Embed Size (px)
Citation preview

Constipation in Infants and Children
DR NANDLAL KELLAASSOCIATE PROFESSOR AND CHAIRMAN DEPARTMENT OF PEDIATRIC SURGERY LUMHS
JAMSHORO

Clinical definition
Any of two of following symptoms for at least 3 month (not necessarily consecutive) in a year
• Straining
• Hard or lumpy stool
• Sensation of incomplete evacuation
• Fewer than 3 defecation per week

Definition• Patient Definition:
• Hard Stools
• Infrequent stools (<3 per week)
• Excessive straining
• Sense of incomplete bowel
emptying
• Excessive, unsuccessful time
spent on toiletRome 3
Must include at least 2 of the following
(1) At least 25% of bowel movements associated with
Straining
Lumpy or hard stools
Incomplete bowel evacuation
Anorectal obstruction
Need for manual manoeuvres
< 3 bowel movements per week
(2) Loose stools rarely present without the use of laxatives

Newborns• First meconium stool usually within the first 36 hours of birth in
normal newborns– 90% pass stool within 24 hours
• This may happen later in preterm infants without underlying structural defects
• First week of life normal newborn has 4 stools per day, with some variability– Breastfed infants can stool with each feeding or only once every
7 to 10 days– Formula fed infants tend to stool more regularly than breastfed
infants– Soy formulas known to cause harder stools– Protein Hydrolysate and Elemental formulas associated with
looser stools

Delayed passage of meconium
• Intestinal Obstruction / Anatomical Malformation
• Hirschsprung’s Disease• Meconium Ileus• Functional Ileus (Prematurity, Sepsis )• Small left colon• Maternal Drugs• Hypothyroidism,

Normal Frequency of Bowel Movements
Journal of Pediatric Gastroenterology & Nutrition. 43(3):e1-e13, September 2006.
Evaluation and Treatment of Constipation in Infants and Children: Recommendations of the North American Society for Pediatric Gastroenterology, Hepatology and Nutrition.

Constipation in Infants and Toddlers
At least two of the following present for at leastone month• Two or fewer defecations per week• At least one episode of incontinence after the
acquisition of toileting skills• History of excessive stool retention• History of painful or hard bowel movements• Presence of a large fecal mass in the rectum• History of large-diameter stools that may
obstruct the toilet

Infantile Dyschezia
In children less than 6 months old
• At least 10 minutes of straining and crying
• Successful passage of a soft stool
• Otherwise healthy and thriving

Constipation in Children 4-18 YO
Children with developmental age of at least 4 to 18 years Two of the following present for at least two months• Two or fewer defecations per week• At least one episode of fecal incontinence per week• History of retentive posturing or excessive volitional stool
retention• History of painful or hard bowel movements• Presence of a large fecal mass in the rectum• History of large-diameter stools that may obstruct the
toilet

Constipation is a symptom, not a disease
Some causes:
IBS,
Diabetes Mellitus, Hypothyroidism

Other Symptoms and Consequences of Constipation
Nausea +/- vomiting
Abdominal and Rectal pain
Flatulence
Loss of appetite
Lethargy
Depression
Nausea and reduced
appetite weight loss
Behavioral disturbances
Extra staff time needed for
increased toileting needs
Overall increased number
of medications in the
regime

Used in Clinical Trials
Correlates with symptoms of straining and difficult evacuation
Also correlates with colonic transit (Type 1 or Type 7 stool is correlated with slow or rapid colonic transit Degen LP, Phillips SF. How well does stool form reflect colonic transit? Gut
1996;39:109-113.
Majority of “constipated”patients have stools that are
Type 1-3
University of Bristol, Scand J Gastroenterol, 1997

Chronic constipation
• 3% of the visits to general pediatrics.
• 25% of the visits to pediatrics G.I.

Epidemiology:
The prevalence of childhood constipation
in the general population ranged from
0.7% to 29.6%
Maartje M. et al
Am J Gastroenterol 2006

Epidemiology:
constipation correlated with low maternal education, female sex, living in a large
community and having no older siblings.
JONAS F et. al. Acta Pædiatrica, 2006

Trend in family / Genetic
• Prominent family history of constipation.
• Identical twins have 6 times folds possibility than non identicals.

