Embed Size (px)
Citation preview

540 American Society of Hematology
Consultations on Patients with Venous or Arterial Diseases
Barbara M. Alving, Charles W. Francis, William R. Hiatt, and Mark R. Jackson
Advances in vascular biology and drug develop-ment, as well as improved interventional tech-niques, are yielding multiple new treatments forpatients with venous and/or arterial thrombosis.Hematologists who are providing consultations forthese patients often participate in a multi-disciplinary approach to provide optimal care.New anticoagulants, simplified and validated testsfor detecting vascular disease, and improvedinterventional procedures can all reduce themorbidity and mortality that result from venousand arterial thrombosis. In this chapter, differentaspects of the diagnosis and treatment of thesedisorders are addressed by a hematologist, anexpert in vascular medicine, and a vascularsurgeon.
The key to the prevention and treatment ofvenous and arterial thrombosis is anticoagulantand antiplatelet therapy. In Section I, Dr. CharlesFrancis, a hematologist with expertise in thrombo-sis and hemostasis, describes the clinical trialsthat have resulted in the approval of newer antico-agulants such as fondaparinux and the thrombin-
specific inhibitors. He also reviews the clinicaltrials that have shown the efficacy of the new oralanticoagulant ximelagatran. Although currentlyunder study primarily for the prevention andtreatment of venous thrombosis, these anticoagu-lants are likely to undergo evaluation for use inarterial thrombosis.
Peripheral arterial disease (PAD), whichaffects as many as 12% of individuals over the ageof 65 years, provides a diagnostic and therapeuticchallenge to physicians across multiplesubspecialties. Dr. William Hiatt, a specialist invascular medicine, discusses in Section II theepidemiology and manifestations of PAD, the bestways in which to diagnose this disorder anddetermine its severity, and the most appropriatepharmacologic treatment.
In Section III, Dr. Mark Jackson, a vascularsurgeon, describes interventional procedures thathave been developed or are under development totreat arterial thrombosis. He also reviews thestatus of inferior vena caval filters that are retriev-able.
I. NEWER ANTICOAGULANT AGENTS FOR THE
CONSULTANT ’S TOOLBOX
Charles W. Francis, MD*
Clinical need and rapid scientific progress are the twopowerful forces driving the rapid development of newanticoagulant drugs. Knowledge of the biochemistryof hemostasis has rapidly expanded in recent years withcharacterization of the structures and details of inter-action of the proteins involved. This knowledge per-mits rational design of specifically targeted drugs andbetter prediction of anticoagulation effects. Drug de-velopment is also driven by the great burden of throm-botic disease, which represents the major cause of mor-
bidity and mortality in developed countries. Before theintroduction of low-molecular-weight heparins(LMWH), warfarin and heparin were the only two drugsavailable, but the introduction of new anticoagulantdrugs has been rapid and is accelerating. The focus ofthis review is the several recently introduced specificfactor Xa and thrombin inhibitors (Table 1). These dif-fer fundamentally from previously available anticoagu-lants because they are synthetic and also are targetedto inhibit a specific enzyme in the coagulation systemrather than to affect multiple factors (Figure 1). Thehematologists’ “tool box” will certainly expand rap-idly, as there are a variety of novel agents in develop-ment targeting these and other sites in the coagulationsystem. Broad application of these new agents requiresthat they meet important clinical needs. Thus, the wide-spread application of low-molecular-weight heparins(LMWH) resulted from their simplicity of dosing andsubcutaneous (SC) administration in comparison with
* University of Rochester Medical Center, 601 ElmwoodAvenue, Box 610, Rochester NY 14642-0001

Hematology 2003 541
Table 1. FDA-approved indications for new anticoagulants.
Anticoagulant FDA-Approved Indication for Use
Fondaparinux (Arixtra) Prophylaxis of venous thromboembolismin hip fracture, hip replacement,knee replacement
Lepirudin (Refludan) Heparin induced thrombocytopenia (HIT)
Argatroban HITHIT with percutaneous coronaryangioplasty
Bivalirudin (Angiomax) Percutaneous coronary angioplasty
Figure 1. Sites of action of new anticoagulants that inhibitspecific single enzymes in the coagulation system ratherthan acting at multiple sites as do heparin, low-molecular-weight heparin and warfarin.
the difficulties with intravenous adjusted-dose heparinfor treatment of venous thromboembolism (VTE). Thetwo parenteral direct thrombin inhibitors, argatrobanand lepirudin, have been successfully introduced to meetthe need for treatment of heparin-induced thrombocy-topenia (HIT).
The value of new anticoagulants is judged by theireffectiveness, safety, convenience, and cost in relationto the seriousness of the clinical problem. Their overalluse can be divided into short-term application for acuteproblems in hospitalized patients and long-term use inpreventing venous thrombosis or systemic emboliza-tion. In this latter group, there is a large unmet need foran alternative oral anticoagulant for warfarin, a drugthat has serious problems with monitoring, dose adjust-ment, and a narrow therapeutic margin. The secondmajor problem is safety, as all available agents can ei-ther cause or exacerbate bleeding in doses within thetherapeutic range, and a major challenge is to developnew anticoagulants with a greater margin of safety.
Expert management of anticoagulation is an im-portant and growing area for the consulting hematolo-gist, particularly in hospitalized patients who often de-velop difficult management problems due to concur-rent bleeding risks and comorbidities. The basis forsuccessful use of these newer anticoagulants is an un-derstanding of their principles, pharmacology, and theclinical trial results that demonstrate their value.
FondaparinuxFondaparinux (Arixtra) is a recently-approved antico-agulant that is novel in two respects: it represents a to-tally synthetic polysaccharide and it has specificity forfactor Xa. Fondaparinux is a pentasaccharide whosestructure is based on the minimal saccharide sequencein heparin that interacts with antithrombin to acceler-ate its activity. Whereas heparin and LMWH are het-
erogeneous and derived from animal sources, fonda-parinux is entirely synthetic with a uniform composi-tion. Binding of fondaparinux to antithrombin acceler-ates inhibition of factor Xa activity approximately 300-fold, but the short chain length renders it incapable ofinactivating thrombin, resulting in a specific Xa inhibi-tor with an activity of approximately 700 U/mg. Thiscontrasts with unfractionated heparin and LMWH,which have varying amounts of both anti-Xa and anti-thrombin activity. The effectiveness of fondaparinuxas an anticoagulant provides the first clear demonstra-tion that specific inhibition of factor Xa alone can pre-vent thrombosis.
Fondaparinux is completely absorbed following SCadministration with a peak concentration in 2 to 3 hoursand a half-life of 17 to 21 hours, allowing once dailyadministration. There is no significant metabolism, andmost drug is excreted unchanged through the kidneys.There is no appreciable interaction with platelets orplasma proteins, including platelet factor-4, suggest-ing that fondaparinux may be useful for patients withHIT. Fondaparinux does not induce release of tissuefactor pathway inhibitor and does not affect plateletfunction or fibrinolysis. It is not neutralized by prota-mine sulfate, and there is no specific agent for reversal.It has minimal effects on the prothrombin time (PT)and activated partial thromboplastin time (aPTT); al-though not recommended routinely, plasma levels canbe measured using an anti-Xa assay employingfondaparinux as the reference.
The clinical development of fondaparinux has fo-cused primarily on prevention and treatment of VTE,and several large Phase III studies have been completed(Table 2). A dose of 2.5 mg SC once daily was veryeffective in prophylaxis of VTE following hip replace-ment, with total rates of 4.1% and 6.1%, which com-pare favorably with those in other large trials. The

542 American Society of Hematology
fondaparinux results in the Ephesus Study1 were sig-nificantly better than enoxaparin using the Europeanregimen, in which enoxaparin was administered pre-operatively, but there was a nonsignificant differencein the groups in the Pentathalon Study2, which usedenoxaparin twice daily beginning postoperatively, theregimen which is used in North America. The resultswith fondaparinux in hip fracture3 and knee replace-ment4 were superior to enoxaparin, and the Penthifra-Plus5 study of prolonged prophylaxis demonstrated avery low rate of 1.4% at 28 days. The surprising find-ing in that study was a high rate of 35% in the groupthat received fondaparinux for only 7 days. A meta-analysis of the 4 trials7 found a relative risk reductionfor VTE of 55% compared with enoxaparin with a com-parable effect across all types of surgery and subgroups,but major bleeding occurred more frequently in thefondaparinux groups. An important contribution to itshigh efficacy may be that fondaparinux was started 6
hours postoperatively, a time that optimizes effective-ness while minimizing bleeding complications.8
Enoxaparin was begun at least 12 hours before or aftersurgery in the comparison groups.
Studies of deep venous thrombosis (DVT) and pul-monary embolism (PE) treatment have been completedand presented in abstract form6 (Table 2). Both studiesused a fondaparinux dose of 7.5 mg once daily but dif-ferent comparators. In the Matisse PE trial, patients wereinitially treated with heparin followed by warfarin,whereas enoxaparin was used for initial treatment inthe Matisse DVT trial. The rates of recurrence werecomparable at 3.8% and 3.9%, respectively, close tothe rates in the comparator groups and met statisticalcriteria for noninferiority. There was no significant dif-ference in bleeding complications, which were low.
Because fondaparinux excretion is renal, increaseddrug levels can occur with renal impairment resultingin bleeding complications. Dose reduction and moni-
Table 2. Fondaparinux Phase III trials.
MajorGroup Study Name Treatment n VTEd P Bleeding P
Orthopedic Surgery Prophylaxis
Hip replacement Ephesus1 fondaparinuxa 908 4.1% < .0001 4.1%
enoxaparinb 919 9.2% 2.8% NS
Hip replacement Pentathalon2 fondaparinuxa 787 6.1% NS 1.8% NSenoxaparinc 797 8.3% 1.0%
Hip fracture Penthifra3 fondaparinuxa 626 8.3% < .001 2.2% NS
enoxaparinb 624 19.1% 2.3%
Knee replacement Pentamarks4 fondaparinuxa 361 12.5% < .001 2.1% < .01
enoxaparinc 363 27.8% 0.2%
Hip fracture Penthifra-Plus5 fondaparinux 7da 35.0% < .001
fondaparinux 28da 1.4%
Treatment of DVT and PE
Pulmonary embolism Matisse PE6 fondaparinuxe 1103 3.8% NS 1.3% NS
heparinf 1110 5.0% 1.1%
Deep vein thrombosis Matisse DVT6 fondaparinuxe 1098 3.9% NS 1.1% NS
enoxaparing 1107 4.1% 1.2%
Abbreviations: DVT, deep venous thrombosis; NS, not significant; PE, pulmonary embolism; VTE, venous thromboembolism.a2.5 mg SC qd starting 6 hrs post-opb40 mg SC given 12 hours pre-op and then dailyc30 mg SC q12h starting 12-24 hours post-opdVTE was determined by venography in prophylaxis studies.e7.5 mg SC qdfIV adjusted-doseg1 mg/kg SC q12h

