Embed Size (px)
Citation preview

Vision for future developmentProgramme NPfIT DOCUMENT NUMBERSub-Prog/Project PACS National
Prog Org Prog/Proj
DocType
Seq
Group Prog. DirectorNat Impl Director
CKM
KM NPFIT PACS PMGPACS Prog. Director
MJ
Author KM/DJ/ED Version No 3.2NPO/PSO Contact Status Final Draft
Picture Archiving and Communications System (PACS)
Vision for future development of PACS and RIS
National Clinical Reference Panel
Page 1 of 30

Vision for future developmentProgramme NPfIT DOCUMENT NUMBERSub-Prog/Project PACS National
Prog Org Prog/Proj
DocType
Seq
Group Prog. DirectorNat Impl Director
CKM
KM NPFIT PACS PMGPACS Prog. Director
MJ
Author KM/DJ/ED Version No 3.2NPO/PSO Contact Status Final Draft
Version Date Amendment HistoryV 1.2 26/09/05 First draft for comment by PACS TeamV 1.3 14/10/05 Draft revisions KM/EDV 1.4 - 5 24 & 25/10/05 Draft revisions by KM/DJV 1.6 - 8 15, 18 &
25/11/05Draft revisions and additions by KM
V 1.9 28/11/05 Additions by DJV 2.0 30/12/05 Major redraft by KM, taking account of stakeholder
commentsV 2.1 09/01/06 Further content addedV2.2 10/01/06 Section 2.2 revisedV2.3 12/01/06 Content addedV2.4 16/01/06 Initial QA comments included. Content added. Issued as
first draft for DH reviewV2.5 20/01/06 Revisions by KM on behalf ED
Technology assessment moved to Appendix BV2.6 28/03/06 Revisions by KM following feedback from stakeholders
including Physiological Measurement GroupV3.0 29/03/06 Revised following review with PACS technical team and
further input from Diagnostics Branch V3.1 31/03/06 Minor revisions following review by ED and NCRP 30/3/06V3.2 Final Draft 25/04/06 Final additions of CRP list and K&M diagram
ApprovalsThis document to be approved by:
Name Signature Title Date of Issue VersionErika Denton National Clinical
Lead for Imaging; Joint Chair PACS NCRP
Michael Thick Joint Chair PACS NCRP
Kathy Mason National Implementation Director
Max Jones PACS Programme Director
This is a controlled document.
To be reviewed by:The PACS National Clinical Reference PanelPACS Connecting for Health Technical Team
Page 2 of 30

Vision for future developmentProgramme NPfIT DOCUMENT NUMBERSub-Prog/Project PACS National
Prog Org Prog/Proj
DocType
Seq
Group Prog. DirectorNat Impl Director
CKM
KM NPFIT PACS PMGPACS Prog. Director
MJ
Author KM/DJ/ED Version No 3.2NPO/PSO Contact Status Final Draft
Table of Contents1. INTRODUCTION............................................................................................................................4
1.1 PURPOSE OF THIS DOCUMENT.................................................................................................41.2 BACKGROUND.........................................................................................................................41.3 SUMMARY OF REVIEW APPROACH..........................................................................................4
2. OVERVIEW OF DEVELOPMENT STRATEGY FOR DIAGNOSTIC IMAGING.............6
2.1 POLICY DRIVERS.....................................................................................................................62.1.1. System reform....................................................................................................................62.1.2. Patient Led NHS...............................................................................................................62.1.3. Patient choice....................................................................................................................72.1.4. Workforce reform and service redesign...........................................................................72.1.5. Organisational change, commissioning a patient-led NHS............................................82.1.6. Integrated Service Improvement Programme (ISIP)......................................................82.1.7. Financial reform, Payment by Results.............................................................................8
2.2 VISION FOR DIAGNOSTIC IMAGING SERVICES.........................................................................82.2.1. Information Vision for Diagnostic Services..................................................................12
3. MEETING THE VISION............................................................................................................13
3.1 VISION ENABLERS.................................................................................................................133.1.1. Imaging workforce modernisation.................................................................................143.1.2. Independent sector capacity............................................................................................143.1.3. Technology solutions......................................................................................................143.1.3.1. PACS solutions...........................................................................................................143.1.3.2. Clinical Information Systems....................................................................................153.1.3.3. Medical Devices (Modalities).....................................................................................163.1.4. Service Transformation..................................................................................................16
4. CONCLUSIONS...........................................................................................................................18
4.1 PROLIFERATION OF MEDICAL DEVICES..................................................................................194.2 IMAGE VOLUMES...................................................................................................................204.3 IMAGE TRAFFIC.....................................................................................................................224.4 INFORMATION GOVERNANCE ISSUES....................................................................................224.5 STANDARD NATIONAL CODING AND REPORTING REQUIREMENTS.......................................224.6 SERVICE TRANSFORMATION IMPACTS...................................................................................234.7 INTEGRATION WITH OTHER NPFIT APPLICATIONS................................................................234.8 INDEPENDENT SECTOR INTERDEPENDENCIES........................................................................244.9 NON-NHS CFH PACS SOLUTIONS.......................................................................................244.10 NON RADIOLOGICAL IMAGING INFORMATION SYSTEMS........................................................254.11 BROADENING PACS ACCESS................................................................................................25
APPENDIX A: NATIONAL PACS CLINICAL REFERENCE PANEL MEMBERSHIP............26
APPENDIX B: INITIAL ASSESSMENT OF TECHNOLOGY SOLUTIONS BY SERVICE .........
Page 3 of 30

