Embed Size (px)
DESCRIPTION
Citation preview
Conservative management Conservative management of blunt abdominal trauma of blunt abdominal trauma
in children at SKMCin children at SKMC
By By Dr Omar El ShiwihyDr Omar El ShiwihyMBBCH-M.Sc-FRCSMBBCH-M.Sc-FRCS
Pediatric surgical division-SKMCPediatric surgical division-SKMC
IntroductionIntroduction
Evoluted due to:Evoluted due to: 1- The remarkable report from 1- The remarkable report from
hospital for sick children in Toronto hospital for sick children in Toronto 1978.1978.
2-Our awareness about the well 2-Our awareness about the well documented danger of OPSI with the documented danger of OPSI with the development of “Save our spleen” development of “Save our spleen” concept which later on was extended concept which later on was extended to include other solid organs.to include other solid organs.
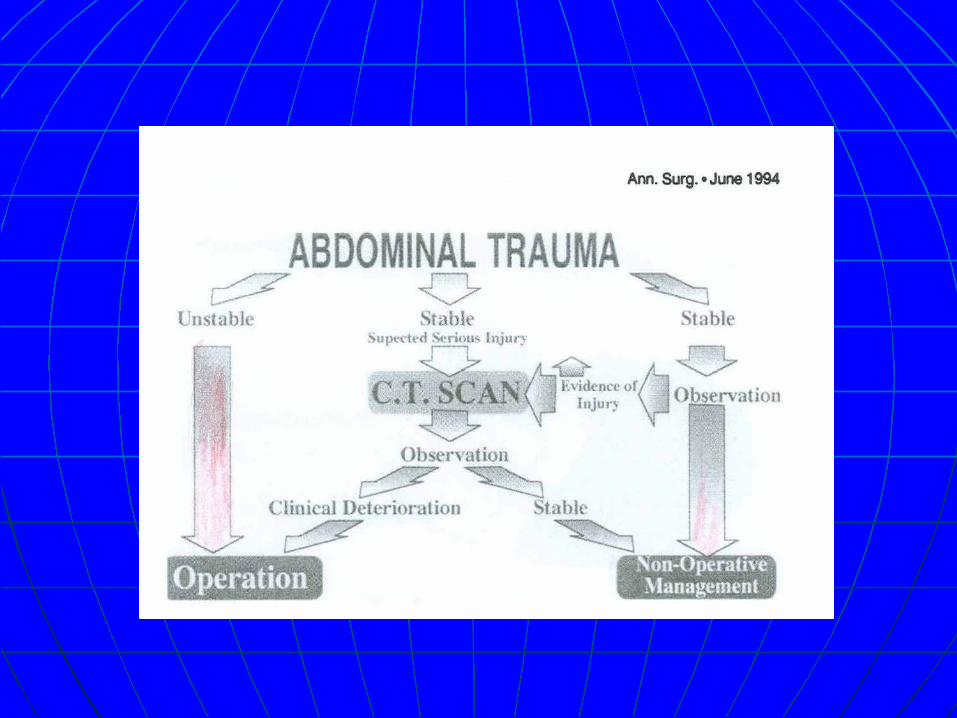
Criteria for conservative T/t of blunt Criteria for conservative T/t of blunt abdominal trauma:abdominal trauma:
1- hemodynamic stability1- hemodynamic stability
2- documentation of the extent of solid 2- documentation of the extent of solid organ injury by CT scan.organ injury by CT scan.
3- admission and observation in a PICU.3- admission and observation in a PICU.
Urgent laparotomy is done if the child Urgent laparotomy is done if the child becomes hemodynamically unstable or becomes hemodynamically unstable or requires repeated blood transfusion .requires repeated blood transfusion .

Aim of the workAim of the work
To determine the results and To determine the results and outcome of the conservative outcome of the conservative approach in the treatment of approach in the treatment of pediatric blunt abdominal trauma at pediatric blunt abdominal trauma at SKMC over a period of 8 year.SKMC over a period of 8 year.
Material and methodsMaterial and methods
Charts of all pediatric patients with Charts of all pediatric patients with blunt abdominal trauma admitted to blunt abdominal trauma admitted to SKMC under care of ped sur. during SKMC under care of ped sur. during the period from Feb 2000 to April the period from Feb 2000 to April 2008 were reviewed and analysed.2008 were reviewed and analysed.
31 charts were available for the 31 charts were available for the review.review.
ResultsResults
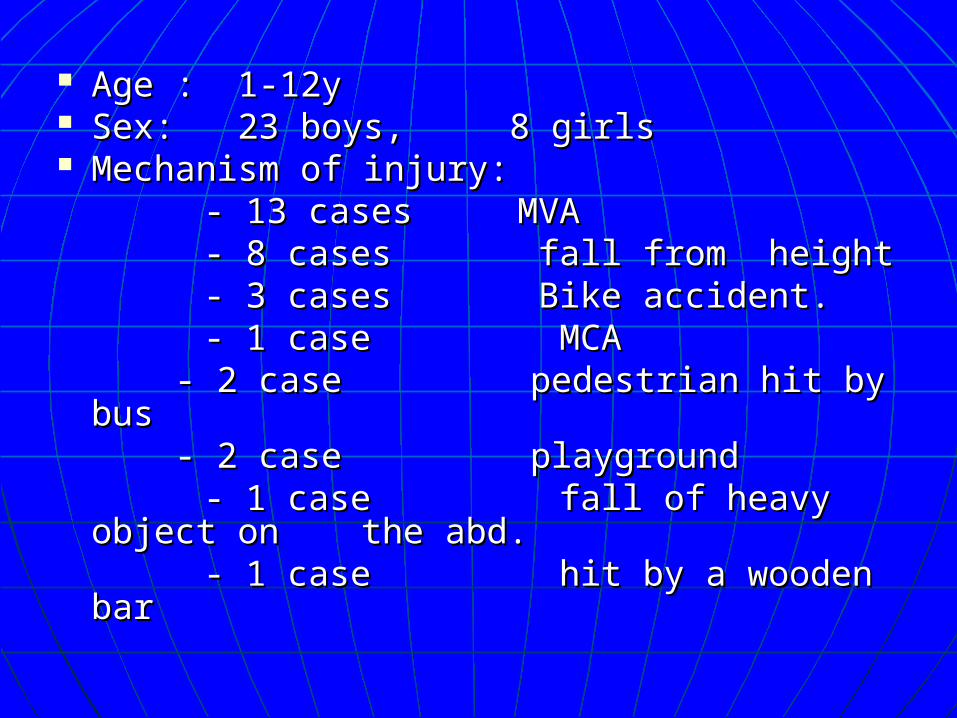
Age : 1-12yAge : 1-12y Sex: 23 boys, 8 girls Sex: 23 boys, 8 girls Mechanism of injury: Mechanism of injury: - 13 cases MVA- 13 cases MVA - 8 cases fall from height- 8 cases fall from height - 3 cases Bike accident.- 3 cases Bike accident. - 1 case MCA- 1 case MCA
- 2 case pedestrian hit by bus - 2 case pedestrian hit by bus - 2 case playground- 2 case playground
- 1 case fall of heavy object on - 1 case fall of heavy object on the abd.the abd.