Functional vs. Organic -- Functional
• Over 95% of Constipated children has functional constipation– Functional: persistent, difficult, infrequent, or
seemingly incomplete defecation without evidence of underlying structural or metabolic defect
• Most commonly due to with-holding after a painful bowel movement
– Presents most commonly at three age periods» At introduction of cereals and solid foods» At toilet training» At the start of school

Functional vs. Organic -- Organic
• Accounts for less than 5% of all constipation– Anatomic malformations– Metabolic causes– Neuropathic conditions– Intestinal nerve and muscle disorders– Drugs– Hypotonia– Miscellaneous

Functional Constipation
• Classic History– Child has a painful bowel movement– When urge to have a bowel movement happens, the
child consciously withholds stool by contracting their external anal sphincter and gluteal muscles
• The child might rise on their toes, rock back and forth, stiffen their buttocks and legs, assume unusual postures, and often will hide in a corner
– Eventually, the rectum habituates to the stimulus of the enlarging fecal mass, the urge to defecate subsides, and the retentive behavior becomes almost second nature or subconscious
» Can develop soiling (encopresis)

Functional / non organic constipation
• Inappropriate toilet training• Anal fissure / Anusitis• Avoidance of response to nature call • Inconvenient / uncomfortable places • Behavioral• Vicious cycle of retention development.

Distinguishing Functional vs. Organic -- History
• Presentation in neonatal period more likely to be organic as compared to older children
• Clues from history (red flags)– Delayed growth– Delayed passage of meconium– Urinary incontinence or bladder disease– Passage of blood (unless attributable to an anal fissure)– Constipation from birth or very early infancy– Acute onset of constipation– Vomiting– Signs of systemic illness, multisystem involvement
• Recurrent respiratory infections– History of sexual, physical, or emotional abuse

Functional vs. Organic – Physical exam clues
• Abdominal distension• Findings of spinal dysraphism• Patulous anus• Absent cremasteric reflex (boys)• Absent anal wink• Pigmentation, dimples, or tufts of hair over lumbosacral region• Anorectal malformation• Anteriorly displaced anus• Sensory or motor defects of the lower extremities• Inability to insert a pinky in the anal canal• Gush of stool after a rectal exam upon which no stool is felt in the
rectal vault


Encopresis:
Incontinence of stool of non organic
Origin (rare before 3 years)

Nonretentive Fecal Incontinence
Must include all of the following in a childwith a developmental age at least 4 years
• Defecation into places inappropriate to the social context at least once per month
• No evidence of an inflammatory, anatomic, metabolic, or neoplastic process that explains the subject’s symptoms
• No evidence of fecal retention

Non retentive encopresis
• Soiling in the absence of fecal impaction or constipation
• Cause unknown• High correlation with attention deficit and
psychological comorbidities• Up to 40% were never fully toilet trained• Treatment
– Unfortunately limited• Psychologist• Regimented toileting schedule

Chronic constipation in children: Organic disorders are a major
cause A significant number of the children with
chronic treatment-resistant constipation may
have organic causes (slow colonic transit and
outlet obstruction) and suggests new
approaches to the management of children
with chronic treatment-resistant constipation. BR Southwell et al J. Paediatr. Child Health (2005)

Stool withholding presenting as a cause of non-epileptic seizures
Anthony Cohn Developmental
Medicine and Child Neurology; Oct 2005

chronic constipation and food hypersensitivity
An increasing number of reports suggest a
relationship between refractory chronic
constipation and food allergy in children.
CARROCCIO & G. IACONO
Alimentary Pharmacology & Therapeutics 2006


Evaluation

Evaluation
• History.
• Physical examination.

History:• Meconium passage.
• Frequency of bowel movement.
• Diet.
• School / travel.
• Painful defecation.
• Family history.
• FTT.

History-taking and physical examination
• Red flags– Constipation from birth/first few weeks of life– Delayed meconium– Ribbon stool– Locomotor/leg symptoms– Abdominal distension with vomiting
• Amber flags– Faltering growth– Concerns over well-being

Physical examination
• Inspection– Abnormal appearance/position/patency of anus
• Abdominal examination– Gross abdominal distension
• Spine/lumbosacral region/gluteal examination– abnormal
• Lower limb– Deformity/abnormal neuromuscular exam/abnormal
reflexes

Physical examination:
• Growth
• Abd. Distention
• Fecal mass felt on abd. exam.
• Rectum full of stool
• Fecal soiling.
• Anogenital index


Anogenital index:
Distance in centimeters:
from the vagina or scrotum to the anus
_______________________________
from the vagina or scrotum to the coccyx.
Females: 0.39 ± 0.09,
Males: 0.56 ± 0.2.


Physical examination:
• Anal fissure / anusitis.
• Signs of trauma (abuse).
• Signs of spinal defects( spina bifida)
• Neurological assessment of L.L. and anal wenk

Myelomeningocele

Spina bifida

Tethered cord syndrome

Neurofibromatosis


Investigations

Investigations:
Non is required routinely.

