Embed Size (px)
Citation preview

Controlled Substances: Education for the Prescriber Presented by the Utah Medical Association Foundation – “Extending the Reach of the Healer’s
Hand.”
Introduction
This education is specifically designed to comply with the Utah State Law, Utah Code Section
58-37-6.5, which requires health care providers licensed to prescribe controlled substances to
complete DOPL approved continuing education on Schedule II and III controlled substances that
are applicable to opioid narcotics, hypnotic depressants, or psychostimulants. The education may
be used toward the continuing education hours required every two years for licensure renewal
specific to their discipline.
Healthcare providers must complete 3.5 hours of SBIRT training prior to their respective
professional license renewal in 2026. This training can be used to fulfill the above controlled
substances education requirement. A licensee need only take the SBIRT training class once
during the controlled substances prescriber’s licensure.
Utah Code 58-37-6.5
This educational program has complementary goals: to assure that patients receive the care they
need to restore and maintain health and mitigate the burdens of illness, injury and aging,
including appropriate prescriptions for controlled substances when indicated; and that individual
patient adverse effects are minimized while concurrently reducing risks to the public health.
This education has been approved by the Division of Occupational and Professional Licensing
for Physicians, Nurses, Physician Assistants, Dentists, and Podiatrists, and satisfies the above
requirement.
The UMA Foundation is accredited by the Utah Medical Association to provide continuing
medical education for physicians. The UMA Foundation designates this internet enduring
material activity for a maximum of 3.5 AMA PRA Category 1 Credits™. Physicians should claim
only the credit commensurate with the extent of their participation in the activity.
Exam Information
In order to be awarded participation or credit for this course, you must complete the online post-
exams for each of the six modules and the program evaluation. After reading the educational
modules, you must complete the exam for each module by going back to your online account.
After you’ve completed all six module exams and the evaluation, you may generate and print
your Certificate of Completion.
Contributors
The following people have contributed to the research and development of this updated course.
Page 2 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Educational Consultants
• Marc E. Babitz, MD – 4th Edition
• Mark Bair, MD – 3rd Edition
• Perry G. Fine, MD – 2nd Edition
• Marc E. Babitz, MD – 1st Edition and 2nd Edition
Opioid Prescribing Guidelines and Education Project Administrators – 2nd Edition, 2017
Anna Fondario, MPH
Epidemiology Manager, Violence and Injury Prevention Program
Utah Department of Health
Marcelle Smith, MPC
Senior Technical Writer and Editor
Education Project Manager, Utah Medical Association
Opioid Prescribing Guidelines Advisory Committee – 2nd Edition, 2017
Marc E. Babitz, M.D.
Deputy Director, Utah Department of Health
Medical Director, Health Clinics of Utah
Family Physician
Kim Bateman, MD
Chairman of the Board, HealthInsight
Family Practice
David A. Cook, M.D.
Board Certified in Orthopaedic Surgery
Quality Director, Tanner Clinic
Member, Utah State Physicians Licensing Board
Perry G. Fine, MD
Professor of Anesthesiology
Department of Anesthesiology, Pain Management and Research Center
School of Medicine, University of Utah
Mark C. Foote, MD
Psychiatry
William L. Hamilton, MD, MBA
Medical Director Administrative Services, Central Region, Intermountain Healthcare
Past President, Utah Medical Association
Page 3 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
B. Zane Horowitz, MD, FACMT
Medical Director, Utah Poison Control Center
University of Utah College of Pharmacy
Mitchell Jones
Assistant Utah Attorney General
Rebecca King, LCSW
Program Administrator - Women, Youth and Families
Utah State Division of Substance Abuse & Mental Health
Larry Marx, MPA
Bureau Manager, Utah Division of Occupational and Professional Licensing
Michelle S. McOmber, MBA, CAE
Chief Executive Officer, Utah Medical Association
Brian Oliver MD
Utah Emergency Physicians
Robert T. Rolfs, MD, MPH
Former Deputy Director, Utah Department of Health
Internal Medicine
Brian Shiozawa, MD
Utah State Senator
Emergency Medicine
Raymond Ward, MD
Utah State Representative
Family Practice and Urgent Care
Faculty – 1st Edition, 2014
• Cris Cowley, MD
• Brad D. Hare, MD
• Kurt T. Hegmann, MD
• Timothy S. Houden, MD
• Stephen Nelson, MD
• Kenneth Schaecher, MD
Expert Content Consultants – 1st Edition, 2014
• Mary Lou Emerson, Utah Substance Abuse Advisory Council
• Anna Fondario, Violence & Injury Prevention Program, Utah Department of Health
• Penny Kaye Jensen, American Association of Nurse Practitioners
• Noël Taxin, Utah Division of Occupational and Professional Licensing
Page 4 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
REMS Project Staff – 1st Edition, 2014
• Marcelle Smith, Utah Medical Association Foundation REMS Project Manager,
Technical Writer, Senior Editor
• Mandy Anger, Assistant Technical Writer
• Jackie Lehman, Utah Medical Association Education and Accreditation Manager
• Michelle S. McOmber, Utah Medical Association CEO
Financial Contributor
This publication was partially supported by the Grant or Cooperative Agreement Number, 6 NU17CE92733-02-01, funded by the Centers for Disease Control and Prevention and partially supported by the Utah Department of Health Drug Overdose Prevention Initiatives funded by the 2016 Utah State Legislature. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention, the Department of Health and Human Services, or the 2016 Utah State Legislature.
Disclosures
Those in control of content have disclosed they have no financial relationships with any
commercial entity producing health-care related products and/or services relevant to the content
of this activity.
Copyright 2021 The Utah Medical Association Foundation All rights reserved.
Disclaimers
No copyright is claimed in text and data from government and other sources quoted within this
work. Submit requests for permission to copy material to The Utah Medical Association
Foundation.
The Utah Medical Association Foundation provides this educational program to help prescribers
of controlled substances in Utah. Prescribers must be informed by the totality of their training
and experience along with the particular circumstances of the individual patient when deciding to
follow any particular course of action. Accordingly, the Utah Medical Association Foundation
disclaims responsibility for any injury or damage resulting from actions taken by prescribers
after taking this training.
If you have questions or comments concerning this course, you may contact the Utah Medical
Association office by email, [email protected]. UMA will refer medical or clinical-related
questions to the appropriate faculty member. If you need administrative assistance, you may call
the Utah Medical Association during normal business hours at (801) 747-3500 x-251.

Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Controlled Substances: Education for the Prescriber
Presented by the Utah Medical Association Foundation –
“Extending the Reach of the Healer’s Hand.”
MODULE 1
Module 1, Understanding the Scope of the Problem
Learning Objectives
After completing this module, you should be able to
1. Describe the current climate of controlled substance use and how it has caused national
and state concern.
2. Review the scope of the current problem in Utah, particularly the rise in overdose deaths.
3. Define “prescriber responsibilities” impacting the solution to this problem.
Understanding the Scope of the Problem
The authority to prescribe drugs comes with the serious responsibility to do so as effectively and
safely as possible. Healthcare professionals have a duty to balance two fundamental ethical
principles: nonmaleficence (doing no harm) and beneficence (doing good). In practical terms,
this means that prescribers need to understand the clinical pharmacology of the drugs determine
to be indicated for a specific indication, and then prescribe them as safely and effectively as
possible. To do so requires conscientiously weighing intended, predicted, and desirable
therapeutic effects against unintended adverse effects, all pursuant to the specific
medical/surgical, psychological and social circumstances of each individual patient. Drug-drug
interactions and strict adherence to using medication as directed – given the risks of misuse and
potential substance abuse or diversion – are especially challenging when prescribing controlled
substances.
The conditions for which controlled substances are indicated are highly prevalent in our society,
including pain, mood, sleep and behavioral disorders. Controlled substances, including opioid
analgesics and other pain-relieving drugs, sedative hypnotics and anxiolytics, and
psychostimulants pose particular challenges, because they can cause physical and psychological
dependence. These drugs cause mood-altering effects that pose risks of recreational use and
substance abuse that can lead to addiction. In addition, these drugs have serious toxicity risks
either due to accidental overdose or due to their additive and synergistic effects on respiratory
depression when the drugs are combined.
With the rise in controlled substance prescribing, statistics have shown an increase in abuse of
controlled substance medications, emergency department visits for adverse drug effects, and
unintended drug overdose deaths. Unintentional overdose is a leading cause of death and a costly
drain on emergency departments in non-fatal cases.
Page 6 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
With the rise in controlled substance prescribing, statistics have shown an increase in abuse of
controlled substance medications, emergency department visits for adverse drug effects, and
unintended drug overdose deaths. Unintentional overdose is a leading cause of death and a costly
drain on emergency departments in non-fatal cases.