PACS Programme: NCRP Vision for future development
1. Introduction1.1Purpose of this DocumentThis document aims to set out the vision and next steps in the ongoing development
of PACS to support the wider strategy for diagnostic imaging across the NHS.
1.2BackgroundAs part of the process that underpinned the decision to proceed with the procurement
of PACS systems as part of the implementation of the National Programme for IT
(NPfIT), a PACS Programme Strategy was developed in December 2003. This was
later reflected in the Programme Initiation Document, finalised in January 20051. The
PACS Programme, in the light of emerging policy and strategy for the development of
diagnostic imaging services in the NHS and the progress with implementation to
date, has identified the need to review these original strategic plans for the
procurement and ongoing development of PACS for the NHS.
1.3Summary of Review ApproachTo commence this review, a facilitated workshop was held with members of the
PACS National Clinical Reference Panel (NCRP) on 31 August 2005. A list of
members of the NCRP is included at Appendix A. This identified the key clinical and
service issues that PACS needs to support in the future.
This document forms the second element of the review; taking the development
strategy for diagnostic imaging and assessing any potential gaps in the current
provision and plans for PACS (and where relevant other national enabling initiatives).
The third element, planned to occur following release of this document, is further
analysis by technical and commercial members of the NHS Connecting for Health
(NHS CfH) PACS central team to provide an action plan for which issues will be
resolved through the NHS CfH contracts and to identify any issues which are beyond
the scope of NHS CfH to resolve.
Following this, an assessment will be made by the PACS NCRP and the National
Diagnostic Imaging Board to recommend any further work to enable delivery of the
diagnostic imaging strategy for the NHS. The three other DH Diagnostics Steering 1 Picture Archive and Communications System (PACS) Programme Initiation Document, version 2.0 Final, 07/01/05, Connecting for Health Programme Office, doc number: NPFIT/PAC/PMG/GOV/0001.
Page 4 of 30

PACS Programme: NCRP Vision for future development
Groups, Endoscopy; Pathology and Physiological Measurement, will also be
consulted, along with the 18 weeks programme.
The timeline for this Strategy Review process is:
1) NCRP Strategy Review Launch Workshop – August 2005
2) Review and discussion with key stakeholders – Sept 05 – March 06
(Including the National Imaging Forum in April 2006)
3) Vision Document approved by NCRP – April 2006
4) NHS CfH PACS Development Roadmap – April – June 2006
Page 5 of 30

PACS Programme: NCRP Vision for future development
2. Overview of Development Strategy for Diagnostic Imaging
Diagnostic imaging is an essential part of the care pathway for a large proportion of
patient care.
It is provided in diverse locations and has to be ‘on-demand’, since further care is
often very dependent on the findings of the diagnostics undertaken. The demand for
diagnostic images, in terms of volume and image diversity, is increasing year on year
and is expected to continue as such.
Many stakeholders rely on diagnostic images, often needing information remote from
the image source and over different time periods.
Technology advances in image acquisition, storage and analysis have changed the
way in which this service operates and is used over the last two decades. The
technology advance is expected to continue over the next decade, thereby further
improving efficiency, value and quality.
2.1Policy Drivers
There are a number of policy drivers directly relevant to diagnostic imaging and
others where diagnostic imaging plays an important role in their wider achievement.
Relevant policy drivers are summarised here:
2.1.1. System reform System reform represents a group of interconnected policies that aim to support the
transformation of the NHS to a system that is truly patient-led. They will give patients
more choice, more personalised care and real control to improve their own health.
Most recently the Primary Care White Paper: Our Health, Our Care, Our Say.2
2.1.2. Patient Led NHSIn March 2005 the Department of Health’s ‘Creating a Patient-led NHS – Delivering
the NHS Improvement Plan’3, set out the next steps in delivery of the NHS
Improvement Plan focusing on the system reform required to put patients at the
centre of care delivery.
2 http://www.dh.gov.uk/ourhealthourcareoursay/3 Creating a Patient-led NHS – Delivering the NHS Improvement Plan; DoH, 17 March 2005.
Page 6 of 30

