analyses.
In addition to the multiple measures used to assess connected language, the within-group
variability of connected language is also problematic when attempting to identify group
differences (Duong et al., 2005). Possible contributing factors to variability in connected
language include age, education, and mood (Le Dorze & BÉDard, 1998; Murray,
2010).Variability can partially be addressed by within-subject study designs, where an
individual’s connected language is compared to his or her baseline over time. However, only a
handful of studies have assessed test-retest reliability of elicited discourse, and these have been
in adults with acquired aphasia (Brookshire & Nicholas, 1994b; Yorkston & Beukelman, 1980) .
One study (Forbes-McKay & Venneri, 2005) examined test-retest reliability of picture
description after one week in 40 cognitively normal individuals ages 23-84 years. The authors
found good reliability for some measures and significant practice effects for other measures,

104
however the small sample size and wide age range limit generalizability to other cohorts. No
study has assessed the stability of discourse measures over time, therefore the variability of these
measures within healthy adults is largely unknown.
We approached the present study with three aims. The first aim was to identify a latent
structure of connected language measures obtained from participants in the Wisconsin Registry
for Alzheimer’s Prevention (WRAP), a late-middle-aged asymptomatic cohort enriched for
familial risk of AD. Second, if the latent structure was confirmed with confirmatory factor
analysis, we aimed to determine the test-retest stability of these measures at two study time
points, approximately two years apart, in a group of cognitively stable individuals. Third, we
compared the factor structure between males and females, to determine if there was factor
invariance (i.e., the factors measured the same construct in the two groups). Studies have shown
that females perform better than males on tests of verbal learning and memory (Bleecker, Bolla-
Wilson, Agnew, & Meyers, 1988), but sex-based differences in connected language are less
understood. Our hypotheses were that there would be a set of factors with underlying constructs
pertaining to the content, speech fluency, and lexical processing of connected language; these
factors would be stable over time in a group of individuals who were identified as being
cognitively stable at two time points; and the factors would be invariant across men and women,
and across people with and without a family history of AD.
METHOD
Participants
WRAP Study Sample. Our study sample was drawn from the Wisconsin Registry for Alzheimer’s
Prevention (WRAP), a longitudinal study of late-middle-aged adults that is enriched for AD risk
105
based on parental family history. WRAP participants are asymptomatic and are between the ages
of 40 and 65 at the time of enrollment (Sager et al., 2005). Approximately 72% of participants
have a parent with either autopsy-confirmed or probable AD as defined by the National Institute
of Neurological and Communicative Disorders and Stroke and the Alzheimer’s disease and
Related Disorders Association (NINCDS-ADRDA) criteria (McKhann et al., 1984). The sample
consists of 71% women, with a mean age at baseline of 54 years. The longitudinal study design
includes a baseline visit and serial follow-up visits every two years thereafter. Collection of a
spontaneous speech sample was implemented at the third wave visit beginning in 2012, and
language sample collection has since been ongoing at each visit.
EFA/CFA Sample. The current study included WRAP participants with completed language
samples and neuropsychological assessments. Participants were drawn from a normative sample
that was created to establish robust normative data for detecting cognitive change in this group
(Clark et al., 2016). Specifically, the normative sample described by Clark et al. (2016) included
WRAP participants (n=476) with both positive and negative parental history of AD, but excluded
those at genetic risk for the disease. The criteria for inclusion in the Clark et al. normative
sample were 1) non-carrier of the APOE ε4 allele, 2) no history of neurological or major
psychiatric disorders by self-report, and 3) classified as cognitively normal at baseline and all
follow-up visits using normative factor scores derived from a previous study of WRAP (Koscik
et al., 2014).
Our study had the additional criteria that 1) participants had completed a language
sampling task and 2) they had not been classified as “Early MCI” or “Clinical MCI” in the
interim between the Clark et al. (2016) study and the collection of the speech sample. The
sample consisted of 399 participants, ranging in age from 43 to 75 (M = 61 years, SD = 7), with
106
an average education level of 16 years (SD = 2.7), and 67.2% were female. The race make-up of
the sample was 95% non-Hispanic White, 2.3% African-American, 1.8 % Spanish/Hispanic, and
.5% Native American. 62% of the sample had a family history of Alzheimer’s Disease (none of
the participants were APOE-ε4 positive, as noted in the exclusion criteria above).
Test/retest reliability sample. To test stability of the factor structure over time, we obtained two
sets of discourse samples from 124 participants, at time intervals ranging from 2.0 to 3.2 years
(mean=2.4 years, SD=1.04) (Longitudinal Group). These participants were then screened for
diagnoses of either “Early MCI” or “Clinical MCI” at the second time point. The sixteen
participants who were thus diagnosed were removed, resulting in a final subset of 108.
Discourse Collection Procedure
Participants provided informed consent to have their speech recorded while describing the
“Cookie Theft” picture from the Boston Diagnostic Aphasia Examination (Goodglass & Kaplan,
1983). Participants were instructed to “Tell me everything you see going on in this picture.”
Feedback was not provided during the descriptions by the test administrators; however, if
responses were unusually brief, evaluators provided the scripted prompt, “Do you see anything
else going on?” Language samples had a mean duration of 50.4 seconds, including prompts from
the examiner. All responses were recorded using an Olympus VN-6200PC digital audio recorder.
Transcriptions
Language samples were transcribed by a trained speech-language pathologist (KDM), and two
trained graduate students, using Codes for Human Analysis of Transcripts (CHAT)
(MacWhinney, 2000). Utterances were segmented into C-Units, an established metric for
discourse analysis defined as “an independent clause and all of its modifiers” (Hughes,
McGillivray, & Schmidek, 1997; Hunt, 1965). Transcriptions were coded for automatic analyses
107
by the Computer Language Analysis (CLAN) program (Macwhinney et al., 2011), including
codes for filled and unfilled pauses, repetitions, revisions, semantic units, errors (semantic,
phonological, lexical), and nonverbal behaviors (coughing, laughing, etc.). Semantic units, parts
of speech, total utterances, grammatical relations, and other quantifiers were then automatically
extracted by the CLAN program using the MOR and MEGRASP programs (MacWhinney,
2000).
Three raters analyzed 15% of samples to calculate inter-rater reliability. Reliability was
calculated using the RELY program within CLAN, and agreement was 92.4% for transcription
and 98% for coding of semantic units.
Discourse Measures
Variables submitted to the initial exploratory factor analysis are defined in Table 1. Variables
were chosen based on findings from previous literature on discourse analysis in MCI or
preclinical Alzheimer’s Disease (S. Ahmed et al., 2012a; Ahmed et al., 2013a; Ahmed et al.,
2013b; Fernando Cuetos, Juan Carlos Arango-Lasprilla, ClaramONika Uribe, Claudia Valencia,
& Francisco Lopera, 2007; Forbes-McKay et al., 2013; Forbes-McKay & Venneri, 2005; Forbes
et al., 2002; Kathleen C Fraser et al., 2015; Kimberly Diggle Mueller et al., 2016).
Analyses
Samples
Analyses were performed using a split-sample approach for cross-validation of the factor
structure. We used a randomization procedure within SPSS to assign 250 participants to the
exploratory factor analysis (EFA) group and 149 participants to the confirmatory factor analysis
(CFA) group. Table 2 shows the demographic composition of the two subsamples. The two
groups were similar across all variables except for Family History of AD, as the CFA group had
108
significantly more participants with a family history of AD than the EFA group. We address this
discrepancy by testing the invariance of the factor solution between family history positive and
family history negative (see below in CFA section).
Exploratory Factor Analysis (EFA)
We examined the latent structure of the discourse measures using a multi-step, exploratory factor
analysis procedure within the EFA group (N=250). Due to the non-normal distributions of the
data, we extracted the factors using "principal axis factor analysis,” which is recommended when
the assumption of normality is violated (Beavers et al., 2013; Fabrigar, Wegener, MacCallum, &
Strahan, 1999). To allow factors to be correlated, we performed an oblique (Promax) rotation of
the latent factors. We determined the optimal number of factors to retain by using a combination
of Kaiser’s K1 rule (Kaiser, 1960) (Eigenvalues greater than 1), Cattell’s scree plot (Cattell,
1966), Very Simple Structure (VSS) determination, and parallel analysis tests. Discourse
variables were selected in the final solution if their loadings were greater than .32 (Tabachnick &
Fidell, 2001), and cross-loadings were less than .32. All models were compared using the
standardized root-mean-square residual (SRMR), the root-mean-squared error of approximation
(RMSEA, the discrepancy between the hypothesized model and the population covariance
matrix), non-normed fit index (NNFI, the comparison of the hypothesized model and the null
model), the comparative fit index (CFI, measures the discrepancy between the data and the
hypothesized model), the goodness of fit index (GFI, measure of fit between the hypothesized
model and the observed covariance matrix), and the adjusted goodness of fit (AGFI) index. We
selected the final model by using the acceptability criteria defined by Dowling et al. (2010) in
their factor analysis of the WRAP neuropsychological test battery: CFI > .90, NNFI > .90,
RMSEA <.08 (Dowling, Hermann, La Rue, & Sager, 2010). In addition, interpretability and
109
theoretical significance were considered in final model selection. EFA models were fitted and
scree tests, Very Simple Structure (VSS)(Revelle & Rocklin, 1979), and parallel tests were
performed using the psych package (Revelle, 2014) in R statistical software version 3.3.2 (Team,
2013).
Confirmatory Factor Analysis (CFA)
After selecting the final EFA model, we evaluated the fit of the factor structure within the CFA
group using strict constraints based on principles of structural equation modeling, whereby the
model is specified ahead of the analysis. All CFA analyses were performed using the R lavaan
package (Rosseel, 2012). Method of extraction was “unweighted least squares” (ULS), due to the
non-normal distribution of some of the variables’ residuals (Jöreskog & Sörbom, 1986).
Multiple-group confirmatory factor analysis was then performed to test for measurement
invariance between male versus female participants, and positive vs. negative family history.
Using the R semtools package, we tested for the following types of invariance: configural
invariance (identical factor structure across groups), metric invariance (identical factor loadings),
and scalar invariance (identical means).
Longitudinal Test-Retest Stability of Factor Structure
In the final step, we measured the test-retest stability of the resulting factor structure within the
Longitudinal Group. Using R, we computed three test-retest reliability estimates: the Pearson’s
correlation coefficient (r), two-way random effects model intra-class correlation coefficients
(ICC), Cronbach’s alpha (Cronbach, 1951), and the coefficient of repeatability (Beckerman et
al., 2001). In interpreting reliability measures, we used Fleiss’s (Fleiss, 1986) criteria for ICC,
which described values from .40 to .75 as “fair to good” and values greater than .75 as
“excellent”; however, due to the arbitrary nature of these inferences and the fact that
110
measurements were taken more than two years apart, we also considered absolute measures of
reliability that take random and systematic error into account. Specifically, we calculated the
coefficient of repeatability (CR), also known as the “Smallest Real Difference” (SMD), which is
calculated by multiplying the Standard Error of Measurement (SEM) by 2.77, and thus provides
the value below which the absolute differences between two measurements would lie with .95
probability (Vaz, Falkmer, Passmore, Parsons, & Andreou, 2013).
RESULTS
Exploratory Factor Analysis
We examined a variety of models and found that some variables were either too strongly
correlated with one another (e.g., total pronouns with unique words (r=.85), total filled pauses
with maze index (r=.72)), or failed to load on any factor within any model iteration (e.g., total
inferences). These variables were then removed from the EFA and models were rerun using the
remaining variables. Scree tests, parallel analyses, and Very Simple Structure analyses revealed
that a four-factor model explained 60% of the total variance among the discourse measures (see
Figure 2). Table 3 shows factors and factor loadings. Factor correlations ranged from .07 to .43,
which justified the Promax rotation. The four-factor model provided a good fit: empirical
χ2=27.86 (p<.05), RMSR = .03, NNFI = .90, RMSEA index = .08 (90% confidence interval =
.06-.117). Correlations between estimated factor scores from the observed variables and related
latent factors were above the cut-off of .80 (Gorsuch, 1997), thus validating the factor score
estimates.
Confirmatory Factor Analysis
Based on the results from the EFA, a four-factor conceptual model was submitted to CFA. Initial
results of the CFA indicated that variance estimates were negative for total unfilled pauses,
111
which may reflect the highly skewed distribution of this variable. Therefore, the submitted model
included only Maze Index as the variable for the Fluency Factor. Figure 3 shows the final
conceptual model.
Once the variable total unfilled pauses was removed, the CFA model proved to be a good
fit, with the following satisfactory fit indices: χ2=35.63, CFI = .99, NNFI = .99, RMSEA=.04,
90% confidence interval=.00-.08, GFI=.98, AGFI=.97, SRMR = .07. Table 4 shows the CFA
results using the cross-validation subsample (N=149). The average variance extracted (AVE) for
each factor, ranging from .53 to .72, was higher than the square of the correlations among the
four factors (ranging from .001 to .37). This provides evidence for discriminant validity among
factors (Fornell & Larcker, 1981).
Factor Invariance Across Sex and Family History
As the small CFA sample size did not allow factor invariance measures to be computed, we
checked for factor invariance using the full sample (N=399). All fit indices yielded acceptable
measures of fit for the four types of invariance: configural model (CFI=.95; RMSEA=.08), equal
loadings (CFI=.94, RMSEA=.08), equal intercepts (CFI=.95, RMSEA=.07), and equal means
(CFI=.95; RMSEA = .07), indicating that there were no sex-based differences in the factor
estimates. Similarly, there were no differences between subgroups with positive vs. negative
family history, with acceptable invariance fit measures of the configural model (CFI=.95;
RMSEA=.08; equal loadings (CFI=.95; RMSEA = .07), and equal means (CFI=.96; RMSEA =
.06).
Test-Retest Stability of the Discourse Factor Scores
The measures of relative and absolute reliability of the factor scores between two time points are
presented in Table 5. Overall, all of the factor scores were not significantly different between the
112
two time points, and each factor yielded a coefficient of repeatability that was within the
expected interval.
Lexical Factor. Factor stability from time 1 to time 2 was classified as “good” (Fleiss, 1986),
with an alpha coefficient of .77, intraclass correlation coefficient of .76, and a mean difference
score of .09 that fell within the repeatability coefficient (CR) of ±.23. A paired sample t-test of
the two time points showed that the two scores were not significantly different (p = .25).
Semantic Factor. The semantic factor yielded an intraclass correlation coefficient of .49 (“fair”;
Fleiss, 1986), an alpha of .50, and a repeatability coefficient of ±.32. The mean difference score
was .02, which falls within the CR interval. The paired sample t-test showed that the scores
between the two time points were not significantly different (p=.86).
Syntax Factor. The syntax factor yielded an ICC of .49 (“fair”), an alpha of .49, and a CR of .32.
The mean difference of .07 fell within the CR, and the paired difference test revealed no
signficant difference (p=.32).
Fluency Factor. The fluency factor had an ICC of .68 (“good”), an alpha of .69, and a CR of .28.
The mean difference of .20 fell within the CR of ±.28, and the paired difference test revealed no
signfificant difference between the two time points (p=.05, adjusted alpha=.0125).
113
DISCUSSION
Several studies have shown that connected language analysis can contribute to early
detection of Alzheimer’s Disease (Ahmed et al., 2013b) and help distinguish Alzheimer’s type
dementia from other disorders (Gorno-Tempini et al., 2011; Murray, 2010; Nicholas et al.,
1985). Because of the multifaceted nature of discourse, there are numerous measures that can be
derived. We set out to determine the underlying constructs of multiple discourse measures
obtained from a picture description task administered to participants in the Wisconsin Registry
for Alzheimer’s Prevention. Once this latent structure was defined, we tested both the structure’s
stability over time in a group of individuals identified as cognitively stable, as well as the
invariance of these factors between males and females, and across participants with and without
a family history.
Results of the exploratory and confirmatory factor analyses revealed a 4-factor solution
that explained 64% of the total variance among the connected language measures. The latent
factors were similar to those identified in the discourse of adults with AD and other dementias
(Ahmed et al., 2013a; Kathleen C Fraser et al., 2015; Wilson et al., 2010). Fraser et al. performed
an exploratory factor analysis of picture descriptions from 240 AD patients (mean age = 71.8)
and 233 controls (mean age = 65.2) taken from the DementiaBank corpus (Macwhinney et al.,
2011). Following a machine-learning classification of 370 linguistic features, the authors found a
four-factor solution that bore some similarities to our EFA/CFA solution. Like us, Fraser et al.
named a semantic factor that included pronoun ratio, percent verbs, and percent nouns; and a
syntax factor that included a measure of verbs and some measures of complex syntactic forms
(e.g., auxiliaries, participles). Duong et al. (2005) performed a cluster analysis of discourse
measures with subsequent principle components analysis, and found significant heterogeniety of
114
discourse patterns among adults with AD, due to factors such as education, age, sex, and
heterogeniety in cognitive decline over time. Our study differed from those of Duong et al.
(2005) and Fraser et al., 2015 in several ways. First, we examined linguistic variables in a group
of individuals that were cognitively stable across at least two time points, which allows us to
establish patterns of unimpaired adults for future comparisons. Second, we performed a
confirmatory factor analysis using a split-sample approach, and tested the stability of factors over
time, which added validity to the latent factor structure. Finally, our study captured a latent
structure in a group that was younger than any other previously reported group (mean age = 61
years). The ability to detect stable discourse patterns in younger adults will allow us to detect
subtle change earlier in the disease process, which may be critical in future longitudinal studies
of preclinical AD.
One of the problems in the discourse literature is the use of different variables to measure
highly similar constructs, which leads to difficulty aggregating findings across samples and
limits replicability and reproducibility. We addressed the problem of multiple measures by using
an exploratory factor analysis to define factors. Our study is the first to use a split-sample
approach to EFA/CFA in order to determine the reliability of a latent factor model of connected
language measures, which lends support to the model’s reproducibility in similar cohorts. We
validated the model by testing factor invariance between males and females, and between those
with a positive vs. negative family history of AD. By demonstrating factor invariance in these
two subgroups of interest, we provide evidence that differences in test scores across subgroups
will represent true differences rather than measurement bias (Byrne, Shavelson, & Muthén,
1989; Dowling et al., 2010).
115
Another major finding of our study was the test-retest stability of the factor structure over
time. Very few studies have examined test-retest stability across intervals typically used in
longitudinal studies. Yorkston & Beukelman (1980) asked 10 adults with aphasia to describe the
cookie theft picture twice in the same day, and found that scores for content units were stable.
Shewan (1988) examined test-retest stability one month between discourse samples and found
correlations of .89 on discourse measures. Both Forbes-McKay & Venneri (2005) and
Brookshire & Nicholas (1994) examined test-retest reliability of picture description tasks one
week between tests. Forbes-McKay found correlations between .81 to 1.00 on some measures,
but lower correlations for measures that improved due to practice effects (information content,
semantic paraphasias). Brookshire & Nicholas found that test-retest stability increased as sample
length increased, and recommended language sample sizes of between 300-400 words for
reliability within the population of people with aphasia. Some of the aforementioned studies
examined reliability in persons with aphasia, which will not generalize to other groups. In the
groups that studied healthy adults, the test intervals were between one week and one month
apart. Because the cookie theft picture is a simple description task, test-retest reliability within
short intervals is most likely going to be subject to significant practice effects in healthy adults
(Bartels, Wegrzyn, Wiedl, Ackermann, & Ehrenreich, 2010).
Our approach was to examine the stability of the factor structure in a group of individuals
who had remained stable on other cognitive measures for an average of more than two years.
This method assumes that cognitive stability on standardized measures would yield stability on
connected language measures, but research to back this assumption is limited. Statistical methods
like Pearson’s correlations or Interclass Correlation Coefficients (ICC) would not account for the
increased variability and measurement error that could occur over a longer time interval, so
116
instead we used the coefficient of reliability (Vaz et al., 2013). All factor scores between the two
time points yielded repeatability coefficients within acceptable intervals.
LIMITATIONS AND FUTURE DIRECTIONS
A limitation of this study is that not all possible dimensions of connected language were
submitted to the factor analyses. We chose measures most commonly associated with discourse
deficits in early AD or MCI, based on a thorough review of the literature. Accordingly, the
measures were related to word-retrieval difficulties, such as production of content units, ratios of
nouns to pronouns, or speech disfluencies that could result from poor search and retrieval. Other
measures, such as error monitoring, words per minute, or response to word-finding delays were
not included and may have loaded on and strengthened one of the latent factors, or perhaps
loaded on a new factor. We chose the variables that were most associated with decline at the
MCI stage, and while timing data can also be a reflection of word retrieval difficulties, the “maze
index” variable, which includes filled and unfilled pauses, revisions, false starts, and repetitions,
is a substantial measure of the search and retrieval process.
Another limitation was the relatively homogenous sample of participants. The sample
was recruited primarily from a highly educated, predominantly non-Hispanic and white
population, and our findings may not generalize to other study populations. The psychometric
properties of connected language measures should be further examined in more diverse samples,
and measurements should be adjusted to represent semantic, grammatical, and phonological rules
of different dialects and languages.
CONCLUSION
This study addressed an urgent priority of the Alzheimer’s Association’s Research
Roundtable (AARR): to identify appropriately sensitive tools to measure cognitive and
117
functional change in “presymptomatic” AD or very early MCI (Snyder et al., 2014). The AARR
noted challenges in accomplishing this goal, including that existing tools are insensitive to very
mild deficits, and may measure different constructs across cultural and ethnic groups, between
men and women, and across lifestyle variables that may influence the development of cognitive
decline. Synder et al. 2014 recommended using performance-based assessments in addition to
self-report scales, and we propose that connected language assessment can be a reliable,
performance-based assessment tool. Standardized assessment of verbal fluency tasks has shown
promising results in distinguishing between healthy aging and MCI (Clark et al., 2009; Mueller
et al., 2015; Murphy, Rich, & Troyer, 2006; Nutter-Upham et al., 2008; Papp et al., 2016), but
performance on standardized tests has provided little information about everday function (Kavé
& Goral, 2016).
To our knowledge, this is the largest cross-sectional or longitudinal study of connected
language in a preclinical AD cohort. It is therefore a valuable resource for documenting
connected language changes in both normally aging adults and also those showing very early
cognitive decline. The next step is to examine the latent factors identified here in those who are
declining on other cognitive measures. By combining information from longitudinal standardized
assessment and longitudinal connected language analyses, we may be able to identify functional
changes associated with early MCI, and not only provide outcome measures for clinical trials but
also identify handicapping and potentially treatable language signs and symptoms in adults with
MCI.
118
REFERENCES
1. Association, A.s.2014 Facts and Figures - Alzheimer's Association. (n.d.). . 2014;
Available from: http://www.alz.org/downloads/facts_figures_2014.pdf.
2. Sager, M.A., B. Hermann, and A. La Rue, Middle-aged children of persons with
Alzheimer's disease: APOE genotypes and cognitive function in the Wisconsin Registry
for Alzheimer's Prevention. J Geriatr Psychiatry Neurol, 2005. 18(4): p. 245-9.
3. Ellis, K.A., et al., The Australian Imaging, Biomarkers and Lifestyle (AIBL) study of
aging: methodology and baseline characteristics of 1112 individuals recruited for a
longitudinal study of Alzheimer's disease. Int Psychogeriatr, 2009. 21(4): p. 672-87.
4. Coats, M. and J.C. Morris, Antecedent biomarkers of Alzheimer's disease: the adult
children study. J Geriatr Psychiatry Neurol, 2005. 18(4): p. 242-4.
5. Soldan, A., et al., Relationship of cognitive reserve and cerebrospinal fluid biomarkers to
the emergence of clinical symptoms in preclinical Alzheimer's disease. Neurobiol Aging,
2013. 34(12): p. 2827-34.
6. Beeri, M.S. and J. Sonnen, Brain BDNF expression as a biomarker for cognitive reserve
against Alzheimer disease progression. Neurology, 2016. 86(8): p. 702-3.
7. Racine, A.M., et al., Biomarker clusters are differentially associated with longitudinal
cognitive decline in late midlife. Brain, 2016. 139(Pt 8): p. 2261-74.
8. McKhann, G.M., et al., The diagnosis of dementia due to Alzheimer's disease:
recommendations from the National Institute on Aging-Alzheimer's Association
workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement, 2011.
7(3): p. 263-9.
9. Dubois, B., et al., Research criteria for the diagnosis of Alzheimer's disease: revising the
NINCDS–ADRDA criteria. The Lancet Neurology, 2007. 6(8): p. 734-746.
10. Clarnette, R.M., et al., Clinical characteristics of individuals with subjective memory loss
in Western Australia: results from a cross‐sectional survey. International journal of
geriatric psychiatry, 2001. 16(2): p. 168-174.
11. Turkstra, L.S., Partner effects in adolescent conversations. Journal of Communication
Disorders, 2001. 34(1–2): p. 151-162.
12. Byom, L.J. and L. Turkstra, Effects of social cognitive demand on theory of mind in
conversations of adults with traumatic brain injury. International journal of language &
communication disorders, 2012. 47(3): p. 310-321.
13. Ahmed, S., et al., Semantic processing in connected speech at a uniformly early stage of
autopsy-confirmed Alzheimer's disease. Neuropsychology, 2013. 27(1): p. 79-85.
14. Ahmed, S., et al., Connected speech as a marker of disease progression in autopsy-
proven Alzheimer's disease. Brain, 2013. 136(Pt 12): p. 3727-37.
119
15. Rentoumi, V., et al., Features and Machine Learning Classification of Connected Speech
Samples from Patients with Autopsy Proven Alzheimer's Disease with and without
Additional Vascular Pathology. Journal of Alzheimer's Disease, 2014. 42(s3).
16. Wilson, S.M., et al., Connected speech production in three variants of primary
progressive aphasia. Brain, 2010. 133(Pt 7): p. 2069-88.
17. Sherratt, S., Multi‐level discourse analysis: A feasible approach. Aphasiology, 2007.
21(3-4): p. 375-393.
18. Sajjadi, S.A., et al., Abnormalities of connected speech in semantic dementia vs
Alzheimer's disease. Aphasiology, 2012. 26(6): p. 847-866.
19. Duong, A., et al., The heterogeneity of picture-supported narratives in Alzheimer's
disease. Brain Lang, 2005. 93(2): p. 173-84.
20. Murray, L.L., Distinguishing clinical depression from early Alzheimer's disease in
elderly people: Can narrative analysis help? Aphasiology, 2010. 24(6-8): p. 928-939.
21. Le Dorze, G. and C. BÉDard, Effects of age and education on the lexico-semantic content
of connected speech in adults. Journal of communication disorders, 1998. 31(1): p. 53-71.
22. Brookshire, R.H. and L.E. Nicholas, Test-retest stability of measures of connected speech
in aphasia. Clinical aphasiology, 1994. 22(1): p. 19-133.
23. Yorkston, K.M. and D.R. Beukelman, An analysis of connected speech samples of
aphasic and normal speakers. Journal of speech and hearing disorders, 1980. 45(1): p.
27-36.
24. Forbes-McKay, K.E. and A. Venneri, Detecting subtle spontaneous language decline in
early Alzheimer's disease with a picture description task. Neurol Sci, 2005. 26(4): p. 243-
54.
25. Bleecker, M.L., et al., Age? related sex differences in verbal memory. Journal of clinical
psychology, 1988. 44(3): p. 403-411.
26. McKhann, G., et al., Clinical diagnosis of Alzheimer's disease Report of the NINCDS‐ADRDA Work Group* under the auspices of Department of Health and Human Services
Task Force on Alzheimer's Disease. Neurology, 1984. 34(7): p. 939-939.
27. Clark, L.R., et al., Mild Cognitive Impairment in Late Middle Age in the Wisconsin
Registry for Alzheimer's Prevention Study: Prevalence and Characteristics Using Robust
and Standard Neuropsychological Normative Data. Arch Clin Neuropsychol, 2016.
28. Koscik, R.L., et al., Emergence of mild cognitive impairment in late middle-aged adults
in the wisconsin registry for Alzheimer's prevention. Dement Geriatr Cogn Disord, 2014.
38(1-2): p. 16-30.
29. Goodglass, H. and E. Kaplan, Boston diagnostic aphasia examination booklet. 1983: Lea
& Febiger.
30. MacWhinney, B., The CHILDES project: Tools for analyzing talk. 3rd Lawrence
Erlbaum Associates. Mahwah, NJ, 2000.
120
31. Hunt, K.W., Grammatical Structures Written at Three Grade Levels. NCTE Research
Report No. 3. 1965.
32. Hughes, D.L., L. McGillivray, and M. Schmidek, Guide to narrative language:
Procedures for assessment. 1997: Thinking Publications Eau Claire, WI.
33. Macwhinney, B., et al., AphasiaBank: Methods for Studying Discourse. Aphasiology,
2011. 25(11): p. 1286-1307.
34. Ahmed, S., et al., Logopenic aphasia in Alzheimer's disease: clinical variant or clinical
feature? J Neurol Neurosurg Psychiatry, 2012. 83(11): p. 1056-62.
35. Fraser, K.C., J.A. Meltzer, and F. Rudzicz, Linguistic Features Identify Alzheimer’s
Disease in Narrative Speech. Journal of Alzheimer's Disease, 2015. 49(2): p. 407-422.
36. Forbes, K.E., A. Venneri, and M.F. Shanks, Distinct patterns of spontaneous speech
deterioration: an early predictor of Alzheimer's disease. Brain Cogn, 2002. 48(2-3): p.
356-61.
37. Forbes-McKay, K., M.F. Shanks, and A. Venneri, Profiling spontaneous speech decline
in Alzheimer's disease: a longitudinal study. Acta neuropsychiatrica, 2013. 25(06): p.
320-327.
38. Cuetos, F., et al., Linguistic changes in verbal expression: a preclinical marker of
Alzheimer's disease. Journal of the International Neuropsychological Society, 2007.
13(03): p. 433-439.
39. Mueller, K.D., et al., Connected Language in Late Middle-Aged Adults at Risk for
Alzheimer’s Disease. Journal of Alzheimer's Disease, 2016(Preprint): p. 1-12.
40. Beavers, A.S., et al., Practical considerations for using exploratory factor analysis in
educational research. Practical assessment, research & evaluation, 2013. 18(6): p. 1-13.
41. Fabrigar, L.R., et al., Evaluating the use of exploratory factor analysis in psychological
research. Psychological methods, 1999. 4(3): p. 272.
42. Kaiser, H.F., The application of electronic computers to factor analysis. Educational and
Psychological Measurement, 1960. 20: p. 141-151.
43. Cattell, R.B., The scree test for the number of factors. Multivariate behavioral research,
1966. 1(2): p. 245-276.
44. Tabachnick, B. and L.S. Fidell, Cleaning up your act: screening data prior to analysis.
Using multivariate statistics, 2001. 5: p. 61-116.
45. Dowling, N.M., et al., Latent structure and factorial invariance of a neuropsychological
test battery for the study of preclinical Alzheimer's disease. Neuropsychology, 2010.
24(6): p. 742.
46. Revelle, W. and T. Rocklin, Very simple structure: An alternative procedure for
estimating the optimal number of interpretable factors. Multivariate Behavioral
Research, 1979. 14(4): p. 403-414.
121
47. Revelle, W., psych: Procedures for psychological, psychometric, and personality
research. Northwestern University, Evanston, Illinois, 2014: p. 165.
48. Team, R.C., R: A language and environment for statistical computing. 2013.
49. Rosseel, Y., lavaan: An R package for structural equation modeling. Journal of Statistical
Software, 2012. 48(2): p. 1-36.
50. Jöreskog, K.G. and D. Sörbom, LISREL VI: Analysis of linear structural relationships by
maximum likelihood, instrumental variables, and least squares methods. 1986: Scientific
Software.
51. Cronbach, L.J., Coefficient alpha and the internal structure of tests. Psychometrika,
1951. 16(3): p. 297-334.
52. Beckerman, H., et al., Smallest real difference, a link between reproducibility and
responsiveness. Qual Life Res, 2001. 10(7): p. 571-8.
53. Fleiss, J.L., Reliability of measurement. The design and analysis of clinical experiments,
1986: p. 1-32.
54. Vaz, S., et al., The case for using the repeatability coefficient when calculating test–retest
reliability. PLoS One, 2013. 8(9): p. e73990.
55. Gorsuch, R.L., Exploratory factor analysis: Its role in item analysis. Journal of
personality assessment, 1997. 68(3): p. 532-560.
56. Fornell, C. and D.F. Larcker, Structural equation models with unobservable variables
and measurement error: Algebra and statistics. Journal of marketing research, 1981: p.
382-388.
57. Nicholas, M., et al., Empty speech in Alzheimer's disease and fluent aphasia. J Speech
Hear Res, 1985. 28(3): p. 405-10.
58. Gorno-Tempini, M., et al., Classification of primary progressive aphasia and its variants.
Neurology, 2011. 76(11): p. 1006-1014.
59. Byrne, B.M., R.J. Shavelson, and B. Muthén, Testing for the equivalence of factor
covariance and mean structures: The issue of partial measurement invariance.
Psychological bulletin, 1989. 105(3): p. 456.
60. Bartels, C., et al., Practice effects in healthy adults: a longitudinal study on frequent
repetitive cognitive testing. BMC neuroscience, 2010. 11(1): p. 118.
61. Snyder, P.J., et al., Assessing cognition and function in Alzheimer's disease clinical trials:
Do we have the right tools? Alzheimer's & Dementia, 2014. 10(6): p. 853-860.
62. Clark, L.J., et al., Longitudinal verbal fluency in normal aging, preclinical, and prevalent
Alzheimer's disease. Am J Alzheimers Dis Other Demen, 2009. 24(6): p. 461-8.
63. Murphy, K.J., J.B. Rich, and A.K. Troyer, Verbal fluency patterns in amnestic mild
cognitive impairment are characteristic of Alzheimer's type dementia. Journal of the
International Neuropsychological Society, 2006. 12(04): p. 570-574.