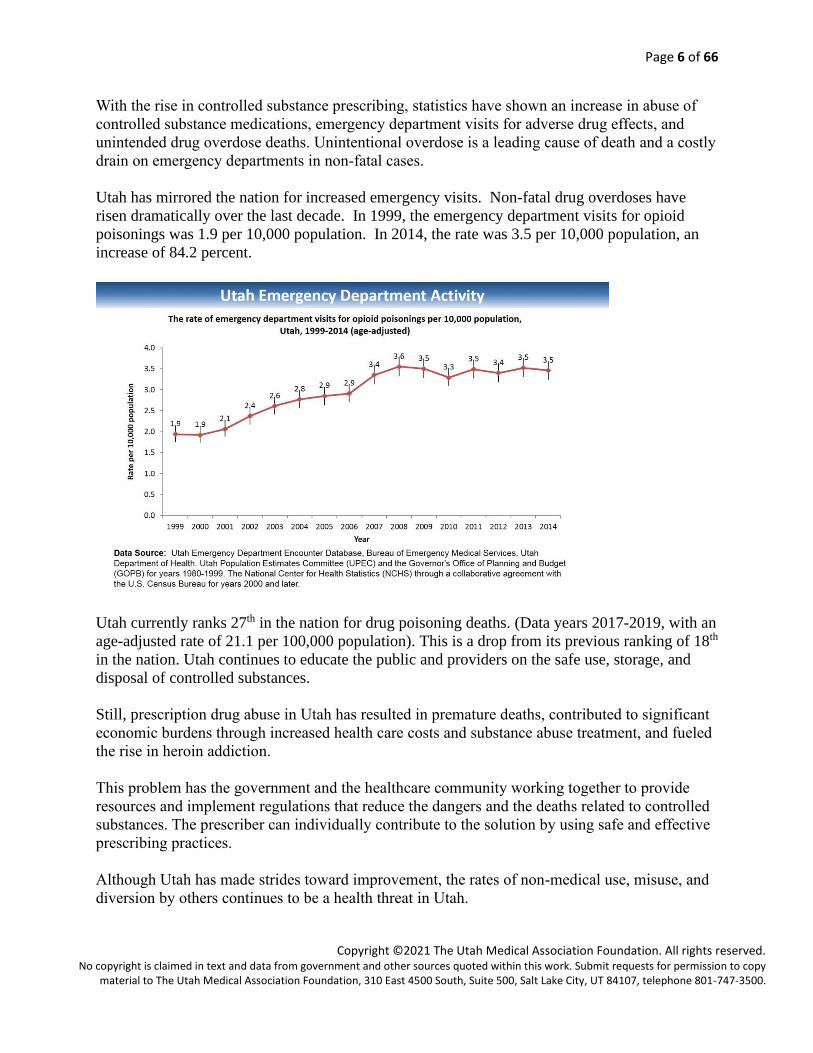
Utah has mirrored the nation for increased emergency visits. Non-fatal drug overdoses have
risen dramatically over the last decade. In 1999, the emergency department visits for opioid
poisonings was 1.9 per 10,000 population. In 2014, the rate was 3.5 per 10,000 population, an
increase of 84.2 percent.
Utah currently ranks 27th in the nation for drug poisoning deaths. (Data years 2017-2019, with an
age-adjusted rate of 21.1 per 100,000 population). This is a drop from its previous ranking of 18th
in the nation. Utah continues to educate the public and providers on the safe use, storage, and
disposal of controlled substances.
Still, prescription drug abuse in Utah has resulted in premature deaths, contributed to significant
economic burdens through increased health care costs and substance abuse treatment, and fueled
the rise in heroin addiction.
This problem has the government and the healthcare community working together to provide
resources and implement regulations that reduce the dangers and the deaths related to controlled
substances. The prescriber can individually contribute to the solution by using safe and effective
prescribing practices.
Although Utah has made strides toward improvement, the rates of non-medical use, misuse, and
diversion by others continues to be a health threat in Utah.
Page 7 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
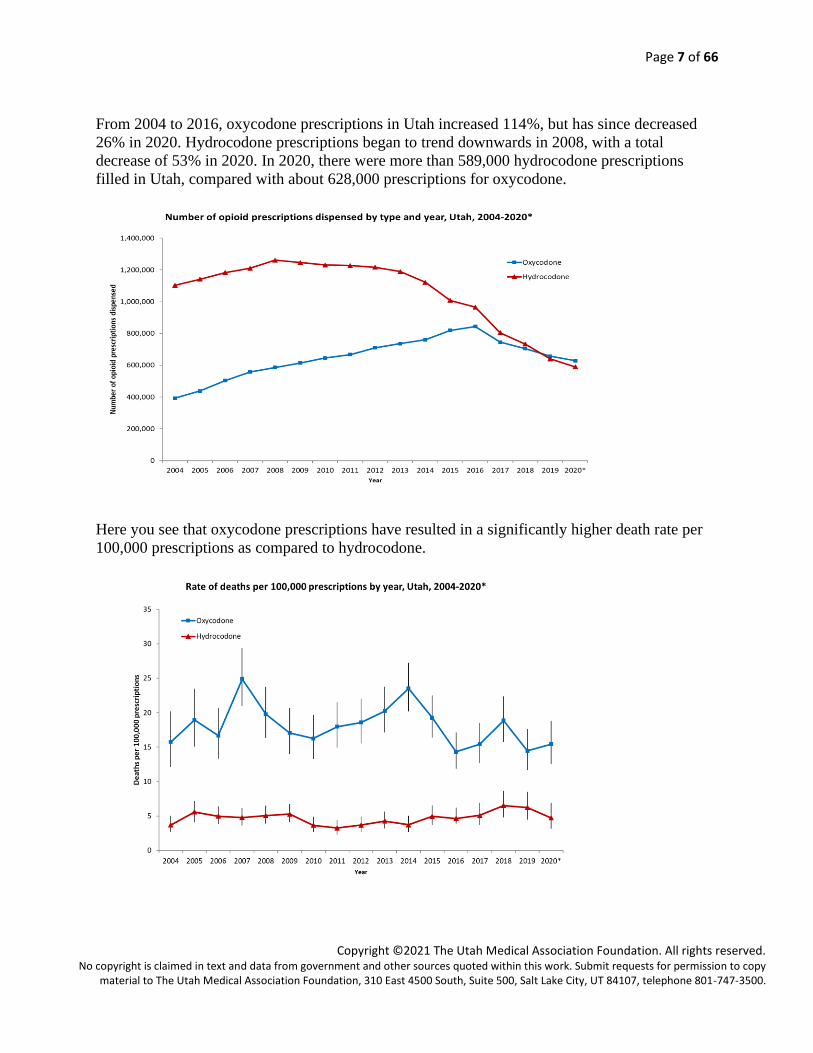
From 2004 to 2016, oxycodone prescriptions in Utah increased 114%, but has since decreased
26% in 2020. Hydrocodone prescriptions began to trend downwards in 2008, with a total
decrease of 53% in 2020. In 2020, there were more than 589,000 hydrocodone prescriptions
filled in Utah, compared with about 628,000 prescriptions for oxycodone.
Here you see that oxycodone prescriptions have resulted in a significantly higher death rate per
100,000 prescriptions as compared to hydrocodone.
Page 8 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
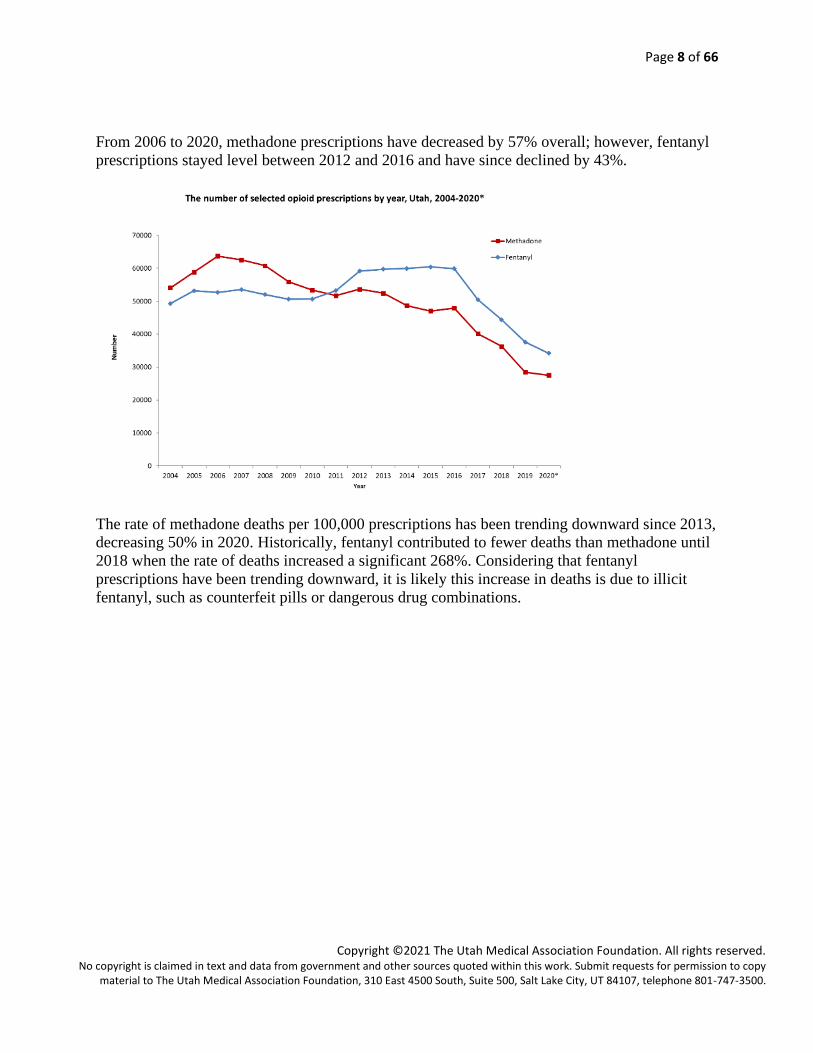
From 2006 to 2020, methadone prescriptions have decreased by 57% overall; however, fentanyl
prescriptions stayed level between 2012 and 2016 and have since declined by 43%.