Hematology 2003 543
toring plasma levels may be needed in patients withrenal impairment and in the elderly, even if renal im-pairment is not evident. Elevated drug levels can occurin patients of low body weight; fondaparinux shouldalso be used with caution with neuraxial anesthesia.
Small clinical studies have also evaluated the useof fondaparinux in the management of coronary arterydisease. The Pentalyse trial compared fondaparinuxwith unfractionated heparin as an adjunct to fibrinoly-sis in 333 patients with ST-elevation myocardial inf-arction in doses from 4 to 12 mg daily for 5 to 7 dayswith no significant difference in angiographic out-comes.9 Four different doses of fondaparinux were alsoinvestigated in the Pentua trial in 929 patients with acutecoronary syndromes in comparison with enoxaparin.No clear dose response was found.10 Fondaparinux doesnot react with platelet factor-4; it may therefore be auseful alternative to heparin in the treatment of patientswith HIT, but clinical trials have not been reported.
Direct thrombin inhibitorsThrombin may be viewed as the central enzyme in he-mostasis, and it has been a key target in developmentof new anticoagulant drugs. Although its major actionis often viewed as conversion of fibrinogen to fibrin,thrombin has other prothrombotic actions through feed-back amplification, activation of factor XIII, and plate-let activation. Other important functions include ananticoagulant effect through activation of protein C,inhibition of fibrinolysis through activation of throm-bin activatable fibrinolysis inhibitor, and a variety ofeffects on endothelial and vascular smooth muscle cells.Thrombin is inhibited physiologically through anti-thrombin, and this forms the basis for the pharmaco-logical effectiveness of both heparin and LMWH.
Direct thrombin inhibitors block the enzymaticaction of thrombin without the need for antithrombinor other cofactors. Detailed structural studies of throm-bin including resolution of its crystallographic struc-ture have led to the development of novel direct throm-bin inhibitors for therapeutic use including lepirudin,bivalirudin, argatroban, melagatran, and ximelagatran.Direct thrombin inhibitors have several potential ad-vantages over anticoagulants that act through antithrom-bin. They show little interaction with plasma proteinsor blood cells, resulting in predictable pharmacokinet-ics and anticoagulant response, and their activity is notreduced when antithrombin levels are low. They arealso able to inhibit thrombin bound to fibrin or fibrindegradation products because of their small size,whereas the large heparin-antithrombin complex doesnot completely inhibit thrombin bound to fibrin or tocells, thus allowing it to maintain coagulant activity.11
HirudinHirudin is the native anticoagulant polypeptide in theleech, and the structure is slightly modified in the bio-synthetic molecule lepirudin (Refludan), which bindstightly and nearly irreversibly to the catalytic site andexosite 1 of thrombin, resulting in prolonged antico-agulant action. In patients with normal renal function,lepirudin has a half-life of 1 to 3 hours and results indose-dependent prolongation of the aPTT, PT, andthrombin time after intravenous administration. Therapyis typically monitored and the dose adjusted based onthe aPTT. Formation of antilepirudin antibodies mayoccur and result in decreased drug clearance and anincreased anticoagulant effect.12 No specific antidoteis available to neutralize its activity, although case re-ports indicate that dialysis may be useful.13
ArgatrobanArgatroban is a synthetic derivative of arginine thatbinds reversibly to the active site of thrombin. It is ad-ministered intravenously and has a short half-life ofapproximately 45 minutes with hepatic metabolism.Therapy is monitored and the dose is adjusted accord-ing to the aPTT. No specific antidote is available, butthe drug is rapidly cleared except in patients with poorhepatic function.
Heparin-induced thrombocytopeniaThe direct thrombin inhibitors show no immunologiccross-reactivity with the antibodies responsible for HIT,and both lepirudin and argatroban are approved by theFDA for treatment of HIT. Approval was based on smallclinical studies using historical controls that showed areduced rate of adverse clinical outcomes.14-17 Argatro-ban is also approved for percutaneous coronary inter-ventions in patients with HIT, based on a small studyshowing satisfactory outcomes.18 Both agents are ef-fective, but argatroban is a better choice in patients withrenal compromise, whereas lepirudin is a better choicein patients with hepatic dysfunction. Both drugs aregiven intravenously with doses titrated to achieve anaPTT 1.5 to 3 times the initial baseline. Because bothprolong the PT as well as the aPTT, monitoring the con-version to warfarin can be problematic. Managementof patients with HIT who require urgent surgery withcardiopulmonary bypass is difficult, although bivali-rudin,19 recombinant hirudin,20 and argatroban21 haveall been used with success.22
BivalirudinBivalirudin (Angiomax) is a small peptide whose struc-ture was engineered based on naturally occurring hiru-din. The domain that inhibits the active site of throm-
544 American Society of Hematology
bin is connected by 4 glycine residues to a dodeca-peptide that interacts with a thrombin exosite.23 Fol-lowing parenteral administration, the half-life is ap-proximately 30 minutes with dose-dependent prolon-gation of the aPTT and activated clotting time (ACT),and elimination through both liver and kidney. In 2000,the FDA approved bivalirudin in combination with as-pirin for patients with unstable angina who were un-dergoing percutaneous transluminal coronary angio-plasty (PTCA); approval was based largely on trialsperformed several years earlier.24 The development ofthe direct thrombin inhibitors for coronary indicationshas been difficult, and early studies were equivocal orshowed excess bleeding.25 The recently-reported RE-PLACE 2 trial evaluated bivalirudin in patients need-ing urgent or elective percutaneous coronary interven-tion and included the use of heparin and a GP II
bIII
a
receptor inhibitor.26 In a composite primary end pointof death, myocardial infarction, urgent repeat re-vascularization, or major bleeding by 30 days, the useof bivalirudin with provisional GP II
bIII
a receptor block-
age was not statistically inferior to heparin plus plannedGP II
bIII
a receptor blockage. Bleeding complications
were somewhat less with bivalirudin, but this advan-tage was mostly related to a reduction in minor bleed-ing. Bivalirudin and other direct thrombin inhibitorsneed further evaluation in the setting of acute coronarysyndromes.27
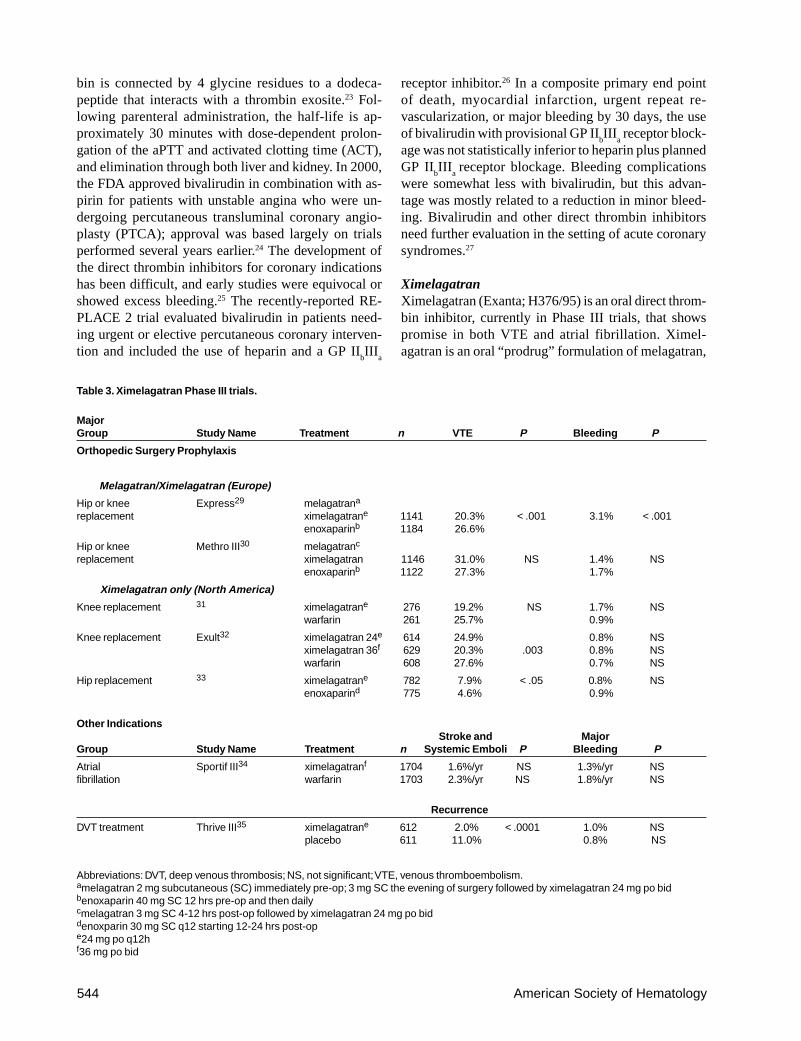
XimelagatranXimelagatran (Exanta; H376/95) is an oral direct throm-bin inhibitor, currently in Phase III trials, that showspromise in both VTE and atrial fibrillation. Ximel-agatran is an oral “prodrug” formulation of melagatran,
Table 3. Ximelagatran Phase III trials.
MajorGroup Study Name Treatment n VTE P Bleeding P
Orthopedic Surgery Prophylaxis
Melagatran/Ximelagatran (Europe)
Hip or knee Express29 melagatrana
replacement ximelagatrane 1141 20.3% < .001 3.1% < .001enoxaparinb 1184 26.6%
Hip or knee Methro III30 melagatranc
replacement ximelagatran 1146 31.0% NS 1.4% NSenoxaparinb 1122 27.3% 1.7%
Ximelagatran only (North America)
Knee replacement 31 ximelagatrane 276 19.2% NS 1.7% NSwarfarin 261 25.7% 0.9%
Knee replacement Exult32 ximelagatran 24e 614 24.9% 0.8% NSximelagatran 36f 629 20.3% .003 0.8% NSwarfarin 608 27.6% 0.7% NS
Hip replacement 33 ximelagatrane 782 7.9% < .05 0.8% NSenoxaparind 775 4.6% 0.9%
Other IndicationsStroke and Major
Group Study Name Treatment n Systemic Emboli P Bleeding P
Atrial Sportif III34 ximelagatranf 1704 1.6%/yr NS 1.3%/yr NSfibrillation warfarin 1703 2.3%/yr NS 1.8%/yr NS
Recurrence
DVT treatment Thrive III35 ximelagatrane 612 2.0% < .0001 1.0% NSplacebo 611 11.0% 0.8% NS
Abbreviations: DVT, deep venous thrombosis; NS, not significant; VTE, venous thromboembolism.amelagatran 2 mg subcutaneous (SC) immediately pre-op; 3 mg SC the evening of surgery followed by ximelagatran 24 mg po bidbenoxaparin 40 mg SC 12 hrs pre-op and then dailycmelagatran 3 mg SC 4-12 hrs post-op followed by ximelagatran 24 mg po biddenoxparin 30 mg SC q12 starting 12-24 hrs post-ope24 mg po q12hf36 mg po bid