122
64. Nutter-Upham, K.E., et al., Verbal fluency performance in amnestic MCI and older
adults with cognitive complaints. Arch Clin Neuropsychol, 2008. 23(3): p. 229-41.
65. Mueller, K.D., et al., Verbal Fluency and Early Memory Decline: Results from the
Wisconsin Registry for Alzheimer's Prevention. Arch Clin Neuropsychol, 2015. 30(5): p.
448-57.
66. Papp, K.V., et al., Biomarker validation of a decline in semantic processing in preclinical
Alzheimer’s disease. Neuropsychology, 2016. 30(5): p. 624.
67. Kavé, G. and M. Goral, Word retrieval in picture descriptions produced by individuals
with Alzheimer’s disease. Journal of clinical and experimental neuropsychology, 2016.
38(9): p. 958-966.
68. Wechsler, D., Wechsler abbreviated scale of intelligence. 1999: Psychological
Corporation.
69. Wilkinson, G.S., WRAT-3: Wide range achievement test. 1993: Wide Range.
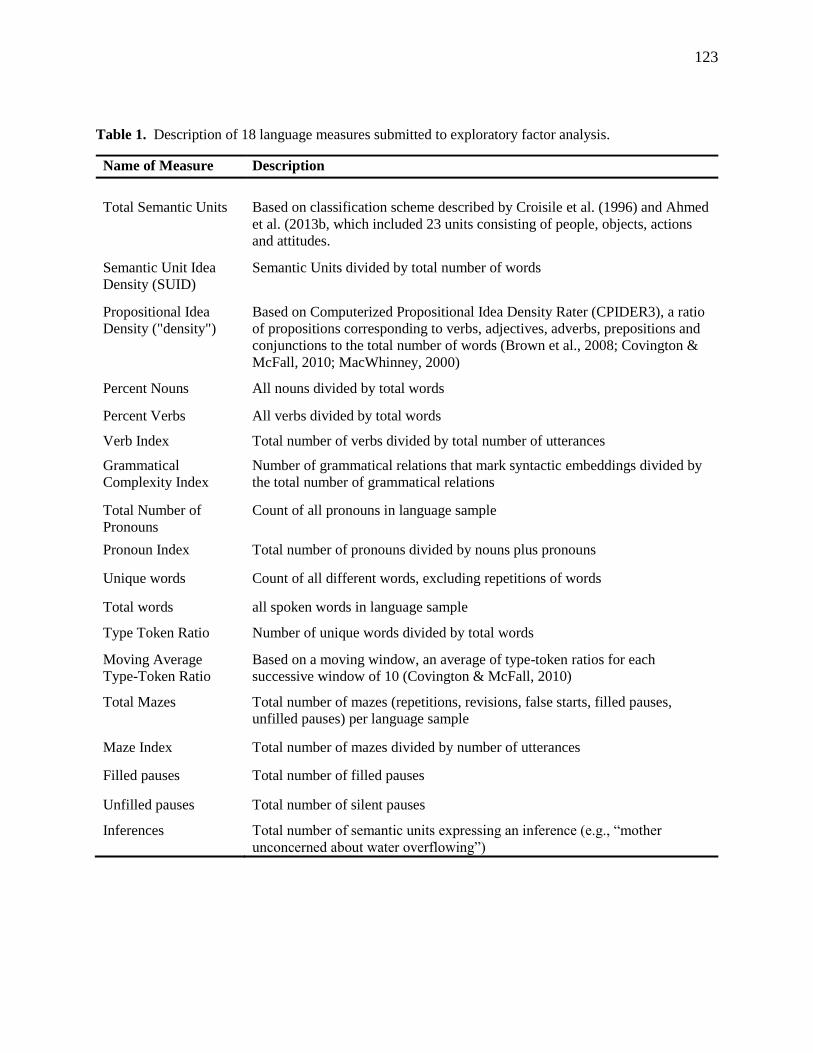
123
Table 1. Description of 18 language measures submitted to exploratory factor analysis.
Name of Measure Description
Total Semantic Units Based on classification scheme described by Croisile et al. (1996) and Ahmed
et al. (2013b, which included 23 units consisting of people, objects, actions
and attitudes.
Semantic Unit Idea
Density (SUID)
Semantic Units divided by total number of words
Propositional Idea
Density ("density")
Based on Computerized Propositional Idea Density Rater (CPIDER3), a ratio
of propositions corresponding to verbs, adjectives, adverbs, prepositions and
conjunctions to the total number of words (Brown et al., 2008; Covington &
McFall, 2010; MacWhinney, 2000)
Percent Nouns All nouns divided by total words
Percent Verbs All verbs divided by total words
Verb Index Total number of verbs divided by total number of utterances
Grammatical
Complexity Index
Number of grammatical relations that mark syntactic embeddings divided by
the total number of grammatical relations
Total Number of
Pronouns
Count of all pronouns in language sample
Pronoun Index Total number of pronouns divided by nouns plus pronouns
Unique words Count of all different words, excluding repetitions of words
Total words all spoken words in language sample
Type Token Ratio Number of unique words divided by total words
Moving Average
Type-Token Ratio
Based on a moving window, an average of type-token ratios for each
successive window of 10 (Covington & McFall, 2010)
Total Mazes Total number of mazes (repetitions, revisions, false starts, filled pauses,
unfilled pauses) per language sample
Maze Index Total number of mazes divided by number of utterances
Filled pauses Total number of filled pauses
Unfilled pauses Total number of silent pauses
Inferences Total number of semantic units expressing an inference (e.g., “mother
unconcerned about water overflowing”)
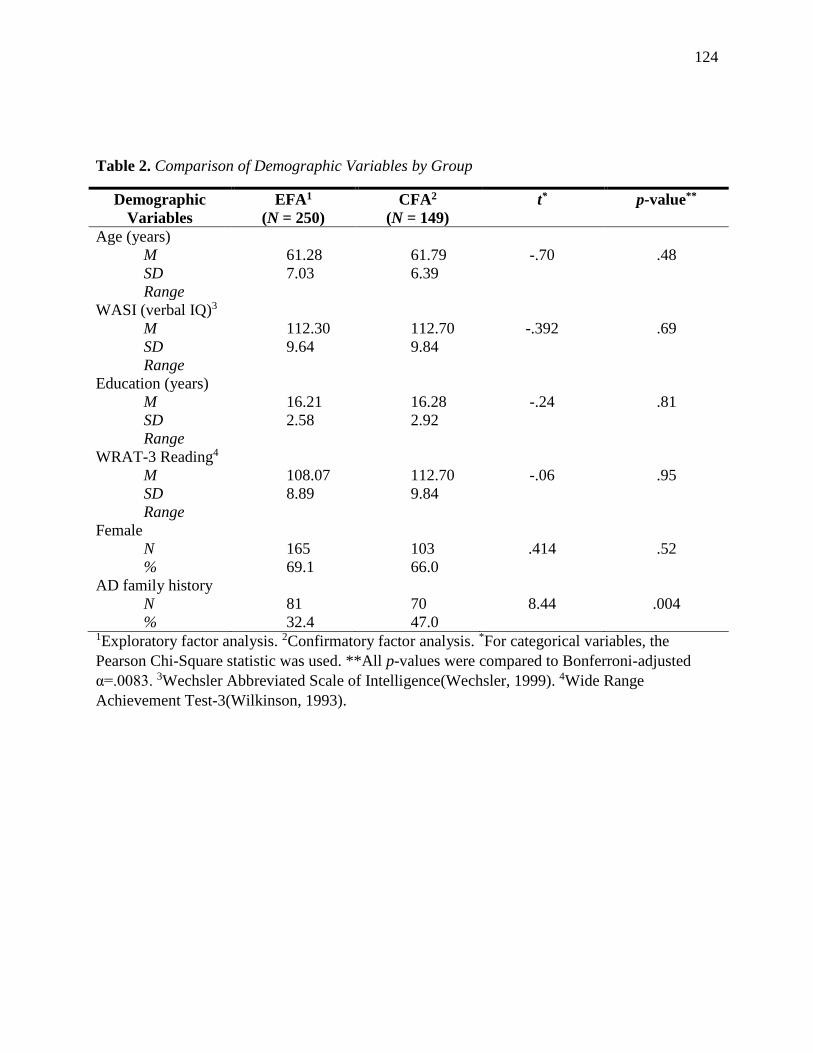
124
Table 2. Comparison of Demographic Variables by Group
Demographic
Variables
EFA1
(N = 250)
CFA2
(N = 149)
t* p-value**
Age (years)
M
SD
Range
61.28
7.03
61.79
6.39
-.70
.48
WASI (verbal IQ)3
M
SD
Range
112.30
9.64
112.70
9.84
-.392
.69
Education (years)
M
SD
Range
16.21
2.58
16.28
2.92
-.24
.81
WRAT-3 Reading4
M
SD
Range
108.07
8.89
112.70
9.84
-.06
.95
Female
N
%
165
69.1
103
66.0
.414
.52
AD family history
N
%
81
32.4
70
47.0
8.44
.004
1Exploratory factor analysis. 2Confirmatory factor analysis. *For categorical variables, the
Pearson Chi-Square statistic was used. **All p-values were compared to Bonferroni-adjusted
α=.0083. 3Wechsler Abbreviated Scale of Intelligence(Wechsler, 1999). 4Wide Range
Achievement Test-3(Wilkinson, 1993).
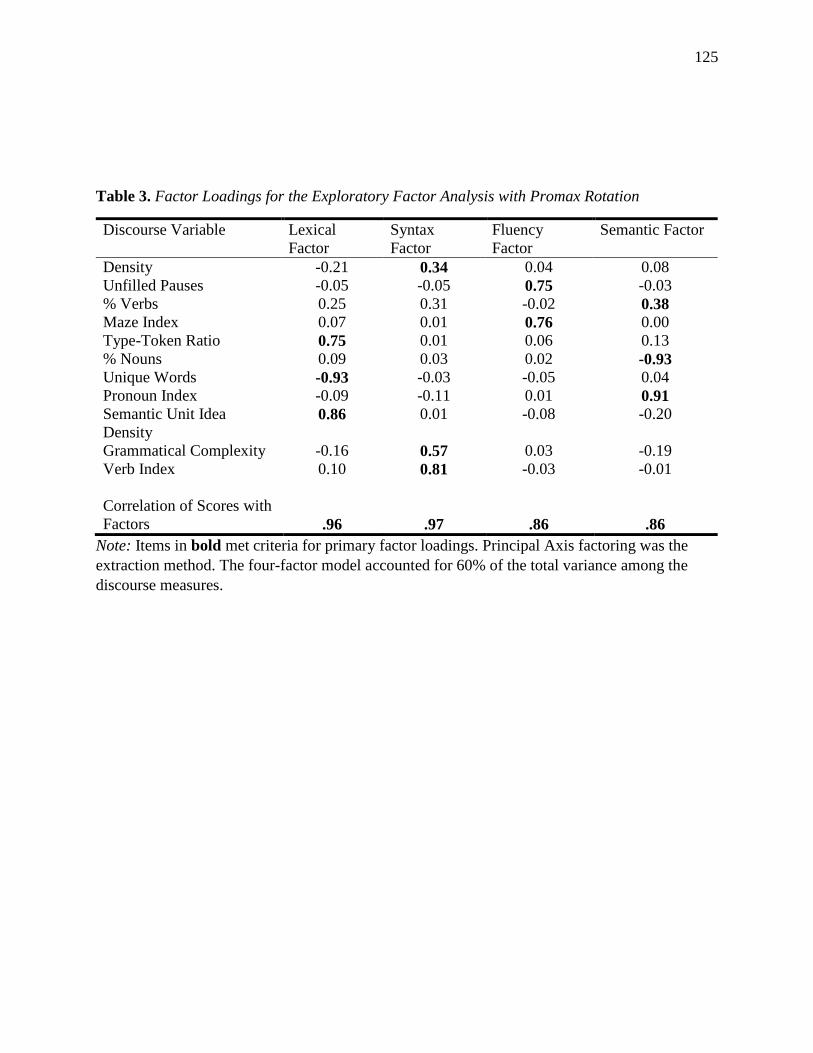
125
Table 3. Factor Loadings for the Exploratory Factor Analysis with Promax Rotation
Discourse Variable Lexical
Factor
Syntax
Factor
Fluency
Factor
Semantic Factor
Density -0.21 0.34 0.04 0.08
Unfilled Pauses -0.05 -0.05 0.75 -0.03
% Verbs 0.25 0.31 -0.02 0.38
Maze Index 0.07 0.01 0.76 0.00
Type-Token Ratio 0.75 0.01 0.06 0.13
% Nouns 0.09 0.03 0.02 -0.93
Unique Words -0.93 -0.03 -0.05 0.04
Pronoun Index -0.09 -0.11 0.01 0.91
Semantic Unit Idea
Density 0.86 0.01 -0.08 -0.20
Grammatical Complexity -0.16 0.57 0.03 -0.19
Verb Index 0.10 0.81 -0.03 -0.01
Correlation of Scores with
Factors
.96
.97
.86
.86
Note: Items in bold met criteria for primary factor loadings. Principal Axis factoring was the
extraction method. The four-factor model accounted for 60% of the total variance among the
discourse measures.
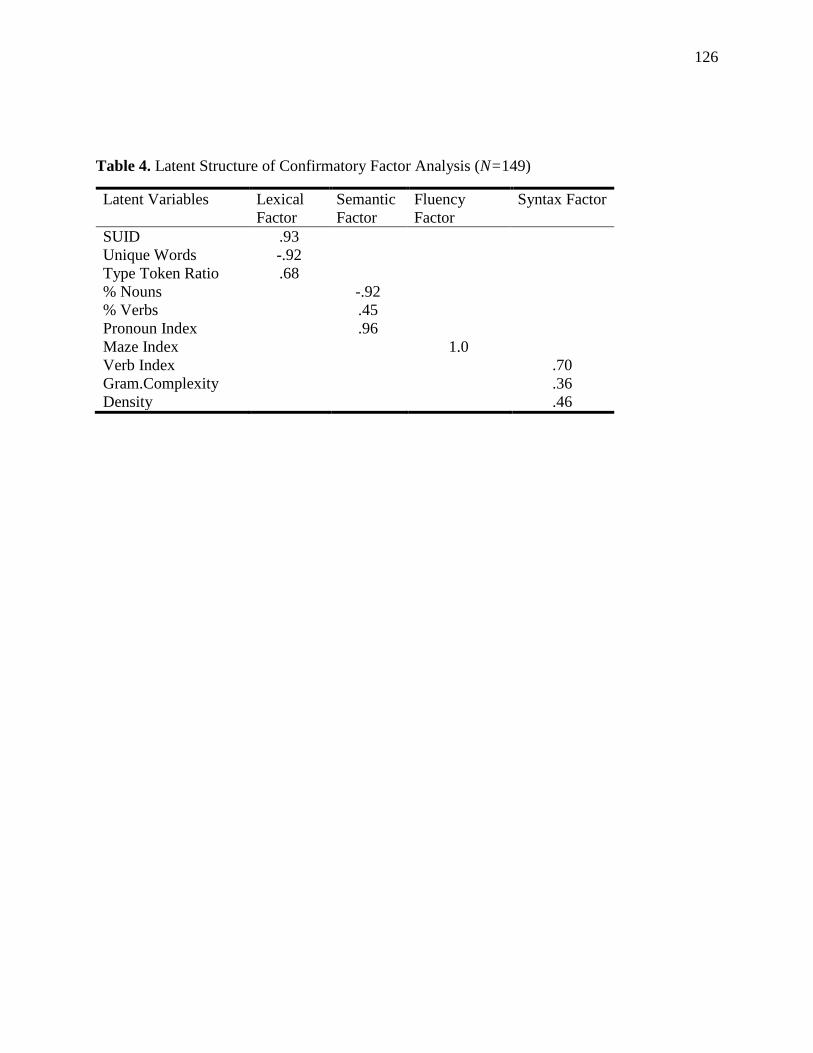
126
Table 4. Latent Structure of Confirmatory Factor Analysis (N=149)
Latent Variables Lexical
Factor
Semantic
Factor
Fluency
Factor
Syntax Factor
SUID .93
Unique Words -.92
Type Token Ratio .68
% Nouns -.92
% Verbs .45
Pronoun Index .96
Maze Index 1.0
Verb Index .70
Gram.Complexity .36
Density .46
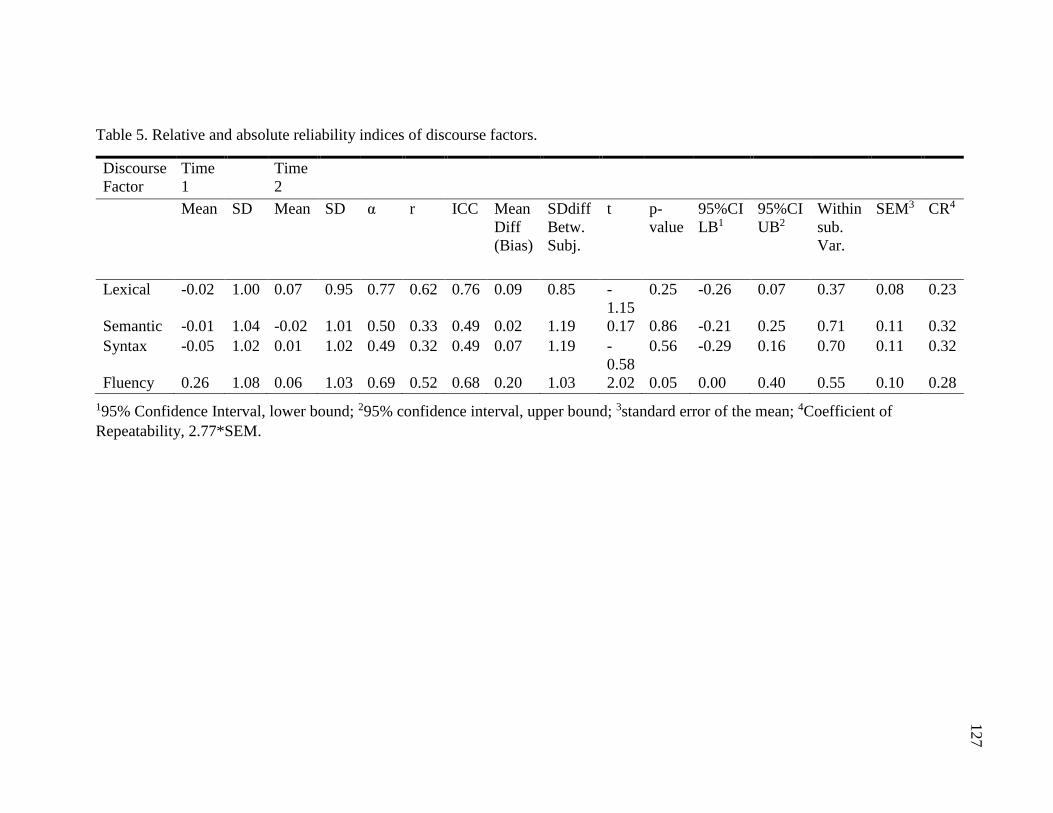
127
Table 5. Relative and absolute reliability indices of discourse factors.
Discourse
Factor
Time
1
Time
2
Mean SD Mean SD α r ICC Mean
Diff
(Bias)
SDdiff
Betw.
Subj.
t p-
value
95%CI
LB1
95%CI
UB2
Within
sub.
Var.
SEM3 CR4
Lexical -0.02 1.00 0.07 0.95 0.77 0.62 0.76 0.09 0.85 -
1.15
0.25 -0.26 0.07 0.37 0.08 0.23
Semantic -0.01 1.04 -0.02 1.01 0.50 0.33 0.49 0.02 1.19 0.17 0.86 -0.21 0.25 0.71 0.11 0.32
Syntax -0.05 1.02 0.01 1.02 0.49 0.32 0.49 0.07 1.19 -
0.58
0.56 -0.29 0.16 0.70 0.11 0.32
Fluency 0.26 1.08 0.06 1.03 0.69 0.52 0.68 0.20 1.03 2.02 0.05 0.00 0.40 0.55 0.10 0.28
195% Confidence Interval, lower bound; 295% confidence interval, upper bound; 3standard error of the mean; 4Coefficient of
Repeatability, 2.77*SEM.
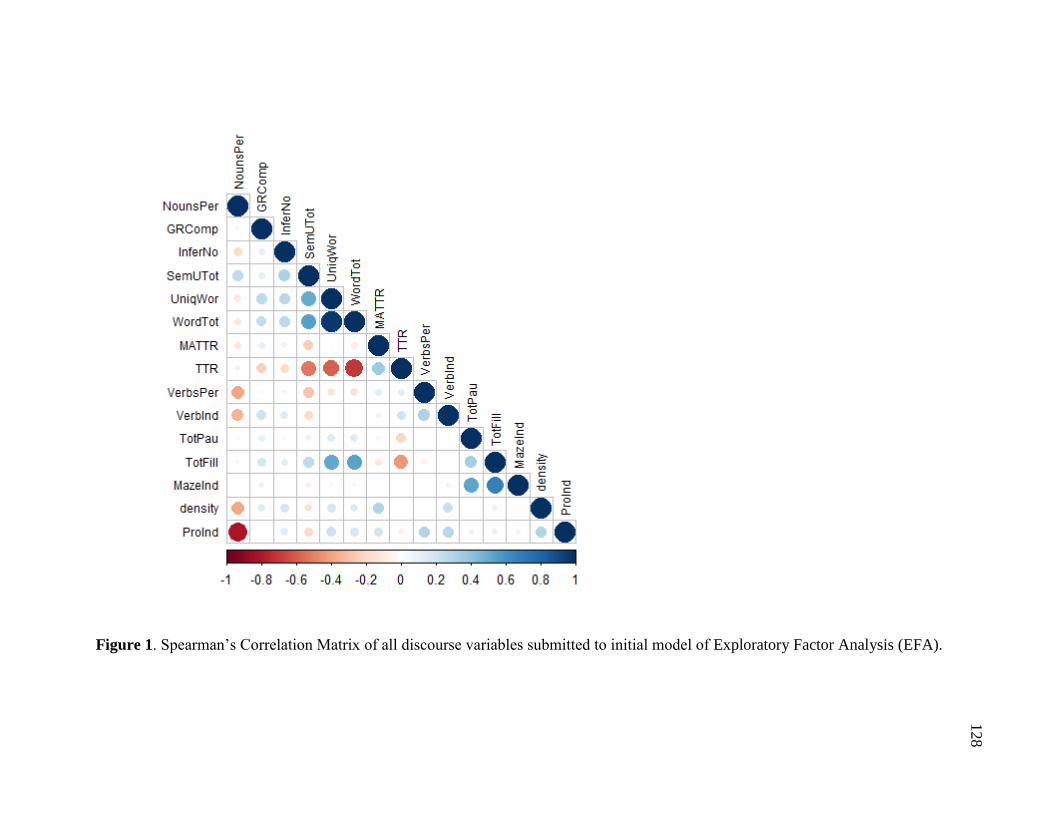
128
Figure 1. Spearman’s Correlation Matrix of all discourse variables submitted to initial model of Exploratory Factor Analysis (EFA).
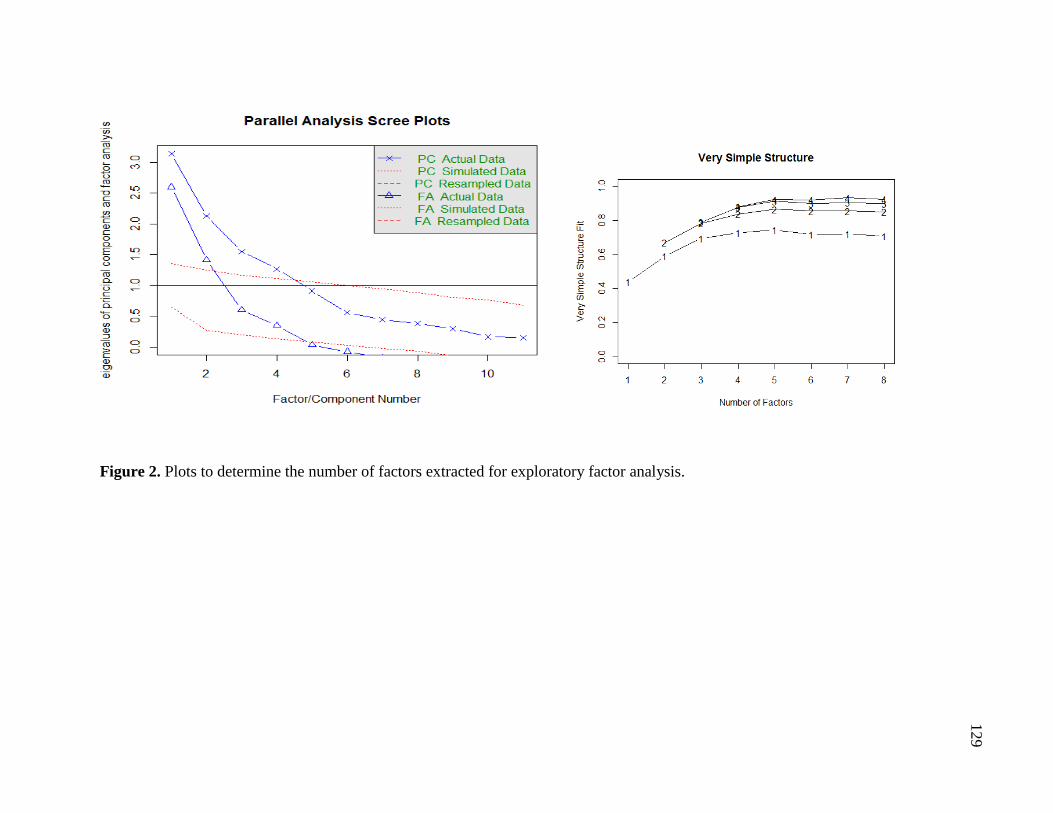
129
Figure 2. Plots to determine the number of factors extracted for exploratory factor analysis.
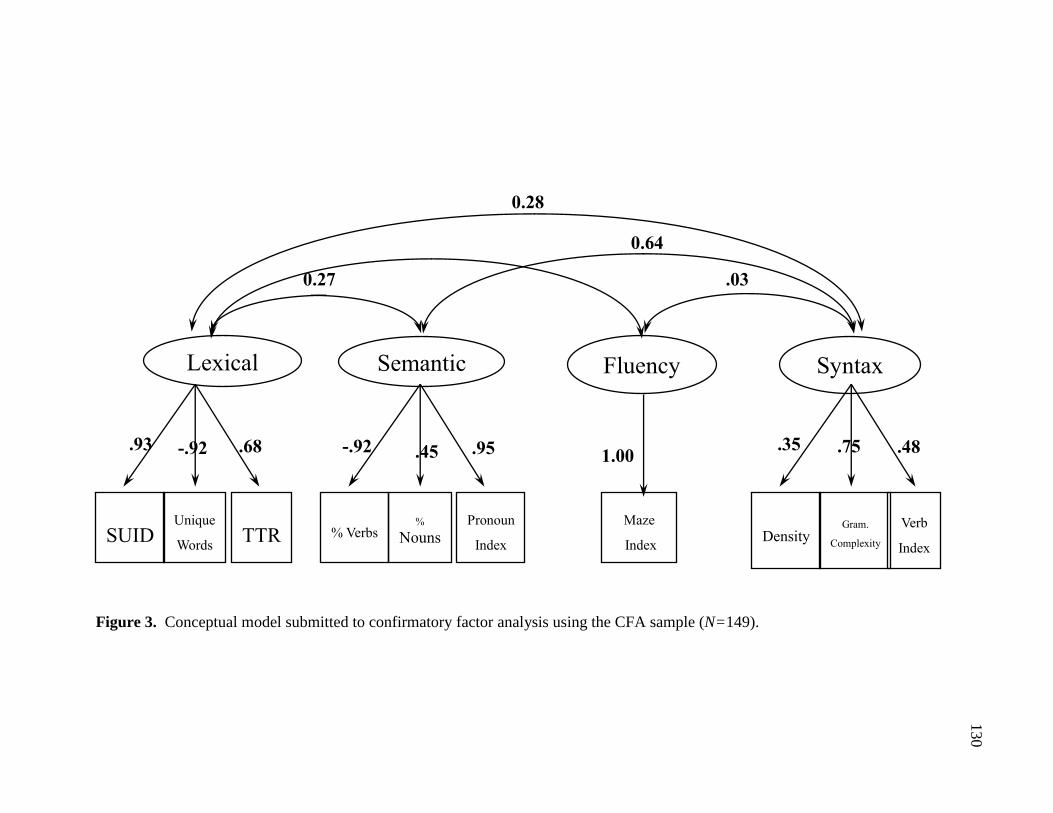
130
Figure 3. Conceptual model submitted to confirmatory factor analysis using the CFA sample (N=149).
% Verbs Pronoun
Index
%
Nouns
Semantic
SUID
TTR Unique
Words
Lexical
Density Verb
Index
Gram.
Complexity
Syntax
Maze
Index
Fluency
0.28
0.27 .03
0.64
.93 -.92 .68 -.92 .45 .95 1.00 .35 .75 .48
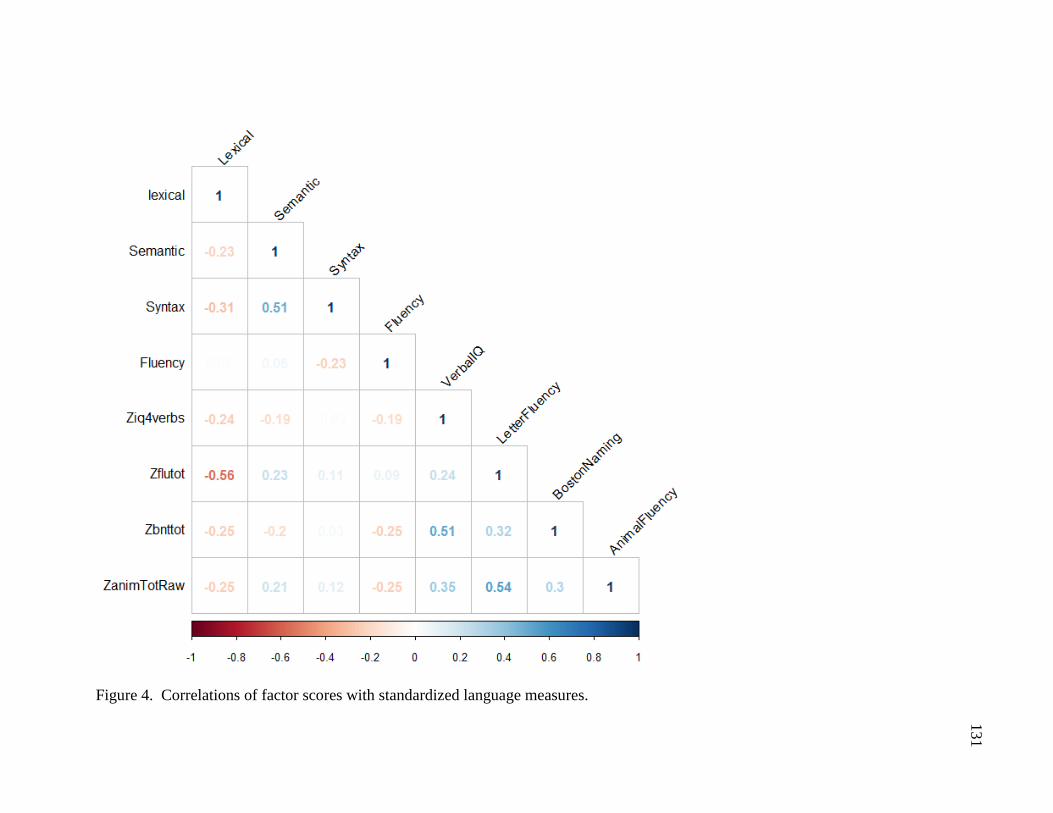
131
Figure 4. Correlations of factor scores with standardized language measures.
132
CHAPTER 5
Manuscript 4: A Longitudinal Study of Connected Language in
Preclinical Mild Cognitive Impairment
133
Connected Language Change in Very Early Mild Cognitive Impairment
KD Mueller, RL Koscik, BP Hermann, SC Johnson, & LS Turkstra
INTRODUCTION
There have been significant advances in detecting neuropathological changes early in the
Alzheimer’s disease (AD) continuum, and these have spurred the development of multiple
clinical trials, investigating both pharmacological and non-pharmacological early interventions.
As a result, there is an urgent need for sensitive tools that measure cognitive and functional
change at very early stages (Snyder et al., 2014). One candidate tool is analysis of connected
language in discourse, which has shown to be an informative measure of language problems
across mid- to later-stages on the AD continuum (Bayles, Tomoeda, & Trosset, 1992; Nicholas
et al., 1985; C. K. Tomoeda & K. A. Bayles, 1993). Connected language analysis may be
sensitive to early changes, and also may yield performance-based measures that are more
representative of actual skills needed for activities of daily living than are typical standardized
language tests. Few studies have examined the earliest point at which connected language
changes are observable (i.e., the Mild Cognitive Impairment (MCI) phase or before), and these
have significant limitations. Additionally, there are few longitudinal studies of preclinical
cohorts that have documented whether or not subtle changes in discourse can be reliably
measured over time. Longitudinal data are important because both discourse features and the
clinical expression of MCI and AD are heterogeneous (Duong et al., 2005), so measurement of
within-person change over time is critical for characterizing change. Thus, there is a need for
both studies of connected language in MCI and also studies that examine performance over time.