The rate of methadone deaths per 100,000 prescriptions has been trending downward since 2013,
decreasing 50% in 2020. Historically, fentanyl contributed to fewer deaths than methadone until
2018 when the rate of deaths increased a significant 268%. Considering that fentanyl
prescriptions have been trending downward, it is likely this increase in deaths is due to illicit
fentanyl, such as counterfeit pills or dangerous drug combinations.

Page 9 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
The number of benzodiazepine deaths has consistently increased every year between 2000 and
2018, representing an increase of 66% from 2000 to 2018; although a decrease of 31% has been
seen between 2018 and 2020.
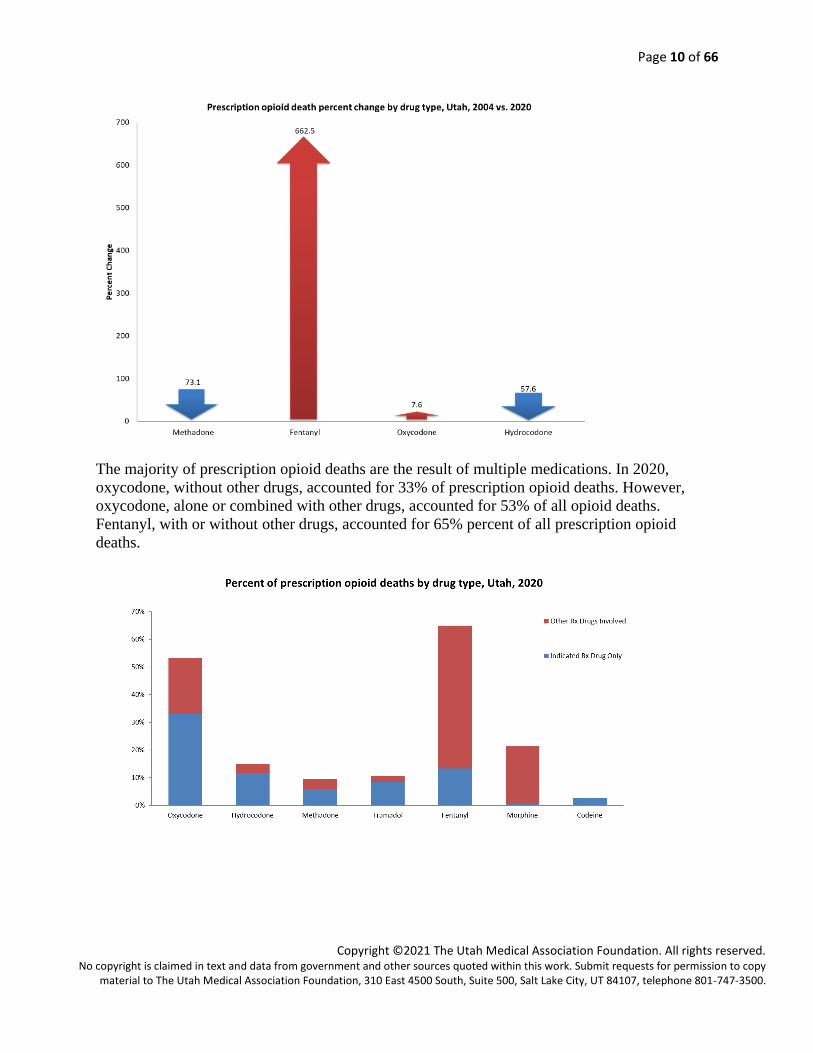
Between 2004 and 2020, fentanyl related deaths had the highest percent increase compared to
other selected opioids (663%).
Page 10 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
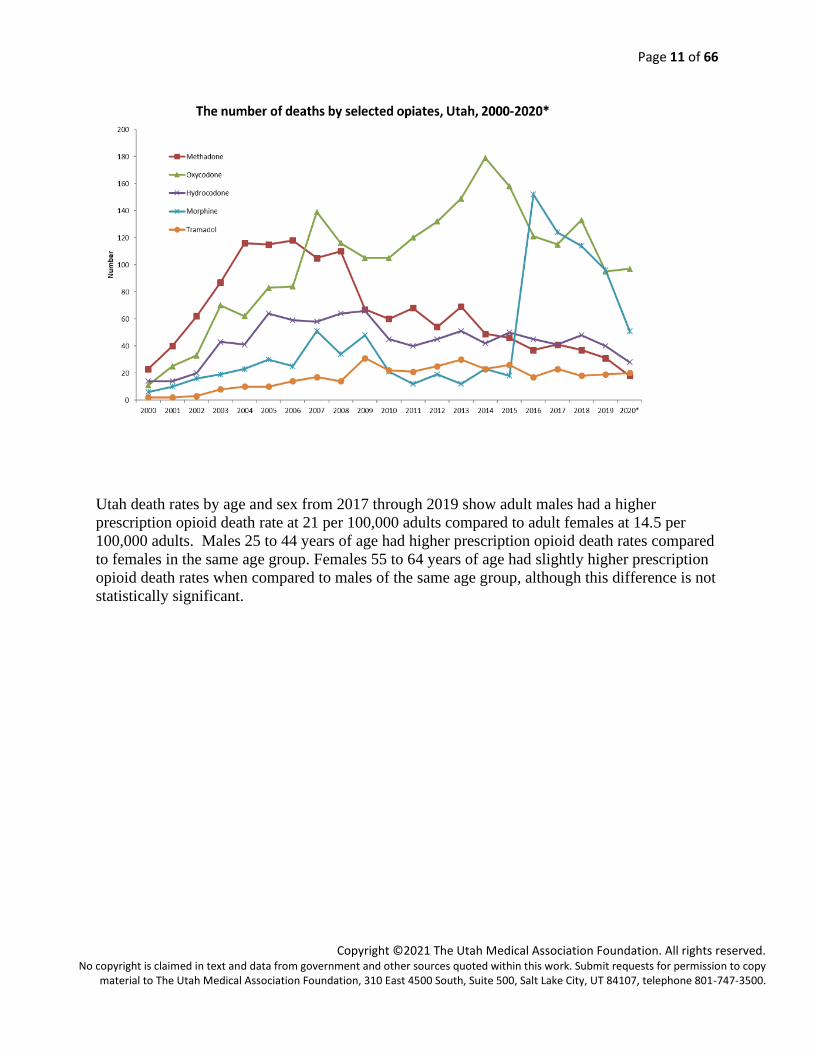
The majority of prescription opioid deaths are the result of multiple medications. In 2020,
oxycodone, without other drugs, accounted for 33% of prescription opioid deaths. However,
oxycodone, alone or combined with other drugs, accounted for 53% of all opioid deaths.
Fentanyl, with or without other drugs, accounted for 65% percent of all prescription opioid
deaths.
Page 11 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
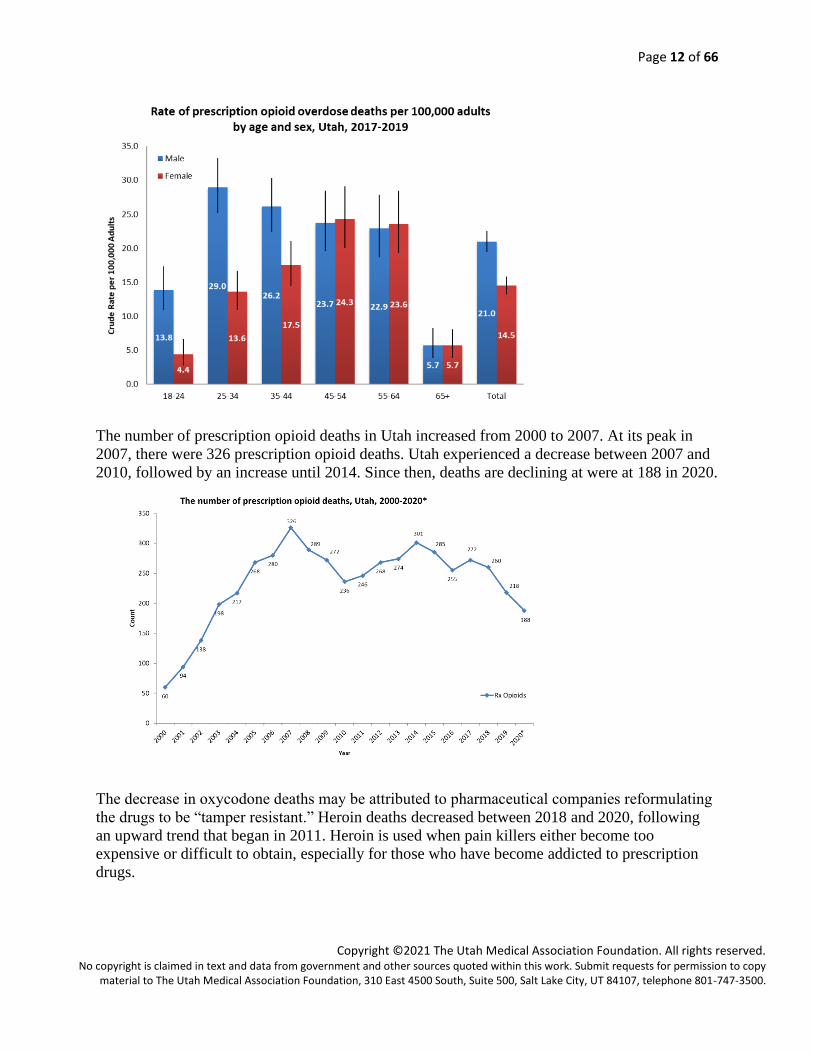
Utah death rates by age and sex from 2017 through 2019 show adult males had a higher
prescription opioid death rate at 21 per 100,000 adults compared to adult females at 14.5 per
100,000 adults. Males 25 to 44 years of age had higher prescription opioid death rates compared
to females in the same age group. Females 55 to 64 years of age had slightly higher prescription
opioid death rates when compared to males of the same age group, although this difference is not
statistically significant.