- 1 case hit by a wooden bar- 1 case hit by a wooden bar
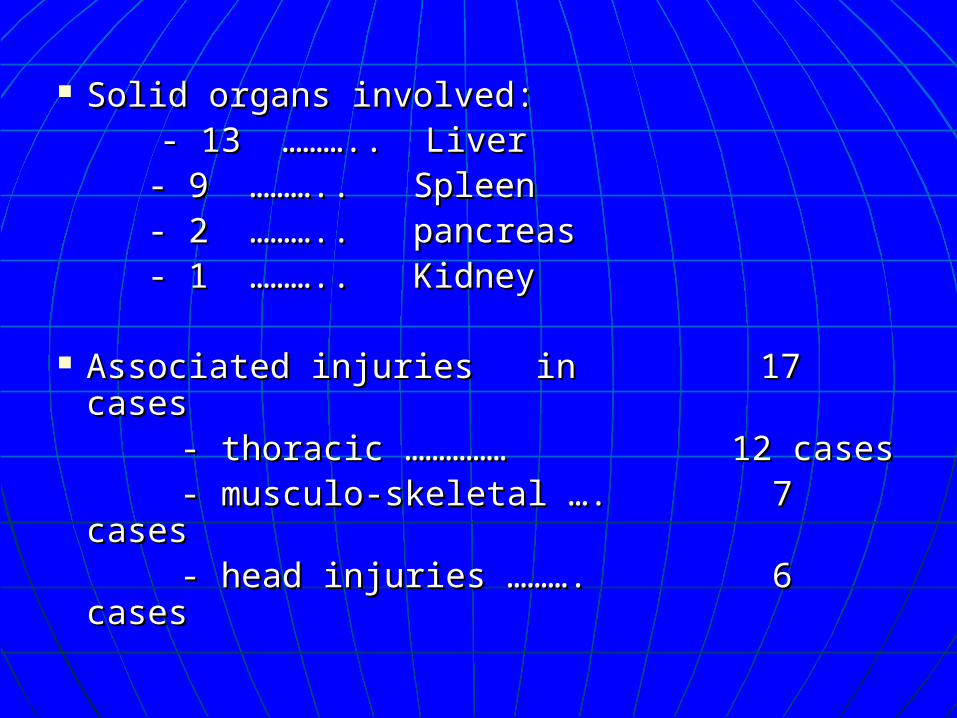
Solid organs involved:Solid organs involved: - 13 ……….. Liver- 13 ……….. Liver
- 9 ……….. Spleen- 9 ……….. Spleen - 2 ……….. pancreas- 2 ……….. pancreas - 1 ……….. Kidney- 1 ……….. Kidney
Associated injuries in 17 casesAssociated injuries in 17 cases - thoracic …………… 12 cases - thoracic …………… 12 cases - musculo-skeletal …. 7 cases- musculo-skeletal …. 7 cases - head injuries ………. 6 cases- head injuries ………. 6 cases
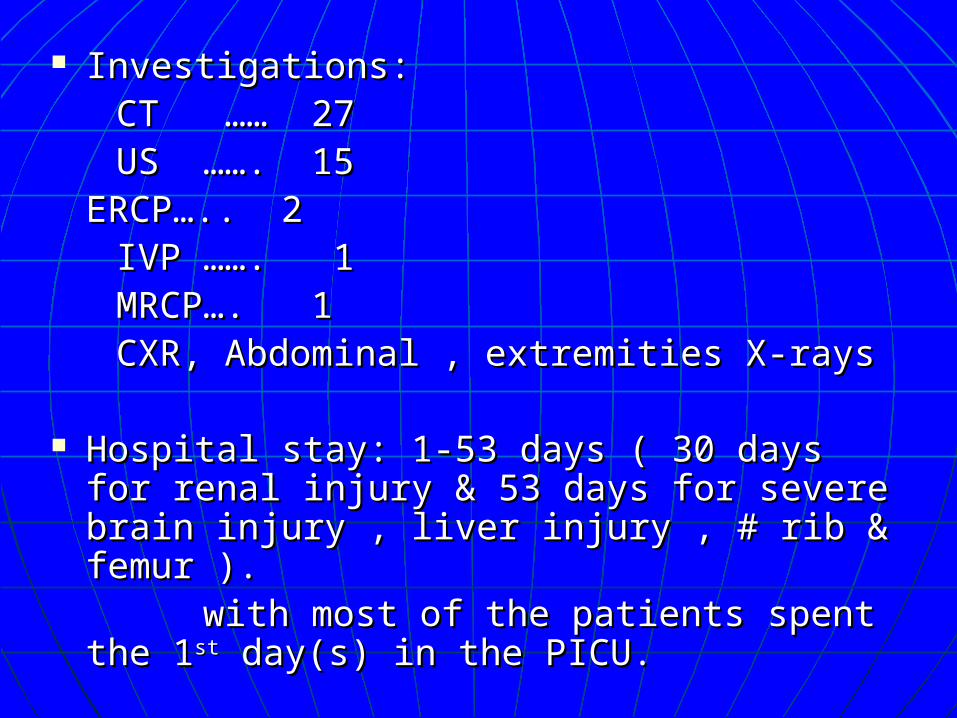
Investigations:Investigations: CT …… 27 CT …… 27 US ……. 15US ……. 15
ERCP….. 2ERCP….. 2 IVP ……. 1IVP ……. 1 MRCP…. 1 MRCP…. 1 CXR, Abdominal , extremities X-raysCXR, Abdominal , extremities X-rays
Hospital stay: 1-53 days ( 30 days for renal Hospital stay: 1-53 days ( 30 days for renal injury & 53 days for severe brain injury , injury & 53 days for severe brain injury , liver injury , # rib & femur ).liver injury , # rib & femur ).
with most of the patients spent the 1with most of the patients spent the 1stst day(s) in the PICU. day(s) in the PICU.
Primary management:Primary management: - close monitoring and observation.- close monitoring and observation. - fluid resuscitation with crystalloid +/- blood - fluid resuscitation with crystalloid +/- blood
transfusion ( 8 patients ).transfusion ( 8 patients ). - ICD …………………. 8 patients.- ICD …………………. 8 patients.
- craniotomy …….. 2 patients.- craniotomy …….. 2 patients. - Splenectomy …. 1 patient - Splenectomy …. 1 patient - perc. insertion of drain for perinephric collection - perc. insertion of drain for perinephric collection
+ insertion of double J stent.+ insertion of double J stent. - Closed reduction & IM nailing for # femur in 1 - Closed reduction & IM nailing for # femur in 1
pt.pt. - Bilateral decompression frontal craniotomy in 1 - Bilateral decompression frontal craniotomy in 1
pt.pt. - Second look laparotomy for removal of liver - Second look laparotomy for removal of liver
pack in 1 pt.pack in 1 pt.
Outcome & mortality:Outcome & mortality:
2 patients required laparotomy : 1 for 2 patients required laparotomy : 1 for splenectomy & 1 second look splenectomy & 1 second look laparotomy for removal of packlaparotomy for removal of pack
2 patient died from severe head injury.2 patient died from severe head injury.1 patient required delayed repair of 1 patient required delayed repair of
traumatic abdominal wall hernia.traumatic abdominal wall hernia.1 patient required delayed SSG. 1 patient required delayed SSG.