134
The few studies of connected language in preclinical AD have shown similar deficiencies
in semantic content as in AD. The earliest prospective evidence of connected language change
came from Cuetos et al. (2007) (F. Cuetos et al., 2007), who compared language samples from a
group of 19 asymptomatic individuals carrying the hereditary mutation of the Presenilin-1 gene,
to similar-aged family members without the mutation. The authors found that the individuals
who carried the mutation expressed less semantic content in the preclinical phase of AD (mean
age = 43) than those who were non-carriers. Retrospective studies of novelist Iris Murdoch’s
writings indicated that impoverished vocabulary and less complex syntax were evident in her
40s, decades before her clinical diagnosis of AD (Le et al., 2011). Similarly, Berisha et al.
(Berisha et al., 2015) retrospectively analyzed unscripted speeches of former president Ronald
Reagan and found increases in filled pauses and decreases in unique words over time, well in
advance of his diagnosis of AD (Berisha et al., 2015). Ahmed et al. (Ahmed et al., 2013b)
retrospectively analyzed picture descriptions of nine autopsy-confirmed patients with AD at
three stages of disease (MCI, Mild AD, Moderate AD), and detected a progressive decline in
efficiency (time required to express ideas) and semantic content.
Although these findings and others (Bschor et al., 2001; Choi, 2009; Drummond et al.,
2015; Fleming & Harris, 2008; Tomoeda et al., 1996) offer encouraging evidence for using
connected language as a measure of change in AD, existing studies have significant limitations.
First, studies either had small sample sizes or were single-case studies, limiting generalizability
to other cohorts. In the few studies with larger sample sizes (Forbes-McKay et al., 2013;
Kathleen C Fraser et al., 2015), patients were in the mild to moderate stages of AD and results
may not generalize to the preclinical phase of disease when compensatory abilities can result in
more subtle impairments in functional language. In the case of retrospective analyses (Ahmed et
135
al., 2013b; Garrard et al., 2005), standardization procedures often were not reported so studies
may be difficult to replicate. In order to determine the feasibility and sensitivity of connected
language analysis, particularly for the purposes of assessment and monitoring within clinical
trials, larger-scale longitudinal studies of preclinical populations are necessary.
The present study investigated connected language over time in a late middle-aged cohort
enriched for risk of AD. The Wisconsin Registry for Alzheimer’s Prevention (WRAP) is an
ongoing longitudinal study that began in 2001, with an objective of identifying cognitive and
biomarker profiles that may be predictors of AD risk. In addition to completing an extensive
neuropsychological test battery at study visits every two years, participants also provide a
connected language sample of a picture description task. The overarching goal of the current
study was to determine whether WRAP participants who were classified with sub-clinical, very
early Mild Cognitive Impairment (“eMCI”) based on standard neuropsychological tests showed
evidence of cognitive decline on connected language measures. Our first aim was to determine
whether being classified as eMCI was associated with longitudinal connected language
trajectories. The second aim investigated whether connected language measures were predictors
of eMCI status at the most recent follow-up. We hypothesized that eMCI would be associated
with greater decline in connected language, and that change in connected language, and/or
baseline connected language performance, would be associated with eMCI diagnosis at the
participant’s most recent visit.
136
METHODS
Participants
WRAP Study Sample. The Wisconsin Registry for Alzheimer’s Prevention (WRAP) is a
longitudinal study of late-middle-aged adults enriched for AD risk based on parental family
history. WRAP participants are asymptomatic, English speaking, and are between the ages of 40
and 65 at the time of enrollment (Sager et al., 2005). Approximately 72% of participants have a
parent with either autopsy-confirmed or probable AD (family history positive (FH+)) as defined
by the National Institute of Neurological and Communicative Disorders and Stroke and the
Alzheimer’s disease and Related Disorders Association (NINCDS-ADRDA) criteria (McKhann
et al., 1984). Approximately 28% of participants had no parental history of AD and met the
criteria that their mothers survived to at least age 75, and their fathers to at least age 70, with no
dementia (family history negative (FH-)).
The WRAP study began in 2001 and currently has enrolled 1551 participants, primarily
from the upper Midwest. The sample is 71% women, 94% white, and has a mean age at baseline
of 54 years. The longitudinal study design includes a baseline visit, followed by a second visit
four years later, and serial follow-up visits every two years thereafter. Participants are tested at
one of three sites: Madison, LaCrosse, and Milwaukee, Wisconsin. WRAP participants undergo
an extensive neuropsychological battery at each visit, and collection of a spontaneous language
sample began at the third wave visit in 2012.
Present study sample. For the present study, we restricted our sample to participants who had
completed language samples and neuropsychological test batteries at two time points (n=280).
Participants also had to have had a consensus diagnosis of either “cognitively healthy” (CH) or
137
“early Mild Cognitive Impairment” (eMCI) at each of the two visits. The following is a brief
description of the two stages of the consensus diagnosis process: 1) each month, new data are
reviewed using an algorithm that applies internally developed robust normative cut-offs (Clark et
al., 2016; Koscik et al., 2014), to 18 neuropsychological test scores, absolute cut-offs to four
neuropsychological test scores, and absolute cut-offs to three informant report measures of
functioning; 2) for all records that meet algorithmic criteria for review, a panel of dementia
experts (neuropsychologists, physicians, clinical nurse practitioners (NPs)) diagnose participants
based on a thorough review of the participant’s cognitive test scores, medical and social history,
and informant reports. Possible diagnoses include: 1) Cognitively normal (referred to in this
paper as “cognitively healthy” (CH)), 2) early MCI (including amnestic subtype and non-
amnestic subtype with impairments in executive functioning or language), 3) clinical MCI, 4)
clinical impairment-not MCI, or 5) dementia. For additional detailed information on the
consensus diagnosis process, see Koscik et al., 2016 (Koscik et al., 2016). Because the aim of
this study was to capture language problems very early on in the possible-AD continuum, we
excluded participants who were diagnosed with clinical MCI or “clinical impairment-not MCI”
(n=9). We also excluded participants who were non-native speakers of English (n=2); those who
had neurological diagnoses including stroke, epilepsy, Parkinson’s disease, and multiple
sclerosis at either visit (n=2); and those whose speech recordings were incomplete (n=1);
resulting in a final sample size of 264 participants.
Discourse Collection Procedure
Participants provided informed consent to have their speech recorded while describing the
“Cookie Theft” picture from the Boston Diagnostic Aphasia Examination (Goodglass & Kaplan,
1983). Participants were instructed to “Tell me everything you see going on in this picture.”
138
Evaluators provided no feedback during participants’ descriptions; however, if responses were
unusually brief (e.g., one or two sentences), evaluators provided the scripted prompt, “Do you
see anything else going on?” Language samples had a mean duration of 50.4 seconds (SD = .02),
including prompts from the examiner. All responses were recorded using an Olympus VN-
6200PC digital audio recorder.
Transcriptions
Language samples were transcribed by a trained speech-language pathologist (KDM), and two
trained graduate students, using Codes for Human Analysis of Transcripts (CHAT)
(MacWhinney, 2000). Transcribers were blinded to the cognitive status of the participant.
Utterances were segmented into C-Units, an established metric for discourse analysis defined as
“an independent clause and all of its modifiers” (Hughes et al., 1997; Hunt, 1965). Transcripts
were coded for automatic analyses by the Computer Language Analysis (CLAN) program
(Macwhinney et al., 2011), including codes for filled and unfilled pauses, repetitions, revisions,
semantic units, errors (semantic, phonological, lexical), and nonverbal behaviors (e.g., coughing,
laughing). Semantic units, parts of speech, total utterances, grammatical relations, and other
quantifiers were then automatically extracted by the CLAN program using the MOR and
MEGRASP programs (MacWhinney, 2000).
Three raters analyzed 15% of samples to calculate inter-rater reliability. Reliability was
calculated using the RELY program within CLAN, and agreement was 92.4% for transcription
and 98% for coding of semantic units.
Discourse Measures
Factor analysis using promax rotation and principal axis factor extraction (Fabrigar et al., 1999)
was used to reduce the set of language measures to a smaller number of factors. We standardized
139
the resulting factors into z scores (i.e., scores that were approximately normally distributed with
mean=0 and sd=1). We multiplied the Fluency factor and Semantic factors by -1 to standardized
directionality across all factor scores, such that negative scores indicated worse performance.
Table 1 shows the factors and the connected language measures that loaded on each factor. For
additional information on factor score development, including details on the exploratory and
confirmatory factor analyses and factor invariance assessments, see Mueller et al. (manuscript in
preparation).
Statistical Analysis
Participant demographics clinical characteristics, and cognitive functioning
Sample characteristics of the cognitively healthy and eMCI groups were compared using t tests
for continuous data and chi-square tests for categorical data. Neuropsychological test
performance was compared with F statistics, adjusting for age, sex and literacy; in the case of
highly skewed data (Mini-Mental State Examination (MMSE), Boston Naming Test (BNT)), we
used Mann-Whitney U tests. We correlated participants’ performance on standardized
neuropsychological tests with language factors using Spearman’s rank correlation coefficients,
due to the skewed distribution of the BNT and MMSE.
Relationship between cognitive status and longitudinal connected language performance
trajectories
Analyses were conducted using R version 3.3.2 and SPSS version 22. We used linear mixed
models to examine longitudinal trends in connected language factor scores and their relation to
cognitive status (CH vs. eMCI ), the predictor of interest. Linear mixed effects modeling allowed
us to examine connected language for participants as a group (fixed effects), while accounting
for variation associated with individual differences (random effect of subject-specific intercept)
140
(Laird & Ware, 1982). Additional covariates were included so that fixed effects could vary by
sex and literacy (scores on the WRAT-III reading subtest (Wilkinson, 1993)). We centered age at
the average of 63 years for ease of interpretation.
Models were fit using the lme4 package within the R environment (Bates, Maechler,
Bolker, & Walker, 2014). First, we examined unconditional means and growth models (i.e.,
subject-level random effects). Growth terms were not significant for any outcome, so random
effects used in subsequent models included only subject-specific intercepts. Subsequent models
also included fixed effects of sex and literacy. We tested interactions between cognitive status
and age, sex, and literacy. Only the cognitive status X age interaction was significant for the
Semantic and Fluency factor models; therefore, we used the base models for the Syntax and
Lexical factors. In each case the final model selected was fit with restricted maximum likelihood
estimation (REML).
Secondary Analyses: Relationship between connected language factor scores and latest cognitive
status
We used a logistic regression analysis to determine if change in factor score (calculated by factor
time two – factor time one, such that negative change indicates declining performance), and/or
factor score at time one, predicted cognitive status at the most recent visit (CN vs. eMCI). We
controlled for age, sex, and literacy. We evaluated models successively by testing the
interactions between change in factor and factor at time one with each of the covariates. Only the
Semantic factor showed a marginally significant interaction between change and age (p = .07).
We then tested this model against the base model comparing the reductions in residual deviances
between models using a likelihood ratio test (Hastie, 1992), and the base model proved to be the
better fit (χ2=3.2, p =.08). Statistical significance of the final models were tested with Wald chi
141
square statistics. We calculated predicted probabilities with odds ratios and confidence intervals,
and we computed sensitivity of predictions using a decision boundary of 0.5.
Other descriptive connected language variables. We extracted connected language variables that
have been shown in the literature to be sensitive to MCI or AD, but did not load on any of our
factors (see Mueller et al., in prep). We performed simple t-tests in order to depict the means at
two time points, and mean change, between the CH and eMCI groups.
RESULTS
Sample Characteristics
Table 2 displays sample characteristics by cognitive status (CH, eMCI). Table 3 presents the raw
scores of neuropsychological tests adjusted for age, sex and literacy (WRAT-III reading). Both
tables reflect data collected at the second speech sample visit. Our final sample consisted of data
from 264 participants at two time points a mean of 2.0 years apart (SD = 1.5), typically the 4th
and 5th wave visits. At the visit with the second speech sample, there were 64 participants
classified as eMCI and 200 as CN; 47 of the 64 eMCI participants were also eMCI at the first
speech sample. The eMCI group was comprised of significantly more males (54%) and they
were slightly older (mean age of 66 at follow-up, versus 64 in the CH group). On average, the
groups were similar in terms of years of education, literacy, APOE-ε4 status, family history
status and depression scores. After adjusting for age, sex and literacy, the two groups differed
significantly on tests of memory (RAVLT, Logical Memory-Delayed), executive functions
(Digit symbol coding, Stroop CW), and language (Boston Naming Test, category and letter
verbal fluency).
142
Figure 1 depicts correlations between the four connected language factors and select
standardized neuropsychological test scores. The Fluency factor was correlated with AVLT
delayed recall (.19), AVLT total score (.18), and Animal Naming (.14). The Lexical factor was
negatively correlated with Letter-Number Sequencing (-.22), letter fluency (-.16), BNT (-.10),
Logical Memory delayed recall (-.12), and Animal Naming (-.15). Syntax was positively
correlated with Trails B (.11), and the MMSE (.10). The semantic factor showed a non-
significant, weakly positive correlation with the Boston Naming Test (.08), the RAVLT delayed
recall (.08), and Trails B (.08).
Relationships between cognitive status and longitudinal connected language trajectories
Results from linear mixed effects regression models examining the relationships between
cognitive status and language factor score at each visit are presented in Table 4. Figure 2 depicts
simple slopes of the interaction between age and cognitive status for mixed model-predicted
fluency and semantic values.
Semantic Factor. A significant interaction between time (centered age) and cognitive status
indicated that individuals who were diagnosed with eMCI declined faster than the CH group on
the semantic language factor over time (β= -.04 p=.03).
Syntax Factor. Interactions between age and cognitive status, or cognitive status and the other
covariates were not significant; therefore Model 1 was used. Cognitive status was not a
significant predictor of syntax performance at either visit.
Lexical Factor. No interactions were significant so we retained Model 1. A significant main
effect for time for the lexical factor indicated that all individuals tended to decrease in lexical
143
diversity from time one to time two, but cognitive status was not a significant predictor of this
decline.
Fluency Factor. A significant interaction between time and cognitive status indicated that
participants who were diagnosed with eMCI declined faster on fluency factor scores over time (β
= -.03, p=.03). Cognitive status had a significant main effect on the fluency factor, indicating
that eMCI status at either both visits or the most recent visit was a significant predictor of poorer
speech fluency scores (β=-.23, p=.03).
Relationship between connected language factor scores and latest cognitive status
Results of logistic regression models for the four connected language factors are presented in
Table 5.
Change in fluency (Wald χ2=11.2, p=.004) and change in semantic scores (Wald χ2=10.1,
p=.007) were significantly associated with a greater likelihood of pMCI classification at the time
2, while lower syntax at time one was associated with eMCI status at time two (Wald χ2=9.8,
p=.02). The fluency model correctly classified 78% of eMCI cases, vs. 79% for the semantic
model and 77% for the syntax model. The lexical factor was not significantly associated with
eMCI status at time two.
Other descriptive connected language variables
Mean scores and results of t-tests for descriptive connected language variables (that were not part
of the factor scores) are presented in Table 6. There were significant differences between the
eMCI group and the CH group for mean length of utterance (MLU) at both time points (p <.001),
words per minute at Time 2 (p =.02), and semantic units per minute at Time 2 (p = .03). Change
from Time 1 to Time 2 was not significant between groups for any of the variables.
144
DISCUSSION
Although a decline in episodic memory is the typical defining feature of Alzheimer’s
disease dementia, changes in language are also evident early in the disease course. Analyses of
connected language in the mild to moderate stages of AD has proved to be a sensitive measure of
subtle changes in performance, but we did not know if connected language analysis would be
similarly sensitive in the preclinical stage of AD. Thus, we set out to investigate whether
connected language performance was associated with a diagnosis of sub-clinical MCI in a risk-
enriched cohort of healthy, late-middle-aged individuals.
Our findings suggest that, in this younger and relatively healthy cohort, subclinical
declines in memory and/or executive function were associated with changes in connected
language. Specifically, as individuals progressed through the study, those who showed eMCI
status declined more rapidly in both semantic and fluency features of connected language. We
also found that aspects of connected language were predictive of cognitive status at the most
recent follow-up: specifically, lower syntactic complexity at baseline and declines in both
semantic content and fluency were associated with a greater likelihood of eMCI classification at
the most recent visit. Lexical diversity was not associated with eMCI status, and in fact showed
small, negative correlations with several standardized neuropsychological tests.
The literature supports our finding that eMCI participants declined more rapidly than CH
participants on semantic measures. Our semantic factor (Mueller, et al. in prep.) is weighted such
that it represents a higher proportion of pronouns, a lower percentage of nouns, and an increase
in use of verbs. Studies using composite scores or factor scores similar to our semantic factor
(Mueller et al., in preparation) have found comparable results later on the AD continuum. For
example, Fraser et al. (2015) trained a machine learning classifier on 370 linguistic features of
145
Cookie Theft picture descriptions from 167 adults with AD and 97 controls. They subsequently
performed a factor analysis of successfully classifying features, which resulted in a semantic
factor that included of a high proportion of pronouns, low proportion of nouns, and high verb
frequency (i.e., less semantic content overall). This semantic factor differentiated speech samples
of adults with AD from those of controls (Kathleen C Fraser et al., 2015). Ahmed et al. (2013)
used a composite score comprised of measures of pronoun ratios and verb ratios, which they
termed “lexical content”, to examine 9 adults across three stages of autopsy-confirmed
Alzheimer’s disease: MCI, mild AD, and moderate AD. Composite scores differentiated between
MCI and mild AD stages, but trends in the difference between controls and patients with MCI
did not reach statistical significance (Ahmed et al., 2013b). Our study sample may represent a
stage that is even earlier on the AD continuum than MCI, and the finding of significant
differences in our group is likely because of our large sample size.
The higher loading of verbs relative to nouns in our semantic factor is a phenomenon that
has been explored previously in language of adults with AD. The verb-noun differential has been
of interest because putative neuroanatomical substrates of verb vs. noun storage are differentially
affected by AD pathology. Studies of patients with regional atrophy and aphasia report that
nouns are predominantly supported by posterior brain regions, while verbs are supported by
anterior brain regions (Damasio & Tranel, 1993; Daniele, Giustolisi, Silveri, Colosimo, &
Gainotti, 1994). The neurodegenerative pattern of AD typically begins in the medial temporal
cortex with gradual spread to the frontal lobes at the later stages of disease (Braak & Braak,
1991; Whitwell et al., 2007). Taken together, these findings suggest preservation of verbs in the
course of AD. Evidence for such verb preservation is mixed, however; some studies have shown
a verb advantage in AD (Bowles, Obler, & Albert, 1987; Robinson, Rossor, & Cipolotti, 1999),
146
while others have not (Ahmed et al., 2013a; Kim & Thompson, 2004; Masterson et al., 2007).
Interpretation of results from our study is problematic, however, because the Cookie Theft task
lends itself to more action-oriented verbs versus mental-state verbs, so data from this task may
not be representative of more typical conversational discourse (Stronach & Turkstra, 2008).
With respect to high pronoun index, Almor et al. (1999) showed that adults with AD
(n=11) used more pronouns in relation to noun phrases than controls (n=9) (Almor et al., 1999).
While several other studies of adults with AD report a similar over-use of pronouns (Ripich &
Terrell, 1988; Ulatowska et al., 1988), such findings in studies of MCI are limited. Our study
adds evidence to the notion that connected language may become semantically impoverished
early on the preclinical AD continuum.
Correlations between the semantic factor and standardized measures of semantic content
(BNT and animal naming) were not statistically significant. This finding is partially supported
by the AD literature, but results of that literature are mixed. Almor et al. (1999) found no
correlation between increased pronoun use and picture naming scores, and theorized that
pronoun measures in discourse may be more a reflection of working memory problems than of
semantic memory. Nicholas et al. (1985) similarly found no correlation between discourse
measures of “empty speech” (e.g., pronouns without referents) and scores on picture naming
tasks. By contrast, Kave et al. (2016) found that picture naming and semantic measures of
Cookie Theft descriptions were correlated in a group of adults with AD (n=20; r=.46-.67),
although not in a control group. In addition, the authors showed that semantic verbal fluency
scores were not correlated with semantic measures of connected language in either the group
with AD or the controls. In our study, the eMCI group differed significantly from the CH group
on verbal fluency and picture naming tasks; the lack of correlation of these measures with
147
discourse measures lends support to the idea that measures of connected language describe not
only semantic knowledge and expression, but also the coordination of multiple cognitive
processes (Almor et al., 1999).
Discourse fluency declined more rapidly in persons with eMCI, and that fluency change
was a predictor of eMCI status. A few studies of MCI have shown similar results; for example,
Berisha et al. (2015) found that former President Ronald Reagan’s unscripted speeches contained
more filled pauses over time ( e.g., “um,” “well”) during a period of 6 to 13 years prior to his
diagnosis of AD. By contrast, discourse fluency was not a distinguishing factor in MCI, mild or
moderate AD in the 9 adults studied by Ahmed (Ahmed et al., 2013b), although this sample was
very small. Other studies of connected language in AD have shown increased repetitions and
revisions (Nicholas et al., 1985; C. K. Tomoeda & K. A. Bayles, 1993), increased pauses or
hesitations (Davis & Maclagan, 2009; Gayraud, Lee, & Barkat-Defradas, 2011; Hoffmann et al.,
2010; Sajjadi et al., 2012), and an increase in repaired errors (McNamara et al., 1992). It is
possible that these mixed results with fluency measures is due to examining only select disfluent
behaviors. Our fluency factor consisted of an index that included filled and unfilled pauses,
repetitions, revisions, and false starts divided by the number of utterances. To our knowledge, no
studies of discourse in MCI or AD have examined a comprehensive fluency measure such as
this, and it is possible that a ratio of fluency behaviors is more sensitive than the individual
measures alone. Further, while semantic deficits are common in connected language of people
with AD, it is possible that at very early stages a surge in dysfluent behavior may reflect the
beginnings of difficulty with word search and retrieval, foreshadowing more problems
expressing semantic content. There is evidence that error monitoring does not decline until later
in the disease (Forbes et al., 2001; McNamara et al., 1992); so perhaps adults with eMCI in our
148
study noticed and repaired more errors (hence had a higher number of “revisions”), resulting in
higher dysfluency scores.
Correlations between the fluency factor and standardized neuropsychological test scores
revealed positive correlations with semantic fluency, AVLT total score, and AVLT delayed
recall. These data suggest that dysfluent behavior in the eMCI group may be related to aspects of
memory (semantic storage of words) (Henry et al., 2004), executive functions (search and
retrieval of words) (Alvarez & Emory, 2006) , and working memory (Almor et al., 1999;
Hartsuiker & Kolk, 2001) .
While syntax is commonly described as “intact” until more severe stages of AD, declines
and differences in syntax complexity have been observed at mild and moderate stages (Croisile et
al., 1996; Kemper et al., 2001). In our sample, lower syntactic complexity at baseline predicted
eMCI status at the latest visit, highlighting the importance of examining syntax beyond basic
structures. Our syntax measure is comprised of a verb index (ratio of verbs to utterances), a
grammatical complexity measure based on embedded clauses (Macwhinney et al., 2011), and a
measure of propositional density. Our participants’ low baseline performance on complexity
measures is similar to findings from the seminal Nun Study regarding early life linguistic
abilities (Snowdon et al., 1996). Authors of that study found that lower idea density at an average
age of 22 significantly increased the risk of AD 58 years later. Kemper et al. (2000) examined
Nun Study data over time and found that those who met criteria for dementia later in life had
lower baseline measures of idea density and grammatical complexity. These results have been
explained by both the cognitive reserve hypothesis and the early neuropathology hypothesis.
According to the cognitive reserve hypothesis, nuns with high linguistic abilities either had AD-
type neuropathology but were able to compensate for changes because of their high linguistic
149
capacity. In both models we tested (logistic and linear mixed models), literacy was significantly
associated with syntax, which lends some support to the cognitive reserve hypothesis.
Conversely, Snowdon et al. (1996) proposed that low linguistic ability early in life might have
signaled that development of neuropathology had already begun, decades before dementia was
expressed. Thus, group differences at baseline were due to neuropathological changes in nuns
who went on to develop dementia. Comparing baseline syntax measures to longitudinal, multi-
modal measures of amyloid deposition and tau protein formation via cerebral spinal fluid and
imaging may help to clarify these associations in WRAP participants in the future.
Our lexical factor was not associated with eMCI status, which was surprising given
evidence of decreases in lexical diversity and efficiency in adults with AD and MCI (Ahmed et
al., 2013b; Kathleen C Fraser et al., 2015). The lexical factor was comprised of measures of
lexical diversity (type-token ratio) and semantic unit idea density. That the lexical factor was
negatively correlated with phonemic fluency was also unexpected. We examined several
transcripts of those with low measures on the lexical factor and found that these picture
descriptions contained an overabundance of words with fewer expression of semantic units (i.e.,
verbosity), as we expected, which would suggest a link between lexical aspects of discourse and
eMCI status. It is possible that our lack of significant findings was related to the variable length
of transcripts, as type-token ratio is influenced by sample size. One small study of 8 people with
MCI and 14 controls found that the MCI group showed significantly higher “potential
vocabulary size” (an adapted type-token ratio) than the controls (Aramaki, Shikata, Miyabe, &
Kinoshita, 2016). The authors argued that the adults with MCI may have been compensating for
cognitive decline by talking more without necessarily conveying more content. An adapted type-
150
token ratio might be more revealing in future studies, as would use of a task that elicited longer
language samples.
We examined other metrics of the language samples that were not included in the factor
structure, but were important to include as descriptors, such as total words and words per minute.
We also examined mean length of utterance (MLU), as some studies have shown shorter
utterance length for individuals with MCI and AD (Ahmed et al., 2013b; Ripich et al., 2000). We
found that the eMCI group had significantly shorter utterances (MLU) at both time points than
the CH group. The groups did not differ on total number of words or total number of semantic
units. The fact that semantic units were similar for both groups at both time points is surprising,
since previous studies of preclinical AD have shown this measure to differentiate between
groups (Ahmed et al., 2013a; F. Cuetos et al., 2007; Kimberly Diggle Mueller et al., 2016). Both
groups showed an increase in total words from Time 1 to Time 2, so it is possible that talking
more also allowed for more elements of the picture to be described. That the eMCI group
expressed fewer words per minute and semantic units per minute indicates that the efficiency of
descriptions was compromised, and the time it takes to convey content is a more sensitive
measure at this stage.
Our study had strengths and limitations. A strength was the sample size, which far
exceeded that of any other prospective longitudinal study of connected language in older adults
at risk for Alzheimer’s disease. In addition, by using a confirmed structure of latent factors, we
were able to summarize measures in broad categories of language performance and better
characterize our results. The standardized and focused nature of the picture description task was
another strength, as it minimized demands on episodic memory, but still yielded spontaneous
language. The Computerized Language Analysis program (CLAN) also was a benefit, as it
151
provided a quick, efficient, objective, and standardized means of extracting data; this combined
with our relatively simple factor structure and the ubiquity of the Cookie Theft picture in the AD
literature will support replication of our analysis in future studies.
One of the limitations of our study was the relatively short length of the language
samples (average total words = 109). While there is no established minimum length for language
samples in adults with MCI, for adults with nonfluent aphasia Brookshire and Nicholas
recommended an average of 300-400 words (Brookshire & Nicholas, 1994a), and others
recommended a minimum of 150 words (Saffran, Berndt, & Schwartz, 1989; Sajjadi et al.,
2012). Longer samples might be needed for individuals with nonfluent aphasia, however, given
their reduced language output. Fraser et al. (2016) also had a mean sample length of 100 words
from patients with AD, and reported findings with some parallels to ours, so 100 words may be
sufficient. The short task may also be considered a strength, as it presents a relatively low burden
for participants compared to demands of typical standardized tests. If subtle changes can be
detected in shorter samples, this will save time for both the participant and the clinician. Future
longitudinal research in order to develop sample size recommendations in this group would be
beneficial.
Although our approach proved to be feasible in this large cohort, the transcription and
coding of these language samples was relatively labor-intensive. The field of computational
linguistics has made advances in machine learning techniques for analyzing linguistic features,
but these methods also require transcriptions of spoken language. Researchers are beginning to
improve upon Automatic Speech Recognition (ASR) to solve this problem, which will allow for
more efficient analyses that can be translated to clinical practice for disease monitoring.

152
Finally, while the very early, sub-clinical construct of eMCI can be considered a strength
since no other studies have examined connected language in an at-risk cohort, the participants
diagnosed with eMCI may be experiencing some other type of cognitive decline besides MCI or
AD. Future research will address this limitation in part by combining connected language data
with other biomarker measures that may confirm the presence of neuropathologic changes
typical of AD. We also plan to continue to follow these participants and collect future language
samples and biomarkers in order to determine the course of connected language change as the
WRAP cohort ages.
CONCLUSIONS
In a review of assessment in AD and dementia, Laske et al. (Laske et al., 2015) listed
connected language analysis as one of the most promising state-of-the-art diagnostic measures
for MCI and AD. The authors described spoken language as a multi-dimensional, non-invasive,
and informative biological sample for the early detection of AD, primary progressive aphasia,
and other dementia syndromes. Our results provide evidence that features of connected language
are associated with very early, sub-clinical declines in memory in late-middle age. This research
contributes toward a better understanding of early language changes in AD, which can not only
improve disease monitoring in clinical trials, but also inform cognitive-communication
interventions and caregiver education programs that maintain and enhance quality of life and life
participation for adults with MCI and AD.
153
REFERENCES
1. Snyder, P.J., et al., Assessing cognition and function in Alzheimer's disease clinical trials:
Do we have the right tools? Alzheimer's & Dementia, 2014. 10(6): p. 853-860.
2. Bayles, K.A., C.K. Tomoeda, and M.W. Trosset, Relation of linguistic communication
abilities of Alzheimer's patients to stage of disease. Brain and language, 1992. 42(4): p.
454-472.
3. Tomoeda, C.K. and K.A. Bayles, Longitudinal effects of Alzheimer disease on discourse
production. Alzheimer Dis Assoc Disord, 1993. 7(4): p. 223-36.
4. Nicholas, M., et al., Empty speech in Alzheimer's disease and fluent aphasia. J Speech
Hear Res, 1985. 28(3): p. 405-10.
5. Duong, A., et al., The heterogeneity of picture-supported narratives in Alzheimer's
disease. Brain Lang, 2005. 93(2): p. 173-84.
6. Cuetos, F., et al., Linguistic changes in verbal expression: a preclinical marker of
Alzheimer's disease. J Int Neuropsychol Soc, 2007. 13(3): p. 433-9.
7. Le, X., et al., Longitudinal detection of dementia through lexical and syntactic changes in
writing: a case study of three British novelists. Literary and Linguistic Computing, 2011:
p. fqr013.
8. Berisha, V., et al., Tracking discourse complexity preceding Alzheimer's disease
diagnosis: a case study comparing the press conferences of Presidents Ronald Reagan
and George Herbert Walker Bush. J Alzheimers Dis, 2015. 45(3): p. 959-63.
9. Ahmed, S., et al., Connected speech as a marker of disease progression in autopsy-
proven Alzheimer's disease. Brain, 2013. 136(Pt 12): p. 3727-37.
10. Tomoeda, C.K., et al., Cross-sectional analysis of Alzheimer disease effects on oral
discourse in a picture description task. Alzheimer Dis Assoc Disord, 1996. 10(4): p. 204-
15.
11. Drummond, C., et al., Deficits in narrative discourse elicited by visual stimuli are
already present in patients with mild cognitive impairment. Front Aging Neurosci, 2015.
7: p. 96.
12. Fleming, V.B. and J.L. Harris, Complex discourse production in mild cognitive
impairment: Detecting subtle changes. Aphasiology, 2008. 22(7-8): p. 729-740.
13. Bschor, T., K.P. Kuhl, and F.M. Reischies, Spontaneous speech of patients with dementia
of the Alzheimer type and mild cognitive impairment. Int Psychogeriatr, 2001. 13(3): p.
289-98.
14. Choi, H., Performances in a picture description task in Japanese patients with
Alzheimer’s disease and with mild cognitive impairment. Korean Journal of
Communication Disorders, 2009. 14(14): p. 326-337.
154
15. Fraser, K.C., J.A. Meltzer, and F. Rudzicz, Linguistic Features Identify Alzheimer’s
Disease in Narrative Speech. Journal of Alzheimer's Disease, 2015. 49(2): p. 407-422.
16. Forbes-McKay, K., M.F. Shanks, and A. Venneri, Profiling spontaneous speech decline
in Alzheimer's disease: a longitudinal study. Acta neuropsychiatrica, 2013. 25(06): p.
320-327.
17. Garrard, P., et al., The effects of very early Alzheimer's disease on the characteristics of
writing by a renowned author. Brain, 2005. 128(Pt 2): p. 250-60.
18. Sager, M.A., B. Hermann, and A. La Rue, Middle-aged children of persons with
Alzheimer's disease: APOE genotypes and cognitive function in the Wisconsin Registry
for Alzheimer's Prevention. J Geriatr Psychiatry Neurol, 2005. 18(4): p. 245-9.
19. McKhann, G., et al., Clinical diagnosis of Alzheimer's disease Report of the NINCDS‐ADRDA Work Group* under the auspices of Department of Health and Human Services
Task Force on Alzheimer's Disease. Neurology, 1984. 34(7): p. 939-939.
20. Koscik, R.L., et al., Emergence of mild cognitive impairment in late middle-aged adults
in the wisconsin registry for Alzheimer's prevention. Dement Geriatr Cogn Disord, 2014.
38(1-2): p. 16-30.
21. Clark, L.R., et al., Mild Cognitive Impairment in Late Middle Age in the Wisconsin
Registry for Alzheimer's Prevention Study: Prevalence and Characteristics Using Robust
and Standard Neuropsychological Normative Data. Arch Clin Neuropsychol, 2016.
22. Koscik, R.L., et al., Intraindividual Cognitive Variability in Middle Age Predicts
Cognitive Impairment 8–10 Years Later: Results from the Wisconsin Registry for
Alzheimer’s Prevention. Journal of the International Neuropsychological Society, 2016.