Page 12 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
The number of prescription opioid deaths in Utah increased from 2000 to 2007. At its peak in
2007, there were 326 prescription opioid deaths. Utah experienced a decrease between 2007 and
2010, followed by an increase until 2014. Since then, deaths are declining at were at 188 in 2020.
The decrease in oxycodone deaths may be attributed to pharmaceutical companies reformulating
the drugs to be “tamper resistant.” Heroin deaths decreased between 2018 and 2020, following
an upward trend that began in 2011. Heroin is used when pain killers either become too
expensive or difficult to obtain, especially for those who have become addicted to prescription
drugs.
Page 13 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
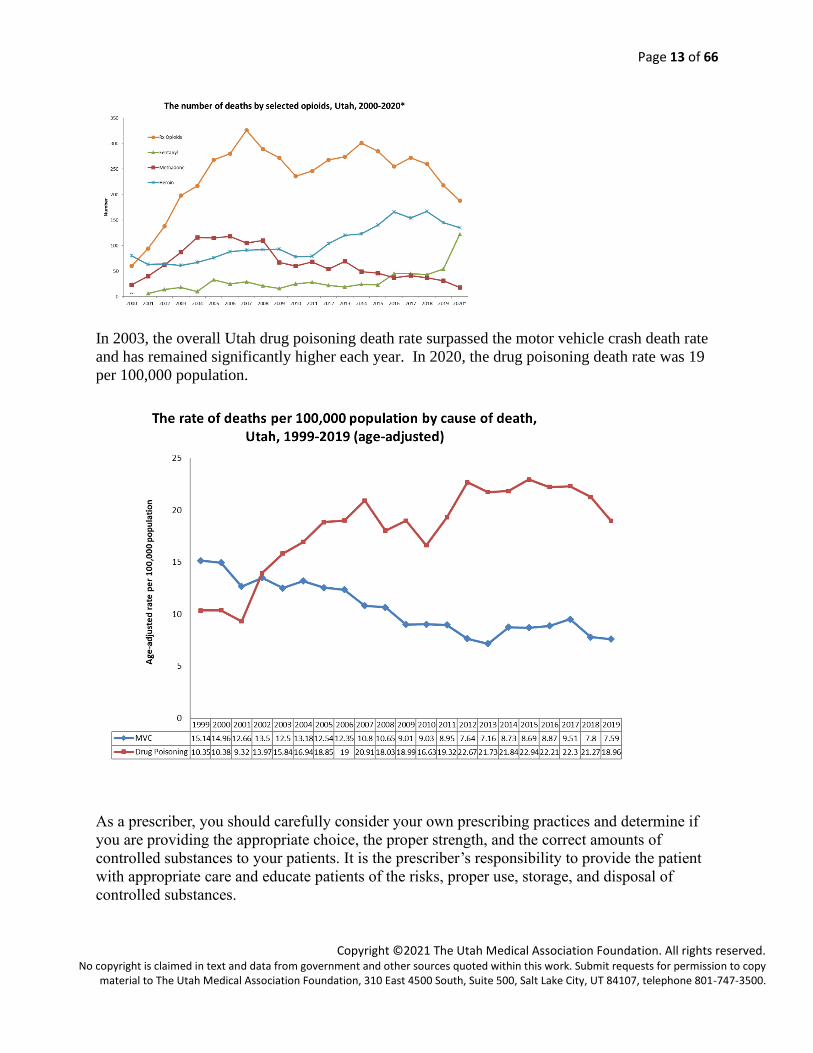
In 2003, the overall Utah drug poisoning death rate surpassed the motor vehicle crash death rate
and has remained significantly higher each year. In 2020, the drug poisoning death rate was 19
per 100,000 population.
As a prescriber, you should carefully consider your own prescribing practices and determine if
you are providing the appropriate choice, the proper strength, and the correct amounts of
controlled substances to your patients. It is the prescriber’s responsibility to provide the patient
with appropriate care and educate patients of the risks, proper use, storage, and disposal of
controlled substances.
**

Page 14 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
These resources have contributed to the educational content in this module:
Utah Department of Health, Violence and injury Prevention Program, provided the data in this
module. References indicated on each graph.
Advance to Module 2 on the next page.
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Controlled Substances: Education for the Prescriber
Presented by the Utah Medical Association Foundation –
“Extending the Reach of the Healer’s Hand.”
MODULE 2
Pharmacology and the Principles of Prescribing
Learning Objectives
After completing this module, you should be able to
1. Identify relative comparative potencies of controlled substances within a drug class.
2. Know indications for prescribing opioid analgesics.
3. Prescribe non-opioid analgesics, including acetaminophen and NSAIDs, based on
maximum safe dosages.
4. List the unique characteristics of methadone that make it an exceptionally high risk
opioid.
Pharmacology and the Principles of Prescribing
Because of potential harms associated with controlled substances that increase with high dosage
formulations (e.g. extended- release opioids), prescribers should reserve all controlled substances
for patients for whom alternative treatment options (e.g. non-opioid analgesics or immediate-
release opioids) are ineffective, not tolerated, or would otherwise be inadequate to provide
sufficient management of pain.
1. Because controlled substances for medical use have abuse liability, prescribers should
a. Only prescribe for specific, well-defined indications.
b. Prescribe the smallest therapeutic dose for the shortest duration required.
c. Counsel patients and caregivers on the safe use, storage, and disposal of medications.
d. Counsel patients and caregivers on the signs and symptoms of abuse and prescribers must
monitor behaviors based on patient risk.
2. Because all controlled substances have medical risks, prescribers should
a. Review the pharmacology of controlled substances prescribed to predict and minimize
potential drug-drug interactions and drug-disease (comorbidity) interactions.
b. Know the pharmacokinetics of the prescribed controlled substances, including:
- Absorption: The formulation of the drug (parenteral, oral, transmucosal, transdermal,
etc.) alters the time to onset of action, peak effects, and duration of effects. Know the
effects of eating versus fasting, body temperature, activity, and other environmental
and behavioral variables on drug absorption.
- Distribution: Know that lipophilic drugs will tend to accumulate in fat, leading to
potentially problematic drug effects. Know the usual half-life of prescribed drugs to
instruct patients appropriately on dose schedules.
Page 16 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
- Metabolism: Know how the body will change the drug once it is in the blood stream,
and whether metabolites are active or inactive, whether or not active metabolites will
accumulate, and whether or not other drugs taken may alter metabolism (e.g., induce
or inhibit metabolism—especially via effects on the hepatic p450 microsomal enzyme
system). Know whether alterations in renal hepatic function will necessitate
modifications in dose and dose schedule for drugs that are metabolized via the liver.
- Elimination: Know how drugs prescribed are cleared from the body. Be aware of
alterations in kidney or liver function that might reduce clearance of drugs or their
active metabolites, and modify dose and dosing schedule.
3. Because some controlled substances are combined with other drugs (e.g. opioids plus
acetaminophen or NSAIDs), prescribers must ensure that the safe maximum doses of co-
analgesics are not exceeded.
Acetaminophen Limitations
The FDA has issued a warning that the safe dose of acetaminophen shouldn’t exceed 3 grams per
24 hours, which is comparable to nine 325mg tablets. Overuse could cause toxicity to the liver
and potentially death. The FDA recommends using caution in prescribing acetaminophen when a
patient drinks 3 or more alcoholic beverages per day due to the increased risk of liver failure.
If acetaminophen is taken with other products, such as cold remedies, then the safe dose of the
prescribed pain medication containing acetaminophen would be even less than the limited
dosage.
Among approved controlled substances, opioids are available in the widest variety of
formulations and each of the many opioids currently available has its own unique
pharmacokinetic profile and relative potency. It is incumbent upon prescribers to review and
know the nuances of the prescribed drugs to minimize toxicity. Prescribers can seek FDA-
approved prescribing information on specific drugs by going to their website. Also, the
prescriber should encourage patients and caregivers to read the relevant Medication Guide once
the prescription is picked up from the pharmacy.
Opioid Analgesics
Indications: Pain severe enough to warrant opioids when pain is ineffectively controlled with
non-pharmacological, non-opioid analgesics alone, or when non-opioids are contraindicated.
Contraindications:
• Allergy history of sensitivity or dysphoric reactions
• Concurrent use of agonist-antagonist drugs (e.g., pentazocine, butorphanol, nalbuphine)
• Meperidine should not be used in patients with renal insufficiency (primary or age-related
reduction in GFR) and history of seizures
Precautions:
• Reduction in Bowel Motility: Anticipate, prevent, and treat as needed.
Page 17 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Substance Use Disorder: Patients with risks of misuse/abuse and those with substance
use disorders require additional monitoring and consideration of co-management with
substance use disorder specialists.
