Embed Size (px)
Citation preview

22 AJN ▼ May 2017 ▼ Vol. 117, No. 5 ajnonline.com
HOURS
ORIGINAL RESEARCHContinuing EducationCE
Health care continues to change at a pace unimaginable even a few decades ago. In re-cent years, the Institute of Medicine (IOM)
and various professional organizations have ad-dressed the need for health care providers and sys-tems to evolve in order to meet the increasingly complex needs of patients, families, and popula-tions.1-6 Yet, although some improvements have been made, preventable adverse events remain a serious problem, causing or contributing to an esti-mated 440,000 deaths per year in this country.7
In 2003 the IOM published two important re-ports. The first, Keeping Patients Safe: Transforming the Work Environment of Nurses, identified the criti-cal role of nurses in providing safe patient care and outlined the systems and structures that were needed to ensure such care.6 The second, Health Professions Education: A Bridge to Quality, focused on the role of education, stating that “[a]ll health professionals should be educated to deliver patient-centered care as members of an interprofessional team, emphasizing evidence-based practice, quality improvement ap-proaches, and informatics.”8 In that second report,
Findings on the developmental progression of eight nursing competencies and related knowledge, skill, and attitudes.
the IOM identified five core competencies: evidence-based practice, informatics, patient-centered care, qual-ity improvement, and teamwork and collaboration. In response to these reports, with funding from the Rob-ert Wood Johnson Foundation, the Quality and Safety Education for Nurses (QSEN) project was developed to identify additional nursing competencies—quality improvement was separated into two competencies, quality improvement and safety—and to integrate these competencies into nursing education.9, 10 The QSEN project also proposed targets for the knowl-edge, skills, and attitudes (KSAs) that nurses would need for each competency.
Although the QSEN competencies have been ad-opted in undergraduate and graduate curricula at schools of nursing nationwide,11 their integration into practice settings remains limited.12, 13 Recognizing the importance of such integration in today’s complex health care environment, Lyle-Edrosolo and Waxman have described the need for alignment of the QSEN competencies with both the Joint Commission accred-itation standards and the American Nurses Creden-tialing Center Magnet model competencies, which are
1.5
Creating an Evidence-Based Progression for Clinical Advancement Programs

[email protected] AJN ▼ May 2017 ▼ Vol. 117, No. 5 23
ABSTRACTBackground: The Institute of Medicine (IOM) and the Quality and Safety Education for Nurses (QSEN) project have identified six nursing competencies and supported their integration into undergraduate and graduate nursing curricula nationwide. But integration of those competencies into clinical practice has been limited, and evidence for the progression of competency proficiency within clinical advancement programs is scant. Using an evidence-based approach and building on the competencies identified by the IOM and QSEN, a team of experts at an academic health system developed eight competency domains and 186 related knowl-edge, skills, and attitudes (KSAs) for professional nursing practice.
Purpose: The aim of our study was to validate the eight identified competencies and 186 related KSAs and determine their developmental progression within a clinical advancement program.
Methods: Using the Delphi technique, nursing leadership validated the newly identified competency domains and KSAs as essential to practice. Clinical experts from 13 Magnet-designated hospitals with clin-ical advancement programs then participated in Delphi rounds aimed at reaching consensus on the devel-opmental progression of the 186 KSAs through four levels of clinical advancement.
Results: Two Delphi rounds resulted in consensus by the expert participants. All eight competency do-mains were determined to be essential at all four levels of clinical practice. At the novice level of practice, the experts identified a greater number of KSAs in the domains of safety and patient- and family-centered care. At more advanced practice levels, the experts identified a greater number of KSAs in the domains of professionalism, teamwork, technology and informatics, and continuous quality improvement.
Conclusion: Incorporating the eight competency domains and the 186 KSAs into a framework for clinical advancement programs will likely result in more clearly defined role expectations; enhance accountability; and elevate and promote nursing practice, thereby improving clinical outcomes and quality of care. With their emphasis on quality and safety, the eight competency domains also offer a framework for enhancing position descriptions, performance evaluations, clinical recognition, initial and ongoing competency assess-ment programs, and orientation and residency programs.
Keywords: clinical advancement program, nursing competency, quality and safety, Quality and Safety Education for Nurses
used by hospitals in identifying and supporting their practice standards and care quality.14
Nursing clinical advancement programs support clinical practice, enhance professional development, recognize clinical expertise, and increase nurse satis-faction and retention; they constitute a hallmark of a professional nursing practice environment.15 Such programs are typically based on Benner’s theoreti-cal novice-to-expert framework.16, 17 They offer nurses a pathway for career advancement without leaving clinical practice by defining stages of competency that reflect the changing practice needs of nurses as they move along a developmental continuum. Mastery of skills at each level is determined by both educational preparation and experience.18 Research has demon-strated that higher levels of nurses’ education and ex-perience are positively correlated with both the quality of patient care provided and the resulting clinical out-comes.19, 20 This suggests that progressive mastery of nursing practice competencies is vital to meeting the complex care needs of patients and families.
As contemporary clinical practice evolves to meet increasingly complex health care needs, so must clinical advancement programs.21 Yet there has been limited
research validating the competencies and defined pro-ficiencies required at each stage in a clinical advance-ment program. In our study, a team of experts at an academic health system used the consensus process to arrive at eight competency domains and 186 related KSAs critical to professional nursing practice. We then sought to validate the results using Delphi methodol-ogy and to determine their developmental progression within a clinical advancement program.
BACKGROUNDIn 2013, the frontline staff and nursing leadership at a multiorganization academic health system recognized the need to revise its four-level clinical advancement program in order to better identify behaviors that re-ward clinical expertise and enhance patient outcomes. The chief nursing officer council, comprising the chief nursing officers from each of the system entities and select other nursing leaders, appointed a committee to update and revise the program, its nursing competen-cies, and the related KSAs. The committee was com-posed of nurses representing all of the nursing roles within the system, including the corporate director of professional development and innovation (one of us,
By Kathleen G. Burke, PhD, RN, CENP, FAAN, Tonya Johnson, DNP, RN, CCRN-K, NEA-BC, Christine Sites, MSN, RN, and Jane Barnsteiner, PhD, RN, FAAN

24 AJN ▼ May 2017 ▼ Vol. 117, No. 5 ajnonline.com
KGB), professional development specialists (including CS), clinical nursing directors (including TJ), nurse managers, clinical advancement committee chairs, shared governance chairs, clinical nurse educators, and clinical nurses. Consultation was obtained from a faculty representative of the affiliated School of Nurs-ing undergraduate nursing program and a faculty
expert in the QSEN initiative (JB). The group met over an 18-month period from June 2013 through December 2014 to identify the competency domains that would form the foundation for the updated clinical advancement program, as well as the KSAs needed.
METHODSLiterature review. The first step was to conduct a lit-erature review. Several databases, including Academic Search Complete (EBSCO), CINAHL, the Cochrane Database of Systematic Reviews, Google Scholar, the Joanna Briggs Institute Evidence-Based Practice Data-base, MEDLINE, Ovid, ProQuest Health and Medi-cal Complete, ProQuest Nursing and Allied Health Source, Web of Science Core Collection Science Cita-tion Index Expanded, and Thoreau (Walden Uni-versity), were searched to identify relevant literature published in English between 1993 and 2015. Search terms included clinical advancement, clinical ladder, competency, domains of nursing practice, healthcare competency, novice to expert, nursing, and practice. After eliminating duplicates and unrelated articles, we used 55 peer-reviewed articles, landmark reports, and white papers to identify competency domains and related KSAs.
Foundational to this work were the six compe-tencies identified in the IOM Health Professions Ed-ucation: A Bridge to Quality report8 and the QSEN project.9, 10 The literature review further yielded profes-sionalism and leadership as essential competencies to contemporary nursing practice.2, 22-26
Identification by consensus. Based on the litera-ture review, the committee identified eight compe-tency domains, with related KSAs, as essential to contemporary nursing practice: continuous quality improvement, evidence-based practice and research, leadership, patient- and family-centered care, profes-sionalism, safety, teamwork, and technology and in-formatics. See Table 1 for a list of these domains and their definitions. The eight competency domains and the related KSAs were then disseminated for feed-back from the health system’s shared governance councils, clinical advancement committees, nursing leadership, and competency domain content experts. The selected content experts were recognized au-thorities on the subject matter (the domain of safety was reviewed by a patient safety clinical nurse spe-cialist, for example). Once consensus on all the com-petency domains and KSAs was reached, the results were presented to and endorsed by the chief nursing officer council and the nursing shared government councils throughout the health system.
The committee then sought to validate the 186 KSAs along a four-level clinical advancement pro-gram using a Delphi technique.