22(10): p. 1016-1025.
23. Goodglass, H. and E. Kaplan, Boston diagnostic aphasia examination booklet. 1983: Lea
& Febiger.
24. MacWhinney, B., The CHILDES project: Tools for analyzing talk. 3rd Lawrence
Erlbaum Associates. Mahwah, NJ, 2000.
25. Hunt, K.W., Grammatical Structures Written at Three Grade Levels. NCTE Research
Report No. 3. 1965.
26. Hughes, D.L., L. McGillivray, and M. Schmidek, Guide to narrative language:
Procedures for assessment. 1997: Thinking Publications Eau Claire, WI.
27. Macwhinney, B., et al., AphasiaBank: Methods for Studying Discourse. Aphasiology,
2011. 25(11): p. 1286-1307.
28. Fabrigar, L.R., et al., Evaluating the use of exploratory factor analysis in psychological
research. Psychological methods, 1999. 4(3): p. 272.
29. Laird, N.M. and J.H. Ware, Random-Effects Models for Longitudinal Data. Biometrics,
1982. 38(4): p. 963-974.
30. Wilkinson, G.S., WRAT-3: Wide range achievement test. 1993: Wide Range.
155
31. Bates, D., et al., lme4: Linear mixed-effects models using Eigen and S4. R package
version, 2014. 1(7).
32. Hastie, T., Generalized additive models in Chambers, JM and TJ Hastie (eds), Statistical
models in S. Wadsworth and Brooks, Pacific Grove, 1992.
33. Daniele, A., et al., Evidence for a possible neuroanatomical basis for lexical processing
of nouns and verbs. Neuropsychologia, 1994. 32(11): p. 1325-1341.
34. Damasio, A.R. and D. Tranel, Nouns and verbs are retrieved with differently distributed
neural systems. Proceedings of the National Academy of Sciences, 1993. 90(11): p. 4957-
4960.
35. Braak, H. and E. Braak, Neuropathological stageing of Alzheimer-related changes. Acta
neuropathologica, 1991. 82(4): p. 239-259.
36. Whitwell, J.L., et al., 3D maps from multiple MRI illustrate changing atrophy patterns as
subjects progress from mild cognitive impairment to Alzheimer's disease. Brain, 2007.
130(7): p. 1777-1786.
37. Bowles, N.L., L.K. Obler, and M.L. Albert, Naming errors in healthy aging and
dementia of the Alzheimer type. Cortex, 1987. 23(3): p. 519-524.
38. Robinson, G., M. Rossor, and L. Cipolotti, Selective sparing of verb naming in a case of
severe Alzheimer's disease. Cortex, 1999. 35(3): p. 443-450.
39. Masterson, J., et al., Selective Naming (and Comprehension) Deficits in Alzheimer's
Disease? Cortex, 2007. 43(7): p. 921-934.
40. Kim, M. and C.K. Thompson, Verb deficits in Alzheimer’s disease and agrammatism:
Implications for lexical organization. Brain and language, 2004. 88(1): p. 1-20.
41. Ahmed, S., et al., Semantic processing in connected speech at a uniformly early stage of
autopsy-confirmed Alzheimer's disease. Neuropsychology, 2013. 27(1): p. 79-85.
42. Stronach, S.T. and L.S. Turkstra, Theory of mind and use of cognitive state terms by
adolescents with traumatic brain injury. Aphasiology, 2008. 22(10): p. 1054-1070.
43. Almor, A., et al., Why do Alzheimer patients have difficulty with pronouns? Working
memory, semantics, and reference in comprehension and production in Alzheimer's
disease. Brain Lang, 1999. 67(3): p. 202-27.
44. Ripich, D.N. and B.Y. Terrell, Patterns of discourse cohesion and coherence in
Alzheimer's disease. J Speech Hear Disord, 1988. 53(1): p. 8-15.
45. Ulatowska, H.K., et al., [Use of discourse analysis for evaluation of the condition of
patients with dementia of the Alzheimer type]. Neurol Neurochir Pol, 1988. 22(1): p. 34-
7.
46. Sajjadi, S.A., et al., Abnormalities of connected speech in semantic dementia vs
Alzheimer's disease. Aphasiology, 2012. 26(6): p. 847-866.
156
47. Davis, B.H. and M. Maclagan, Examining pauses in Alzheimer's discourse. Am J
Alzheimers Dis Other Demen, 2009. 24(2): p. 141-54.
48. Hoffmann, I., et al., Temporal parameters of spontaneous speech in Alzheimer's disease.
International journal of speech-language pathology, 2010. 12(1): p. 29-34.
49. Gayraud, F., H.R. Lee, and M. Barkat-Defradas, Syntactic and lexical context of pauses
and hesitations in the discourse of Alzheimer patients and healthy elderly subjects. Clin
Linguist Phon, 2011. 25(3): p. 198-209.
50. McNamara, P., et al., Speech monitoring skills in Alzheimer's disease, Parkinson's
disease, and normal aging. Brain and language, 1992. 42(1): p. 38-51.
51. Forbes, K.E., A. Venneri, and M.F. Shanks, Distinct patterns of spontaneous speech
deterioration: an early predictor of Alzheimer's disease. Brain and cognition, 2001. 48(2-
3): p. 356-361.
52. Henry, J.D., J.R. Crawford, and L.H. Phillips, Verbal fluency performance in dementia of
the Alzheimer’s type: a meta-analysis. Neuropsychologia, 2004. 42(9): p. 1212-1222.
53. Alvarez, J.A. and E. Emory, Executive function and the frontal lobes: a meta-analytic
review. Neuropsychology review, 2006. 16(1): p. 17-42.
54. Hartsuiker, R.J. and H.H. Kolk, Error monitoring in speech production: A computational
test of the perceptual loop theory. Cognitive psychology, 2001. 42(2): p. 113-157.
55. Kemper, S., M. Thompson, and J. Marquis, Longitudinal change in language production:
effects of aging and dementia on grammatical complexity and propositional content.
Psychology and aging, 2001. 16(4): p. 600.
56. Croisile, B., et al., Comparative study of oral and written picture description in patients
with Alzheimer's disease. Brain Lang, 1996. 53(1): p. 1-19.
57. Snowdon, D.A., et al., Linguistic ability in early life and cognitive function and
Alzheimer's disease in late life. Findings from the Nun Study. JAMA, 1996. 275(7): p.
528-32.
58. Aramaki, E., et al., Vocabulary size in speech may be an early indicator of cognitive
impairment. PloS one, 2016. 11(5): p. e0155195.
59. Ripich, D.N., et al., Compensatory strategies in picture description across severity levels
in Alzheimer's disease: A longitudinal study. American Journal of Alzheimer's Disease
and Other Dementias, 2000. 15(4): p. 217-228.
60. Mueller, K.D., et al., Connected Language in Late Middle-Aged Adults at Risk for
Alzheimer’s Disease. Journal of Alzheimer's Disease, 2016(Preprint): p. 1-12.
61. Brookshire, R.H. and L.E. Nicholas, Speech sample size and test-retest stability of
connected speech measures for adults with aphasia. Journal of Speech, Language, and
Hearing Research, 1994. 37(2): p. 399-407.
62. Saffran, E.M., R.S. Berndt, and M.F. Schwartz, The quantitative analysis of agrammatic
production: Procedure and data. Brain and language, 1989. 37(3): p. 440-479.
157
63. Laske, C., et al., Innovative diagnostic tools for early detection of Alzheimer's disease.
Alzheimer's & Dementia, 2015. 11(5): p. 561-578.
64. Covington, M.A. and J.D. McFall, Cutting the Gordian knot: The moving-average type–
token ratio (MATTR). Journal of Quantitative Linguistics, 2010. 17(2): p. 94-100.
65. Brown, C., et al., Automatic Measurement of Propositional Idea Density from Part-of-
Speech Tagging. Behavior research methods, 2008. 40(2): p. 540-545.
66. Ahmed, S., et al., Logopenic aphasia in Alzheimer's disease: clinical variant or clinical
feature? Journal of Neurology, Neurosurgery & Psychiatry, 2012: p. jnnp-2012-302798.
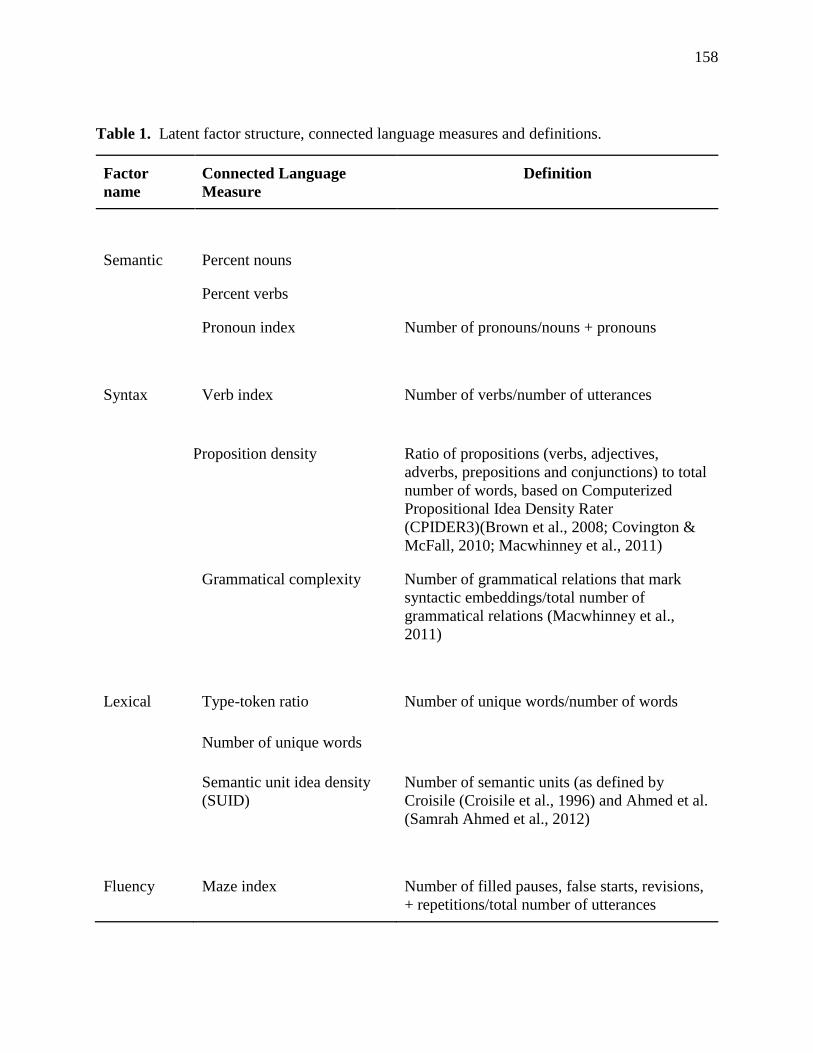
158
Table 1. Latent factor structure, connected language measures and definitions.
Factor
name
Connected Language
Measure
Definition
Semantic Percent nouns
Percent verbs
Pronoun index Number of pronouns/nouns + pronouns
Syntax Verb index Number of verbs/number of utterances
Proposition density Ratio of propositions (verbs, adjectives,
adverbs, prepositions and conjunctions) to total
number of words, based on Computerized
Propositional Idea Density Rater
(CPIDER3)(Brown et al., 2008; Covington &
McFall, 2010; Macwhinney et al., 2011)
Grammatical complexity Number of grammatical relations that mark
syntactic embeddings/total number of
grammatical relations (Macwhinney et al.,
2011)
Lexical Type-token ratio Number of unique words/number of words
Number of unique words
Semantic unit idea density
(SUID)
Number of semantic units (as defined by
Croisile (Croisile et al., 1996) and Ahmed et al.
(Samrah Ahmed et al., 2012)
Fluency Maze index Number of filled pauses, false starts, revisions,
+ repetitions/total number of utterances
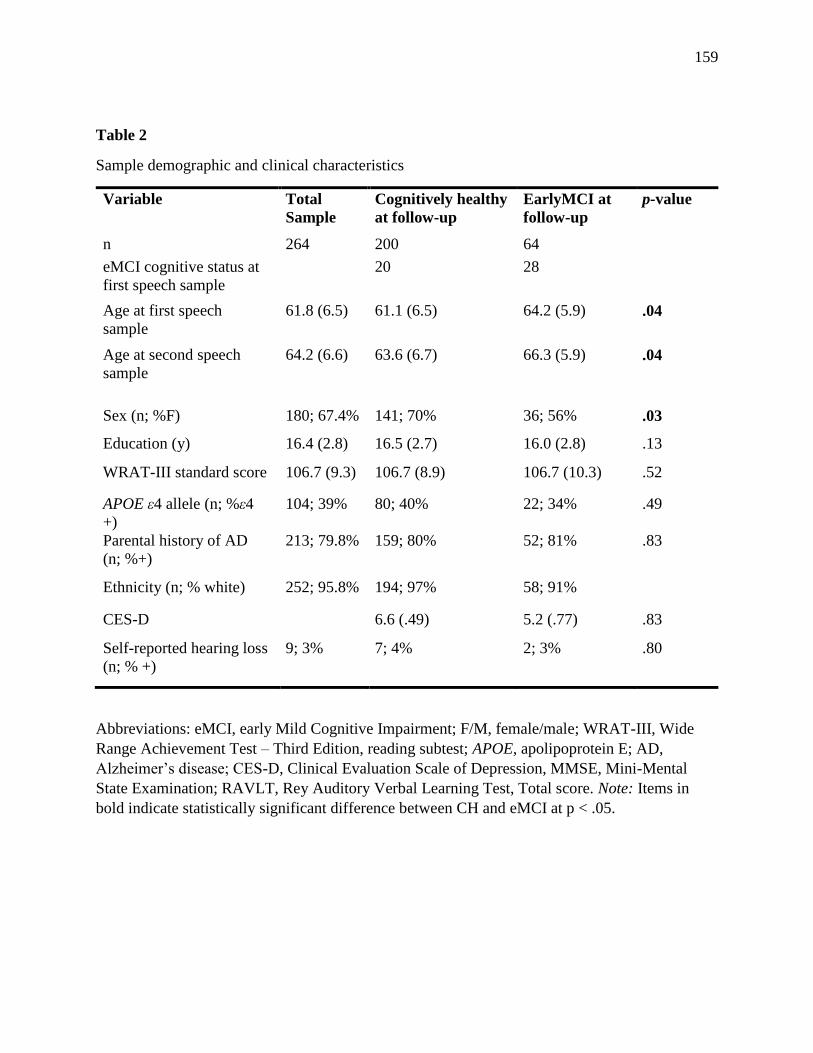
159
Table 2
Sample demographic and clinical characteristics
Variable Total
Sample
Cognitively healthy
at follow-up
EarlyMCI at
follow-up
p-value
n 264 200 64
eMCI cognitive status at
first speech sample
20 28
Age at first speech
sample
61.8 (6.5) 61.1 (6.5) 64.2 (5.9) .04
Age at second speech
sample
64.2 (6.6) 63.6 (6.7) 66.3 (5.9) .04
Sex (n; %F) 180; 67.4% 141; 70% 36; 56% .03
Education (y) 16.4 (2.8) 16.5 (2.7) 16.0 (2.8) .13
WRAT-III standard score 106.7 (9.3) 106.7 (8.9) 106.7 (10.3) .52
APOE ε4 allele (n; %ε4
+)
104; 39% 80; 40% 22; 34% .49
Parental history of AD
(n; %+)
213; 79.8% 159; 80% 52; 81% .83
Ethnicity (n; % white) 252; 95.8% 194; 97% 58; 91%
CES-D 6.6 (.49) 5.2 (.77) .83
Self-reported hearing loss
(n; % +)
9; 3% 7; 4% 2; 3% .80
Abbreviations: eMCI, early Mild Cognitive Impairment; F/M, female/male; WRAT-III, Wide
Range Achievement Test – Third Edition, reading subtest; APOE, apolipoprotein E; AD,
Alzheimer’s disease; CES-D, Clinical Evaluation Scale of Depression, MMSE, Mini-Mental
State Examination; RAVLT, Rey Auditory Verbal Learning Test, Total score. Note: Items in
bold indicate statistically significant difference between CH and eMCI at p < .05.
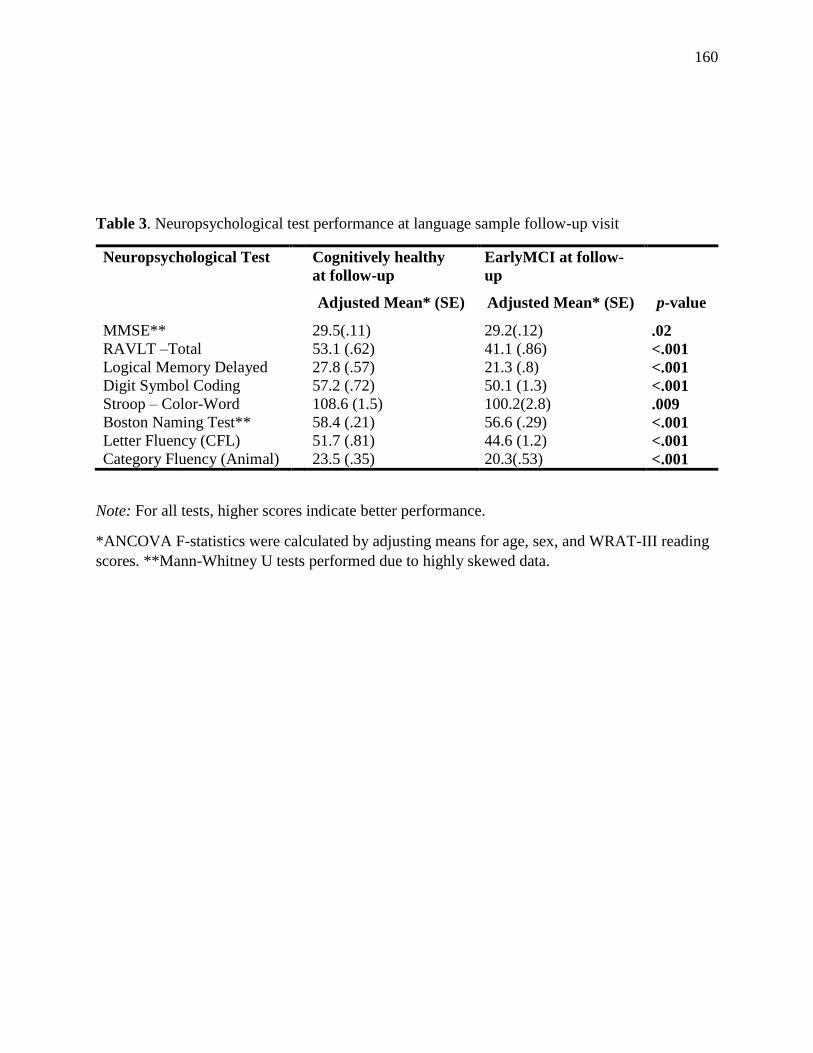
160
Table 3. Neuropsychological test performance at language sample follow-up visit
Neuropsychological Test Cognitively healthy
at follow-up
EarlyMCI at follow-
up
Adjusted Mean* (SE) Adjusted Mean* (SE) p-value
MMSE** 29.5(.11) 29.2(.12) .02
RAVLT –Total 53.1 (.62) 41.1 (.86) <.001
Logical Memory Delayed 27.8 (.57) 21.3 (.8) <.001
Digit Symbol Coding 57.2 (.72) 50.1 (1.3) <.001
Stroop – Color-Word 108.6 (1.5) 100.2(2.8) .009
Boston Naming Test** 58.4 (.21) 56.6 (.29) <.001
Letter Fluency (CFL) 51.7 (.81) 44.6 (1.2) <.001
Category Fluency (Animal) 23.5 (.35) 20.3(.53) <.001
Note: For all tests, higher scores indicate better performance.
*ANCOVA F-statistics were calculated by adjusting means for age, sex, and WRAT-III reading
scores. **Mann-Whitney U tests performed due to highly skewed data.
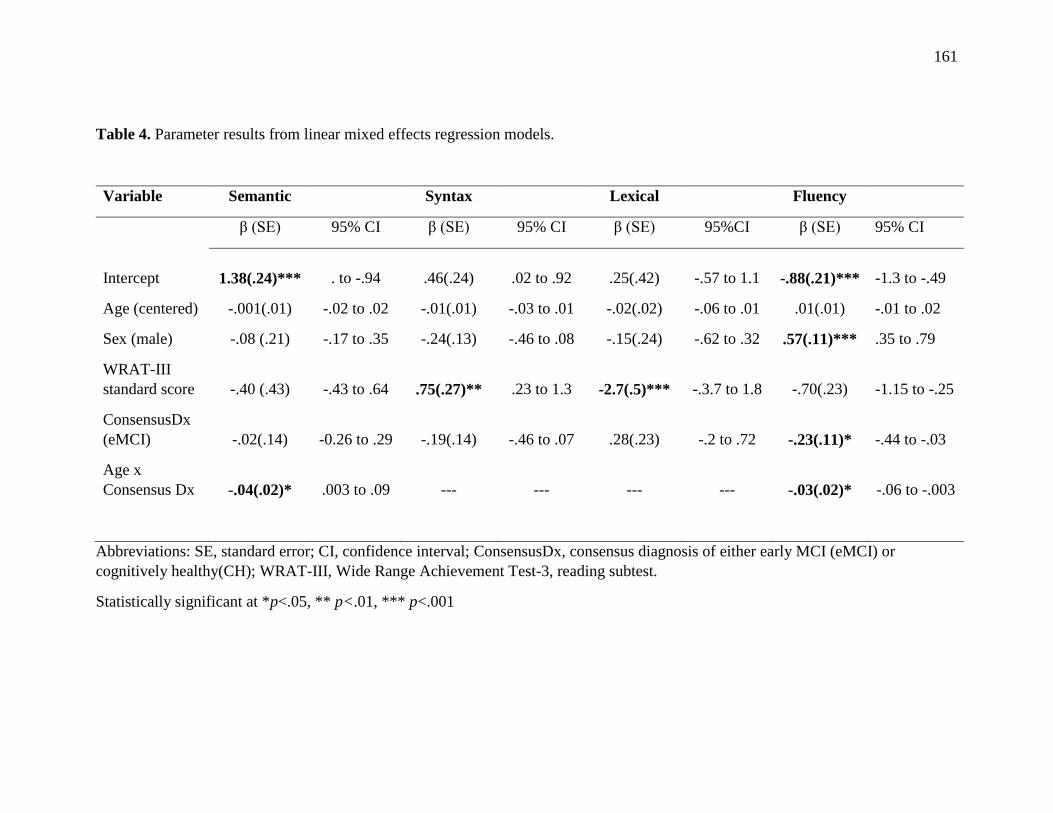
161
Table 4. Parameter results from linear mixed effects regression models.
Variable Semantic
Syntax
Lexical
Fluency
β (SE) 95% CI β (SE) 95% CI β (SE) 95%CI β (SE) 95% CI
Intercept 1.38(.24)*** . to -.94 .46(.24) .02 to .92 .25(.42) -.57 to 1.1 -.88(.21)*** -1.3 to -.49
Age (centered) -.001(.01) -.02 to .02 -.01(.01) -.03 to .01 -.02(.02) -.06 to .01 .01(.01) -.01 to .02
Sex (male) -.08 (.21) -.17 to .35 -.24(.13) -.46 to .08 -.15(.24) -.62 to .32 .57(.11)*** .35 to .79
WRAT-III
standard score -.40 (.43) -.43 to .64 .75(.27)** .23 to 1.3 -2.7(.5)*** -.3.7 to 1.8 -.70(.23) -1.15 to -.25
ConsensusDx
(eMCI) -.02(.14) -0.26 to .29 -.19(.14) -.46 to .07 .28(.23) -.2 to .72 -.23(.11)* -.44 to -.03
Age x
Consensus Dx -.04(.02)* .003 to .09 --- --- --- --- -.03(.02)* -.06 to -.003
Abbreviations: SE, standard error; CI, confidence interval; ConsensusDx, consensus diagnosis of either early MCI (eMCI) or
cognitively healthy(CH); WRAT-III, Wide Range Achievement Test-3, reading subtest.
Statistically significant at *p<.05, ** p<.01, *** p<.001
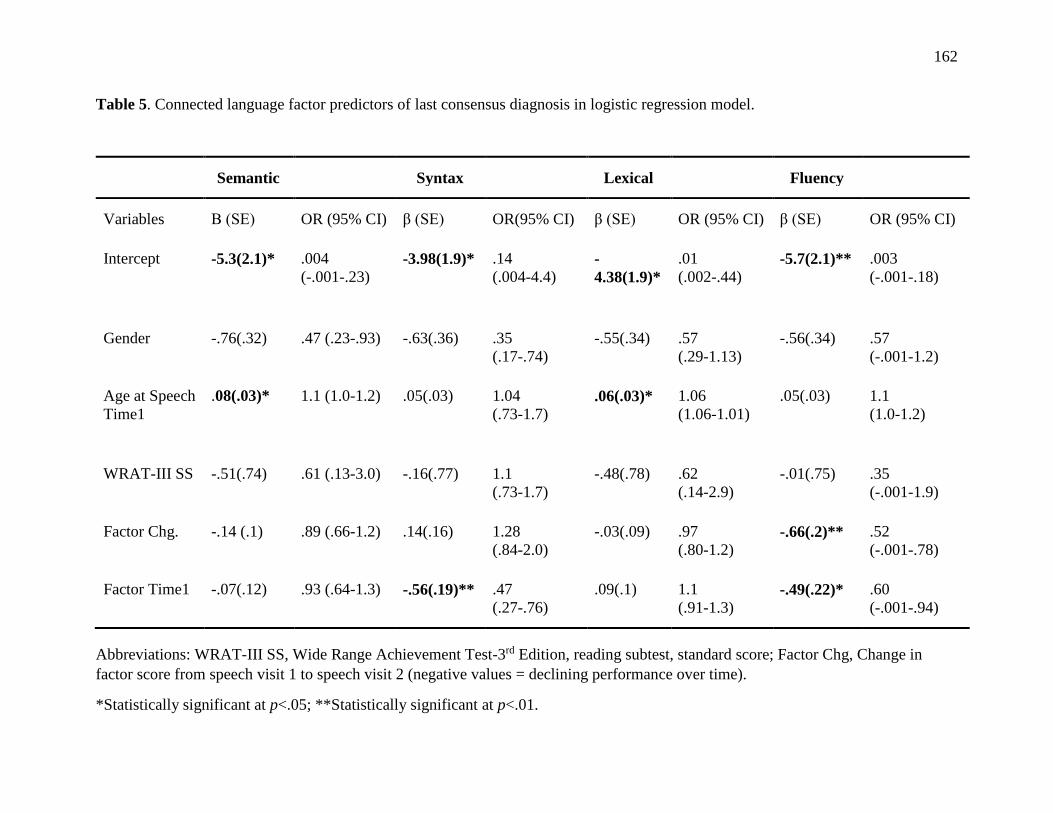
162
Table 5. Connected language factor predictors of last consensus diagnosis in logistic regression model.
Semantic Syntax Lexical Fluency
Variables Β (SE) OR (95% CI) β (SE) OR(95% CI) β (SE) OR (95% CI) β (SE) OR (95% CI)
Intercept -5.3(2.1)* .004
(-.001-.23) -3.98(1.9)* .14
(.004-4.4) -
4.38(1.9)*
.01
(.002-.44) -5.7(2.1)** .003
(-.001-.18)
Gender -.76(.32) .47 (.23-.93) -.63(.36) .35
(.17-.74)
-.55(.34) .57
(.29-1.13)
-.56(.34) .57
(-.001-1.2)
Age at Speech
Time1
.08(.03)* 1.1 (1.0-1.2) .05(.03) 1.04
(.73-1.7) .06(.03)* 1.06
(1.06-1.01)
.05(.03) 1.1
(1.0-1.2)
WRAT-III SS -.51(.74) .61 (.13-3.0) -.16(.77) 1.1
(.73-1.7)
-.48(.78) .62
(.14-2.9)
-.01(.75) .35
(-.001-1.9)
Factor Chg. -.14 (.1) .89 (.66-1.2) .14(.16) 1.28
(.84-2.0)
-.03(.09) .97
(.80-1.2) -.66(.2)** .52
(-.001-.78)
Factor Time1 -.07(.12) .93 (.64-1.3) -.56(.19)** .47
(.27-.76)
.09(.1) 1.1
(.91-1.3) -.49(.22)* .60
(-.001-.94)
Abbreviations: WRAT-III SS, Wide Range Achievement Test-3rd Edition, reading subtest, standard score; Factor Chg, Change in
factor score from speech visit 1 to speech visit 2 (negative values = declining performance over time).
*Statistically significant at p<.05; **Statistically significant at p<.01.
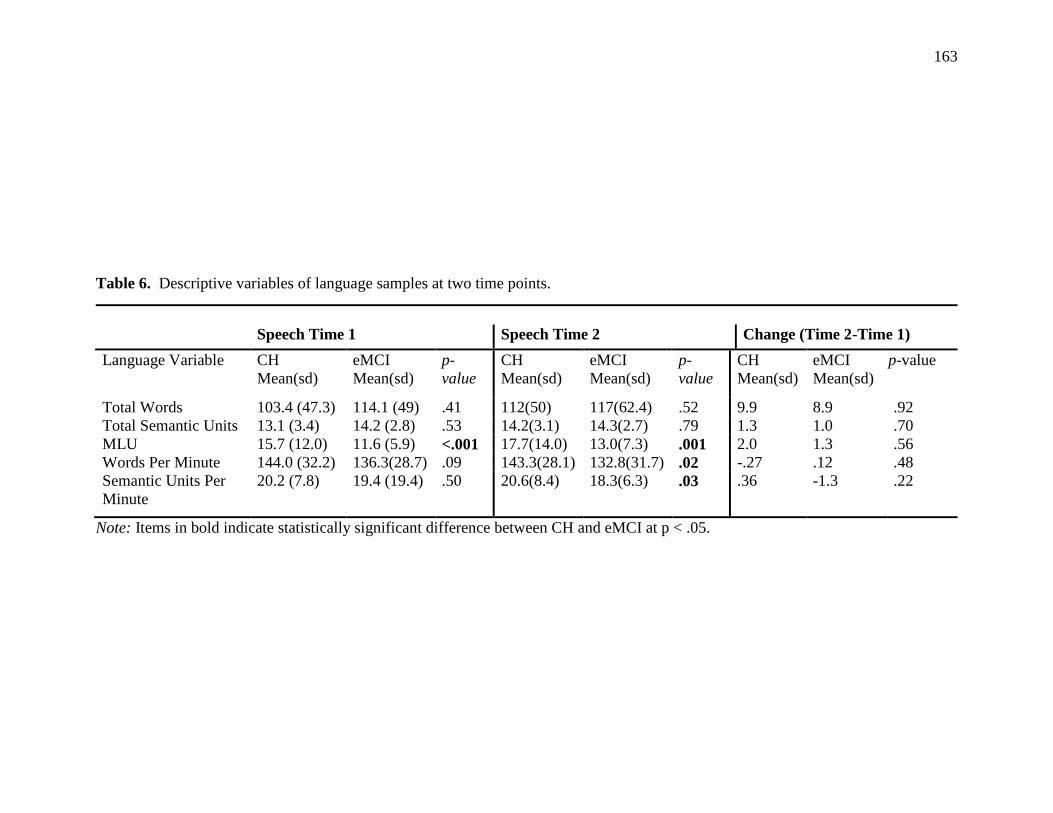
163
Table 6. Descriptive variables of language samples at two time points.
Speech Time 1 Speech Time 2 Change (Time 2-Time 1)
Language Variable CH
Mean(sd)
eMCI
Mean(sd)
p-
value
CH
Mean(sd)
eMCI
Mean(sd)
p-
value
CH
Mean(sd)
eMCI
Mean(sd)
p-value
Total Words 103.4 (47.3) 114.1 (49) .41 112(50) 117(62.4) .52 9.9 8.9 .92
Total Semantic Units 13.1 (3.4) 14.2 (2.8) .53 14.2(3.1) 14.3(2.7) .79 1.3 1.0 .70
MLU 15.7 (12.0) 11.6 (5.9) <.001 17.7(14.0) 13.0(7.3) .001 2.0 1.3 .56
Words Per Minute 144.0 (32.2) 136.3(28.7) .09 143.3(28.1) 132.8(31.7) .02 -.27 .12 .48
Semantic Units Per
Minute
20.2 (7.8) 19.4 (19.4) .50 20.6(8.4) 18.3(6.3) .03 .36 -1.3 .22
Note: Items in bold indicate statistically significant difference between CH and eMCI at p < .05.
