-
8/7/2019 Conquest_Article_Health Insurance in India
1/6
Health Insurance in IndiaUnique challenges, opportunities and
strategies
Anurag Prasad
-
8/7/2019 Conquest_Article_Health Insurance in India
2/6
Gopal, a farmer in rural Orissa is contemplating suicide. Last
year, he borrowed a sum of 50
thousand rupees from a local moneylender for the treatment of
his young daughter. He is now
burdened with the interest payments so much so that he is not
even able to feed his family.
Ramesh, a software engineer is frustrated at his insurance
company. He had bought an insurance
policy two years ago. He now wants to undergo treatment at
Fortis hospital for a chronic lung
disease. He is unable to do so because his insurer had removed
Fortis from its network of
hospitals.
The above situations depict a sad but true story of the state of
healthcare industry in India. Few
months back, the group of public sector insurance companies -
National Insurance Co Ltd, New
India Assurance Co Ltd, Oriental Insurance Co Ltd and United
India Insurance Co Ltd stopped
providing cashless services to its policy-holders at some of the
biggest hospitals citing exorbitant
claim amounts and subsequent losses suffered as the reasons. The
hospitals in turn argued that
higher claim amounts are not because of their high prices. They
assert that the insurance policies
are more value based rather than ailment based and hence as a
result, the policy holders seek the
most expensive treatment even for smaller ailments. After a lot
of negotiations and pressure, the
hospitals came again in the network chain. However, the presence
of high claim ratios and
subsequent losses to insurers cannot be denied. Even the private
insurers who seem to be
profitable upfront have underneath their structures inherent
problems such as high premium
amounts, less customer satisfaction, inefficient administration
of claims, low penetration levels,
etc. that cannot be ignored. Despite the arrival of Third Party
Administrators (TPAs) for handling
the claims since the IRDA regulations regarding the same in
2001, the situation hasnt improved
much. Most of the insurance companies have suffered huge losses
due to high Income-Claim
Ratios (ICR).
The healthcare industry in India is already huge. Currently
standing at $34 billion and growing at
around 15%, it is expected to reach $40billion by 2012. Indias
thriving economy, rising medical
tourism, rapid urbanization, an expanding middle class
population with significant disposable
income and greater awareness towards the health are the
significant growth drivers in this
industry. Considering the huge market and the quality of
healthcare needed, it becomes
imperative to develop the existing infrastructure for healthcare
delivery and appropriate models
of health financing available in the country, which in light of
statistics present a grim picture.
-
8/7/2019 Conquest_Article_Health Insurance in India
3/6
Less than 15% Indians are covered under some form of health
financing and out-of-pocket
payments form the bulk of the healthcare expenditure. The poor,
who are generally not covered
under health insurance schemes often have to resort to buying at
exorbitant rates which they face
difficulty in repaying.
Tackling this grave problem needs a multi-pronged approach. The
sector is profitable provided
appropriate policies are in place and operations are efficient.
Insurance companies especially the
public sector ones who currently hold nearly 70% of the market
share, are often accused of being
un-innovative in bringing about newer products catering to
market needs. Most of the existing
insurance schemes such as Mediclaim are very generic in nature
and hence not meeting specific
needs of the people. As an example consider the case of youth in
urban areas and rural people.
They are unwilling to buy insurance as they perceive that they
are healthy and there is no need to
buy insurance. They are more concerned with savings and
investment. An insurance product that
combines insurance with savings or investment would be appealing
to them. Hence as a first
step, the insurance companies need to come up with product
portfolios that better reflect market
demands.
Another consideration during the product design should be cost
savings in the long run. An
example can be including the coverage of preventive healthcare
in the insurance scheme. It is a
well-known fact that many diseases such as diabetes when
diagnosed early can be treated
effectively but at later stages, the treatment costs spiral as a
result of other diseases that the
patient suffers because of diabetes. Therefore, it becomes
imperative for insurance companies to
offer preventive healthcare facilities and tie-up with network
hospitals to offer regular screenings
and check-ups for the policy-holders. These might increase
operational costs in the short run but
will result in significant reduction in claim amounts in the
longer run. Apart from the advantage
of savings, it will cover greater exposure to health-related
events and hence attract more number
of people towards insurance schemes.
The next consideration is minimizing operational costs and
reducing fraudulent activities.
Standardizing procedures and hospital charges has emerged as one
of the strategies for achieving
that. Presently there are no standard procedures to be followed
by all the hospitals. The hospitals
have the independence for framing the charges for the treatments
done. This leads to different
hospitals charging differently. This often gives scope for
unethical practices wherein the doctors
-
8/7/2019 Conquest_Article_Health Insurance in India
4/6
and patients collaborate in issuing fake medical certificates
and bills leading to losses for
insurers. The TPAs too find it difficult to provide a check
against these unethical practices
because of lack of standardized procedures.
