Embed Size (px)
Citation preview

Consensus or Controversy? Chronic Lymphocytic Leukemia and
Follicular LymphomaTuesday, June 29, 20215:00 PM – 6:00 PM ET
Nathan H Fowler, MDProf John G Gribben, MD, DSc, FMedSci
Brad S Kahl, MD
ModeratorNeil Love, MD
Faculty

Faculty
Nathan H Fowler, MDProfessor, Department of Lymphoma/MyelomaThe University of TexasMD Anderson Cancer CenterHouston, Texas
Brad S Kahl, MDProfessor of MedicineWashington University School of MedicineDirector, Lymphoma ProgramSiteman Cancer CenterSt Louis, Missouri
Prof John G Gribben, MD, DSc, FMedSciChair of Medical OncologyBarts Cancer InstituteQueen Mary University of LondonCharterhouse SquareLondon, United Kingdom

Commercial Support
This activity is supported by educational grants from AbbVie Inc, Adaptive Biotechnologies Corporation, AstraZeneca Pharmaceuticals LP, Bayer HealthCare Pharmaceuticals, Bristol-Myers Squibb Company, Genentech, a member of the Roche Group, GlaxoSmithKline, Incyte Corporation, Oncopeptides, Pharmacyclics LLC, an AbbVie Company and Janssen Biotech Inc, administered by Janssen Scientific Affairs LLC, Sanofi Genzyme, Seagen Inc, and Takeda Oncology.

Dr Love — Disclosures
Dr Love is president and CEO of Research To Practice. Research To Practice receives funds in the form of educational grants to develop CME activities from the following companies: AbbVie Inc, Adaptive Biotechnologies Corporation, Agios Pharmaceuticals Inc, Alexion Pharmaceuticals, Amgen Inc, Array BioPharma Inc, a subsidiary of Pfizer Inc, Astellas, AstraZeneca Pharmaceuticals LP, Aveo Pharmaceuticals, Bayer HealthCare Pharmaceuticals, BeiGene Ltd, Blueprint Medicines, Boehringer Ingelheim Pharmaceuticals Inc, Bristol-Myers Squibb Company, Celgene Corporation, Clovis Oncology, Daiichi Sankyo Inc, Eisai Inc, Epizyme Inc, Exact Sciences Inc, Exelixis Inc, Five Prime Therapeutics Inc, Foundation Medicine, Genentech, a member of the Roche Group, Gilead Sciences Inc, GlaxoSmithKline, Grail Inc, Halozyme Inc, Helsinn Healthcare SA, ImmunoGen Inc, Incyte Corporation, Ipsen Biopharmaceuticals Inc, Janssen Biotech Inc, administered by Janssen Scientific Affairs LLC, Jazz Pharmaceuticals Inc, KaryopharmTherapeutics, Kite, A Gilead Company, Lilly, Loxo Oncology Inc, a wholly owned subsidiary of Eli Lilly & Company, Merck, Novartis, Novocure Inc, Oncopeptides, Pfizer Inc, Pharmacyclics LLC, an AbbVie Company, Puma Biotechnology Inc, Regeneron Pharmaceuticals Inc, Sanofi Genzyme, Seagen Inc, Sumitomo Dainippon Pharma Oncology Inc, Taiho Oncology Inc, Takeda Oncology, Tesaro, A GSK Company, TG Therapeutics Inc, Turning Point Therapeutics Inc and Verastem Inc.

Research To Practice CME Planning Committee Members, Staff and Reviewers
Planners, scientific staff and independent reviewers for Research To Practice have no relevant conflicts of interest to disclose.

Dr Fowler — Disclosures
No relevant conflicts of interest to disclose.

Prof Gribben — Disclosures
Advisory CommitteeAbbVie Inc, AstraZeneca Pharmaceuticals LP, Bristol-Myers Squibb Company, Janssen Biotech Inc, Karyopharm Therapeutics, Kite, A Gilead Company, MorphoSys, Novartis
Consulting Agreements AstraZeneca Pharmaceuticals LP, Celgene Corporation, Janssen Biotech Inc
Data and Safety Monitoring Board/Committee
AstraZeneca Pharmaceuticals LP

Dr Kahl — Disclosures
Advisory Committee AstraZeneca Pharmaceuticals LP
Consulting AgreementsAbbVie Inc, Acerta Pharma — A member of the AstraZeneca Group, Genentech, a member of the Roche Group, Pharmacyclics LLC, an AbbVie Company, Roche Laboratories Inc, TG Therapeutics Inc
Contracted Research Acerta Pharma — A member of the AstraZeneca Group, BeiGene Ltd, Celgene Corporation, Genentech, a member of the Roche Group
Data and Safety Monitoring Board/Committee Celgene Corporation

We Encourage Clinicians in Practice to Submit Questions
Feel free to submit questions now before the program begins and throughout the program.

Familiarizing Yourself with the Zoom InterfaceHow to answer poll questions
When a poll question pops up, click your answer choice from the available options. Results will be shown after everyone has answered.

Familiarizing Yourself with the Zoom Interface
Expand chat submission box
Drag the white line above the submission box up to create more space for your message.

