Embed Size (px)
Citation preview

HOURSContinuing Education
36 AJN ▼ May 2016 ▼ Vol. 116, No. 5 ajnonline.com
CE 2.5
According to the American Cancer Society, more than 1.6 million new cases of cancer were diagnosed in the United States in 2014.1
Among patients with a cancer diagnosis, pain is one of the most commonly reported symptoms, though prevalence and quality of pain varies with type of treatment and stage of disease. A multinational sur-vey of nearly 5,100 adult patients with cancer found that the overall prevalence of reported pain was 84%, and among those who experienced pain sev-eral times a month, the quality of pain was charac-terized as moderate to severe by 94%, severe by 43%, and “worst pain imaginable” by 2%.2
The effect of cancer pain on quality of life is sub-stantial and multidimensional. It frequently results in high levels of depression, poor general health, poor physical and social functioning, and impaired ability to perform activities of daily living.2-4 It may engender feelings of being a burden to others and of wanting
to die.2 Cancer pain can also be refractory to anal-gesic medications, and many of the medications used to alleviate it can produce adverse effects that are dif-ficult to manage. With intrathecal delivery, however, some of these same analgesics can provide greater pain relief at dramatically lower doses and thus with fewer adverse effects.
The first known use of intrathecal drug adminis-tration for pain occurred in 1898 when the German surgeon August Bier successfully eliminated surgical pain by injecting intrathecal cocaine into a young man before resecting an infected ankle joint.5 In the late 1970s, U.S. physicians published the first report of intrathecal morphine administration for cancer pain.6 By the late 1980s two systems had been devel-oped for delivering intrathecal drugs.7
This article provides an overview of intrathecal analgesia, explaining how and why intrathecal ad-ministration may prolong the duration of action and
ABSTRACT: It is estimated that more than 1.6 million new cases of cancer were diagnosed in the United States in 2014. Among patients with cancer, moderate to severe pain is prevalent and can be refractory, even with the use of systemic opioids, which may cause adverse effects that are difficult to manage at the doses required to control pain. When delivered intrathecally, however, opioids and adjuvant analgesics may pro-vide greater pain relief at dramatically lower doses and with fewer adverse effects. Although the use of intra-thecal drug delivery systems for cancer pain management has increased dramatically over the past several years and is expected to continue growing, patients with intrathecal pumps often report interactions with nurses unfamiliar with the technology. This article provides an overview of intrathecal pump therapy and explains how it prolongs duration of action and improves the efficacy of certain analgesics while reducing their adverse effects. The author discusses the costs involved, the patients most likely to derive benefit, the types of pumps currently used in the United States, the medications that can be delivered intrathecally, the potential risks and complications associated with intrathecal therapy, and the nursing care required by pa-tients who use an intrathecal pump.
Keywords: analgesic therapy, cancer pain management, intrathecal drug delivery systems, intrathecal therapy, opioids
What every nurse should know about these programmable medication delivery systems.
Intrathecal Pumps for Managing Cancer Pain

[email protected] AJN ▼ May 2016 ▼ Vol. 116, No. 5 37
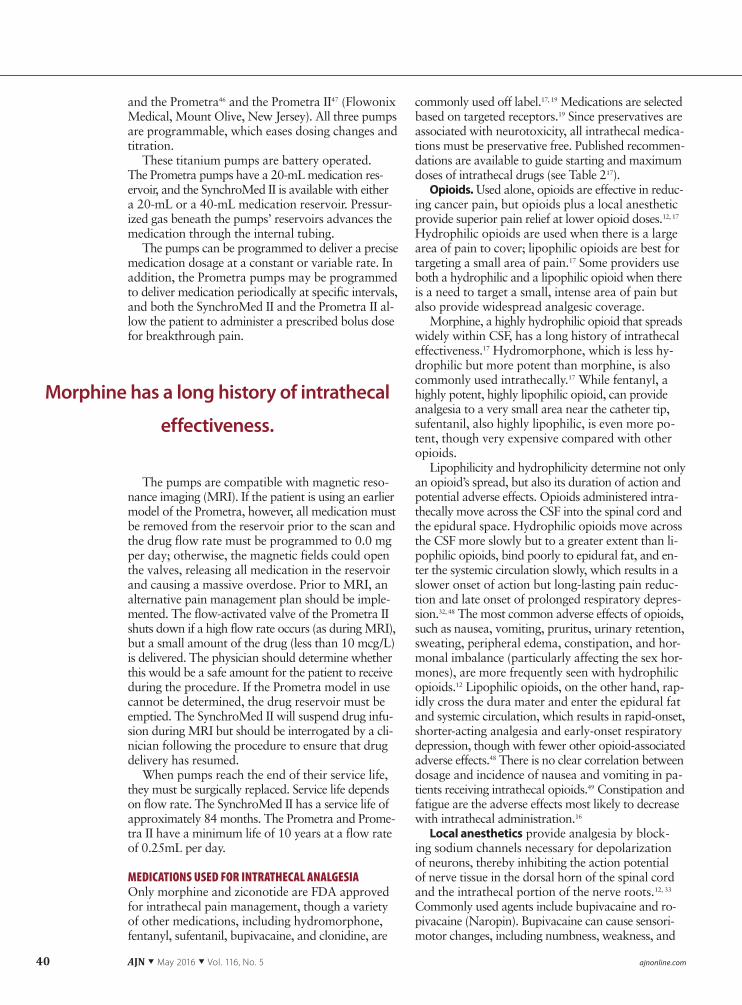
of the spinal cord.8 Located within the dural sheath, the intrathecal space, also known as the subarach-noid space, contains cerebrospinal fluid (CSF) and the spinal cord (see Figure 1). In the intrathecal space, opioids and other adjuvant analgesics encounter no anatomic barriers and vascular absorption of drugs is slow. Therefore, intrathecal administration of very small quantities of opioids, either alone or in combina-tion with adjuvant agents, introduces a highly con-centrated reservoir of analgesic medication close to the site of action, where it diffuses passively into the dor-sal horn, providing superior pain relief with minimal
By Laura Hanssen Textor, MSN, APRN
improve the efficacy of certain analgesics. It also iden-tifies which drugs can be delivered intrathecally. It dis-cusses the costs of intrathecal drug delivery systems (IDDSs), describes the patients most likely to derive benefit from intrathecal administration, and outlines the nursing care required by patients who use intra-thecal pumps, highlighting potential risks and com-plications associated with intrathecal drug therapy.