PACS Programme: NCRP Vision for future development
Service models will be developed to give patients more choice, control and improved
access. Integrated patient pathways will follow the patient’s journey; ensuring
services are designed and delivered around the patient. Diagnostic imaging is a key
component in a very high proportion of such patient pathways and work is in hand to
develop much more flexible and accessible services across the country. There is
also an increasing move towards use of diagnostics in screening services and early
diagnosis in priority pathways such as cancer and CHD, contributing to better health
promotion, protection and improvement.
Diagnostics is identified as one of the five key targets set for the NHS to enable
delivery of the overall system reform. The other four key target areas are:
18 week waiting targets4
Health improvement
Long term conditions
Unscheduled care
Clearly, improved diagnostic services will also impact on the other target areas
2.1.3. Patient choice Patient choice is at the core of the governments’ current policy, this is reflected in the
current targets that are being implemented to give patients a choice. Of particular
relevance to this review is the ‘choice of scan’ target.5
2.1.4. Workforce reform and service redesignEffective implementation of Agenda for Change6, the new consultants’ contract7 and
realising the benefits in terms of a workforce appropriately skilled and available to
deliver the health service of the future is a key factor in achieving these changes.
The appropriate and effective use of extended roles is another aspect of workforce
reform that has been identified as one of the Modernisation Agency’s Ten High
Impact Changes8.
4 http://www.18weeks.nhs.uk/public/default.aspx5 http//www.18weeks.nhs.uk/documents/Choice_of_scan.pdf6http://www.dh.gov.uk/PolicyAndGuidance/HumanResourcesAndTraining/ModernisingPay/fs/en7 as above8 http://www.wise.nhs.uk/cmsWISE/HIC/HIC+Intro.htm
Page 7 of 30

PACS Programme: NCRP Vision for future development
2.1.5. Organisational change, commissioning a patient-led NHSThe planned organisational changes for Strategic Health Authorities, Primary Care
Trusts and the inclusion of private healthcare providers in the ongoing provision of
NHS services to patients must not constrain patient choice or access to services. It
is also essential that future service transformation in the NHS is coordinated across
providers to provide seamless and cost effective services.
2.1.6. Integrated Service Improvement Programme (ISIP)The Integrated Service Improvement Programme (ISIP)9 is a national initiative
enabling health economy-wide service transformation with consistent, transparent
and comparable measures across the whole of the NHS. For diagnostic imaging
services spread over a large number of organisations, this planning regime will be
essential to focus scare resources and make best use of capital investment.
2.1.7. Financial reform, Payment by ResultsIn future, all services, including diagnostic imaging will need to be able to be
identified and accurately costed in line with standard national tariffs in order to
support the new financial regime, where services will be invoiced to commissioners
on the basis of activity.
This approach is being supported by the development of standard national coding for
all diagnostic imaging interventions and activities to enable compilation of invoices
based on activity.
2.2Vision for Diagnostic Imaging Services
The delivery of diagnostic imaging services across the NHS is a wide ranging and
complex challenge. The vision is described below, grouped within a number of
change areas.
Access
It is planned that, patients will not wait longer than six weeks for any imaging
and in many cases this will be available on demand in order to deliver this
target of maximum waiting times for treatment overall of 18 weeks, from GP
9 See ISIP website: http://www.isip.nhs.uk/
Page 8 of 30

PACS Programme: NCRP Vision for future development
referral to hospital treatment. This is a psa target to achievable by December
200810.
To achieve this target will require redesign of the referral pathways and
protocols, including increased and earlier use of diagnostics imaging. It is
also likely to include direct access to imaging services from primary care.
Availability
Different delivery models, where services are provided in different
environments such as one stop diagnostic and treatment centres and walk in
centres, tailored to local health community needs.
Further development of specialist clinical networks, such as those currently in
place for cancer, CHD and emergency care.
More centralised diagnostic imaging reporting services, able to provide
services to a wide health community 24 hours a day 7 days a week. Such
models will maximise the benefits from capital equipment and enable greater
flexibility of the imaging workforce.
There will be plurality and contestability of the provision of imaging services,
which will be delivered through a combination of NHS and independent sector
provision.
Choice
Patients will be offered a choice of time and place for their diagnostic imaging.
Scope of diagnostic services
The following have been identified by the PACS National Clinical Reference
Panel for inclusion within the vision scope:
o Diagnostic Imaging
Angiography inc cardiology
Breast screening
CT
Dental imaging
10 ‘Commissioning an 18 week patient pathway, Proposed Principles and definitions: Discussion document’, DH October 2005.
Page 9 of 30

PACS Programme: NCRP Vision for future development
DEXA
Fluoroscopy
MRI
Nuclear medicine
PET
Plain film radiography
Radiotherapy
Symptomatic mammography
Thermography
Ultrasound
o Pathology
Cytology
Haematology
Histology
Microbiology
Pathology
Virology
o Endoscopy (including gastro and intestinal)
o Physiological measurement
Dermatology
ECG waveforms
Echo cardiography
Electrophysiological measurement
Endoscopy (other, eg. Laproscopy)
Medical photography
Ophthalmology
Clinical Standards
Page 10 of 30

PACS Programme: NCRP Vision for future development
All services commissioned by the NHS will be delivered to the same
comprehensive framework of national standards that encompasses all
providers, both public and independent sector.
Professional training will be carried out in line with DH policy and
recommendations made by the Royal Colleges and other appropriate bodies.
Diagnostic imaging services will be delivered in line with best practice as
advised by the Royal Colleges and other appropriate bodies. This will include
policy on National retention of appropriate images.
Technology and information
PACS solutions are central to the delivery of the vision for diagnostic imaging,
supporting the development and improvement of clinical practice. Current
and future generations of medical devices and associated peripherals that are
required to capture and translate diagnostic images and associated data will
also form the basis of delivery of this vision.
This will include:
o A transition towards Direct Digital Radiology
o Increased use of imaging as an interventional treatment, eg. Stroke
and other image guided therapies,
o Non-invasive autopsy
o Use of enhanced modalities such as:
Multislice Computerised Tomography (CT)
Positron Electron Tomography (PET) scanning
Diagnostic images and reports will be available as clinically required,
accessible as part of a national care record for every patient. This will be
securely accessible to relevant clinicians and other healthcare professional
requiring it to support delivery of healthcare, 24 hours a day, 7 days a week.
Information on wider care issues, pathways and protocols, relating to diagnostic
imaging will be made available through the National Knowledge Service, providing
robust evidence-based information for clinicians.
Page 11 of 30