Selected casesSelected cases
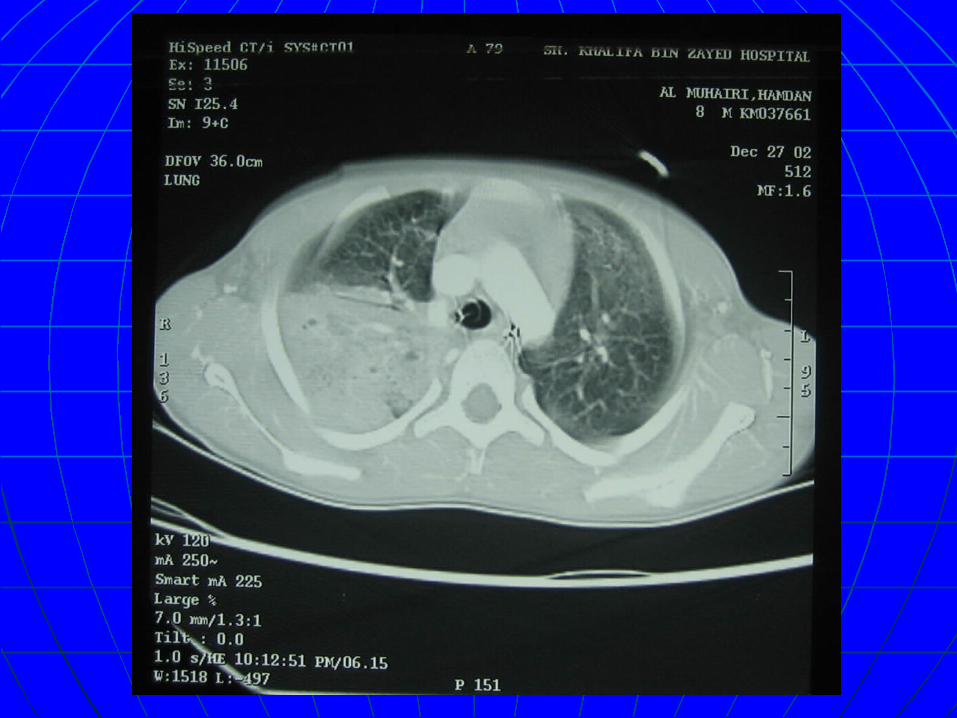
Case 1Case 1 KM # 037661. 27KM # 037661. 27thth -12-2002 -12-2002 8 y, boy .8 y, boy . Involved in Motor cycle accident.Involved in Motor cycle accident. ER: hemodynamicallly stable .ER: hemodynamicallly stable . CT: - Rt lung contusion and CT: - Rt lung contusion and
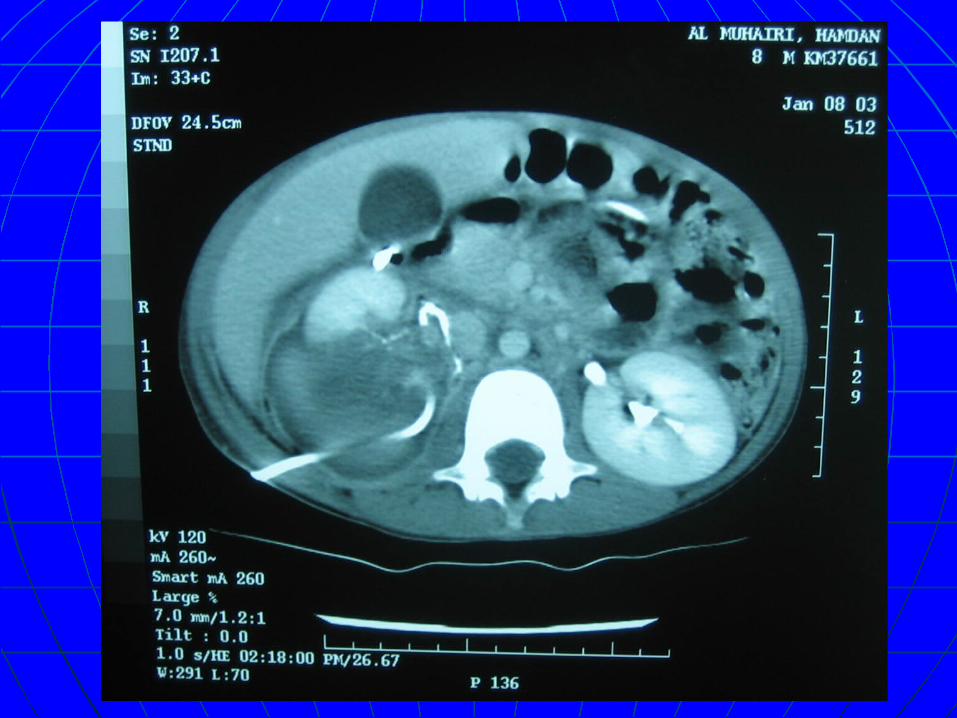
hemopneumothorax.hemopneumothorax. - transverse disruption of the Rt - transverse disruption of the Rt
kidney extending into the pelvis kidney extending into the pelvis with large perinephric collection.with large perinephric collection.
- # Rt clavicle and Rt 2- # Rt clavicle and Rt 2ndnd rib. rib. - no intra peritoneal fluid- no intra peritoneal fluid

Chest tube inserted and CV Line.Chest tube inserted and CV Line. Admitted to ICU and ventilated.Admitted to ICU and ventilated. Remained stable.Remained stable. on Day 7 FU with IVP; complete disruption of the on Day 7 FU with IVP; complete disruption of the
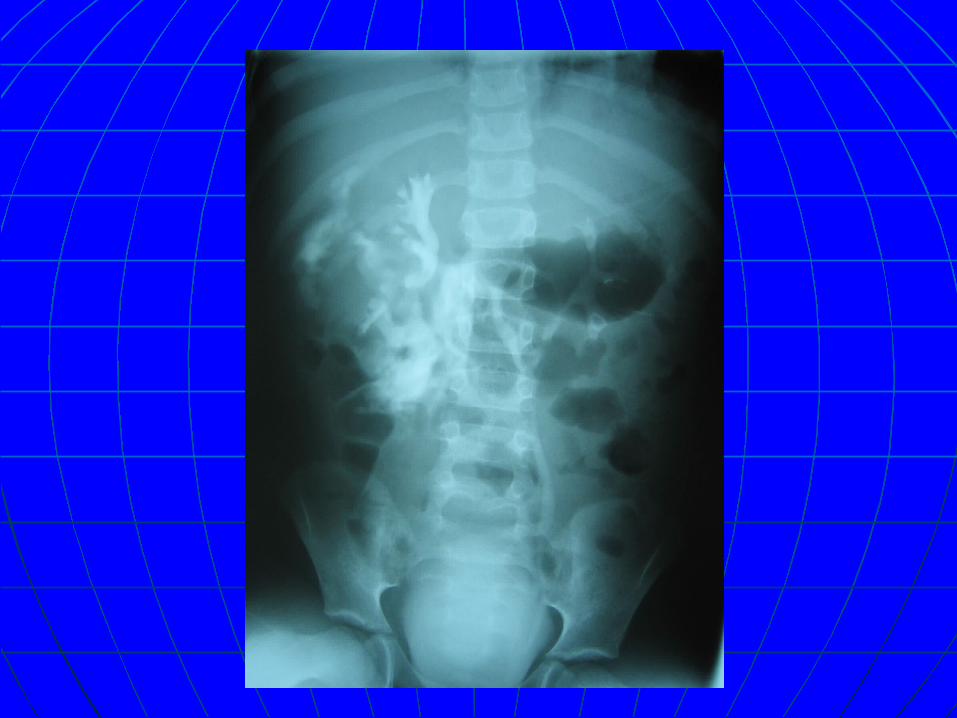
pelvicalyceal system …………percutaneous pelvicalyceal system …………percutaneous insertion of a drain( 3 wks).insertion of a drain( 3 wks).