Hematology 2003 545
which is the active thrombin inhibitor. Melagatran isbeing developed in Europe as a parenteral direct throm-bin inhibitor. It is a dipeptide whose structure mimicsthe sequence immediately N-terminal to the thrombincleavage site on the Aα chain of fibrinogen. Melagatranis very selective for thrombin with minimal activity to-ward other relevant serine proteases. Because of itssmall size and high affinity, it inhibits clot-bound aswell as free thrombin. Absorption is nearly completeafter SC administration, reaching a maximum after 30minutes with a half-life of approximately 1.6 hours.Clearance is primarily renal with over 80% excretedunchanged. Following oral administration, ximelagatranis rapidly absorbed and yields melagatran as its mainmetabolite with maximum plasma concentrations ofmelagatran between 1.5–2 hrs and a half-life of approxi-mately 3 hours. Plasma concentrations of melagatranare linearly related to ximelagatran doses with low in-ter- and intra-individual variability. There appear to beno significant food or drug interactions. The thrombintime, PT, and aPTT are all prolonged after administra-tion of ximelagatran and other direct thrombin inhibi-tors, but monitoring with the ecarin clotting time mayalso be useful, especially for elevated drug levels suchas are needed during cardiopulmonary bypass surgery.28
Clinical studies have excluded patients with poor renalfunction because the drug is excreted renally.
Melagatran and ximelagatran are not approved forclinical use but are in advanced Phase III clinical trials(Table 3). Several large studies have been published orreported in prevention of VTE after orthopedic surgerywith different approaches in Europe compared withNorth America. The European Express29 and MethroIII 30 studies used an initial dose of melagatran to pro-vide rapid anticoagulation, and this treatment was fol-lowed by oral ximelagatran. In the Express study, 2 mgof melagatran was given SC immediately before sur-gery, another 3 mg on the evening of surgery, followedby ximelagatran 24 mg orally twice daily. This regi-men had superior efficacy to the enoxaparin compara-tor, but there was also an increase in major bleedingdefined as “excessive bleeding as judged by the inves-tigator.” A modified regimen was used in Methro III,which started ximelagatran 3 mg SC 4 to12 hours aftersurgery followed by 24 mg of ximelagatran orally twicedaily.30 This study showed comparable efficacy andsimilar bleeding results to enoxaparin. Notably, the Eu-ropean studies have combined hip and knee replace-ment subjects together for primary analysis.
The North American program in orthopedic pro-phylaxis has differed, with separate studies for kneeand hip replacement and use of oral ximelagatran only.The initial dose of 24 mg twice daily was chosen after
a Phase II study compared ximelagatran in several dosesto enoxaparin after knee replacement in 594 patients.36
A dose-response effect on efficacy or safety was notestablished, but the 24 mg dose was comparable in ef-fectiveness and safety to enoxaparin and was chosenfor initial studies. The initial Phase III study in kneereplacement31 compared ximelagatran with warfarin andshowed comparable efficacy and safety. A study in hipreplacement compared ximelagatran 24 mg twice dailywith enoxaparin.33 Designed to show noninferiority, thisstudy demonstrated that enoxaparin was better thanximelagatran at this dose with no difference in bleed-ing end points. Based on these 2 studies, the dosingwas reevaluated, and a larger study in knee replace-ment was performed comparing 24 and 36 mg twicedaily with warfarin after knee replacement. The resultswith 24 mg were similar to warfarin and comparablewith that reported previously, whereas efficacy withximelagatran 36 mg twice daily was significantly bet-ter than with warfarin with comparable bleeding.32
Overall, the results with the oral ximelagatran only pro-gram are mixed, and dependent on dosing, type of sur-gery, and choice of comparator. The knee replacementstudies are encouraging and suggest that the lower, 24mg dose, is comparable with warfarin, whereas the 36mg dose is superior.
Studies with long-term ximelagatran treatment ofestablished DVT include the Thrive II and V study thatcompared standard treatment with enoxaparin (followedby adjusted-dose warfarin) to a regimen of ximelagatran36 mg twice daily as both initial and chronic therapy.37
The results have yet to be reported in detail. The ThriveIII study examined 1233 patients with VTE who re-ceived 6 months of initial anticoagulation and then wererandomized to receive either ximelagatran (24 mg twicedaily) or placebo for another 18 months.35 The resultsshowed a clear benefit for prolonged treatment withximelagatran, with recurrence in significantly fewerpatients than in those assigned to placebo (P < .0001).
Treatment of patients with atrial fibrillation to pre-vent stroke is a common indication for long-term war-farin anticoagulation and the subject of the large SportifIII study.34 Patients with atrial fibrillation and 1 or moreadditional risk factors for stroke were randomized inan open-label study with blinded adjudication to treat-ment with adjusted-dose warfarin or ximelagatran 36mg twice daily to establish noninferiority. The inten-tion-to-treat analysis of the primary efficacy end pointof stroke and systemic embolism showed 40 events inthe ximelagatran group (1.6%/yr) and 56 events (2.3%/yr) in the warfarin group, indicating noninferiority. Anon-treatment analysis showed a significantly better out-come in the ximelagatran group. There were no differ-

546 American Society of Hematology
ences in major bleeding or all-cause mortality.The interpretation of studies of long-term therapy
with ximelagatran must consider the problem of tran-saminase elevations. Elevations of greater than 3 timesthe upper limit of normal of alanine aminotransferaseoccurred in 6.4% of ximelagatran-treated patients inThrive III and in 6.5% in Sportif III. The clinical impli-cations are unclear, as levels may decline to normalwith continued treatment. However, ongoing trials re-quire discontinuation of ximelagatran in participantswho develop marked or persistent transaminase eleva-tions; this side effect may eventually result in the needfor routine monitoring of liver function tests if ximel-agatran treatment is continued for longer than 30 days.
The potential clinical application of ximelagatranand melagatran will depend on the results of additionalstudies and regulatory review. A new oral anticoagu-lant would be welcome, and ximelagatran appears tohave comparable or better efficacy and safety thanwarfarin in short-term prophylaxis studies. Initial long-term studies with ximelagatran show promise, but limi-tations include the need for twice-daily administrationand monitoring of liver function. Additionally, no spe-cific agent to reverse the anticoagulant effect is avail-able, as is also true with other direct thrombin inhibi-tors. Given the short half-life of the drug, this is un-likely to be a problem unless ximelagatran is adminis-tered to patients with poor renal function.
Future DirectionsThe development of fondaparinux and direct thrombininhibitors has established that effective anticoagulationcan be provided with a drug specifically targeted to asingle enzyme in the coagulation system, representinga new therapeutic concept. The availability of multipledrugs targeting different enzymes raises the possibilityof combined therapy using several agents in individu-alized doses, based on the characteristics of a patient’shemostatic system or pattern of vascular disease andthrombosis. Many other new anticoagulant agents arein the early phases of clinical development and showpromise. Idraparinux is a parenteral antithrombin-de-pendent specific anti-Xa inhibitor similar to fonda-parinux but with a much longer half-life, allowing once-weekly administration. Heparin can be chemicallyderivatized to permit oral bioavailability and 1 suchagent, SNAC-heparin, has shown promise in prophy-laxis in orthopedic patients.38 NAPc2, an inhibitor offactor VIIa/tissue factor derived from the nematode,showed effectiveness in Phase II studies in thrombo-prophylaxis,39 and an oral anti-Xa agent has been inPhase II trials in orthopedic thromboprophylaxis. Otheragents targeting factor VIIa and factor IXa are being
developed, as are soluble thrombomodulin and otherdirect thrombin inhibitors.
SummaryThe availability of new anticoagulants is expandingchoices for prevention and treatment of thrombotic dis-ease. The synthetic pentasaccharide, fondaparinux, pro-vides excellent prophylaxis in orthopedic patients, andnew studies suggest it may have a role in treating DVTand PE with once-daily injections. Either argatrobanor lepirudin is an excellent choice for patients with HIT,with argatroban preferable in patients with renal com-promise and lepirudin in those with liver dysfunction.Bivalirudin should be considered for patients undergo-ing percutaneous coronary intervention and may offerthe advantage of reduced bleeding complications.Ximelagatran is not yet approved, but studies in atrialfibrillation, DVT treatment, and prophylaxis in ortho-pedic surgery suggest this new oral agent will be animportant anticoagulant.
II. E VALUATION OF PATIENTS WITH
PERIPHERAL VASCULAR DISEASE
William R. Hiatt, MD*
Peripheral arterial disease (PAD) of the arterial circu-lation to the lower extremities is one of the major mani-festations of systemic atherosclerosis. The disease isinitially asymptomatic (patients are identified only bya reduced blood pressure in the ankle) but with pro-gression will cause exertional symptoms of intermit-tent claudication. In rare cases, the disease progressesto severe chronic leg ischemia which can result in limbloss. All patients with PAD have an increased risk ofcardiovascular morbidity and mortality. Thus, therapyis directed to both the limb and the systemic athero-sclerotic disorder. Venous thromboembolic diseases alsoaffect a large segment of the population, but have a dif-ferent pathophysiology from arterial disease. However,recent reports describe an association between theseconditions, suggesting that many patients with sponta-neous venous thrombosis also have atherosclerosis inthe peripheral arterial circulation.1 Patients with primaryclotting disorders may therefore need assessment oftheir arterial circulation, with special attention to ad-dressing their cardiovascular risk.
* University of Colorado Health Sciences Center, 4200 East9th Avenue, Box 180, Denver CO 80262

