Embed Size (px)
Citation preview

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 1
Examining the cranial nerves
I Olfactory
II Optic
III Oculomotor
IV Trochlear
V Trigeminal
VI Abducens
VII Facial
VIIIAcoustic (auditory & vestibular)
IX Glossopharyngeal
X Vagus
XI Accessory
XII Hypoglossal

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 2
1st (Olfactory) nerve
Responsible for the sense of smell
Sense of smell may be lost as a result of
trauma
infection
ageing
Smell is an important component of the
appreciation of taste (which may be the principal
complaint of a patient)
Crude bedside test may be to identify the odour of
coffee or fresh orange

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 3
1st (Olfactory) nerve- formal test
One nostril at a time - occlude the other
Use several test smells.
Ask patient to sniff and signal detection
Prompt response needed, else spreads to other
side
Few can identify the classic test smells
Exclude misinterpretation / malingering
Ammonia - detected through nasal pain fibres
Should still taste sugar, salt, vinegar, quinine

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 4
The 2nd (Optic) nerve
Various tests are possible which depend to
some extent (though not exclusively) on the
integrity of the optic nerve(s)
These include
Ophthalmoscopy (See separate study guide)
pupillary reflexes
visual acuity
visual fields

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 5
The pupils - Inspection
Size and shape
Regularity in outline and equality of both
sides
Defects in iris
Foreign bodies in anterior chamber
Obvious cataract

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 6
Pupillary light reflexes
Ask patient to look at a distant object.
Swing light beam in from behind onto one eye, or
switch on from in front. Ensure abrupt stimulus.
Shield other eye effectively.
Direct response- constriction of pupil to light shone
into that eye.
Consensual response - constriction of pupil to light
shone in opposite eye.

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 7
Pupillary light reflexes 2
Shield the non-examined eye
Move light beam abruptly in
from the side, or switch on from
the front
Direct reflex - ipsilateral pupil
constricts
Consensual reflex -
contralateral pupil constricts
Direct
Consensual

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 8
Pupillary accommodation reflex
Ask patient to fix on a distant object and then
to focus on finger held about 10 cms from
face. Keep target high or eyelids will obscure
the pupil.
The eyes should converge
The pupils should constrict equally

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 9
Accommodation
The person fixes on
a distant object
The person is then
asked to look at a
close object - their
eyes converge and
pupils constrict

Documenting P.E.R.L.A.
The acronym P.E.R.L.A. is used to both help remind us
what tests we should do and for documentation purposes.
Pupils
Equal and
Reactive to Light and
Accommodation
When documenting, it is permissible to write PERLA this
signifies that it was checked and is ok.
If there was a problem then you should document in full
what the problem is.
12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 10

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 11
Visual acuity testing
A series of different sized
letters on the chart
Viewed at 6 metres (half
sized charts are viewed at 3
metres)
Under each line is a number
that represents in metres
the distance from which that
size letter would be visible
in someone with normal
eyesight

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 12
Visual acuity test results
The result of the test is recorded as the distance from which the patient was positioned (in metres) over the smallest set of letters that can be read on a chart
6/6 (capable of reading letters expected to be visible at 6 metres whilst looking from a distance of 6 meters)
6/60 (only capable of reading letters expected to be visible at 60 metres at 6 metres)
For general examination purposes, if the patient wears glass’s they can be kept on but their lens prescription should be documented
Small
numbers
above
letters
indicate
the
distance at
which a
person
with
normal
vision can
identify
them

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 13
Visual acuity measurement
Ask the patient to cover each eye in turn and determine the smallest
print size that can be read
Record separately for each eye e.g. R = 6/6 L = 6/5.
For short-sighted patients glasses should be worn, but if not available
reading through a pin-hole will help to compensate.
For patient unable to read the 60 print size, move them nearer to the
chart (e.g. 3 metres) and record acuity as 3/xx.
For patients unable to read the chart as close as 1 metre record acuity
as:
For children and illiterate patients there are charts showing shapes
rather than letters
CF = Count fingers (Hold hand 0.5 of a metre from the patient )
HM = Hand movement
PL = Perceives light
NPL = No perception of light

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 14
Visual field testing
The “bedside” test: face the
patient at a distance of
about 1 metre. Keep
patient’s visual background
uncluttered, with light
behind patient
To test the right eye
Close or cover your right
eye. Say “cover your left
eye and look at my left
eye”. This matches the
visual fields.
Fig 1
Fig 2

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 15
Visual field testing 2
Ensure patient doesn’t look away
from your eye
Keeping in a plane midway
between you and the patient,
bring a white pin head from the
extreme of vision (arm’s length)
in towards pupil. Test each
quadrant using diagonal track
bisecting the quadrant. Establish
rough boundary then define with
slower target movements (see
Fig. 1-4)
Fig 3
Fig 4