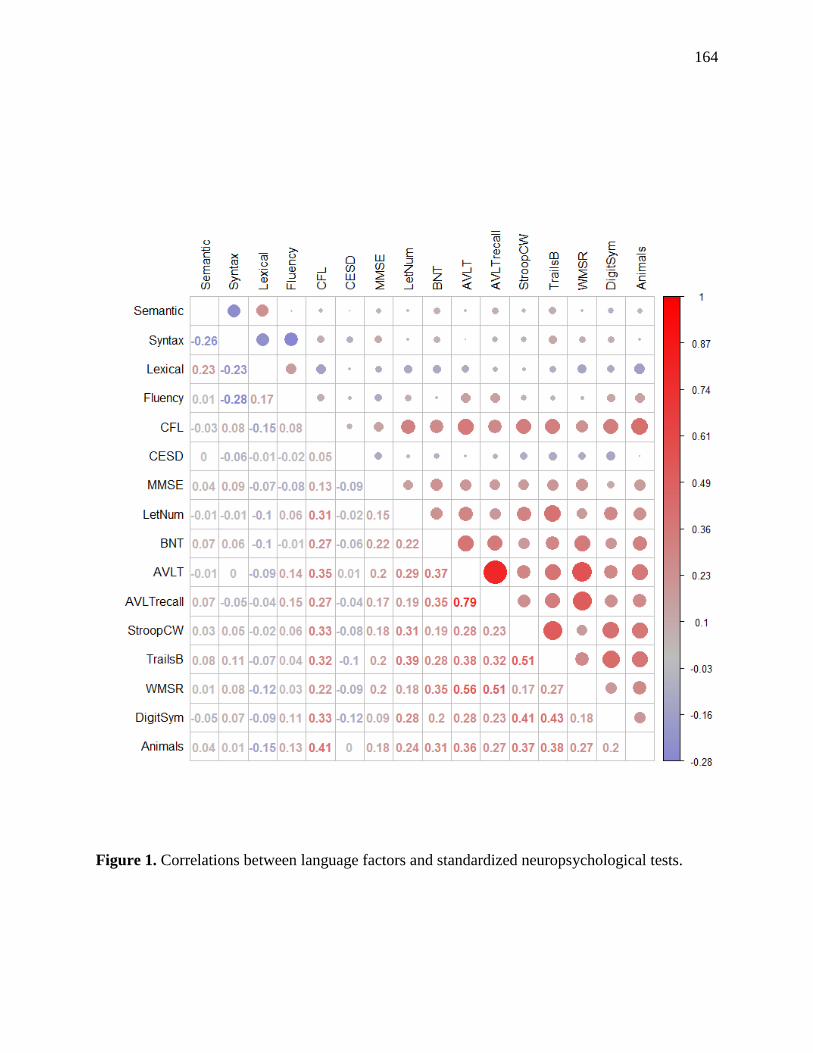
164
Figure 1. Correlations between language factors and standardized neuropsychological tests.
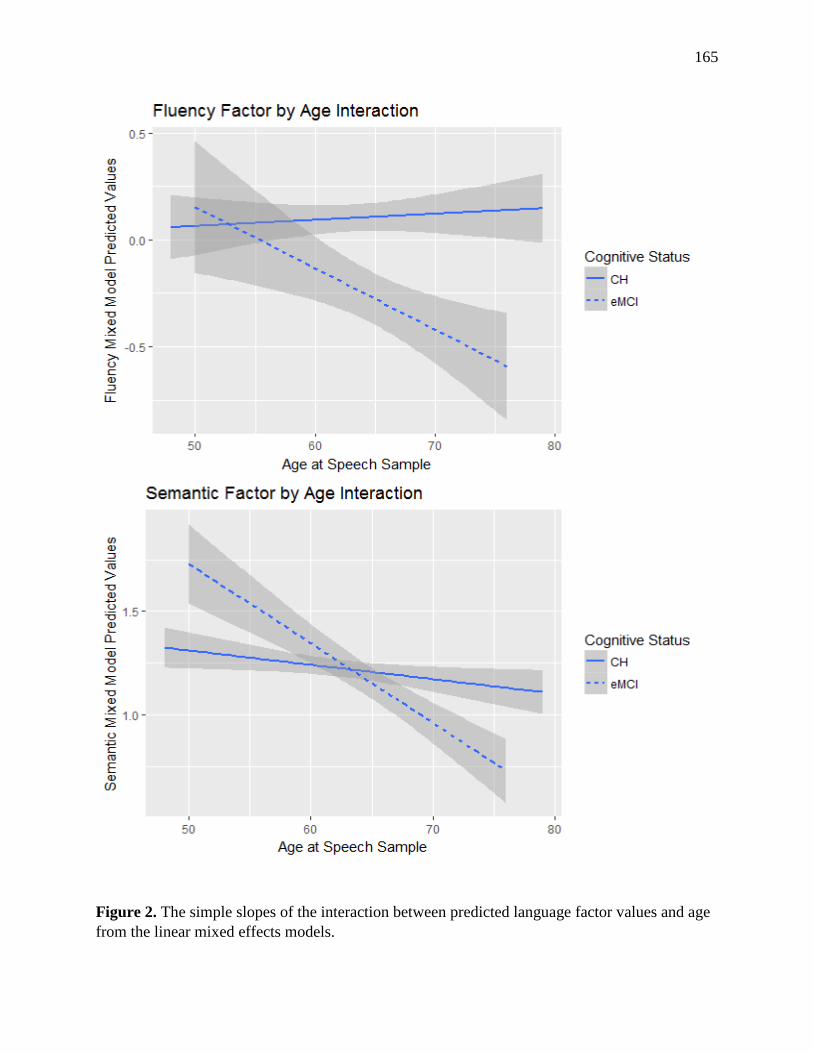
165
Figure 2. The simple slopes of the interaction between predicted language factor values and age
from the linear mixed effects models.
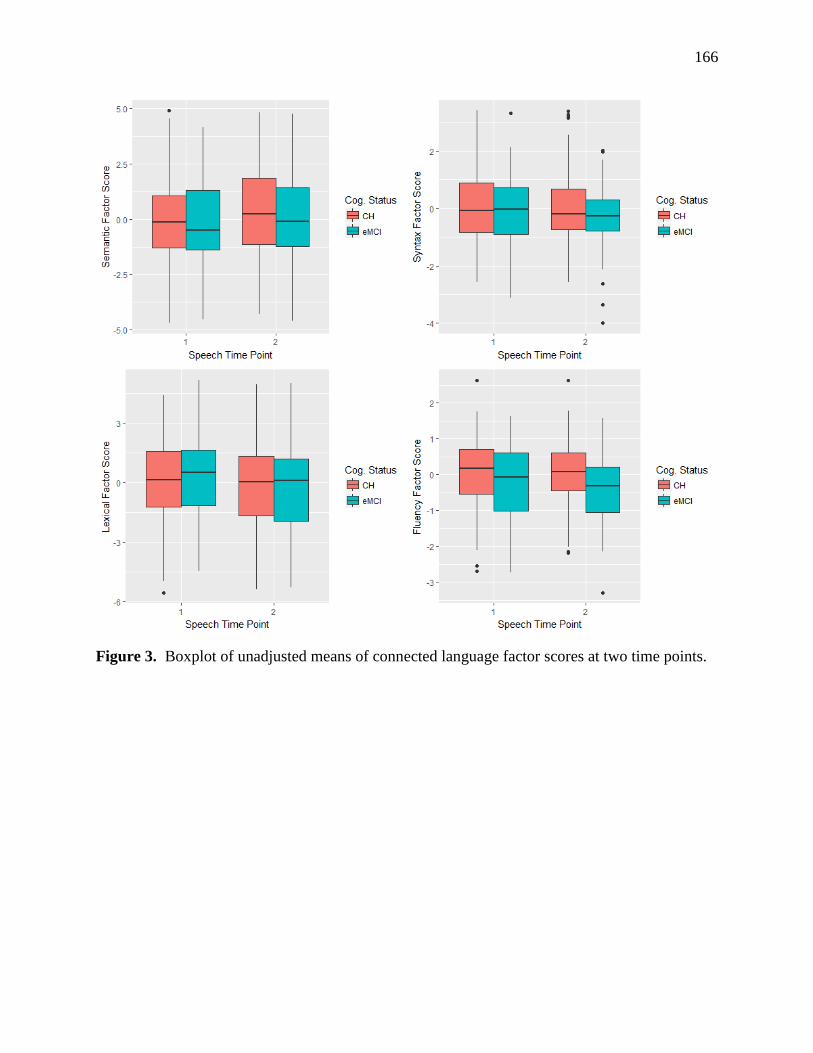
166
Figure 3. Boxplot of unadjusted means of connected language factor scores at two time points.
167
CHAPTER 6
Conclusion and Future Directions
168
CONCLUSIONS AND FUTURE DIRECTIONS
One of the most pressing needs in Alzheimer’s disease research is understanding the
earliest point at which cognitive decline co-occurs with AD neuropathology. Often by the time
patients present in the clinic, behavioral symptoms have already negatively affected daily
function and quality of life, and neurodegeneration due to AD pathology likely had begun
decades prior (Jack et al., 2013). Therefore, finding means of accurately detecting subtle declines
before they impact function is a goal for developing and monitoring interventions. A growing
body of evidence suggests that analyzing spontaneous, spoken language may help to achieve
this goal: detecting subtle cognitive decline and assessing function in an everyday, relatively
effortless activity. The purpose of the work presented here was to thoroughly examine and
characterize spoken language samples provided by participants who showed very early cognitive
declines, prior to clinical diagnosis of mild cognitive impairment or AD. The overarching goal
was to determine if connected language analysis could be an important and useful contributor to
detection of preclinical MCI, as well as a descriptive tool for understanding how early cognitive
decline may impact functional communication.
In the first paper, we described a detailed literature review that summarized all of the
measures derived from picture description tasks in adults with MCI and AD. We focused on
picture description tasks because of their limited demands on episodic memory, and thus the
measures are more representative of semantic memory and other language processes. The
ubiquitous use of picture description tasks in the AD literature also allowed for comparison
across studies. By constraining the review to one elicitation method, we provided a new and
focused addition to the literature on connected language performance in MCI and AD. We
concluded that there were disproportionately fewer studies of adults with MCI than those of
169
adults with AD, and that most of these studies had relatively small sample sizes. Evidence of
test-retest reliability and stability was minimal, so the feasibility of using these measures over
time was unknown. Finally, the review indicated that a large array of language variables were
examined with very little standardization across studies for terminology or ways in which
measures were derived. These conclusions led to the specific aims of this work.
In a series of studies, we first set out to determine if differences in connected language
were even detectable at a very early, preclinical phase of probable MCI. Next, we defined a
latent structure of discourse measures that resulted in four factors, and then tested the invariance
and stability of these factors over time. Finally, we used these factors to determine if aspects of
connected language were associated with cognitive decline over time.
In the first study (Manuscript 1—Chapter 3), we analyzed language samples from
participants of the Wisconsin Registry for Alzheimer’s Prevention (WRAP) and showed that
participants with psychometrically-defined memory declines (pMCI) expressed fewer semantic
content units than those who were cognitively stable. We also showed that the pMCI group had
significantly lower phonemic and semantic verbal fluency scores. Interestingly, however, the
semantic units measure was not correlated with either verbal fluency measure, but was positively
correlated with scores on tests of auditory verbal learning and memory. This suggested that
connected language measures may tap into different processes than verbal fluency tasks, an
assertion supported by another study that showed a lack of correlation between semantic
measures of connected speech and semantic verbal fluency in a group of adults with AD (Kavé
& Goral, 2016).
To our knowledge, our second study (Manuscript 2—Chapter 4) was the first to define
and confirm a latent structure of discourse variables. Although several studies have proposed
170
domains of connected language (e.g., semantics, syntax, lexical processing; (Samrah Ahmed et
al., 2012; Ahmed et al., 2013b; Wilson et al., 2010), and one study performed an exploratory
factor analysis (Kathleen C Fraser et al., 2015), no studies had confirmed these constructs and
tested their stability over time. Our factor structure consisted of four factors, which we proposed
corresponded to semantic, syntactic, lexical, and fluency domains of connected language. We
used confirmatory factor analysis in a separate subgroup of individuals and demonstrated that the
structure met goodness-of-fit criteria. We confirmed that the factors were invariant across sex
and family history status in our WRAP cohort. Finally, we examined these factors two years
apart in a group of cognitively healthy individuals, and found that the scores were adequately
stable at the two time points.
The third study (Manuscript 3—Chapter 5) used the novel factor scores developed from
study 2 in a subgroup of WRAP participants with transcribed language samples from two time
points, approximately two years apart. We demonstrated that the eMCI group declined more
rapidly than the cognitively healthy (CH) group in fluency and semantics. We also showed that
lower baseline syntax was predictive of eMCI status at time 2, and that a worsening of fluency
scores predicted eMCI status. We described metrics of the language samples using measures that
were not included in the factor structure, and showed that eMCI participants produced shorter
utterances, and took more time to express the same amount of content as the CH group.
Taken together, some results of the three studies were expected and others were
surprising. First, in both group comparison studies (Manuscripts 2 and 4), one or more elements
of semantic content were shown to differentiate between the two groups. Specifically, semantic
units and propositional idea density (Manuscript 2), semantic unit efficiency (semantic units per
minute), and an increased use of pronouns (Manuscript 4) were associated with very early
171
memory declines. This finding supports the hypothesis that problems with semantic memory
may coexist with declining episodic memory (Venneri et al., 2016). In our first cross-sectional
study, the psychometric MCI group expressed fewer semantic units than the cognitively stable
group, a finding that has been demonstrated in both the MCI and AD literature (Ahmed et al.,
2013a; Croisile et al., 1996; F. Cuetos et al., 2007). In our last study (Manuscript 4), semantic
units per minute (efficiency), increased use of pronouns, and decreased use nouns were
associated with early memory declines, which also was consistent with the MCI and AD
literature (Ahmed et al., 2013b; Almor et al., 1999). Paper 4 shows that total semantic units were
not associated with eMCI status; in fact, the group means were nearly identical at both time
points, which is contrary to our initial study and others (Croisile et al., 1996; F. Cuetos et al.,
2007). Further, total semantic units did not load on any factor in our factor analysis in a group of
cognitively healthy individuals. It is possible that semantic units alone may not be sensitive to
very early language declines, as in our early MCI construct. However, when evaluated in the
context of time (semantic units per minute), the measure was significantly different between the
eMCI and CH groups. This finding could suggest a slowing of word retrieval due to executive
functions or may reflect working memory deficits (Almor et al., 1999; Bayles, 2003). Future
research could address this by separating subtypes of eMCI (i.e., amnestic only versus executive
function subtypes), as well as combining temporal measures of connected language with tests of
speed and flexibility and timed verbal fluency.
That the fluency factor, “maze index,” was associated with eMCI status was somewhat
surprising, as some previous studies of MCI have not found this association (Ahmed et al.,
2013b; Kathleen C Fraser et al., 2015). As mentioned in the preceding chapter, our measure may
be a more comprehensive way to capture dysfluent behaviors than other studies that tested such
172
behaviors in isolation (e.g., “filled pauses” vs “repetitions”). The fluency factor showed a small
but significant correlation with the AVLT total and delayed recall scores, suggesting that it may
partially reflect an underlying problem with semantic memory, especially since the AVLT is
dependent on both episodic and lexical-semantic processes (Venneri et al., 2016). Like semantic-
units-per-minute, it is also possible that dysfluent behaviors reflect limitations in working
memory or executive functions and are compensatory in nature, particularly at very early stages
of the disease (Gayraud et al., 2011).
The fluency factor has an inherent advantage over the semantic factor in language
analysis: dysfluent behaviors are not dependent on the stimulus, whereas semantic factor
measures like idea density depend on carefully researched and predetermined semantic units
(Croisile et al., 1996) that are specific to the stimulus picture. Spontaneous discourse analysis
would be even more clinically meaningful if it were analyzed in a format more akin to typical
conversations (e.g., a back-and-forth conversation between a clinician or caregiver and the adult
with MCI) (Coelho, Ylvisaker, & Turkstra, 2005). Future research to determine if the fluency
factor remains a viable and sensitive measure across elicitation formats, such as open-ended
questions or back-and-forth conversations, would be an important next step toward assessing
actual function and developing detailed and stage-specific communication interventions.
These studies add both novel methods (exploratory and confirmatory factor analyses,
development of factor scores) and a unique study sample (late-middle-aged adults at risk for AD)
to the existing literature on connected language in MCI and AD. One obvious strength of this
work is the sample size: the factor analyses used language samples from 399 participants, and the
longitudinal study included data from 264 adults, whereas most other studies of MCI had
considerably smaller samples. The work here was completed prospectively, so data collection
173
procedures and scoring procedures were well documented and controlled, whereas many of the
frequently cited studies were based on retrospective analyses. Finally, to our knowledge, our
study is the largest longitudinal study of connected language in the MCI and AD literature.
Because of the demonstrated heterogeneity of both connected language performance (Duong et
al., 2005) and neurodegeneration due to AD pathology (Dong et al., 2016), the longitudinal
analyses and statistical methods used in this work are a strength as they may help to address
these sources of variability.
This work is not without limitations. First, although the CLAN program provided quick
and automated computation of a wide range of morphosyntactic features, it still required labor-
intensive transcription of individual language samples. With continuing advancement of Natural
Language Processing (NLP), Automatic Speech Recognition (ASR), and machine learning
algorithms, this limitation can be addressed in the near future. These automated techniques have
been used to extract linguistic features (Kathleen C Fraser et al., 2015), articulation rate and
duration of unfilled pauses (Tóth, Gosztolya, Vincze, Hoffmann, & Szatlóczki, 2015), vocal and
periodic segments (König et al., 2015), and “emotional temperature” based on measures of pitch,
intensity, and vocal quality (Alonso, Cabrera, Medina, & Travieso, 2015; López-de-Ipiña et al.,
2013). The WRAP study’s language sample data would be a rich source for these techniques to
further enhance our understanding of preclinical AD biomarkers, while developing analysis
methods that are quick, sensitive, and feasible for large-scale studies or for use with patients in
the clinic.
One strength of this work can also be considered a limitation: the WRAP study sample, a
large, longitudinal cohort study of a unique at-risk group, is primarily self-selected, and with that
comes inherent factors that limit generalizability to other populations. Namely, many of the
174
participants with positive family history were caregivers for a parent with AD, and many of the
participants with negative family histories were spouses of caregivers. Their exposure to the
disease course of AD, their knowledge about risk, and the stress that may have been induced by
caregiving may introduce psycho-social differences that are not typical of the general population.
The WRAP study sample is predominantly white, and largely from the college town of Madison,
Wisconsin, which also does not represent the general population. A growing body of evidence
suggests that the prevalence of Alzheimer’s disease may be twice as high among adults who are
African American than non-Hispanic whites (Barnes & Yaffe, 2011). The WRAP study is
working to address this limitation by increasing and enhancing recruitment efforts of under-
represented groups in urban and rural areas of Wisconsin (Green-Harris, Houston, Skora, &
Farrar-Edwards, 2016).
Our early MCI construct, while innovative and necessary for detecting sub-clinical
declines that fall within the range of standardized test norms, can also be considered a limitation
in these particular analyses. The participants with eMCI may be experiencing declines
attributable to a different neurodegenerative process other than Alzheimer’s disease. Future
analyses will address this limitation by combining our language analyses with fluid and
neuroimaging markers, such as accumulation of beta-amyloid (Aβ) and tau protein collected
from positron emission tomography (PET) imaging, cerebrospinal fluid (CSF) assays, and
diffusion tensor imaging (DTI) and structural magnetic resonance imaging (MRI). These future
analyses may strengthen our results, as well as help to further understand the distinct neural
networks associated with speech and language decline.
In conclusion, these findings provide support for using connected language analysis as a
means toward understanding the earliest point at which communication skills may be affected on
175
the probable AD continuum. We have presented the relevance and rationale of this method as an
innovative, performance-based measure for early detection of problems with language and
everyday function, but the results may have farther-reaching effects for individuals living with
MCI and AD. Speech-language pathologists (SLPs) are a largely untapped resource in the
clinical field of MCI and AD, despite being highly trained in understanding the brain-behavior
relationships, pathophysiology, and neuropsychological processes underpinning cognitive
aspects of communication. Efficacy has been established for SLP early interventions including
assistive technology (including Hearing Assisted Technology Systems (HATS), cognitive
stimulation therapy, environmental modifications, external memory aids, memory training
programs; and caregiver, community, and healthcare professional communication training and
education (Arkin & Mahendra, 2001; Bharucha et al., 2009; Brush, Meehan, & Calkins, 2002;
Camp & Skrajner, 2004; Hopper, Drefs, Bayles, Tomoeda, & Dinu, 2010; Mahendra, 2001).
Adults with MCI and AD and their caregivers are entitled to these evidence-based interventions,
yet federal funding and insurance dollars do not match the need. One route toward improving
this discrepancy is research. The work presented here adds support to the theory that very early
declines can be detected in everyday speech, and it is our hope that this and future work will lead
to better detection of functional decline, and improved, stage-specific cognitive-communication
interventions for adults with MCI and dementia.
176
REFERENCES
Ahmed, S., de Jager, C. A., Haigh, A.-M. F., & Garrard, P. (2012). Logopenic aphasia in
Alzheimer's disease: clinical variant or clinical feature? Journal of Neurology,
Neurosurgery & Psychiatry, jnnp-2012-302798.
Ahmed, S., de Jager, C. A., Haigh, A. M., & Garrard, P. (2012a). Logopenic aphasia in
Alzheimer's disease: clinical variant or clinical feature? J Neurol Neurosurg Psychiatry,
83(11), 1056-1062. doi:10.1136/jnnp-2012-302798
Ahmed, S., de Jager, C. A., Haigh, A. M., & Garrard, P. (2013a). Semantic processing in
connected speech at a uniformly early stage of autopsy-confirmed Alzheimer's disease.
Neuropsychology, 27(1), 79-85. doi:10.1037/a0031288
Ahmed, S., de Jager, C. A., Haigh, A. M. F., & Garrard, P. (2012b). Logopenic aphasia in
Alzheimer's disease: clinical variant or clinical feature? Journal of Neurology
Neurosurgery and Psychiatry, 83(11), 1056-1062. doi:10.1136/jnnp-2012-302798
Ahmed, S., Haigh, A. M., de Jager, C. A., & Garrard, P. (2013b). Connected speech as a marker
of disease progression in autopsy-proven Alzheimer's disease. Brain, 136(Pt 12), 3727-
3737. doi:10.1093/brain/awt269
Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., . . . Phelps,
C. H. (2011). The diagnosis of mild cognitive impairment due to Alzheimer's disease:
recommendations from the National Institute on Aging-Alzheimer's Association
workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement, 7(3),
270-279. doi:10.1016/j.jalz.2011.03.008
Alcolea, D., Carmona-Iragui, M., Suarez-Calvet, M., Sanchez-Saudinos, M. B., Sala, I., Anton-
Aguirre, S., . . . Lleo, A. (2014). Relationship between beta-Secretase, inflammation and
core cerebrospinal fluid biomarkers for Alzheimer's disease. J Alzheimers Dis, 42(1),
157-167. doi:10.3233/JAD-140240
Almor, A., Kempler, D., MacDonald, M. C., Andersen, E. S., & Tyler, L. K. (1999). Why do
Alzheimer patients have difficulty with pronouns? Working memory, semantics, and
reference in comprehension and production in Alzheimer's disease. Brain Lang, 67(3),
202-227. doi:10.1006/brln.1999.2055
Alonso, J. B., Cabrera, J., Medina, M., & Travieso, C. M. (2015). New approach in
quantification of emotional intensity from the speech signal: emotional temperature.
Expert Systems with Applications, 42(24), 9554-9564.
Alvarez, J. A., & Emory, E. (2006). Executive function and the frontal lobes: a meta-analytic
review. Neuropsychology review, 16(1), 17-42.

177
Aramaki, E., Shikata, S., Miyabe, M., & Kinoshita, A. (2016). Vocabulary size in speech may be
an early indicator of cognitive impairment. PLoS One, 11(5), e0155195.
Arkin, S., & Mahendra, N. (2001). Discourse analysis of Alzheimer's patients before and after
intervention: Methodology and outcomes. Aphasiology, 15(6), 533-569.
Association, A. s. (2014).
2014 Facts and Figures - Alzheimer's Association. (n.d.). . Retrieved from
http://www.alz.org/downloads/facts_figures_2014.pdf
Barbeau, E. J., Didic, M., Joubert, S., Guedj, E., Koric, L., Felician, O., . . . Ceccaldi, M. (2012).
Extent and neural basis of semantic memory impairment in mild cognitive impairment. J
Alzheimers Dis, 28(4), 823-837. doi:10.3233/JAD-2011-110989
Barnes, D. E., & Yaffe, K. (2011). The projected effect of risk factor reduction on Alzheimer's
disease prevalence. The Lancet Neurology, 10(9), 819-828.
Barnes, L. L., Wilson, R. S., Bienias, J. L., Schneider, J. A., Evans, D. A., & Bennett, D. A.
(2005). Sex differences in the clinical manifestations of alzheimer disease pathology.
Archives of General Psychiatry, 62(6), 685-691. doi:10.1001/archpsyc.62.6.685
Bartels, C., Wegrzyn, M., Wiedl, A., Ackermann, V., & Ehrenreich, H. (2010). Practice effects
in healthy adults: a longitudinal study on frequent repetitive cognitive testing. BMC
neuroscience, 11(1), 118.
Bates, D., Maechler, M., Bolker, B., & Walker, S. (2014). lme4: Linear mixed-effects models
using Eigen and S4. R package version, 1(7).
Bates, E., Harris, C., Marchman, V., Wulfeck, B., & Kritchevsky, M. (1995). Production of
complex syntax in normal ageing and Alzheimer's disease. Language and Cognitive
Processes, 10(5), 487-539.
Bayles, K. A. (2003). Effects of working memory deficits on the communicative functioning of
Alzheimer’s dementia patients. J Commun Disord, 36(3), 209-219.
Bayles, K. A., Azuma, T., Cruz, R. F., Tomoeda, C. K., Wood, J. A., & Montgomery Jr, E. B.
(1999). Gender differences in language of Alzheimer disease patients revisited. Alzheimer
Disease and Associated Disorders, 13(3), 138-146.
Bayles, K. A., & Tomoeda, C. K. (1983). Confrontation naming impairment in dementia. Brain
Lang, 19(1), 98-114.

178
Bayles, K. A., Tomoeda, C. K., Kaszniak, A. W., Stern, L. Z., & Eagans, K. K. (1985). Verbal
perseveration of dementia patients. Brain Lang, 25(1), 102-116.
Bayles, K. A., Tomoeda, C. K., & Trosset, M. W. (1992). Relation of linguistic communication
abilities of Alzheimer's patients to stage of disease. Brain Lang, 42(4), 454-472.
Bayles, K. A., Tomoeda, C. K., & Trosset, M. W. (1993). Alzheimer's disease: Effects on
language. Developmental Neuropsychology, 9(2), 131-160.
Beavers, A. S., Lounsbury, J. W., Richards, J. K., Huck, S. W., Skolits, G. J., & Esquivel, S. L.
(2013). Practical considerations for using exploratory factor analysis in educational
research. Practical assessment, research & evaluation, 18(6), 1-13.
Beckerman, H., Roebroeck, M. E., Lankhorst, G. J., Becher, J. G., Bezemer, P. D., & Verbeek,
A. L. (2001). Smallest real difference, a link between reproducibility and responsiveness.
Qual Life Res, 10(7), 571-578.
Beeri, M. S., & Sonnen, J. (2016). Brain BDNF expression as a biomarker for cognitive reserve
against Alzheimer disease progression. Neurology, 86(8), 702-703.
doi:10.1212/WNL.0000000000002389
Berisha, V., Wang, S., LaCross, A., & Liss, J. (2015). Tracking discourse complexity preceding
Alzheimer's disease diagnosis: a case study comparing the press conferences of
Presidents Ronald Reagan and George Herbert Walker Bush. J Alzheimers Dis, 45(3),
959-963. doi:10.3233/JAD-142763
Bharucha, A. J., Anand, V., Forlizzi, J., Dew, M. A., Reynolds, C. F., Stevens, S., & Wactlar, H.
(2009). Intelligent assistive technology applications to dementia care: current capabilities,
limitations, and future challenges. The American Journal of Geriatric Psychiatry, 17(2),
88-104.
Bickel, C., Pantel, J., Eysenbach, K., & Schröder, J. (2000). Syntactic comprehension deficits in
Alzheimer's disease. Brain Lang, 71(3), 432-448.
Bird, H., Lambon Ralph, M. A., Patterson, K., & Hodges, J. R. (2000). The rise and fall of
frequency and imageability: noun and verb production in semantic dementia. Brain Lang,
73(1), 17-49. doi:10.1006/brln.2000.2293
Blair, M., Marczinski, C. A., Davis-Faroque, N., & Kertesz, A. (2007). A longitudinal study of
language decline in Alzheimer's disease and frontotemporal dementia. Journal of the
International Neuropsychological Society, 13(02), 237-245.
179
Bleecker, M. L., Bolla-Wilson, K., Agnew, J., & Meyers, D. A. (1988). Age? related sex
differences in verbal memory. Journal of clinical psychology, 44(3), 403-411.
Bowles, N. L., Obler, L. K., & Albert, M. L. (1987). Naming errors in healthy aging and
dementia of the Alzheimer type. Cortex, 23(3), 519-524.
Braak, H., & Braak, E. (1991). Neuropathological stageing of Alzheimer-related changes. Acta
neuropathologica, 82(4), 239-259.
Bretsky, P., Guralnik, J., Launer, L., Albert, M., & Seeman, T. E. (2003). The role of APOE-ε4
in longitudinal cognitive decline MacArthur Studies of Successful Aging. Neurology,
60(7), 1077-1081.
Brookshire, R. H., & Nicholas, L. E. (1994a). Speech sample size and test-retest stability of
connected speech measures for adults with aphasia. Journal of Speech, Language, and
Hearing Research, 37(2), 399-407.
Brookshire, R. H., & Nicholas, L. E. (1994b). Test-retest stability of measures of connected
speech in aphasia. Clinical aphasiology, 22(1), 19-133.
Brown, C., Snodgrass, T., Kemper, S. J., Herman, R., & Covington, M. A. (2008). Automatic
Measurement of Propositional Idea Density from Part-of-Speech Tagging. Behavior
research methods, 40(2), 540-545.
Brush, J. A., Meehan, R. A., & Calkins, M. P. (2002). Using the environment to improve intake
for people with dementia. Alzheimer's Care Today, 3(4), 330-338.
Bschor, T., Kuhl, K. P., & Reischies, F. M. (2001). Spontaneous speech of patients with
dementia of the Alzheimer type and mild cognitive impairment. Int Psychogeriatr, 13(3),
289-298.
Buckner, R. L. (2004). Memory and executive function in aging and AD: multiple factors that
cause decline and reserve factors that compensate. Neuron, 44(1), 195-208.
Byom, L. J., & Turkstra, L. (2012). Effects of social cognitive demand on theory of mind in
conversations of adults with traumatic brain injury. International Journal of Language &
Communication Disorders, 47(3), 310-321.
Byrne, B. M., Shavelson, R. J., & Muthén, B. (1989). Testing for the equivalence of factor
covariance and mean structures: The issue of partial measurement invariance.
Psychological bulletin, 105(3), 456.
180
Camp, C. J., & Skrajner, M. J. (2004). Resident-Assisted Montessori Programming (RAMP):
training persons with dementia to serve as group activity leaders. Gerontologist, 44(3),
426-431.
Carlomagno, S., Santoro, A., Menditti, A., Pandolfi, M., & Marini, A. (2005). Referential
communication in Alzheimer's type dementia. Cortex, 41(4), 520-534.
Cattell, R. B. (1966). The scree test for the number of factors. Multivariate behavioral research,
1(2), 245-276.
Chapman, S. B., Ulatowska, H. K., King, K., Johnson, J. K., & McIntire, D. D. (1995).
Discourse in early Alzheimer's disease versus normal advanced aging. American Journal
of Speech-Language Pathology, 4(4), 124-129.
Choi, H. (2009). Performances in a picture description task in Japanese patients with
Alzheimer’s disease and with mild cognitive impairment. Korean Journal of
Communication Disorders, 14(14), 326-337.
Chung, J. A., & Cummings, J. L. (2000). Neurobehavioral and neuropsychiatric symptoms in
Alzheimer's disease. Neurologic clinics, 18(4), 829-846.
Ciccia, A. (2011). Pragmatic Communication. In J. S. Kreutzer, J. DeLuca, & B. Caplan (Eds.),
Encyclopedia of Clinical Neuropsychology (pp. 1994-1995). New York, NY: Springer
New York.
Ciccia, A. H., & Turkstra, L. S. (2002). Cohesion, communication burden, and response
adequacy in adolescent conversations. Advances in Speech Language Pathology, 4(1), 1-
8.
Clark, L. J., Gatz, M., Zheng, L., Chen, Y. L., McCleary, C., & Mack, W. J. (2009). Longitudinal
verbal fluency in normal aging, preclinical, and prevalent Alzheimer's disease. Am J
Alzheimers Dis Other Demen, 24(6), 461-468. doi:10.1177/1533317509345154
Clark, L. R., Koscik, R. L., Nicholas, C. R., Okonkwo, O. C., Engelman, C. D., Bratzke, L. C., . .
. Johnson, S. C. (2016). Mild Cognitive Impairment in Late Middle Age in the Wisconsin
Registry for Alzheimer's Prevention Study: Prevalence and Characteristics Using Robust
and Standard Neuropsychological Normative Data. Arch Clin Neuropsychol.
doi:10.1093/arclin/acw024
Clarnette, R. M., Almeida, O. P., Forstl, H., Paton, A., & Martins, R. N. (2001). Clinical
characteristics of individuals with subjective memory loss in Western Australia: results
from a cross‐sectional survey. Int J Geriatr Psychiatry, 16(2), 168-174.
181
Coats, M., & Morris, J. C. (2005). Antecedent biomarkers of Alzheimer's disease: the adult
children study. J Geriatr Psychiatry Neurol, 18(4), 242-244.
doi:10.1177/0891988705281881
Cockrell, J., & Folstein, M. F. (1987). Mini-Mental State Examination (MMSE).
Psychopharmacology bulletin, 24(4), 689-692.
Coelho, C., Ylvisaker, M., & Turkstra, L. S. (2005). Nonstandardized assessment approaches for
individuals with traumatic brain injuries. Paper presented at the Semin Speech Lang.
Coelho, C. A., Liles, B. Z., & Duffy, R. J. (1995). Impairments of discourse abilities and
executive functions in traumatically brain-injured adults. Brain injury, 9(5), 471-477.