BENEFITS OF INTRATHECAL ANALGESIAPain can be modulated downward in the central ner-vous system via connections within the dorsal horn
Figure 1. The catheter from an intrathecal pump is inserted in the lumbar region of the spinal cord at the L3 level. The insert highlights the cauda equina and surrounding structures. CSF = cerebrospinal fluid. Illustration by Anne Rains.
Intrathecal pump
Filling port
Pump catheter
Intrathecal(subarachnoid)
space
Arachnoid
Dura
Epiduralspace
CSF Cauda equina
Intrathecal catheter
Intrathecal
Arachnoid
Dura CSF Cauda equinaCSFDura
Epidural
L1
L2
L3
L4
catheter
DuraDuraDura

38 AJN ▼ May 2016 ▼ Vol. 116, No. 5 ajnonline.com
adverse effects.9, 10 Bioavailability of an opioid depends on how hydrophilic (water soluble) or lipophilic (fat soluble) it is, with the more hydrophilic opioids (such as hydromorphone [Dilaudid] and morphine) having greater bioavailability than the more lipophilic opi-oids (such as alfentanil, fentanyl [Sublimaze], and suf-entanil [Sufenta]).11, 12
There is strong evidence to support use of an IDDS to manage cancer pain.7, 10, 13-16 When compared with comprehensive medical management of cancer pain that excluded spinally administered drugs, intrathe-cal analgesia has been shown to significantly reduce pain and medication toxicity7, 14, 16; improve mood10; enhance mental and physical function10, 14; improve quality of life10, 14; increase survival16; and demonstrate efficacy against neuropathic, mixed visceral, and so-matic pain.10, 13 Long-term intrathecal analgesia is ef-fective against chronic pain, including cancer pain, in up to 77% of patients, with some patients reporting pain relief within one month that was sustained over three years.17
When administered intrathecally, morphine and hydromorphone have been shown to have more than 400 times the potency they have when delivered sub-cutaneously.18 Though the relative potency of oral morphine to intrathecal morphine has not been de-finitively established, an oral to intrathecal ratio of 300 mg to 1 mg is commonly accepted in clinical practice (see Table 112, 19).19 The intrathecal route also makes it possible to target multiple pain recep-tors using a wide variety of medications,9, 20 includ-ing medications that cannot be administered by any other route.
When compared with epidural or systemic admin-istration, the intrathecal route has the lowest poten-tial for adverse effects. This is because most of the medication delivered remains concentrated within one centimeter of the catheter tip, having bypassed peripheral receptors responsible for many of the ad-verse effects associated with opioids.21, 22 When com-pared with comprehensive medical management, intrathecal administration has been shown to re-duce opioid toxicity by 51%.23
It’s easy to make dose changes with an IDDS us-ing wireless telemetry communication with the help
of a remotely controlled programming device pro-vided by the manufacturer. Refilling a pump requires only a brief in-office procedure. Using aseptic tech-nique and a refill kit provided by the manufacturer, the pump can be accessed, and medication remain-ing in the reservoir can be aspirated and replaced with new medication. Refill intervals can be as long as three months, depending on the concentration and amount of drugs required for pain control.
For patients with opioid-refractory cancer pain, un-manageable opioid adverse effects, or the expectation of severe pain with disease progression, the benefits of intrathecal therapy generally outweigh any con-cerns associated with its use.
COST CONCERNSIn 2011, the Medicare allowable cost for implanting an intrathecal pump was $35,601, which is a realistic estimate of the total cost, including the cost of the de-vice and catheter, professional fees, facility fees, and initial fill medication.24 Despite this high initial cost, a 2013 study found that when used to manage intrac-table cancer pain, intrathecal therapy (including med-ications, pump implantation, and maintenance) may achieve cost equivalence to that of high-cost, conven-tional analgesic therapy within 7.4 months.24 The authors calculated the median monthly cost of can-cer pain medication for 36 patients receiving either low cost (n = 24) or high cost (n = 12) conventional analgesic therapy as $400 and $5,246, respectively, before the use of an IDDS and as $487 after IDDS implantation. They concluded that, for patients with refractory cancer pain and a relatively long life ex-pectancy, intrathecal therapy may be cost beneficial within six months. An IDDS is generally indicated for patients with a life expectancy of at least three months.
