Embed Size (px)
Citation preview

Control of breathing by ECMO in ARDS
Tommaso Mauri
University of Milan – ItalyPlug working group – ESICM

I have nothing to disclose.
Within the last 12 months I have not had any type of financial arrangement or affiliation with commercial interests related to the
content of this continuing education activity that requires disclosure.
DISCLOSURE

Control of breathing in ARDS
63 yo, severe ARDS, ECMO day 13, SURVIVED

If ECMO is able to maintain normal PaCO2 and PaO2, then ventilation is no more needed
Nunn’s Applied Resp Phys 2010
Control of breathing during ECMO
ECMO

ECMO can replace ventilation
• Five anesthetized and paralyzed healthy lambs
• NO ventilation (PEEP 5) + AV ECMO for 24 hours
Kolobow T et al. J Thor Cardiovasc Surg 1978

ECMO and spontaneous ventilation?
Seven healthy lambs
Awake, spont. breathing
AV ECMO
Increasing gas flow to increase VCO2 ML

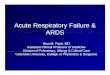
Control of ventilation by ECMO
Linear decrease of minute ventilation at increased VCO2-ML
At 90-100% of VCO2
removed, ventilation decreased to 5-20% of the baseline (no ECMO)
Kolobow T et al. Anesthesiology 1977

ECMO VCO2 / total VCO2
0 20 40 60 80 100
Red
uctio
nin
Min
ute
Ve
ntila
tio
n
[% o
f C
ontr
ol]
0
20
40
60
80
100r
2=0.74
p<0.001slope=0.94y0= -3.6
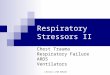
Langer T Crit Care Med 2014
Control of breathing by ECMO
Healthy non-sedated spontaneously breathing sheep.
vvECMO.
Linear reduction of minute ventilation down to <20%.

ECMO-induced apnea in healthy lungs
Canet E, J Appl Physiol 1993
ECMO-induced apnea at different levels of hypoxemia
Apnea thresholds: PaCO2 has to be lower to induce apnea in the presence of hypoxemia

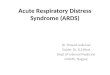
Physiologic control of breathing
Vaporidi K. et al. Am J Respir Crit Care Med 2019
Minute ventilation is the intersection between the:metabolic hyperbola and the PaCO2-MVe curve
Sleep

Min
ute
ven
tila
tio
n
PaCO2
GF low
GF intermediate
GF high
ECMO shifts the metabolic hyperbola
ECMO can control minute ventilation by shifting down the metabolic hyperbola through decreased VCO2 of the pt
↓VCO2-ECMO↑ VCO2-NL
↑VCO2-ECMO↓ VCO2-NL

Interim conclusions
Experimental studies show that in healthy animals increased elimination of CO2 by ECMO can decrease minute ventilation down to apnea
But..
Is ARDS equal to health?
= ???

Respiratory drive in ARDS
First difference:
In ARDS, respiratory drive is increased by multiple derangements of physiology that determine exaggerated response to changes in PaCO2
Even in the presence of low PaCO2 values, drive might remain elevated
Spinelli E. et al. Respiratory drive in the acute respiratory distress syndrome: pathophysiology, monitoring and clinical targets. Submitted.
IN ARDS

Second difference: in ARDS, the PaCO2-MVe curve separates from the central brain curve because of sedation, diaphragm weakness and increased lung elastance
Even in the presence of increased drive, minute ventilation could remain low
Vaporidi K. et al. Am J Respir Crit Care Med 2019
Minute ventilation in ARDS

On the one hand, control of minute ventilation could be ineffective because of increased drive
????????????????
On the other, control could be effective because ventilation is far lower than the level desired by brain centers
ECMO and control of breathing in ARDS

Control of breathing during recovery from ARDS
Marcolin R Trans Am Soc Artif Inter Organs 1986
Six patients recovering from severe ARF, ECMO could reduce minute ventilation to almost zero
Mean 0.22 36