Delphi study. The purpose of the Delphi study was to reach consensus on the essential KSAs and assign
Competency Domain Definition
Continuous quality improvement
Utilizes data and quality improvement methods to identify potential and actual problems and opportunities to provide care that is safe, timely, efficient, effective, and equitable
Evidence-based practice and research
Evaluates and integrates the best current evidence with clinical expertise and patient and family preferences and values for deliv-ery of optimal health care and system effec-tiveness
Leadership Effectively collaborates and applies innova-tive systems thinking to engage in systematic, evidence-based problem solving and deci-sion making to promote effective changes within a complex care delivery system, sup-porting the vision of the organization
Patient- and family- centered carea
Recognizes the patient (or the patient’s designee) as the source of control and full partner in providing compassionate and coordinated care based on respect for the patient’s preferences, values, and needs
Professionalism Demonstrates a commitment to the nursing profession through lifelong learning, adher-ence to the ANA’s Code of Ethics for Nurses, participation in a professional organization, and advancement of community outreach
Safety Minimizes the risk of harm to patients, families, providers, and self through system effectiveness and individual performance
Teamwork Effectively engages in the process of cooper-ation, coordination, and collaboration in an effort to provide safer, high-quality outcomes for patients within inter- and intraprofessional teams, including virtual teams
Technology and informatics
Utilizes appropriate information and tech-nology to communicate, manage knowl-edge, mitigate error, and support decision making across the continuum
Table 1. Competency Domains and Definitions
ANA = American Nurses Association.a ”Patient- and family-centered care” was later changed by our multiorganizational health sys-tem to “person- and family-centered care,” to reflect updated terminology.

[email protected] AJN ▼ May 2017 ▼ Vol. 117, No. 5 25
each to the appropriate level of the four-level clinical advancement program. The Delphi method is a struc-tured process that uses a series of questionnaires or “rounds” to gather information; rounds are contin-ued until group consensus is reached.27 We used Sur-veyMonkey software to disseminate each round. The technique involves presenting a questionnaire to a panel of informed experts in a specific field in order to seek their opinion or judgment. The recom-mended process includes maintaining anonymity among the panel members in order to help control for bias in their responses, and offering controlled feedback. We used a modified Delphi technique in this study, inviting the panel members to respond to information that was initially provided, rather than to open-ended questions.28 Although opinion varies among researchers on what constitutes the point of consensus when using a Delphi technique, consen-sus is generally defined as at least a 51% agreement among respondents on an expert panel.29 We used this definition. The study protocol was approved as exempt from full board review by the University of Pennsylvania’s institutional review board.
Magnet hospital program directors were contacted and asked to identify an expert in their organization to whom the survey should be sent. Experts invited to participate were from acute care health care organiza-tions that met all of the following criteria: the facility held Magnet designation, offered a nursing profes-sional clinical advancement program, and either was a member of the University HealthSystem Consor-tium (now known as Vizient) or was recognized as a top hospital by U.S. News and World Report in its 2014–15 honor roll. Twenty organizations met these criteria; the organization conducting the Delphi study also met all of the set criteria. Potential study partici-pants were invited to participate via e-mail and were given information on anonymity, risks, and benefits. A link to the SurveyMonkey questionnaire was em-bedded in the body of the e-mail. The survey link re-mained active for three weeks during each Delphi round. Consent was obtained through agreement to participate in the study.
Participants were asked to respond to three ques-tions, as follows: 1. At what level (CN I–IV) is a particular KSA of
a competency domain essential to professional practice?
2. Are any of the KSAs not essential?3. Would you add any additional KSAs to any of
the competencies?Clinical nurse (CN) practice levels were defined as follows: CN I, a new-to-practice RN with less than two years of experience; CN II, an RN with at least two years of experience whose area of impact lies pri-marily within a single clinical unit; CN III, an RN with more than three years of experience whose area of impact lies within a unit, department, or service
line, or a combination thereof; CN IV, an RN with more than four years of experience whose area of im-pact is realized throughout the health care organiza-tion and beyond.
Responses were collected in aggregate. Consensus was reached when a majority of respondents (51% or more) selected the same clinical level for a KSA. KSAs meeting consensus were then eliminated from the second Delphi round. KSAs not meeting consen-sus were moved to the second round. The panel ex-perts responded to the same three questions in the second round for the remaining KSAs. Consensus was reached on all KSAs after two rounds, and a third round was not needed.
RESULTSTwenty clinical experts representing the 20 organi-zations that met the study criteria were contacted; of these, 13 (65%) agreed to participate. Eleven partici-pants provided demographic information (see Table 2). Sample respondents included Magnet program di-rectors, directors of professional development, and nurses responsible for a clinical advancement pro-gram. Thirteen experts responded to round one and 10 responded to both rounds. After round one, agree-ment was reached for 60% of the KSA assignments along the four-level clinical advancement program. After round two, agreement was reached for 90% of the KSA assignments. For the remaining 10%, the ex-perts were evenly divided about assignment to one of two bordering clinical levels. Using their professional judgment, the QSEN consultant and the research team made the final determination in assigning each of the remaining 18 KSAs.
The experts’ survey responses indicated that the competencies and the KSAs were essential to and complete for all four levels of clinical practice. The experts did not recommend adding, modifying, or deleting any of the competency domains or KSAs. For the final assignment of the KSAs under the eight competency domains at the four levels of practice, see Table 3.
The highest number of KSAs were assigned to the domains of professionalism (31 or 16.7% of the total KSAs) and patient- and family-centered care (31 or 16.7% of the total). The domain of safety was assigned 26 KSAs or 14% of the total. The domains of leadership and teamwork were each assigned 22 KSAs or 11.8% of the total. The domain of technol-ogy and informatics was assigned 21 KSAs or 11.3% of the total; that of continuous quality improvement, 18 KSAs or 9.7% of the total; and that of evidence-based practice and research, 15 KSAs or 8.1% of the total. See Table 4 for the number of KSAs assigned to each competency domain.
In terms of practice levels, 84 (45.2%) of the KSAs were designated CN I, 47 (25.3%) were CN II, 46 (24.7%) were CN III, and nine (4.8%) were CN IV.

26 AJN ▼ May 2017 ▼ Vol. 117, No. 5 ajnonline.com
At the CN I level, the competency domains with the highest percentage of KSAs were patient- and family-centered care (20 KSAs or 23.8%), safety (17 KSAs or 20.2%), and professionalism (16 KSAs or 19%). At
the CN II level, the domain with the highest percent-age of KSAs was technology and informatics (10 KSAs or 21.3%). At the CN III level, the domains with the highest percentage of KSAs were professionalism and leadership (eight KSAs or 17.4% each). And at the CN IV level, the domains with the highest percentage of KSAs were continuous quality improvement and evidence-based practice and research (four KSAs or 44.4% each).
It’s important to note that, although the num-ber of KSAs decreases as one advances along the continuum—from 84 at CN I to nine at CN IV—one cannot reach the next level without first mas-tering the KSAs at the previous levels. Thus, a nurse at the CN IV level must have demonstrated mastery of the 84 CN I–level KSAs, the 47 CN II–level KSAs, and the 46 CN III–level KSAs, as well as the nine KSAs required at the CN IV level.
DISCUSSIONData analysis revealed several notable themes. First, the Delphi study results provided clear support for the application of the eight competency domains and the 186 KSAs in defining practice expectations in a competency-based, four-level clinical advancement program. These domains and accompanying KSAs reflect the wide variety of competencies that front-line nurses need when caring for patients and fami-lies in today’s complex health care environment. The results also reinforce the importance of including the KSAs as essential content in prelicensure programs, as the majority were identified as necessary for new nurses.
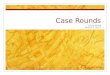
The identification of specific quality- and safety-related competencies reflects the strong link between nursing practice competencies and patient outcomes. For example, in the domain of continuous quality im-provement, frontline nurses participating in quality improvement initiatives may directly influence and help to reduce hospital-acquired infection rates, fall rates, and other nursing-sensitive quality indicators. And as Dolansky and Moore have noted, effective improvements in the quality and safety of care must involve applying nursing competencies not only to in-dividuals but also to systems,30 and this is supported by the experts’ assignments of KSAs across four prac-tice levels. For examples of the application of KSAs in the safety and continuous quality improvement domains over the four levels, see Figures 1 and 2, respectively.