POTENTIAL RISKSIntrathecal therapy is not without risk. The catheter can become dislodged, fractured, or occluded.25-29 A granuloma, which is a noninfectious mass of cellular debris that can form at the tip of the catheter,19, 28, 30 can potentially cause spinal cord compression. Sur-gical site infection can occur31, 32 and, if infection mi-grates up the catheter, could result in life-threatening meningitis.19, 25, 28, 33 During refills, medication may inadvertently be instilled into the pocket around the pump, resulting in a potentially fatal drug over-dose.25, 30, 34 Like all mechanical devices, the pump can malfunction, fail, or leak.19, 25, 33, 35 In addition, programming errors can result in overdose or insuf-ficient dosing.28, 33
The incidence of complications is generally con-sidered to be low, with reported rates as follows: • catheter migration, 5.3%36 • catheter fracture, 5.3%36 • occlusion, 1.8%37
Morphine Dose Route of Administration
300 mg Oral
100–200 mg Intravenous
10 mg Epidural
1 mg Intrathecal
Table 1. Approximate Equivalent Doses of Mor-phine Based on Route of Administration12, 19

[email protected] AJN ▼ May 2016 ▼ Vol. 116, No. 5 39
• bacterial meningitis, 2.8%38 • surgical wound infection, 2.7%31 to 8.8%36 • granuloma, less than 3%39 to 3.5%36 • mechanical failure of pump or battery, 5%40
Actual incidence of complications may be higher, however, owing to underreporting.
PATIENT SELECTIONDetermining which patients might benefit from an IDDS is important. Certain cancers are known to be associated with a high prevalence of pain, including the following19, 41: • prostate, 56% to 94%• head and neck, 67% to 91%• uterine, 30% to 90%• urogenital, 58% to 90%• breast, 40% to 89%• pancreatic, 72% to 85%• multiple myeloma, 73%• lung, 61%
In patients with cancer known to cause refrac-tory pain, early implantation of an IDDS can be considered even before the use of systemic opioids.42 Postponing implantation until widespread meta-static disease has developed—when the patient may experience extreme pain and demonstrate significant opioid tolerance—often results in suboptimal relief. Patients with cancer pain that has responded poorly to escalating opioid therapy and those with intolera-ble opioid adverse effects may also be candidates for intrathecal therapy.19
Contraindications include ongoing infection, in-ability to implant the pump an inch or less from the skin’s surface (due to anasarca, for example), insuffi-cient body size to accept the pump’s bulk and weight, spinal abnormalities,43, 44 and inability to interrupt anticoagulant therapy.10 Other factors to consider in-clude• patient expectations of the device capabilities.33 • patient history of adherence to a treatment plan
and ability to keep appointments for pump main-tenance.45
• patient’s general medical status, psychological sta-tus, social support, and disease prognosis.10
• availability of skilled, knowledgeable physicians and nurses able to provide ongoing pump man-agement if hospice is required.
PLACEMENT OF AN INTRATHECAL PUMPIn the past, a prepump psychological evaluation followed by an intrathecal trial was considered criti-cal in determining likelihood of therapy success. As evidence supporting the efficacy of intrathecal ther-apy for cancer pain has grown, however, many in-surance companies have relaxed that requirement. Today—with the exception of Medicare, which still requires an intrathecal trial—it is relatively uncom-mon for insurance payers to require patients with
cancer pain to undergo a trial. Medications used during a trial include morphine, hydromorphone, fentanyl, ziconotide (Prialt), bupivacaine (Marcaine Spinal), clonidine (Duraclon), and sufentanil. The trial medication is injected into the intrathecal space as a one-time dose or administered over several hours or days through an intrathecal catheter connected to an external pump.17
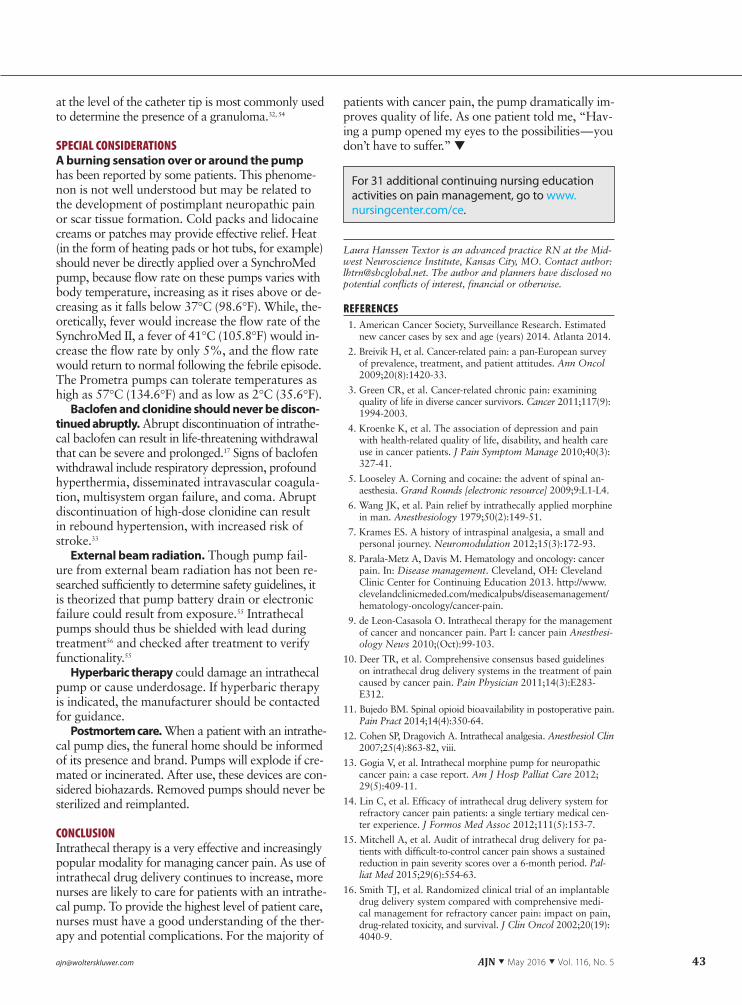
Placement of an intrathecal pump involves two surgical procedures: one to place the catheter into the intrathecal space and another to place the pump un-der the skin. A small incision is made over the lum-bar spine and, unless anatomy or other circumstances require alternative placement, a needle is inserted at L2–L3 or L3–L4 because lower areas of the spine are more mobile, increasing the risk of catheter displace-ment or damage.32 Under fluoroscopic guidance, the catheter is then threaded to the appropriate level of the spinal cord and anchored in place. Next, a shal-low pump pocket is created between the skin and the fascia (see Figure 2). Manufacturers recommend that the pump be placed in the lower abdomen,32 though the flank or posterior buttock can also be used. The pump is placed in the pocket and sutured to the fas-cia. A special tool provided by the pump manufac-turer is used to create a tunnel under the skin from the pump pocket to the catheter. The catheter is then pulled through to the pump pocket, and the pump is filled with medication. The catheter is secured to the pump and the incision is closed. The pump is pro-grammed to deliver the ordered dose of medication.