22ndnd week retrograde pyelography ;complete week retrograde pyelography ;complete rupture of the renal collecting system rupture of the renal collecting system …………….double J stent inserted. …………….double J stent inserted.
On 3On 3rdrd week , developed septic episode (Staph week , developed septic episode (Staph aureous) ……..treated with antibiotic .aureous) ……..treated with antibiotic .
Perinephric collection completely Perinephric collection completely disappeared ,The pt. recovered well and D/c disappeared ,The pt. recovered well and D/c home after 1 month on antibiotic for another 2 home after 1 month on antibiotic for another 2 wks. wks.
FU after 2 wks with US …….no collection ,stent FU after 2 wks with US …….no collection ,stent was removed.was removed.
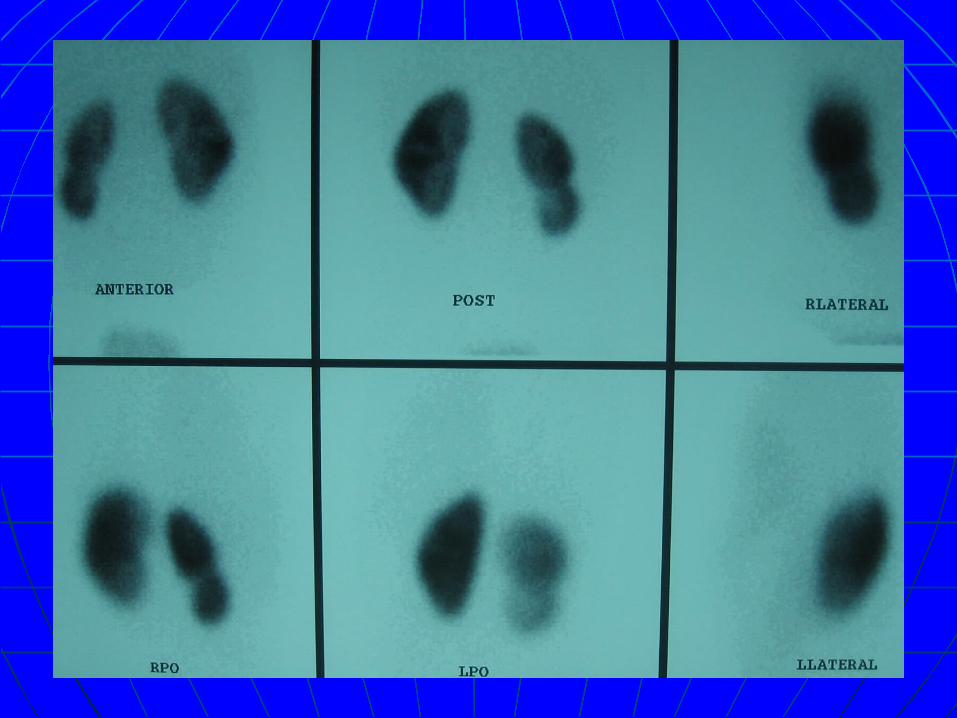