Covington, M. A., & McFall, J. D. (2010). Cutting the Gordian knot: The moving-average type–
token ratio (MATTR). Journal of Quantitative Linguistics, 17(2), 94-100.
Croisile, B., Ska, B., Brabant, M. J., Duchene, A., Lepage, Y., Aimard, G., & Trillet, M. (1996).
Comparative study of oral and written picture description in patients with Alzheimer's
disease. Brain Lang, 53(1), 1-19. doi:10.1006/brln.1996.0033
Cronbach, L. J. (1951). Coefficient alpha and the internal structure of tests. Psychometrika,
16(3), 297-334. doi:10.1007/bf02310555
Cuetos, F., Arango-Lasprilla, J. C., Uribe, C., Valencia, C., & Lopera, F. (2007). Linguistic
changes in verbal expression: a preclinical marker of Alzheimer's disease. Journal of the
International Neuropsychological Society, 13(03), 433-439.
Cuetos, F., Arango-Lasprilla, J. C., Uribe, C., Valencia, C., & Lopera, F. (2007). Linguistic
changes in verbal expression: a preclinical marker of Alzheimer's disease. J Int
Neuropsychol Soc, 13(3), 433-439. doi:10.1017/S1355617707070609
Damasio, A. R., & Tranel, D. (1993). Nouns and verbs are retrieved with differently distributed
neural systems. Proceedings of the National Academy of Sciences, 90(11), 4957-4960.
Daniele, A., Giustolisi, L., Silveri, M. C., Colosimo, C., & Gainotti, G. (1994). Evidence for a
possible neuroanatomical basis for lexical processing of nouns and verbs.
Neuropsychologia, 32(11), 1325-1341.
Davis, B. H., & Maclagan, M. (2009). Examining pauses in Alzheimer's discourse. Am J
Alzheimers Dis Other Demen, 24(2), 141-154. doi:10.1177/1533317508328138

182
De Jager, C., Blackwell, A. D., Budge, M. M., & Sahakian, B. J. (2005). Predicting cognitive
decline in healthy older adults. The American Journal of Geriatric Psychiatry, 13(8),
735-740.
De Jager, C. A., & Budge, M. M. (2005). Stability and predictability of the classification of mild
cognitive impairment as assessed by episodic memory test performance over time.
Neurocase, 11(1), 72-79.
De Renzi, A., & Vignolo, L. A. (1962). Token test: A sensitive test to detect receptive
disturbances in aphasics. Brain: a journal of neurology.
Didic, M., Barbeau, E. J., Felician, O., Tramoni, E., Guedj, E., Poncet, M., & Ceccaldi, M.
(2011). Which memory system is impaired first in Alzheimer's disease? J Alzheimers Dis,
27(1), 11-22. doi:10.3233/JAD-2011-110557
Dobie, D. (2002). Depression, dementia, and pseudodementia. Paper presented at the Seminars
in clinical neuropsychiatry.
Dong, A., Toledo, J. B., Honnorat, N., Doshi, J., Varol, E., Sotiras, A., . . . Initiative, A. s. D. N.
(2016). Heterogeneity of neuroanatomical patterns in prodromal Alzheimer’s disease:
links to cognition, progression and biomarkers. Brain, aww319.
Dowling, N. M., Hermann, B., La Rue, A., & Sager, M. A. (2010). Latent structure and factorial
invariance of a neuropsychological test battery for the study of preclinical Alzheimer's
disease. Neuropsychology, 24(6), 742.
Drummond, C., Coutinho, G., Fonseca, R. P., Assuncao, N., Teldeschi, A., de Oliveira-Souza,
R., . . . Mattos, P. (2015). Deficits in narrative discourse elicited by visual stimuli are
already present in patients with mild cognitive impairment. Front Aging Neurosci, 7, 96.
doi:10.3389/fnagi.2015.00096
Dubois, B., Feldman, H. H., Jacova, C., DeKosky, S. T., Barberger-Gateau, P., Cummings, J., . .
. Jicha, G. (2007). Research criteria for the diagnosis of Alzheimer's disease: revising the
NINCDS–ADRDA criteria. The Lancet Neurology, 6(8), 734-746.
Duong, A., Giroux, F., Tardif, A., & Ska, B. (2005). The heterogeneity of picture-supported
narratives in Alzheimer's disease. Brain Lang, 93(2), 173-184.
doi:10.1016/j.bandl.2004.10.007
Ehrlich, J. S., Obler, L. K., & Clark, L. (1997). Ideational and semantic contributions to narrative
production in adults with dementia of the Alzheimer's type. J Commun Disord, 30(2), 79-
98; quiz 98-79.
183
Ellis, K. A., Bush, A. I., Darby, D., De Fazio, D., Foster, J., Hudson, P., . . . Group, A. R. (2009).
The Australian Imaging, Biomarkers and Lifestyle (AIBL) study of aging: methodology
and baseline characteristics of 1112 individuals recruited for a longitudinal study of
Alzheimer's disease. Int Psychogeriatr, 21(4), 672-687.
doi:10.1017/S1041610209009405
Engelman, M., Agree, E. M., Meoni, L. A., & Klag, M. J. (2010). Propositional density and
cognitive function in later life: Findings from the Precursors Study. The Journals of
Gerontology Series B: Psychological Sciences and Social Sciences, 65(6), 706-711.
Faber-Langendoen, K., Morris, J. C., Knesevich, J. W., LaBarge, E., Miller, J. P., & Berg, L.
(1988). Aphasia in senile dementia of the Alzheimer type. Ann Neurol, 23(4), 365-370.
doi:10.1002/ana.410230409
Fabrigar, L. R., Wegener, D. T., MacCallum, R. C., & Strahan, E. J. (1999). Evaluating the use
of exploratory factor analysis in psychological research. Psychological methods, 4(3),
272.
Fergadiotis, G., Wright, H. H., & Capilouto, G. J. (2011). Productive vocabulary across
discourse types. Aphasiology, 25(10), 1261-1278. doi:10.1080/02687038.2011.606974
Fischer, P., Jungwirth, S., Zehetmayer, S., Weissgram, S., Hoenigschnabl, S., Gelpi, E., . . .
Tragl, K. H. (2007). Conversion from subtypes of mild cognitive impairment to
Alzheimer dementia. Neurology, 68(4), 288-291.
doi:10.1212/01.wnl.0000252358.03285.9d
Fleiss, J. L. (1986). Reliability of measurement. The design and analysis of clinical experiments,
1-32.
Fleming, V. B., & Harris, J. L. (2008). Complex discourse production in mild cognitive
impairment: Detecting subtle changes. Aphasiology, 22(7-8), 729-740.
Forbes-McKay, K., Shanks, M. F., & Venneri, A. (2013). Profiling spontaneous speech decline
in Alzheimer's disease: a longitudinal study. Acta neuropsychiatrica, 25(06), 320-327.
Forbes-McKay, K. E., & Venneri, A. (2005). Detecting subtle spontaneous language decline in
early Alzheimer's disease with a picture description task. Neurol Sci, 26(4), 243-254.
doi:10.1007/s10072-005-0467-9
Forbes, K. E., Venneri, A., & Shanks, M. F. (2001). Distinct patterns of spontaneous speech
deterioration: an early predictor of Alzheimer's disease. Brain Cogn, 48(2-3), 356-361.
184
Forbes, K. E., Venneri, A., & Shanks, M. F. (2002). Distinct patterns of spontaneous speech
deterioration: an early predictor of Alzheimer's disease. Brain Cogn, 48(2-3), 356-361.
Fornell, C., & Larcker, D. F. (1981). Structural equation models with unobservable variables and
measurement error: Algebra and statistics. Journal of marketing research, 382-388.
Fraser, K. C., Meltzer, J. A., Graham, N. L., Leonard, C., Hirst, G., Black, S. E., & Rochon, E.
(2014). Automated classification of primary progressive aphasia subtypes from narrative
speech transcripts. Cortex, 55, 43-60. doi:10.1016/j.cortex.2012.12.006
Fraser, K. C., Meltzer, J. A., & Rudzicz, F. (2015). Linguistic features identify Alzheimer's
disease in narrative speech. Journal of Alzheimer's Disease, 49(2), 407-422.
Fraser, K. C., Meltzer, J. A., & Rudzicz, F. (2015). Linguistic Features Identify Alzheimer’s
Disease in Narrative Speech. Journal of Alzheimer's Disease, 49(2), 407-422.
Frisoni, G. B., Fratiglioni, L., Fastbom, J., Viitanen, M., & Winblad, B. (1999). Mortality in
nondemented subjects with cognitive impairment: the influence of health-related factors.
American journal of epidemiology, 150(10), 1031-1044.
Garrard, P., Haigh, A.-M., & de Jager, C. (2011). Techniques for transcribers: assessing and
improving consistency in transcripts of spoken language. Literary and Linguistic
Computing, fqr018.
Garrard, P., Maloney, L. M., Hodges, J. R., & Patterson, K. (2005). The effects of very early
Alzheimer's disease on the characteristics of writing by a renowned author. Brain, 128(Pt
2), 250-260. doi:10.1093/brain/awh341
Gayraud, F., Lee, H. R., & Barkat-Defradas, M. (2011). Syntactic and lexical context of pauses
and hesitations in the discourse of Alzheimer patients and healthy elderly subjects. Clin
Linguist Phon, 25(3), 198-209. doi:10.3109/02699206.2010.521612
Giles, E., Patterson, K., & Hodges, J. R. (1996). Performance on the Boston Cookie Theft picture
description task in patients with early dementia of the Alzheimer's type: Missing
information. Aphasiology, 10(4), 395-408.
Gitlin, L. N., Winter, L., Dennis, M. P., Hodgson, N., & Hauck, W. W. (2010). Targeting and
managing behavioral symptoms in individuals with dementia: A randomized trial of a
nonpharmacological intervention. Journal of the American Geriatrics Society, 58(8),
1465-1474.
Gleason, J. B. (2005). THE DEVELOPMENT OF LANGUAGE, 6/e.
185
Goodglass, H., & Kaplan, E. (1983). Boston diagnostic aphasia examination booklet: Lea &
Febiger.
Gorno-Tempini, M., Hillis, A., Weintraub, S., Kertesz, A., Mendez, M., Cappa, S. e., . . . Boeve,
B. (2011). Classification of primary progressive aphasia and its variants. Neurology,
76(11), 1006-1014.
Gorsuch, R. L. (1997). Exploratory factor analysis: Its role in item analysis. Journal of
personality assessment, 68(3), 532-560.
Green-Harris, G., Houston, S., Skora, T., & Farrar-Edwards, D. (2016). CONNECTING THE
DOTS: MEETING THE DIAGNOSTIC AND TREATMENT NEEDS OF
UNDERSERVED URBAN AFRICAN AMERICAN ELDERS WITH MEMORY LOSS.
Alzheimer's & Dementia: The Journal of the Alzheimer's Association, 12(7), P793.
Grossman, M., D'Esposito, M., Hughes, E., Onishi, K., Biassou, N., White-Devine, T., &
Robinson, K. (1996). Language comprehension profiles in Alzheimer's disease, multi-
infarct dementia, and frontotemporal degeneration. Neurology, 47(1), 183-189.
Groves-Wright, K., Neils-Strunjas, J., Burnett, R., & O'Neill, M. J. (2004). A comparison of
verbal and written language in Alzheimer's disease. J Commun Disord, 37(2), 109-130.
doi:10.1016/j.jcomdis.2003.08.004
Halliday, M. A. K., & Hasan, R. (2014). Cohesion in english: Routledge.
Hart, D., Craig, D., Compton, S., Critchlow, S., Kerrigan, B., McIlroy, S., & Passmore, A.
(2003). A retrospective study of the behavioural and psychological symptoms of mid and
late phase Alzheimer's disease. Int J Geriatr Psychiatry, 18(11), 1037-1042.
Hartsuiker, R. J., & Kolk, H. H. (2001). Error monitoring in speech production: A computational
test of the perceptual loop theory. Cognitive psychology, 42(2), 113-157.
Hastie, T. (1992). Generalized additive models in Chambers, JM and TJ Hastie (eds), Statistical
models in S. Wadsworth and Brooks, Pacific Grove.
Henry, J. D., Crawford, J. R., & Phillips, L. H. (2004). Verbal fluency performance in dementia
of the Alzheimer’s type: a meta-analysis. Neuropsychologia, 42(9), 1212-1222.
Hier, D. B., Hagenlocker, K., & Shindler, A. G. (1985). Language disintegration in dementia:
effects of etiology and severity. Brain Lang, 25(1), 117-133.
186
Hoffmann, I., Nemeth, D., Dye, C. D., Pákáski, M., Irinyi, T., & Kálmán, J. (2010). Temporal
parameters of spontaneous speech in Alzheimer's disease. International journal of
speech-language pathology, 12(1), 29-34.
Hopper, T., Drefs, S. J., Bayles, K. A., Tomoeda, C. K., & Dinu, I. (2010). The effects of
modified spaced-retrieval training on learning and retention of face–name associations by
individuals with dementia. Neuropsychological Rehabilitation, 20(1), 81-102.
Hughes, D. L., McGillivray, L., & Schmidek, M. (1997). Guide to narrative language:
Procedures for assessment: Thinking Publications Eau Claire, WI.
Hunt, K. W. (1965). Grammatical Structures Written at Three Grade Levels. NCTE Research
Report No. 3.
Irish, M., Kamminga, J., Addis, D. R., Crain, S., Thornton, R., Hodges, J. R., & Piguet, O.
(2015). ‘Language of the past’–Exploring past tense disruption during autobiographical
narration in neurodegenerative disorders. Journal of neuropsychology.
Jack, C. R., Jr., Albert, M. S., Knopman, D. S., McKhann, G. M., Sperling, R. A., Carrillo, M.
C., . . . Phelps, C. H. (2011). Introduction to the recommendations from the National
Institute on Aging-Alzheimer's Association workgroups on diagnostic guidelines for
Alzheimer's disease. Alzheimers Dement, 7(3), 257-262. doi:10.1016/j.jalz.2011.03.004
Jack, C. R., Jr., Knopman, D. S., Jagust, W. J., Petersen, R. C., Weiner, M. W., Aisen, P. S., . . .
Trojanowski, J. Q. (2013). Tracking pathophysiological processes in Alzheimer's disease:
an updated hypothetical model of dynamic biomarkers. Lancet Neurol, 12(2), 207-216.
doi:10.1016/S1474-4422(12)70291-0
Johnson, S. C., La Rue, A., Hermann, B. P., Xu, G., Koscik, R. L., Jonaitis, E. M., . . . Sager, M.
A. (2011). The effect of TOMM40 poly-T length on gray matter volume and cognition in
middle-aged persons with APOE epsilon3/epsilon3 genotype. Alzheimers Dement, 7(4),
456-465. doi:10.1016/j.jalz.2010.11.012
Jöreskog, K. G., & Sörbom, D. (1986). LISREL VI: Analysis of linear structural relationships by
maximum likelihood, instrumental variables, and least squares methods: Scientific
Software.
Kaiser, H. F. (1960). The application of electronic computers to factor analysis. Educational and
Psychological Measurement, 20, 141-151. doi:10.1177/001316446002000116
Kave, G., & Goral, M. (2016). Word retrieval in picture descriptions produced by individuals
with Alzheimer's disease. Journal of Clinical and Experimental Neuropsychology, 38(9),
958-966. doi:10.1080/13803395.2016.1179266
187
Kavé, G., & Goral, M. (2016). Word retrieval in picture descriptions produced by individuals
with Alzheimer’s disease. Journal of Clinical and Experimental Neuropsychology, 38(9),
958-966.
Kave, G., & Levy, Y. (2003). Morphology in picture descriptions provided by persons with
Alzheimer's disease. J Speech Lang Hear Res, 46(2), 341-352.
Kavé, G., & Levy, Y. (2003). Morphology in picture descriptions provided by persons with
Alzheimer's disease. Journal of Speech, Language, and Hearing Research, 46(2), 341-
352.
Kemper, S., LaBarge, E., Ferraro, F. R., Cheung, H., Cheung, H., & Storandt, M. (1993). On the
preservation of syntax in Alzheimer's disease: Evidence from written sentences. Archives
of Neurology, 50(1), 81-86.
Kemper, S., Thompson, M., & Marquis, J. (2001). Longitudinal change in language production:
effects of aging and dementia on grammatical complexity and propositional content.
Psychology and aging, 16(4), 600.
Kertesz, A. (1982). Western aphasia battery test manual: Psychological Corp.
Kim, M., & Thompson, C. K. (2004). Verb deficits in Alzheimer’s disease and agrammatism:
Implications for lexical organization. Brain Lang, 88(1), 1-20.
König, A., Satt, A., Sorin, A., Hoory, R., Toledo-Ronen, O., Derreumaux, A., . . . Robert, P. H.
(2015). Automatic speech analysis for the assessment of patients with predementia and
Alzheimer's disease. Alzheimer's & Dementia: Diagnosis, Assessment & Disease
Monitoring, 1(1), 112-124.
Koscik, R. L., Berman, S. E., Clark, L. R., Mueller, K. D., Okonkwo, O. C., Gleason, C. E., . . .
Johnson, S. C. (2016). Intraindividual Cognitive Variability in Middle Age Predicts
Cognitive Impairment 8–10 Years Later: Results from the Wisconsin Registry for
Alzheimer’s Prevention. Journal of the International Neuropsychological Society,
22(10), 1016-1025.
Koscik, R. L., La Rue, A., Jonaitis, E. M., Okonkwo, O. C., Johnson, S. C., Bendlin, B. B., . . .
Sager, M. A. (2014). Emergence of mild cognitive impairment in late middle-aged adults
in the wisconsin registry for Alzheimer's prevention. Dement Geriatr Cogn Disord, 38(1-
2), 16-30. doi:10.1159/000355682
La Rue, A., Hermann, B., Jones, J. E., Johnson, S., Asthana, S., & Sager, M. A. (2008). Effect of
parental family history of Alzheimer's disease on serial position profiles. Alzheimers
Dement, 4(4), 285-290. doi:10.1016/j.jalz.2008.03.009
188
Lai, Y. H., Pai, H. H., & Lin, Y. T. (2009). To be semantically-impaired or to be syntactically-
impaired: Linguistic patterns in Chinese-speaking persons with or without dementia.
Journal of Neurolinguistics, 22(5), 465-475. doi:10.1016/j.jneuroling.2009.03.004
Laine, M., Laakso, M., Vuorinen, E., & Rinne, J. (1998). Coherence and informativeness of
discourse in two dementia types. Journal of Neurolinguistics, 11(1), 79-87.
Laird, N. M., & Ware, J. H. (1982). Random-Effects Models for Longitudinal Data. Biometrics,
38(4), 963-974. doi:10.2307/2529876
Laske, C., Sohrabi, H. R., Frost, S. M., López-de-Ipiña, K., Garrard, P., Buscema, M., . . .
O'Bryant, S. E. (2015). Innovative diagnostic tools for early detection of Alzheimer's
disease. Alzheimer's & Dementia, 11(5), 561-578.
doi:http://dx.doi.org/10.1016/j.jalz.2014.06.004
Le Dorze, G., & BÉDard, C. (1998). Effects of age and education on the lexico-semantic content
of connected speech in adults. J Commun Disord, 31(1), 53-71.
Le, X., Lancashire, I., Hirst, G., & Jokel, R. (2011). Longitudinal detection of dementia through
lexical and syntactic changes in writing: a case study of three British novelists. Literary
and Linguistic Computing, fqr013.
Lewin, C., Wolgers, G., & Herlitz, A. (2001). Sex differences favoring women in verbal but not
in visuospatial episodic memory. Neuropsychology, 15(2), 165.
Lira, J. O. d., Minett, T. S. C., Bertolucci, P. H. F., & Ortiz, K. Z. (2014). Analysis of word
number and content in discourse of patients with mild to moderate Alzheimer's disease.
Dementia & Neuropsychologia, 8(3), 260-265.
López-de-Ipiña, K., Alonso, J.-B., Travieso, C. M., Solé-Casals, J., Egiraun, H., Faundez-Zanuy,
M., . . . Martinez-Lage, P. (2013). On the selection of non-invasive methods based on
speech analysis oriented to automatic Alzheimer disease diagnosis. Sensors, 13(5), 6730-
6745.
MacDonald, M. C., Almor, A., Henderson, V. W., Kempler, D., & Andersen, E. S. (2001).
Assessing working memory and language comprehension in Alzheimer's disease. Brain
Lang, 78(1), 17-42.
MacWhinney, B. (2000). The CHILDES project: Tools for analyzing talk. 3rd Lawrence
Erlbaum Associates. Mahwah, NJ.
189
Macwhinney, B., Fromm, D., Forbes, M., & Holland, A. (2011). AphasiaBank: Methods for
Studying Discourse. Aphasiology, 25(11), 1286-1307.
doi:10.1080/02687038.2011.589893
Mahendra, N. (2001). Direct interventions for improving the performance of individuals with
Alzheimer's disease. Paper presented at the Semin Speech Lang.
March, E. G., Wales, R., & Pattison, P. (2006). The uses of nouns and deixis in discourse
production in Alzheimer's disease. Journal of Neurolinguistics, 19(4).
Martin, A., & Fedio, P. (1983). Word production and comprehension in Alzheimer's disease: The
breakdown of semantic knowledge. Brain Lang, 19(1), 124-141.
Masterson, J., Druks, J., Kopelman, M., Clare, L., Garley, C., & Hayes, M. (2007). Selective
Naming (and Comprehension) Deficits in Alzheimer's Disease? Cortex, 43(7), 921-934.
doi:http://doi.org/10.1016/S0010-9452(08)70691-9
McKhann, G., Drachman, D., Folstein, M., Katzman, R., Price, D., & Stadlan, E. M. (1984).
Clinical diagnosis of Alzheimer's disease Report of the NINCDS‐ADRDA Work Group*
under the auspices of Department of Health and Human Services Task Force on
Alzheimer's Disease. Neurology, 34(7), 939-939.
McKhann, G. M., Knopman, D. S., Chertkow, H., Hyman, B. T., Jack, C. R., Jr., Kawas, C. H., .
. . Phelps, C. H. (2011). The diagnosis of dementia due to Alzheimer's disease:
recommendations from the National Institute on Aging-Alzheimer's Association
workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimers Dement, 7(3),
263-269. doi:10.1016/j.jalz.2011.03.005
McNamara, P., Obler, L. K., Au, R., Durso, R., & Albert, M. L. (1992). Speech monitoring skills
in Alzheimer's disease, Parkinson's disease, and normal aging. Brain Lang, 42(1), 38-51.
Medina, L. D., Rodriguez-Agudelo, Y., Geschwind, D. H., Gilbert, P. E., Liang, L.-J.,
Cummings, J. L., & Ringman, J. M. (2011). Propositional density and apolipoprotein e
genotype among persons at risk for familial Alzheimer’s disease. Dementia and geriatric
cognitive disorders, 32(3), 188-192.
Moher, D., Liberati, A., Tetzlaff, J., Altman, D. G., & and the, P. G. (2009). Preferred reporting
items for systematic reviews and meta-analyses: The prisma statement. Annals of Internal
Medicine, 151(4), 264-269. doi:10.7326/0003-4819-151-4-200908180-00135
Mueller, K. D., Koscik, R. L., LaRue, A., Clark, L. R., Hermann, B., Johnson, S. C., & Sager, M.
A. (2015). Verbal Fluency and Early Memory Decline: Results from the Wisconsin
190
Registry for Alzheimer's Prevention. Arch Clin Neuropsychol, 30(5), 448-457.
doi:10.1093/arclin/acv030
Mueller, K. D., Koscik, R. L., Turkstra, L. S., Riedeman, S. K., Larue, A., Clark, L. R., . . .
Johnson, S. C. (2016). Connected Language in Late Middle-Aged Adults at Risk for
Alzheimer's Disease. Journal of Alzheimers Disease, 54(4), 1539-1550. doi:10.3233/jad-
160252
Mueller, K. D., Koscik, R. L., Turkstra, L. S., Riedeman, S. K., LaRue, A., Clark, L. R., . . .
Johnson, S. C. (2016). Connected Language in Late Middle-Aged Adults at Risk for
Alzheimer’s Disease. Journal of Alzheimer's Disease(Preprint), 1-12.
Murphy, K. J., Rich, J. B., & Troyer, A. K. (2006). Verbal fluency patterns in amnestic mild
cognitive impairment are characteristic of Alzheimer's type dementia. Journal of the
International Neuropsychological Society, 12(04), 570-574.
Murray, L. L. (2010). Distinguishing clinical depression from early alzheimer's disease in elderly
people: Can narrative analysis help? Aphasiology, 24(6-8), 928-939.
Nicholas, M., Obler, L. K., Albert, M. L., & Helm-Estabrooks, N. (1985). Empty speech in
Alzheimer's disease and fluent aphasia. J Speech Hear Res, 28(3), 405-410.
Nilsson, L. G. (2003). Memory function in normal aging. Acta Neurologica Scandinavica,
107(s179), 7-13.
Nutter-Upham, K. E., Saykin, A. J., Rabin, L. A., Roth, R. M., Wishart, H. A., Pare, N., &
Flashman, L. A. (2008). Verbal fluency performance in amnestic MCI and older adults
with cognitive complaints. Arch Clin Neuropsychol, 23(3), 229-241.
doi:10.1016/j.acn.2008.01.005
Oren, S., Willerton, C., & Small, J. (2014). Effects of Spaced Retrieval Training on Semantic
Memory in Alzheimer's Disease: A Systematic Review. Journal of Speech, Language,
and Hearing Research, 57(1), 247-270.
Papp, K. V., Mormino, E. C., Amariglio, R. E., Munro, C., Dagley, A., Schultz, A. P., . . . Rentz,
D. M. (2016). Biomarker validation of a decline in semantic processing in preclinical
Alzheimer’s disease. Neuropsychology, 30(5), 624.
Petersen, R. C., Smith, G. E., Waring, S. C., Ivnik, R. J., Tangalos, E. G., & Kokmen, E. (1999).
Mild cognitive impairment: clinical characterization and outcome. Archives of
Neurology, 56(3), 303-308.
191
Price, B. H., Gurvit, H., Weintraub, S., Geula, C., Leimkuhler, E., & Mesulam, M. (1993).
Neuropsychological patterns and language deficits in 20 consecutive cases of autopsy-
confirmed Alzheimer's disease. Archives of Neurology, 50(9), 931-937.
Price, S. E., Kinsella, G. J., Ong, B., Storey, E., Mullaly, E., Phillips, M., . . . Perre, D. (2012).
Semantic verbal fluency strategies in amnestic mild cognitive impairment.
Neuropsychology, 26(4), 490-497. doi:10.1037/a0028567
Racine, A. M., Koscik, R. L., Berman, S. E., Nicholas, C. R., Clark, L. R., Okonkwo, O. C., . . .
Johnson, S. C. (2016). Biomarker clusters are differentially associated with longitudinal
cognitive decline in late midlife. Brain, 139(Pt 8), 2261-2274. doi:10.1093/brain/aww142
Radloff, L. S. (1991). The use of the Center for Epidemiologic Studies Depression Scale in
adolescents and young adults. Journal of youth and adolescence, 20(2), 149-166.
Rao, J. K., Anderson, L. A., Inui, T. S., & Frankel, R. M. (2007). Communication interventions
make a difference in conversations between physicians and patients: a systematic review
of the evidence. Medical care, 45(4), 340-349.
Rentoumi, V., Raoufian, L., Ahmed, S., de Jager, C. A., & Garrard, P. (2014). Features and
machine learning classification of connected speech samples from patients with autopsy
proven Alzheimer's disease with and without additional vascular pathology. J Alzheimers
Dis, 42 Suppl 3, S3-17. doi:10.3233/JAD-140555
Rentoumi, V., Raoufian, L., Ahmed, S., de Jager, C. A., & Garrard, P. (2014). Features and
Machine Learning Classification of Connected Speech Samples from Patients with
Autopsy Proven Alzheimer's Disease with and without Additional Vascular Pathology.
Journal of Alzheimer's Disease, 42(s3).
Revelle, W. (2014). psych: Procedures for psychological, psychometric, and personality
research. Northwestern University, Evanston, Illinois, 165.
Revelle, W., & Rocklin, T. (1979). Very simple structure: An alternative procedure for
estimating the optimal number of interpretable factors. Multivariate behavioral research,
14(4), 403-414.
Riley, K. P., Snowdon, D. A., Desrosiers, M. F., & Markesbery, W. R. (2005). Early life
linguistic ability, late life cognitive function, and neuropathology: findings from the Nun
Study. Neurobiology of aging, 26(3), 341-347.
Ripich, D. N., Fritsch, T., Ziol, E., & Durand, E. (2000). Compensatory strategies in picture
description across severity levels in Alzheimer's disease: A longitudinal study. American
Journal of Alzheimer's Disease and Other Dementias, 15(4), 217-228.
192
Ripich, D. N., & Terrell, B. Y. (1988). Patterns of discourse cohesion and coherence in
Alzheimer's disease. J Speech Hear Disord, 53(1), 8-15.
Robinson, G., Rossor, M., & Cipolotti, L. (1999). Selective sparing of verb naming in a case of
severe Alzheimer's disease. Cortex, 35(3), 443-450.
Rosseel, Y. (2012). lavaan: An R package for structural equation modeling. Journal of Statistical
Software, 48(2), 1-36.
Saffran, E. M., Berndt, R. S., & Schwartz, M. F. (1989). The quantitative analysis of agrammatic
production: Procedure and data. Brain Lang, 37(3), 440-479.
Sager, M. A., Hermann, B., & La Rue, A. (2005). Middle-aged children of persons with
Alzheimer's disease: APOE genotypes and cognitive function in the Wisconsin Registry
for Alzheimer's Prevention. J Geriatr Psychiatry Neurol, 18(4), 245-249.
doi:10.1177/0891988705281882
Sajjadi, S. A., Patterson, K., Tomek, M., & Nestor, P. J. (2012). Abnormalities of connected
speech in semantic dementia vs Alzheimer's disease. Aphasiology, 26(6), 847-866.
Savundranayagam, M. Y., Hummert, M. L., & Montgomery, R. J. (2005). Investigating the
effects of communication problems on caregiver burden. The Journals of Gerontology
Series B: Psychological Sciences and Social Sciences, 60(1), S48-S55.
Savundranayagam, M. Y., & Orange, J. (2014). Matched and mismatched appraisals of the
effectiveness of communication strategies by family caregivers of persons with
Alzheimer's disease. International Journal of Language & Communication Disorders,
49(1), 49-59.
Semenza, C., & Cipolotti, L. (1989). Neuropsicologia con carta e matita. Padova: Cleup Editrice
Padova.
Shafto, M. A., Burke, D. M., Stamatakis, E. A., Tam, P. P., & Tyler, L. K. (2007). On the tip-of-
the-tongue: neural correlates of increased word-finding failures in normal aging. J Cogn
Neurosci, 19(12), 2060-2070.
Sherratt, S. (2007). Multi‐level discourse analysis: A feasible approach. Aphasiology, 21(3-4),
375-393.
Shimada, M., Meguro, K., Yamazaki, H., Horikawa, A., Hayasaka, C., Yamaguchi, S., . . .
Yamadori, A. (1998). Impaired verbal description ability assessed by the Picture
Description Task in Alzheimer's disease. Archives of Gerontology and Geriatrics, 27(1),
57-65.
193
Sitek, E. J., Kluj-Kozłowska, K., Barczak, A., Kozłowski, M., Wieczorek, D., Przewłócka, A., . .
. Sławek, J. (2015). Overlapping and distinguishing features of descriptive speech in
Richardson variant of progressive supranuclear palsy and non-fluent progressive aphasia.
Postępy Psychiatrii i Neurologii, 24(2), 62-67.
Small, S. A., Perera, G. M., DeLaPaz, R., Mayeux, R., & Stern, Y. (1999). Differential regional
dysfunction of the hippocampal formation among elderly with memory decline and
Alzheimer's disease. Annals of neurology, 45(4), 466-472.
Smith, S. R., Chenery, H. J., & Murdoch, B. E. (1989). Semantic abilities in dementia of the
Alzheimer type. II. Grammatical semantics. Brain Lang, 36(4), 533-542.
Snowdon, D. A., Kemper, S. J., Mortimer, J. A., Greiner, L. H., Wekstein, D. R., & Markesbery,
W. R. (1996). Linguistic ability in early life and cognitive function and Alzheimer's
disease in late life. Findings from the Nun Study. JAMA, 275(7), 528-532.
Snyder, P. J., Kahle-Wrobleski, K., Brannan, S., Miller, D. S., Schindler, R. J., DeSanti, S., . . .
Chandler, J. (2014). Assessing cognition and function in Alzheimer's disease clinical
trials: Do we have the right tools? Alzheimer's & Dementia, 10(6), 853-860.
Soldan, A., Pettigrew, C., Li, S., Wang, M. C., Moghekar, A., Selnes, O. A., . . . Team, B. R.
(2013). Relationship of cognitive reserve and cerebrospinal fluid biomarkers to the
emergence of clinical symptoms in preclinical Alzheimer's disease. Neurobiol Aging,
34(12), 2827-2834. doi:10.1016/j.neurobiolaging.2013.06.017
Sperling, R. A., Aisen, P. S., Beckett, L. A., Bennett, D. A., Craft, S., Fagan, A. M., . . . Montine,
T. J. (2011). Toward defining the preclinical stages of Alzheimer’s disease:
Recommendations from the National Institute on Aging-Alzheimer's Association
workgroups on diagnostic guidelines for Alzheimer's disease. Alzheimer's & Dementia,
7(3), 280-292.
Stronach, S. T., & Turkstra, L. S. (2008). Theory of mind and use of cognitive state terms by
adolescents with traumatic brain injury. Aphasiology, 22(10), 1054-1070.
