Embed Size (px)
Citation preview

Control of fungal biofilm formation in dental environment
W. Mazari1, I. A. El Haci2 and Z. Boucherit Otmani1 1 Department of Biology, University Abou Bekr Belkaid, Tlemcen, Algeria 2 Scientific and Technical Research Center in Physico-Chemical Analysis CRAPC, BP 384, Industrial zone of Bou-Ismail,
RP 42004, Tipaza, Algeria
Nosocomial infections or care related infections are spreading more and more in clinical settings. These infections represent an additional financial burden for our health system but, unfortunately, these infections are not limited to hospitals and the risk is spreading even in dental offices. The area of dental care deserves special attention given the character of most surgical procedures and the use of many complex and reusable instruments in a naturally-septic environment. In addition, the specificity of the dental materials, the dental unit and the design of dental instruments promote the multiplication and growth of microorganisms inside the water circuits and instruments used, consequently; the formation of a biofilm. One of the determining characteristics of biofilm is resistance or tolerance to the antimicrobials used. This phenomenon is multifactorial and complex.
In dentistry, methods of disinfection are not always well known or are used insufficiently by practitioners, which make it difficult to eradicate biofilms. Control of the spread of care related infections in the hospital or dental environment is achieved by new evolving techniques. However, identification of the germ responsible for infection is the first act performed by the diagnostic laboratory. Nevertheless, conventional systems of identification have limitations, which need to the development of new rapid detection methods to meet the needs of public health. The present identification no longer includes the comparison of morphological and biochemical properties, it is based on the global identification of the ribosomal proteins and the sequencing of the DNA.
Keyword: fungal biofilm, dental unit waterlines, Maldi-tof, PCR, resistance/tolerance.
Introduction
The human oral flora consists of more than 700 different species. It represents the typical example of a diverse and mixed microbial flora colonizing the body. This particularity of the oral cavity provides the dental care area with special attention given the conditions of the working environment, the quality of surgical procedures and the use of many complex and reusable instruments in a naturally septic environment [1]. The activity of dentistry involves risks of direct or cross-contamination; the dental unit care to the patient, the patient to the patient, the patient to the practitioner or instrumentation to the assistant. The infections transmitted in the dental environment are underestimated because of the difficulty to highlight them [2]. According to the European Directives, the dental unit is a complex medical device designed to provide the necessary equipment for a wide variety of dental procedures. It brings together most of the tools needed to achieve care [3].
The yeasts and the oral health
According to the World Health Organization, 60% of nosocomial infections are due to the use of medical implants [4]. These medical implants serve as a support for the adhesion of microorganisms and the formation of biofilms, which is a permanent source of microorganisms that escape the immune defenses of humans and antimicrobial treatments. Yeasts are considered to be the main pathogens responsible for health-related infections, particularly, in immunocompromised patients [5]. As a result, fungal infections are the fourth most common health-care-associated infection with poor prognosis due to therapeutic difficulties, diagnosis and fragility of the terrain on which they occur [6]. The genus Candida sp is the most frequently isolated human fungal pathogen and is involved in many fungal infections [7]. Yeasts live in rather free structured microbial communities: planktonic cells. These dynamic microbial communities are called biofilms: sessile cells, in which transitions between planktonic and sessile growth patterns occur in response to different environmental selections. In a dental environment, the sessile lifestyle is predominant in aqueous media such as the mouth. Among the alterations due to the formation of biofilms in the buccal cavity, plaque and tartar are the example. By definition, tartar is a hardening of the dental plaque. This one is the accumulation of food residues, bacteria, etc. It forms a whitish layer that deposits on the teeth and forms the dental plaque in case it is not quickly eliminated [8]. Tartar provides a more fertile soil for the development of commensal or pathogenic yeasts. It has a persistent source of oral infections.
Antimicrobial research: Novel bioknowledge and educational programs (A. Méndez-Vilas, Ed.)
315
_____________________________________________________________________________

On the other hand, dental care is the main activity of the dentist. This dental care contains a risk of contamination for the patient, the dentist and, even, the assistant. The specificity of dental instruments lies in the complexity of their structure and in the environment in which they operate. The oral cavity is a naturally septic environment. The use of dynamic dental instruments, particularly, rotating hand pieces (in the absence of anti-reflux valves) allows the return of biological fluids, such as blood and saliva, within these environments. This fact facilitates the passage of yeasts into the water pipes of the dental units. These dental water pipes are characterized by a small diameter that allows stagnation of water, a temperature suitable for microbial growth and moisture. All this, promotes the adhesion, multiplication and formation of fungal biofilms on the internal walls of these dental water pipes. Therefore, the risk of catching an infection is possible [9, 10].