DMSA scan 2 yrs post injury.DMSA scan 2 yrs post injury.
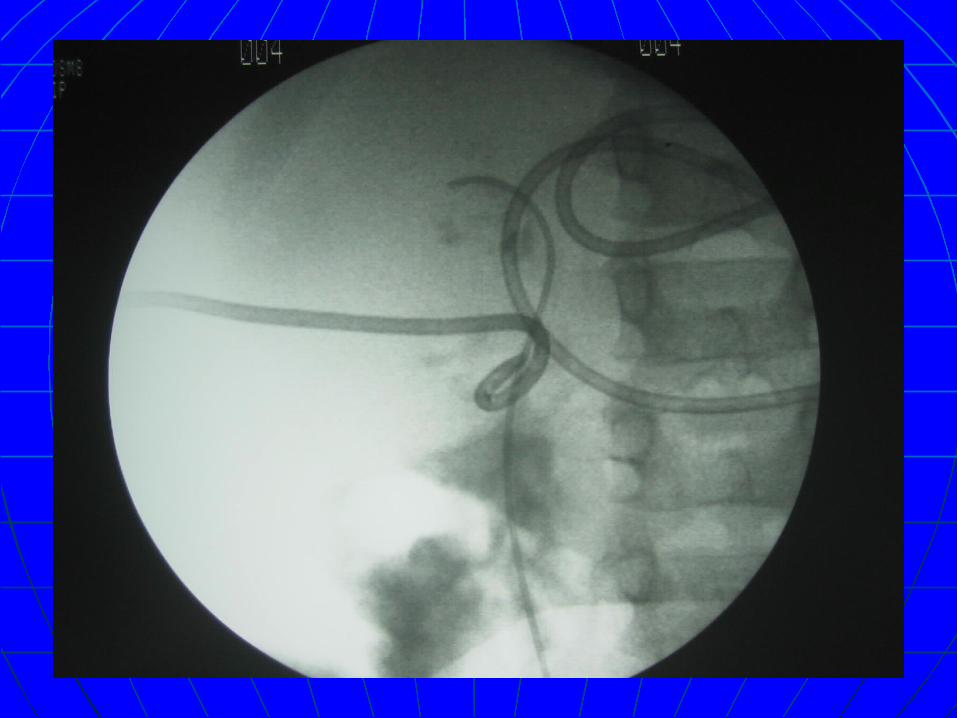
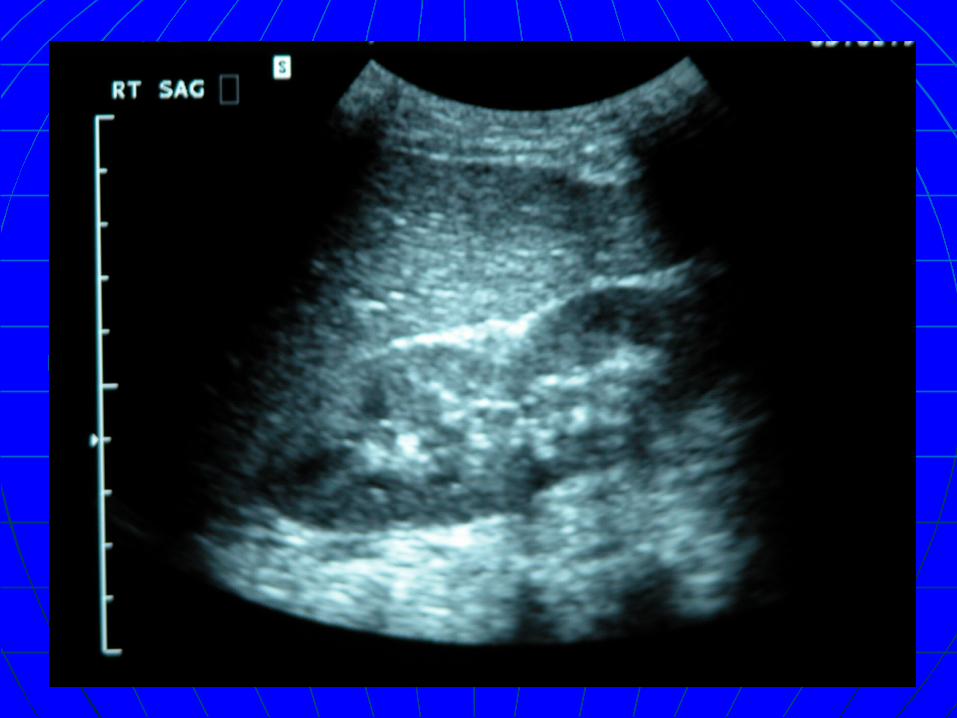
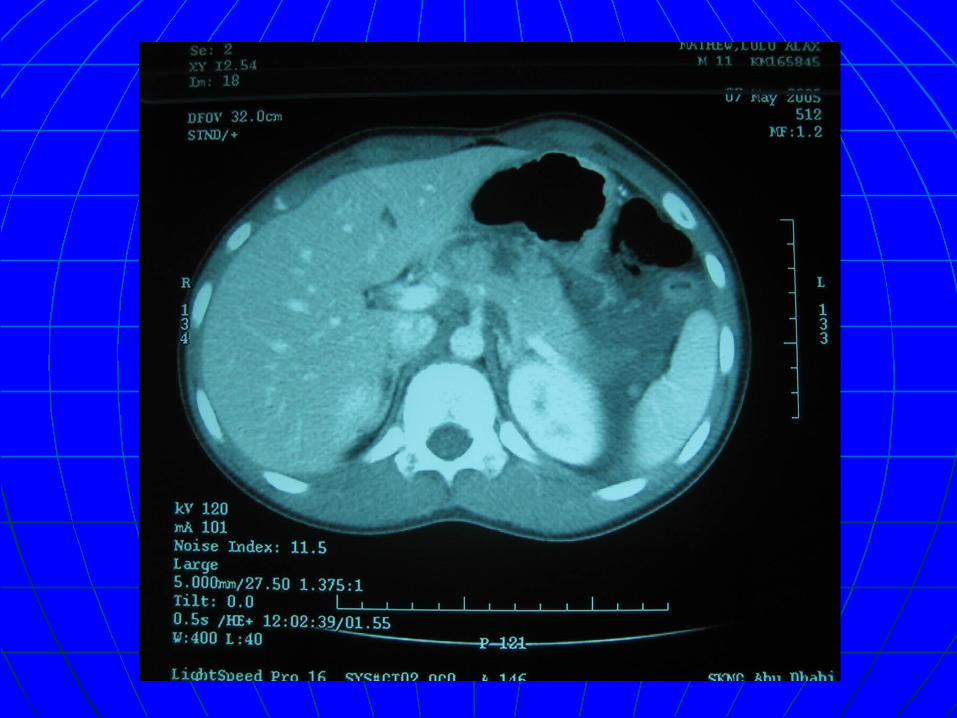
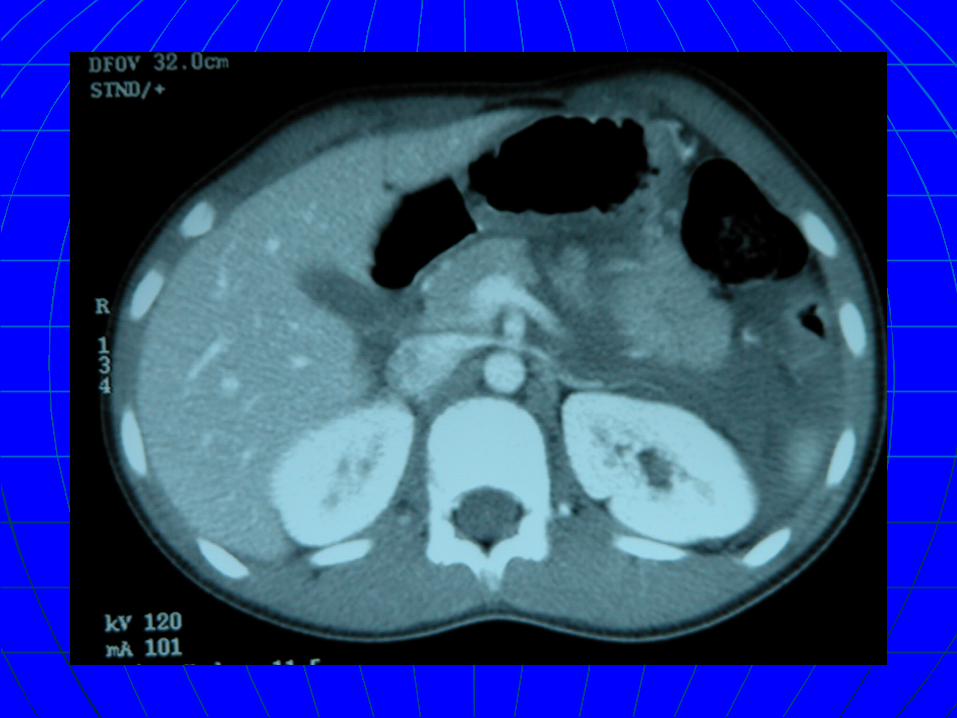
Case 2Case 2 KM # 165845. 6KM # 165845. 6thth-5-05-5-05 11 y boy.11 y boy. Fell on his abdomen.Fell on his abdomen. ER: hemodynamically stable , abd pain ER: hemodynamically stable , abd pain
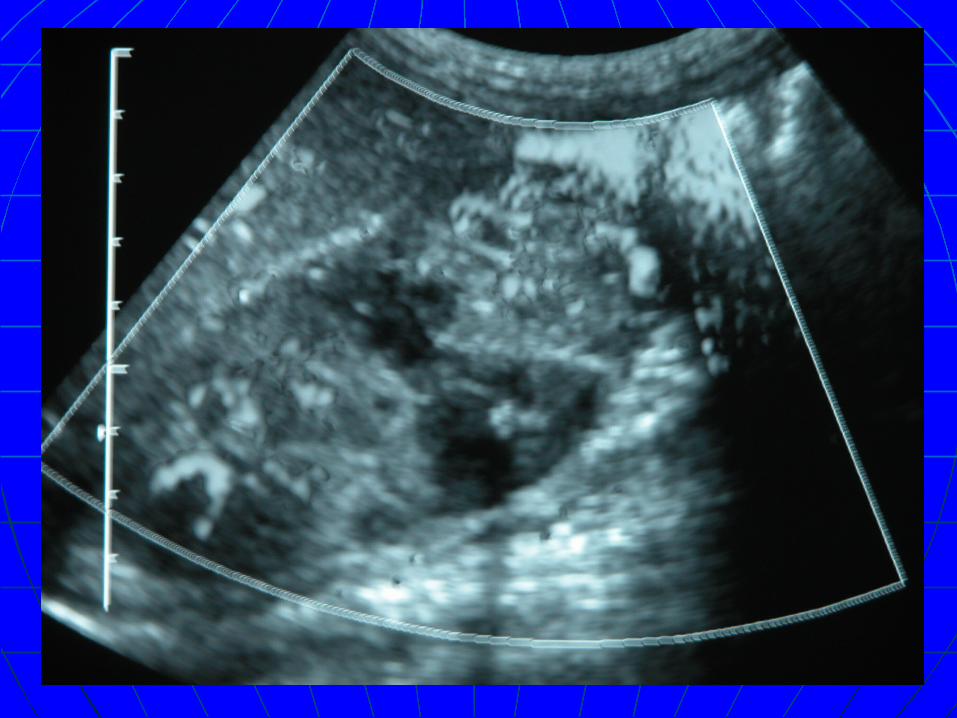
and vomiting, tender upper abd.and vomiting, tender upper abd. with Raised amylase 1with Raised amylase 1stst = 350. = 350. CT : laceration in the pancreas with CT : laceration in the pancreas with
possible involvement of the main possible involvement of the main pancreatic duct pancreatic duct retroperitoneal fluid collection.retroperitoneal fluid collection.