• Respiratory Depression: Medical conditions that increase risk of respiratory depression
(e.g., pulmonary disease, sleep apnea, and concurrent use of medically indicated CNS
depressant drugs)
Safe storage and disposal: Patients and caregivers should be advised to keep all opioid
analgesics and other controlled substances under “lock and key,” except for an immediately
needed dose of breakthrough pain medication or the next dose of a scheduled medication. Proper
disposal of excess or expired medications prevents accidental usage, especially by children or by
diversion. The preferred method for disposing of unused controlled substances is dropping the
medication off at a collection site. If a site is unavailable, most tablets, capsules, and liquids
should be mixed with dirt, used coffee grounds, or cat litter or should be dissolved in water and
placed in usual trash receptacles. Opioid patches should be folded over on themselves and
flushed down the toilet.
Driving and functional safety instructions:
There are inadequate data from which to make definitive recommendation from available
studies. The circumstances of each patient need to be evaluated on their own merits, including
disease-related and drug-related impairments that would make driving or other activities
dangerous for the patient or others. At the very least, patients should be counseled against
driving during dose titration and stabilization of opioids and other CNS-depressant drugs.
Dose conversions for opioid rotation: Changing from one opioid to another, or one route to
another, incurs risks of toxicity due to incomplete cross tolerance and requires calculation based
upon reference to a standard conversion table, a safety step reduction a patient-specific step
consideration, and ongoing careful monitoring for toxicity.
Indications for opioid rotation or exchange:
• Occurrence of intolerable adverse effects during dose titration
• Poor analgesic efficacy despite aggressive dose titration
• Problematic drug–drug interactions
• Preferences or need for a different route of administration
• Change in clinical status (e.g., concern about drug abuse or the development of
malabsorption syndrome) or clinical setting that suggests benefit from an opioid with
different pharmacokinetic properties
• Financial or drug availability considerations
Page 18 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
ER/LA opioid analgesics containing buprenorphine, fentanyl, hydrocodone, hydromorphone,
morphine/codeine, oxycodone, oxymorphone, methadone levorphanol , tramadol, and tapentadol,
are indicated for the management of pain severe enough to require daily, around-the-clock, long-
term opioid treatment and for which alternative treatment options are inadequate. ER/LA opioid
analgesics are not indicated for acute pain.
Buprenorphine
• Partial mu agonist available in transdermal patch and buccal film formulations. Indicated
for patients with severe pain for whom other opioids are ineffective, poorly tolerated, or
other delivery routes are not feasible
• Buprenorphine transdermal patch: 5-, 10-, 20-mcg/hr transdermal patch dose strengths.
- Initial dosing: 5-mcg/hr patch, applied once weekly; titrate up as necessary; or if
previously on opioid (up to 80 mg oral morphine equivalent/day), may start on 5- to 10-
mcg/hr patch once weekly (medication for breakthrough pain should also be provided).
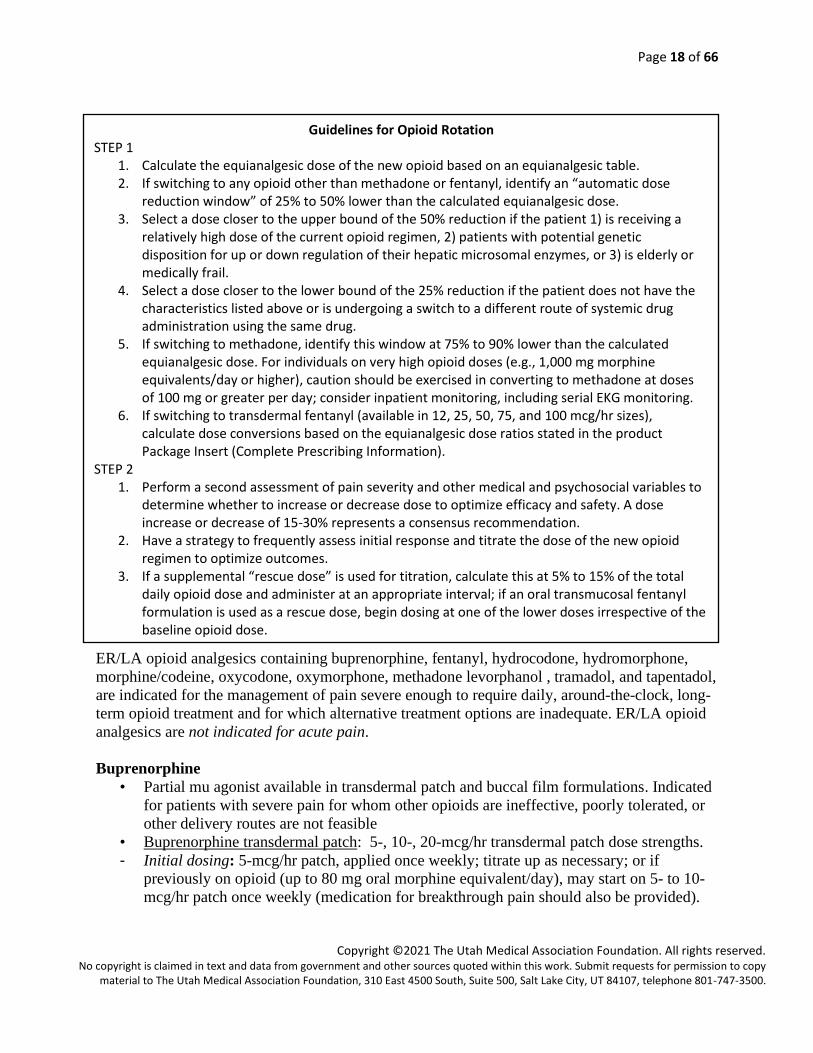
Guidelines for Opioid Rotation STEP 1
1. Calculate the equianalgesic dose of the new opioid based on an equianalgesic table. 2. If switching to any opioid other than methadone or fentanyl, identify an “automatic dose
reduction window” of 25% to 50% lower than the calculated equianalgesic dose. 3. Select a dose closer to the upper bound of the 50% reduction if the patient 1) is receiving a
relatively high dose of the current opioid regimen, 2) patients with potential genetic disposition for up or down regulation of their hepatic microsomal enzymes, or 3) is elderly or medically frail.
4. Select a dose closer to the lower bound of the 25% reduction if the patient does not have the characteristics listed above or is undergoing a switch to a different route of systemic drug administration using the same drug.
5. If switching to methadone, identify this window at 75% to 90% lower than the calculated equianalgesic dose. For individuals on very high opioid doses (e.g., 1,000 mg morphine equivalents/day or higher), caution should be exercised in converting to methadone at doses of 100 mg or greater per day; consider inpatient monitoring, including serial EKG monitoring.
6. If switching to transdermal fentanyl (available in 12, 25, 50, 75, and 100 mcg/hr sizes), calculate dose conversions based on the equianalgesic dose ratios stated in the product Package Insert (Complete Prescribing Information).
STEP 2 1. Perform a second assessment of pain severity and other medical and psychosocial variables to
determine whether to increase or decrease dose to optimize efficacy and safety. A dose increase or decrease of 15-30% represents a consensus recommendation.
2. Have a strategy to frequently assess initial response and titrate the dose of the new opioid regimen to optimize outcomes.
3. If a supplemental “rescue dose” is used for titration, calculate this at 5% to 15% of the total daily opioid dose and administer at an appropriate interval; if an oral transmucosal fentanyl formulation is used as a rescue dose, begin dosing at one of the lower doses irrespective of the baseline opioid dose.
Page 19 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
- Dose adjustments: generally recommended after 7 days, and not more frequently than
after 3 days.
- Doses 40 mcg/hr or higher may be associated with QT prolongation.
- Buprenorphine patch is worn for 7 days; has a well-defined ceiling effect for respiratory
depression and respiratory rate that rarely drops below 10 breaths per minute (50% of
baseline).
• Buprenorphine buccal film: Buccal film available in 75 mcg, 150 mcg, 300 mcg, 450
mcg, 600 mcg, 750 mcg, and 900 mcg dosage strengths.
• For opioid-naïve patients, initiate therapy with 75 mcg once daily or every 12 hours, as
tolerated, for at least 4 days before increasing dose to 150 mcg every 12 hours.
• Conversion from other opioids to buprenorphine buccal film: Taper current daily opioid
dose to 30 mg oral morphine sulfate equivalents (MSE) or less prior to initiating therapy
with buprenorphine buccal film.
• For patients taking less than 30 mg oral MSE, initiate therapy with 75 mcg once daily or
every 12 hours.
• For patients taking between 30 mg and 89 mg oral MSE, initiate therapy with 150 mcg
buprenorphine buccal film every 12 hours following analgesic taper.
• For patients taking between 90 mg and 160 mg oral MSE, initiate therapy with 300 mcg
buprenorphine buccal film every 12 hours following analgesic taper.
• For patients taking greater than 160 mg oral MSE, consider alternate analgesic.
• Buprenorphine buccal film doses of 600 mcg, 750 mcg, and 900 mcg are only for use
following titration from lower doses of buprenorphine buccal film.
• Do not abruptly discontinue buprenorphine buccal film in a physically dependent patient.
• For patients with severe hepatic impairment, reduce the starting and incremental dose by
half that of patients with normal liver function.
• For patients with oral mucositis, reduce the starting and incremental dose by half that of
patients without mucositis.
Codeine
Codeine is a prodrug of morphine, and its relative potency varies markedly to the extent in which
it is converted to its active metabolite according to individual genetic characteristics. This
property of codeine makes efficacy safety unpredictable.