Dental care associated to fungal infections
According to the health and social services agency of Montérégie Québec, nosocomial infections are infections acquired during the delivery of care, wherever they are administered. These infections are now a major concern at the health facility level. They are responsible for high morbidity and mortality and a high socio-economic cost [11]. Yeasts are increasingly involved in these prolonged intensive care conditions or in populations at risk, which is a serious problem in the medical field [6]. The incidence of fungal infections related to care has increased, significantly, in recent years [12]. The prognosis of these infections is very poor because of the therapeutic difficulties, the diagnosis and the fragility of the patients [6]. Indeed, taking control and evaluation measures of fungal infections are essential for a good understanding of care related infections. However, the risk of transmission of infectious agents in health care is not limited to hospitals, this risk also exists in private medical practices and dental offices, although it’s quantitative importance is difficult to assess. The dental environment deserves particular consideration and attention given the invasiveness of most surgical procedures and the use of many complex and reusable instruments in a naturally septic environment [1, 13]. The oral cavity ecosystem consists of a mixed and complex microbial flora that is distributed among bacteria, yeasts and fungi [14] (Table 1). Control of fungal infections is of utmost priority given the natural environment of yeast in the mouth and the favorable conditions of fungal growth such as humidity and temperature. There is a much greater risk for immunosuppressed patients whose oral flora is altered. In the case of poor dental hygiene, the microbial population is multiplied, making dental care a risk for the patient and the healthcare team.
Biofilms in dental environment
1. What is a biofilm?
Biofilm is a living, dynamic microbial community attached to an inert or living surface maintained by secretion of an adhesive and protective matrix. This form constitutes the majority mode of life of microorganisms as opposed to the free mode which are the planktonic cells [18]. Biofilms have the ability to form on biotic or inert surfaces. In dentistry, the main focus of microorganisms is the dental unit. The latter is equipped with complex networks of narrow tubes of a narrow light of about 2 mm in diameter, made of polyurethane or polyvinyl chloride, which provide water for operating or cooling dental instruments [9] (Figure 1). These dental water pipes provide an ideal environment for the growth of microorganisms. Long periods of water stagnation, ambient temperature, small tubing diameter and water flow, all this favor the development of biofilms inside dental tubing. The main problem of the dental units seems to be the direct or cross contamination of the patients or the dental staff. To better understand this phenomenon, many studies have focused on the sources of contamination of dental water pipes. The water network and cross contamination are the main sources studied. The risk of this contamination depends on the nature and origin of the microorganisms involved, either from the water network, from the environment or from the human being. According to Mazari et al. [17], Candida species, in particular Candida guilliermondii, Candida albicans and Candida glabrata are recovered from the water tubes of the dental units. These isolated strains are of human origin and form part of the normal fungal flora of the human skin and buccal cavity. In addition, [19, 9] were able to recover human oral microorganisms from dental water lines such as Pseudomonas aeruginosa, Legionella, and non-tuberculosis mycobacteria.
Antimicrobial research: Novel bioknowledge and educational programs (A. Méndez-Vilas, Ed.)
316
_____________________________________________________________________________
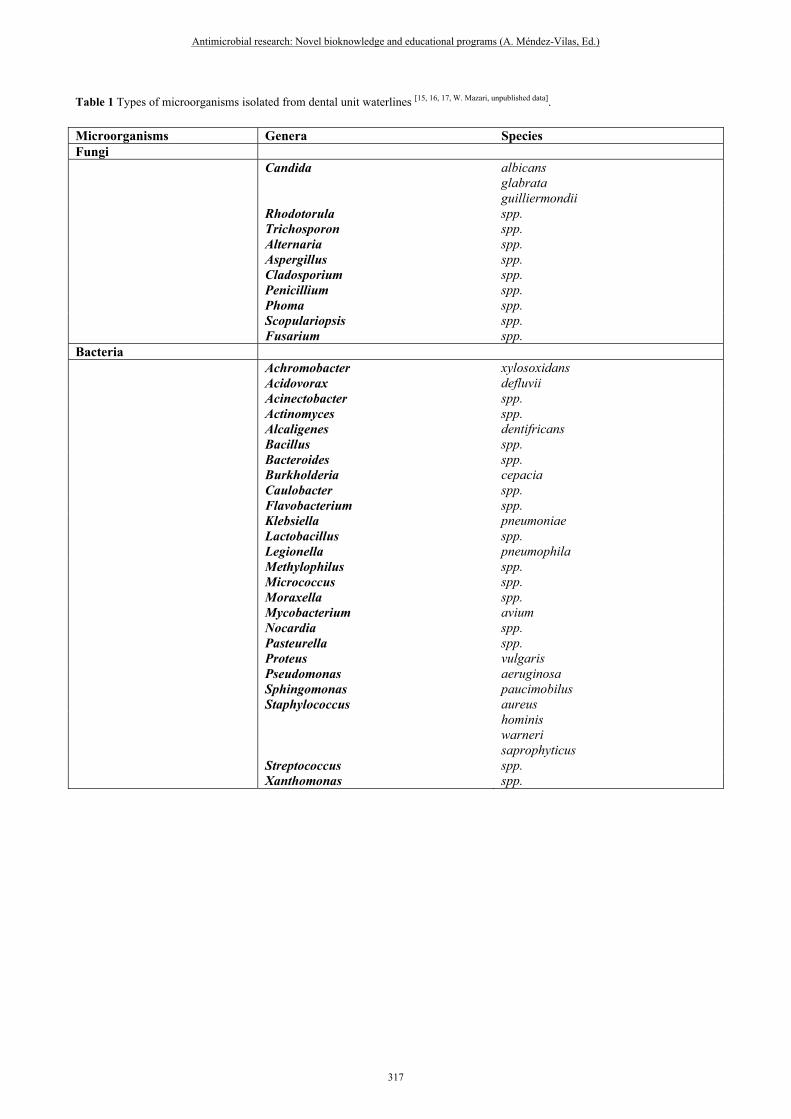
Table 1 Types of microorganisms isolated from dental unit waterlines [15, 16, 17, W. Mazari, unpublished data].