Investigations:
• Plain abdominal X RAY. ( obese child or refusing exam)
• Lumbosacral X RAY / MRI
• Ba. Enema
• Rectal biopsy.
• T4, Na, K, Osmolality.

Investigations:
• Anorectal manometry.
• Anal sphincter EMG.
• Defecography.
• Colorectal transit study.

Investigate possible underlying causes
• Red flag: don’t treat, URGENT referral• Amber flag:
– Faltering growth: treat, test for coeliac and hypothyroidism– Maltreatment: treat constipation and refer to ‘When to suspect
child maltreatment’
• As a GP • Shouldn’t do: rectal biopsy, manometry, , endoscopy,
transit studies


Management

Management:
• Education.
• Disimpaction.
• Maintenance.
• Behavioral modification.

Education
• Family friendly explanation of constipation
• Reassure that this is not a willful or defiant behavior
• Maintain consistent, positive, supportive attitude
• Avoid punishment
• Establish a reward system


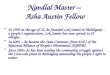
Toilet Hygiene
Dynamicsof the
AnorectalAngle
Anorectal Angle in Action
• Twice a day for 10-15 minutes after breakfast and dinner– Gastrocolic reflex
• Sit up straight
• Thighs parallel to ground
• Good foot support
• Valsalva maneuver to increase abd pressure
– Blow up balloon
• No distractions
• Reasonable reward system

Disimpaction
• Impaction – a hard mass in the lower abdomen identified during
physical examination, or– A dilated rectum filled with a large amount of stool on
rectal exam, or– Excessive stool in the colon identified by radiography
• Disimpaction– Oral– Rectal– Oral and Rectal
• Best determined after discussion with family– Manual

Disimpaction• LCH approach
– High dose Polyethylene Glycol (Miralax)• Age 1-2
– 2 teaspoons of Miralax with 4 oz of clear liquid and drink repeat every hour until stool is clear
• Age 3-5– 4 capfuls of Miralax in 24 ounces of Gatorade given 4 oz q 30 – 60
minutes until gone• Age 6-11
– 6 capfuls of Miralax in 32 oz of Gatorade given 4 oz q 30-60 minutes until gone
• Age 12 and older– 8 capfuls of Miralax in 32 oz of Gatorade given 4 oz q 30-60 minutes
until gone– Stimulant laxative
• Age 3-11– Bisacodyl 5 mg at beginning and end of cleanout
• Age 12 and up– Bisacodyl 10 mg at beginning and end of cleanout

Maintenance:
• Mieral oil (paraffin oil); 1-3 ml/kg/day
• Polyethylene glycol (PEG 3350) electrolyte free; 1 g/kg/day

Maintenance:
• Lactulose, Mg hydroxide, Sorbitol, others have been used
• On and off laxatives e.g. Senna

Maintenance:
• In case of anal fissure, apply petroleum gel to anal area frequently

Diet
• Controversial whether dietary changes can treat constipation
• Mild constipation– Increase fluid intake– Increase fiber intake
• Goal is age + 5 in grams per day
• Mild to severe constipation– Diet alone unlikely to treat constipation
• Role of excessive cow’s milk intake– controversial

Maintenance:
Increase dietary fibers
• Prune ((قراصيه• Pear juice
• Apple juice

A comparative study: The efficacy of liquid paraffin and Lactulose in
management of chronic functional constipation
Liquid paraffin is more effective in the treatment
of children with constipation.
NAFIYE URGANCI et al
Pediatrics International (2005)

• Similar to that of Children > 1 YO
• Differences– If delayed passage of meconium
• Refer to Pediatric GI or Surgery for rectal biopsy– If rectal biopsy normal – sweat test
– 1st line treatment can be diet alone• Prune or apple juice, 2-4 ounces a day
Management and treatment of Constipation -- < 1 YO

Goals of treatment
• 1 to 2 soft (mashed potato or soft ice cream) consistency stools per day
• Resolution of soiling
• Return of rectal sensation
• Empowerment of child
• Make defecation a positive experience

Non absorbed sugars
• Juices– Prune– Apple– White grape juice
• Increase osmotic load and draw water into bowel
• OK to use after roughly 2 mo of age

Behavioral modification:
• Regular toilet habit (after meals)
• Keep diary and record (use calendar and stars)
• Motivation (avoid negative comments)