Hematology 2003 547
EpidemiologyIn the Framingham study, both men and women had asimilar incidence of intermittent claudication, whichincreased with age, and had a peak incidence in olderindividuals of approximately 60 new cases per 10,000persons per year.2 When noninvasive screening instru-ments are used (the ankle/brachial index [ABI] de-scribed below), the prevalence of PAD is quite high,affecting 12% of the adult population and 20% of indi-viduals over the age of 70.3,4 These figures extrapolateto approximately 8 million persons affected with PADin the United States.
Patients with PAD are at high risk for concomitantcoronary and carotid arterial diseases, resulting in in-creased morbidity and mortality. For example, in pa-tients with PAD, the adjusted all-cause mortality risk isincreased 3-fold and cardiovascular mortality is in-creased 6-fold.5 This risk is approximately the samefor both men and women, and remains high even if thepatient has had no prior evidence of cardiovascular dis-ease.6,7 With increasing severity of PAD, as measuredby the ABI, there is a concomitant increased risk ofmyocardial infarction, ischemic stroke, and vasculardeath.8,9 Thus, the ABI provides important informationregarding the diagnosis and prognosis of PAD.
Clinical Evaluation and Differential DiagnosisChronic arterial insufficiency of the lower extremitycauses two very characteristic types of pain: intermit-tent claudication and ischemic rest pain. Claudicationdiscomfort most commonly involves the calf and is re-solved within 10 minutes of rest. In contrast, patientswith chronic critical limb ischemia typically presentwith rest pain in their distal foot that occurs at nightand is relieved with dependency. These patients are atrisk for developing painful ischemic ulcers at the distalpoints of the foot.
Palpation should be performed of the brachial,femoral, and pedal arteries. The location of the poste-rior tibial pulse is behind the medial malleolus, and thedorsal pedis pulse runs along the dorsum of the footbetween the first and the second metatarsal bones. Thegrading of pulses can be described as normally present(easily palpable), diminished (difficult to palpate), orabsent. Patients with a palpable femoral pulse, but ab-sent pedal pulses, typically have arterial disease con-fined to the leg, whereas a diminished or absent femo-ral pulse indicates disease of the aorta or iliac arteries(the inflow).
The differential diagnosis in these patients includesdiabetic sensory neuropathy that produces burning andnumbness in both feet at rest. Severe neuropathy canlead to chronic diabetic malperforans ulcers (these ul-
cers are usually on the plantar surface of the foot atpressure points). Patients with diabetic neuropathy mayhave normal pedal pulses, but even diabetic ulcers areoften associated with some degree of arterial occlusivedisease. Reflex sympathetic dystrophy may be presentafter trauma to the limb, and leads to a painful, discol-ored, swollen extremity. Patients with arteritis maypresent with ischemic limbs, particularly those withBuerger’s disease (thromboangitis obliterans). Claudi-cation-like symptoms may also arise from spinal steno-sis, which is due to osteophytic narrowing of the lum-bar neurospinal canal. These symptoms include numb-ness and weakness in the lower extremity that is pro-duced by standing. Patients with arthritis of the knee orhip may also have pain in the joint with ambulation,but also pain at rest or with weight bearing. Finally,patients with prior venous thrombosis can developvenous claudication. This is characterized by venousengorgement in the affected leg with walking that causesswelling and discomfort. Relief requires leg elevation.
Vascular TestingThe noninvasive evaluation of patients with PAD be-gins in the physician’s office. Patients considered at riskfor PAD are older, have cardiovascular risk factors ofsmoking or diabetes, or have exercise-induced legsymptoms. The initial evaluation includes a thoroughvascular history and physical examination, followed bythe measurement of an ABI.
Ankle/brachial indexPatients considered to be at risk for PAD should havean ABI. Patients considered for screening would bethose between the ages of 50-69 years who have a his-tory of smoking or diabetes, and all patients over theage of 70 years.10 In these patients, the prevalence ofPAD can be as high as 29%. Patients with exertionalsymptoms in their legs or foot ulcers should also havean ABI to determine if their symptoms are due to vas-cular disease. Performing an ABI allows the physicianto make the diagnosis of PAD, judge the severity of theleg arterial disease and risk of cardiovascular events,and identify patients with severe limitations in theirexercise capacity. Arteriography is not necessary tomake the diagnosis of PAD, but rather should be re-served for patients who are being considered forrevascularization therapy.
In order to perform an ABI, the physician needs ablood pressure cuff and a handheld Doppler. Figure 2demonstrates the locations of the ankle and arm cuffsto obtain the ABI. The higher of the two systolic bra-chial pressures is used as the denominator of the ABIcalculation. The higher of the two ankle pressures (ei-

548 American Society of Hematology
ther the dorsalis pedis or posterior tibial artery) is usedas the numerator of the ABI calculation for each leg. Anormal ABI is defined as a resting measurement ≥ 0.90.Any value < 0.90 represents the presence of PAD, withlower values indicating more severe disease. ABI val-ues < 0.40 suggest the most advanced stages of PAD,which can result in ischemic rest pain, nonhealing ul-cerations, and gangrene.
Vascular laboratory testing. The ABI is generallysufficiently accurate to determine the presence and se-verity of PAD. However, if the ankle tibial vessels arecalcified (patients with diabetes mellitus or end-stagerenal disease), an accurate ankle pressure cannot beobtained. The cuff pressures are typically greater than250 mmHg, or the ABI value is > 1.30, indicating non-compressible vessels under the cuff. If not recognizedas artificially high, the physician may falsely concludethat arterial circulation is adequate, or even normal, inthese patients. With high ABI values, other tests avail-able in the vascular diagnostic laboratory are neces-sary to make the diagnosis of PAD, including toe pres-sures, arterial duplex ultrasonography, and transcutane-ous oximetry (TcPO
2) to assess wound healing potential.
Occasional patients with classic symptoms of clau-dication may have a normal physical examination andABI at rest. This condition often reflects iliac arterystenosis with a normal distal circulation. In this case,exercise treadmill testing should be performed in thevascular diagnostic laboratory. Patients have restingpressures measured, and are then placed on a treadmillat a constant speed and constant grade of incline. The
patient is asked to report initial symptoms of limb dis-comfort, and then terminate the exercise when the dis-comfort is limiting, or after 5 minutes. After exercise,pressures are again measured. A significant decreasein postexercise pressures confirms the diagnosis of PAD.
If the treatment plan includes consideration forrevascularization, location of the arterial occlusive dis-ease is required. These tests include segmental limbpressures, pulse volume recordings, and arterial duplexultrasonography. The use of sequential limb blood pres-sure cuffs placed on the thigh, calf, and ankle providesa rough localization of the arterial segment(s) involved.11
Each vascular laboratory will have developed standardsfor determining significant changes in systolic bloodpressure between cuffs. For example, the pressure ob-tained in the proximal thigh cuff is normally > 30 mmHghigher than the brachial pressure. Lower pressures sug-gest the presence of inflow aortoiliac artery disease.These patients typically respond well to angioplasty interms of treatment success.
Pulse volume recordings (PVRs) are also obtainedfrom cuffs placed on the thigh, calf, and ankle that de-scribe arterial waveforms. In the normal setting, thiswaveform is similar in appearance to an intra-arterialpressure waveform. As the arterial circulation wors-ens, the PVR changes morphology and decreases itsamplitude. This methodology is often used when theABI is noncompressible, since the arterial waveformsare not affected by calcification.
Arterial duplex ultrasonography is a highly accu-rate examination, which may be performed from the
Figure 2. Measurement ofthe Ankle/Brachial Index.

Hematology 2003 549
aortic bifurcation to the ankles. Utilizing currently avail-able Duplex ultrasound scanners, arteries are visual-ized, often with color imaging, and Doppler velocitiesare obtained. A doubling in the peak systolic velocitysuggests a 50-99% stenosis. In patients who are in needof revascularization, this examination is as accurate asarteriography in predicting the optimal revascularizationmethod.
Functional assessmentPatients with claudication have a severe limitation inexercise performance and walking ability. The severityof this functional limitation should be determined as ameans to assess response to claudication therapies.12
Treadmill testing can be performed using a low-levelprotocol usually set at 2 mph and increasing the grade2% every 2 minutes until patients reach their individualmaximal claudication pain. In addition to treadmill test-ing, several questionnaire measures of functional sta-tus have been developed and validated in this patientpopulation. The walking impairment questionnaire(WIQ) is a disease-specific instrument that asks a se-ries of questions regarding the patient’s claudicationseverity and ability to walk defined distances, speeds,and stairs.12 This questionnaire is simple to administer,and has been shown to predict the response to claudi-cation therapies.13
Medical Management of Ischemic Risk
Risk factor modificationCigarette smoking is associated with a marked increasedrisk for peripheral atherosclerosis.4,14 The number ofpack years is associated with disease severity, an in-creased risk of amputation, peripheral graft occlusion,and mortality.15,16 Given these associations, smokingcessation has been a cornerstone of the management ofPAD. While advice to stop smoking is associated withmodest quit rates, pharmacologic therapy can assist insmoking cessation, including nicotine replacement andantidepressant drug therapy.17,18
Current recommendations for the management oflipid disorders in PAD are to achieve an LDL choles-terol level to less than 100 mg/dL and to modulate theincreased triglyceride and low HDL pattern.19 The datafrom the Heart Protection Study (HPS) provide the firstprimary data supporting the role of statin therapy inpatients with PAD.20 Simvastatin was associated with a12% reduction in total mortality, 17% reduction in vas-cular mortality, 24% reduction in CHD events, 27%reduction in all strokes, and a 16% reduction in non-coronary revascularizations. Similar results were ob-tained in the PAD subgroup, whether they had evidence
of coronary disease at baseline or not. Thus, the HPSdemonstrated that in patients with PAD (even in theabsence of a prior myocardial infarction or stroke),aggressive LDL lowering was associated with a markedreduction in cardiovascular events (myocardial infarc-tion, stroke, and vascular death).
Hypertension is an independent risk factor forPAD.4 Guidelines also support the aggressive treatmentof blood pressure in patients with atherosclerosis, indi-cating that PAD is equivalent in risk to ischemic heartdisease.21 Regarding specific drug choices, theangiotension-converting enzyme (ACE) inhibitor drugshave shown benefit beyond blood pressure lowering inhigh-risk groups. Results from the Heart Outcomes Pre-vention Evaluation study indicated that the ACE inhibi-tor ramipril was cardioprotective in patients at high risk,including those with PAD.22
Diabetes increases the risk of PAD approximately3- to 4-fold.4 While diabetes is highly associated withperipheral atherosclerosis, the degree of glycemic con-trol does not predict the severity of the peripheral ath-erosclerosis.23 These observations suggest that diabe-tes is a critical risk factor for PAD primarily in con-junction with other cardiovascular risk factors. Severalstudies in patients with type 1 and type 2 diabetes haveshown that aggressive blood glucose control does noteffectively prevent cardiovascular disease.24,25 Thus, itis increasingly important to control other cardiovascu-lar risk factors in patients with diabetes, including op-timal management of blood pressure and lipid disor-ders. A recent study demonstrated that in patients withdiabetes and PAD, intensive lowering of blood pres-sure with an ACE inhibitor or calcium channel blockerwas associated with a large reduction in the risk of car-diovascular events (myocardial infarction, ischemicstroke, and vascular death).26
Antiplatelet drug therapyAspirin is a well-recognized antiplatelet drug that reducesthe risk of cardiovascular events 25% in patients withcardiovascular diseases.27 What is remarkable is that spe-cific studies in the PAD population using aspirin have notshown a statistically significant reduction in cardiovas-cular events.28 Thus, while antiplatelet drugs are clearlyindicated in the overall management of PAD, aspirin doesnot have FDA approval in this patient population.29
In addition to aspirin, the thienopyridienes are animportant class of antiplatelet agents that have been wellstudied in patients with cardiovascular disease.Ticlopidene has been evaluated in several trials in pa-tients with PAD, and has benefit in reducing the risk ofmyocardial infarction, stroke and vascular death, butwith an unacceptable side effect profile.30 In contrast,