Microorganisms Genera Species Fungi Candida albicans glabrata guilliermondii Rhodotorula spp. Trichosporon spp. Alternaria spp. Aspergillus spp. Cladosporium spp. Penicillium spp. Phoma spp. Scopulariopsis spp. Fusarium spp. Bacteria Achromobacter xylosoxidans Acidovorax defluvii Acinectobacter spp. Actinomyces spp. Alcaligenes dentifricans Bacillus spp. Bacteroides spp. Burkholderia cepacia Caulobacter spp. Flavobacterium spp. Klebsiella pneumoniae Lactobacillus spp. Legionella pneumophila Methylophilus spp. Micrococcus spp. Moraxella spp. Mycobacterium avium Nocardia spp. Pasteurella spp. Proteus vulgaris Pseudomonas aeruginosa Sphingomonas paucimobilus Staphylococcus aureus hominis warneri saprophyticus Streptococcus spp. Xanthomonas spp.
Antimicrobial research: Novel bioknowledge and educational programs (A. Méndez-Vilas, Ed.)
317
_____________________________________________________________________________
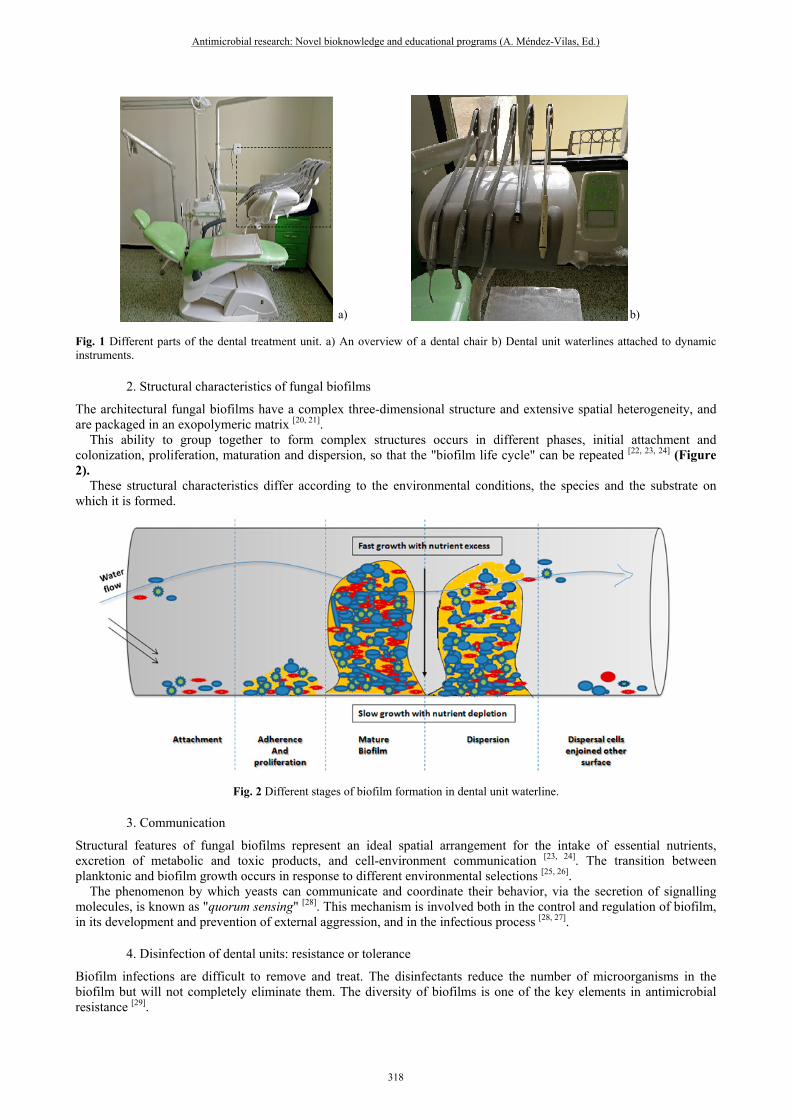
Fig. 1 Different parts of the dental treatment unit. a) An overview of a dental chair b) Dental unit waterlines attached to dynamic instruments.
2. Structural characteristics of fungal biofilms
The architectural fungal biofilms have a complex three-dimensional structure and extensive spatial heterogeneity, and are packaged in an exopolymeric matrix [20, 21]. This ability to group together to form complex structures occurs in different phases, initial attachment and colonization, proliferation, maturation and dispersion, so that the "biofilm life cycle" can be repeated [22, 23, 24] (Figure 2). These structural characteristics differ according to the environmental conditions, the species and the substrate on which it is formed.
Fig. 2 Different stages of biofilm formation in dental unit waterline.
3. Communication
Structural features of fungal biofilms represent an ideal spatial arrangement for the intake of essential nutrients, excretion of metabolic and toxic products, and cell-environment communication [23, 24]. The transition between planktonic and biofilm growth occurs in response to different environmental selections [25, 26]. The phenomenon by which yeasts can communicate and coordinate their behavior, via the secretion of signalling molecules, is known as "quorum sensing" [28]. This mechanism is involved both in the control and regulation of biofilm, in its development and prevention of external aggression, and in the infectious process [28, 27].