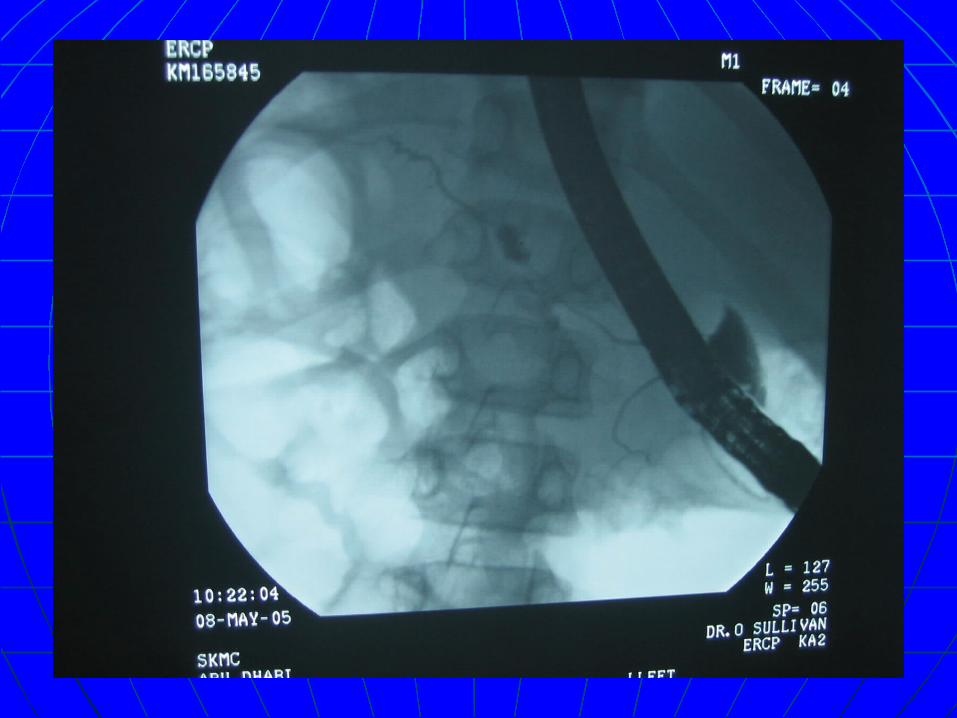
ERCP ….. Partial laceration of the proximal ERCP ….. Partial laceration of the proximal part of the main pancreatic duct .part of the main pancreatic duct .
Admission to ICU 1 day.Admission to ICU 1 day. NPO for 3 wks.NPO for 3 wks. CV Line inserted, TPN started.CV Line inserted, TPN started. FU with CT, US to R/o cyst formation and FU with CT, US to R/o cyst formation and
Serial amylase level.Serial amylase level. Pt. recovered well with no complication Pt. recovered well with no complication
and sent home 26 days later.and sent home 26 days later. FU with US…….free. FU with US…….free.
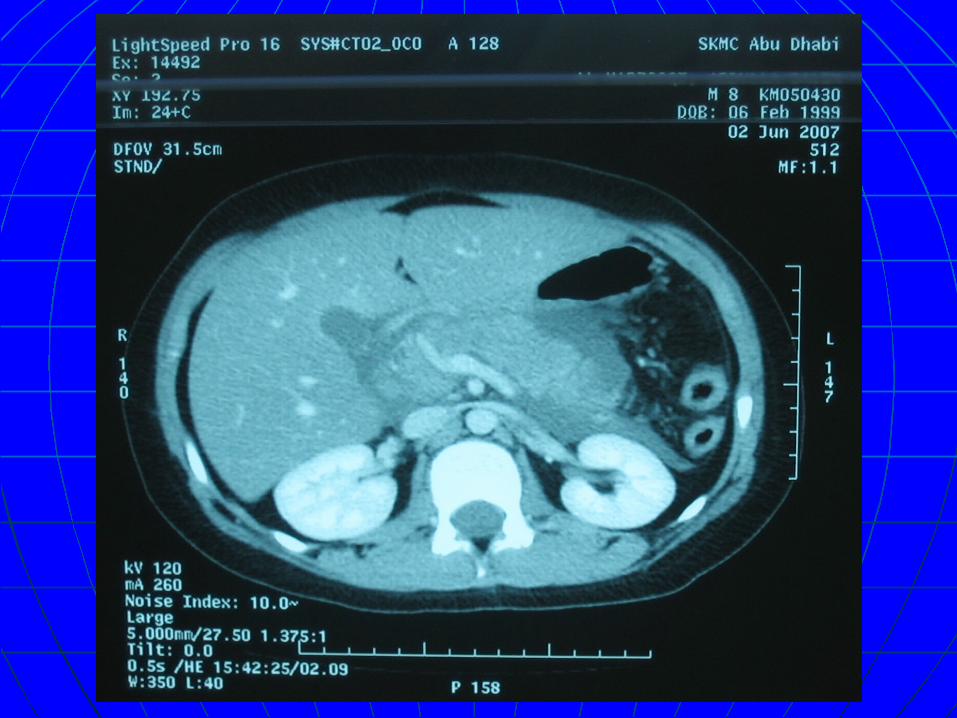
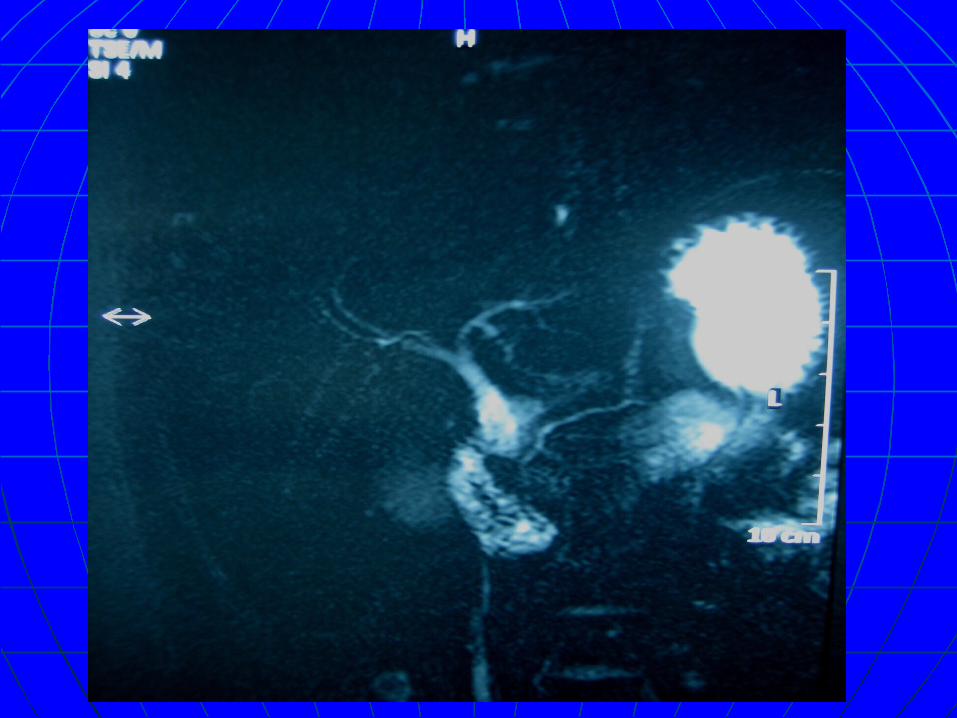
Case 3Case 3 KM # 050430KM # 050430 8 yrs boy 8 yrs boy Kick in the abdomen Kick in the abdomen Admitted on 2Admitted on 2ndnd June 2007 with abd. pain and vomitting & high June 2007 with abd. pain and vomitting & high
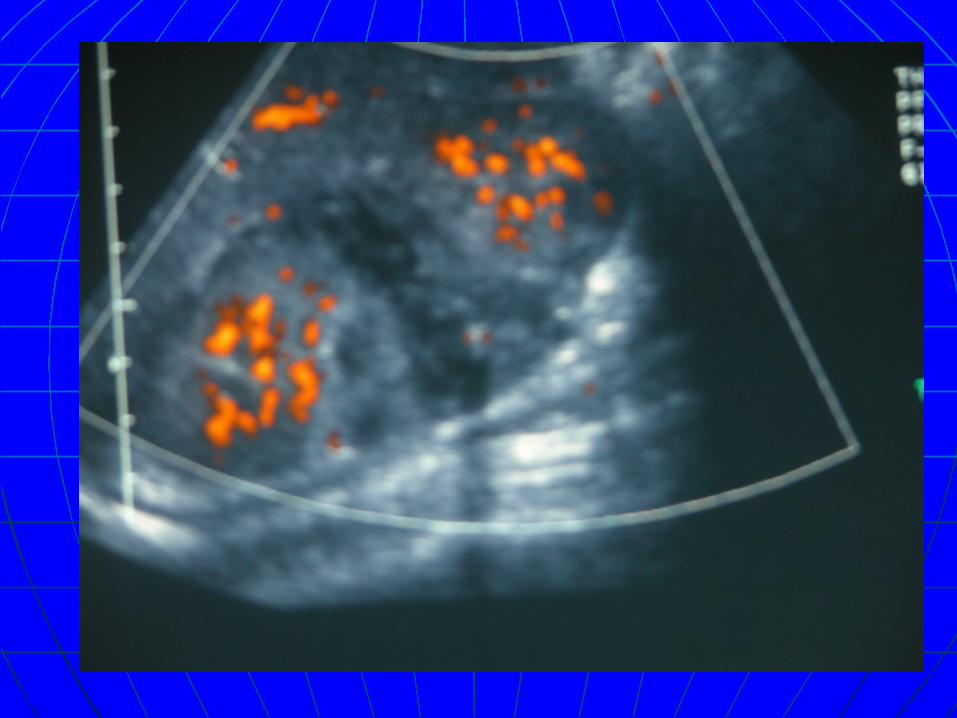
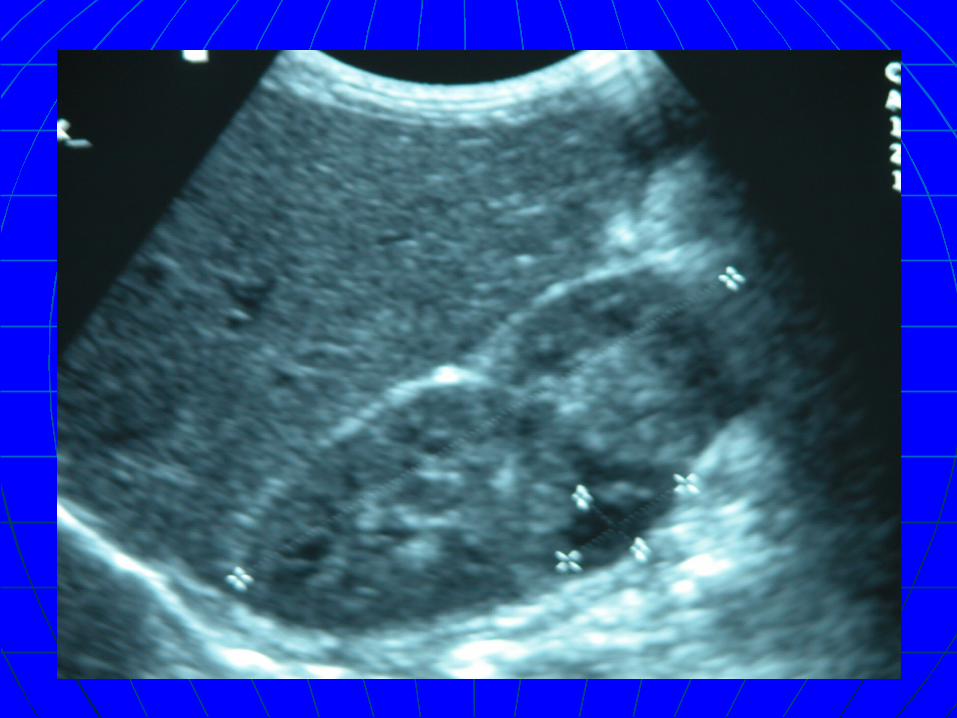
pancreatic enzymes.pancreatic enzymes. CT : Laceration of head & uncinate process , large peripancreatic CT : Laceration of head & uncinate process , large peripancreatic
fluid collection.fluid collection. CVL inserted , TPN , NPO , Antibiotics , octreotide --- 3 weeks.CVL inserted , TPN , NPO , Antibiotics , octreotide --- 3 weeks. CT (14CT (14THTH June ) : Normal study June ) : Normal study Discharged on 19Discharged on 19thth June June Readmitted on 17Readmitted on 17thth July with picture of pancreatitis July with picture of pancreatitis