Familiarizing Yourself with the Zoom Interface
Increase chat font size
Press Command (for Mac) or Control (for PC) and the + symbol. You may do this as many times as you need for readability.


17 Exciting CME/MOC Events You Do Not Want to MissHER2-Positive Breast CancerTuesday, June 225:00 PM – 6:00 PM ETER-Positive and Triple-Negative Breast CancerWednesday, June 235:00 PM – 6:00 PM ETChronic Lymphocytic Leukemiaand Follicular Lymphoma
Tuesday, June 295:00 PM – 6:00 PM ET Multiple Myeloma Wednesday, June 305:00 PM – 6:00 PM ETOvarian CancerWednesday, July 75:00 PM – 6:00 PM ET
Chimeric Antigen Receptor T-Cell TherapyTuesday, July 135:00 PM – 6:00 PM ETAcute Myeloid Leukemia and Myelodysplastic SyndromesWednesday, July 145:00 PM – 6:00 PM ETMetastatic Castration-Resistant Prostate CancerTuesday, July 205:00 PM – 6:00 PM ETBladder CancerWednesday, July 215:00 PM – 6:00 PM ETEndometrial and Cervical CancersMonday, July 265:00 PM – 6:00 PM ET
Immunotherapy and Other Nontargeted Approaches for Lung CancerWednesday, July 285:00 PM – 6:00 PM ET
A Live Webinar Series Held in Conjunction with the 2021 ASCO Annual Meeting
Colorectal and Gastroesophageal CancersTuesday, August 35:00 PM – 6:30 PM ET
Hepatocellular Carcinoma and Pancreatic CancerWednesday, August 45:00 PM – 6:30 PM ET
Head and Neck CancerWednesday, August 115:00 PM – 6:00 PM ET
Hormonal Therapy for Prostate CancerMonday, July 125:00 PM – 6:00 PM ET
Targeted Therapy for Non-Small Cell Lung CancerTuesday, July 275:00 PM – 6:00 PM ET
Mantle Cell, Diffuse Large B-Cell and Hodgkin LymphomaMonday, August 25:00 PM – 6:00 PM ET

Consensus or Controversy? Multiple Myeloma
Wednesday, June 30, 20215:00 PM – 6:00 PM ET
Natalie S Callander, MDShaji K Kumar, MDSagar Lonial, MD
ModeratorNeil Love, MD
Faculty

Ask the Expert: Clinical Investigators Provide Perspectives on the Management
of Renal Cell Carcinoma In Partnership with Project Echo® and Florida Cancer Specialists
Tuesday, July 6, 20215:00 PM – 6:00 PM ET
David I Quinn, MBBS, PhD
ModeratorNeil Love, MD
Faculty

A Conversation with the Investigators: Ovarian Cancer Wednesday, July 7, 2021
5:00 PM – 6:00 PM ET
Michael J Birrer, MD, PhDKathleen Moore, MD
Richard T Penson, MD, MRCP
ModeratorNeil Love, MD
Faculty

A Conversation with the Investigators: Hormonal Therapy for Prostate Cancer
Monday, July 12, 20215:00 PM – 6:00 PM ET
Simon Chowdhury, MD, PhDTanya B Dorff, MD
Matthew R Smith, MD, PhD
ModeratorNeil Love, MD
Faculty

A Conversation with the Investigators: Chimeric Antigen Receptor T-Cell Therapy in Hematologic Cancers
Tuesday, July 13, 20215:00 PM – 6:00 PM ET
Caron Jacobson, MDDavid G Maloney, MD, PhD
Nikhil C Munshi, MD
ModeratorNeil Love, MD
Faculty

A Conversation with the Investigators: Acute Myeloid Leukemia and Myelodysplastic Syndromes
Wednesday, July 14, 20215:00 PM – 6:00 PM ET
Courtney D DiNardo, MD, MSCEGail J Roboz, MD
Eytan M Stein, MD
ModeratorNeil Love, MD
Faculty

Consensus or Controversy? Clinical Investigator Perspectives on the
Current and Future Management of Mantle Cell, Diffuse Large B-Cell and Hodgkin Lymphoma
Monday, August 2, 20215:00 PM – 6:00 PM ET
Stephen M Ansell, MD, PhDCraig Moskowitz, MD
Laurie H Sehn MD, MPH
ModeratorNeil Love, MD
Faculty

Thank you for joining us!
CME and MOC credit information will be emailed to each participant within 24 hours.

Consensus or Controversy? Chronic Lymphocytic Leukemia and
Follicular LymphomaTuesday, June 29, 20215:00 PM – 6:00 PM ET
Nathan H Fowler, MDProf John G Gribben, MD, DSc, FMedSci
Brad S Kahl, MD
ModeratorNeil Love, MD
Faculty

Faculty
Nathan H Fowler, MDProfessor, Department of Lymphoma/MyelomaThe University of TexasMD Anderson Cancer CenterHouston, Texas
Brad S Kahl, MDProfessor of MedicineWashington University School of MedicineDirector, Lymphoma ProgramSiteman Cancer CenterSt Louis, Missouri
Prof John G Gribben, MD, DSc, FMedSciChair of Medical OncologyBarts Cancer InstituteQueen Mary University of LondonCharterhouse SquareLondon, United Kingdom

Consensus or Controversy Consulting Investigators
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

Consensus or Controversy Consulting Investigators
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

We Encourage Clinicians in Practice to Submit Questions
Feel free to submit questions now before the program begins and throughout the program.