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 16
Visual field testing 3
Ask the patient to indicate when they first appreciate
the white ball entering their visual field
Compare this to your own detection
Produce a more detailed “map” of a defect by
increasing the number of spokes used
The field is limited superiorly by the supra-orbital ridge
and medially by the nose
Any defect should be assessed formally

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 17
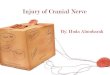
The blind spot = optic disc
Align patients visual horizontal with yours. Close (eg)your right eye. Tell patient “cover your left eye, and gaze at my left eye”.
Use a red pinhead (approx 1cm diameter). Check patient can see target when aligned with pupil.
Move target slowly, horizontally and laterally from pupil, ask the patient to signal when it disappears and reappears.
Sit approx. 1 metre apart, fix gaze on
each other’s open eye (right to left). Move
the pin slowly across the axis of fixation.
The red pin will disappear when it
coincides with the optic disc.

Left RightTemporalTemporal
Nasal
A B
CD E
F
A
B
C
D
E
Light from images in the temporal region stimulates
the nasal fibres of the retina and visa versa.
left
eye
Optic nerve
Optic chiasm
Optic radiation
F
Optical
cortex
nose
right
eye

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 19
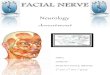
Eye movements (3rd, 4th & 6th)
The arrows indicate the direction of movement of the eyes and
not necessarily the position of the muscles.
Medial Lateral
Up
Down
Superior Rectus III
Left eye
Inferior Rectus IIISuperior Oblique IV
Inferior oblique III
Medial
Rectus
III
Lateral
Rectus
VI

Muscle nerve links
A way to remember which muscle is controlled
by which nerve is LR 6 SO4 EE 3
LR 6 Lateral rectus muscle is controlled by
6th nerve. Abducens.
SO4 Superior oblique muscle is controlled
by 4th nerve. Trochlear.
EE 3 Everything else is controlled by the
3rd nerve. Oculomotor
12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 20

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 21
Rectus Muscles
© 2002 Sinauer Associates

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 22
Testing eye movements
Hold a pen or similar object 50 cm from the patient in the midline and on a level with the patient’s eyes
Lateral gaze - vertical target Up / down gaze - horizontal target
Ask patient to follow object (“with your eyes”), keeping head still, and to report any double vision
Move the object slowly
side to side
up and down centrally, then at extremes of lateral gaze
stay in binocular range

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 23
Eye movements
Observe
range of movement
smoothness and speed
whether conjugate (moving together)
nystagmus (see 8th nerve for details)
If obvious dysconjugate eye movements
Is there double vision?
If present, establish muscle(s) affected
If not, test for latent squint

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 24
Diplopia – which eye and muscle?
If patient reports diplopia remember:
False image is from the affected eye
Outer image is the false one
Double vision is maximal in the direction of gaze of
the affected muscle

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 25
Diplopia – which eye and muscle?
For each direction of gaze with diplopia
establish position where images are widest apart
cover each eye in turn and confirm binocular diplopia
(present only with both eyes looking).
cover one eye and if outer image disappears that eye
and the muscle turning it that way are the abnormal
ones.
cross-check by covering the other eye. Inner image
should disappear.

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 26
3rd (Oculomotor) nerve palsy
RestingPtosis
On lifting ptosis,
the eye deviated
laterally and
downwards
Affected eye (left)
In complete palsy, pupil dilated and unreactive

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 27
4th (Trochlear) nerve palsy
Resting
Looking to right and
downwards
Affected eye (left)

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 28
6th (Abducens) nerve palsy
Resting position
Look to L
On command to look to the left the affected eye (LEFT) does not
move
Affected eye

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 29
The cover test for latent squint
Ask the patient to look with both eyes at examiner’s right eye
Cover patient’s left eye, then uncover left eye and rapidly cover right eye
Observe to see if left eye corrects to fix on examiner’s eye
Repeat for patient’s right eye
R L
Example above:
left latent squint

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 30
The 5th (Trigeminal) nerve
The trigeminal nerve supplies
Sensory divisions
Ophthalmic (V1)
Maxillary (V2)
Mandibular (V3)
Motor
Muscles of mastication

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 31
Sensory branches of 5th nerve
Ophthalmic
Maxillary
Mandibular
Test light touch with
cotton wool
For pain use sharp
end of a neuro tip
Use the blunt end to
act as a discriminator
if the patient is
unable to readily
sense pain
Compare sides

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 32
Sensation - trigeminal nerve
Motor - facial nerve
Twist a wisp of cotton wool to a
point.
Ask the patient to look up and in
Touch the lateral cornea
Both eyes should blink
Be careful to touch the peripheral
cornea and not the conjunctiva
Avoid the central cornea.
Don’t drag the cotton across the
cornea
Corneal reflex
Unlikely to work on people who
wear contact lenses