Second, the panel experts identified the need for proficiency—in a large number of KSAs in all eight competency domains—at earlier levels of practice. A total of 70.4% (131) of the 186 KSAs were deemed essential at the CN I and CN II levels (84 KSAs at CN I and 47 KSAs at CN II). The fact that so many competencies were identified as required early in a clinical nurse’s career has important implications for
Characteristic n (%)
Current role in organization
Clinical nurse 1 (9)
Clinical nurse leader 4 (36)
Corporate director 1 (9)
Director 1 (9)
Director of nursing education 1 (9)
Nurse manager 2 (18)
Professional advancement coordinator 1 (9)
Length of time in current rolea
0–2 years 2 (18)
3–5 years 2 (18)
11–19 years 3 (27)
20+ years 4 (36)
Highest nursing degree obtained
Bachelor’s degree 1 (9)
Master’s degree 7 (64)
DNP 1 (9)
PhD 2 (18)
State where currently practicing (n = 10)b
California 1 (10)
Delaware 1 (10)
Georgia 1 (10)
Illinois 1 (10)
Maryland 3 (30)
North Carolina 1 (10)
Ohio 1 (10)
Pennsylvania 1 (10)
Organization type
Academic medical center 8 (73)
Multihospital system 3 (27)
Size in licensed beds
251–500 1 (9)
501–750 4 (36)
751+ 6 (55)
Table 2. Characteristics of Respondents (n = 11)
a There were no respondents with 6–10 years in current role.b One respondent did not answer this question.

[email protected] AJN ▼ May 2017 ▼ Vol. 117, No. 5 27
Com
pete
ncy:
Con
tinuo
us Q
ualit
y Im
prov
emen
tU
tiliz
es d
ata
and
QI m
etho
ds to
iden
tify
pote
ntia
l and
act
ual p
robl
ems a
nd o
ppor
tuni
ties t
o pr
ovid
e ca
re th
at is
safe
, tim
ely,
eff
icie
nt, e
ffec
tive,
and
equ
itabl
e
CN I
CN II
CN II
ICN
IV
• Re
cogn
izes
how
dat
a ar
e us
ed in
QI e
ffort
s•
Desc
ribes
the
use
of Q
I pro
cess
es•
Unde
rsta
nds h
ow u
nit q
ualit
y af
fect
s sys
tem
ef
fect
iven
ess
• Pa
rtic
ipat
es a
s a te
am m
embe
r on
a pe
rform
ance
im
prov
emen
t pro
ject
• Pa
rtic
ipat
es in
the
desig
n, re
view
, and
ev
alua
tion
of Q
I dat
a an
d in
itiat
ives
at t
he
unit
leve
l •
Inte
grat
es Q
I ini
tiativ
es in
to in
divi
dual
pl
ans o
f car
e•
Link
s ini
tiativ
es o
r pro
ject
s to
Penn
M
edic
ine’s
Qua
lity
Blue
prin
t Im
pera
tives
• Fo
cuse
s effo
rts t
o im
prov
e th
e qu
ality
of
heal
th c
are
• Id
entif
ies Q
I too
ls, m
etho
ds, a
nd m
inds
et
• Pa
rtic
ipat
es in
the
desig
n, re
view
, and
ev
alua
tion
of Q
I dat
a an
d in
itiat
ives
at t
he
depa
rtm
ent o
r ser
vice
-line
leve
l •
Inte
grat
es m
ultip
le so
urce
s of d
ata
(suc
h as
ND
NQ
I, HCA
HPS
, and
oth
ers)
in
initi
ativ
es to
impr
ove
outc
omes
• Le
ads a
nd h
elps
sust
ain
a Q
I pro
ject
with
in
a un
it•
Anal
yzes
QI d
ata
with
resp
ect t
o or
gani
zatio
nal g
oals
and
natio
nal
benc
hmar
ks, a
nd u
ses t
hese
dat
a to
in
form
and
sele
ct Q
I ini
tiativ
es•
Acce
sses
uni
t-spe
cific
dat
a an
d id
entif
ies
tren
ds to
impr
ove
outc
omes
• Ha
s mas
tery
of a
ll KS
As•
Part
icip
ates
in th
e de
sign,
revi
ew, a
nd
eval
uatio
n of
QI d
ata
and
initi
ativ
es a
t the
en
tity
or sy
stem
leve
l•
Cons
ider
s rol
e of
ext
erna
l sta
keho
lder
s in
QI i
nitia
tives
and
prio
ritie
s•
Men
tors
CN
II a
nd C
N II
I lev
el n
urse
s to
build
thei
r cap
abili
ty a
nd c
apac
ity fo
r QI
with
in n
ursin
g•
Lead
s and
hel
ps su
stai
n a
QI p
roje
ct w
ithin
a
depa
rtm
ent o
r ser
vice
line
Com
pete
ncy:
Evi
denc
e-Ba
sed
Prac
tice
and
Rese
arch
Eval
uate
s and
inte
grat
es th
e be
st cu
rren
t evi
denc
e w
ith cl
inic
al e
xper
tise
and
patie
nt a
nd fa
mily
pre
fere
nces
and
val
ues f
or d
eliv
ery
of o
ptim
al h
ealth
care
and
syst
em e
ffec
tiven
ess
CN I
CN II
CN II
ICN
IV
• El
icits
and
resp
ects
pat
ient
and
fam
ily v
alue
s whe
n co
nsid
erin
g EB
P de
cisio
ns
• Pa
rtic
ipat
es in
dat
a co
llect
ion,
rese
arch
, or b
oth
• Co
nsul
ts w
ith e
xper
ts w
hen
the
basis
for p
ract
ice
is
ques
tione
d
• Util
izes t
he E
BP p
roce
ss: g
ener
ates
clin
ical
qu
estio
ns, s
earc
hes a
nd e
valu
ates
the
qual
ity o
f evi
denc
e, co
nsid
ers e
xper
t clin
ical
kn
owle
dge
and
patie
nt p
refe
renc
es a
nd
valu
es, a
nd a
pplie
s thi
s to
prac
tice
• Q
uest
ions
cur
rent
pra
ctic
e an
d de
velo
ps
a se
nse
of c
linic
al in
quiry
• Lo
cate
s cur
rent
evi
denc
e an
d re
sour
ces
rela
ted
to c
linic
al p
ract
ice
• M
ento
rs st
aff,
acts
as a
role
mod
el, a
nd
acts
as a
reso
urce
rega
rdin
g us
e of
the
EBP
proc
ess
• Ev
alua
tes c
linic
al p
ract
ice
guid
elin
es•
Anal
yzes
the
appl
icab
ility
of r
esea
rch
findi
ngs t
o in
divi
dual
pat
ient
situ
atio
ns•
Eval
uate
s pol
icie
s to
ensu
re a
lignm
ent
with
cur
rent
pra
ctic
e an
d th
e be
st
avai
labl
e ev
iden
ce•
Eval
uate
s the
out
com
es o
f EBP
initi
ativ
es
• Ha
s mas
tery
of a
ll KS
As•
Men
tors
and
lead
s oth
ers
• Ta
kes a
lead
ersh
ip ro
le in
the
deve
lopm
ent
or im
plem
enta
tion
of re
sear
ch a
nd E
BP
proj
ects
• Se
eks o
ppor
tuni
ties t
o pr
esen
t evi
denc
e fin
ding
s at l
ocal
, sta
te, o
r nat
iona
l co
nfer
ence
s, or
thro
ugh
publ
icat
ion
in
peer
-rev
iew
ed jo
urna
ls•
Inte
rpre
ts re
sear
ch a
nd u
ses s
cien
tific
in
quiry
to v
alid
ate
or c
hang
e cl
inic
al
prac
tice
• Di
ssem
inat
es fi
ndin
gs
Tabl
e 3.
Del
phi S
tudy
Res
ults
Sho
win
g Pr
ogre
ssio
n of
KSA
s Alo
ng a
Fou
r-Lev
el C
linic
al A
dvan
cem
ent P
rogr
am
CN I,
a ne
w-to
-pra
ctic
e RN
with
less
than
two
year
s of e
xper
ienc
e; C
N II
, an
RN w
ith a
t lea
st tw
o ye
ars o
f exp
erie
nce
who
se a
rea
of im
pact
lies
prim
arily
with
in a
sing
le c
linic
al u
nit;
CN II
I, an
RN w
ith
mor
e th
an th
ree
year
s of e
xper
ienc
e w
hose
are
a of
impa
ct li
es w
ithin
a u
nit,
depa
rtm
ent,
or se
rvic
e lin
e, o
r a c
ombi
natio
n th
ereo
f; CN
IV, a
n RN
with
mor
e th
an fo
ur y
ears
of e
xper
ienc
e w
hose
are
a of
impa
ct is
real
ized
thro
ugho
ut th
e he
alth
car
e or
gani
zatio
n an
d be
yond
. N
ote:
Com
pete
ncie
s are
pro
gres
sive.
Ach
ieve
men
t of c
ompe
tenc
y at
a g
iven
leve
l req
uire
s com
pete
ncy
at p
revi
ous l
evel
s. Fo
r exa
mpl
e, C
N II
I com
pete
ncy
also
requ
ires c
ompe
tenc
y at
the
CN II
and
CN
I lev
els.