Kept NPO , peripheral nutrition. Kept NPO , peripheral nutrition. MRCP done to exclude congenital anomalies.MRCP done to exclude congenital anomalies. Discharged 7 days later and on followup he was free with no Discharged 7 days later and on followup he was free with no
complicationcomplication
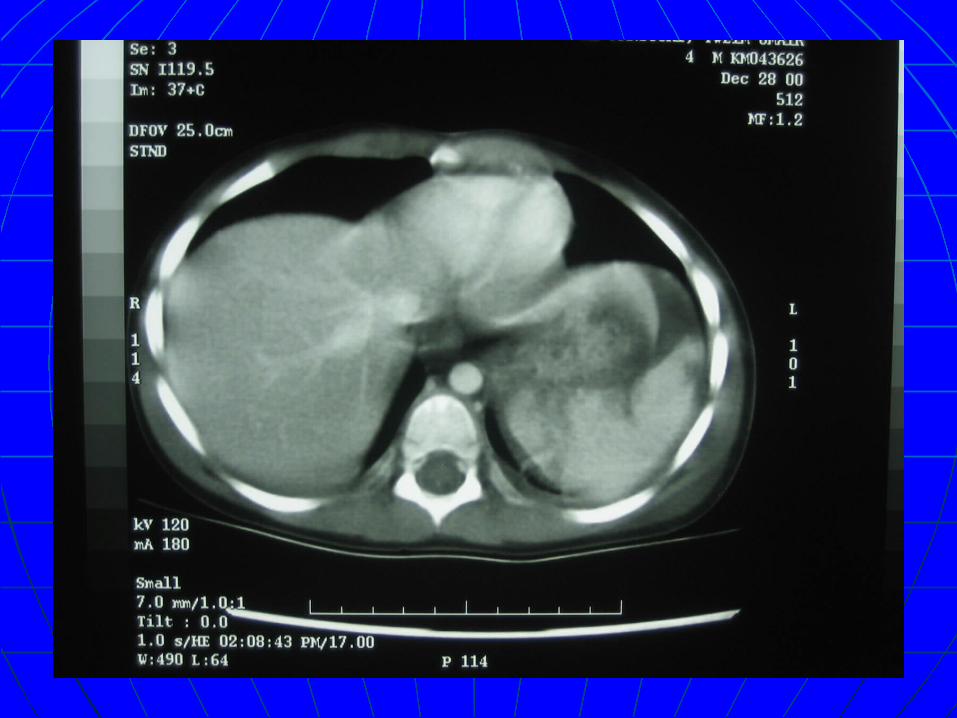
Case 4Case 4
KM # 043626, 28-12-00.KM # 043626, 28-12-00. 4 y boy.4 y boy. Involved in MVA. referred from Mafraq Involved in MVA. referred from Mafraq
Hospital.Hospital. ER: hemodynamically stable.ER: hemodynamically stable. Ct : - splenic injury.Ct : - splenic injury.
- Rt lung contusion.- Rt lung contusion.
- partial dehiscence of the abdominal - partial dehiscence of the abdominal wall with herniation of the colon.wall with herniation of the colon.

Admitted to ICU for observation …1 Admitted to ICU for observation …1 day.day.
Recovered well , DC home 9 days Recovered well , DC home 9 days later,later,
Came for hernial repair after 2 Came for hernial repair after 2 months.months.
FU with abd US…..free.FU with abd US…..free.
Case 5Case 5
KM # 188789, 8-3-06.KM # 188789, 8-3-06. 8 y boy.8 y boy. Received a kick to his abdomen while Received a kick to his abdomen while
playing referred from ZMH as a liver playing referred from ZMH as a liver haematoma with his CT scan. haematoma with his CT scan.
ER: hemodynamically stable.ER: hemodynamically stable. Admitted to ICU……..1 day.Admitted to ICU……..1 day. Review of CT revealed???????Review of CT revealed???????
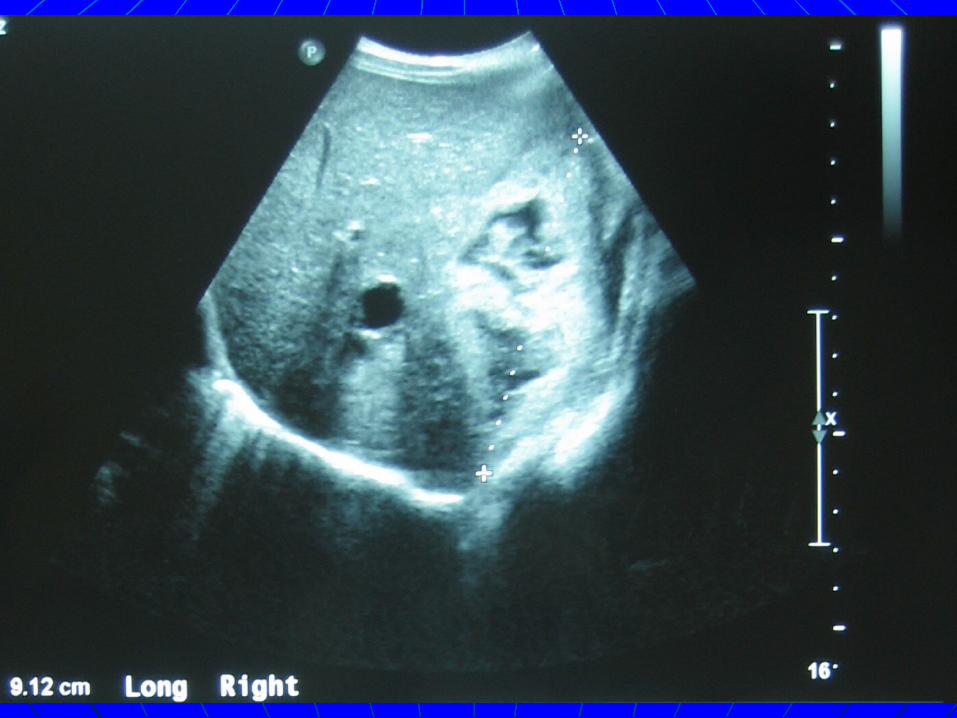
Case 6Case 6