PACS Programme: NCRP Vision for future development
PACS will also need to be developed in the context of the implementation of the
Map of Medicine.
The development of PACS will be in the context of the commitment to meet the
Care Record Guarantee in respect of security and confidentiality of patient
information.
2.2.1. Information Vision for Diagnostic ServicesFor the purposes of this document, we have focused on the information aspect of the
overall service vision. The ‘information vision’ for diagnostic imaging for the NHS is
“to have relevant diagnostic images and associated data
available and useable in a timely manner at the point of care for all
clinicians, irrespective of the location and timing of the care being
provided. This would apply to any aspect of care delivery
requiring images and associated data and would integrate
relevant diagnostic images and data seamlessly with wider
pertinent clinical information.
Further, to have relevant diagnostic images and associated data
securely available and useable for all clinicians as appropriate and
relevant to support service improvements in care delivery, service
planning, research or education.”
Page 12 of 30

PACS Programme: NCRP Vision for future development
3. Meeting the vision
3.1Vision enablers
To achieve the service vision set out above will require comprehensive development
of a range of enabling elements, which are being driven and overseen by the
Diagnostics Branch of the Department of Health. Diagnostics has been grouped into
four main areas, each with a national steering group led by a national clinical lead:
Endoscopy
Imaging
Pathology
Physiological Measurement
The PACS Programme is already working closely with the National Imaging Board
and the National Clinical Lead for Imaging, formally linking governance arrangements
to ensure effective links and communication.
Links with the other three areas are being established.
Within these arrangements, the key areas for development to enable development
towards the future vision in all four areas include:
Workforce modernisation
Independent Sector capacity
Technology solutions (PACS, related information systems and medical
devices)
Service Transformation
This set of changes will, collectively, support diagnostics services as a seamless
component part of the patient’s pathway from GP referral to delivery of secondary
care, all within the 18 week timeframe.
This document focuses on the technology solutions area. Other areas are
summarised briefly below but are not within the scope of this analysis.
Page 13 of 30

PACS Programme: NCRP Vision for future development
3.1.1. Imaging workforce modernisationThe Diagnostics Branch of the Department of Health are leading the work, in
partnership with the Workforce Review Team11, to identify and plan for the workforce
requirements of the future to support the delivery of diagnostic services in line with a
patient-led NHS. This incorporates issues such as recruitment/ retention, skill mix,
education and learning.
These changes in workforce are further supported by the establishment of three
National Radiology Academies, which, in addition to addressing shortages in the
radiologist workforce, will train these professionals in line with the new ways of
working including maximising the benefits of PACS and CRS (Care Records Service)
technology as it is deployed across the country.
3.1.2. Independent sector capacity To achieve the goals set by the NHS Plan and subsequent policy and plans, there
was the requirement to increase capacity in key areas, including diagnostic imaging.
This has resulted in the procurement of a first phase of independent sector diagnostic
imaging services for MRI and CT. A second phase encompassing most imaging
modalities is currently being procured.
This procurement from the independent sector has also contributed to the objective
of increasing contestability between providers in the NHS.
3.1.3. Technology solutions
3.1.3.1. PACS solutionsA vision for the implementation and subsequent development of PACS solutions
within the National Programme for IT (NPfIT) was set out in the Programme Initiation
Document (PID)12. This document made it clear that deployment of PACS
technology across the whole of the NHS is seen as a key enabler to the delivery of
diagnostic imaging services in line with the vision and strategic policy context
outlined above.
An overriding objective is to ensure that the right images and related clinical
information is available in the right place at the right time to support patient care.
11 www.healthcareworkforce.org.uk12
Page 14 of 30

PACS Programme: NCRP Vision for future development
This will require complete integration of data and functionality across all areas of
healthcare, including primary, community and secondary care.
PACS can already be deployed to achieve filmless radiology departments. The
scope of the current PACS programme has an initial objective to deliver 100% digital
and filmless radiology services in acute Trusts across England by March 2007. To
support progress beyond this the current programme has contracts structured such
that local health communities (LHCs) are able to evolve further, from a single Trust’s
radiology service becoming filmless to the ultimate community-wide PACS
encompassing a number of other diagnostic services that use images of various
kinds, e.g. digital images of microscopic images such as those used in pathology and
services being delivered across a number of provider organisations acting in
collaboration. PACS is intended as the storage and retrieval tool for providing the
complete suite of medical images as part of the Clinical patient record.
PACS solutions have always required the availability of powerful and resilient data
communications networks. At a community level, PACS will require an acceptable
level of both local and wide area networking through N3.
3.1.3.2. Clinical Information SystemsPACS is an excellent storage, retrieval and viewing technology but it relies on other
information systems to process image data and handle image transactions.
Within the present NHS CfH solution, the focus has been on ensuring RIS solutions
and, ultimately, CRS functionality operate seamlessly with the PACS solutions
provided to the NHS. While provision in the contracts has been made for extending
the range of information systems that potentially could connect to PACS solutions,
this is not currently planned for deployment to a specific timeframe. It remains
unclear whether the incorporation of further separate information systems or awaiting
the deployment of CRS functionality to link to PACS solutions is the best route
forward in the short to medium term.
Of equal importance is the relationship of NHS CfH PACS solutions to wider
functionality and information, including:
Choose and Book
Page 15 of 30