28 AJN ▼ May 2017 ▼ Vol. 117, No. 5 ajnonline.com
Com
pete
ncy:
Lea
ders
hip
Effe
ctiv
ely
colla
bora
tes a
nd a
pplie
s inn
ovat
ive
syst
ems t
hink
ing
to e
ngag
e in
syst
emat
ic, e
vide
nce-
base
d pr
oble
m so
lvin
g an
d de
cisi
on m
akin
g to
pro
mot
e ef
fect
ive
chan
ges w
ithin
a
com
plex
care
del
iver
y sy
stem
, sup
port
ing
the
visi
on o
f the
org
aniz
atio
n
CN I
CN II
CN II
ICN
IV
• De
lega
tes a
nd c
olla
bora
tes e
ffect
ivel
y to
mee
t pat
ient
ca
re n
eeds
• Li
sten
s obj
ectiv
ely
to a
ll sid
es o
f an
issue
bef
ore
mak
ing
a ju
dgm
ent
• De
mon
stra
tes e
ngag
emen
t in
unit
and
syst
em
initi
ativ
es•
Com
mun
icat
es th
ough
ts, f
eelin
gs, a
nd id
eas t
o ju
stify
a
posit
ion
• Em
ploy
s app
ropr
iate
soci
al sk
ills
• De
mon
stra
tes a
bilit
y to
lear
n on
the
fly•
Supe
rvise
s nur
sing
care
that
is p
rovi
ded
by o
ther
s and
fo
r whi
ch th
e nu
rse
is re
spon
sible
by
usin
g be
st
prac
tices
of m
anag
emen
t, le
ader
ship
, and
eva
luat
ion
• De
velo
ps c
onfli
ct re
solu
tion
skill
s for
self
and
team
m
embe
rs•
Initi
ates
act
ions
to re
solv
e co
nflic
t
• Co
mm
unic
ates
con
fiden
tly w
ith te
am
mem
bers
, ada
ptin
g on
e’s o
wn
styl
e of
co
mm
unic
atin
g to
mee
t the
nee
ds o
f the
te
am a
nd si
tuat
ion
• Id
entif
ies a
nd e
mbr
aces
the
need
for
chan
ge a
nd n
ew a
ppro
ache
s to
care
that
ar
e su
ppor
ted
by e
vide
nce
• De
mon
stra
tes t
he a
ppro
pria
te u
se a
nd
allo
catio
n of
reso
urce
s•
Esta
blish
es o
nese
lf as
a c
redi
ble
heal
th
care
pro
vide
r and
reso
urce
• Id
entif
ies d
iver
se v
iew
poin
ts a
nd m
anag
es
conf
lict
• De
velo
ps a
nd le
ads c
hang
e st
rate
gies
ba
sed
on sy
stem
initi
ativ
es a
nd c
urre
nt
evid
ence
• M
odel
s and
faci
litat
es e
ffect
ive
com
mun
i-ca
tion
amon
g pe
ers a
nd th
e in
trap
rofe
s-sio
nal t
eam
thro
ugh
the
use
of d
ebrie
fings
, pe
er fe
edba
ck, h
uddl
es, c
hain
s of c
omm
u-ni
catio
n an
d co
mm
and,
and
coa
chin
g•
Colla
bora
tes w
ith o
ther
s to
impr
ove
qual
-ity
and
clin
ical
effe
ctiv
enes
s by
enha
ncin
g ef
ficie
ncy,
optim
al re
sour
ce u
se, a
nd fi
scal
re
spon
sibili
ty•
Cont
ribut
es to
the
prof
essio
nal d
evel
op-
men
t of o
ther
s (fo
r exa
mpl
e, th
roug
h m
en-
torin
g, a
ctin
g as
a p
rece
ptor
, or s
ervi
ng a
s a
team
lead
er)
• Pa
rtic
ipat
es in
the
desig
n an
d im
plem
en-
tatio
n of
syst
ems t
hat s
uppo
rt e
ffect
ive
in-
trap
rofe
ssio
nal c
olla
bora
tion
• Co
nsid
ers t
he im
pact
of n
ursin
g de
cisio
ns
on h
ealth
car
e as
a w
hole
• Se
rves
as a
cha
nge
agen
t, as
sistin
g ot
hers
in
und
erst
andi
ng th
e im
port
ance
, ne
cess
ity, im
pact
, and
pro
cess
of c
hang
e•
Prom
otes
nur
sing
lead
ersh
ip a
s bot
h a
scie
nce
and
an a
rt
• Ha
s mas
tery
of a
ll KS
As•
Men
tors
and
lead
s oth
ers
Com
pete
ncy:
Pat
ient
- and
Fam
ily-C
ente
red
Care
Reco
gniz
es th
e pa
tient
(or t
he p
atie
nt’s
desi
gnee
) as t
he so
urce
of c
ontr
ol a
nd fu
ll pa
rtne
r in
prov
idin
g co
mpa
ssio
nate
and
coor
dina
ted
care
bas
ed o
n re
spec
t for
the
patie
nt’s
pref
eren
ces,
va
lues
, and
nee
ds
CN I
CN II
CN II
ICN
IV
• See
ks to
dev
elop
and
und
erst
and
effe
ctiv
e co
mm
unic
a-tio
n w
ith p
atie
nts a
nd fa
milie
s reg
ardi
ng th
e pl
an o
f car
e •
Enga
ges p
atie
nts a
nd fa
mili
es in
act
ive
part
ners
hips
to
pla
n an
d de
liver
car
e•
Com
plet
es co
mpr
ehen
sive
syst
emat
ic a
sses
smen
ts re
le-
vant
to th
e pr
actic
e se
tting
• In
tegr
ates
clin
ical
reas
onin
g an
d kn
owle
dge
as th
e fo
unda
tion
for d
ecisi
on m
akin
g
• M
anag
es m
ore
com
plex
pat
ient
car
e as
signm
ents
app
ropr
iate
to sk
ill
leve
l•
Part
icip
ates
in b
uild
ing
cons
ensu
s and
re
solv
ing
conf
lict i
n th
e co
ntex
t of p
atie
nt
care
• De
mon
stra
tes t
he a
bilit
y to
see
the
big
pict
ure
• M
ento
rs o
ther
s to
inco
rpor
ate
patie
nts
and
fam
ilies
in th
e de
velo
pmen
t of c
linic
al
care
pla
ns a
nd g
oals
•
Anal
yzes
and
inte
rpre
ts b
arrie
rs to
the
deliv
ery
of p
atie
nt- a
nd fa
mily
-cen
tere
d ca
re w
ithin
the
heal
th c
are
sett
ing,
and
de
velo
ps st
rate
gies
to re
solv
e iss
ues a
nd
impr
ove
outc
omes
for p
atie
nts
• Ha
s mas
tery
of a
ll KS
As•
Men
tors
and
lead
s oth
ers
Tabl
e 3.