Fentanyl
(e.g., Abstral, Actiz, Duragesic, Fentora, Ionsys, Lazanda, Onsolis, Subsys)
• Transdermal fentanyl (fentanyl patch): Opioid-naïve patients should be titrated to
effective analgesia using short-acting or immediate-release opioid analgesics; and then,
converted to transdermal fentanyl, based upon conversion tables provided in the product
prescribing information. See “opioid rotation” above for conversion from another opioid
to transdermal fentanyl or from transdermal fentanyl to another opioid formulation.
• The lowest dose of transdermal fentanyl is 12 mcg/hr. This may be suitable for low-
weight and frail elderly patients. It may also be an alternative delivery route in those
patients on relatively low-intermediate doses of opioids (30-60 mg oral morphine
equivalents per 24 hours) but who can no longer use oral agents.
Page 20 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Time to peak and steady-state blood levels for patients starting the patch is usually 12 to
24 hours. Make sure other rapid-onset dosage forms of an opioid analgesic are available
during this time period and later for breakthrough pain.
• Although the currently available fentanyl patch is formulated for 72-hour use, end-of-
dose failure often occurs as early as 48 hours. It is important to closely monitor the
efficacy, duration of effect, breakthrough pain episodes and medication use, and adverse
effects during the first several days of use and during periods of advancing disease with
increasing pain until a stable pattern of effectiveness is reached.
Oral transmucosal fentanyl for cancer breakthrough pain: (formulations: lozenge on a
stick, buccal patch, buccal tablet, sublingual spray, nasal spray) For adults, start with the
lowest dose of the preferred formulation for breakthrough pain, and monitor efficacy,
advancing to higher-dose units as needed. Onset of pain relief can usually be expected within
10 to 15 minutes after beginning use. Any remaining partial units should be disposed of
safely by following instructions in complete prescribing information; patients and caregivers
should be counseled about safe storage and disposal and provided with written information.
Hydrocodone
(e.g., Loratab, Lorcet, Norco, Vicodin)
This mu opioid analgesic has recently been rescheduled from a C-III to a C-II drug controlled
substance, making it no longer available for prescription by phone nor refillable without a new
prescription.
Hydromorphone
(e.g., Dilaudid)
• Hydromorphone is five to eight times more potent than morphine, permitting analgesic
equivalence at lower doses and smaller volumes.
• Hydromorphone can be administered through oral, parenteral (SQ, IM, IV), rectal, or
intraspinal (epidural and intrathecal) routes.
• Hydromorphone’s relatively short half-life of elimination (2 to 3 hours) facilitates dose
titration. Onset of action occurs within 15 minutes after parenteral administration and
within 30 minutes after oral or rectal administration.
Instructions to Patients when Fentanyl is Prescribed 1. Place patch on the upper body in a clean, dry, hairless area. 2. Check daily to make sure patch is not peeling off or has fallen off. If this is
consistently problematic, an occlusive dressing should be applied. 3. Avoid heat application over the patch as this will accelerate absorption of
medication into body and pose risk of overdose. 2. Choose a different site when placing a new patch, then remove the old patch. 3. Remove the old patch(es) and fold sticky surfaces together, then flush down the
toilet. 4. Wash hands after handling patches. 5. All unused patches should be removed from wrappers, folded in half with sticky
surfaces together, and flushed down the toilet.
Page 21 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Since hydromorphone is highly soluble in water (up to a maximum concentration of
about 300 mg/ml), it is particularly suitable for SQ administration when clinical
conditions warrant continuous parenteral infusion (e.g., cancer care; terminal care),
including continuous subcutaneous infusion (CSCI) and post-operative intravenous
patient-controlled analgesia (PCA).
• Hydromorphone is hydrophilic and extensively distributes in the cerebral spinal fluid
(CSF) on epidural administration.
• A high-potency preparation (10 mg/ml) is commercially available for opioid-tolerant
patients. This preparation is particularly useful for CSCI in patients where small volumes
are necessary.
• Side effects associated with hydromorphone are qualitatively similar to those associated
with opioids in general and most often include constipation, nausea, and sedation.
Hydromorphone may be preferred in patients with decreased renal clearance in order to
prevent toxic metabolite accumulation associated with high dose morphine.
Morphine
• One of the lowest cost immediate-release and controlled-release agents due to several
generic formulations.
• Some patients cannot tolerate morphine due to itching, headache, dysphoria, or other
adverse effects.
• The metabolites of morphine (morphine-3-glucuronide and morphine-6-glucuronide) may
contribute to sedation, myoclonus, and psychotomimetic effects.
• Convert to an equianalgesic dose of a different opioid if adverse effects exceed benefit.
• Anticipate adverse effects, especially constipation, nausea, and sedation, and prevent or
treat appropriately.
• Oral morphine solution can be swallowed, or small volumes (1/4 to 1 ml = 5 to 20 mg) of
a proprietarily available concentrated solution (20 mg/ml) can be placed under the
tongue, recognizing that most of the effect is obtained by enteral absorption after
swallowing.
• Morphine’s bitter taste may be prohibitive in unflavored forms. “Immediate-release”
tablets are not recommended for patients who cannot swallow.
Oxycodone
(e.g., Oxycontin, Percocet, Roxicodone, Endocet)
• For reasons that have not been well-defined, oxycodone tends to be a preferred drug of
abuse. However, a preference for oxycodone over other oral opioids by patients who have
had prior clinical experience may also reflect gene splice variants in mu opioid receptors
that infer greater analgesic efficacy for oxycodone and sometimes other opioids.
• Prescribers must exercise caution in jumping to conclusions, because this patient-specific
preference may be confused with “drug seeking”. Differentiate aberrant behavior from
variations in drug-specific efficacy due to genetic polymorphism by observing
problematic drug-use behaviors and assessing other substance abuse risk factors.
Page 22 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Oxymorphone
(e.g., Opana)
• Oxymorphone (OM) is the active metabolite of oxycodone (OC).
• Oral oxymorphone is about 3 times as potent as oral morphine; i.e. in patients whose
opioid receptor systems are responsive to both drugs, an opioid naive patient taking 3 mg
of oral morphine will obtain the same pain relief from 1 mg of oral oxymorphone.
• A potential advantage of oxymorphone is its absence of active metabolites and drug-drug
interactions due to glucuronide metabolism (conjugation) rather than CYP 450
metabolism.
• The equianalgesic dose ratio between oxymorphone extended-release and oxycodone
controlled-release in patients with cancer pain was OM:OC 1:2.
• The occurrence of side effects is qualitatively and quantitatively similar for the two drugs
at equianalgesic doses.
• Available in immediate-release, extended-release, and rectal suppository formulations.
Tapentadol
(e.g., Nucynta)
• Tapentadol is a dual-mechanism analgesic, with both mu opioid agonist effects and
norepinephrine reuptake inhibition that is believed to amplify the analgesic potency; it is
indicated for moderate to severe acute and chronic pain in adults, currently available in
“immediate-release” tablets (50-, 75-, 100-mg dosage strengths) and “extended-release”
tablets.
• The initial immediate-release dose is 50 to 100 mg q4hr (although a second dose can be
given 1 hour after the initial dose) with a maximum dose of 600 mg/24hr.
• Associated with significantly lower incidences of nausea and/or vomiting and
constipation; and a significantly lower rate of treatment discontinuation and withdrawal
symptoms compared with oxycodone.
• Renally cleared inactive metabolite after glucuronidation, making it relatively safer in
patients with renal insufficiency than opioids with active metabolites (e.g., morphine); no
significant interaction with liver microsomal enzymes, so minimal drug–drug
interactions.
Tramadol
(e.g., Ultram)
• Centrally acting analgesic.
• Binds weakly to the mu opioid receptor; inhibits the reuptake of serotonin and
norepinephrine; and promotes neuronal serotonin release.
• Maximum daily dose is 400mg/24hrs; in patients >75 years old, maximum dose is
300mg/24hrs.
• High-quality studies in patients with noncancer neuropathic pain confirm its efficacy in
treating these painful conditions.
• Adverse effects resemble those of opioids, and caution is advised when using tramadol
with selective serotonin reuptake inhibitor (SSRIs), monoamine oxidase inhibitors
(MAOIs), or tricyclic antidepressants (TCAs) given the potential for serotonin syndrome.
Page 23 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Available in immediate-release form as a single agent and in combination with
acetaminophen; also available in an extended-release preparation.
• Contraindications include risk of seizures in patients with lowered seizure threshold.
Methadone
• This drug is useful in selected patients as a long-acting analgesic due to its long
biological half-life, making dosing intervals (q8hr) relatively convenient.
• The potential for drug accumulation prior to achievement of steady-state blood levels
(four to six doses) puts patients at risk for over-sedation and respiratory depression. Close
monitoring for excessive sedation is required by an observant caregiver.
• Methadone is an option for maintenance therapy for opioid addicted patients; however,
the DEA requires special registration for prescribers to use for this purpose.
• Recent evidence suggests that even low doses of methadone may put patients at risk for
arrhythmias due to prolongation of the QT interval. Caution needs to be exercised in
patients with electrolyte abnormalities or cardiac conduction abnormalities, and when
escalating doses of the drug. Nonlinear dose equivalency of methadone requires close
attention to dosing recommendations and extensive experience. FDA approved
prescribing information suggests EKG evaluation pre-treatment in patients with cardiac
conditions and with higher dose therapy.
• An ECG screening should be performed on patients who will be receiving methadone.