Hence, achieving standardization is a must for
effective claim administration. The lead has
been taken by certain government initiatives
e.g. in Aarogyasari a public health care
initiative started by YSR Reddy in Andhra
Pradesh, a group of 30 doctors from
government and corporate came up with 389
surgical procedurescovering 144 diseases. The group of public
sector insurance companies alsohave realised the importance of
standardization and have standardized around 40 diseases and
procedures. The private insurance companies have also expressed
the desire to implement the
packaged rates determined by the public insurance companies.
Framing standardized procedures and practices would be
meaningless until they are implemented
and administered properly. In India, under the current system
the responsibility of effective
administration lies with the TPAs. But, the TPAs do not have any
incentive for effective
administration. Hence, there is a need for providing financial
incentives to TPAs. The incentive
structure should not be fee model, but it should be a sharing
model, where some portion of
costs saved should be given to the TPA. In 2002 GIPSA (an
association of four PSU insurers)
has suggested an incentive structure wherein the TPA would get
10 to 20 per cent of the amount
by which the incurred claim was reduced against last financial
year.
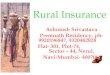
The current review process of TPAs also has certain inherent
faults. The figure alongside details
the steps adopted in the current procedure. As evident
from the figure, the current system does not have any
mechanism to detect fraudulent activities on the part of
the patient or the hospital. For example, a patient and
hospital can collaborate in the current system to get
high claims from the TPAs for minor or even in-fact no
actual treatment done. For dealing with such cases, a
-
8/7/2019 Conquest_Article_Health Insurance in India
5/6
methodology wherein there are checks in place at regular
intervals needs to be devised. Share
Microfin in collaboration with Medicare as TPA and United India
Insurance Company (UIIC) as
insurer in Nagpur has come up with an innovative procedure that
incorporates standardization,
TPA peer reviews and random visits to hospitals by TPAs
executive for detecting frauds. The
program has been a success and is now being implemented in many
other places.
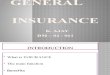
The procedure works in the following manner. When a patient
requires hospital treatment, he
goes to a network hospital and shows his ID card. The hospital
checks the ID card and fills a pre-
authorized form before starting treatment of the patient.
Pre-authorization form contains details
like presenting complaints, clinical
finding, line of treatment, past ailment
history, date of admission, approx.
duration of hospitalization, approx.
costs (with break-up) and signature of
treating doctor. The hospital faxes or
mails the pre-authorized form to the
TPA. The doctors employed by TPA do
a peer review of the form. If the TPA
has any question in the form, it contacts
the hospital. If TPA is satisfied with the
pre-authorization form, an agreement is
send to hospital. Moreover random visits to the hospital are
done by a client executive appointed
by the TPA to verify the details presented by the hospital
regarding the treatment in the pre-
authorization form. After the treatment is done, the hospital
sends the bills to the TPA. TPA
examines the bills thoroughly to ensure legitimacy of coverage,
treatment of protocol and correct
drug patterns usage. If the bills are found to be correct, the
TPA pays the hospital otherwise a
report is sent to the insurer. Finally, the insurer pays the
claim amount to the TPAs.
The final consideration for effective health financing is
increasing the reachability of the
insurance especially to the rural areas where the people who are
in dire need of health financing
live. Rural India, despite having enormous growth potential is
deprived of voluntary insurance
schemes. The rural people when in need of health financing often
have to resort to buying at
-
8/7/2019 Conquest_Article_Health Insurance in India
6/6
exorbitant rates which they find difficult to pay later. For
serving such a sector effectively, any
insurance scheme has to take into consideration the significant
challenges such as inability to pay
high premiums by the rural people, low awareness levels, lack of
distribution infrastructure, etc.
present in rural India. The companies need to understand that if
they can come up with suitable
business models to serve this sector, it can lead to huge
profits. In this respect, the micro
insurance scheme started by Bajaj Allianz in collaboration with
CARE India in the villages of
Tamilnadu in 2009 can be looked into. The basic premise of this
scheme is sharing of the
collected premium between the insurer and the community people
in a fix ratio (say 35:65). The
community itself does the claim administration and premium
collection. Low ticket value claims
are paid from the amount held by the community whereas higher
ticket value claims are paid by
the insurer. The policy cost less than 400 rupees per year.
The health insurance in India can be viewed as a problem worthy
of attack proving its worth by
hitting back. Despite the numerous efforts by government, IRDA
and the insurance companies, itis presenting unique challenges.
There is a need for all the stakeholders to collaborate and
come
up with unique initiatives so that this tremendously important
service can be delivered to the
needy in an efficient manner. The rewards are equally great as
it presents an opportunity of
universal acceptance after awareness is increased.