Con
tinue
d

[email protected] AJN ▼ May 2017 ▼ Vol. 117, No. 5 29
• Id
entif
ies c
ultu
ral n
eeds
and
per
spec
tives
in th
e re
lief
of p
ain,
disc
omfo
rt, a
nd su
fferin
g•
Man
ages
pat
ient
car
e as
signm
ents
app
ropr
iate
to sk
ill
leve
l•
Inco
rpor
ates
cul
tura
l com
pete
nce,
div
ersit
y, an
d in
clu-
sion
prin
cipl
es in
to p
ract
ice
• Us
es e
thic
al, le
gal, a
nd re
gula
tory
prin
cipl
es in
the
prov
ision
of c
are
• Es
tabl
ishes
a th
erap
eutic
rela
tions
hip
with
the
patie
nt
and
fam
ily•
View
s eac
h pa
tient
as a
uni
que
pers
on•
Is aw
are
of a
nd is
abl
e to
loca
te a
ll ad
vanc
e ca
re p
lan-
ning
doc
umen
tatio
n, a
nd k
now
s who
the
desig
nate
d de
cisio
n m
aker
s are
in th
e ev
ent t
hat p
atie
nts c
anno
t sp
eak
for t
hem
selv
es•
Asse
sses
the
patie
nt’s
and
fam
ily’s
abili
ties a
nd re
adi-
ness
to le
arn,
and
ada
pts t
he te
achi
ng p
lan
acco
rdin
gly
• Cr
eate
s and
doc
umen
ts a
n in
divi
dual
pla
n of
car
e ba
sed
on th
e go
als o
f the
pat
ient
and
fam
ily•
Fost
ers a
hea
ling
envi
ronm
ent f
or p
atie
nts a
nd fa
mili
es• K
eeps
the
patie
nt a
nd fa
mily
at t
he ce
nter
of a
ll dec
ision
s•
Bala
nces
the
patie
nt’s
right
s and
the
orga
niza
tion’
s re-
spon
sibili
ties i
n pr
ovid
ing
prof
essio
nal a
nd e
thic
al
care
• Em
pow
ers t
he p
atie
nt a
nd fa
mily
to ta
ke a
n ac
tive
role
in
the
care
dev
elop
men
t pro
cess
• Est
ablis
hes a
ther
apeu
tic n
urse
–pat
ient
rela
tions
hip
• Su
ppor
ts a
cul
ture
that
val
ues d
iver
sity
and
prom
otes
in
clus
ion
• Pr
omot
es fa
mily
pre
senc
e an
d pa
rtic
ipat
ion
in c
are
in
acco
rdan
ce w
ith p
atie
nt p
refe
renc
es
• Us
es c
linic
al e
xper
ienc
e an
d hi
stor
ical
pa
tient
resp
onse
s as a
way
to d
evel
op a
nd
refin
e pr
actic
e•
Is ab
le to
spea
k to
the
patie
nt a
bout
ad
vanc
e ca
re p
lann
ing,
val
ues,
and
end-
of-li
fe c
are
befo
re th
e ne
ed fo
r an
acut
e de
cisio
n ar
ises
• Ev
alua
tes a
nd c
onsid
ers t
he im
plem
enta
-tio
n of
alte
rnat
ive
appr
oach
es to
est
ablis
h-in
g a
heal
ing
envi
ronm
ent
• En
gage
s in
prob
lem
solv
ing
to a
ddre
ss
com
plex
issu
es re
gard
ing
the
deliv
ery
of
safe
r, hi
gh-q
ualit
y pa
tient
- and
fam
ily-
cent
ered
car
e•
Ensu
res t
hat t
he sy
stem
s with
in th
e ar
ea o
f pr
actic
e su
ppor
t pat
ient
-cen
tere
d ca
re
• Di
ssem
inat
es in
form
atio
n ab
out o
utco
mes
as
a re
sult
of th
e us
e of
alte
rnat
ive
ther
apie
s in
the
heal
ing
envi
ronm
ent
Com
pete
ncy:
Pro
fess
iona
lism
Dem
onst
rate
s a co
mm
itmen
t to
the
nurs
ing
prof
essi
on th
roug
h lif
elon
g le
arni
ng, a
dher
ence
to th
e A
NA’
s Cod
e of
Eth
ics f
or N
urse
s, p
artic
ipat
ion
in a
pro
fess
iona
l org
aniz
atio
n, a
nd
adva
ncem
ent o
f com
mun
ity o
utre
ach
CN I
CN II
CN II
ICN
IV
• Se
eks t
o de
velo
p ef
fect
ive
com
mun
icat
ion
skill
s and
ac
tivel
y co
ntrib
utes
to a
hea
lthy
wor
k en
viro
nmen
t •
Adhe
res t
o th
e AN
A’s C
ode
of E
thic
s for
Nur
ses a
nd
prof
essio
nal n
ursin
g an
d or
gani
zatio
nal s
tand
ards
• De
mon
stra
tes w
illin
gnes
s to
lear
n an
d ac
tivel
y en
gage
in p
erso
nal p
rofe
ssio
nal g
row
th•
Activ
ely
seek
s and
acc
epts
con
stru
ctiv
e fe
edba
ck
thro
ugh
supe
rvisi
on a
nd p
eer r
evie
w•
Dem
onst
rate
s res
pons
ibili
ty fo
r con
tinue
d co
mpe
tenc
y in
nur
sing
prac
tice
and
deve
lops
insig
ht th
roug
h re
flect
ion,
self-
anal
ysis,
self-
care
, and
life
long
lear
ning
• Pr
omot
es id
entif
icat
ion
and
disc
ussio
n of
et
hica
l con
cern
s •
Prep
ares
for c
ertif
icat
ion
in a
spec
ialty
• Fo
ster
s and
supp
orts
the
deve
lopm
ent o
f ot
hers
thro
ugh
prec
eptin
g•
Iden
tifie
s opp
ortu
nitie
s for
impr
oved
pr
oces
ses r
elat
ed to
mor
al a
nd e
thic
al
dile
mm
as•
Prom
otes
the
ANA’
s Cod
e of
Eth
ics f
or
Nur
ses a
nd p
rofe
ssio
nal n
ursin
g an
d or
gani
zatio
nal s
tand
ards
• Ex
empl
ifies
the
abili
ty to
bui
ld co
nsen
sus
and
arriv
e at
a c
omm
on u
nder
stan
ding
th
roug
h ef
fect
ive
and
skill
ed co
mm
unic
a-tio
n •
Fost
ers a
nd su
ppor
ts th
e de
velo
pmen
t of
othe
rs th
roug
h ac
ting
as a
pre
cept
or a
nd
men
tors
hip
• Us
es re
sour
ces t
o en
gage
oth
ers i
n th
e pr
oces
s of m
oral
and
eth
ical
dec
ision
m
akin
g
• Ha
s mas
tery
of a
ll KS
As•
Men
tors
and
lead
s oth
ers

30 AJN ▼ May 2017 ▼ Vol. 117, No. 5 ajnonline.com
• Us
es a
ppro
pria
te c
hann
els o
f com
mun
icat
ion
to
voic
e co
ncer
ns a
nd id
entif
y so
lutio
ns (s
uch
as
shar
ed g
over
nanc
e)•
Artic
ulat
es th
e ap
plic
atio
n of
and
inte
grat
es h
igh
ethi
cal s
tand
ards
and
cor
e va
lues
into
eve
ryda
y w
ork
activ
ities
• Di
spla
ys so
und
mor
al a
nd e
thic
al c
hara
cter
and
ju
dgm
ent,
and
prom
otes
acc
ount
abili
ty•
Esta
blish
es a
nd fo
llow
s thr
ough
with
per
sona
l goa
ls
that
supp
ort u
nit,
orga
niza
tiona
l, and
Pen
n M
edic
ine
goal
s and
impe
rativ
es•
Supp
orts
dec
ision
s onc
e th
ey h
ave
been
mad
e an
d ag
reed
upo
n, a
nd a
djus
ts p
ract
ice
acco
rdin
gly
• Pa
rtic
ipat
es in
form
al a
nd in
form
al p
eer r
evie
w•
Valu
es re
com
men
datio
ns o
f pro
fess
iona
l nur
sing
orga
niza
tions
• Pa
rtic
ipat
es in
com
mun
ity o
utre
ach
• Ac
tivel
y co
ntrib
utes
to a
hea
lthy
wor
k en
viro
nmen
t (re
fer t
o th
e AA
CN S
tand
ards
for E
stab
lishi
ng a
nd
Sust
aini
ng H
ealth
y W
ork
Envi
ronm
ents
)•
Part
icip
ates
in sh
ared
dec
ision
mak
ing
and
shar
ed
gove
rnan
ce a
ctiv
ities
• Pa
rtic
ipat
es in
act
iviti
es th
at p
rom
ote
the
deve
lop-
men
t and
pra
ctic
e of
nur
sing
• Ac
tivel
y de
liver
s con
stru
ctiv
e fe
edba
ck to
pe
ers f
or th
e pu
rpos
e of
fost
erin
g de
vel-
opm
ent a
nd im
prov
ing
perfo
rman
ce•
Obt
ains
mem
bers
hip
and
part
icip
ates
in
prof
essio
nal o
rgan
izat
ions
• Us
es c
oach
ing
and
debr
iefin
g st
rate
gies
to
help
oth
ers l
earn
• Id
entif
ies t
he n
eeds
of t
he u
nit a
nd
orga
nize
s dev
elop
men
tal o
ppor
tuni
ties
• Pr
omot
es c
ertif
icat
ion
and
form
al
educ
atio
n in
oth
ers
• An
alyz
es a
nd in
terp
rets
bar
riers
to
effe
ctiv
e co
mm
unic
atio
n w
ithin
the
heal
th
care
sett
ing
and
deve
lops
stra
tegi
es to
im
prov
e ou
tcom
es•
Lead
s act
iviti
es th
at p
rom
ote
the
deve
lopm
ent a
nd p
ract
ice
of n
ursin
g
Com
pete
ncy:
Saf
ety
Min
imiz
es th
e ris
k of
har
m to
pat
ient
s, fa
mili
es, p
rovi
ders
, and
self
thro
ugh
syst
em e
ffec
tiven
ess a
nd in
divi
dual
per
form
ance
CN I
CN II
CN II
ICN
IV
• Re
cogn
izes
an
unsa
fe si
tuat
ion
• En
gage
s pat
ient
and
fam
ily in
par
tner
ship
to p
rom
ote
safe
ty•
Resp
onds
app
ropr
iate
ly to
uns
afe
situa
tions
and
to
patie
nt a
nd fa
mily
safe
ty c
once
rns
• In
tegr
ates
safe
ty p
rinci
ples
and
the
Join
t Co
mm
issio
n’s N
atio
nal P
atie
nt S
afet
y G
oals
into
ow
n pr
actic
e•
Uses
ava
ilabl
e re
sour
ces t
o pr
even
t inj
ury
• Re
cogn
izes
ow
n lim
itatio
ns a
nd se
eks a
ssist
ance
w
hen
indi
cate
d•
Prac
tices
with
in h
er o
r his
scop
e as
def
ined
by
the
stat
e bo
ard
of n
ursin
g an
d th
e AN
A’s N
ursi
ng: S
cope
an
d St
anda
rds o
f Pra
ctic
e, in
clud
ing
stan
dard
s for
safe
m
edic
atio
n ad
min
istra
tion
• Us
es o
rgan
izat
iona
l err
or re
port
ing
syst
ems f
or n
ear-
miss
and
err
or re
port
ing
• Se
rves
as a
reso
urce
per
son
for s
afet
y co
ncer
ns•
Dem
onst
rate
s ski
lls in
pro
blem
solv
ing,
co
nflic
t res
olut
ion,
and
neg
otia
tion
• Pa
rtic
ipat
es a
ppro
pria
tely
in a
naly
zing
er
rors
and
des
igni
ng sy
stem
im
prov
emen
ts
• De
signs
stra
tegi
es to
cre
ate
a cu
lture
of
safe
ty b
ased
on
best
pra
ctic
es a
nd
evid
ence
in th
e lit
erat
ure
• Co
ordi
nate
s com
plex
car
e ac
ross
di
scip
lines
and
pro
fess
ions
• Ch
ampi
ons t
echn
olog
ies t
hat s
uppo
rt
clin
ical
dec
ision
mak
ing
and
erro
r pr
even
tion
• Im
plem
ents
stra
tegi
es to
cre
ate
a cu
lture
of
safe
ty b
ased
on
best
pra
ctic
es a
nd
evid
ence
in th
e lit
erat
ure
• Us
es b
ench
mar
k da
ta to
iden
tify
gaps
in
safe
ty•
Men
tors
staf
f in
deve
lopi
ng, im
plem
ent-
ing,
and
eva
luat
ing
stra
tegi
es to
clo
se
gaps
in c
are
qual
ity a
nd sa
fety
• Ha
s mas
tery
of a
ll KS
As•
Men
tors
and
lead
s oth
ers
Tabl
e 3.