4. Disinfection of dental units: resistance or tolerance
Biofilm infections are difficult to remove and treat. The disinfectants reduce the number of microorganisms in the biofilm but will not completely eliminate them. The diversity of biofilms is one of the key elements in antimicrobial resistance [29].
a) b)
Antimicrobial research: Novel bioknowledge and educational programs (A. Méndez-Vilas, Ed.)
318
_____________________________________________________________________________
In dentistry, the control of biofilms in dental surgery systems deserves special attention by studying biofilm control methods for oral health. Despite the development of different physical and chemical methods of prevention and decontamination of dental units, it appears that these methods are not always effective. Moreover, the unregulated use of disinfectants in the disinfection of water lines constitutes a chemical risk for the patient and for the dental team. Several studies focus on the development and improvement of biofilm eradication methods in dentistry, from the simplest method (tubing purging) to chemical disinfection (use of biocides) [3, 30]. Biofilm eradication is difficult because of the resistance / tolerance of biofilm cells to the available disinfectants and antimicrobial molecules [31, 32]. Tolerance is the ability of an organism to survive in the presence of an antimicrobial at growth inhibiting concentrations. It is a non-hereditary phenotype associated with biofilm lifestyle. That is when the adherent yeasts detached, they regain their sensitivity again. On the other hand, the resistance of the biofilm is related to its planktonic form [33, 32]. However, several factors are related to the resistance of the biofilm cells; the secretion of exo-polysaccharides which protect them against the action of antimicrobial agents [34]; the density of cells in the biofilm, a simple concept of "safety in numbers" [31]; the existence of "persistent" cells that are highly tolerant to anti-infectious treatments [35, 36]; differences in the metabolic and physiological status of biofilm cells [37]; the composition of the membranes of the sessile cells with respect to their planktonic counterparts, the sterols [38] and the regulation of efflux pumps, which occur physiologically during formation and the development of biofilm to facilitate the elimination of toxic products [38, 39].
Risk of nosocomial transmission in dental environment
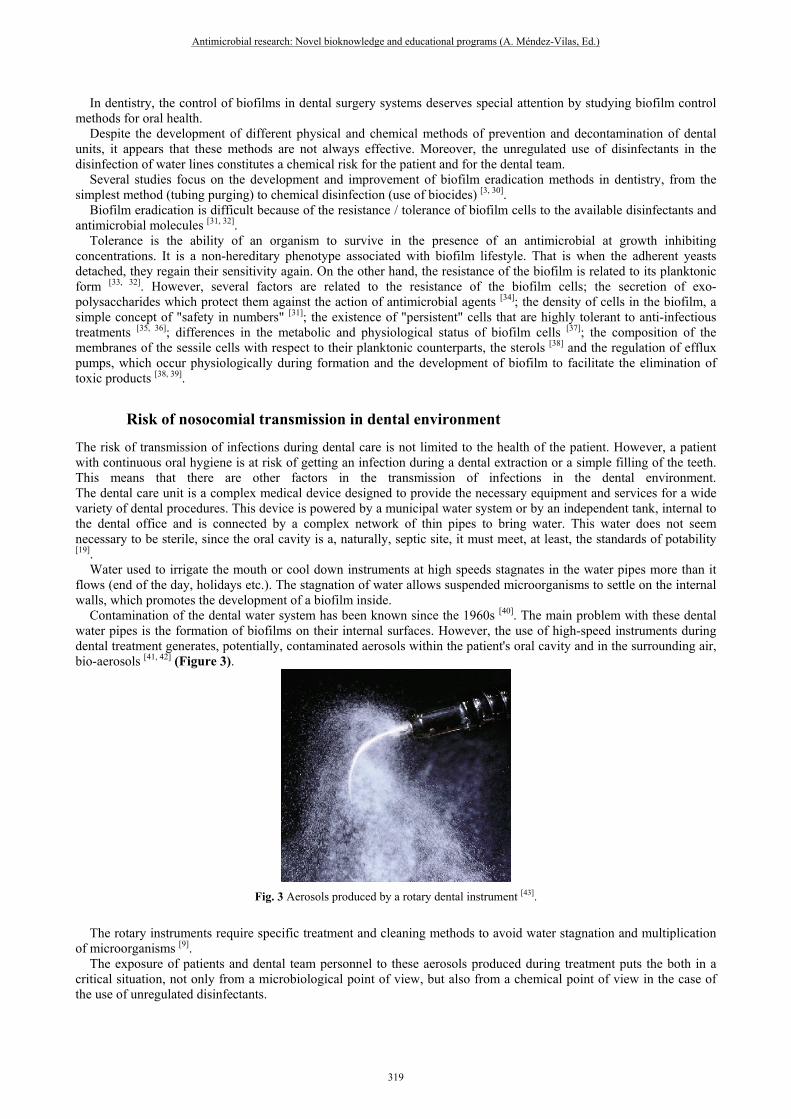
The risk of transmission of infections during dental care is not limited to the health of the patient. However, a patient with continuous oral hygiene is at risk of getting an infection during a dental extraction or a simple filling of the teeth. This means that there are other factors in the transmission of infections in the dental environment. The dental care unit is a complex medical device designed to provide the necessary equipment and services for a wide variety of dental procedures. This device is powered by a municipal water system or by an independent tank, internal to the dental office and is connected by a complex network of thin pipes to bring water. This water does not seem necessary to be sterile, since the oral cavity is a, naturally, septic site, it must meet, at least, the standards of potability [19]. Water used to irrigate the mouth or cool down instruments at high speeds stagnates in the water pipes more than it flows (end of the day, holidays etc.). The stagnation of water allows suspended microorganisms to settle on the internal walls, which promotes the development of a biofilm inside. Contamination of the dental water system has been known since the 1960s [40]. The main problem with these dental water pipes is the formation of biofilms on their internal surfaces. However, the use of high-speed instruments during dental treatment generates, potentially, contaminated aerosols within the patient's oral cavity and in the surrounding air, bio-aerosols [41, 42] (Figure 3).