Familiarizing Yourself with the Zoom InterfaceHow to answer poll questions
When a poll question pops up, click your answer choice from the available options. Results will be shown after everyone has answered.


17 Exciting CME/MOC Events You Do Not Want to MissHER2-Positive Breast CancerTuesday, June 225:00 PM – 6:00 PM ETER-Positive and Triple-Negative Breast CancerWednesday, June 235:00 PM – 6:00 PM ETChronic Lymphocytic Leukemiaand Follicular Lymphoma
Tuesday, June 295:00 PM – 6:00 PM ET Multiple Myeloma Wednesday, June 305:00 PM – 6:00 PM ETOvarian CancerWednesday, July 75:00 PM – 6:00 PM ET
Chimeric Antigen Receptor T-Cell TherapyTuesday, July 135:00 PM – 6:00 PM ETAcute Myeloid Leukemia and Myelodysplastic SyndromesWednesday, July 145:00 PM – 6:00 PM ETMetastatic Castration-Resistant Prostate CancerTuesday, July 205:00 PM – 6:00 PM ETBladder CancerWednesday, July 215:00 PM – 6:00 PM ETEndometrial and Cervical CancersMonday, July 265:00 PM – 6:00 PM ET
Immunotherapy and Other Nontargeted Approaches for Lung CancerWednesday, July 285:00 PM – 6:00 PM ET
A Live Webinar Series Held in Conjunction with the 2021 ASCO Annual Meeting
Colorectal and Gastroesophageal CancersTuesday, August 35:00 PM – 6:30 PM ET
Hepatocellular Carcinoma and Pancreatic CancerWednesday, August 45:00 PM – 6:30 PM ET
Head and Neck CancerWednesday, August 115:00 PM – 6:00 PM ET
Hormonal Therapy for Prostate CancerMonday, July 125:00 PM – 6:00 PM ET
Targeted Therapy for Non-Small Cell Lung CancerTuesday, July 275:00 PM – 6:00 PM ET
Mantle Cell, Diffuse Large B-Cell and Hodgkin LymphomaMonday, August 25:00 PM – 6:00 PM ET

Consensus or Controversy? Multiple Myeloma
Wednesday, June 30, 20215:00 PM – 6:00 PM ET
Natalie S Callander, MDShaji K Kumar, MDSagar Lonial, MD
ModeratorNeil Love, MD
Faculty

Ask the Expert: Clinical Investigators Provide Perspectives on the Management
of Renal Cell Carcinoma In Partnership with Project Echo® and Florida Cancer Specialists
Tuesday, July 6, 20215:00 PM – 6:00 PM ET
David I Quinn, MBBS, PhD
ModeratorNeil Love, MD
Faculty

A Conversation with the Investigators: Ovarian Cancer Wednesday, July 7, 2021
5:00 PM – 6:00 PM ET
Michael J Birrer, MD, PhDKathleen Moore, MD
Richard T Penson, MD, MRCP
ModeratorNeil Love, MD
Faculty

A Conversation with the Investigators: Hormonal Therapy for Prostate Cancer
Monday, July 12, 20215:00 PM – 6:00 PM ET
Simon Chowdhury, MD, PhDTanya B Dorff, MD
Matthew R Smith, MD, PhD
ModeratorNeil Love, MD
Faculty

A Conversation with the Investigators: Chimeric Antigen Receptor T-Cell Therapy in Hematologic Cancers
Tuesday, July 13, 20215:00 PM – 6:00 PM ET
Caron Jacobson, MDDavid G Maloney, MD, PhD
Nikhil C Munshi, MD
ModeratorNeil Love, MD
Faculty

A Conversation with the Investigators: Acute Myeloid Leukemia and Myelodysplastic Syndromes
Wednesday, July 14, 20215:00 PM – 6:00 PM ET
Courtney D DiNardo, MD, MSCEGail J Roboz, MD
Eytan M Stein, MD
ModeratorNeil Love, MD
Faculty

Consensus or Controversy? Clinical Investigator Perspectives on the
Current and Future Management of Mantle Cell, Diffuse Large B-Cell and Hodgkin Lymphoma
Monday, August 2, 20215:00 PM – 6:00 PM ET
Stephen M Ansell, MD, PhDCraig Moskowitz, MD
Laurie H Sehn MD, MPH
ModeratorNeil Love, MD
Faculty

Consensus or Controversy? Chronic Lymphocytic Leukemia and
Follicular LymphomaTuesday, June 29, 20215:00 PM – 6:00 PM ET
Nathan H Fowler, MDProf John G Gribben, MD, DSc, FMedSci
Brad S Kahl, MD
ModeratorNeil Love, MD
Faculty