APPROVED PROGRAMMABLE INTRATHECAL PUMPSThree implantable intrathecal pumps are approved for patient use by the U.S. Food and Drug Administration (FDA): the SynchroMed II (Medtronic, Minneapolis),44
Figure 2. Creating the pump pocket. Used with permission from William S. Rosenberg, MD.
40 AJN ▼ May 2016 ▼ Vol. 116, No. 5 ajnonline.com
and the Prometra46 and the Prometra II47 (Flowonix Medical, Mount Olive, New Jersey). All three pumps are programmable, which eases dosing changes and titration.
These titanium pumps are battery operated. The Prometra pumps have a 20-mL medication res-ervoir, and the SynchroMed II is available with either a 20-mL or a 40-mL medication reservoir. Pressur-ized gas beneath the pumps’ reservoirs advances the medication through the internal tubing.
The pumps can be programmed to deliver a precise medication dosage at a constant or variable rate. In addition, the Prometra pumps may be programmed to deliver medication periodically at specific intervals, and both the SynchroMed II and the Prometra II al-low the patient to administer a prescribed bolus dose for breakthrough pain.
The pumps are compatible with magnetic reso-nance imaging (MRI). If the patient is using an earlier model of the Prometra, however, all medication must be removed from the reservoir prior to the scan and the drug flow rate must be programmed to 0.0 mg per day; otherwise, the magnetic fields could open the valves, releasing all medication in the reservoir and causing a massive overdose. Prior to MRI, an alternative pain management plan should be imple-mented. The flow-activated valve of the Prometra II shuts down if a high flow rate occurs (as during MRI), but a small amount of the drug (less than 10 mcg/L) is delivered. The physician should determine whether this would be a safe amount for the patient to receive during the procedure. If the Prometra model in use cannot be determined, the drug reservoir must be emptied. The SynchroMed II will suspend drug infu-sion during MRI but should be interrogated by a cli-nician following the procedure to ensure that drug delivery has resumed.
When pumps reach the end of their service life, they must be surgically replaced. Service life depends on flow rate. The SynchroMed II has a service life of approximately 84 months. The Prometra and Prome-tra II have a minimum life of 10 years at a flow rate of 0.25mL per day.
MEDICATIONS USED FOR INTRATHECAL ANALGESIAOnly morphine and ziconotide are FDA approved for intrathecal pain management, though a variety of other medications, including hydromorphone, fentanyl, sufentanil, bupivacaine, and clonidine, are
commonly used off label.17, 19 Medications are selected based on targeted receptors.19 Since preservatives are associated with neurotoxicity, all intrathecal medica-tions must be preservative free. Published recommen-dations are available to guide starting and maximum doses of intrathecal drugs (see Table 217).
Opioids. Used alone, opioids are effective in reduc-ing cancer pain, but opioids plus a local anesthetic provide superior pain relief at lower opioid doses.12, 17 Hydrophilic opioids are used when there is a large area of pain to cover; lipophilic opioids are best for targeting a small area of pain.17 Some providers use both a hydrophilic and a lipophilic opioid when there is a need to target a small, intense area of pain but also provide widespread analgesic coverage.
Morphine, a highly hydrophilic opioid that spreads widely within CSF, has a long history of intrathecal effectiveness.17 Hydromorphone, which is less hy-drophilic but more potent than morphine, is also commonly used intrathecally.17 While fentanyl, a highly potent, highly lipophilic opioid, can provide analgesia to a very small area near the catheter tip, sufentanil, also highly lipophilic, is even more po-tent, though very expensive compared with other opioids.
Lipophilicity and hydrophilicity determine not only an opioid’s spread, but also its duration of action and potential adverse effects. Opioids administered intra-thecally move across the CSF into the spinal cord and the epidural space. Hydrophilic opioids move across the CSF more slowly but to a greater extent than li-pophilic opioids, bind poorly to epidural fat, and en-ter the systemic circulation slowly, which results in a slower onset of action but long-lasting pain reduc-tion and late onset of prolonged respiratory depres-sion.32, 48 The most common adverse effects of opioids, such as nausea, vomiting, pruritus, urinary retention, sweating, peripheral edema, constipation, and hor-monal imbalance (particularly affecting the sex hor-mones), are more frequently seen with hydrophilic opioids.12 Lipophilic opioids, on the other hand, rap-idly cross the dura mater and enter the epidural fat and systemic circulation, which results in rapid-onset, shorter-acting analgesia and early-onset respiratory depression, though with fewer other opioid-associated adverse effects.48 There is no clear correlation between dosage and incidence of nausea and vomiting in pa-tients receiving intrathecal opioids.49 Constipation and fatigue are the adverse effects most likely to decrease with intrathecal administration.16
Local anesthetics provide analgesia by block-ing sodium channels necessary for depolarization of neurons, thereby inhibiting the action potential of nerve tissue in the dorsal horn of the spinal cord and the intrathecal portion of the nerve roots.12, 33 Commonly used agents include bupivacaine and ro-pivacaine (Naropin). Bupivacaine can cause sensori-motor changes, including numbness, weakness, and
Morphine has a long history of intrathecal
effectiveness.