Con
tinue
d

[email protected] AJN ▼ May 2017 ▼ Vol. 117, No. 5 31
• De
lega
tes w
ork
appr
opria
tely
and
pro
vide
s dire
ctio
n an
d gu
idan
ce to
clin
ical
supp
ort p
erso
nnel
• Co
mm
unic
ates
con
cern
s rel
ated
to sa
fety
risk
s to
patie
nts,
fam
ilies
, and
the
heal
th c
are
team
• Ac
know
ledg
es a
nd d
iscus
ses r
isks a
ssoc
iate
d w
ith
tran
sitio
ns•
Activ
ely
part
icip
ates
in p
eer r
evie
w•
Is ab
le to
art
icul
ate
the
appr
opria
te d
ocum
enta
tion
of
unsa
fe e
vent
s and
pro
pose
solu
tions
to c
orre
ct fu
ture
oc
curr
ence
s•
Look
s for
an
unsa
fe si
tuat
ion
and
reac
ts a
ppro
pria
tely
• Pr
omot
es a
ctiv
e pa
tient
and
fam
ily e
ngag
emen
t in
care
• Us
es p
harm
acot
hera
py to
ens
ure
the
best
pos
sible
ou
tcom
es fo
r pat
ient
s•
Reco
gniz
es th
e be
nefit
s and
lim
itatio
ns o
f saf
ety-
enha
ncin
g te
chno
logi
es
Com
pete
ncy:
Team
wor
kEf
fect
ivel
y en
gage
s in
the
proc
ess o
f coo
pera
tion,
coor
dina
tion,
and
colla
bora
tion
in a
n ef
fort
to p
rovi
de sa
fer,
high
-qua
lity
outc
omes
for p
atie
nts w
ithin
inte
r- a
nd in
trap
rofe
ssio
nal
team
s, in
clud
ing
virt
ual t
eam
s
CN I
CN II
CN II
ICN
IV
• Pa
rtic
ipat
es a
s an
effe
ctiv
e te
am m
embe
r by
fost
erin
g op
en c
omm
unic
atio
n an
d sh
ared
dec
ision
mak
ing
• In
itiat
es re
ferr
als
• Re
cogn
izes
the
impa
ct o
f her
or h
is be
havi
or o
n ot
hers
• Em
brac
es th
e cu
ltura
l div
ersit
y an
d in
divi
dual
ity o
f he
alth
car
e te
am m
embe
rs•
Ackn
owle
dges
her
or h
is ow
n co
ntrib
utio
ns to
ef
fect
ive
and
inef
fect
ive
team
func
tioni
ng•
Uses
resp
ectfu
l lan
guag
e ap
prop
riate
for a
giv
en
diffi
cult
situa
tion,
a c
ruci
al c
onve
rsat
ion,
or a
n in
terp
rofe
ssio
nal c
onfli
ct•
Dem
onst
rate
s act
ive
enga
gem
ent i
n en
hanc
ing
patie
nt c
are
and
prom
otin
g a
posit
ive
wor
kpla
ce
envi
ronm
ent
• So
licits
inpu
t fro
m o
ther
team
mem
bers
to im
prov
e in
divi
dual
and
team
per
form
ance
• Co
ntin
uous
ly p
lans
for i
mpr
ovem
ent i
n ef
fect
ive
team
dev
elop
men
t •
Asse
rts h
er o
r his
posit
ion
or p
ersp
ectiv
e,
and
supp
orts
disc
ussio
ns a
bout
pat
ient
ca
re a
nd w
ork
envi
ronm
ent
• In
itiat
es p
lan
for s
elf-d
evel
opm
ent a
s a
team
mem
ber
• Ap
plie
s lea
ders
hip
skill
s tha
t sup
port
co
llabo
rativ
e pr
actic
e an
d te
am
effe
ctiv
enes
s•
Dem
onst
rate
s tea
m v
alue
s tha
t orie
nt
peop
le to
car
e ab
out p
erfo
rman
ce a
nd th
e su
cces
s of o
ther
s and
the
orga
niza
tion
• De
scrib
es th
e ro
les a
nd sc
opes
of p
ract
ice
of in
terp
rofe
ssio
nal t
eam
mem
bers
, as
wel
l as h
er o
r his
own
role
with
in th
e te
am
• Pe
rform
s effe
ctiv
ely
on in
terp
rofe
ssio
nal
team
s in
vario
us te
am ro
les a
nd se
ttin
gs
• M
ento
rs o
ther
s who
will
ass
ume
the
role
of
team
lead
er•
Crea
tes a
team
bas
ed o
n id
entif
ied
gaps
an
d ne
eds i
n pa
tient
car
e or
wor
kpla
ce
envi
ronm
ent
• An
alyz
es st
rate
gies
that
influ
ence
the
abil-
ity to
initi
ate
and
sust
ain
part
ners
hips
with
m
embe
rs o
f nur
sing
and
inte
rpro
fess
iona
l te
ams
• Cr
eate
s con
ditio
ns th
at p
rom
ote
crea
tive,
in
nova
tive,
and
pos
itive
pro
cess
out
com
es•
Eval
uate
s a te
am b
ased
on
prin
cipl
es o
f te
am d
ynam
ics a
nd id
entif
ied
gaps
and
ne
eds i
n pa
tient
car
e or
wor
kpla
ce
envi
ronm
ent
• Ap
prai
ses l
eade
rshi
p pr
actic
es th
at
supp
ort c
olla
bora
tive
prac
tice
and
team
ef
fect
iven
ess
• Ha
s mas
tery
of a
ll KS
As•
Men
tors
and
lead
s oth
ers
• Ef
fect
ivel
y le
ads i
nter
- or i
ntra
prof
essio
nal
team
s in
a va
riety
of s
ettin
gs

32 AJN ▼ May 2017 ▼ Vol. 117, No. 5 ajnonline.com
Com
pete
ncy:
Tech
nolo
gy a
nd In
form
atic
sU
tiliz
es a
ppro
pria
te in
form
atio
n an
d te
chno
logy
to co
mm
unic
ate,
man
age
know
ledg
e, m
itiga
te e
rror
, and
supp
ort d
ecis
ion
mak
ing
acro
ss th
e co
ntin
uum
CN I
CN II
CN II
ICN
IV
• De
mon
stra
tes t
he a
bilit
y to
use
clin
ical
syst
ems a
nd
tech
nolo
gy to
acc
ompl
ish a
spec
ific
task
•
Prot
ects
pat
ient
con
fiden
tialit
y•
Docu
men
ts a
nd p
lans
pat
ient
car
e in
an
EHR
• Co
nsist
ently
pro
vide
s acc
urat
e, ti
mel
y, an
d co
mpl
ete
docu
men
tatio
n in
the
EHR
• Co
nsist
ently
use
s the
EH
R to
com
mun
icat
e w
ith th
e ca
re te
am a
nd e
valu
ate
patie
nt n
eeds
• Id
entif
ies a
nd re
spon
ds a
ppro
pria
tely
to c
linic
al
deci
sion
supp
ort n
otifi
catio
ns a
nd a
lert
s•
Take
s par
t in
risk
eval
uatio
ns a
nd u
nder
stan
ds th
e le
gal i
mpl
icat
ions
of l
ate
or in
accu
rate
EH
R do
cum
enta
tion
• Se
rves
as a
reso
urce
for o
ther
nur
ses i
n ho
w to
doc
umen
t and
pla
n nu
rsin
g ca
re
usin
g te
chno
logy
•
Mod
els b
ehav
iors
that
supp
ort t
he
impl
emen
tatio
n an
d ap
prop
riate
use
of
clin
ical
syst
ems a
nd te
chno
logy
in
prov
idin
g sa
fe p
atie
nt c
are
• Pr
omot
es c
omm
unic
atio
n te
chno
logi
es
that
supp
ort c
linic
al d
ecisi
on m
akin
g, e
rror
pr
even
tion,
car
e co
ordi
natio
n, a
nd
prot
ectio
n of
pat
ient
priv
acy
• Se
arch
es, r
etrie
ves,
and
man
ages
dat
a ne
eded
to m
ake
deci
sions
, usin
g in
form
atio
n an
d kn
owle
dge
man
agem
ent
syst
ems
• Ev
alua
tes i
nfor
mat
ion
and
its so
urce
s cr
itica
lly, a
nd in
corp
orat
es se
lect
ed
info
rmat
ion
into
her
or h
is ow
n kn
owle
dge
base
and
val
ue sy
stem
• W
ith n
ursin
g co
lleag
ues,
acts
as a
ch
ampi
on fo
r cle
ar, c
onci
se, a
nd ti
mel
y do
cum
enta
tion
• An
ticip
ates
uni
nten
ded
cons
eque
nces
of
new
tech
nolo
gy a
nd re
spon
ds p
roac
tivel
y•
Unde
rsta
nds t
he p
rinci
ples
upo
n w
hich
or
gani
zatio
nal a
nd p
rofe
ssio
nal h
ealth