Fig. 3 Aerosols produced by a rotary dental instrument [43].
The rotary instruments require specific treatment and cleaning methods to avoid water stagnation and multiplication of microorganisms [9]. The exposure of patients and dental team personnel to these aerosols produced during treatment puts the both in a critical situation, not only from a microbiological point of view, but also from a chemical point of view in the case of the use of unregulated disinfectants.
Antimicrobial research: Novel bioknowledge and educational programs (A. Méndez-Vilas, Ed.)
319
_____________________________________________________________________________

In the context of maintaining the quality of dental care and improving the safety of care, it is important to use for dental care water that corresponds at least to the criteria of potability. Dental instruments must be equipped with check valves to limit the passage of microorganisms from the oral cavity to the instruments (Figure 4).
Fig. 4 Infectious risk in dental environment.
Infection control programs in medical and dental field
In the hospital or other health care institution, the patient is in contact with a microbial world where he or she is at risk of contracting a health-related or nosocomial infection. Invasive infections due to yeasts represent both diagnostic and therapeutic problems. Identification of micro-organisms is the first act performed by a diagnostic laboratory, which is essential information in the microbiological diagnosis of an infection [44]. Diagnosis relies mainly on direct approaches of isolation and then identification. Given the high number of yeasts involved in these infections and the inability of conventional identification systems to identify them, new rapid detection methods are required to meet the needs of public health. The present identification no longer includes the comparison of morphological and biochemical properties, it is based on the global identification of the ribosomal proteins and the sequencing of the DNA. MALDI-TOF (Matrix Assisted Laser Desorption/Time-of-Flight) is a technique for the analysis and the identification of yeasts according to their proteins by measuring their "flight times" which is proportional to their masses. This technique of identification is increasingly used because of its speed, simplicity of implementation, reduced cost of reagents and reliability of results using a regularly enriched database, which greatly improves the identification of clinical strains (Figure 5). Several authors confirm the performance of MALDI-TOF MS [44-47].