[email protected] AJN ▼ May 2016 ▼ Vol. 116, No. 5 41
bowel or bladder incontinence. Ropivacaine is nearly identical to bupivacaine in terms of onset, quality, and duration of block, though the intensity of its motor block tends to be lower.17 Potential adverse effects in-clude sensory deficits, paresthesia, motor impairment, urinary retention, hypotension, diaphoresis, fatigue, somnolence, autonomic dysfunction, and neurotox-icity, though adverse effects are generally not seen at low doses (less than 15 mg per day).28, 33 `2-adrenergic agonists provide analgesia two
ways: by inhibiting spinal cord glial cell activation and by binding to receptors on primary afferent neu-rons, thus hyperpolarizing the neurons and reducing the release of neurotransmitters involved in pain sig-naling.17, 28 One such agent, clonidine, is associated with such adverse effects as nausea, dizziness, confu-sion, sedation, orthostatic hypotension, bradycardia, and dry mouth.33 Depression, insomnia, and night ter-rors have also been reported.33 f-aminobutyric acid (GABA)-A receptors play a
critical role in inhibiting the system responsible for implementing and perpetuating pain. Baclofen (Ga-blofen, Lioresal) is a GABA agonist with antihyper-algesic effects at the spinal level that has been shown to produce analgesia and reduce sensitivity at doses that do not impair motor function.12 Baclofen may be particularly helpful in reducing pain secondary to underlying muscle spasm, which is commonly asso-ciated with bony metastasis.
Ziconotide is a synthetic form of the toxin pro-duced by the Conus magus snail.50 This nonopioid, atypical analgesic is FDA approved as a first-line agent for managing cancer pain.17 Within the dorsal horn of the spinal cord, N-type calcium channel blockers are present in pain pathways. Ziconotide reversibly and selectively blocks the influx of cal-cium into the cells, reducing the release of multiple neurotransmitters responsible for pain transmis-sion.50, 51 Ziconotide, which can be given only intra-thecally, has no mu activity and is not associated with respiratory depression. However, it has a very
narrow therapeutic window and is associated with numerous adverse effects, including suicidal thoughts, worsening mood disorders, cognitive impairment, psychosis (with auditory or visual hallucinations), impaired memory, vertigo, speech disorders, hypo-tension, diaphoresis, nausea, acute urinary retention, muscle cramps, creatine phosphokinase elevation, nystagmus, abnormal gait, and amblyopia.9, 17, 50, 51
In a study of 77 patients with cancer pain who were treated with ziconotide, 44 (57%) reported ex-periencing adverse events, but discontinuation was re-quired in only seven (9%).51 The FDA recommends that starting dosages of ziconotide should not exceed 2.4 mcg per day and that dosages should increase in steps no greater than 2.4 mcg per day, titrated up-ward no more frequently than every 48 hours.51 Most serious adverse drug effects are associated with too high a starting dose or too rapid titration.50
N-methyl-d-aspartate (NMDA) antagonists. Ket-amine is an NMDA receptor antagonist that blocks the action of glutamate and facilitates GABA.17 On the basis of postmortem spinal cord tissue studies, it is considered neurotoxic; but it is unknown which pa-tients will develop neurotoxicity, at what dose, over what duration, and how they will present. Ketamine, however, can be very effective in reducing cancer pain that is unresponsive to other agents and for severe neuropathic pain.52
CARING FOR THE PATIENT WITH AN INTRATHECAL PUMPAdmission nursing care. When admitting a patient with an intrathecal pump, ask the patient or family to provide the name of the physician managing the pump. Then contact the managing physician’s office and request the following information in printed form:• the level of the catheter tip• medications and concentrations administered by
basal or continuous dose• patient-administered dosage, if applicable• pump reservoir volume• refill alarm date
Drug Starting Dosage Range Maximum Dosage
Morphine 0.1–0.5 mg/day 15 mg/day
Hydromorphone 0.02–0.5 mg/day 10 mg/day
Ziconotide 0.5–2.4 mcg/day 19.2 mcg/day
Fentanyl 25–75 mcg/day No known upper limit
Bupivacaine 1–4 mg/day 10 mg/day
Clonidine 40–100 mcg/day 40–600 mcg/day
Sufentanil 10–20 mcg/day No known upper limit
Table 2. Recommended Starting and Maximum Dosages of Intrathecal Medications17

42 AJN ▼ May 2016 ▼ Vol. 116, No. 5 ajnonline.com
The office staff should also provide contact informa-tion for manufacturer representatives in the event that an emergency occurs or the nursing staff is unfa-miliar with the product.