550 American Society of Hematology
clopidogrel has been shown to be highly effective inthe PAD population.31 Thus, current consensus docu-ments would recommend clopidogrel as an importantagent for patients with PAD and intermittent claudica-tion; clopidogrel may in fact be more effective thanaspirin alone.32
Treatment of Limb Symptoms
Exercise rehabilitation for claudicationThe use of a formal exercise program to treat claudica-tion is the best-studied and most effective nonsurgicaltherapy for claudication. This topic has been extensivelyreviewed.33 The most successful training regimens aresupervised in a cardiac rehabilitation environment andemploy repeated treadmill-walking exercise. The ini-tial evaluation should establish the baseline treadmillwalking time as described above. A typical supervisedexercise program is 60 minutes in duration and is moni-tored by a skilled nurse or technician. Patients shouldbe encouraged to walk primarily on a treadmill, sincethis most closely reproduces walking in the commu-nity setting. The initial workload of the treadmill is setto a speed and grade that brings on claudication painwithin 3-5 minutes. Patients walk at this work rate untilthey achieve claudication of moderate severity. Theythen rest until the claudication abates, and then resumeexercise. Patients should be reassessed clinically on aweekly basis as they are able to walk further and fur-ther at their chosen workload. The typical duration ofan exercise program is 3-6 months. This interventionwill allow patients to walk 100% to 150% farther andimprove their quality of life.
Drug therapy for claudicationPentoxifylline has been approved for the treatment ofclaudication since 1984. However, a meta-analysis con-cluded that although the drug produced modest in-creases in treadmill walking distance over placebo, theoverall clinical benefits were questionable.34 Cilostazolis currently the most effective drug for claudication.The primary action of cilostazol is to inhibit phosphodi-esterase type 3, which results in vasodilation and inhi-bition of platelet aggregation, arterial thromboses, andvascular smooth muscle proliferation. A recent meta-analysis demonstrated that the drug significantly im-proved both treadmill exercise performance and ques-tionnaire-assessed quality of life.13 Cilostazol shouldnot be given to patients with claudication who also haveheart failure. This is based on previous concerns of amortality risk with use of the phosphodiesterase inhibi-tor class of drugs in patients with heart failure.
Additional drugs for treating claudication are be-
ing studied in clinical trials. Propionyl-l-carnitine is ametabolic agent that has been shown to improve tread-mill performance and quality of life in patients withclaudication.35 Prostaglandins have been extensivelystudied in patients with PAD, but with mixed results.Therapeutic angiogenesis is also being studied withinitial positive results.36 However, these therapies arein their infancy.
III. I NTERVENTIONAL APPROACHES IN THE
MANAGEMENT OF THROMBOSIS
Mark R. Jackson, MD*
Arterial thrombosis is a major contributor to limb lossand amputation. Approximately 60,000 major limbamputations are performed annually in the US. Periph-eral arterial occlusive disease and arterial embolicevents are the primary underlying etiologies. Whileopen vascular surgery is the traditional gold standardfor major limb revascularization, the development ofnew endoluminal devices has resulted in rapid advancesin minimally invasive techniques for limb revascular-ization, most of which are performed percutaneously.Similar devices and techniques have also allowed “lessinvasive” variations of standard open surgical tech-niques of limb revascularization. This chapter will sum-marize these recent advances.
Just as newer interventional devices are being de-veloped for arterial thrombosis, new developments arealso occurring in the design of devices, such as inferiorvena cava filters, to prevent pulmonary emboli in well-defined, high-risk patients. Examples of these improve-ments will also be provided.
Arterial Interventions
Thrombolytic therapyThrombolytic therapy has been evaluated in numerousclinical trials involving patients with thrombotic orembolic occlusions of lower extremity arteries. Withthe initial use of systemic thrombolytic therapy (intra-venous) in the early 1970s, partial or substantial lysiswas observed in approximately 40% of patients, andno discernible lysis was observed in the remaining60%.1 Results were influenced by the duration of oc-clusion, and serious bleeding complications were ob-served in approximately one third of the patients.
Since the mid-1970s, regional or intra-arterial ad-
* Greenville Hospital System, 701 Grove Road, GreenvilleSC 29605

Hematology 2003 551
ministration of thrombolytic agent directly into the siteof clot has been the preferred approach.2 The rate ofsuccessful reperfusion (50% to 85%) appears higherthan with systemic thrombolytic therapy. Other advan-tages of the selective approach are that it provides use-ful diagnostic information (determination of embolicversus thrombotic occlusion) and allows simultaneousangiographic definition of the nature of vessel wall ab-normalities that would lead to rethrombosis if not cor-rected by surgery or balloon angioplasty. A major draw-back is that arterial catheterization is required for pro-longed periods (hours to days), leading to major bleed-ing and thromboembolic complications in 6% to 20%of patients3,4 and added costs, as this therapy requiresICU observation for signs or symptoms of bleedingduring thrombolysis. Despite this, intra-arterial throm-bolytic therapy appears superior to systemic treatment.Tissue plasminogen activator (tPA) and urokinase haveproven to be superior to streptokinase for peripheralarterial thrombolysis.5-7
Randomized trials have compared surgical throm-bectomy and thrombolytic therapy in patients with acutelower extremity arterial ischemia. A larger, multicentertrial compared intra-arterial thrombolytic therapy withurokinase or tPA with surgery in patients presentingwith acute lower extremity ischemia.8 The study wasstopped prematurely when an interim analysis showedthat patients randomized to surgery did significantlybetter than those given thrombolytic therapy. However,in patients presenting with symptoms of greater than 2weeks’ duration, surgery was superior; in patients pre-senting with symptoms of less than 2 weeks’ duration,amputation rates were lower with thrombolytic therapy.There was no difference in efficacy or safety betweentPA and urokinase.
In a multicenter trial of thrombolysis or peripheralarterial surgery (TOPAS), the role of thrombolytictherapy and surgical intervention in the setting of acuteischemia of the lower extremity was evaluated.9 In thisclinical trial, 213 patients were studied who had lowerextremity ischemia for up to 14 days. No differencewas observed in 1-year mortality or amputation-freesurvival in the urokinase-treated patients or those un-dergoing surgery. Open surgery was avoided in 45.8%of patients randomized to urokinase. The TOPAS in-vestigators recently published their follow-up study ofa total of 548 patients.10 Amputation-free survival at 6months was the same for both groups (urokinase, 71.8%;surgery, 74.8%). There was a significant increase inthe rate of major hemorrhage in the urokinase group com-pared with the surgery group; and 4 patients treated withurokinase sustained intracranial hemorrhage, one of whichwas fatal. The only apparent benefit of urokinase was
that fewer patients required standard surgical procedures.From these studies and subsequent clinical experi-
ence, thrombolytic therapy appears most useful for dis-tal thromboembolic occlusions in surgically inacces-sible small arteries of the leg, and foot, or in patientswho are too ill to undergo conventional open surgery.Thrombolytic therapy can also be applied for acuteembolic occlusions not readily amenable to surgical em-bolectomy. Thrombolytic therapy is also used to “buytime” in high-risk patients while underlying medicalproblems are treated prior to conventional surgicalrevascularization.
Until recently, rt-PA was the only available throm-bolytic agent after urokinase was removed from themarket in 1998. Urokinase has been recently reintro-duced, but most interventionalists are now very com-fortable and familiar with rt-PA and retavase, a non-glycosylated deletion mutation of rt-PA. The existingliterature would appear to support the use of rt-PA as asubstitute for urokinase for peripheral arterial throm-bolysis. In the STILE study, rt-PA was as effective andas safe as urokinase.8
Catheter thrombectomyIntroduction of the Fogarty balloon catheter in 1963dramatically altered the management of peripheralemboli. It reduced mortality from this disorder by nearly50% and decreased the incidence of amputation byapproximately 35%.11 The Fogarty balloon catheter isthe standard in surgical thrombectomy, although varia-tions of the design are used. These devices consist of asmall caliber (2F–6F) catheter with a central port forinflation of a soft, compliant latex balloon (Figure 3).The catheter is advanced through an open artery, andthen passed through the region containing thrombus orembolism. The balloon is gently inflated while the cath-eter is withdrawn, removing the thrombotic materialfrom the opening in the artery. Since the inflated bal-loon is at least as large as the diameter of the treatedartery, such devices are not well suited to percutaneoususe through an introducer sheath. Several passages aregenerally required to remove all of the thrombus.
More recently, variations on this design have beenintroduced by Fogarty. There are two newer catheters—one that removes adherent clots within an artery, andanother that removes clots adherent to the lumen of aprosthetic bypass graft. Older, chronic clots are noteasily removed with the compliant latex balloon cath-eters—the balloon simply deforms, leaving much of themore tenacious clot within the artery or graft. The Ad-herent Clot Catheter (Edward Lifesciences, Irvine, CA)works like a latex-covered corkscrew (Figure 4). Thecatheter has a deployment trigger that winds the inner

552 American Society of Hematology
wire loop, which is covered with an outer layer of pro-tective latex to minimize the prospect of arterial injury,in a cork screw configuration. The author has used thisdevice with success in arteries that cannot be adequatelytreated by a balloon catheter alone.
The other Fogarty design catheter is used to re-move chronic thrombi from occluded prosthetic grafts.It consists of a wire loop that deploys around the cath-eter in a cloverleaf configuration (Figure 5). In theauthor’s experience, this catheter will remove any oc-clusive material if the occlusion can be traversed. Thewire loops are robust, and therefore should not be usedin a native artery.
Rheolytic thrombectomy cathetersRheolytic thrombectomy achieves removal of intra-ar-terial thrombus using a suction type of catheter. A num-ber of such catheters are used for thrombectomy ofthrombosed arteriovenous access dialysis grafts, but onecatheter is also approved by the FDA for use in periph-eral arteries. The Possis AngioJet system uses a highvelocity stream of saline within the catheter to producea low-pressure region (Bernoulli effect) within the cath-eter tip. This low pressure results in extraction of clotmaterial through a lumen in the catheter, and is therebyremoved from the body. Potential advantages of thissystem include reduced time to achieve thrombectomycompared to many hours or even days with thrombolysis.Rheolytic thrombectomy is particularly attractive for pa-tients with contraindications to thrombolytic therapy.
An initial report on the use of the Possis device forperipheral arterial use in cases of acute, limb-threaten-ing ischemia was reported by Silva and associates in1998.12 In their study, 21 patients with acute limb is-chemia (presentation within 2 weeks of symptom on-set) were treated. Contraindications to thrombolytictherapy were present in 52% of the patients. The au-thors reported an initial technical success rate of 91%,with a 6-month limb salvage rate of 89%. In a morerecent study of 86 patients undergoing rheolytic throm-bectomy using the AngioJet device, investigators fromthe Cleveland Clinic reported successful arterial reca-nalization in 61%, partial success in 23%, and failureto recanalize the occluded artery in 16% of cases.13 In-terestingly, adjunctive thrombolytic therapy was usedin 58% of cases, highlighting the potential to use mul-tiple modalities in cases of acute arterial ischemia ofthe leg. An underlying arterial stenosis was found in 53cases, 51 of which were successfully treated. This ex-perience illustrates how thrombolysis, rheolytic throm-bectomy, and percutaneous balloon angioplasty can beused in combination to effect a minimally invasive
Figure 5. Fogarty Graft Thrombectomy Catheter.
Bare metal loops remove tenacious, prosthetic graft-boundthrombus. Not to be used in native arteries.
Figure 3. Fogarty balloon catheter.
Figure 4. Edwards Lifesciences Fogarty Adherent ClotCatheter.
Inner wire loop is protected by outer latex covering. Catheter isused for arterial and graft occlusions.