Swinburn, K., Porter, G., & Howard, D. (2004). CAT: comprehensive aphasia test: Psychology
Press.
Tabachnick, B., & Fidell, L. S. (2001). Cleaning up your act: screening data prior to analysis.
Using multivariate statistics, 5, 61-116.
Taler, V., & Phillips, N. A. (2008). Language performance in Alzheimer's disease and mild
cognitive impairment: a comparative review. J Clin Exp Neuropsychol, 30(5), 501-556.
doi:10.1080/13803390701550128
194
Team, R. C. (2013). R: A language and environment for statistical computing.
Testa, J. A., Ivnik, R. J., Boeve, B., Petersen, R. C., Pankratz, V. S., Knopman, D., . . . Smith, G.
E. (2004). Confrontation naming does not add incremental diagnostic utility in MCI and
Alzheimer's disease. J Int Neuropsychol Soc, 10(4), 504-512.
doi:10.1017/S1355617704104177
Thompson, C. K., & Mack, J. E. (2014). Grammatical impairments in PPA. Aphasiology, 28(8-
9), 1018-1037.
Tomoeda, C. K., & Bayles, K. A. (1993). Longitudinal effects of Alzheimer disease on discourse
production. Alzheimer Dis Assoc Disord, 7(4), 223-236.
Tomoeda, C. K., & Bayles, K. A. (1993). Longitudinal effects of Alzheimer disease on discourse
production. Alzheimer Dis Assoc Disord.
Tomoeda, C. K., Bayles, K. A., Trosset, M. W., Azuma, T., & McGeagh, A. (1996). Cross-
sectional analysis of Alzheimer disease effects on oral discourse in a picture description
task. Alzheimer Dis Assoc Disord, 10(4), 204-215.
Tóth, L., Gosztolya, G., Vincze, V., Hoffmann, I., & Szatlóczki, G. (2015). Automatic detection
of mild cognitive impairment from spontaneous speech using ASR.
Turkstra, L. S. (2001). Partner effects in adolescent conversations. J Commun Disord, 34(1–2),
151-162. doi:http://dx.doi.org/10.1016/S0021-9924(00)00046-0
Ulatowska, H. K. (1985). The aging brain: Communication in the elderly: College-Hill.
Ulatowska, H. K., Allard, L., Donnell, A., Bristow, J., Haynes, S. M., Flower, A., & North, A. J.
(1988). [Use of discourse analysis for evaluation of the condition of patients with
dementia of the Alzheimer type]. Neurol Neurochir Pol, 22(1), 34-37.
Vaz, S., Falkmer, T., Passmore, A. E., Parsons, R., & Andreou, P. (2013). The case for using the
repeatability coefficient when calculating test–retest reliability. PLoS One, 8(9), e73990.
Venneri, A., Mitolo, M., & De Marco, M. (2016). Paradigm shift: semantic memory decline as a
biomarker of preclinical Alzheimer's disease. Biomark Med, 10(1), 5-8.
doi:10.2217/bmm.15.53
Vuorinen, E., Laine, M., & Rinne, J. (2000). Common pattern of language impairment in
vascular dementia and in Alzheimer disease. Alzheimer Dis Assoc Disord, 14(2), 81-86.
Wechsler, D. (1999). Wechsler abbreviated scale of intelligence: Psychological Corporation.

195
Welsh, K. A., Butters, N., Hughes, J. P., Mohs, R. C., & Heyman, A. (1992). Detection and
staging of dementia in Alzheimer's disease: Use of the neuropsychological measures
developed for the Consortium to Establish a Registry for Alzheimer's Disease. Archives
of Neurology, 49(5), 448-452.
Whitwell, J. L., Przybelski, S. A., Weigand, S. D., Knopman, D. S., Boeve, B. F., Petersen, R.
C., & Jack, J. C. R. (2007). 3D maps from multiple MRI illustrate changing atrophy
patterns as subjects progress from mild cognitive impairment to Alzheimer's disease.
Brain, 130(7), 1777-1786. doi:10.1093/brain/awm112
Wilkinson, G. S. (1993). WRAT-3: Wide range achievement test: Wide Range.
Willers, I. F., Feldman, M. L., & Allegri, R. F. (2008). Subclinical naming errors in mild
cognitive impairment. Demant Neuropsychol, 2, 217-222.
Wilson, S. M., Henry, M. L., Besbris, M., Ogar, J. M., Dronkers, N. F., Jarrold, W., . . . Gorno-
Tempini, M. L. (2010). Connected speech production in three variants of primary
progressive aphasia. Brain, 133(Pt 7), 2069-2088. doi:10.1093/brain/awq129
Woodward, M. (2013). Aspects of communication in Alzheimer's disease: clinical features and
treatment options. International Psychogeriatrics, 25(06), 877-885.
Xu, J., Murphy, S. L., Kochanek, K. D., & Arias, E. (2016). Mortality in the United States, 2015.
NCHS data brief(267), 1.
Yorkston, K. M., & Beukelman, D. R. (1980). An analysis of connected speech samples of
aphasic and normal speakers. Journal of speech and hearing disorders, 45(1), 27-36.
Zimmer, E. R., Leuzy, A., Benedet, A. L., Breitner, J., Gauthier, S., & Rosa-Neto, P. (2014).
Tracking neuroinflammation in Alzheimer's disease: the role of positron emission
tomography imaging. J Neuroinflammation, 11, 120. doi:10.1186/1742-2094-11-120
196
APPENDIX 1
Reasons to Participate in Alzheimer’s Research: Varying Perspectives of Participants
from The Wisconsin Registry for Alzheimer’s Prevention
Authors: Kimberly Diggle Mueller, Rebecca L. Koscik, Asenath LaRue, Erin McMullen
Jonaitis, Sarah Kate Riedeman, Bruce Hermann, Mark A. Sager
Presented at the Alzheimer’s Association International Conference (AAIC), Boston, MA, 2013
BACKGROUND:
Longitudinal studies are essential to developing effective Alzheimer’s Disease
interventions, yet participation requires long-term commitment. Evidence from several
longitudinal studies suggests varying reasons for participation in research, such as
societal/altruistic reasons (cite Jefferson, Lambe, et al. 2011) and personal benefit (cite
Ejiogu, 2011)
By investigating motivation for particular subgroups, recruitment and retention strategies
can be tailored more specifically to participant needs (cite Arean, 1996; cite Yancey et al
2006)
OBJECTIVE:
To identify themes for participating in longitudinal research provided by people enrolled
in the Wisconsin Registry for Alzheimer’s Prevention (WRAP) using qualitative content
analysis of speech sample narratives
To investigate whether themes varied across subgroups such as gender or AD family
history status
METHODS:
Participants: The Wisconsin Registry for Alzheimer’s Prevention (WRAP) is a longitudinal
study of a cohort (n > 1500) enriched with positive family history of AD (FH+). We used multi-
stage sampling to obtain a set of 32 speech samples that balanced representation across gender
(16 male, 16 female), FH status (15 FH+, 17 FH-) and site (19 Madison, 13 La Crosse).
Materials: At the third and fourth wave visits, participants are asked, “Why is being involved in
the WRAP study important to you?” Responses are digitally recorded.
Qualitative Analysis: Participant samples were transcribed and analyzed according to qualitative
research methods (Bogdan & Biklen, 1982; Corbin, J., & Strauss, A., 2008). Process notes were
recorded during the analysis and 24 categories emerged, which fell into three broad themes:
Personal, Family, and Societal. For each of the 32 speech samples, two independent coders
197
assigned yes/no ratings to the 19 identified categories. Inter-rater reliability was calculated at
91% agreement.
RESULTS:
19 content categories representing three broad themes emerged
o Personal (9 Categories)
o Family (3 Categories)
o Societal (7 Categories)
The median sample listed 3 reasons (range: 1-8) representing 2 of the 3 broad themes
56%, 19%, and 91%, respectively, cited at least one personal, family, and societal reason
for participating. We explored subgroup differences in reasons for participation. In the
small sample, no differences were statistically significant, but we observed the following
trends: FH+ participants in this subsample were no more likely than their FH-
counterparts to cite categories within the Family theme (20% vs.18%), and surprisingly, a
higher percentage of FH- participants cited a desire to help their own children or
grandchildren (18% vs 7%). A few specific categories within the Societal theme tended
to show up more often in FH- responses, such as an enjoyment of volunteering in general
(12% vs 0%) and the sense that “it feels like I am helping in my own way” (35% vs
13%).
More women listed at least one category within the Personal themes (69% vs 44%) and
fewer listed a Societal reason (81% vs 100%). More women than men expressed desire to
participate for their children or grandchildren (25% vs. 0%)
More Madison participants cited a desire to learn more about AD (21% vs 0%) or a sense
that AD is becoming a big social problem (21% vs 0%). These site differences were not
explained by education level.
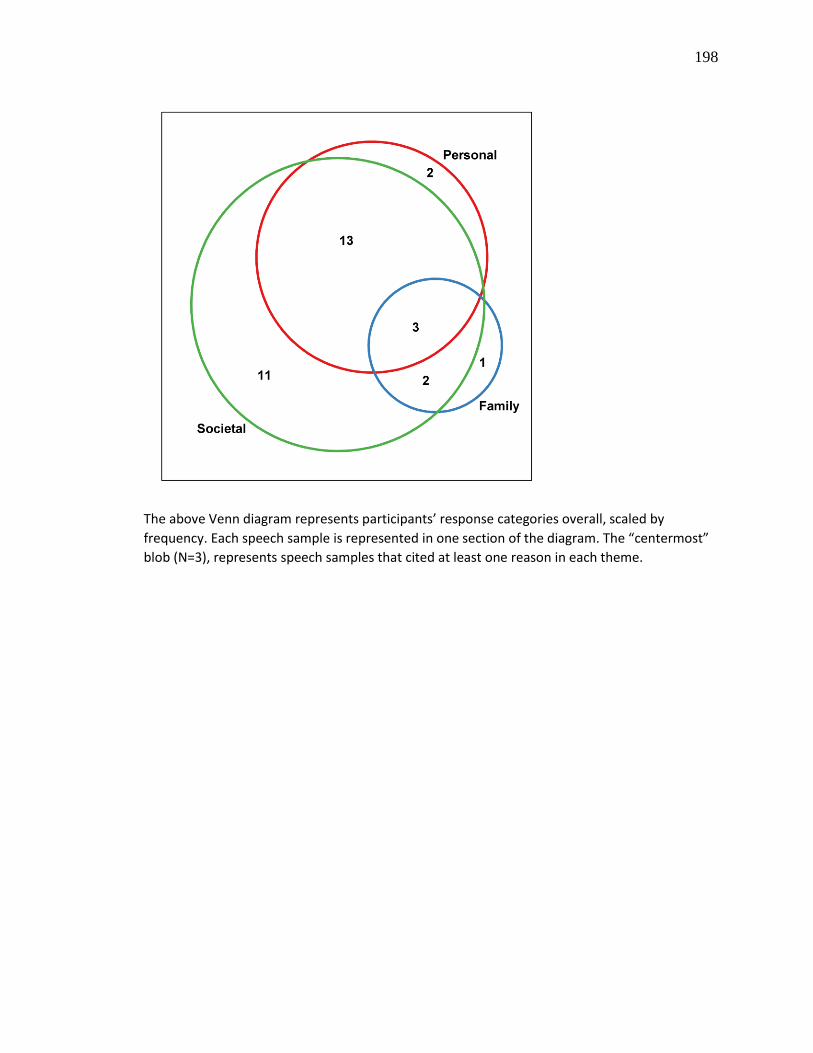
198
The above Venn diagram represents participants’ response categories overall, scaled by
frequency. Each speech sample is represented in one section of the diagram. The “centermost”
blob (N=3), represents speech samples that cited at least one reason in each theme.
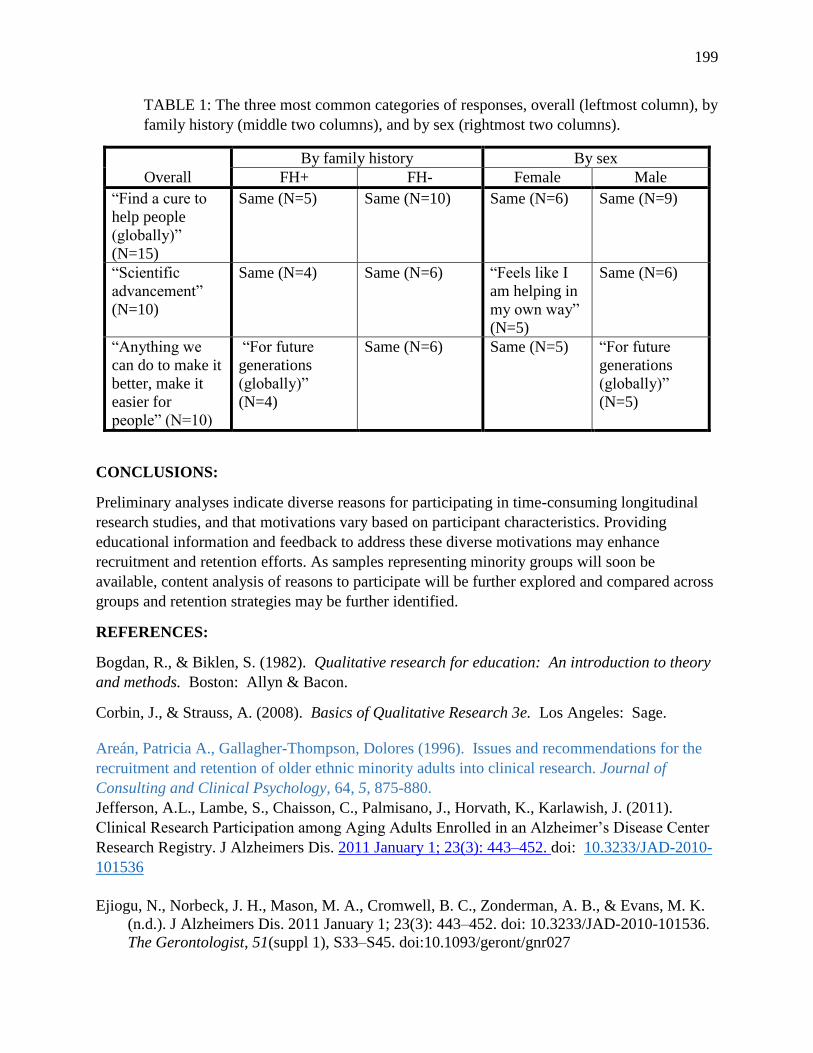
199
TABLE 1: The three most common categories of responses, overall (leftmost column), by
family history (middle two columns), and by sex (rightmost two columns).
Overall
By family history By sex
FH+ FH- Female Male
“Find a cure to
help people
(globally)”
(N=15)
Same (N=5) Same (N=10) Same (N=6) Same (N=9)
“Scientific
advancement”
(N=10)
Same (N=4) Same (N=6) “Feels like I
am helping in
my own way”
(N=5)
Same (N=6)
“Anything we
can do to make it
better, make it
easier for
people” (N=10)
“For future
generations
(globally)”
(N=4)
Same (N=6) Same (N=5) “For future
generations
(globally)”
(N=5)
CONCLUSIONS:
Preliminary analyses indicate diverse reasons for participating in time-consuming longitudinal
research studies, and that motivations vary based on participant characteristics. Providing
educational information and feedback to address these diverse motivations may enhance
recruitment and retention efforts. As samples representing minority groups will soon be
available, content analysis of reasons to participate will be further explored and compared across
groups and retention strategies may be further identified.
REFERENCES:
Bogdan, R., & Biklen, S. (1982). Qualitative research for education: An introduction to theory
and methods. Boston: Allyn & Bacon.
Corbin, J., & Strauss, A. (2008). Basics of Qualitative Research 3e. Los Angeles: Sage.
Areán, Patricia A., Gallagher-Thompson, Dolores (1996). Issues and recommendations for the
recruitment and retention of older ethnic minority adults into clinical research. Journal of
Consulting and Clinical Psychology, 64, 5, 875-880.
Jefferson, A.L., Lambe, S., Chaisson, C., Palmisano, J., Horvath, K., Karlawish, J. (2011).
Clinical Research Participation among Aging Adults Enrolled in an Alzheimer’s Disease Center
Research Registry. J Alzheimers Dis. 2011 January 1; 23(3): 443–452. doi: 10.3233/JAD-2010-
101536
Ejiogu, N., Norbeck, J. H., Mason, M. A., Cromwell, B. C., Zonderman, A. B., & Evans, M. K.
(n.d.). J Alzheimers Dis. 2011 January 1; 23(3): 443–452. doi: 10.3233/JAD-2010-101536.
The Gerontologist, 51(suppl 1), S33–S45. doi:10.1093/geront/gnr027
200
Yancey, A.K., Ortega, A.N., Kumanyika, S.K., (2006). Effective recruitment and retention of
minority research participants. Annual Review of Public Health, Vol. 27, 1-28.
N., Norbeck, J. H., Mason, M. A., Cromwell, B. C., Zonderman, A. B., & Evans, M. K. (2011).
Recruitment and Retention Strategies for Minority or Poor Clinical Research Participants:
Lessons From the Healthy Aging in Neighborhoods of Diversity Across the Life Span
Study. The Gerontologist , 51 (suppl 1 ), S33–S45. doi:10.1093/geront/gnr027
ACKNOWLEDGEMENTS:
We would like to thank our WRAP participants and WAI staff for their contributions to the
WRAP study. Without their efforts this research would not be possible. WRAP is supported by
NIA grant R01AG27161 (Wisconsin Registry for Alzheimer Prevention: Biomarkers of
Preclinical AD), Helen Bader Foundation, Northwestern Mutual Foundation, Extendicare
Foundation and State of Wisconsin.
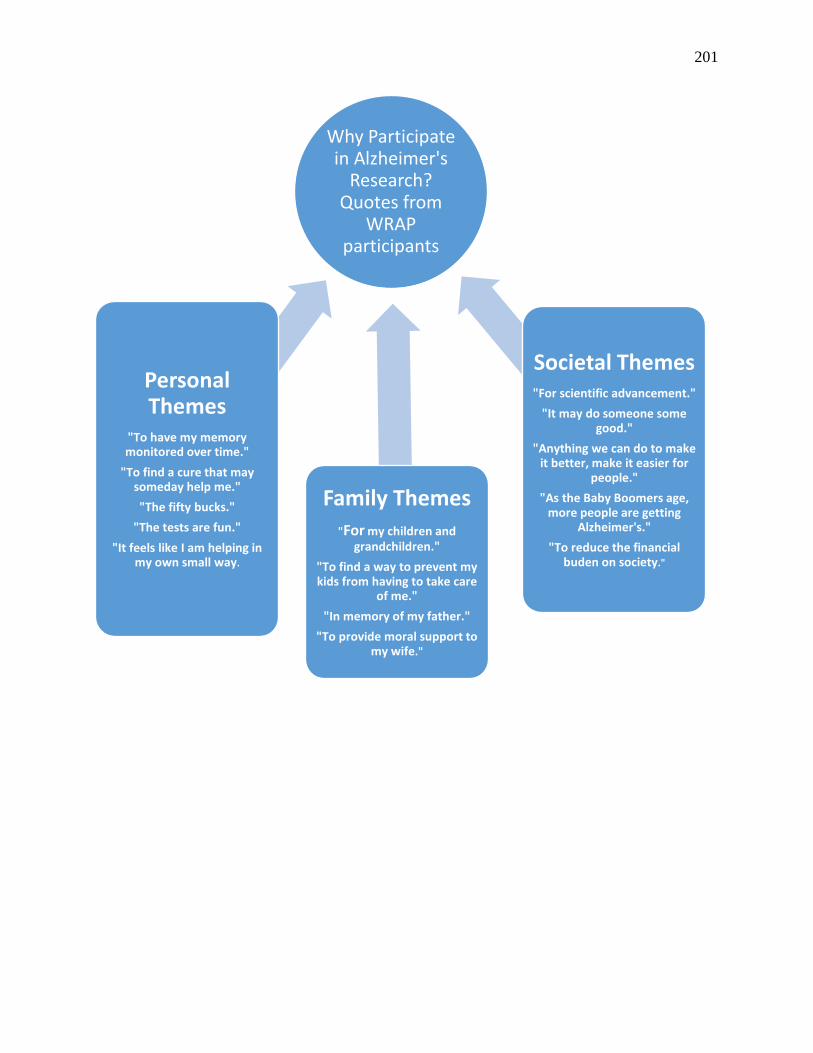
201
Why Participate in Alzheimer's
Research? Quotes from
WRAP participants
Personal Themes
"To have my memory monitored over time."
"To find a cure that may someday help me."
"The fifty bucks."
"The tests are fun."
"It feels like I am helping in my own small way.
Family Themes"For my children and
grandchildren."
"To find a way to prevent my kids from having to take care
of me."
"In memory of my father."
"To provide moral support to my wife."
Societal Themes"For scientific advancement."
"It may do someone some good."
"Anything we can do to make it better, make it easier for
people."
"As the Baby Boomers age, more people are getting
Alzheimer's."
"To reduce the financial buden on society."

202
APPENDIX 2
The Association Between Amyloid Burden and Language Outcomes in the Wisconsin
Registry for Alzheimer’s Prevention (WRAP)
Authors: Kimberly D. Mueller, MS, Rebecca L. Koscik, PhD, Sarah K. Riedeman, BS, Lyn
S. Turkstra, PhD, Jennifer M. Oh, Annie M. Racine, Bruce P. Hermann, PhD, Mark A.
Sager, MD, Bradley T. Christian, PhD, Sterling C. Johnson, PhD
Presented at the Alzheimer’s Association International Conference (AAIC) 2015, Washington,
D.C.
Background
The early diagnosis of Alzheimer’s Disease (AD) depends upon clinical manifestations of
difficulties with learning and memory which negatively impact activities of daily living1. Beta-
amyloid (1-42) (Aβ) accumulation may be a first major stage of preclinical AD2. Examination
of naturalistic connected language samples based on retrospective analysis and prospective
cohort studies have shown language deficits years or decades before diagnosis3,4,5,6. Given these
findings, we investigated whether rates of amyloid burden would be associated with language
outcomes from both standardized tests and non-standardized connected speech samples in a
healthy, at-risk cohort.
Objective
This study examined the relationship between rates Aβ deposition and 6 speech and language
variables in a group of late middle-aged participants at increased familial risk for AD.
Method
Sample: Participants were recruited from the Wisconsin Registry for Alzheimer’s Prevention
(WRAP), a longitudinal cohort (n>1500) enriched for positive family history of AD. The present
analyses included 158 right-handed WRAP participants (mean age=62 at speech sample; 66%
female; 41% APOE ɛ4+) who were native speakers of English.
Standardized Language Assessments: Standardized language outcomes were raw scores from
the Boston Naming Test (BNT)7, a category fluency test (animals), and a phonemic fluency task
(C,F,L from the COWAT8).
Experimental Language Outcomes: Content (Semantic Units6, 8), syntactic complexity (Verb
Index), and speech fluency (Maze Index) outcomes are described in Table 2 and were based on
verbal responses from a picture description task (“Cookie Theft” from the Boston Diagnostic
Aphasia Examination7). Responses were transcribed by a trained speech-language pathology
student using the CHAT/CLAN transcription program9. 10% of samples were re-transcribed by
a speech-language pathologist and inter-rater reliability was 94.3%. Prior to analyzing the

203
association between amyloid and speech, the maze index variable was transformed using a
square root transformation to make it normally distributed.
Imaging: Participants underwent a 70-minute dynamic [C-11]Pittsburgh compound B ([C-
11]PiB) positron emission tomography (PET) scan from which DVR maps were derived, and a
3.0 Tesla magnetic resonance imaging (MRI) scan. Based on Tomasi & Volkow (2012)10’s
classification of a language network using resting-state functional connectivity, we constructed a
global measure consisting of an average of left-hemisphere language network regions of interest
(ROI; “LngNtwk”), including areas from the inferior frontal network, middle frontal gyrus, and
inferior temporal and temporo-parietal areas.
Statistical Analyses: Primary regression analyses examined whether Aβ in the LngNtwk was a
significant predictor of each language outcome after adjusting for covariates of age at speech
sample, gender, APOE ɛ4 carrier status and literacy level. Secondary/exploratory analyses were
added examining whether gender moderated the effects of LngNtwk Aβ. Interaction plots depict
the simple intercepts and slope for LngNtwk Aβ for each gender after adjusting for other
covariates
Results
Sample characteristics are presented overall and by gender in Table 2. Men and women were
similar across most variables, except that men performed better on the BNT and worse on the
AVLT and Maze Index than women. Women had higher values of Aβ in LgNtwk than men (p =
.04).
Results from the ANCOVAs are presented in Table 3. Aβ accumulation in the language
network (LngNtwk) was not a significant predictor of any of the 6 language outcomes. Among
the covariates, age was a significant predictor only among the standardized language variables;
gender was a significant predictor of Semantic Units, Maze Index, and Boston Naming Test
scores; APOE ɛ4 was significantly associated with BNT; and literacy level was significantly
associated with Verb Index and BNT. Secondary analyses revealed that the association between
Aβ and language outcomes did not vary across gender except for marginal interaction effects
(p=.10) for Maze Index and Animal Naming. For Maze Index, higher amyloid was associated
with worse (higher) Maze Index scores in men while it had minimal effect in women. In contrast,
higher amyloid was associated with lower Animal Naming scores in women but not in men.
These relationships are depicted in Figures 1 and 2, respectively.
Conclusions
Within this relatively young and cognitively healthy cohort, we did not find a significant
relationship between Aβ deposition and any of the language outcomes despite having adequate
statistical power to detect relatively small effect sizes (e.g., 80% power to detect Cohen’s f2
effect size of .093). Given that 90% of the amyloid values were between .9 and 1.3, the lack of
significant association with speech outcomes could be due to the truncated range of amyloid in
the regions examined.
204
The finding that men produced more mazes than females is not a phenomenon explained by the
literature on normal disfluency rates between sexes.11,12.
The marginal interaction between gender and LngNtwk Aβ for some speech outcomes should be
re-examined as the group ages and greater ranges are observed in the variables. As connected
language draws upon multiple brain regions13, future directions include performing a voxelwise
analysis using the language variables, and examining the trajectory of Aβ deposition and these
standardized and experimental language outcomes over time.
Acknowledgements
We would like to thank study participants, Waisman Center and WAI staff, Caitlin Cleary and
Amy Hawley for their contributions. Without their efforts this research would not be possible.
This research was supported by NIA grants AG021155 (SCJ), AG027161 (SCJ), and P50
AG033514 (SA); by P50 HD03352, and by a Clinical and Translational Science Award
(UL1RR025011) to the University of Wisconsin, Madison. WRAP is supported by NIA grant
R01AG27161 (Wisconsin Registry for Alzheimer Prevention: Biomarkers of Preclinical AD),
Helen Bader Foundation, Northwestern Mutual Foundation, Extendicare Foundation and State of
Wisconsin. WRAP is also supported by the Clinical and Translational Science Award (CTSA)
program, through the NIH National Center for Advancing Translational Sciences (NCATS),
grant UL1TR000427. The content is solely the responsibility of the authors and does not
necessarily represent the official views of the NIH.
Kimberly Diggle Mueller, MS CCC-SLP, Wisconsin Alzheimer’s Institute, University of
Wisconsin School of Medicine & Public Health, Madison, Wisconsin USA
Phone: 608-829-3300 Email: [email protected] Web: www.wai.wisc.edu
References
1 DuBois et al., 2007
2 Sperling et al., 2011
3 Snowdon et al, 1996
4 Garrard et al 2005
5 Forbes-McKay & Venneri, 2005
6 Ahmed et al 2013
7 Goodglass & Kaplan, 2000
8 Benton et al., 1983

205
9 MacWhinney, 2000
10 Tomasi & Volkow, 2012
11 Bortfeld et al., 2001
12 Duchin & Mysak, 1987
13 Price, 2010
14Lezak et al., 2004

206
Semantic Content # Correct Semantic Units
(range 0 – 23)
Objects: cookie, stool, sink
Actions: washing, stealing, falling, overflowing
People: mother, boy, girl
Attitudes: mother unaware of children
Syntactic Complexity Total # verbs/ total # utterances
(range .375 – 4.40)
More Complex: “well I see two young children
attempting to raid the cookie jar which is a favorite
activity that I engaged in in my youth.
Less Complex: “he’s got a cookie in his left hand.
And he’s reaching with more with his right hand.
Mom’s wearing a dress.”
Speech Fluency Maze Index = sum of repetitions,
revisions, false starts, fillers/ total #
utterances (range 0 – 2.38)
Revision + filler + repetition:
“He uh the boy is reaching for a a cookie.”
TABLE 1. WRAP Language Variables from the “Cookie Theft” Picture Description Task1
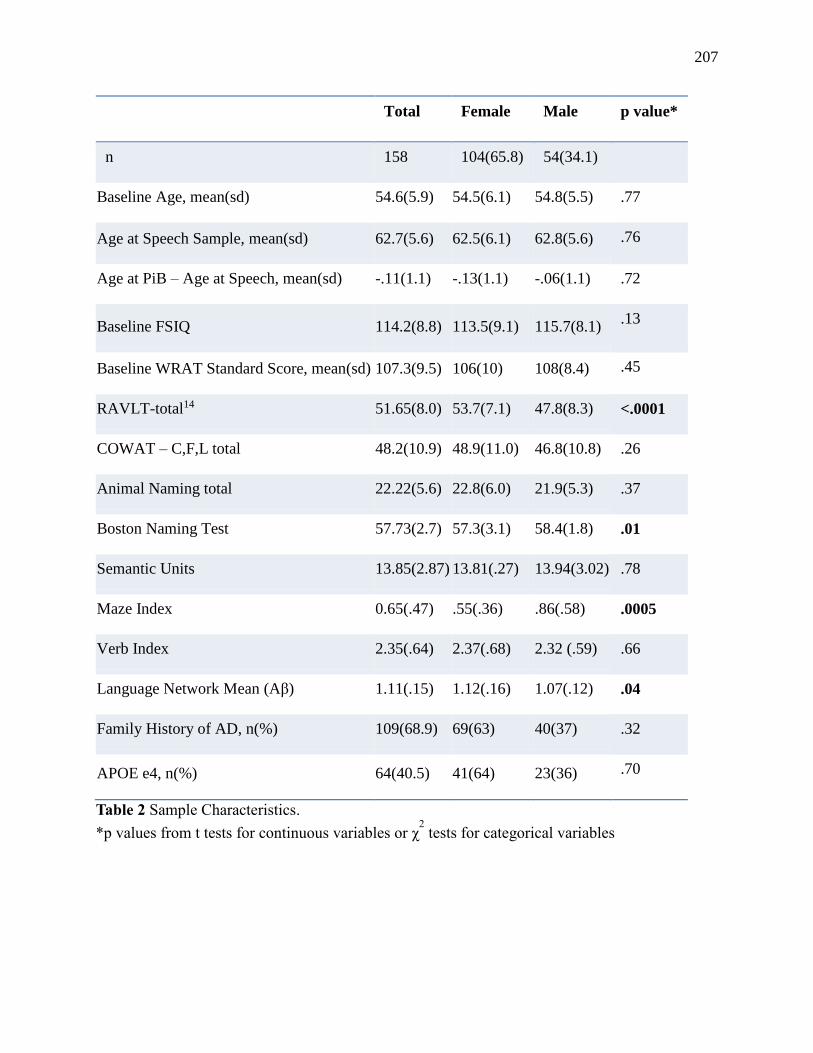
207
Total Female Male p value*
n 158 104(65.8) 54(34.1)
Baseline Age, mean(sd) 54.6(5.9) 54.5(6.1) 54.8(5.5) .77
Age at Speech Sample, mean(sd) 62.7(5.6) 62.5(6.1) 62.8(5.6) .76
Age at PiB – Age at Speech, mean(sd) -.11(1.1) -.13(1.1) -.06(1.1) .72
Baseline FSIQ 114.2(8.8) 113.5(9.1) 115.7(8.1) .13
Baseline WRAT Standard Score, mean(sd) 107.3(9.5) 106(10) 108(8.4) .45
RAVLT-total14 51.65(8.0) 53.7(7.1) 47.8(8.3) <.0001
COWAT – C,F,L total 48.2(10.9) 48.9(11.0) 46.8(10.8) .26
Animal Naming total 22.22(5.6) 22.8(6.0) 21.9(5.3) .37
Boston Naming Test 57.73(2.7) 57.3(3.1) 58.4(1.8) .01
Semantic Units 13.85(2.87) 13.81(.27) 13.94(3.02) .78
Maze Index 0.65(.47) .55(.36) .86(.58) .0005
Verb Index 2.35(.64) 2.37(.68) 2.32 (.59) .66
Language Network Mean (Aβ) 1.11(.15) 1.12(.16) 1.07(.12) .04
Family History of AD, n(%) 109(68.9) 69(63) 40(37) .32
APOE e4, n(%) 64(40.5) 41(64) 23(36) .70
Table 2 Sample Characteristics.