Agenda
MODULE 1: Chronic Lymphocytic Leukemia• Choice of front-line therapy• Selection of a BTK inhibitor• Second-line therapy• Third-line therapy• Ongoing research: Combination strategies, noncovalent BTK inhibitors,
CAR T-cell therapy
MODULE 2: Follicular Lymphoma• Selection of first- and second-line treatment• Third-line therapy: Tazemetostat, PI3K inhibitors, CAR T-cell therapy

Agenda
MODULE 1: Chronic Lymphocytic Leukemia• Choice of front-line therapy• Selection of a BTK inhibitor• Second-line therapy• Third-line therapy• Ongoing research: Combination strategies, noncovalent BTK inhibitors,
CAR T-cell therapy
MODULE 2: Follicular Lymphoma• Selection of first- and second-line treatment• Third-line therapy: Tazemetostat, PI3K inhibitors, CAR T-cell therapy

Regulatory and reimbursement issues aside, what is your preferred initial regimen for a 60-year-old patient with IGHV-mutated chronic lymphocytic leukemia without del(17p) or TP53 mutation who requires treatment?
1. FCR2. Ibrutinib +/- CD20 antibody3. Acalabrutinib +/- CD20 antibody4. Zanubrutinib 5. Venetoclax + obinutuzumab6. Venetoclax + ibrutinib7. Other

What is your usual preferred initial regimen a 60-year-old patient with IGHV-mutated chronic lymphocytic leukemia (CLL) without del(17p) or TP53 mutation who requires treatment?
Ibrutinib
FCR
Venetoclax + obinutuzumab
Ibrutinib + obinutuzumab
Ibrutinib + rituximab
FCR or acalabrutinib
Venetoclax + obinutuzumab
FCR
Acalabrutinib
FCR or venetoclax + obinutuzumab

Young patients with IGHV-mutated disease
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

Younger (fit) patient with newly diagnosed IGHV-mutated CLL –optimal treatment
PFS
(%)
Years0 6 8 1642 141210
p<0.0001
IGHV mutated (n=88)
IGHV unmutated (n=126)
0
60
100
80
40
20
FCR Ibrutinib
Chlorambucil-Obinutuzumab
VenetoclaxObinutuzumab
Chalk talk – Prof Gribben

Regulatory and reimbursement issues aside, what is your preferred initial regimen for a 60-year-old patient with IGHV-unmutated chronic lymphocytic leukemia without del(17p) or TP53 mutation who requires treatment?
1. FCR2. Ibrutinib +/- CD20 antibody3. Acalabrutinib +/- CD20 antibody4. Zanubrutinib 5. Venetoclax + obinutuzumab6. Venetoclax + ibrutinib7. Other

What is your usual preferred initial regimen for a 60-year-old patient with IGHV-unmutated CLL without del(17p) or TP53 mutation who requires treatment?
Ibrutinib
Ibrutinib
Venetoclax + obinutuzumab
Ibrutinib + obinutuzumab
Venetoclax + obinutuzumab
Venetoclax + obinutuzumab
Venetoclax + obinutuzumab
Acalabrutinib OR venetoclax +
obinutuzumab
Acalabrutinib
Venetoclax + obinutuzumab

Younger (fit) patient with newly diagnosed IGHV-unmutated CLL – optimal treatment
PFS
(%)
Years0 6 8 1642 141210
p<0.0001
IGHV mutated (n=88)
IGHV unmutated (n=126)
0
60
100
80
40
20
FCR Ibrutinib ECOG1912
Ibrutinib
FCR
OS survival advantage for IbrutinibHR: 0.34 (95% CI: 0.15–0.79); p=0.009
Chalk talk – Prof Gribben

What is your usual preferred initial regimen for a 75-year-old patient with IGHV-mutated CLL without del(17p) or TP53 mutation who requires treatment?
Acalabrutinib
Venetoclax + obinutuzumab
Venetoclax + obinutuzumab
Ibrutinib
Acalabrutinib
Venetoclax + obinutuzumab
Venetoclax + obinutuzumab
Acalabrutinib
Venetoclax + obinutuzumab
Venetoclax + obinutuzumab

What is your usual preferred initial regimen for a 75-year-old patient with IGHV-unmutated CLL without del(17p) or TP53 mutation who requires treatment?
Acalabrutinib
Acalabrutinib
Venetoclax + obinutuzumab
Ibrutinib + obinutuzumab
Acalabrutinib
Venetoclax + obinutuzumab
Venetoclax + obinutuzumab
Acalabrutinib OR venetoclax +
obinutuzumab
Venetoclax + obinutuzumab
Venetoclax + obinutuzumab

Older patients; choice of BTK inhibitor
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

Older (unfit) patient with newly diagnosed CLL – optimal treatment with novel agents is independent of IGHV-mutational status
Ibrutinib
b
VenetoclaxObinutuzumab
Continuous therapy One year fixed duration therapy
Chalk talk – Prof Gribben

ELEVATE RR Trial Acalabrutinib vs Ibrutinib in R/R CLL
J Byrd et al ASCO 2021 Courtesy of Prof John G Gribben, MD, DSc, FMedSci

ELEVATE RR – Adverse events of special interest
Byrd et al SCO 20221 Courtesy of Prof John G Gribben, MD, DSc, FMedSci