Hematology 2003 553
revascularization approach to selected patients withacute limb ischemia.
Laser-assisted angioplastyLaser-assisted balloon angioplasty is an endovasculartechnique that allows recanalization of long segmentarterial occlusions that are too long to be successfullycrossed with a guidewire and conventional techniquesalone. Most short segment arterial occlusions can becrossed using standard guidewires with hydrophiliccoatings that enable the wire to be “slipped” throughan obstructed area. In some long segment lesions, how-ever, this is not possible. The excimer laser device(Spectranetics, Colorado Springs, CO), on the otherhand, is advanced in small increments along with theguidewire, while the laser energy recanalizes the oc-cluded arterial segment. Once the diseased segment iscrossed, a standard guidewire is placed through the areaand it is treated with balloon angioplasty as with otherarterial stenotic lesions (Figure 6). These devices comein a range of diameters (0.9–2.5 mm) and can be usedfor coronary and peripheral arterial lesions.
These newer peripheral laser catheters are not inwidespread use, and there is little published clinical datain the peripheral arterial system. There are two ongo-ing clinical trials, one for long segment (> 10 cm) oc-clusions of the superficial femoral artery, and the otherfor patients with critical ischemia of the leg who arepoor-risk candidates for conventional surgicalrevascularization. In a pilot study of the feasibility ofthis device for treating patients with critical ischemia
of the legs, Gray and associates reported the use of theexcimer laser and balloon angioplasty in 23 patientswith ischemic ulcers or gangrene of the legs.14 In 88%of cases, crossing of the lesion with successful angio-plasty was accomplished. Over a 6-month follow-up, 3patients required major limb amputation, and 4 otherseventually required surgical bypass to revascularize theleg. Patency data were not described. While these re-sults appear to be inferior to that generally reportedwith conventional surgical revascularization, these werehigh-risk patients, many of whom likely would not havebeen offered surgery. For such patients, catheter-basedinterventions such as laser-assisted balloon angioplastyremain an attractive alternative. In our practice, laser-assisted balloon angioplasty of the tibial arteries is re-served for medical high-risk patients and those in whomautologous vein conduit for bypass graft is not available.
Tibial artery balloon angioplastyBalloon angioplasty has emerged as an effective andwell-accepted treatment for occlusive disease of the iliacarteries. However, clinical success and long-term pa-tency rates have generally not been as good when ap-plied to the smaller arteries of the lower leg, particu-larly the tibial arteries. Nonetheless, several reports havebeen published that indicate at least a reasonable de-gree of effectiveness. This, along with advances in smalldiameter angioplasty systems developed for the coro-nary circulation, has led to an increased use of thesetechniques, particularly in those patients who are medi-cally unfit for standard surgical bypass. For the most
part, clinical applicability of bal-loon angioplasty of tibial arteryocclusive disease is much thesame as summarized above forlaser-assisted balloon angio-plasty. In fact, the techniques andindications are largely the same,except that the laser device isused to recanalize long segmentocclusions that cannot be crossedwith a guidewire alone.
Much of the reported experi-ence with tibial angioplasty isfrom the work of Amman Bolia,in Leicester, England.15 Bolia andcolleagues reported a summary oftheir experience of angioplasty ofisolated infragenicular arteries in2002.16 In this study of 67 patientstreated from 1997 to 2000, theyreport an initial technical successof 86%, and a 3-year limb salvage
Figure 6. Occluded popliteal artery, before (A) and after (B) laser-assisted balloonangioplasty.

554 American Society of Hematology
rate of 94%. Reflecting the advanced, end-stage natureof this pattern of peripheral vascular disease, 51% ofthe patients had died by 3 years. Although patency rateswere not reported in this study, it can be assumed thatmany of these arteries did not remain patent at the same94%, 3-year rate as was the case with limb salvage.However, if the offending ischemic lesion heals, andthen the treated artery reoccludes later, this can stillresult in a clinically stable situation in which limb sal-vage is achieved.
In a recent report of peripheral angioplasty in 221diabetics with ischemic foot ulcers, the authors wereso encouraged by the good clinical outcomes as to rec-ommend balloon angioplasty as the first line treatmentfor such patients, in preference to surgical bypass.17 Inthis retrospective study, balloon angioplasty of tibialartery occlusive disease was performed at the time ofthe original angiogram regardless of lesion length orany anatomic criteria of the arterial occlusive disease.In 191 (85.3%) cases, balloon angioplasty was per-formed. At a mean follow-up of 14.7 months only 10patients (5.2%) required a major limb amputation (am-putation at or above the ankle joint). Clinical recurrencewas noted in 14 patients, 10 of whom underwent re-peat balloon angioplasty.
In spite of these encouraging results, the mainstayof treatment for peripheral arterial occlusive disease ofthe tibial arteries continues to be surgical revascular-ization, primarily due to better long-term patency rates.Nonetheless, for many of these patients, particularlythose with advanced comorbidities and age, tibial ar-tery balloon angioplasty is an attractive alternative tosurgical revascularization. Despite lower reported pa-tency rates compared with surgical bypass, even lim-ited primary patency of several months can be suffi-cient to allow healing of ischemic lesions of the foot.The exact role of tibial artery angioplasty will remain amatter of controversy until the appropriate clinical tri-als can be performed and published.
Remote EndarterectomyOcclusion of the superficial femoral artery is a com-mon anatomic pattern in patients suffering from inter-mittent claudication. When combined with additionalanatomic levels of atherosclerotic occlusive disease,such as the aortoiliac segment or tibial arteries, it cancause critical, or limb-threatening ischemia. Occlusionof the superficial femoral artery generally involves theentire length of the artery rendering it relatively un-suitable for balloon angioplasty. Surgical bypass is mostcommonly utilized to revascularize these occlusions.Another option is that of endarterectomy, where theplaque is physically removed from the artery. Endart-
erectomy procedures are typically done with conven-tional open surgical technique, but such long segmentendarterectomies have generally fared poorly in termsof patency rates, and require a long incision on the thighto expose the entire superficial femoral artery.
With the advent of catheter-based techniques, it ispossible to perform a remote endarterectomy of an oc-cluded superficial femoral artery utilizing only a singlesmall incision in the groin area. The procedure is termed“remote” because the devices used to perform theendartectomy are manipulated under fluoroscopy, fromthe “remote” location of the proximal aspect of the su-perficial femoral artery while the entire length of theartery is internally stripped of the occluding plaque.
The use of the remote endarterectomy was cham-pioned by Moll and associates18 and has only recentlyreceived more attention in the United States as the cut-ting device has only recently become available. Re-cently reported clinical results with the technique havebeen mixed. In a report of 60 patients undergoing re-mote endarterectomy of the superficial femoral artery,Rosenthal and associates reported a 3-year primarypatency rate of 61%, with a primary assisted patencyrate of 83%.19 Only 1 patient required major amputation.A more sobering analysis of the remote endarterectomytechnique has been reported by Nelson and associates.20
In their study of 17 patients, the initial technical successwas only 65%, and at 1 year the primary patency was26%. No patients, however, required amputation. Giventhe disparate results from these 2 centers, one mightinfer that a significant procedural learning curve existswith this technique.
SummaryThrombolytic therapy is the mainstay of catheter-basedtreatment of acute arterial occlusion. Rheolytic throm-bectomy allows for treatment of acute arterial occlu-sions without the bleeding risks associated with throm-bolytic therapy. Balloon thrombectomy catheters canbe used during arterial revascularization in a form of“hybrid” procedure that requires some open surgery andthe use of Fogarty balloon catheters. Chronic arterialocclusions are increasingly being treated with endo-vascular techniques such as balloon angioplasty, laser-assisted angioplasty, and remote endarterectomy asminimally invasive alternatives to conventional opensurgery. From a clinical practice standpoint it is clear thatthese techniques are here to stay and that further devicerefinement will only expand their applicability to the treat-ment of peripheral arterial occlusive disorders.

Hematology 2003 555
Update on Vena Cava FiltersIndications for placement of vena cava filters are notclearly established; the situations in which their use ismost justified are in patients with venous thromboem-bolism who have an absolute contraindication for anti-coagulation (e.g., cerebral or gastrointestinal bleeding)or a complication of anticoagulation therapy and inpatients who have sustained massive trauma, which in-cludes brain or spinal cord injuries or fracture of thepelvis and long bones of the extremities.21,22
Although vena cava filters may be efficacious inpreventing fatal pulmonary embolism initially,23 withtime their efficacy is counterbalanced by complicationsin recipients such as deep venous thrombosis (6%–32%), inferior vena cava thrombosis (3.6%–11.2%), andthrombosis at the insertion site (23%–36%).21
Recently, a newer filter, the TrapEase filter (CordisEuropa, NV, LJ Roden, The Netherlands), has under-gone approval by the FDA. The advantage of this filteris that it can be introduced through a small catheter(6F), allowing delivery through an antecubital, jugular,or femoral vein approach.22 The filter, which is com-patible with magnetic resonance imaging (MRI), is sym-metrical, so that orientation of the filter is not an issue.A prospective study in 65 patients showed protectionfrom pulmonary embolism at 6 months, with 2 episodesof thrombosis at the site of the filter. This filter designhas been modified so that it can be manipulated or po-tentially removed (OptEase), although the safety of re-moval has not been specifically studied.24
An ideal vena cava filter is one that could be placedon a temporary basis. The Gunther Tulip RetrievableVena Cava Filter is approved in the US for permanentplacement, with trials of retrieval currently in progress.In Canada, the filter has been approved for both per-manent placement and for retrieval since March 1998.The Canadian Interventional Radiology Association hasestablished a registry for the patients who have receivedthe Gunther Tulip Filter.25 In this registry of 90 patientswho have received the filter between 1998 and 2000,retrieval was successful in 51 of the 52 patients in whomit was attempted. Implantation times at retrieval rangedfrom 2 to 25 days (mean, 9 days). The manufacturer rec-ommends the filter be removed after a period of 2 weeks.
Recently, the Nitinol Recovery Filter has been ap-proved for permanent implantation. This filter can be re-moved several weeks to months after implantation.26,27
The availability of newer vena cava filters with im-proved characteristics as well as additional studies onthe success of retrieval of temporary filters will increasethe range of options for patients who are candidates fortemporary or permanent vena cava filter placement.
REFERENCES
I. Newer Anticoagulant Agents for theConsultant’s Toolbox
1. Lassen MR, Bauer KA, Ericksson BI, Turpie AG; EuropeanPentasaccharide Elective Surgery (EPHESUS) SteeringCommittee. Postoperative fondaparinux versus preoperativeenoxaparin for prevention of venous thromboembolism inelective hip-replacement surgery: a randomised double-blindcomparison. Lancet. 2002;359(9319):1715-1720.
2. Turpie AG, Bauer KA, Eriksson BI, Lassen MR;PENTATHALON 2000 Study Steering Committee. Postopera-tive fondaparinux versus postoperative enoxaparin forprevention of venous thromboembolism after elective hip-replacement surgery: a randomised double-blind trial. Lancet.2002;359(9319):1721-1726.
3. Eriksson BI, Bauer KA, Lassen MR, Turpie AGG, for theSteering Committee of the Pentasaccharide in Hip-FractureSurgery Study. Fondaparinux compared with enoxaparin forthe prevention of venous thromboembolism after hip-fracturesurgery. N Engl J Med. 2001;345:1298-1304.
4. Bauer KA, Eriksson BI, Lassen MR, Turpie AGG, for theSteering Committee of the Pentasaccharide in Major KneeSurgery Study. Fondaparinux compared with enoxaparin forthe prevention of venous thromboembolism after electivemajor knee surgery. N Engl J Med. 2002;345:1305-1310.
5. Bauer KA, Eriksson BI, Lassen MR, Turpie AGG. Influence ofthe duration of fondaparinux prophylaxis in preventing venousthromboembolism following hip fracture surgery. Blood.2002;100:83a.
6. The Matisse Investigators. Fondaparinux (Arixtra®) incomparison to low molecular weight heparin for the initialtreatment of symptomatic deep venous thrombosis orpulmonary embolism. The Matisse clinical outcome studies.Blood. 2002;100:83a.
7. Turpie AG, Bauer KA, Eriksson BI, Lassen MR. Fondaparinuxvs enoxaparin for the prevention of venous thromboembolismin major orthopedic surgery: a meta-analysis of 4 randomizeddouble-blind studies. Arch Intern Med. 2002;162:1833-1840.
8. Hull RD, Pineo GF, Stein PD, et al. Timing of initial adminis-tration of low-molecular-weight heparin prophylaxis againstdeep vein thrombosis in patients following elective hiparthroplasty: a systematic review. Arch Int Med.2001;161:1952-1960.
9. Coussement PK, Bassand J-P, Convens C, et al, for thePENTALYSE Investigators. A synthetic factor-Xa inhibitor(ORG31540/SR9017A) as an adjunct to fibrinolysis in acutemyocardial infarction. The PENTALYSE Study. Eur Heart J.2001;22:1716-1724.
10. Simoons M, for the PENTUA study group. Pentasaccharide inpatients with unstable angina: PENTUA study [abstract]. 74thAnnual Scientific Sessions of the American Heart Assoc. AHACongress; Anaheim, CA, 2001.
11. Weitz JI, Hudoba M, Massel D, et al. Clot-bound thrombin isprotected from inhibition by heparin-antithrombin III but issusceptible to inactivation by antithrombin III-independentinhibitors. J Clin Invest. 1983;102:220-230.
12. Song X, Huhle G, Wang L, et al. Generation of anti-hirudinantibodies in heparin-induced thrombocytopenic patientstreated with r-hirudin. Circulation. 1999;100:1528-1532.
13. Frank RD, Farber H. Stefanidis I, et al. Hirudin elimination byhemofiltration: a comparative in vitro study of differentmembranes. Kidney Int. 1999;72:541-545.
14. Greinacher A, Janssens U, Berg G, et al. Lepirudin (recombi-