Cardio vascular side effects include:
- QT interval prolongation
- Palpitations
- ECG abnormalities
- Torsade de pointes
- Ventricular Fibrillation
- Ventricular tachycardia
- Cardiac arrest
• Caution: Anti-depressants may prolong the QT interval and increase the risk of cardiac
death when taken with methadone
• According to the methadone packaging information, life-threatening QT prolongation
cases of QT interval prolongation and serious arrhythmia (torsades de pointes) have been
observed during treatment with methadone. These cases appear to be more commonly
associated with, but not limited to, higher dose treatment of >200 mg/day. The evidence
strongly suggests that methadone possesses the potential for adverse cardiac conduction
effects in some patients.
Sustained or Continuous-Release Oral Formulations
Chewing or crushing continuous-release formulations causes the substance to act like
IMMEDIATE RELEASE, potentially subjecting the patient to overdose.
Page 24 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
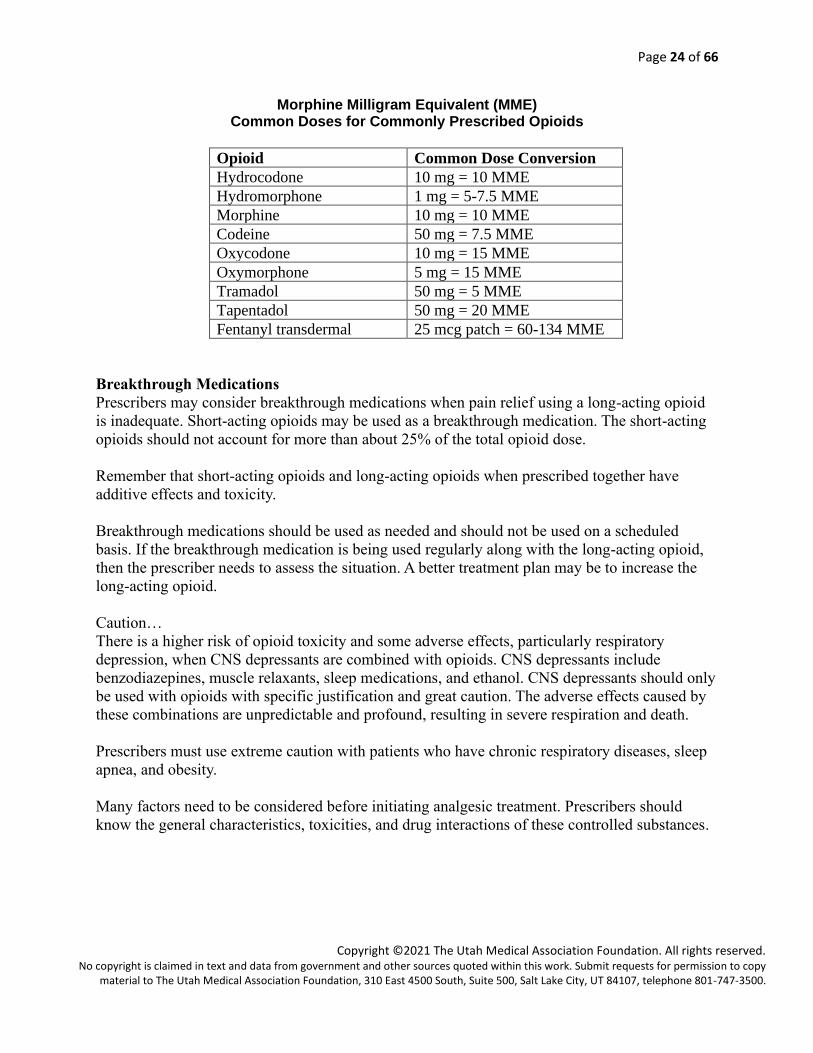
Morphine Milligram Equivalent (MME) Common Doses for Commonly Prescribed Opioids
Opioid Common Dose Conversion
Hydrocodone 10 mg = 10 MME
Hydromorphone 1 mg = 5-7.5 MME
Morphine 10 mg = 10 MME
Codeine 50 mg = 7.5 MME
Oxycodone 10 mg = 15 MME
Oxymorphone 5 mg = 15 MME
Tramadol 50 mg = 5 MME
Tapentadol 50 mg = 20 MME
Fentanyl transdermal 25 mcg patch = 60-134 MME
Breakthrough Medications
Prescribers may consider breakthrough medications when pain relief using a long-acting opioid
is inadequate. Short-acting opioids may be used as a breakthrough medication. The short-acting
opioids should not account for more than about 25% of the total opioid dose.
Remember that short-acting opioids and long-acting opioids when prescribed together have
additive effects and toxicity.
Breakthrough medications should be used as needed and should not be used on a scheduled
basis. If the breakthrough medication is being used regularly along with the long-acting opioid,
then the prescriber needs to assess the situation. A better treatment plan may be to increase the
long-acting opioid.
Caution…
There is a higher risk of opioid toxicity and some adverse effects, particularly respiratory
depression, when CNS depressants are combined with opioids. CNS depressants include
benzodiazepines, muscle relaxants, sleep medications, and ethanol. CNS depressants should only
be used with opioids with specific justification and great caution. The adverse effects caused by
these combinations are unpredictable and profound, resulting in severe respiration and death.
Prescribers must use extreme caution with patients who have chronic respiratory diseases, sleep
apnea, and obesity.
Many factors need to be considered before initiating analgesic treatment. Prescribers should
know the general characteristics, toxicities, and drug interactions of these controlled substances.
Page 25 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
These resources have contributed to the educational content in this module:
Fine PG, Mahajan G, McPherson ML: 2009. Long-acting and short-acting opioids: Appropriate
use in chronic pain management. Pain Med; 10 (S2): S1-10
Knotkova H, Fine PG, Portenoy RK: 2009. Opioid rotation: The science and limitations of the
equianalgesic dose table. J Pain Symptom Manage; 38 (3): 426-439
The Extended-Release and Long-Acting Opioid Analgesics Risk Evaluation and Mitigation
Strategy Program, http://www.er-la-opioidrems.com/IwgUI/rems/home.action
Advance to Module 3 on the next page.
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Controlled Substances: Education for the Prescriber
Presented by the Utah Medical Association Foundation –
“Extending the Reach of the Healer’s Hand.”
MODULE 3
Overview of Pain and Treating ACUTE Pain with Less Risk
Learning Objectives
After completing this module, you should be able to
1. Treat acute pain using the seven recommendations for treating acute pain.
2. Consider alternative treatments prior to prescribing controlled substances.
3. Explain Utah Code 58-37-6 (7)(f)(iii) on the quantity of opiates that can be issued for an
acute condition.
4. Recognize the reasons that may cause acute pain to advance to chronic pain and employ
approaches to reduce its advancement.
Overview of Pain
Pain can be defined as an unpleasant sensory and emotional experience. Pain is one of the most
common reason patients seek medical care. Pain is a highly personal experience modified and
amplified by past experience; immediate psychological, physical, and social context; future
expectations; cultural norms; and spiritual orientation. Pain often interferes with a patient’s basic
functions, activities, sleep, or social interaction, eroding the patient’s quality of life to any
meaningful extent. When pain is severe enough to interfere with usual activities or healing, pain
assessment and treatment plans should be placed as a high priority to restore patient’s optimal
health with minimal harm. Preventative approaches to pain management, rapid responses to calls
for help when pain is out of control, and timely re-evaluation and intervention are key
fundamental measures of quality health care.
A patient’s expectation for “no pain” may be unreasonable and can lead to excessive risk of
over-reliance of opioids. Preventative approaches to pain management, rapid responses to a
patient’s need to control pain, and the ability to re-evaluate and intervene effectively in a timely
manner are key and fundamental measures of quality health care.
There are two causes of pain: biomedical and psychosocial/spiritual.
Biomedical
Basic principle: Identify the underlying pathophysiology causing the pain and treat with the most
appropriate intervention.
1. Acute and usually self-limiting pain due to injury (trauma) or surgery: The cause of pain
is generally self-evident, but unusual causes must be kept in mind (e.g., compartment
syndrome, bowel or urinary obstruction, complex regional pain syndrome). Pain that is
disproportionally severe or functionally impactful in relation to the inciting event or stage
Page 27 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
of healing requires thorough re-assessment and early referral to a specialist if causes are
not obvious or usual treatments are not effective.
2. Cancer-related: Pain associated with direct or metastatic tumor involvement of bone,
nerves, viscera, or soft tissues (60% to 80% of all cancer patients)
3. Cancer treatment-related: Pain associated with antineoplastic therapy (20% to 25% of
cancer patients), including surgery, radiation therapy (early and late effects), and
chemotherapy.
4. Other common painful disorders associated with recurrent, chronic and progressive
disease states or stand-alone chronic pain conditions:
a. Somatic: Musculoskeletal damage (e.g, arthropathies, spine facet disease, and
myofascial pain), skin and mucosal ulceration, cervicogenic headache.
b. Visceral: Ischemic, gastrointestinal and genitourinary insults (e.g, myocardial
infarction, fecal and/or urinary retention; bowel obstruction).
c. Neuropathic: Centrally-mediated (such as post-stroke pain; Parkinsonism; phantom
limb pain; post-herpetic neuralgia), peripherally-mediated (e.g, HIV, diabetes,
peripheral vascular disease), and less well-understood chronic pain syndromes,
including post-operative, post-radiation therapy and post-chemotherapy and HIV
treatment pain conditions.
d. Mixed or indeterminate: “Tension pattern” headache, migraine headache, chronic
daily headache, other types of headache, chronic low back and neck pain, abdominal
and pelvic pain syndromes, vulvodynia, complex regional pain syndrome.