Postoperative nursing care following pump im-plantation includes vigilant monitoring of respira-tory status, surgical sites, and control of surgical pain. Respiratory depression is a rare but life-threatening event. After initiation of intrathecal opioid therapy, patients should be monitored for respiratory de-pression (that is, for respiratory rate, oxygenation, and level of consciousness) every one to two hours during the first 12 hours following initiation and every two hours for the next 12 hours.17 Comorbid-ities that place patients at greatest risk for respira-tory depression include central or obstructive sleep apnea, chronic obstructive pulmonary disease, smok-ing, obesity, and concurrent use of sedating drugs.17 Respiratory depression is managed with respira-tory and cardiac support, transfer to a high acuity level of care, reducing intrathecal medication to the lowest possible dosage, discontinuation of sys-temic sedating medications, and ruling out other causes.25
To reduce postoperative bleeding, anticoagulants should be withheld until their administration is ap-proved by the physician who implants the pump. Anticoagulants can usually be resumed two to three days after surgery. An abdominal binder may be used to hold the pump flat within the pocket for two to four weeks following surgery. This will al-low time for the pump to become further embed-ded in the pocket, reducing the chance that it will flip over or that fluid will accumulate in the pocket. Patient education should reinforce the need to ad-here vigilantly to postoperative restrictions, which include• no lifting more than five pounds.• no raising arms overhead.• no bending or twisting at the waist for six weeks.
Individual surgeons may further restrict postopera-tive activity.
A common misperception is that the pump is ca-pable of relieving any pain the patient experiences. Do not expect the pump to provide relief from pain related to surgery, including pain along the tunneling path. Systemic short-acting opioids will be necessary to manage such situations. For pain related to cancer, a patient-managed bolus should be used if available.
In the interest of patient safety, long-acting opioids should not be given.
MONITORING FOR COMPLICATIONSPatients with intrathecal pumps must be monitored for three types of complications: surgical, pump re-lated, or catheter related.
Surgical complications include infection, menin-gitis, bleeding, pocket seromas or hematomas, and post–dural puncture headaches. A CSF leak can occur anytime and presents as a raised, swollen, nonred, nonwarm, nontender area under the lum-bar incision. It may or may not be accompanied by a postural headache, depending on the extent of the leak. If a CFS leak occurs, the physician who implanted the pump should be notified. It is not considered an emergency, however, and is treated with bed rest.17
Pump-related complications include pump mal-function and pump flipping or tilting.32 Pump malfunc-tion, which is uncommon, tends to cause underdosing or overdosing of medication,32, 53 and manifests as loss of pain control or sudden somnolence. If there is reason to believe the pump has flipped or tilted,
apply an abdominal binder. No attempt should be made to manually return the pump to its normal position. In either case, notify the physician.
Catheter complications, the most common rea-sons for therapy failure, include microfracture, leaks, disconnection, breakage, kinks, migration, partial oc-clusion, or granuloma formation.25, 32, 45 Symptoms are frequently subtle, presenting as a change in pain con-trol or as opioid withdrawal.32 When such symptoms occur, X-ray or computed tomography to evaluate catheter location is indicated, though a catheter dye study performed under fluoroscopy may be neces-sary.
Granuloma formation, though uncommon, is a particularly concerning complication that should be considered any time there is evidence of reduced medication efficacy or the patient presents with new neurologic symptoms at or below the level of the catheter tip, including new pain onset, numbness, limb weakness, or bowel or bladder incontinence.32, 54 A complete patient history and a thorough neuro-logic examination—including assessment of deep ten-don reflexes, sensory changes, and proprioception—is indicated.32 The physician should be notified imme-diately. Thin-slice MRI with gadolinium performed
Constipation and fatigue are the adverse effects most likely
to decrease with intrathecal administration.
[email protected] AJN ▼ May 2016 ▼ Vol. 116, No. 5 43
at the level of the catheter tip is most commonly used to determine the presence of a granuloma.32, 54
SPECIAL CONSIDERATIONS A burning sensation over or around the pump has been reported by some patients. This phenome-non is not well understood but may be related to the development of postimplant neuropathic pain or scar tissue formation. Cold packs and lidocaine creams or patches may provide effective relief. Heat (in the form of heating pads or hot tubs, for example) should never be directly applied over a SynchroMed pump, because flow rate on these pumps varies with body temperature, increasing as it rises above or de-creasing as it falls below 37°C (98.6°F). While, the-oretically, fever would increase the flow rate of the SynchroMed II, a fever of 41°C (105.8°F) would in-crease the flow rate by only 5%, and the flow rate would return to normal following the febrile episode. The Prometra pumps can tolerate temperatures as high as 57°C (134.6°F) and as low as 2°C (35.6°F).
Baclofen and clonidine should never be discon-tinued abruptly. Abrupt discontinuation of intrathe-cal baclofen can result in life-threatening withdrawal that can be severe and prolonged.17 Signs of baclofen withdrawal include respiratory depression, profound hyperthermia, disseminated intravascular coagula-tion, multisystem organ failure, and coma. Abrupt discontinuation of high-dose clonidine can result in rebound hypertension, with increased risk of stroke.33
External beam radiation. Though pump fail-ure from external beam radiation has not been re-searched sufficiently to determine safety guidelines, it is theorized that pump battery drain or electronic failure could result from exposure.55 Intrathecal pumps should thus be shielded with lead during treatment56 and checked after treatment to verify functionality.55
Hyperbaric therapy could damage an intrathecal pump or cause underdosage. If hyperbaric therapy is indicated, the manufacturer should be contacted for guidance.
Postmortem care. When a patient with an intrathe-cal pump dies, the funeral home should be informed of its presence and brand. Pumps will explode if cre-mated or incinerated. After use, these devices are con-sidered biohazards. Removed pumps should never be sterilized and reimplanted.