556 American Society of Hematology
nant hirudin) for parenteral anticoagulation in patients withheparin-induced thrombocytopenia. Circulation.1999;100:587-593.
15. Greinacher A, Volpel H, Janssens U, et al. Recombinanthirudin (lepirudin) provides safe and effective anticoagulationin patients with heparin-induced thrombocytopenia: Aprospective study. Circulation. 1999;99:73-80.
16. Lewis B, Wallis D, Berkowitz S, et al. Argatroban anticoagu-lant therapy in patients with heparin-induced thrombocytope-nia. Circulation. 2001;103:1838-1843.
17. Greinacher A, Eichler P, Lubenow N, et al. Heparin-inducedthrombocytopenia with thromboembolic complications: meta-analysis of 2 prospective trials to assess the value ofparenteral treatment with lepirudin and its therapeutic aPTTrange. Blood. 2000;96:846-851.
18. Lewis BE, Matthai WH Jr, Cohen M, et al. Argatrobananticoagulation during percutaneous coronary intervention inpatients with heparin-induced thrombocytopenia. CatheterCardiovasc Interv. 2002;57:177-184.
19. Davis Z, Anderson R, Short D, et al. Favorable outcome withbivalirudin anticoagulation during cardiopulmonary bypass.Ann Thorac Surg. 2003;75:264-265.
20. Koster A, Loebe M, Hansen R, et al. A quick assay formonitoring recombinant hirudin during cardiopulmonarybypass in patients with heparin-induced thrombocytopeniatype II: adaption of the Ecarin clotting time to the act IIdevice. J Thorac Cardiovasc Surg. 2000;119:1278-1283.
21. Kawada T, Kitagawa H, Hoson M, et al. Clinical application ofargatroban as an alternative anticoagulant for extracorporealcirculation. Hematol Oncol Clin No Amer. 2000;14:445-457.
22. Alving BM. How I treat heparin-induced thrombocytopeniaand thrombosis. Blood. 2003;101:31-37.
23. Maraganore JM, Bourdon P, Jablonski J, et al. Design andcharacterization of hirulogs: a novel class of bivalent peptideinhibitors of thrombin. Biochemistry. 1990;29:7095-7101.
24. Bittl JA, Strony J, Brinker JA, et al. Treatment with bivalirudin(Hirulog) as compared with heparin during angioplasty forunstable or postinfarction angina. N Engl J Med.1995;333:764-769.
25. Organization to assess strategies for ischemic syndromes(OASIS-2) Investigators. Effects of recombinant hirudin(lepirudin) compared with heparin on death, myocardialinfarction, refractory angina, and revascularization proceduresin patients with myocardial infarction without ST elevation: arandomized trial. Lancet. 1999;353:429-438.
26. Lincoff AM, Bittl JA, Harrington RA, et al. Bivalirudin andprovisional glycoprotein IIb/IIIa blockade compared withheparin and planned glycoprotein IIb/IIIa blockade duringpercutaneous coronary intervention: REPLACE-1 RandomizedTrial. JAMA. 2003;289:853-863.
27. Antman EM. Should bivalirudin replace heparin duringpercutaneous coronary interventions? JAMA. 2003;289:903-905.
28. Hafner G, Roser M, Nauck M. Methods for the monitoring ofdirect thrombin inhibitors. Semin Thromb Hemost.2002;28:425-430.
29. Eriksson BI. The oral direct thrombin inhibitor ximelagatran,and its subcutaneous (sc) form melagatran, compared withenoxaparin for prophylaxis of venous thromboembolism(VTE) in total hip or total knee replacement (THR or TKR):the EXPRESS Study. Blood. 2002;100:82a
30. Eriksson BI, Agnelli G, Cohen AT, et al, for the METHRO IIIStudy Group. Direct thrombin inhibitor melagatran followedby oral ximelagatran in comparison with enoxaparin forprevention of venous thromboembolism after total hip or knee
replacement. Thromb Haemost. 2003;89:288-296.31. Francis CW, Davidson BL, Berkowitz SD, et al. Ximelagatran
versus warfarin for the prevention of venous thromboembo-lism after total knee arthroplasty. A randomized, double-blindtrial. Ann Intern Med. 2002;137:648-655.
32. Francis CW, Berkowitz SD, Comp PC, et al. Randomized,double-blind, comparison of ximelagatran, an oral directthrombin inhibitor, and warfarin to prevent venous throm-boembolism (VTE) after total knee replacement (TKR).Blood. 2002;100:82a.
33. Colwell C Jr, Berkowitz SD, Davidson BL, et al. Comparisonof ximelagatran, an oral direct thrombin inhibitor, withenoxaparin for the prevention of venous thromboembolismfollowing total hip replacement. A randomized, double-blindstudy. J Thromb Haemost. 2003;1:2119-2130.
34. Halperin J. The Stroke Prophylaxic using an Oral ThrombinInhibitor in Atrial Fibrillation Trial (SPORTIF III). Am HeartJ. 2003;146:24.
35. Eriksson H, Wahlander K, Lundstrom T, et al. Extendedsecondary prevention with the oral direct thrombin inhibitorximelagatran for 18 months after 6 months of anticoagulationin patients with venous thromboembolism: a randomized,placebo-controlled trial. Blood. 2002;100:81a.
36. Heit JA, Colwell CW, Francis CW, et al, for the AstraZenecaArthroplasty Study Group. Comparison of the oral directthrombin inhibitor ximelagatran with enoxaparin as prophy-laxis against venous thromboembolism after total kneereplacement. Arch Intern Med. 2001;161:2215-2221.
37. Huisman M. Efficacy and safety of the oral direct thrombininhibitor ximelagatran compared with current standard therapyfor acute symptomatic deep vein thrombosis, with or withoutpulmonary embolism, a double-blind, multinational trial.[abstract 0C003]. Abstracts of the XIX Congress of the ISTH,Birmingham, UK 12-18 July 2003 (CD-ROM publication).
38. Kakkar AK, Marder VJ, Pineo GF, et al. Oral SNAC-Heparinvs enoxaparin for preventing venous thromboembolismfollowing total hip replacement. Blood. 2002;100:148a.
39. Lee A, Agnelli G, Buller H, et al. Dose-response study ofrecombinant factor VIIa/tissue factor inhibitor recombinantnematode anticoagulant protein c2 in prevention of postopera-tive venous thromboembolism in patients undergoing totalknee replacement. Circulation. 2001;104:74-78.
II. Evaluation of Patients with Peripheral VascularDisease
1. Prandoni P, Bilora F, Marchiori A, et al. An associationbetween atherosclerosis and venous thrombosis. N Engl JMed. 2003;348:1435-1441.
2. Kannel WB, McGee DL. Update on some epidemiologicfeatures of intermittent claudication: The Framingham Study. JAm Geriatr Soc. 1985;33:13-18.
3. Criqui MH, Fronek A, Barrett-Connor E, et al. The prevalenceof peripheral arterial disease in a defined population.Circulation. 1985;71:510-515.
4. Hiatt WR, Hoag S, Hamman RF. Effect of diagnostic criteriaon the prevalence of peripheral arterial disease. The San LuisValley diabetes study. Circulation. 1995;91:1472-1479.
5. Criqui MH, Langer RD, Fronek A, et al. Mortality over aperiod of 10 years in patients with peripheral arterial disease.N Engl J Med. 1992;326:381-386.
6. Newman AB, Shemanski L, Manolio TA, et al. Ankle-armindex as a predictor of cardiovascular disease and mortality inthe Cardiovascular Health Study. The Cardiovascular HealthStudy Group. Arterioscler Thromb Vasc Biol. 1999;19:538-545.