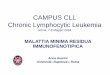
ALPINE STUDY – Zanubrutinib vs Ibrutinib in RR CLLORR (INV assessment): Zanubrutinib 78.3%, ibrutinib 62.5% (2-sided p = 0.0006)
*Not a prespecified analysis; formal analysis of PFS will be based on all patients when the target number of events is reached.Median PFS follow-up was 14.0 months for both zanubrutinib and ibrutinib arms by reverse KM method.PFS, progression-free survival Courtesy of Prof John G Gribben, MD, DSc, FMedSci

ALPINE
Courtesy of Prof John G Gribben, MD, DSc, FMedSci

TTNTPFS
Median observation: 52.4 mos
Al-Sawaf O, et al., Presented at ASH 2020. Abstract 127
Author conclusions• Individual clonal growth rates can be used to estimate growth
dynamics after a fixed-duration treatment. • Clonal growth was lower after Ven-Obi than after Clb-Obi,
indicating more effective MRD eradication and clonal growth modulation with Ven-Obi.
• In a considerable subgroup (approx. 20%) of Ven-Obi treated patients, no clonal growth was measurable during observation, indicating deepest remissions.
• This translates into a sustained PFS benefit for several years after treatment completion, with a 4-year-PFS rate of 74% for Ven-Obitreated patients.
Venetoclax plus obinutuzumab (CLL14): 4-year progression-free survival and overall survival
Overall survival
Courtesy of Prof John G Gribben, MD, DSc, FMedSci

CLL14: Clonal dynamics after venetoclax-obinutuzumab therapyMRD by NGS at EOT • About 1/3 of patients had a
continued reduction in MRD from C7 onward
• Some patients have deep responses that deepen even further
• At EOT some were MRD+ (black box) – would more treatment help?
Of 20 pts with known PB MRD+ status at EOT:
MRD During and After Ven-Obi
Al-Sawaf O, et al., Presented at ASH 2020. Abstract 127 Courtesy of Prof John G Gribben, MD, DSc, FMedSci

Regulatory and reimbursement issues aside, what is your preferred initial regimen for a 60-year-old patient with del(17p) CLL who requires treatment?
1. FCR2. Ibrutinib +/- CD20 antibody3. Acalabrutinib +/- CD20 antibody4. Zanubrutinib 5. Venetoclax + obinutuzumab6. Venetoclax + ibrutinib7. Other

What is your usual preferred initial regimen for a 60-year-old patient with del(17p) CLL who requires treatment?
Ibrutinib
Ibrutinib
Acalabrutinib + obinutuzumab
Ibrutinib + obinutuzumab
Venetoclax + obinutuzumab
Acalabrutinib
Acalabrutinib
Acalabrutinib
Acalabrutinib
Acalabrutinib + obinutuzumab

What is your usual preferred initial regimen for a 75-year-old patient with del(17p) CLL who requires treatment?
Acalabrutinib
Ibrutinib
Acalabrutinib
Ibrutinib + obinutuzumab
Venetoclax + obinutuzumab
Acalabrutinib
Acalabrutinib
Acalabrutinib
Venetoclax + obinutuzumab
Acalabrutinib + obinutuzumab

High-risk disease (eg, del[17p])
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

CIT: chemoimmunotherapy; Obin: obinutuzumab; CLBO: Chlorambucil plus Obinutuzumab; R: rituximab; a if approved and available;bChemoimmunotherapy as alternative treatment only if no TP53 dysfunction and reasons against continuous treatment with ibrutinib or non-availability; c CLBO might be considered as well, but no data in fit patients are available.
First-Line Ibrutinib for CLL in Pts With TP53 Aberrations
Early stage CLL with symptoms or advanced stage CLL
TP53mutation or
del(17p)
IGHV unmutatedNo TP53 mutation or
del(17p)
IGHV mutatedNo TP53 mutation or
del(17p)
Ibrutinib/ Acalabrutinibd
Venetoclax+Oa
VenetoclaxIdelalisib+R
[III, A]
Ibrutinib CITa: FCRb
[I, A]
CITa: FCRb
Ibrutinib[I, A]
Venetoclax+Oc
Ibrutinib / Acalabrutinibd
CITa: CLBO[I, A]
Venetoclax+Oc
CITa: CLBOIbrutinib /
Acalabrutinibd
[I, A] a
Fit patients Unfit patients
Fit patients Unfit patients All patients
No CITrecommended
Allan J, et al., ASH 2020. Abstract #2219
What is the optimal first-line therapy for a patient with CLL and del(17p) or a TP53 mutation?Ibrutinib
VenetoclaxObinutuzumab
Chalk talk – Prof Gribben

Which second-line systemic therapy would you recommend for a 60-year-old patient with IGHV-unmutated CLL without del(17p) or TP53 mutation who responds to ibrutinib and then experiences disease progression 3 years later?
1. FCR2. Acalabrutinib3. Acalabrutinib + obinutuzumab4. Venetoclax5. Venetoclax + rituximab6. Venetoclax + obinutuzumab7. A PI3K inhibitor 8. Other