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 33
Testing 5th nerve motor function
Place your fingers on muscles first. Ask patient to clench teeth and you feel masseter and temporalis contracting.
Ask patient to open mouth to left, and stop you trying to push the open jaw back to midline. Repeat for right side. Testing power of lateral and medial pterygoids.
Jaw jerk
ask the patient to open their mouth slightly
place a finger on the chin
percuss the finger
observe and feel jaw movementTesting the jaw reflex

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 34
The 7th (Facial) nerve
The facial nerve supplies
Muscles of facial expression
Stapedius muscle in the ear
Taste to the anterior 2/3rds of the tongue
Parasympathetic nerves to the lacrimal gland
LMN lesions affect all facial muscles on that side (final common pathway).
Unilateral UMN lesions spare the forehead (bilateral cortical representation).

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 35
Tests of facial nerve function
Ask person to
Show their teeth
Purse lips
Blow out cheeks
Close eyes tightly
Open eyes as wide as they can

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 36
Tests of facial nerve power
With eyes tightly shut
attempt to gently pull the eyelids apart
With eyebrows raised
attempt to pull eyebrows downwards
With lips pursed tightly
attempt to pull lips apart
With cheeks blown out
press against the cheek to assess strength

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 37
The 8th (Acoustic) nerve
The 8th nerve has two functions
Auditory (hearing)
Vestibular (balance)

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 38
Tests of auditory function
Test each ear, one at a time
Block the opposite ear
Use a watch or rubbing
fingers together (in a quiet
environment), judge how far
away the sound can be
detected
If impaired in either ear
perform Rinne’s and Weber’s
test

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 39
Rinne’s test 1a
Use a 512 Hz tuning fork,
set it vibrating by gently
tapping on your knee
Place on mastoid process
(bone conduction)
Ask the person to tell you
when they can no longer
“hear” the sound

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 40
Rinne’s test 1b
Then place fork in front
of ear directly over the
auditory meatus (air
conduction)
Ask the patient again if
they can hear the
sound (normally louder
as air conduction is
better than bone
conduction)

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 41
Interpretation of Rinnes (method 1)
In a normal hearing the sound will be heard better when the tuning fork is placed in front of the ear
In conductive deafness (the sounds cannot conduct from the external to the inner ear) the sound will not be heard when the tuning fork is placed in front of the ear
In partial sensorineural deafness (due to damage to the cochlea, auditory nerve or auditory centres of the brain) the sound may be heard when the tuning fork is placed in front of the ear (but at a higher pitch normal hearing).
In complete sensorineural deafness no sound will be heard when the tuning for is placed in either position. (although there are exceptions to this)

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 42
Rinne’s 2
Alternatively
Place base of tuning fork
on mastoid process
Confirm it can be heard
Then immediately place
prongs in front of external
auditory meatus
Ask patient which is louder
- “behind the ear or in
front?

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 43
Interpretation of Rinnes (method 2)
In normal hearing the sound is loudest when the
tuning fork is placed in front of the ear
In conductive deafness the sound is loudest on the
mastoid process
In partial sensorineural deafness the sound is
loudest when the tuning fork is placed in front of the
ear (but at a higher pitch than in normal hearing).
In complete sensorineural deafness no sound will
be heard at the mastoid process or in front of the
ear.

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 44
Weber’s test
Hold the base of the
512 Hz tuning fork on
the vertex of the
patient’s head.
Ask which ear seems
to hear it louder.

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 45
Interpretation of Webers
In normal hearing the sound is equal in both
ears
In conductive deafness then the sound will
be loudest in the affected ear (as all external
sound is removed and effected ear picks up
the vibrating sound more acutely)
In sensorineural deafness all sounds are
diminished or absent.

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 46
Interpreting hearing tests
(an overview)
Interpretation of Rinne and Weber tests
Normal Conductive deafness
Partial sensorineural deafness
Weber Equal in both Deaf ear > good ear
Good ear > deaf ear
Rinne Air conduction > bone
Bone conduction > air
Air conduction > bone
Loss of hearing may be conductive (transmission of sound to the nerves
of hearing fails)
Sensorineural deafness reflects disorders of the nerve tissues)

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 47
Vestibular function of the 8th nerve
Gait
Ask patient to walk heel to toe
Gait veers to the affected side and is
unsteady
Usually worse with eyes shut

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 48
Nystagmus
Involuntary rhythmic eye movements
Peripheral or central vestibular, or cerebellum
Tested during eye movement assessment
Look in central position
Look during up, down and lateral movement
Hold the target steady at the limit of binocular
vision in each direction
Care: Normal people may have a few jerks at extreme lateral
gaze, especially if the target is outside the field of binocular
vision - ensure it is visible to both eyes.