ca
re in
form
atio
n sy
stem
s are
bas
ed•
Inte
grat
es th
e us
e of
clin
ical
info
rmat
ion
syst
ems t
o co
ordi
nate
and
ant
icip
ate
care
ac
ross
the
cont
inuu
m•
Stay
s kno
wle
dgea
ble
abou
t tec
hnol
ogy
on th
e ho
rizon
• Se
rves
as a
n ex
pert
and
cha
mpi
on in
the
use
of te
chno
logi
es th
at su
ppor
t clin
ical
de
cisio
n m
akin
g, e
rror
pre
vent
ion,
and
pr
otec
tion
of p
atie
nt p
rivac
y•
Assis
ts o
ther
s in
retr
ievi
ng a
nd m
anag
ing
data
nee
ded
to m
ake
deci
sions
, usin
g in
form
atio
n an
d kn
owle
dge
man
agem
ent
syst
ems
• Ap
plie
s clin
ical
exp
ertis
e to
the
sele
ctio
n,
desig
n, im
plem
enta
tion,
and
eva
luat
ion
of
info
rmat
ion
syst
ems a
nd th
eir a
pplic
atio
n in
the
clin
ical
sett
ing
• Pa
rtic
ipat
es in
the
desig
n an
d on
goin
g op
timiz
atio
n of
the
EHR
to a
dapt
to th
e ch
angi
ng te
chno
logi
cal e
nviro
nmen
t of
the
inpa
tient
sett
ing
• Ha
s mas
tery
of a
ll KS
As•
Men
tors
and
lead
s oth
ers
Tabl
e 3.
Con
tinue
d
AAC
N =
Am
eric
an A
ssoc
iatio
n of
Crit
ical
-Car
e N
urse
s; A
NA
= A
mer
ican
Nur
ses
Asso
ciat
ion;
CN
= c
linic
al n
urse
; EBP
= e
vide
nce-
base
d pr
actic
e; E
HR
= el
ectr
onic
hea
lth re
cord
; HCA
HPS
= H
ospi
tal C
onsu
mer
Ass
essm
ent o
f H
ealth
care
Pro
vide
rs a
nd S
yste
ms;
KSAs
= k
now
ledg
e, s
kills
, and
att
itude
s; N
DN
QI =
Nat
iona
l Dat
abas
e of
Nur
sing
Qua
lity
Indi
cato
rs; Q
I = q
ualit
y im
prov
emen
t. “P
enn
Med
icin
e’s Q
ualit
y Bl
uepr
int I
mpe
rativ
es” i
s th
e U
nive
r-si
ty o
f Pen
nsyl
vani
a H
ealth
Sys
tem
’s qu
ality
str
ateg
ic p
lan.

[email protected] AJN ▼ May 2017 ▼ Vol. 117, No. 5 33
health care and academic settings as they strive to address the preparation-to-practice gap.31 The incor-poration of the competency domains and KSAs into prelicensure and residency program curricula, orien-tation programs, and preceptor programs will better prepare new nurses to deliver higher quality and safer
care, improve patient outcomes, and decrease errors. It may also help to reduce nurses’ stress and increase job retention.
Third, the largest number of KSAs were assigned to the competency domains of professionalism (31 or 16.7%), patient- and family-centered care (31 or
Competency Domain
Practice Level Total KSAs Per DomainCN I CN II CN III CN IV
Continuous quality improvement 4 5 5 4 18
Evidence-based practice and research 3 3 5 4 15
Leadership 9 5 8 0 22
Patient- and family-centered care 20 8 3 0 31
Professionalism 16 7 8 0 31
Safety 17 3 6 0 26
Teamwork 8 6 7 1 22
Technology and informatics 7 10 4 0 21
Total KSAs per practice level 84 47 46 9 186
Table 4. Delphi Study Results: Number of KSAs Assigned to Each Practice Level and Competency Domain
CN = clinical nurse; KSAs = knowledge, skills, and attitudes.
Leads implementation of and evaluates ID armband improvement strategy across service lines, departments, and health system as appropriate. Mentors other staff on how to sustain a culture of safety as it involves proper ID armband usage.
Responds to staff concerns regarding patient identification errors. Creates data collection sheet, analyzes and reviews patient safety data related to identification, and validates that such errors are an issue. Consults unit council and collaborates with other affected departments to design and implement an evidence-based improvement strategy.
Brings patient identification data to unit council meeting. Ensures that data have been entered into the hospital’s Safety Net database. Delegates to new nurses the appropriate follow-up steps. Notifies charge nurse, who informs admissions staff that patient was brought to room without armband.
Notices patient without an ID armband. Asks colleague where to get one and delegates obtaining it to unit clerk. Explains to patient and family why ID armband is important for patient safety. Uses two identifiers when applying the new ID armband. Seeks out preceptor for consultation on next steps.
Clinical Nurse I
Clinical Nurse II
Clinical Nurse III
Clinical L
adder
Clinical Nurse IV
Figure 1. Example in Practice—Safety: ID Armband

34 AJN ▼ May 2017 ▼ Vol. 117, No. 5 ajnonline.com
16.7%), and safety (26 or 14%). This underscores the essential role that nurses have, as practicing pro-fessionals, in engaging patients and families in the plan of care and in ensuring patient safety.
Practice implications. Clearly, the eight competency domains and 186 KSAs offer a useful overall frame-work for clinical advancement programs. They also provide an evidence-based foundation for how expec-tations about nursing practice can promote a culture of high-quality care and safety. For example, in our multiorganization health system, nurse recruiters are beginning to use the eight domains in structuring their behavioral interview questions in order to help identify nurses with competency in the necessary KSAs. The competency domains can further provide a framework for position descriptions and performance appraisals. Our organization is using the study findings to develop new clinical nurse position descriptions and a perfor-mance appraisal tool. A system-wide learning needs assessment, aimed at identifying nurses’ learning needs in each competency domain, was completed for all nurses, since many were educated before this con-tent was taught in prelicensure programs. The eight
domains can also provide a structure for initial and ongoing competency assessment programs, and can be used in designating KSAs for nurse residency, orien-tation, and preceptor programs.