Which second-line systemic therapy would you recommend for a 60-year-old patient with IGHV-unmutated CLL without del(17p) or TP53 mutation who responded to ibrutinib and then experienced disease progression 3 years later?
Acalabrutinib
Venetoclax + rituximab
Venetoclax + rituximab
Venetoclax + rituximab
Venetoclax + obinutuzumab
Venetoclax + rituximab
Venetoclax + obinutuzumab
Venetoclax + rituximab
Venetoclax + obinutuzumab
Venetoclax + rituximab

Choice of anti-CD20 antibody
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

What would be your most likely approach for a patient with newly diagnosed CLL to whom you decide to administer up-front venetoclax/obinutuzumab who has detectable MRD after completing 1 year of treatment?
1. Continue treatment 2. Discontinue treatment

What would be your most likely approach for a patient with newly diagnosed CLL to whom you decided to administer up-front venetoclax/obinutuzumab and who had detectable minimal residual disease after completing 1 year of treatment?
Discontinue treatment
Discontinue treatment
Discontinue treatment
Continue treatment
Continue treatment
Discontinue treatment
Discontinue treatment
Continue treatment
Discontinue treatment
Discontinue treatment

Off-protocol role, if any, of MRD testing
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

Should you monitor MRD in CLL?
Not for Prime Time Yet!
8
5926
2665
131 2
0
20
40
60
80
100
IR (n=276) FCR (n=103)
Not interpretable High (>1%) Int. (MRD ≤1%) uMRD
Rare with BTKi
0 6 12 18 24 30 36 42Time since EoT (Months)
0
20
40
60
80
100
Patie
nts (
%)
VenO, uMRD
OClb, uMRD
OClb, L-MRD
VenO, L-MRD
OClb, H-MRD
VenO, H-MRDEoT
Predictive with Ven-O
But … we give 1 year fixed duration therapy and not yet any evidence that longer treatment matters
Chalk talk – Prof Gribben

Have you or would you administer ibrutinib or acalabrutinib in combination with venetoclax to a patient with CLL outside of a clinical trial setting?
1. I haven’t and would not 2. I haven’t but would for the right patient 3. I have

Have you administered or would you administer ibrutinib or acalabrutinib in combination with venetoclax to a patient with CLL outside of a clinical trial setting?
I haven’t and would not
I haven’t and would not
I haven’t and would not
I haven’t and would not
I haven’t and would not
I haven’t and would not
I have: Ven resistant and PI3Ki resistant
I haven’t but would for the right patient
I haven’t and would not
I haven’t and would not

Combining BTK inhibitors and venetoclax
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

S I T E M A N C A N C E R C E N T E R
Chalk Talk – Dr Kahl
• The appeal comes if it facilitates time limited therapy
• More side effects encountered during dual therapy (personal experience in CLL and MCL)
• Theoretically possible dual therapy advantageous in scenarios of unfavorable biology (17p del, p53 mutated)
• No situation where I would do it outside a trial in CLL at present
Do you believe there is a benefit to administering BTK inhibitors and venetoclax in combination as opposed to sequentially in patients with CLL? Are there any situations in which you would do so outside of a clinical trial today?

Primary analysis of the Phase III GLOW Study: Fixed duration Ibrutinib and Venetoclax (I+V) versus Chlorambucil plus Obinutuzumab (Clb+O) for first-line CLL
• Patients aged ≥65 years or 18-64 years with cumulative illness rating scale (CIRS) score >6 or creatinine clearance <70 mL/min randomized to I+V or Clb+O
• All-oral, fixed duration I+V demonstrated superior PFS versus Clb+O as first-line treatment (HR 0.216, p < 0.0001)
• At 3 mo after end of treatment, rate of uMRD was significantly higher for I+V vs Clb+O in BM (51.9% vs 17.1%; p < 0.0001) and peripheral blood (PB; 54.7% vs 39.0%; p = 0.0259)
Kater A et al. EHA 2021;Abstract LB1902Courtesy of Prof John G Gribben, MD, DSc, FMedSci

Primary analysis of the fixed duration cohort from the Phase II CAPTIVATE study of first-line ibrutinib + venetoclax for CLL
• First-line ibrutinib plus venetoclax, an all-oral, once-daily, chemotherapy-free fixed-duration regimen provides deep, durable responses in patients with CLL/SLL
• Benefit was observed regardless of genomic high-risk features.
• No new safety signals were identified
Allan J et al. EHA 2021;Abstract S147Courtesy of Brad S Kahl, MD

If you could access one of the novel noncovalent BTK inhibitors (eg, pirtobrutinib) for your patients with relapsed CLL today, would you want to use it in clinical practice?
Yes: In second line, ibrutinib failure
No
Yes: Would prefer it over idelalisib
No
Yes: Far better BTK inhibitor, will be drug of choice when
approved
Yes: Covalent BTK refractory
Yes: BTK failure c481 mutated
Yes: Covalent BTK refractory
Yes: For BTKi-resistant patients
Yes: Generally post covalent inhibitor with progression

Future role of noncovalent BTKi (pirtobrutinib)
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

S I T E M A N C A N C E R C E N T E R
Chalk Talk – Dr Kahl
• Attractive when encountering resistance to 1st and 2nd generation BTKi
• Attractive when encountering intolerance to 1st and 2nd generation BTKi
• True for CLL and MCL and WM and MZL
• RCTs will determine whether 3rd generation will supplant 1st and 2nd
generation
If you could access one of the novel noncovalent BTK inhibitors, would you want to use it in clinical practice? For which type of patient would you be inclined to use these agents?