Antimicrobial research: Novel bioknowledge and educational programs (A. Méndez-Vilas, Ed.)
320
_____________________________________________________________________________
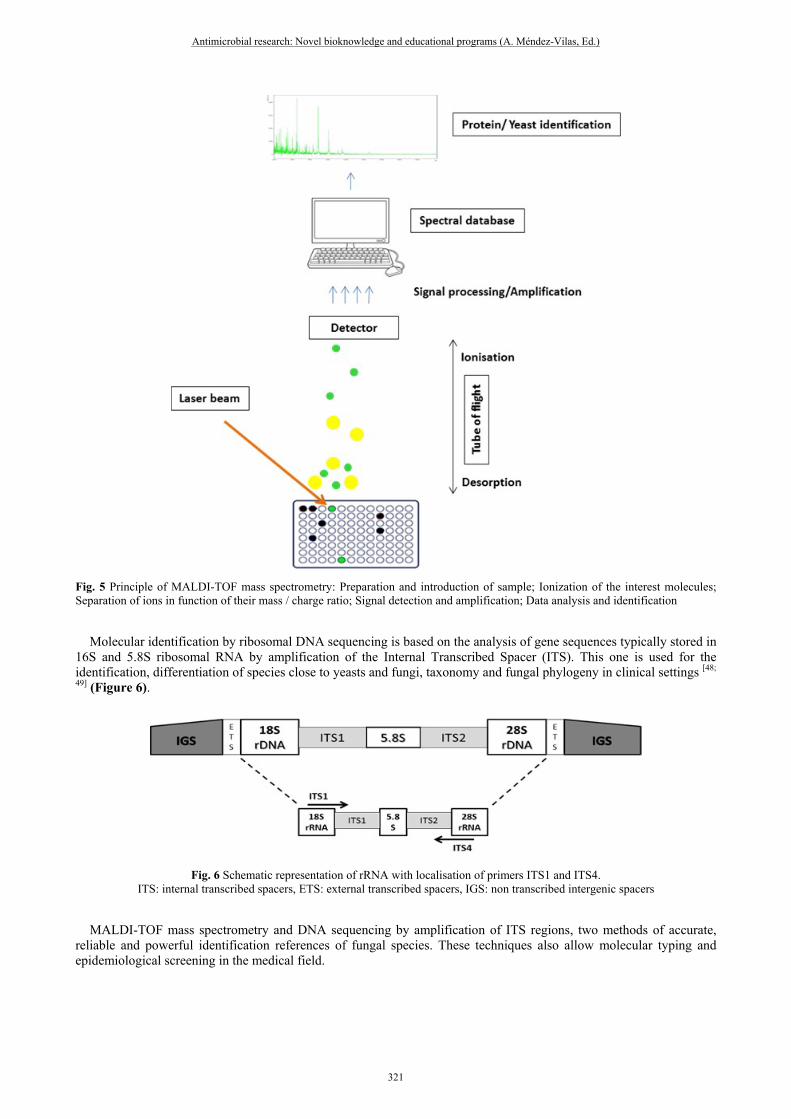
Fig. 5 Principle of MALDI-TOF mass spectrometry: Preparation and introduction of sample; Ionization of the interest molecules; Separation of ions in function of their mass / charge ratio; Signal detection and amplification; Data analysis and identification
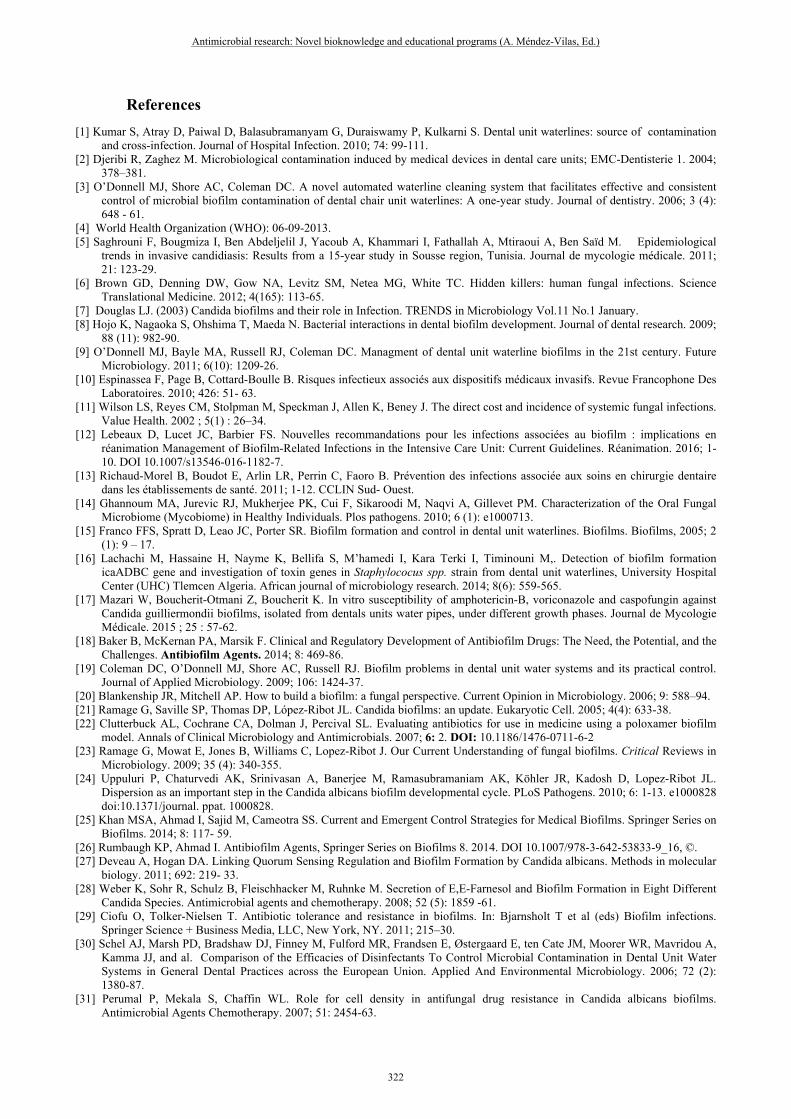
Molecular identification by ribosomal DNA sequencing is based on the analysis of gene sequences typically stored in 16S and 5.8S ribosomal RNA by amplification of the Internal Transcribed Spacer (ITS). This one is used for the identification, differentiation of species close to yeasts and fungi, taxonomy and fungal phylogeny in clinical settings [48;
49] (Figure 6).
Fig. 6 Schematic representation of rRNA with localisation of primers ITS1 and ITS4.
ITS: internal transcribed spacers, ETS: external transcribed spacers, IGS: non transcribed intergenic spacers
MALDI-TOF mass spectrometry and DNA sequencing by amplification of ITS regions, two methods of accurate, reliable and powerful identification references of fungal species. These techniques also allow molecular typing and epidemiological screening in the medical field.
Antimicrobial research: Novel bioknowledge and educational programs (A. Méndez-Vilas, Ed.)
321
_____________________________________________________________________________
References [1] Kumar S, Atray D, Paiwal D, Balasubramanyam G, Duraiswamy P, Kulkarni S. Dental unit waterlines: source of contamination
and cross-infection. Journal of Hospital Infection. 2010; 74: 99-111. [2] Djeribi R, Zaghez M. Microbiological contamination induced by medical devices in dental care units; EMC-Dentisterie 1. 2004;
378–381. [3] O’Donnell MJ, Shore AC, Coleman DC. A novel automated waterline cleaning system that facilitates effective and consistent
control of microbial biofilm contamination of dental chair unit waterlines: A one-year study. Journal of dentistry. 2006; 3 (4): 648 - 61.
[4] World Health Organization (WHO): 06-09-2013. [5] Saghrouni F, Bougmiza I, Ben Abdeljelil J, Yacoub A, Khammari I, Fathallah A, Mtiraoui A, Ben Saïd M. Epidemiological
trends in invasive candidiasis: Results from a 15-year study in Sousse region, Tunisia. Journal de mycologie médicale. 2011; 21: 123-29.