PACS Programme: NCRP Vision for future development
Existing PACS solutions supplied outside of the current programme (including
independent sector provision)
GP systems
Order Communications and Results Reporting
Decision support and the use of protocols
3.1.3.3. Medical Devices (Modalities)The pace of technology change in medical devices relevant to the diagnostic imaging
service is significant. Each year, technology increases the service’s potential to
acquire more images and in ever greater detail.
This growth in digital medical devices will transform the diagnostic imaging service
for the NHS; one impact of this will be the requirement for NHS CfH technology
solutions to cope with increasing volumes of data to be stored.
In relation to PACS solutions, there are two essential elements to be achieved for all
medical devices and modalities; to ensure images are produced to a DICOM
standard and to provide storage and retrieval infrastructure able to handle anticipated
image volumes.
3.1.4. Service TransformationThere are many aspects to service transformation in relation to imaging services.
Services within NHS organisations will benefit from the new investment in
technology, the modernised workforce and the inclusion of the Independent sector in
this service area but only holistic and community-wide service improvement will fully
deliver the government’s transformation agenda and maintain continuous
improvement of services.
The DH has an initiative in place, the Integrated Service Improvement Programme
(ISIP), which is providing a methodology to enable and coordinate local health
economies, including all relevant service partners, to plan service change
collaboratively to optimise efficiency, value and quality.
Page 16 of 30

PACS Programme: NCRP Vision for future development
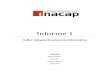
One of the leading SHAs in using PACS technology to underpin integrated service
transformation across the local community has identified the following transformation
pathway13.
13 Kent & Medway Strategic Health Authority
Page 17 of 30
Federation Network Mutual Network Managed Network
Advice and guidance group Some central management of services
All radiology services centrally managed
Sharing best practice Centralised film archives
Central training and educationPooled reportingReporting Centres
Teaching files
During PACS implementation
On completion of implementation
With a matured PACS

PACS Programme: NCRP Vision for future development
4. Conclusions
The next stage of this Strategy refresh process is for the NHS CfH PACS team to
prepare a development roadmap taking account of the vision set out in this report. In
addition, an initial analysis has been prepared of some of the key services using
imaging, Appendix B, and the extent to which current PACS and RIS functionality
supports clinical practice. This analysis uses a red/amber/green rating to indicate the
current state of play. For red items, it is concluded that substantial work needs to be
delivered to improve the current PACS applications to meet the vision. For amber
items, the requirement is to consider these further and determine if they are green or
red.
Overall, a number of emergent general themes requiring resolution are already
evident:
Proliferation of medical devices
Image volumes - retention policy and volume modelling
Image traffic and system performance
Information governance issues
Standard national coding and reporting requirements
Service transformation impacts
Integration with other NPfIT applications in line with clinical and business
priorities
Independent sector interdependencies
Non-NHS CfH NHS PACS solutions
Non radiological imaging information systems
Broadening PACS Access to other clinical services
In taking this agenda forward the following are key stakeholders that will need to be
involved and in some cases, take a lead:
NHS CfH PACS Team, National & Cluster levels
Page 18 of 30

PACS Programme: NCRP Vision for future development
NHS CfH Other key programmes
NHS CfH Service Implementation Directorate
NHS CfH Information Standards Board
DH Diagnostics Branch
National Imaging Board
Other Diagnostic Steering Groups
Royal Colleges
PPI Representatives
DH ISTC Directorate
ISIP Initiative
DH Medical Devices Directorate
PASA
Monitor
4.1Proliferation of medical devices
It is clear that there are continuing advances taking place in medical imaging devices.
These increase service access to/usage of digital images and/or increase the volume
of digital images acquired.
In planning the original PACS solution, a national stock-take was attempted to
ascertain the extent to which relevant medical devices were already deployed. This
exercise demonstrated that there was insufficient clarity over what was already out
there and deployments are happening all the time.
Further work is required to obtain data on what relevant devices are currently
deployed and an update mechanism put in place to monitor new devices. These
devices often represent a major capital investment by the NHS and need to be fully
utilised. Funding sources are variable, including local charitable donations and
National Lottery funds, so it is not always traceable through normal NHS funding
sources.
Page 19 of 30