Consultation with specialist:
• Pediatric G.I. (Celiac disease, etc.)
• Endocrine (hypothyroidism, etc.)
• Nephrology (diabetes insipidus)
• Pediatric surgery (Herschsprung)

Pediatric GI
• After referral is made– Determine appropriate workup
• Vast majority of referral patients can be managed without much diagnostics
• When refractory to treatment, consider further workup
– Anorectal manometry– Barium enema– Spine MRI– Radio-opaque marker studies– Full thickness rectal biopsy– Colonic manometry

Biofeedback:
Lack of coordinated relaxation of
external sphincter while defecation
On manometry



Biofeedback:
There is no evidence that biofeedback
training adds any benefit to conventional
treatment in the management of
functional fecal incontinence in children
Brazzelli, M et al
The Cochrane
Library, Copyright 2006

Long-Term Outcome of Functional Childhood Constipation
Childhood constipation appears to be a
predictor of IBS in adulthood.
Seema Khan et al Digestive
Diseases & Sciences; Jan 2007

Surgical causes
• Hirschsprung disease
• Anorectal malformation
• ectopic anus/ anocutaneous fistula
• Spinal dysraphism
• Rectal prolapse
• Perianal infection

Delayed passage of meconium
• Intestinal Obstruction / Anatomical Malformation
• Hirschsprung’s Disease• Meconium Ileus• Functional Ileus (Prematurity, Sepsis )• Small left colon• Maternal Drugs• Hypothyroidism,

Other Metabolic Causes of Constipation
• Celiac disease
• Hypothyroidism
• Cystic Fibrosis
• Botulism
• Hypokalemia / Hypercalcemia
• Lead poisoning

Clues to Hirschsprung’s disease
• Aganglionic bowel extending for variable lengths from the internal anal sphincter – 75-80% confined to rectosigmoid– Incidence about 1:5000– Male to female 4:1– Almost exclusively a disease of full term
infants– 80-90% diagnosed within first 3 years
• Mean age of diagnosis is 2.6 months

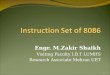
Barium enema for Hirschsprung’s
Transition zone


Treatment of HD
• Confirm by
• Barium enema
• Rectal biopsy
• Treatment
• Surgical intervention

Anorectal malformation
• Diagnosed on clinical examination
• Treatment
• surgical intervention according to the type of lesion


Myelomeningocele

Colonic motility disorderThis is very difficult to diagnosis

Colonic Manometry

Colonic Manometery

Anorectal Manometry

Anorectal Manometry
RAIR Study
• Internal anal sphincter relaxation in response to rectal distension– Volume incremental

What you think

Thank you

Case 1
3 YO male with infrequent, hard bowel movements. Stools can clog the toilet. He has a normal physical and is thriving?
--What is the diagnosis
--Is any workup indicated
--What is the treatment?

Case 2
18 month old femaleConstipation, abdominal distension, poor
growth, frequent wheezing and chronic cough
Mom can not remember if she passed meconium within 1st day of life
What is the differential diagnosis?Would you do any workup?

Case 3
3 month old male, full term infant
Abdominal distension, poor growth, has developed vomiting
Rectal exam – can not get pinky into anal canal
Differential diagnosis?
Workup?

Case 4
• 3 YO female. Was doing well until about 9 months of age, then started to fall off growth curve. Has distended abdomen, extremity wasting, no history of respiratory infection.
Differential diagnosis
Workup?

Case 5
• 2 YO female with constipation since birth
• Did pass meconium on day of life 1
• No abdominal distension, normal growth
• Physical exam reveals a pit over the lumbosacral area with hair covering it?
• Differential diagnosis
• Workup

Question 1
• What is the appropriate screening test for celiac disease– A. Anti gliadin antibody– B. HLA DQ2-DQ8 genotype– C. Ttg IgG and serum IgA– D. Ttg IgA and serum IgA– E. TgG Iga alone

Question 2
• Infantile dyschezia is straining with passage of soft bowel movements in babies up to _____ months old.– A. 3– B. 6– C. 9– D. 12– E. 15

Question 3
• The presence of meconium ileus is almost pathognomonic for– A. Hirschsprung’s disease– B. Infant of diabetic mother– C. Ileal atresia– D. Cystic Fibrosis– E. Hypothyroidism

Question 4
• Which of the following home remedies is strongly discouraged for fecal disimpaction– A. Milk and Molasses enema– B. Soap Suds enema– C. Tap Water enema– D. All of the above– E. None of the above

Question 5
• The following tests should be routinely performed in all constipated children– A. TSH– B. Sweat test– C. Basic metabolic panel– D. All of the above– E. None of the above