Modifying VCO2 by ECMO
Mauri T et al. Anesthesiology 2016
Resting GF GF 050% 25%
VCO2 NL
4.4±1.2 l/min
ECMO can modulate patient’s VCO2 by changing the VCO2 of the membrane lung
Eight patients recovering from severe ARDS, enrolled after the clinical team switched them to PSV

Decreasing ECMO support during PSV and NAVA
Mauri T Anesthesiology 2016

Control of respiratory drive and effort
At resting, 100% GF:
Two patients with Eadi 10-15
One pt with P0.1 >2
No pts with RR >30Two pts with RR >20
One pt with Pmus >10
Mauri T Anesthesiology 2016

Control of transpulmonary pressure
Mauri T Anesthesiology 2016

0 20 40 60 80 100
0
20
40
60
80
100r
2=0.59
p<0.001
slope=1.1
y0= -24.0
Reduction in M
inute
Ventila
tion
[% o
f C
ontr
ol]
ECMO VCO2 / total VCO2
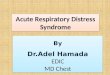
Langer T Crit Care Med 2014
Control of breathing in early severe ARDS
Early severe ARDS in non-sedated spontaneously breathing sheep
VCO2 almost completely removed by ECMO but small reduction of spont MV

Control of spontaneous breathing in early severe ARDS – clinical series 1
• 6 severe ARDS pts treated by awake ECMO to avoid intubation
• 50% successfully treated to recovery without intubation
• Reasons for intubation: PNX, accidental removal of ECMO and CA, exhaustion. Two (66%) died after intubation.
Hoeper et al. Int Care Med 2013

30 consecutive ARDS pts on controlled ventilation and ECMO
Stop sedation and paralysis within 5-7 days form ECMO start
Extubated if:
• RASS -1 to +1
• Adequate airway protection
• Able to cough
• Fever controlled
• No alveolar plasma leak
• Hemodynamic stability
• No major bleeding
Crotti et al. Anesthesiology 2017
Control of spontaneous breathing in early severe ARDS – clinical series 2

Awake ECMO in Milan: 50% success
Crotti et al. Anesthesiology 2017
ARDS SB-ECMO
re-intubated4/8 (50%)

Crotti et al. Anesthesiology 2017
Characteristics of ARDS that allow SB
Factors associated with impossibility to perform a spontaneous breathing test: p/f, days of ventilation, SOFA, lung weight.

Mauri T Int Care Med 2016
Sometimes, ECMO can’t control ventilation
ECMO day 7, Crs 15 ml/cmH2O, lack of control of respiratory drive by ECMO
What are the risk factors correlated with poor control of respiratory drive?

Control of breathing in early ARDS
15 subjects with severe ARDS on ECMO since 1-7 days
Sedation decreased to obtain RASS -2 to 0, presence of inspiratory trigger, PSV 5-10 cmH2O, clinical PEEP (15 [12-18] cmH2O)
PaCO2, pH and PaO2 within physiologic ranges
ECMO GF increased to obtain VCO2-ECMO/tot >90%:
• Apnea in 3 subjects
• Normal breathing pattern in 6 (RSBI ≤105 bpm/l)
• Rapid shallow breathing in 6 (RSBI >105 bpm/l)
Spinelli E. et al. Spontaneous breathing patterns during maximal extra-corporeal CO2 removal in subjects with early severe ARDS. Respir Care, in press

Worse control correlates with severity and outcome?
Hospital mortality within the study population was 0/3 vs. 0/6 vs. 3/6 (apnea vs. RSBI ≤105 bpm/l vs. RSBI >105 bpm/l; p = 0.169)
Spinelli E. et al. Spontaneous breathing patterns during maximal extra-corporeal CO2 removal in subjects with early severe ARDS. Respir Care, in press

Conclusions
• In healthy animals and in patients recovering from severe ARDS, ECMO can control spontaneousbreathing
• In early severe ARDS large variability exists and ECMO can’t control breathing in a subgroup of patients
• These might be the most severe one