Limitations. The competency domains were vali-dated with a convenience sample of nurse experts from similar organizations, rather than with practicing nurses at different levels from various types of orga-nizations. We specifically chose experts in clinical ad-vancement and professional development programs in like organizations because they have similar practice environments. Since practice is constantly evolving, additional competencies may be needed; the current list may not be exhaustive. Further research is also needed to examine the relationships between nurs-ing competencies and ongoing competency and per-formance evaluations of practicing clinical nurses, as well as patient outcomes.
CONCLUSIONThis study identified 186 KSAs required at each devel-opmental stage in a clinical advancement program for RNs, incorporating eight quality- and safety-related
OR = operating room; PACU = postanesthesia care unit; QI = quality improvement; SICU = surgical ICU.
Leads a system-wide QI project across all ORs, PACUs, and SICUs aimed at decreasing skin breakdown in patients who undergo long OR procedures. Mentors colleagues to work more effectively within a large interprofessional team to monitor and analyze QI data and to sustain evidence-based practices that reduce skin breakdown.
Reviews skin breakdown data on patients with long OR procedures who are transferred to the PACU and SICU. Collaborates with QI teams in designing a QI initiative aimed at standardizing practices across all PACUs and SICUs in order to increase use of new evidence-supported products that help reduce skin breakdown. Monitors and analyzes QI data and makes recommendations.
Partners with the quality department staff and participates in trial and evaluation of products designed to reduce skin breakdown during long OR procedures. Evaluates the resulting data and makes recommendations.
Knows how proper positioning and support surfaces help to prevent skin breakdown in surgical patients who transfer to the PACU and SICU. Understands the need for “time-outs” prior to surgeries or other procedures to decrease error rates. Integrates understanding of how patient positioning in the OR can result in subsequent skin breakdown and of the health system’s infection rates.
Clinical Nurse I
Clinical Nurse II
Clinical Nurse III
Clinic
al L
adde
r
Clinical Nurse IV
Figure 2. Example in Practice—Continuous Quality Improvement: Skin Breakdown in the OR

[email protected] AJN ▼ May 2017 ▼ Vol. 117, No. 5 35
competencies that are vital to meeting patient and family needs in today’s complex health care environ-ment. The findings may be used to inform position descriptions, hiring interview questions, performance appraisals, learning needs assessments, residency pro-grams, orientation programs, ongoing competency as-sessment programs, and preceptor programs. As such, they can help promote a culture of high-quality care and safety. ▼
Kathleen G. Burke is corporate director of nursing professional development and innovation at the University of Pennsylvania Health System (UPHS), assistant dean of clinical nurse learning and innovation at the University of Pennsylvania School of Nurs-ing, and senior fellow at the Leonard Davis Institute of Health Economics, University of Pennsylvania, all in Philadelphia. Tonya Johnson is associate chief nursing officer at Southcoast Health System, New Bedford, MA; at the time of this study, she was nursing clinical director at the UPHS’s Pennsylvania Hospital. Christine Sites is a nursing professional development specialist at the UPHS. Jane Barnsteiner is a professor emerita of pediatric nursing at the University of Pennsylvania School of Nursing, Philadelphia, and editor of translational research and quality im-provement at AJN. Contact author: Kathleen G. Burke, [email protected]. The authors and planners have disclosed no potential conflicts of interest, financial or otherwise.
REFERENCES1. Committee on Quality Health Care in America, Institute of
Medicine, editor. Crossing the quality chasm: a new health system for the 21st century. Washington, DC: National Academy Press; 2001. Quality chasm series. https://www.nap.edu/catalog/10027/crossing-the-quality-chasm-a-new-health-system-for-the.
2. Committee on the Robert Wood Johnson Foundation Initia-tive on the Future of Nursing, at the Institute of Medicine, ed-itor. The future of nursing: leading change, advancing health. Washington, DC: National Academies Press; 2011. https://www.nap.edu/catalog/12956/the-future-of-nursing-leading-change-advancing-health.
3. Interprofessional Education Collaborative. Core competen-cies for interprofessional collaborative practice: report of an expert panel. Washington, DC; 2011 May. http://www.aacn.nche.edu/education-resources/ipecreport.pdf.
4. Interprofessional Education Collaborative. Core competencies for interprofessional collaborative practice: 2016 update. Washington, DC; 2016. https://ipecollaborative.org/uploads/IPEC-2016- Updated-Core-Competencies-Report__final_release_.PDF.
5. Kohn LT, et al., editors. To err is human: building a safer health system. Washington, DC: National Academy Press; 2000. https://www.nap.edu/catalog/9728/to-err-is-human-building-a-safer-health-system.
6. Page AE, Committee on the Work Environment for Nurses and Patient Safety, Board on Health Care Services, editors. Keeping patients safe: transforming the work environment of nurses. Washington, DC: National Academies Press; 2004. https://www.nap.edu/catalog/10851/keeping-patients-safe-transforming-the-work-environment-of-nurses.
7. James JT. A new, evidence-based estimate of patient harms associated with hospital care. J Patient Saf 2013;9(3):122-8.
8. Greiner AC, et al., editors. Health professions education: a bridge to quality. Washington, DC: National Academies Press;
2003. Quality chasm series. https://www.nap.edu/catalog/ 10681/health-professions-education-a-bridge-to-quality.
9. Cronenwett L, et al. Quality and safety education for nurses. Nurs Outlook 2007;55(3):122-31.
10. Cronenwett L, et al. Quality and safety education for ad-vanced nursing practice. Nurs Outlook 2009;57(6):338-48.
11. Barnsteiner J, et al. Diffusing QSEN competencies across schools of nursing: the AACN/RWJF Faculty Development Institutes. J Prof Nurs 2013;29(2):68-74.
12. Didion J, et al. Academic/Clinical partnership and collabora-tion in Quality and Safety Education for Nurses education. J Prof Nurs 2013;29(2):88-94.
13. McKown T, et al. Using Quality and Safety Education for Nurses to guide clinical teaching on a new dedicated educa-tion unit. J Nurs Educ 2011;50(12):706-10.
14. Lyle-Edrosolo G, Waxman KT. Aligning healthcare safety and quality competencies: Quality and Safety Education for Nurses (QSEN), the Joint Commission and American Nurses Credentialing Center (ANCC) Magnet standards crosswalk. Nurse Lead 2016;14(1):70-5.
15. Knoche EL, Meucci JH. Competencies within a professional clinical ladder: differences in understanding between nurse managers and staff nurses. J Nurses Prof Dev 2015;31(2):91-9.
16. Benner P. From novice to expert. Am J Nurs 1982;82(3):402-7. 17. Benner PE. From novice to expert: excellence and power in
clinical nursing practice. Menlo Park, CA: Addison-Wesley Publishing Co., Nursing Division; 1984.
18. Benner PE. From novice to expert: excellence and power in clinical nursing practice. Commemorative ed. Upper Saddle River, NJ: Prentice-Hall; 2001.
19. Aiken LH, et al. The Magnet nursing services recognition program: a comparison of two groups of Magnet hospitals. J Nurs Adm 2009;39(7-8 Suppl):S5-S14.
20. Burket TL, et al. Clinical ladder program evolution: journey from novice to expert to enhancing outcomes. J Contin Educ Nurs 2010;41(8):369-74.
21. Bitanga ME, Austria M. Climbing the clinical ladder—one rung at a time. Nurs Manage 2013;44(5):23-7.
22. American Nurses Association. Nursing: scope and standards of practice. Silver Spring, MD; 2015.
23. American Nurses Credentialing Center. Magnet model. 2013. http://www.nursecredentialing.org/magnet/programoverview/new-magnet-model.
24. American Organization of Nurse Executives. AONE nurse executive competencies. Chicago; 2015. http://www.aone.org/resources/nec.pdf.
25. Sroczynski M, et al. Creativity and connections: the future of nursing education and practice: the Massachusetts Initiative. J Prof Nurs 2011;27(6):e64-e70.
26. Timmins F. Professional behaviour in healthcare professions: professionalism and self-presentation. Nurse Educ Pract 2013; 13:e8.
27. Hasson F, et al. Research guidelines for the Delphi survey tech-nique. J Adv Nurs 2000;32(4):1008-15.
28. Duffield C. The Delphi technique: a comparison of results ob-tained using two expert panels. Int J Nurs Stud 1993;30(3): 227-37.
29. Loughlin KG, Moore LF. Using Delphi to achieve congruent objectives and activities in a pediatrics department. J Med Educ 1979;54(2):101-6.
30. Dolansky MA, Moore SM. Quality and safety education for nurses (QSEN): the key is systems thinking. Online J Issues Nurs 2013;18(3). http://www.nursingworld.org/Quality-and-Safety-Education-for-Nurses.html.
31. Hickerson KA, et al. The preparation-practice gap: an integra-tive literature review. J Contin Educ Nurs 2016;47(1):17-23.
For 118 additional continuing nursing educa-tion activities on professional issues, go to www.nursingcenter.com/ce.