S I T E M A N C A N C E R C E N T E R
Courtesy of Brad S Kahl, MD
Pirtobrutinib (LOXO-305): Response

S I T E M A N C A N C E R C E N T E R
Courtesy of Brad S Kahl, MD

Which third-line therapy would you generally recommend for a 75-year-old patient with IGHV-unmutated CLL without del(17p) or TP53 mutation who responded to ibrutinib for 3 years, experienced disease relapse, then received venetoclax for 18 months followed by disease progression?
Obinutuzumab
Idelalisib
Idelalisib
Duvelisib
Idelalisib
Duvelisib
Duvelisib
Umbralisib
Idelalisib
Idelalisib + rituximab

Double-refractory CLL (BTKi, venetoclax)
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

Agenda
MODULE 1: Chronic Lymphocytic Leukemia• Choice of front-line therapy• Selection of a BTK inhibitor• Second-line therapy• Third-line therapy• Ongoing research: Combination strategies, noncovalent BTK inhibitors,
CAR T-cell therapy
MODULE 2: Follicular Lymphoma• Selection of first- and second-line treatment• Third-line therapy: Tazemetostat, PI3K inhibitors, CAR T-cell therapy

Regulatory and reimbursement issues aside, what would be your most likely initial treatment choice for a 78-year-old patient with Stage III, Grade I or II follicular lymphoma (FL) with fatigue and symptomatic bulky adenopathy who required treatment?
Rituximab/lenalidomide
BR
BR
BR
BR
BR
BR
BR
BR
BR

First-line therapy for FL
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

Do you believe community-based oncologists/hematologists should be presenting the R2 regimen of lenalidomide/rituximab as a front-line option to patients with newly diagnosed FL?
• Patients with bulky/symptomatic low-grade lymphoma should be treated with combination regimens.
• RELEVANCE study compared R-Chemo to R2 in untreated FL.• Overall response rate and progression-free survival was excellent (and similar) in both arms.• Lenalidomide combination has more rash, chemotherapy had more neutropenia and severe
infections.• No increased risk of secondary cancers was seen in either arm.• Treatment should be individualized for each patient.
Chalk talk – Dr Fowler

Regulatory and reimbursement issues aside, what is your usual second-line therapy for a 65-year-old patient with FL who achieves a complete response to 6 cycles of BR but then experiences disease relapse 4 years later?
1. Re-treatment with BR2. Obinutuzumab/bendamustine3. R-CHOP4. Rituximab/lenalidomide5. A PI3K inhibitor6. Tazemetostat7. Other

Regulatory and reimbursement issues aside, what is your usual second-line therapy for a 65-year-old patient with FL who achieves a complete response to 6 cycles of BR but then experiences disease relapse 4 years later?
Rituximab/lenalidomide
Chemotherapy àautologous transplant
Rituximab/lenalidomide
Rituximab/lenalidomide
Rituximab/lenalidomide
Rituximab/lenalidomide
Rituximab/lenalidomide
Rituximab/lenalidomide
Rituximab/lenalidomide
Rituximab/lenalidomide

What is your usual third-line treatment for a patient with FL with an EZH2 mutation who received first-line BR, second-line lenalidomide/rituximab and then develops disease progression?
1. Idelalisib 2. Copanlisib3. Duvelisib4. Umbralisib5. Tazemetostat6. R-CHOP7. Obinutuzumab +/- chemotherapy8. Other

What is your usual third-line treatment for a patient with FL with an EZH2 mutation who receives first-line BR, second-line lenalidomide/rituximab and then develops disease progression?
Tazemetostat
Tazemetostat
Tazemetostat
Tazemetostat
Tazemetostat
Tazemetostat
Tazemetostat
Tazemetostat
Tazemetostat
Tazemetostat or consider CAR-T therapy

If you were going to administer a PI3 kinase inhibitor to a patient with relapsed/refractory FL, which do you generally prefer?
1. Idelalisib2. Copanlisib3. Duvelisib4. Umbralisib

What is your usual third-line treatment for a patient with FL (EZH2 wild type) who receives first-line BR, second-line lenalidomide/rituximab and then develops disease progression?
Tazemetostat
Rituximab/lenalidomide
Tazemetostat
Tazemetostat
Umbralisib
Obinutuzumab +/-chemotherapy
Rituximab/lenalidomide or
umbralisib
Tazemetostat
Idelalisib
Umbralisib or consider CAR-T therapy