PACS Programme: NCRP Vision for future development
Data recorded needs to take account of what impact any given device might have on
the PACS solution. For example, a new device that is not to a DICOM agreed
standard will require some level of interface device to connect it to the LSP PACS
solution, which may be at additional cost. These costs need to be factored into the
purchase of the device itself.
Recommendation 1: That a review is completed using already established data flows if possible, to estimate the current and future size of increased image volumes arising from this source.
Recommendation 2: That guidance is developed and issued to Trusts procuring devices to highlight the need to ensure data standards are met and that increases in image volumes is factored into business cases for such devices.
4.2Image volumes
Image volumes are certain to rise over time due to the advances in acquisition
technology and in the innovative use of this technology by clinicians as well as by the
national roll out of PACS solutions to the NHS. This is a desired state; the
investment made in PACS solutions and supporting technologies needs to be fully
utilised by the NHS. However, the consequences of this growth are based on
estimates derived from historical data.
The planning assumptions made for image storage in the original contract for LSP
PACS solutions took a baseline position from DH statistical returns (based primarily
on radiological image data) and extrapolated this based on extending PACS across
all of England, retaining every image that was created and a 12% per annum
compound growth rate in image creation. These assumptions did not take into
account i) image data from non-radiological sources and ii) adopting a policy of
selective image retention.
Given the bulk of images acquired at present (in storage capacity terms) are
Radiological images and growth was factored for 10 years (the life of the contract)
there is plenty of capacity for the short and medium term at least. Another
assumption made at the time of contract was that storage technology would continue
to reduce in price and improve in efficiency. This is still valid; however the LSPs are
Page 20 of 30

PACS Programme: NCRP Vision for future development
still costing additional storage at high rates by taking onto account peripheral
resources (servers, manpower, networks, back ups, etc). This means that the initial
strategy of simply buying more storage as we need it may not now be the best
approach.
We do know the prices to be charged for additional storage but there are two other
areas where further analysis is required to inform decision making; volume modelling
and image retention.
Volume modelling – It is not clear at this time what impact all the different service
users will have on image storage capacity needs over time. Each clinical specialty
(or in some cases sub-speciality) has different variables in the areas of image
volumes, image size and breadth of need for service access. The first two areas
directly relate to storage issues, while all three have a potential impact on image
traffic and therefore solution and infrastructure performance. Further work is required
to model each of the proposed service users of PACS solutions and consider what
storage issues could be involved over the contract term.
Image retention – The architecture for LSP PAS solutions currently allows for every
image to be retained online, but this is at a considerable cost. However, work in
Scotland has demonstrated that it is not necessary for every image to be retained
and that PACS solutions have the capability (through rules engines) to keep or
remove images based on user rules. To keep every image acquired in case it might
be needed and deploy infrastructure to store, move and access all these images may
be cost prohibitive and creates a storage legacy cost that lasts far beyond the LSP
contract term. Further work is required to assess the legal and clinical reasons for
retaining images and the timescale involved for their retention. This has two sub
strands to explore; what image data is not required at all to be stored on PACS
solutions, for example a whole cardiology video or a the full set of slices from a CT
body scan as opposed to selecting the images of interest and ignoring the rest, and
what image data is stored on PACS solutions and for how long.
Recommendation 3: That work is undertaken to clarify and prepare guidance on image retention policies, in conjunction with the Royal Colleges
Recommendation 4: That estimates are updates and commercial options reviewed for most cost efficient methods of storage
Page 21 of 30

PACS Programme: NCRP Vision for future development
Recommendation 5: That Business Case guidance for PACS is updated to reflect the findings of 3 and 4 above, to support business cases for current and future implementations and upgrades.
4.3Image traffic
LSP PACS solutions are presently architected to handle PACS traffic based on the
historical data about image volumes NHS CfH supplied. While the contracts oblige
the LSPs to deploy scalable solutions, there will be physical limits on how much
image traffic can be coped with by LSP PACS solutions.
The volume modelling work and the image retention analysis are both necessary to
fully understand this issue. Following results from these two areas, further work is
required to assess the implications on N3 and PACS technical architectures to
ensure service performance is maintained.
Recommendation 6: That the capacity of N3, both within Trusts and between Trusts and the Cluster Stores and the Spine are reviewed in the light of updated information on image volumes and traffic in the future and recommendations prepared for the most cost efficient and effective procurement of any additional capacity identified.
4.4Information Governance Issues
As one of the vanguard applications to be implemented within the NPfIT, the PACS
deployments are having to deal with information governance issues ahead of the
strategic planned solutions, such as smart card access control and legitimate
relationships, that have been developed to ensure appropriate access taking account
of patient confidentiality. This has resulted in the requirement for acceptable
pragmatic tactical solutions in the interim.
Recommendation 7: That the NHS CfH Information Standards Board reviews these interim solutions and that worthwhile lessons learned are shared across the PACS and other Programmes and effectively communicated to the service.
Page 22 of 30