CONCLUSIONIntrathecal therapy is a very effective and increasingly popular modality for managing cancer pain. As use of intrathecal drug delivery continues to increase, more nurses are likely to care for patients with an intrathe-cal pump. To provide the highest level of patient care, nurses must have a good understanding of the ther-apy and potential complications. For the majority of
patients with cancer pain, the pump dramatically im-proves quality of life. As one patient told me, “Hav-ing a pump opened my eyes to the possibilities—you don’t have to suffer.” ▼
Laura Hanssen Textor is an advanced practice RN at the Mid-west Neuroscience Institute, Kansas City, MO. Contact author: [email protected]. The author and planners have disclosed no potential conflicts of interest, financial or otherwise.
REFERENCES1. American Cancer Society, Surveillance Research. Estimated
new cancer cases by sex and age (years) 2014. Atlanta 2014.
2. Breivik H, et al. Cancer-related pain: a pan-European survey of prevalence, treatment, and patient attitudes. Ann Oncol 2009;20(8):1420-33.
3. Green CR, et al. Cancer-related chronic pain: examining quality of life in diverse cancer survivors. Cancer 2011;117(9): 1994-2003.
4. Kroenke K, et al. The association of depression and pain with health-related quality of life, disability, and health care use in cancer patients. J Pain Symptom Manage 2010;40(3): 327-41.
5. Looseley A. Corning and cocaine: the advent of spinal an-aesthesia. Grand Rounds [electronic resource] 2009;9:L1-L4.
6. Wang JK, et al. Pain relief by intrathecally applied morphine in man. Anesthesiology 1979;50(2):149-51.
7. Krames ES. A history of intraspinal analgesia, a small and personal journey. Neuromodulation 2012;15(3):172-93.
8. Parala-Metz A, Davis M. Hematology and oncology: cancer pain. In: Disease management. Cleveland, OH: Cleveland Clinic Center for Continuing Education 2013. http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/hematology-oncology/cancer-pain.
9. de Leon-Casasola O. Intrathecal therapy for the management of cancer and noncancer pain. Part I: cancer pain Anesthesi-ology News 2010;(Oct):99-103.
10. Deer TR, et al. Comprehensive consensus based guidelines on intrathecal drug delivery systems in the treatment of pain caused by cancer pain. Pain Physician 2011;14(3):E283-E312.
11. Bujedo BM. Spinal opioid bioavailability in postoperative pain. Pain Pract 2014;14(4):350-64.
12. Cohen SP, Dragovich A. Intrathecal analgesia. Anesthesiol Clin 2007;25(4):863-82, viii.
13. Gogia V, et al. Intrathecal morphine pump for neuropathic cancer pain: a case report. Am J Hosp Palliat Care 2012; 29(5):409-11.
14. Lin C, et al. Efficacy of intrathecal drug delivery system for refractory cancer pain patients: a single tertiary medical cen-ter experience. J Formos Med Assoc 2012;111(5):153-7.
15. Mitchell A, et al. Audit of intrathecal drug delivery for pa-tients with difficult-to-control cancer pain shows a sustained reduction in pain severity scores over a 6-month period. Pal-liat Med 2015;29(6):554-63.
16. Smith TJ, et al. Randomized clinical trial of an implantable drug delivery system compared with comprehensive medi-cal management for refractory cancer pain: impact on pain, drug-related toxicity, and survival. J Clin Oncol 2002;20(19): 4040-9.
For 31 additional continuing nursing education activities on pain management, go to www. nursingcenter.com/ce.

44 AJN ▼ May 2016 ▼ Vol. 116, No. 5 ajnonline.com
17. Deer TR, et al. Polyanalgesic Consensus Conference 2012: recommendations for the management of pain by intrathecal (intraspinal) drug delivery: report of an interdisciplinary ex-pert panel. Neuromodulation 2012;15(5):436-64; discussion 464-6.
18. Abram SE, et al. Assessment of the potency and intrinsic ac-tivity of systemic versus intrathecal opioids in rats. Anesthe-siology 1997;87(1):127-34; discussion 27A-29A.
19. Bhatia G, et al. Intrathecal drug delivery (ITDD) systems for cancer pain [version 4]. 2014. http://f1000research.com/articles/2-96/v4.
20. Abdolmohammadi S, et al. Efficacy of an intrathecal multi-drug infusion for pain control in older adults and in end-stage malignancies: a report of three cases. Pain Res Manag 2015; 20(3):118-22.
21. Bernards CM. Cerebrospinal fluid and spinal cord distribu-tion of baclofen and bupivacaine during slow intrathecal in-fusion in pigs. Anesthesiology 2006;105(1):169-78.
22. Miljanich G, et al. Spinal mechanisms of pain and analgesia. Pain Pract 2013;13(2):114-30.
23. Smith TJ, Coyne PJ. Implantable drug delivery systems (IDDS) after failure of comprehensive medical management (CMM) can palliate symptoms in the most refractory cancer pain pa-tients. J Palliat Med 2005;8(4):736-42.
24. Brogan SE, et al. A cost utilization analysis of intrathecal ther-apy for refractory cancer pain: identifying factors associated with cost benefit. Pain Med 2013;14(4):478-86.
25. Deer TR, et al. Polyanalgesic Consensus Conference—2012: recommendations to reduce morbidity and mortality in intra-thecal drug delivery in the treatment of chronic pain. Neuro-modulation 2012;15(12):467-82.
26. Fabiano AJ, et al. Distal baclofen pump catheter migration as-sociated with far-lateral paraspinal surgical placement. Neuro-modulation 2009;12(2):130-3.