Hematology 2003 557
7. Newman AB, Tyrrell KS, Kuller LH. Mortality over four yearsin SHEP participants with a low ankle-arm index. J AmGeriatr Soc. 1997;45:1472-1478.
8. McKenna M, Wolfson S, Kuller L. The ratio of ankle and armarterial pressure as an independent predictor of mortality.Atherosclerosis. 1991;87:119-128.
9. Vogt MT, McKenna M, Anderson SJ, Wolfson SK, Kuller LH.The relationship between ankle-arm index and mortality inolder men and women. J Am Geriatr Soc. 1993;41:523-530.
10. Hirsch AT, Criqui MH, Treat-Jacobson D, et al. Peripheralarterial disease detection, awareness, and treatment in primarycare. JAMA. 2001;286:1317-1324.
11. Rutherford RB, Lowenstein DH, Klein MF. Combiningsegmental systolic pressures and plethysmography to diagnosearterial occlusive disease of the legs. Am J Surg.1979;138:211-218.
12. Hiatt WR, Hirsch AT, Regensteiner JG, Brass EP. Clinicaltrials for claudication. Assessment of exercise performance,functional status, and clinical end points. Vascular ClinicalTrialists. Circulation. 1995;92:614-621.
13. Regensteiner JG, Ware JE, Jr., McCarthy WJ, et al. Effect ofcilostazol on treadmill walking, community-based walkingability, and health-related quality of life in patients withintermittent claudication due to peripheral arterial disease:meta-analysis of six randomized controlled trials. J AmGeriatr Soc. 2002;50:1939-1946.
14. Kannel WB, McGee DL, Castelli WP. Latest perspectives oncigarette smoking and cardiovascular disease: TheFramingham Study. J Cardiac Rehabil. 1984;4:267-277.
15. Stewart CP. The influence of smoking on the level of lowerlimb amputation. Prosthet Orthot Int. 1987;11:113-116.
16. Ameli FM, Stein M, Prosser RJ, Provan JL, Aro L. Effects ofcigarette smoking on outcome of femoral popliteal bypass forlimb salvage. J Cardiovasc Surg. 1989;30:591-596.
17. Daughton D, Susman J, Sitorius M et al. Transdermal nicotinetherapy and primary care. Importance of counseling,demographic, and participant selection factors on 1-year quitrates. The Nebraska Primary Practice Smoking Cessation TrialGroup. Arch Fam Med. 1998;7:425-430.
18. Holm KJ, Spencer CM. Bupropion: a review of its use in themanagement of smoking cessation. Drugs. 2000;59:1007-1024.
19. Executive Summary of The Third Report of The NationalCholesterol Education Program (NCEP) Expert Panel onDetection, Evaluation, And Treatment of High BloodCholesterol In Adults (Adult Treatment Panel III). JAMA.2001;285:2486-2497.
20. MRC/BHF Heart Protection Study of cholesterol loweringwith simvastatin in 20,536 high-risk individuals: a randomizedplacebo-controlled trial. Lancet. 2002;360:7-22.
21. The seventh report of the Joint National Committee onprevention, detection, evaluation, and treatment of high bloodpressure: the JNC 7 Report. JAMA 2003;289:2560-2572.
22. Yusuf S, Sleight P, Pogue J, et al. Effects of an angiotension-converting-enzyme inhibitor, Ramipril, on cardiovascularevents in high-risk patients. The Heart Outcomes PreventionEvaluation Study Investigators. N Engl J Med. 2000;342:145-153.
23. Beach KW, Strandness DE. Arteriosclerosis obliterans andassociated risk factors in insulin-dependent and non-insulin-dependent diabetes. Diabetes. 1980;29:882-888.
24. Effect of intensive diabetes management on macrovascularevents and risk factors in the Diabetes Control and Complica-tions Trial. Am J Cardiol. 1995;75:894-903.
25. UK Prospective Diabetes Study (UKPDS) Group. Intensive
blood-glucose control with sulphonylureas or insulincompared with conventional treatment and risk of complica-tions in patients with type 2 diabetes (UKPDS 33). Lancet.1998;352:837-853.
26. Mehler PS, Coll JR, Estacio R et al. Intensive blood pressurecontrol reduces the risk of cardiovascular events in patientswith peripheral arterial disease and type 2 diabetes. Circula-tion. 2003;107:753-756.
27. Collaborative meta-analysis of randomized trials ofantiplatelet therapy for prevention of death, myocardialinfarction, and stroke in high risk patients. BMJ. 2002;324:71-86.
28. Collaborative overview of randomized trials of antiplatelettherapy—I: Prevention of death, myocardial infarction, andstroke by prolonged antiplatelet therapy in various categoriesof patients. Antiplatelet Trialists’ Collaboration. BMJ.1994;308:81-106.
29. Food and Drug Administration. Internal analgesic, antipyretic,and antirheumatic drug products for over-the-counter humanuse; final rule for professional labeling of aspirin, bufferedaspirin, and aspirin in combination with antacid drugproducts. Federal Register. 1998;63:56802-56819.
30. Janzon L, Bergqvist D, Boberg J, et al. Prevention ofmyocardial infarction and stroke in patients with intermittentclaudication; effects of ticlopidine. Results from STIMS, theSwedish Ticlopidine Multicenter Study. J Int Med.1990;227:301-308.
31. CAPRIE Steering Committee. A randomized, blinded, trial ofclopidogrel versus aspirin in patients at risk of ischaemicevents (CAPRIE). Lancet. 1996;348:1329-1339.
32. Jackson MR, Clagett GP. Antithrombotic therapy in peripheralarterial occlusive disease. Chest. 2001;119:283s-299s.
33. Stewart KJ, Hiatt WR, Regensteiner JG, Hirsch AT. Exercisetraining for claudication. N Engl J Med. 2002;347:1941-1951.
34. Girolami B, Bernardi E, Prins MH, et al. Treatment ofintermittent claudication with physical training, smokingcessation, pentoxifylline, or nafronyl: a meta-analysis. ArchIntern Med. 1999;159:337-345.
35. Hiatt WR, Regensteiner JG, Creager MA, et al. Propionyl-L-carnitine improves exercise performance and functional statusin patients with claudication. Am J Med. 2001;110:616-622.
36. Lederman RJ, Mendelsohn FO, Anderson RD, et al. Therapeu-tic angiogenesis with recombinant fibroblast growth factor-2for intermittent claudication (the TRAFFIC study): arandomized trial. Lancet. 2002;359:2053-2058.
III. Interventional Approaches in theManagement of Thrombosis
1. Brogden RN, Speight TM, Avery GS. Streptokinase: a reviewof its clinical pharmacology, mechanism of action andtherapeutic uses. Drugs. 1973;5:357-445.
2. Dotter CT, Rosch J, Seaman AJ. Selective clot lysis with low-dose streptokinase. Radiology. 1974;111:31-37.
3. Andaz S, Shields DA, Scurr JH, et al. Thrombolysis in acutelower limb ischaemia. Eur J Vasc Surg. 1993;7:595-603.
4. Ricotta JJ, Green RM, DeWeese JA. Use and limitations ofthrombolytic therapy in the treatment of peripheral arterialischemia: results of a multi-institutional questionnaire. J VascSurg. 1987;6:45-50.
5. Berridge DC, Gregson RHS, Hopkinson BR, et al. Random-ized trial of intra-arterial recombinant tissue plasminogenactivator, intravenous recombinant tissue plasminogenactivator and intra-arterial streptokinase in peripheral arterialthrombolysis. Br J Surg. 1991;78:988-995.

558 American Society of Hematology
6. Bell W. Update on urokinase and streptokinase: a comparisonof their efficacy and safety. Hospital Formulary. 1988;23:230-241.
7. VanBreda A, Katzen B, Deutsch A. Urokinase versus strepto-kinase in local thrombolysis. Radiology. 1987;165:109-111.
8. STILE Investigators. Results of a prospective randomized trialevaluating surgery versus thrombolysis for ischemia of thelower extremity. Ann Surg. 1994;220:251-268.
9. Ouriel K, Veith FJ, Sasahara AA. Thrombolysis or peripheralarterial surgery: phase I results—TOPAS Investigators. J VascSurg. 1996;23:64-73.
10. Ouriel K, Veith FJ, Sasahara AA. A comparison of recombi-nant urokinase with vascular surgery as initial treatment foracute arterial occlusion of the legs. N Engl J Med.1998;338:1105-1111.
11. Elliott JP Jr, Hageman JH, Szilagyi E, et al. Arterial emboliza-tion: problems of source, multiplicity, recurrence, and delayedtreatments. Surgery. 1980;88:833-845.
12. Silva JA, Ramee SR, Collins TJ, et al. Rheolytic thrombec-tomy in the treatment of acute limb-threatening ischemia:immediate results and six-month follow-up of the multicenterAngioJet registry. Possis Peripheral AngioJet Investigators.Cathet Cardiovasc Diagn. 1998;45:386-393.
13. Kasirajan K, Gray B, Beavers FP, et al. Rheolytic thrombec-tomy in the management of acute and subacute lim-threaten-ing ischemia. J Vasc Interv Radiol. 2001;12:413-421.
14. Gray BH, Laird JR, Ansel GM, Shuck JW. Complexendovascular treatment for critical limb ischemia in poorsurgical candidates: a pilot study. J Endovasc Ther.2002;9:599-604.
15. Bolia A, Sayers RD, Thompson MM, Bell PRF. Subintimal andintraluminal recanalisation of occluded crural arteries bypercutaneous balloon angioplasty. Eur J Vasc Surg.1994;8:214-219.
16. Ingle HI, Nasim A, Bolia A, et al. Subintimal angioplasty ofisolated infragenicular vessels in lower limb ischemia: long-term results. J Endovasc Ther. 2002;9:411-416.
17. Faglia E, Mantero M, Caminiti M, et al. Extensive use ofperipheral angioplasty, particularly infrapopliteal, in thetreatment of ischaemic diabetic foot ulcers: clinical results ofa multicenter study of 221 consecutive diabetic patients. JIntern Med. 2002;252:225-232.
18. Ho GH, Moll FL, Joosten PP, van de Pavoordt ED, OvertoomTT. The MollRing Cutter remote endarterectomy: preliminaryexperience with a new endovascular technique for treatment ofocclusive superficial femoral femoral artery disease. JEndovasc Surg. 1995;2:278-287.
19. Rosenthal D, Schubart PJ, Kinney EV, et al. Remote superfi-cial femoral artery endarterectomy: multicenter medium-termresults. J Vasc Surg. 2001;34:428-433.
20. Nelson PR, Powell RJ, Proia RR, et al. Results of endovascularsuperficial femoral endarterectomy. J Vasc Surg. 2001;34:526-531.
21. Streiff MB. Vena caval filters: a comprehensive review. Blood.2000;95:3669-3677.
22. Kinney TB. Update on inferior vena cava filters. J Vasc IntervRadiol. 2003;14:425-440.
23. Decousus H, Leizorovicz A, Parent F, et al. A clinical trial ofvena caval filters in the prevention of pulmonary embolism inpatients with proximal deep-vein thrombosis. N Engl J Med.1998;338:409-415.
24. Rousseau H, Perreault P, Otal P, et al. The 6-F nitinol TrapEaseinferior vena cava filter: results of a prospective multicentertrial. J Vasc Interv Radiol. 2001;12:299-304.
25. Millward SF, Oliva VL, Bell SD, et al. Gunther Tulipretrievable vena caval filter: results from the registry of theCanadian Interventional Radiology Association. J Vasc IntervRadiol. 2001;12:1053-1058.
26. Asch MR. Initial experience in humans with a new inferiorvena cava filter. Radiology. 2002;225:835-844.
27. Brountzos EN, Kaufman JA, Venbrux AC, et al. A newoptional vena cava filter: retrieval at 12 weeks in an animalmodel. J Vasc Interv Radiol. 2003;14:763-772.