[6] Brown GD, Denning DW, Gow NA, Levitz SM, Netea MG, White TC. Hidden killers: human fungal infections. Science Translational Medicine. 2012; 4(165): 113-65.
[7] Douglas LJ. (2003) Candida biofilms and their role in Infection. TRENDS in Microbiology Vol.11 No.1 January. [8] Hojo K, Nagaoka S, Ohshima T, Maeda N. Bacterial interactions in dental biofilm development. Journal of dental research. 2009;
88 (11): 982-90. [9] O’Donnell MJ, Bayle MA, Russell RJ, Coleman DC. Managment of dental unit waterline biofilms in the 21st century. Future
Microbiology. 2011; 6(10): 1209-26. [10] Espinassea F, Page B, Cottard-Boulle B. Risques infectieux associés aux dispositifs médicaux invasifs. Revue Francophone Des
Laboratoires. 2010; 426: 51- 63. [11] Wilson LS, Reyes CM, Stolpman M, Speckman J, Allen K, Beney J. The direct cost and incidence of systemic fungal infections.
Value Health. 2002 ; 5(1) : 26–34. [12] Lebeaux D, Lucet JC, Barbier FS. Nouvelles recommandations pour les infections associées au biofilm : implications en
réanimation Management of Biofilm-Related Infections in the Intensive Care Unit: Current Guidelines. Réanimation. 2016; 1-10. DOI 10.1007/s13546-016-1182-7.
[13] Richaud-Morel B, Boudot E, Arlin LR, Perrin C, Faoro B. Prévention des infections associée aux soins en chirurgie dentaire dans les établissements de santé. 2011; 1-12. CCLIN Sud- Ouest.
[14] Ghannoum MA, Jurevic RJ, Mukherjee PK, Cui F, Sikaroodi M, Naqvi A, Gillevet PM. Characterization of the Oral Fungal Microbiome (Mycobiome) in Healthy Individuals. Plos pathogens. 2010; 6 (1): e1000713.
[15] Franco FFS, Spratt D, Leao JC, Porter SR. Biofilm formation and control in dental unit waterlines. Biofilms. Biofilms, 2005; 2 (1): 9 – 17.
[16] Lachachi M, Hassaine H, Nayme K, Bellifa S, M’hamedi I, Kara Terki I, Timinouni M,. Detection of biofilm formation icaADBC gene and investigation of toxin genes in Staphylococus spp. strain from dental unit waterlines, University Hospital Center (UHC) Tlemcen Algeria. African journal of microbiology research. 2014; 8(6): 559-565.
[17] Mazari W, Boucherit-Otmani Z, Boucherit K. In vitro susceptibility of amphotericin-B, voriconazole and caspofungin against Candida guilliermondii biofilms, isolated from dentals units water pipes, under different growth phases. Journal de Mycologie Médicale. 2015 ; 25 : 57-62.
[18] Baker B, McKernan PA, Marsik F. Clinical and Regulatory Development of Antibiofilm Drugs: The Need, the Potential, and the Challenges. Antibiofilm Agents. 2014; 8: 469-86.
[19] Coleman DC, O’Donnell MJ, Shore AC, Russell RJ. Biofilm problems in dental unit water systems and its practical control. Journal of Applied Microbiology. 2009; 106: 1424-37.
[20] Blankenship JR, Mitchell AP. How to build a biofilm: a fungal perspective. Current Opinion in Microbiology. 2006; 9: 588–94. [21] Ramage G, Saville SP, Thomas DP, López-Ribot JL. Candida biofilms: an update. Eukaryotic Cell. 2005; 4(4): 633-38. [22] Clutterbuck AL, Cochrane CA, Dolman J, Percival SL. Evaluating antibiotics for use in medicine using a poloxamer biofilm
model. Annals of Clinical Microbiology and Antimicrobials. 2007; 6: 2. DOI: 10.1186/1476-0711-6-2 [23] Ramage G, Mowat E, Jones B, Williams C, Lopez-Ribot J. Our Current Understanding of fungal biofilms. Critical Reviews in
Microbiology. 2009; 35 (4): 340-355. [24] Uppuluri P, Chaturvedi AK, Srinivasan A, Banerjee M, Ramasubramaniam AK, Köhler JR, Kadosh D, Lopez-Ribot JL.
Dispersion as an important step in the Candida albicans biofilm developmental cycle. PLoS Pathogens. 2010; 6: 1-13. e1000828 doi:10.1371/journal. ppat. 1000828.
[25] Khan MSA, Ahmad I, Sajid M, Cameotra SS. Current and Emergent Control Strategies for Medical Biofilms. Springer Series on Biofilms. 2014; 8: 117- 59.
[26] Rumbaugh KP, Ahmad I. Antibiofilm Agents, Springer Series on Biofilms 8. 2014. DOI 10.1007/978-3-642-53833-9_16, ©. [27] Deveau A, Hogan DA. Linking Quorum Sensing Regulation and Biofilm Formation by Candida albicans. Methods in molecular
biology. 2011; 692: 219- 33. [28] Weber K, Sohr R, Schulz B, Fleischhacker M, Ruhnke M. Secretion of E,E-Farnesol and Biofilm Formation in Eight Different
Candida Species. Antimicrobial agents and chemotherapy. 2008; 52 (5): 1859 -61. [29] Ciofu O, Tolker-Nielsen T. Antibiotic tolerance and resistance in biofilms. In: Bjarnsholt T et al (eds) Biofilm infections.