*p values from t tests for continuous variables or χ2 tests for categorical variables
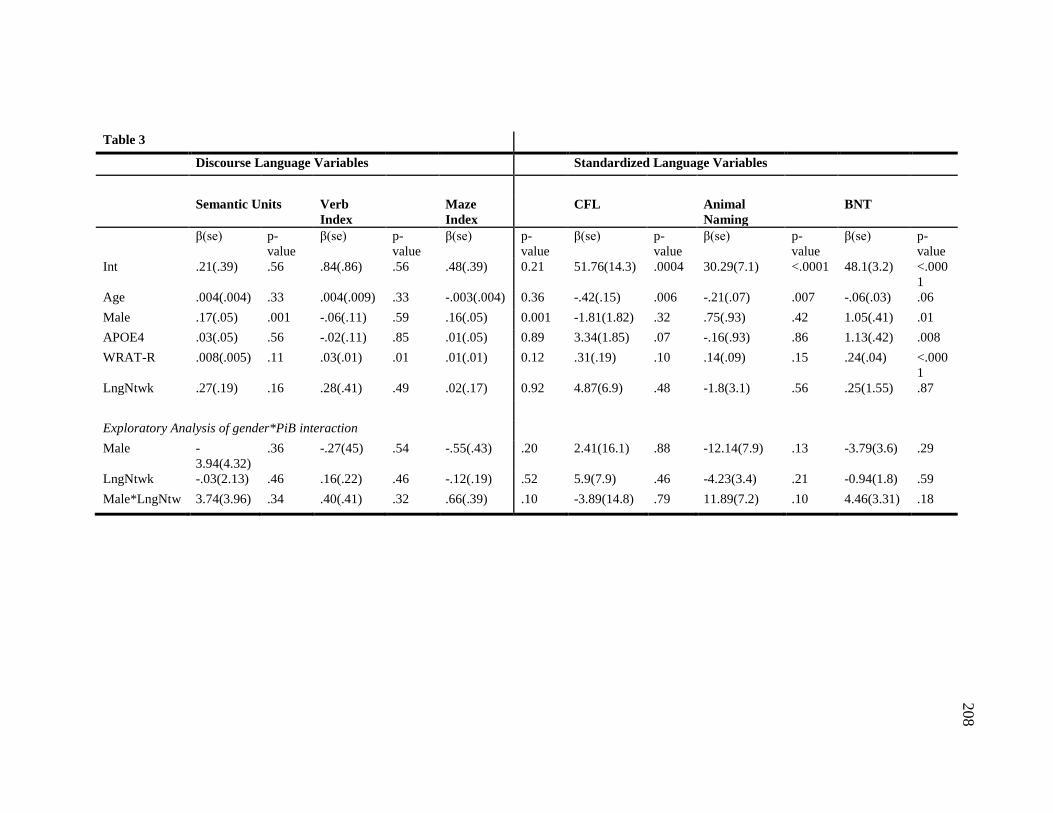
Table 3
Discourse Language Variables
Standardized Language Variables
Semantic Units Verb
Index
Maze
Index
CFL
Animal
Naming
BNT
β(se) p-
value
β(se) p-
value
β(se) p-
value
β(se) p-
value
β(se) p-
value
β(se) p-
value
Int .21(.39) .56 .84(.86) .56 .48(.39) 0.21 51.76(14.3) .0004 30.29(7.1) <.0001 48.1(3.2) <.000
1
Age .004(.004) .33 .004(.009) .33 -.003(.004) 0.36 -.42(.15) .006 -.21(.07) .007 -.06(.03) .06
Male .17(.05) .001 -.06(.11) .59 .16(.05) 0.001 -1.81(1.82) .32 .75(.93) .42 1.05(.41) .01
APOE4 .03(.05) .56 -.02(.11) .85 .01(.05) 0.89 3.34(1.85) .07 -.16(.93) .86 1.13(.42) .008
WRAT-R .008(.005) .11 .03(.01) .01 .01(.01) 0.12 .31(.19) .10 .14(.09) .15 .24(.04) <.000
1
LngNtwk .27(.19) .16 .28(.41) .49 .02(.17) 0.92 4.87(6.9) .48 -1.8(3.1) .56 .25(1.55) .87
Exploratory Analysis of gender*PiB interaction
Male -
3.94(4.32)
.36 -.27(45) .54 -.55(.43) .20 2.41(16.1) .88 -12.14(7.9) .13 -3.79(3.6) .29
LngNtwk -.03(2.13) .46 .16(.22) .46 -.12(.19) .52 5.9(7.9) .46 -4.23(3.4) .21 -0.94(1.8) .59
Male*LngNtw 3.74(3.96) .34 .40(.41) .32 .66(.39) .10 -3.89(14.8) .79 11.89(7.2) .10 4.46(3.31) .18
208
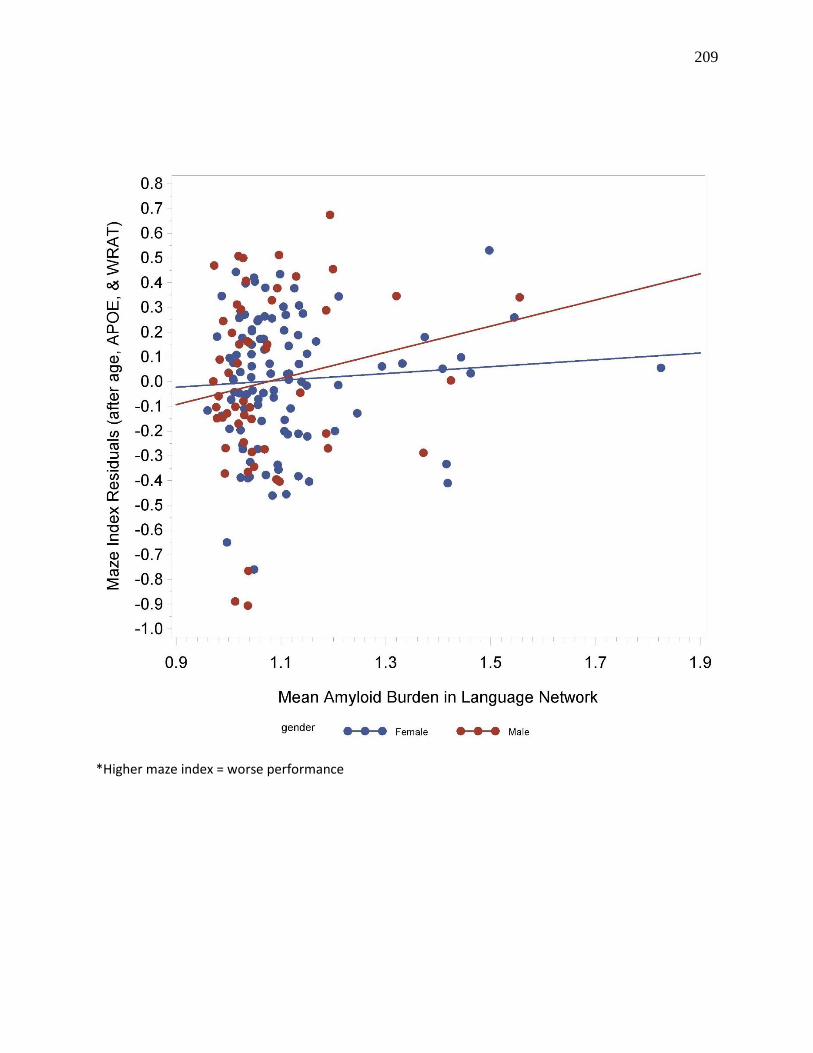
209
*Higher maze index = worse performance
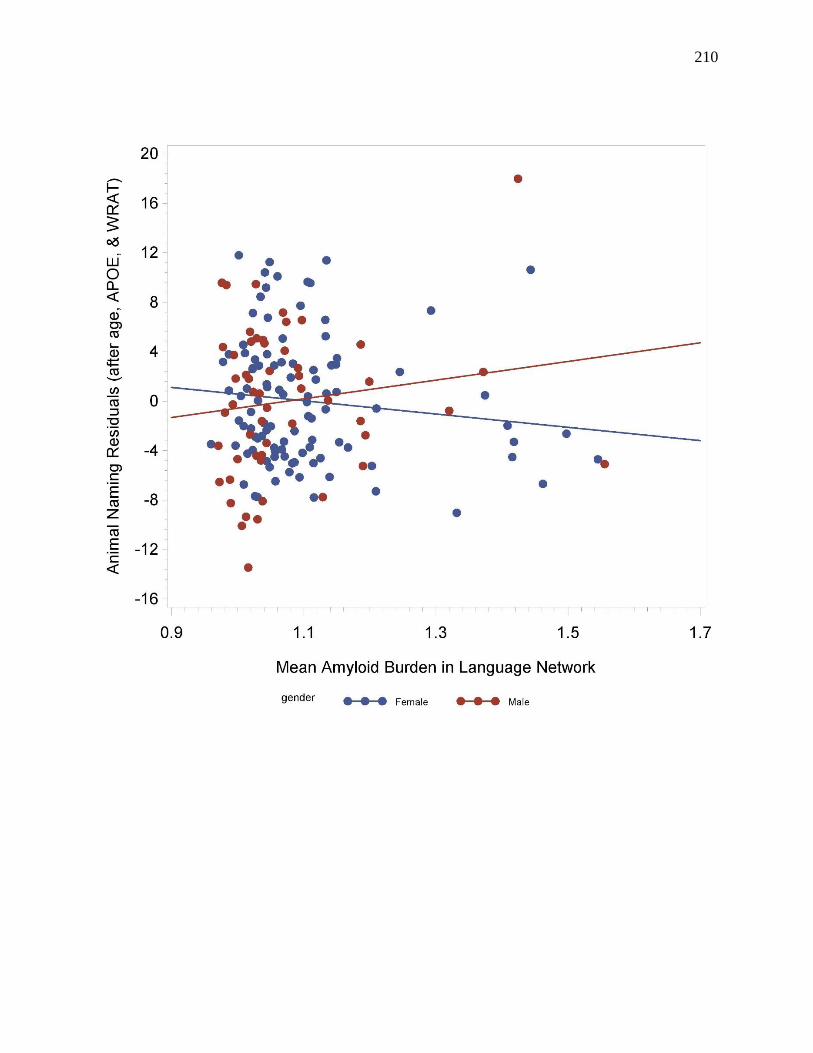
210
211
APPENDIX 3
Characteristics of Connected Language Subtypes in the Wisconsin Registry for
Alzheimer’s Prevention
Authors: Kimberly D. Mueller, MS a,c, Rebecca L. Koscik, PhD a, Lindsay R. Clark, PhD a,c,
Annie M. Racine, MAc,d,e, Sarah K. Riedeman, BSa,c, Lyn S. Turkstra, PhDc, Bruce P.
Hermann, PhDa,h, Sterling C. Johnsona,b,c,g
Abstract presented at the Alzheimer’s Association International Conference, AAIC, 2016
aWisconsin Alzheimer’s Institute, University of Wisconsin School of Medicine and Public
Health, USA, Madison, WI 53705
bGeriatric Research Education and Clinical Center, Wm. S. Middleton Veterans Hospital, USA,
Madison WI 53705.
cAlzheimer’s Disease Research Center, University of Wisconsin School of Medicine and Public
Health, USA, Madison, WI 53705
dInstitute on Aging, University of Wisconsin-Madison, USA, Madison, WI 53706
eNeuroscience & Public Policy Program, University of Wisconsin-Madison, USA, Madison, WI
53705
fDepartment of Communication Sciences and Disorders, University of Wisconsin College of
Letters and Science, USA, Madison, WI 53705
gWaisman Laboratory for Brain Imaging and Behavior, University of Wisconsin-Madison, USA,
Madison, WI 53705
hDepartment of Neurology, University of Wisconsin School of Medicine and Public Health,
USA, Madison, WI 53705
Background:
Although memory is mainly affected in Mild Cognitive Impairment (MCI) and
Alzheimer’s Disease (AD), language decline can also be observed.
Connected language examination is ecologically valid and may provide insights into
discourse production processes and how these may relate to early clinical AD subtypes.
No studies have examined connected discourse patterns in a late middle-aged sample
enriched for AD risk
212
Objectives:
Describe patterns of discourse performance in late middle-age using cluster analysis
Compare subgroups on clinical outcomes
Methods: Participants were from the Wisconsin Registry for Alzheimer's Prevention (WRAP),
mean(sd) age 64(6); 67% female, 37% APOE4+, 77% Family History of AD. Language samples
were transcribed for 268 participants who had completed a connected language task in which
they described the “Cookie Theft” picture from the Boston Diagnostic Aphasia Examination.
Transcriptions were analyzed for semantic content units, syntactic complexity, speech fluency
and lexical diversity (Table 1). Hierarchical cluster analysis of 4 variables with bivariate
correlations < .35 indicated a 6 cluster solution. Cluster characteristics were compared using
ANOVA, chi-square or ANCOVA (covariates age, sex, APOE4, and literacy).
Results: Participants were clustered into 6 language subtypes. We used interquartile ranges to
describe language performance measures as “low,” “medium,” and “high” (Table 2). The
weakest clusters, Clusters 1-3, contained low content measures; Cluster 2 was distinguished by a
high pronoun ratio and Cluster 3 by low syntactic complexity combined with moderate
disfluency. Cluster 4 is separated particularly by high disfluency. Clusters 5 and 6 showed
higher semantic content, but Cluster 5 had the lowest verb count. The demographics and clinical
characteristics of each subtype differed significantly on WRAT-reading and education (Table 3),
but not on depression, APOE-ε4 status, subjective language complaint, MMSE, nor family
history. Neuropsychological test performance differed significantly among the clusters for
Logical Memory delayed recall (p = .01), Boston Naming Test (p = .007), Animal Fluency (p =
.005), and marginally for Letter Fluency switches (p = .051; Tables 4, 5). Bonferroni-corrected
pairwise comparisons showed that Clusters 1, 2, and 5 had lower scores on some
neuropsychological measures (Fig 1).
Conclusions: Language performance subtypes were empirically derived by examining
spontaneous speech samples, and these subtypes were associated with neuropsychological test
scores of both language and memory. Identifying language phenotypes earlier may help to
identify people at higher risk of progressing to dementia.
Acknowledgements
We would like to thank WRAP participants and WAI staff for their contributions to the WRAP
study. Without their efforts this research would not be possible. This research is supported by
NIA grants R01AG27161 (Wisconsin Registry for Alzheimer Prevention: Biomarkers of
Preclinical AD) the Holland Postdoctoral Fund, Helen Bader Foundation, Northwestern Mutual
Foundation, Extendicare Foundation and State of Wisconsin. WRAP is also supported by the
Clinical and Translational Science Award (CTSA) program, through the NIH National Center for
Advancing Translational Sciences (NCATS), grant UL1TR000427. The content is solely the
responsibility of the authors and does not necessarily represent the official views of the NIH.
Kimberly D Mueller, MS
Associate Researcher, Wisconsin Alzheimer’s Institute
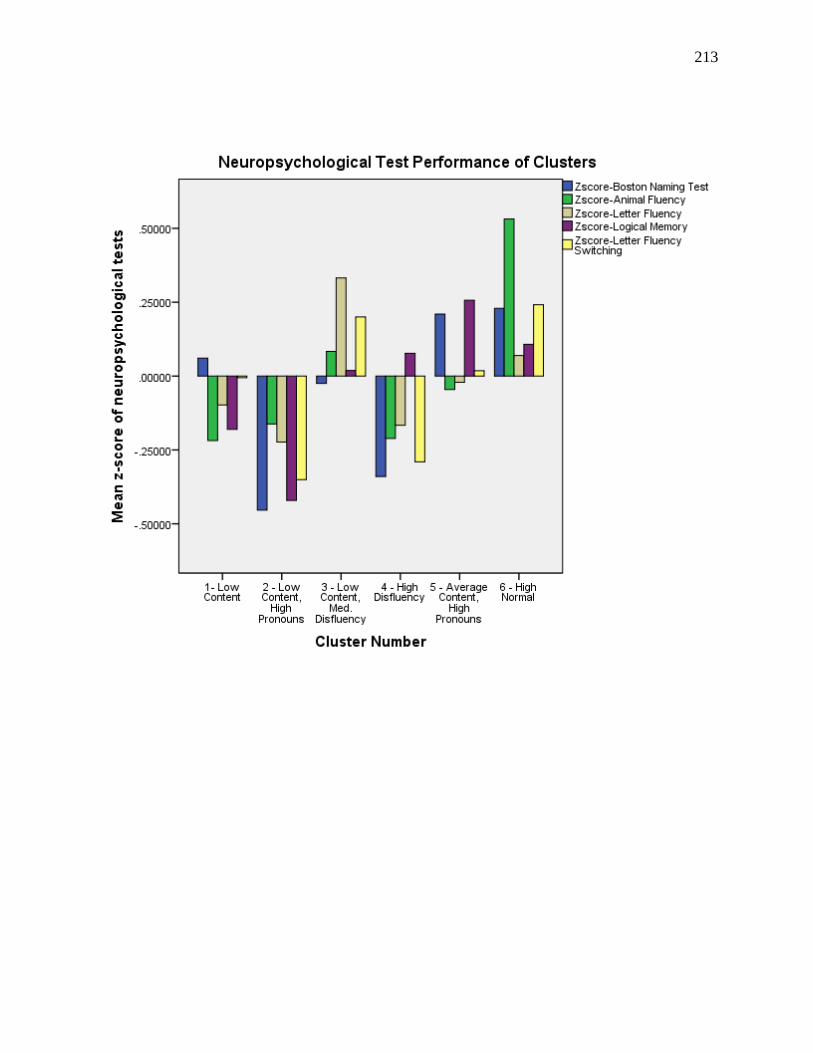
213
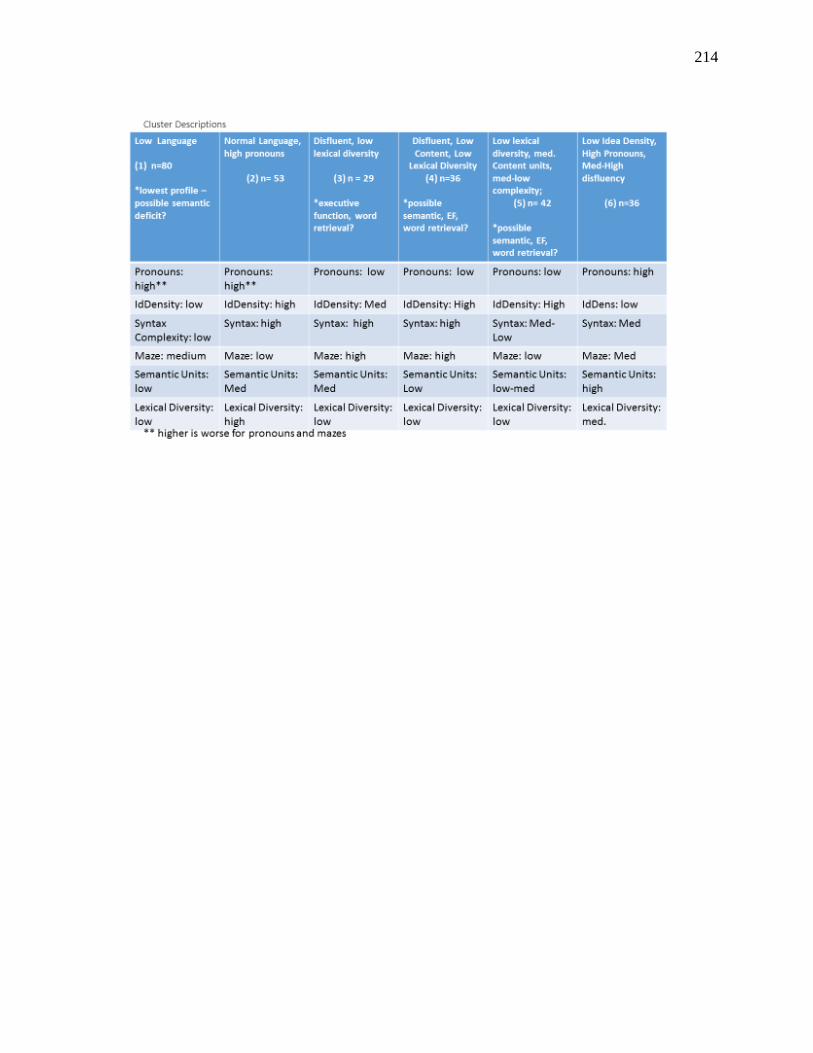
214
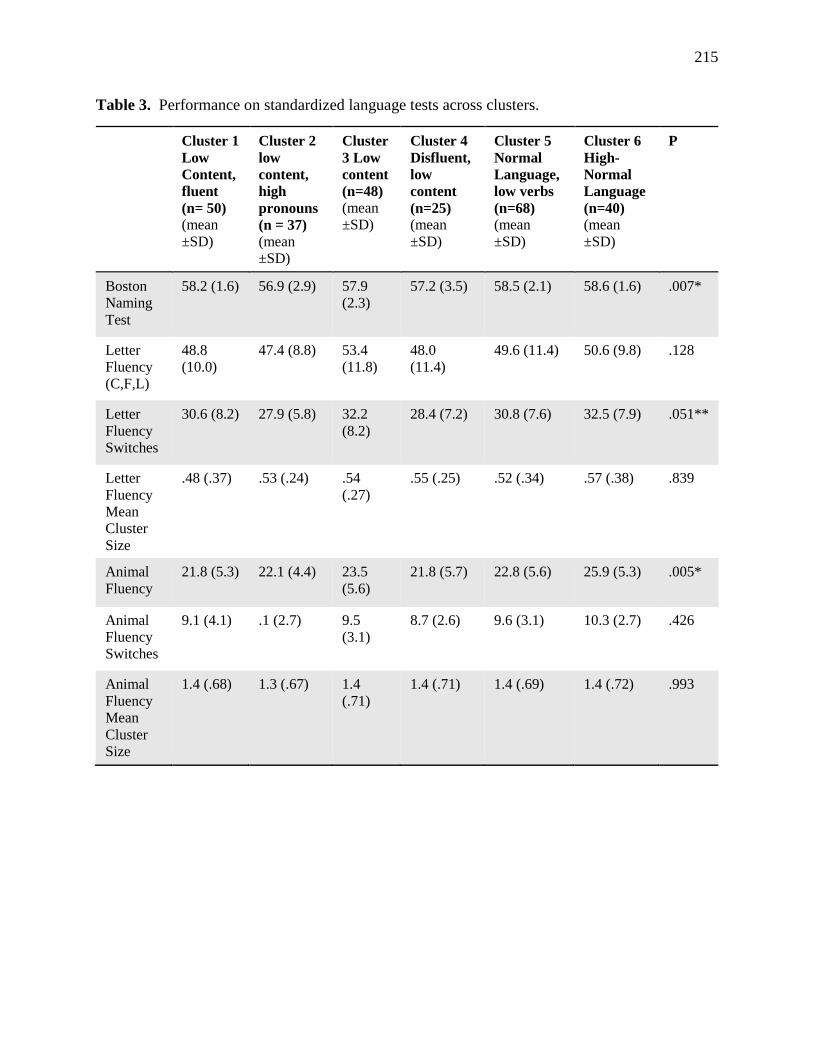
215
Table 3. Performance on standardized language tests across clusters.
Cluster 1
Low
Content,
fluent
(n= 50) (mean
±SD)
Cluster 2
low
content,
high
pronouns
(n = 37) (mean
±SD)
Cluster
3 Low
content
(n=48) (mean
±SD)
Cluster 4
Disfluent,
low
content
(n=25) (mean
±SD)
Cluster 5
Normal
Language,
low verbs
(n=68) (mean
±SD)
Cluster 6
High-
Normal
Language
(n=40) (mean
±SD)
P
Boston
Naming
Test
58.2 (1.6) 56.9 (2.9) 57.9
(2.3) 57.2 (3.5) 58.5 (2.1) 58.6 (1.6) .007*
Letter
Fluency
(C,F,L)
48.8
(10.0) 47.4 (8.8) 53.4
(11.8) 48.0
(11.4) 49.6 (11.4) 50.6 (9.8) .128
Letter
Fluency
Switches
30.6 (8.2) 27.9 (5.8) 32.2
(8.2) 28.4 (7.2) 30.8 (7.6) 32.5 (7.9) .051**
Letter
Fluency
Mean
Cluster
Size
.48 (.37) .53 (.24) .54
(.27) .55 (.25) .52 (.34) .57 (.38) .839
Animal
Fluency 21.8 (5.3) 22.1 (4.4) 23.5
(5.6) 21.8 (5.7) 22.8 (5.6) 25.9 (5.3) .005*
Animal
Fluency
Switches
9.1 (4.1) .1 (2.7) 9.5
(3.1) 8.7 (2.6) 9.6 (3.1) 10.3 (2.7) .426
Animal
Fluency
Mean
Cluster
Size
1.4 (.68) 1.3 (.67) 1.4
(.71) 1.4 (.71) 1.4 (.69) 1.4 (.72) .993
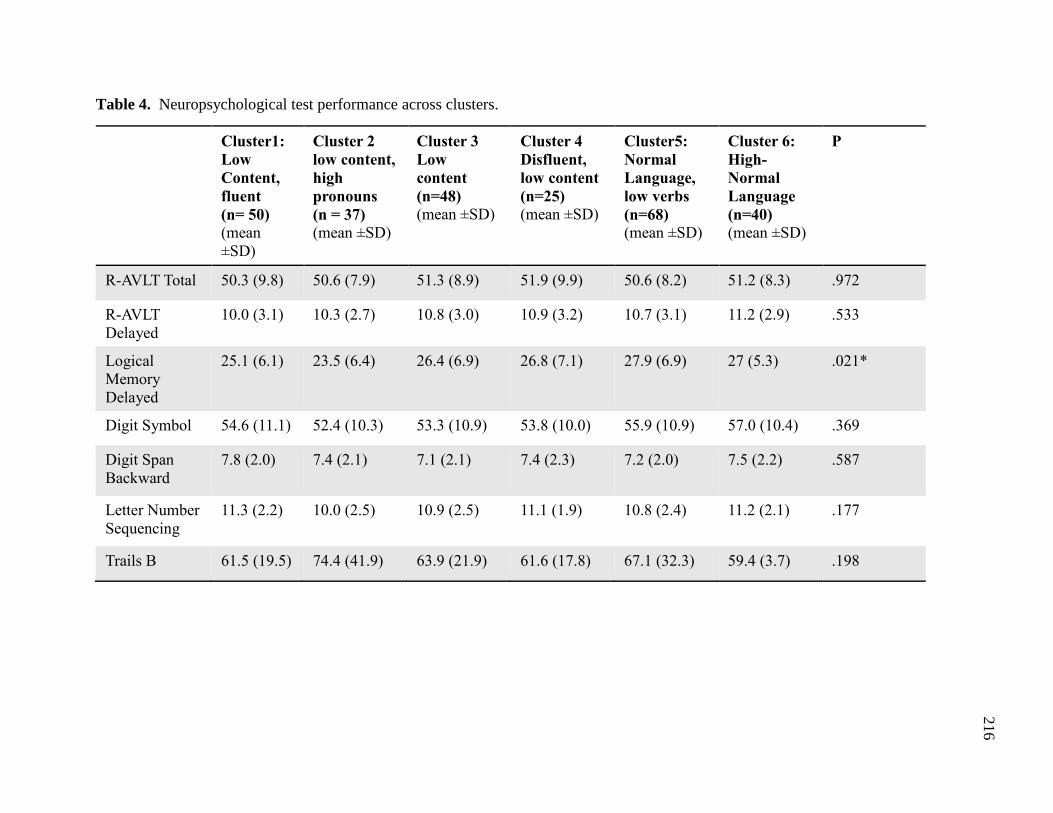
216
Table 4. Neuropsychological test performance across clusters.
Cluster1:
Low
Content,
fluent (n= 50) (mean
±SD)
Cluster 2 low content,
high
pronouns (n = 37) (mean ±SD)
Cluster 3 Low
content (n=48) (mean ±SD)
Cluster 4
Disfluent,
low content (n=25) (mean ±SD)
Cluster5:
Normal
Language,
low verbs (n=68) (mean ±SD)
Cluster 6:
High-
Normal
Language
(n=40) (mean ±SD)
P
R-AVLT Total 50.3 (9.8) 50.6 (7.9) 51.3 (8.9) 51.9 (9.9) 50.6 (8.2) 51.2 (8.3) .972
R-AVLT
Delayed 10.0 (3.1) 10.3 (2.7) 10.8 (3.0) 10.9 (3.2) 10.7 (3.1) 11.2 (2.9) .533
Logical
Memory
Delayed
25.1 (6.1) 23.5 (6.4) 26.4 (6.9) 26.8 (7.1) 27.9 (6.9) 27 (5.3) .021*
Digit Symbol 54.6 (11.1) 52.4 (10.3) 53.3 (10.9) 53.8 (10.0) 55.9 (10.9) 57.0 (10.4) .369
Digit Span
Backward 7.8 (2.0) 7.4 (2.1) 7.1 (2.1) 7.4 (2.3) 7.2 (2.0) 7.5 (2.2) .587
Letter Number
Sequencing 11.3 (2.2) 10.0 (2.5) 10.9 (2.5) 11.1 (1.9) 10.8 (2.4) 11.2 (2.1) .177
Trails B 61.5 (19.5) 74.4 (41.9) 63.9 (21.9) 61.6 (17.8) 67.1 (32.3) 59.4 (3.7) .198
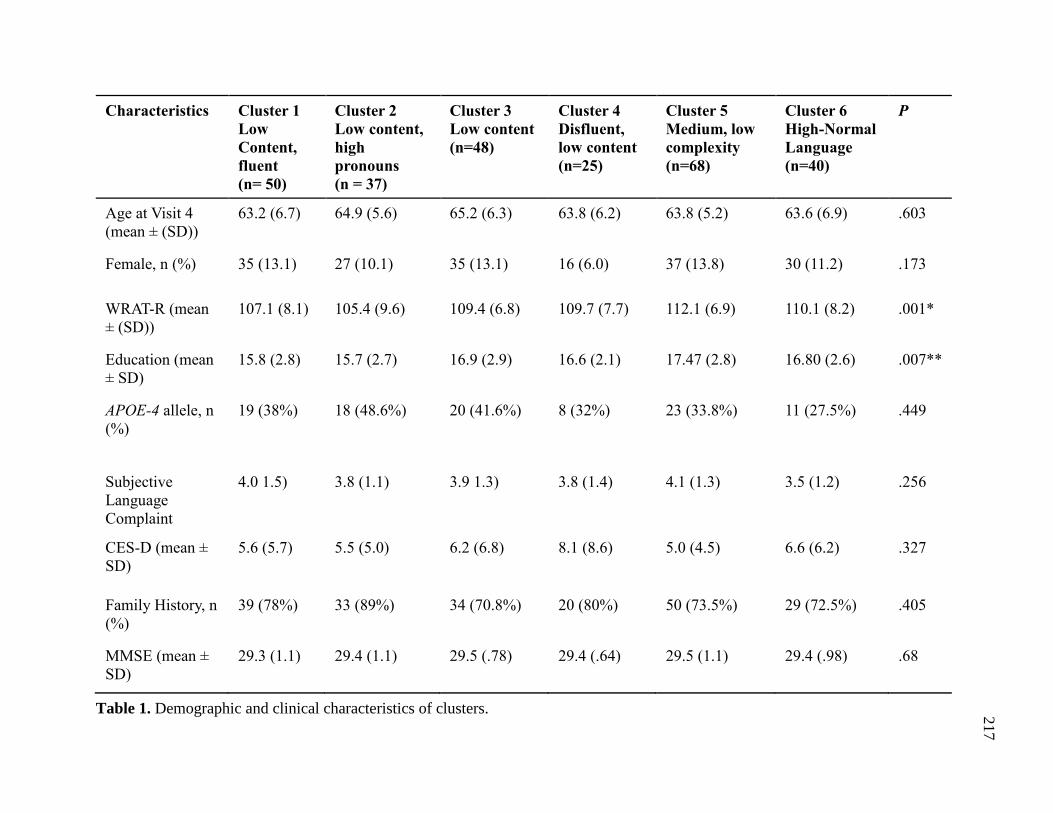
217
Characteristics Cluster 1 Low
Content,
fluent (n= 50)
Cluster 2 Low content,
high
pronouns (n = 37)
Cluster 3 Low content (n=48)
Cluster 4
Disfluent,
low content (n=25)
Cluster 5
Medium, low
complexity (n=68)
Cluster 6
High-Normal
Language
(n=40)
P
Age at Visit 4
(mean ± (SD)) 63.2 (6.7) 64.9 (5.6) 65.2 (6.3) 63.8 (6.2) 63.8 (5.2) 63.6 (6.9) .603
Female, n (%) 35 (13.1) 27 (10.1) 35 (13.1) 16 (6.0) 37 (13.8) 30 (11.2) .173
WRAT-R (mean
± (SD)) 107.1 (8.1) 105.4 (9.6) 109.4 (6.8) 109.7 (7.7) 112.1 (6.9) 110.1 (8.2) .001*
Education (mean
± SD) 15.8 (2.8) 15.7 (2.7) 16.9 (2.9) 16.6 (2.1) 17.47 (2.8) 16.80 (2.6) .007**
APOE-4 allele, n
(%) 19 (38%) 18 (48.6%) 20 (41.6%) 8 (32%) 23 (33.8%) 11 (27.5%) .449
Subjective
Language
Complaint
4.0 1.5) 3.8 (1.1) 3.9 1.3) 3.8 (1.4) 4.1 (1.3) 3.5 (1.2) .256
CES-D (mean ±
SD) 5.6 (5.7) 5.5 (5.0) 6.2 (6.8) 8.1 (8.6) 5.0 (4.5) 6.6 (6.2) .327
Family History, n
(%) 39 (78%) 33 (89%) 34 (70.8%) 20 (80%) 50 (73.5%) 29 (72.5%) .405
MMSE (mean ±
SD) 29.3 (1.1) 29.4 (1.1) 29.5 (.78) 29.4 (.64) 29.5 (1.1) 29.4 (.98) .68
Table 1. Demographic and clinical characteristics of clusters.









![Galantamine for Alzheimer's disease and mild cognitive impairment … · [Intervention Review] Galantamine for Alzheimer’s disease and mild cognitive impairment Clement Loy1, Lon](https://img.pdfslide.net/doc/110x75/5f171c96f6354220cc16d6f0/galantamine-for-alzheimers-disease-and-mild-cognitive-impairment-intervention.jpg)



