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 49
Nystagmus types
May be rotary or linear
Jerk - slow drift of eye position in one
direction with a fast correction in the opposite
direction.
Nystagmus direction is that of fast phase
Pendular – oscillations roughly equal in both
directions

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 50
Points to note if nystagmus present
Eye position and gaze direction when nystagmus occurs
Direction of the fast movement and plane - horizontal,
vertical, rotatory
Is the abducting eye affected more than the adducting?
Does it occurs in other directions of gaze?
Typical description: linear nystagmus, fast phase to the left,
in both eyes on left lateral gaze.

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 51
Hallpike’s test
Examiner supports head
Hallpike’s
test
Used in testing for positional vertigo
Sit person up in a position so that when (s)he lies down, the head will extend over the end of couch
Turn the head to one side, ask person to look over the shoulder to that side.
Lie the patient back quickly, so that head extends and is supported by the examiner
Ensure continues to look over shoulder (now towards floor)
Ask about sensation of vertigo. Observe for nystagmus in direction of gaze, whether it fatigues with repeating the test.
Repeat for other side

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 52
Hallpike’s test interpretation
No vertigo, no nystagmus - normal
Vertigo plus nystagmus Central (brainstem) vestibular
non-fatigable
persists indefinitely during test posture
Repeatable indefinitely
Peripheral vestibular
Delayed-onset rotatory nystagmus
Fatigues
wears off in < 4 minutes
Repeat test less intense, shorter duration features

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 53
9th (Glossopharyngeal) nerve
Sensory
posterior 1/3rd of tongue, the pharynx and
middle ear
Motor
stylopharyngeus
Autonomic
parotid salivary gland
afferents from carotid baroreceptors

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 54
Testing the 9th nerve (sensory)
Gag reflex (not routinely done); test both sides
Afferent – glossopharyngeal; efferent – vagus (10th)
touch pharyngeal wall behind the pillars of the fauces
ask if patient can feel it, and observe any gag
no feeling or gag may mean ipsilateral 9th nerve dysfunction.
deviation of uvula one way indicates weakness on the other side = UMN / LMN lesion of vagus, 10th nerve –not 9th
Uvula moves on saying “Ahh” but not on gag isolated 9th nerve palsy (rare)

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 55
The 10th (Vagus) nerve
Sensory
tympanic membrane, external auditory canal, external ear
Motor
muscles of palate, pharynx and larynx
Autonomic
parasympathetic supply to and from thorax and abdomen

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 56
Testing the 10th nerve
Look at the uvula (use tongue depressor if
necessary)
Ask patient to say “Ahh”
Deviation to one side indicates weakness on
the other side (muscle normally “pulls”)
upper or lower motor neurone lesion
Does not move on saying “Ahh” or gag
bilateral palatal muscle paresis

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 57
11th (Accessory) nerve
Purely motor
Each cerebral hemisphere supplies
the ipsilateral sternomastoid muscle
the contralateral trapezius muscle
Therefore, a lesion on one side can give rise
to signs on both sides

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 58
Testing the 11th nerve
Sternomastoid
Ask patient to turn their head to one side. Stabilise
patient with shoulder counterpressure. Then put your
hand against patient’s chin and cheek and ask patient to
resist your rotating their head back to midline. Watch the
opposite sternomastoid contract, and test its power.
Trapezius
Ask the patient to shrug shoulders, push down against
movement. Do one side at a time.

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 59
Testing the 11th nerve
Inspect both
sternomastoid and
trapezius muscles for
wasting and fasciculation
Upward shrug
of shoulders -
test of trapezius
Turning head - test
of contralateral
sternomastoid
Weakness of
sternomastoid and
trapezius on the same side
- ipsilateral peripheral
accessory nerve lesion
Weakness of
sternomastoid and
contralateral trapezius -
upper motor neurone
lesion on the side of the
sternomastoid

12/1/2011 © Clinical Skills Resource Centre, University of Liverpool, UK 60
12th (Hypoglossal) nerve
Motor: intrinsic muscles of the tongue
Testing the 12th nerve
Open mouth. Examine tongue at rest inside mouth.
Fasciculation and / or wasting (atrophy)
LMN lesion (one side = nerve, both usually = bulbar palsy).
Put out tongue
Deviation to one side indicates weakness on that side (tongue muscle “pushes”).
Fasciculation during active movement is normal.
Waggle tongue (demonstrate to patient)
Normal smooth bulk, poor movement control, usually bilateral
UMN lesion (“pseudobulbar” palsy).
To test power: patient pushes tongue against cheek and examiner presses against skin - repeat for the other side.