KM : 199680KM : 199680

Hollow visceral injuryHollow visceral injury None in our pts. None in our pts. A concern with nonoperative managementA concern with nonoperative management CT findings suggestive of perforationCT findings suggestive of perforation
PneumoperitoneumPneumoperitoneum Bowel wall thickening or enhancementBowel wall thickening or enhancement Dilated bowel loopsDilated bowel loops Streaking of mesenteric fatStreaking of mesenteric fat Peritoneal fluid in absence of SVIPeritoneal fluid in absence of SVI
? Free peritoneal fluid? Free peritoneal fluid In a study of over 10 yrs. period : 2971 cases , sustained In a study of over 10 yrs. period : 2971 cases , sustained
SVI. The incidence was 3.2% (Childrens hospital of SVI. The incidence was 3.2% (Childrens hospital of Philadelphia).Philadelphia).
More with assault cases & pts. with multiple SVI & More with assault cases & pts. with multiple SVI & pancreatic injurypancreatic injury

ConclusionConclusion
Conservative management of blunt Conservative management of blunt abdominal trauma with solid organ injury abdominal trauma with solid organ injury is safe and appropriate if carried out under is safe and appropriate if carried out under continuous surgical observation in a PICU.continuous surgical observation in a PICU.
CT scan is our method of choice to CT scan is our method of choice to investigate patients with abdominal investigate patients with abdominal trauma.trauma.
GIT perforations are uncommon in blunt GIT perforations are uncommon in blunt abdominal traumaabdominal trauma