27. Kim JH, et al. An intrathecally located broken catheter used for an intrathecal drug delivery system. J Korean Med Sci 2012;27(10):1278-81.
28. Pasero C, et al. Intraspinal analgesia (epidural and intrathe-cal). In: Pasero C, McCaffery M, eds. Pain assessment and pharmacologic management. St. Louis: Elsevier/Mosby; 2011. p. 404-41.
29. Williams BS, Christo PJ. Obstructed catheter connection pin discovered during intrathecal baclofen pump exchange. Clin J Pain 2009;25(3):256-9.
30. Pope JE, Deer TR. Guide to implantable devices for intrathe-cal therapy. Pract Pain Manag 2013;12(8):56-62.
31. Engle MP, et al. Infectious complications related to intrathe-cal drug delivery system and spinal cord stimulator system implantations at a comprehensive cancer pain center. Pain Physician 2013;16(3):251-7.
32. Prager J, et al. Best practices for intrathecal drug delivery for pain. Neuromodulation 2014;17(4):354-72.
33. Tay W, Ho KY. The role of interventional therapies in can-cer pain management. Ann Acad Med Singapore 2009;38(11): 989-97.
34. Peccora CD, et al. Aberrant intrathecal pump refill: ultrasound-guided aspiration of a substantial quantity of subcutaneous hydromorphone. Reg Anesth Pain Med 2013;38(6):544-6.
35. Perruchoud C, et al. Silicone septum leakage at the origin of a drug overdose in a patient implanted with an intrathecal pump. Neuromodulation 2013;16(5):467-70.
36. Atli A, et al. Intrathecal opioid therapy for chronic nonma-lignant pain: a retrospective cohort study with 3-year follow-up. Pain Med 2010;11(7):1010-6.
37. Rauck RL, et al. Long-term intrathecal opioid therapy with a patient-activated, implanted delivery system for the treat-ment of refractory cancer pain. J Pain 2003;4(8):441-7.
38. Ver Donck A, et al. An open-label, multicenter study of the safety and efficacy of intrathecal ziconotide for severe chronic pain when delivered via an external pump. Neuromodulation 2008;11(2):103-11.
39. Medel R, et al. Catheter-tip mass mimicking a spinal epidural hematoma. J Neurosurg Spine 2010;12(1):66-71.
40. Turner JA, et al. Programmable intrathecal opioid delivery systems for chronic noncancer pain: a systematic review of ef-fectiveness and complications. Clin J Pain 2007;23(2):180-95.
41. Porta-Sales J, et al. Have we improved pain control in can-cer patients? A multicenter study of ambulatory and hospi-talized cancer patients. J Palliat Med 2015;18(11):923-32.
42. Vissers KC, et al. 23. Pain in patients with cancer. Pain Pract 2011;11(5):453-75.
43. Medtronic. SynchroMed II infusion system patient man-ual. Minneapolis; 2012. #8637 2012-03 https://professional.medtronic.com/wcm/groups/mdtcom_sg/@mdt/@neuro/ documents/documents/pump-syc28637-ptmanl.pdf.
44. Medtronic. SynchroMed programmable infusion systems: clinical reference guide. Minneapolis; 2013. https://professional.medtronic.com/wcm/groups/mdtcom_sg/@mdt/@neuro/ documents/documents/synchii-ref-guide.pdf.
45. Bottros MM, Christo PJ. Current perspectives on intrathecal drug delivery. J Pain Res 2014;7:615-26.
46. Flowonix Medical. Prometra programmable pump system brief summary: indications, safety, and warnings. Mt. Olive, NJ; 2013 Apr. http://www.flowonix.com/sites/default/files/Indications-Safety-Warnings.pdf.
47. Flowonix Medical. Prometra II programmable pump for use with intrathecal catheter. Mt. Olive, NJ; 2015. http://www.flowonix.com/sites/default/files/PL-31790-00%20-%20Prometra%20II%20Programmable%20Pump%20IFU%20(Flowonix%20-%20US%20Commercial).pdf.
48. Rathmell JP, et al. The role of intrathecal drugs in the treat-ment of acute pain. Anesth Analg 2005;101(5 Suppl):S30-S43.
49. Raffaeli W, et al. Opioid-related side-effects after intrathe-cal morphine: a prospective, randomized, double-blind dose- response study. Eur J Anaesthesiol 2006;23(7):605-10.
50. Sanford M. Intrathecal ziconotide: a review of its use in pa-tients with chronic pain refractory to other systemic or intra-thecal analgesics. CNS Drugs 2013;27(11):989-1002.
51. Dupoiron D, et al. Ziconotide adverse events in patients with cancer pain: a multicenter observational study of a slow titra-tion, multidrug protocol. Pain Physician 2012;15(5):395-403.
52. Vranken JH, et al. Treatment of neuropathic cancer pain with continuous intrathecal administration of S +-ketamine. Acta Anaesthesiol Scand 2004;48(2):249-52.
53. Maino P, et al. Fentanyl overdose caused by malfunction of SynchroMed II intrathecal pump: two case reports. Reg Anesth Pain Med 2014;39(5):434-7.
54. Deer TR, et al. Polyanalgesic Consensus Conference—2012: consensus on diagnosis, detection, and treatment of catheter-tip granulomas (inflammatory masses). Neuromodulation 2012;15(5).
55. Gebhardt R, et al. Implanted intrathecal drug delivery sys-tems and radiation treatment. Pain Med 2013;14(3):398-402.
56. Stearns L, et al. Intrathecal drug delivery for the management of cancer pain: a multidisciplinary consensus of best clinical practices. J Support Oncol 2005;3(6):399-408.