PACS Programme: NCRP Vision for future development
4.5Standard National Coding and Reporting Requirements
The implementation of a national system clearly requires coherent and consistent
coding for the effective sharing of images and related information for activity and
financial reporting. Work is well underway on this aspect of the programme.
Recommendation 8: That the PACS Programme continues to coordinate and support effective and integrated development of coding and reporting requirements.
4.6Service transformation impacts
The delivery of modernised diagnostic imaging services requires a holistic approach
bringing changes in workforce, process, technology and organisation together.
Current deployment plans for NHS CfH PACS solutions mostly consider architectures
where each acute hospital is a ‘hub’ (containing the main PACS components) with
other smaller service outlets stretching from each hub, for example a health centre or
community hospital.
However, initiatives like the DH-sponsored Integrated Service Improvement
Programme are highlighting the need for diagnostic imaging services to be
transformed at a local health economy level. Such change may result in a disparity
between what PACS solutions, supporting technology infrastructure and medical
imaging devices are planned for individual hospitals and what is the optimal
arrangement for the health economy.
Further work is required to analyse the plans emerging from ISIP, the local
aspirations of NHS organisations and the current PACS deployment plans to ensure
that changes are factored in to LSP deployment arrangements over the next two
years.
Recommendation 9: That the PACS team collaborate with the ISIP team and RSU to map the service improvements that are planned that will require additional PACS services beyond the core deployments and ensure that the commercial framework can accommodate them in the most cost effective and efficient way
Page 23 of 30

PACS Programme: NCRP Vision for future development
4.7Integration with other NPfIT applications
Clearly this will already be a factor within the NPfIT planning process, however as the
different aspects of overall programme are subject to inevitable replanning and
reprioritising the PACS Programme will need to ensure that the clinical and business
priorities of diagnostic imaging services and their development programmes are
appropriately taken account of.
Recommendation 10: That the PACS Programme continues to coordinate and support effective and integrated development of integration requirements and priorities.
4.8Independent sector interdependencies
The independent sector is increasingly being used to support diagnostic imaging
service provision to the NHS. This means that even more digital images are being
created as part of care delivery.
The NHS CfH contracts will deliver PACS solutions to support those NHS
organisations taking the solution but private sector providers are not covered by
these contracts. It is possible that private sector providers have made their own
arrangements for the acquisition, storage and access to digital images created
through their own business units.
Further work is required to understand i) what arrangements private sector providers
have made for digital images, ii) how these are shared with the NHS and iii) how the
NHS will share its images with the independent sector.
Recommendation 11: That the PACS Team collaborate with the IS Procurement Team to review the requirements for enabling images captured by independent providers to be transferred into the cluster stores
4.9Non-NHS CfH PACS solutions
There are a number of PACS solutions (35+) currently operating the NHS that are not
part of the NHS CfH contracts. These are either i) legacy PACS solutions that were
in place prior to NHS CfH contracts being agreed or ii) PACS solutions procured by
NHS Foundation Trusts in the last three years from suppliers outside of NHS CfH
contracts. All these solutions are expected to link in with the Cluster data stores.
Page 24 of 30

PACS Programme: NCRP Vision for future development
However, no plans have been finalised to ensure local service provision is
maintained for all NHS organisations over the duration of the current contract term for
the LSP PACS solution. Any NHS organisations operating outside the LSP contracts
for PACS would incur additional costs to be brought into the programme.
Further work is required to identify which PACS solutions remain outside the national
contract and, on a case by case basis, what implications there are for guaranteeing
service provision over the next 8 years.
Recommendation 12: That the PACS team review legacy implementations and identify recommendations for future developments and implementations to bring them into line with the NPfIT in a cost effective and efficient way.
4.10 Non radiological imaging information systems
The NHS CfH PACS solution is technically able to interact with a wide range of
clinical information systems but to date the effort on deployment has been with RIS
solutions only. Further work is already underway to ensure necessary interfacing
with NHS CRS solutions as they come on line.
But there are a large number of diagnostic imaging service users that currently rely
on clinical information systems other than RIS to support them.
Further work is required to determine i) what functionality and systems are required
for each service user to work with PACS solutions, ii) whether the NHS CRS solution
will incorporate this functionality (making legacy systems obsolete), iii) whether it is
better to integrate existing systems or await NHS CRS deployment for wider PACS
deployment to diagnostic image users and iv) how a mixture of different information
systems/ functionality will have to operate collectively with a common PACS solution.
Recommendation 13: To review the scale and scope of PACS solutions required for images outside of radiological imaging in collaboration with the DH Diagnostics Branch and the Royal Colleges.
4.11 Broadening PACS Access
The NHS Connecting for Health PACS solution is founded on an architecture that
makes the ‘traditional’ teleradiology function largely obsolete (other than perhaps
where the service is required in a consultant’s own home). Essentially, the PACS
Page 25 of 30

PACS Programme: NCRP Vision for future development
solution can be wherever it is needed. But NHS CfH PACS solutions are demanding
on equipment and infrastructure, especially networking, and therefore extending the
full functionality of the solution to everywhere may not be cost effective.
There needs to be a further debate on the optimal access required for different users
(particularly service users outside of the Radiology department) that incorporates
wider service access, including traditional teleradiology where this is still required. It
is likely that PACS vendors will remain keen to extend their solution where they are
able to charge more additional services; however we should describe the nature and
complexity of the remote solution so that implementation is consistent and fit for
purpose.
Recommendation 14: As part of the review of scope and scale in 10, above. To included the requirement for remote access to images by clinicians.
Page 26 of 30