Third-line therapy for FL
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

What is the optimal therapeutic approach for a patient with FL with and without an EZH2 mutation who has experienced disease progression on bendamustine/rituximab and then R2?
• Several effective options exist for patients with relapsed FL.• Single agent anti-CD20 agents• EZH2 inhibitors (also effective in EZH2 wild type disease)• CAR-T• Auto SCT• PI3K• Clinical trials (anti-CD19, BiTE, anti-CD47, anti-Syk, BTKi)
• Always repeat a biopsy to confirm the dx and exclude transformed disease.• The selection of next-line therapy should be informed by patient’s prior disease course
and length of prior remissions.• Helps understand patient’s short- and long-term risk from FL.• There is no “right answer.”
Chalk talk – Dr Fowler

Do you believe that there are discernible differences in terms of efficacy or tolerability that make one of the four FDA-approved PI3K inhibitors for relapsed/refractory FL a better therapeutic option?
• Currently approved PI3K inhibitors are associated with remarkable and similar efficacy.• PFS ranging from 10-11 mo.• ORR of around 50%.
• Different isoforms and drug structures have resulted in very different toxicity profiles.• ↑↓ colitis, infection, hyperglycemia, hypertension and rash.
• Patients should be counseled on the potential risks as well as how to manage side effects.• Especially infection risk and GI side effects.
• Dose interruption and/or reduction is effective and often allows for re-starting the drug.• Choice of drug should be individualized.• Ongoing studies looking at different schedules to reduce toxicity look promising.
Chalk talk – Dr Fowler

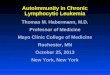
Approved PI3K inhibitors in R/R Follicular LymphomaIdelalisib Copanlisib Duvelisib Umbralisib
FDA approval Jul 29, 2014 Sep 14, 2017 Sep 24, 2018 Feb 5, 2021
Isoforms PI3K delta Pan-PI3K PI3K delta/gamma PI3K-delta and CK1-epsilon
Formulation 150 mg PO BID 60 mg IV Q weekly3 wks on, 1 wk off
25 mg PO BID 800 mg PO QD
Indication in FL Relapsed after at least two prior systemic therapies
Relapsed after at least two prior systemic therapies
Relapsed after at least two prior systemic therapies
Relapsed after at least three prior systemic therapies
Pivotal trial Study 101-09 CHRONOS-1 NCT02204982 UTX-TGR-205
Results iNHL, n=125 ORR 57%, CR 6%
FL, n=104ORR 59%, CR 14%
FL, n=83ORR 42%, 1 CR
FL, n = 117ORR 43%, CR 3%
mDOR 12.5 mo mDOR 12.2 mo 43% maintained responses for >6mo, 17% maintained responses for >12mo
mDOR 11.1 mo
Side effects Pneumonitis, transaminitis, colitis Hyperglycemia, hypertension, infections, neutropenia
Infection, diarrhea or colitis, pneumonia
Infection, neutropenia, diarrhea or noninfectiouscolitis
(Gopal A, et al. NEJM 2014; 370:1008-18) (https://www.fda.gov/Drugs/Information)S deVos Sep 2019

Patient demographics and baseline cancer characteristics (full analysis set)
CHRONOS-3 Trial: Copanlisib plus rituximab vs Rituximab plus placebo for Patients with R/R iNHL
Matasar M, et al ASCO 2021

PFS by independent review (full analysis set)
CHRONOS-3 Trial: Copanlisib plus rituximab vs Rituximab plus placebo
Matasar M, et al ASCO 2021

S I T E M A N C A N C E R C E N T E R
Courtesy of Brad S Kahl, MD

S I T E M A N C A N C E R C E N T E R
Courtesy of Brad S Kahl, MD
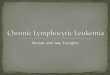
Mosunetuzumab: Adverse events

• High and durable response rates were observed in patients with aggressive (n=28) and indolent R/R NHL (n=24) who had failed multiple lines of therapy and who were treated with the bispecific antibody glofitamab
• CRS, the most common adverse event, was mostly manageable
Glofitamab step-up dosing: Complete response rates in updated efficacy data in heavily pretreated relapsed/refractory (R/R) non-Hodgkin lymphoma (NHL) patients
Carlo-Stella C et al ASCO 2021 Abstract 7519Courtesy of Brad S Kahl, MD

• Phase I/II Study: patients with R/R CD20+ B-NHL (FL n=12, DLBCL n=46, MCL n=4, others n=6) were treated with subcutanouesepcoritamab, a bispecific CD20xCD3 antibody
• Epcoritamab demonstrated substantial single-agent activity, inducing deep and durable clinically meaningful responses, with a consistent safety profile.
Subcutaneous epcoritamab in patients with relapsed/refractory B-cell non-Hodgkin lymphoma: Safety profile and antitumor activity
Clausen MR et al ASCO 2021 Abstract 7518Courtesy of Brad S Kahl, MD

Consensus or Controversy Consulting Investigators
Dr Jeff Sharman Dr Ian Flinn
Dr Christopher Flowers Dr John Leonard

Consensus or Controversy? Multiple Myeloma
Wednesday, June 30, 20215:00 PM – 6:00 PM ET
Natalie S Callander, MDShaji K Kumar, MDSagar Lonial, MD
ModeratorNeil Love, MD
Faculty

Thank you for joining us!
CME and MOC credit information will be emailed to each participant within 24 hours.