Springer Science + Business Media, LLC, New York, NY. 2011; 215–30. [30] Schel AJ, Marsh PD, Bradshaw DJ, Finney M, Fulford MR, Frandsen E, Østergaard E, ten Cate JM, Moorer WR, Mavridou A,
Kamma JJ, and al. Comparison of the Efficacies of Disinfectants To Control Microbial Contamination in Dental Unit Water Systems in General Dental Practices across the European Union. Applied And Environmental Microbiology. 2006; 72 (2): 1380-87.
[31] Perumal P, Mekala S, Chaffin WL. Role for cell density in antifungal drug resistance in Candida albicans biofilms. Antimicrobial Agents Chemotherapy. 2007; 51: 2454-63.
Antimicrobial research: Novel bioknowledge and educational programs (A. Méndez-Vilas, Ed.)
322
_____________________________________________________________________________

[32] Bujdáková H, Management of Candida biofilms – state of knowledge and new options for prevention and eradication. Future Microbiology. 2016; 10.2217/fmb.15.139.
[33] Sanglard D, Ischer F, Marchetti O, Entenza J, Bille J. Calcineurin A of Candida albicans: involvement in antifungal tolerance, cell morphogenesis and virulence. Molecular microbiology. 2003; 48 (4): 959- 76.
[34] Bridier A, Briandet R, Thomas V, Dubois-Brissonnet F. Comparative biocidal activity of peracetic acid, benzalkonium chloride and ortho-phthalaldehyde on 77 bacterial strains. Journal of Hospital Infection. 2011; 78: 208-13.
[35] Lafleur MD, Kumamoto CA, Lewis K. Candida albicans Biofilms Produce Antifungal-Tolerant Persister Cells. Antimicrobial agents and chemotherapy. 2006; 50 (11): 3839-46.
[36] Lafleur MD, Qi Q, Lewis K. Patients with Long-Term Oral Carriage Harbor High-Persister Mutants of Candida albicans. Antimicrobial agents and chemotherapy. 2010; 54 (1): 39-44.
[37] Baillie GS. and Douglas J. Matrix Polymers of Candida biofilms and their possible role in biofilm resistance to antifungal agent. Journal of antimicrobial chemotherapy. 2000; 46: 397- 403.
[38] Mukherjee PK, Chandra J, Kuhn DM, et al. Mechanism of fluconazole resistance in Candida albicans biofilms: phase-specific role of efflux pumps and membrane sterols. Infection and Immunity. 2003; 71: 4333- 40.
[39] Ramage G, Rajendran R, Sherry L, Williams C. Fungal biofilm resistance. International Journal of Microbiology. 2012; p14. Article ID 528521.
[40] Barbeau J. Waterborne biofilms and dentistry: the changing face of infection control. Journal of Canadian Dental Association. 2000; 66: 539-41.
[41] Kohn WG, Harte JA, Malvitz DM, Collins AS, Cleveland JL, Eklund KJ. Cover story guidelines for infection control in dental health care setting- 2003. The journal of American dental association. 2004; 135 (1): 33-47.
[42] O’Donnell MJ, Tuttlebee CM, Falkiner FR, Coleman DC. Bacterial contamination of dental chair units in a modern dental hospital caused by leakage from suction system hoses containing extensive biofilm. Journal of hospital infection, 2005; 59 (4): 348-60.
[43] Harrel SK, Molinari J. Aerosols and splatter in dentistry: a breif rewiew of the literature and infection control implications.The journal of American dental association. 2004; 135 (4): 429-37.
[44] Riegel P, de Briel D, Dauwalder O. Automatisation de l’identification bactérienne. Revue francophone des laboratoires. 2016; 482: 39- 47.
[45] L’Ollivier C, Cassagne C, Normand AC, Bouchara JP, Contet-Audonneau N, Hendrickx M, Fourquet P, Coulibaly O, Piarroux R, RANQUE S. A MALDI-TOF MS procedure for clinical dermatophyte species identification in the routine laboratory. Medical Mycology. 2013; 1-8.
[46] Ranque S, Normand AC, Cassagne C, Murat JB, Bourgeois N, Dalle F, Gari-Toussaint M, Fourquet P, Hendrickx M, Piarroux R. MALDI-TOF mass spectrometry identification of filamentous fungi in the clinical laboratory. Mycoses diagnosis therapy and prophylaxis of fungal Diseases. 2013; 1-6. Doi:10.1111/myc.12115.
[47] Munier AL, Leflon-Guibout V. Infections à Campylobacter : tableaux cliniques, prise en charge diagnostique et thérapeutique. Journal des Anti-infectieux. 2016; 18: 169 -76
[48] Shokohi T, Hashemi Soteh MB, Pouri ZS, Hedayati MT, Mayahi S. Identification of Candida species using PCR-RFLP in cancer patients in Iran. Indian Journal of Medical Microbiology. 2010; 28 (2): 147- 51.
[49] Normand AC, Cassagne C, Ranque S, L’Ollivier C, Fourquet P, Roesems S, Hendrickx M, Piarroux R. Assessment of various parameters to improve MALDI-TOF MS reference spectra libraries constructed for the routine identification of filamentous fungi. BMC Microbiology. 2013; 13: 76.
Antimicrobial research: Novel bioknowledge and educational programs (A. Méndez-Vilas, Ed.)
323
_____________________________________________________________________________