PACS Programme: NCRP Vision for future development
APPENDIX A: NATIONAL PACS CLINICAL REFERENCE PANEL MEMBERSHIP
Role Name Title Email AddressJoint Chair Erika Denton Consultant Radiologist, Norfolk and Norwich University
Hospital NHS Trust.National Clinical Lead for Diagnostic Imaging, Department of Health
Joint Chair Michael Thick Heart and Lung Transplant Surgeon and National Medical Director for Choose & Book and PACS
Secretary Margaret Budd PACS Implementation Coordinator NHS Connecting for Health
Department of Health PACS Lead
Kathy Mason DH National Implementation Director - PACS [email protected]
Royal College of Radiologists
Nicola Strickland
Consultant Radiologist, Hammersmith, representing the Royal College of Radiologists as Chair of the IT Sub-Committee
RCR Representative Rhidian Bramley
Consultant Radiologist, Chair of the Royal College of Radiologists PACS and Teleradiology Special Interest Group
National PACS Team David Jennings PACS Implementation Manager, Department of Health (Radiographer)
National PACS Team Gavin Mander PACS Technical Manager NHS Connecting for Health [email protected] PACS Team Jerry Norman PACS Technical Team Lead NHS Connecting for Health [email protected] PACS Team Moira Crotty NHS CFH NE Cluster PACS Implementation Advisor
(Radiographer)[email protected]
Cluster PACS Team Judi Humphreys
NHS CFH NWWM Cluster PACS Implementation Advisor (Radiographer)
Page 27 of 30

PACS Programme: NCRP Vision for future development
Cluster PACS Team Pam Kemp NHS CFH Southern Cluster PACS Implementation Advisor (Radiographer)
Cluster PACS Team Mona Pal-Singh NHS CFH Southern Cluster PACS Implementation Advisor (Radiographer)
Primary and Secondary care healthcare professionals and managers
Maxine Bullock Norfolk & Norwich University Hospital NHS Trust (Radiographer and PACS Manager)
Primary and Secondary care healthcare professionals and managers
Tony Corkett Kent and Medway PACS Programme Director (Also representative for College and Society of Radiographers)
Primary and Secondary care healthcare professionals and managers
Sarah Cush National Breast Screening Service (Radiographer) [email protected]
Primary and Secondary care healthcare professionals and managers
Jonathan Davies
Specialist Registrar in Dental Radiology, Dept. of Dental Radiology, Guy’s Hospital
Primary and Secondary care healthcare professionals and managers
Phil Dunmall Radiographer and ex PACS Implementation Advisor [email protected]
Primary and Secondary care healthcare professionals and managers
Keith Foord Consultant Radiologist, East Sussex Hospitals NHS Trust. [email protected]
Primary and Secondary care healthcare professionals and managers
Keith Goldsworthy
Radiology Services Manager (South Devon Healthcare NHS Trust)
Primary and Secondary care healthcare professionals and managers
David Grant Consultant Radiologist and Clinical Director of Diagnostics and Therapies at the Whittington Hospital NHS Trust
Page 28 of 30

PACS Programme: NCRP Vision for future development
Primary and Secondary care healthcare professionals and managers
Charles Hutchinson
Consultant Radiologist, Salford Royal Hospitals NHS Trust [email protected]
Primary and Secondary care healthcare professionals and managers
Robin Kantor Consultant Radiologist, Hillingdon Hospital NHS Trust [email protected]
Primary and Secondary care healthcare professionals and managers
Kim Krarup Consultant Radiologist, University Hospitals of Leicester [email protected]
Primary and Secondary care healthcare professionals and managers
Roddy McColl Head of DepartmentOxford Medical Illustration John Radcliffe Hospital - Representing Medical Photography
Primary and Secondary care healthcare professionals and managers
Nigel Morris Royal Free Hampstead NHS Trust - Radiology General Manager. Radiographer and ex PACS Implementation Advisor
Primary and Secondary care healthcare professionals and managers
Jackie Nicklin Senior Radiology Manager (Poole Hospitals NHS Trust) [email protected]
Primary and Secondary care healthcare professionals and managers
William Saywell Consultant Radiologist, Caldicott Guardian, NPfIT Clinical Lead, East Somerset NHS Trust
Primary and Secondary care healthcare professionals and managers
Richard Seymour
Consultant Radiologist, South Devon and National Clinical Lead for Radiology Service Improvement
AHP Clinical Champion, CfH Clinical Leads Group
Jan Laidlow National Clinical Lead for AHPs for NHS CfH (Radiographer)
Page 29 of 30

PACS Programme: NCRP Vision for future development
Nationally appointed Clusters PACS Programme Clinical Advisors
Tony Newman-Sanders
Consultant Radiologist, Mayday Healthcare NHS Trust , London Cluster representative and National Clinical Advisor
Nationally appointed Clusters PACS Programme Clinical Advisors
Kishore Reddy Consultant Radiologist, Medway NHS Trust. Southern Cluster representative and National Clinical Advisor.
Nationally appointed Clusters PACS Programme Clinical Advisors
John Somers Consultant Radiologist, Nottingham City Hospital. East of England & East Midlands Cluster representative and National Clinical Advisor.
Nationally appointed Clusters PACS Programme Clinical Advisors
Laurence Sutton
Consultant Radiologist, Huddersfield and Calderdale. North East Cluster representative and National Clinical Advisor
Radiology Service Improvement Team
Graham Hoadley
Consultant Radiologist, Blackpool and National Clinical Lead for Radiology Service Improvement
Page 30 of 30