Psychosocial/Spiritual
Basic principle: Any amount of pain can lead to psychological suffering which can greatly
amplify the biomedical pain experience.
1. Pain due to any injury, illness, disease or condition is often greatly amplified by
interpersonal conflict or unresolved intrapersonal issues (psychological or spiritual),
especially when the pain is a constant reminder of the seriousness of the illness.
2. Pain, anxiety, and depression reinforce each other as complex psycho-physiological
interactions that often cannot be readily separated; detailed assessment is necessary in
order to direct therapy in the most specific and efficacious way.
3 Sleep and mood changes and disorders are common concomitants of poorly controlled
acute and chronic pain. Initiating Opioid Treatment
Providing thorough documentation throughout the treatment plan is essential for patient safety
and prescriber protection. Records should remain current and be maintained in an accessible
manner and readily available for review. According to ruling R156-37-603(9), each prescription
for a controlled substance and the number of refills authorized shall be documented in the patient
records by the prescribing practitioner. In addition, ruling R156-37-602(5) requires all records
relating to Schedule II controlled substances received, purchased, administered, or dispensed by the
practitioner shall be maintained separately from all other records of the pharmacy or practice.
Focus of Module Four Based on national and state data, opioids continue to be the major problem of controlled substance use, so we’ll primarily focus on opioid treatment in this module. This module will provide recommendations on ways to treat acute pain.
Page 28 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Treating ACUTE Pain with Less Risk
Acute Pain is usually self-limited lasting hours to days to weeks. Acute pain has a clear pathological explanation such as injury and surgical procedure and the pain improves as the pathology resolves. The treatment of acute pain is expected to be of short duration. Pain may be mild to moderate,
and the patient may require minimal treatment; or the pain may be severe and the patient may
require short-term aggressive treatment. Good treatment of acute pain is necessary not only to
address pain but to maintain and restore function, improve mobility, and reduce post-injury or
surgery complications.
The following recommendations can protect patients and allow prescribers to more effectively
treat acute pain.
Acute Pain Recommendation 1: Use Alternative Treatments to Opioids
Opioid medications should only be used for treatment of acute pain when the severity of the pain
warrants that choice and after determining that other non-opioid pain medications or therapies
are either contraindicated or will not provide adequate pain relief.
Most acute pain can be effectively and safely treated with non-opioid medications (e.g.,
acetaminophen, non-steroidal anti-inflammatory drugs NSAIDs, or therapies such as exercise, or
specific stretching) rather than opioid medications which have less desirable adverse effects.
Care should be taken to assure that use of opioid pain treatment does not interfere with early
implementation of functional restoration programs.
Always consider the inclusion of non-medication-based treatment and self-management tactics to
help reduce acute pain. The decision to use one or more of these approaches is based on the
practitioner’s expertise; system access to trained and “credentialed” therapists; patient and family
expectations, values, interests, and goals; and patient’s insurance coverage or personal funds for
added service. These treatments may be effective alone or in conjunction with pain medications.
Alternative treatments for acute pain may include:
• Diet
• Weight Loss
• Cooling or heating techniques
• Sleep hygiene
• Smoking Cessation
• Aerobic and Strengthening Exercises
• Meditation & Relaxation Strategies
• Cognitive Behavioral therapy (CBT)
• Physical therapy (PT)
• Occupational therapy (OT)
• Massage therapy
• Music therapy
• Aroma therapy
• Acupuncture
• Yoga
• Ultrasound
• Transcutaneous Electrical Nerve
Simulation (TENS)
Page 29 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Acute Pain Recommendation 2: Check the Utah Controlled Substance Database (CSD)
The CSD should be checked to learn more about the patient’s controlled substance prescription
history at the inception of a patient-prescriber relationship and when prescribing opioids in an
emergency treatment setting. Document the results of this review in the patient’s record.
The Utah Division of Occupational and Professional Licensing (DOPL) maintains the CSD
Program. Access to the data is provided to authorized individuals by going online at
www.dopl.utah.gov. Individuals who are licensed to prescribe controlled substances in Utah or
staff assigned by the prescriber must register with DOPL to use the CSD. A prescriber can
designate one or more employees who can access the CSD on the prescriber’s behalf.
Utah Code 58-37f-301(2)(i)
Utah law requires a prescriber to check the database before the first time the prescriber issues a
patient a Schedule II or III opioid prescription. A prescriber is also required to periodically check
the database or similar records if the prescriber is repeatedly prescribing Schedule II or III
opioids to a patient. The CSD check is not required 1) in an emergency situation; 2) when the
CSD is not working; or 3) when the internet is not working.
Utah Code 58-37f-304(2).
Information from the CSD may be included in a patient’s medical chart or file and shared with other
medical professionals authorized to receive the information pursuant to Utah law and HIPAA.
The following controlled substances are not required to be reported in the CSD:
• Prescriptions filled at federal facilities, such as military. The Veteran’s Administration
provides data in accordance to Public Law 115-86 115th Congress.
• Prescriptions filled for individuals located outside the State of Utah.
• Controlled substances administered in an inpatient setting.
• Methadone maintenance clinics.
Acute Pain Recommendation 3: Consider Patient Risks
Proactively consider initial and ongoing risks associated with opioid exposure based on age of
the patient; history of substance use disorder; or psychiatric, physical, or medical comorbidities.
The developing brain may be more susceptible to addiction when exposed to opioid medications
and nonmedical use is more common among younger people. Those risks should be considered
when prescribing to an adolescent.
Patients with mental health conditions are at increased risk for developing chronic pain;
therefore, physicians should be cognizant of a patient’s psychological status and potential risk of
substance use disorder.
“Because psychological distress frequently interferes with improvement of pain and function in
patients with chronic pain, using validated instruments such as the Generalized Anxiety Disorder
(GAD)-7 and the Patient Health Questionnaire (PHQ)-9 or the PHQ-4 to assess for anxiety, post-
traumatic stress disorder, and/or depression (205), might help clinicians improve overall pain
treatment outcomes. Clinicians should use additional caution and increased monitoring to lessen
Page 30 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
the increased risk for opioid use disorder among patients with mental health conditions
(including depression, anxiety disorders, and PTSD), as well as increased risk for drug overdose
among patients with depression.”
GAD-7 and PHQ-4 and PHQ-9 can be found in the Material Resources Tab.
Acute Pain Recommendation 4: Prescribe Immediate-Release/Short-Acting Opioids
When opioids are indicated for the treatment of acute pain, prescribe immediate-release and
short-acting (IR/SA) opioids. Extended-release/long-acting (ER/LA) opioids, including
methadone, should rarely, if ever, be prescribed for acute pain, including post-operative pain.
Severe acute pain that persists longer than the expected healing time warrants re-examination.
Patients with acute pain who fail to recover in a usual timeframe or otherwise deviate from the
expected clinical course for their diagnosis should be carefully evaluated. The continuation of
opioid treatment in this situation may represent the initiation of opioid treatment for a chronic
pain condition. The diagnosis and appropriateness of interventions should be re-evaluated and
the patient’s medical history should be reviewed for comorbidities that could interact with opioid
treatment and for risk factors during opioid treatment, including current or history of substance
use disorder. It is also recommended that the prescriber check the Utah Controlled Substance
Database at the time they prescribe controlled substances.
Before issuing an initial opiate prescription*, a prescriber must discuss with the patient, or the
patient's parent or guardian:
• the risks of addiction and overdose associated with opiate drugs;
• the dangers of taking opiates with alcohol, benzodiazepines, and other central nervous
system depressants;
• the reasons why the prescription is necessary;
• alternative treatments that may be available; and
• the risks associated with the use of the drugs being prescribed.
* “Initial opiate prescription” includes a prescription for a patient who was last prescribed an
opiate more than a year ago.
This discussion is not required for:
• a patient who is currently in active treatment for cancer;
• a patient who is receiving hospice care from a licensed hospice; or
• a medication that is being prescribed to a patient for the treatment of the
patient's substance abuse or opiate dependence.
Utah Code 58-37-19
Acute Pain Recommendation 5: Prescribe the Lowest Effective Dose
When opioid medications are prescribed for treatment of acute pain, prescribers should prescribe
the lowest effective dose and no more than the number needed for the usual duration of pain
associated with that condition, usually 3-5 days and rarely more than 7 days.
Page 31 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Utah law states that a prescription for a Schedule II or III opiate for an acute condition shall not
be filled to exceed a seven-day supply as directed on the daily dosage rate of prescription. This
limitation does not apply when a prescription is issued for complex or chronic conditions which
are documented in the medical record. For acute surgery pain, when the prescriber determines
the initial seven-day supply is insufficient, subsequent seven-day prescriptions may be issued.
Utah Code 58-37-6(7)(f)(iii)
Prescribers or patients may request that a Schedule II prescription be partially filled and then, if
more is needed, the patient may pick up the rest of the prescription within the time period
allowed for that prescription. The intent is to help keep unused prescriptions out of medicine
cabinets. Utah Code 58-17b-610.7
Prescribing more medication than the amount likely to be needed leads to unused medications
being available for abuse or diversion. Use of opioid pain medications should be stopped when
pain severity no longer requires opioid medications and when function and quality of life has
improved.
Acute Pain Recommendation 6: Avoid and Counsel Against Combining Opioids with CNS
Depressants
Avoid prescribing, and counsel against, concurrent use of opioids and benzodiazepines. Patients
should also be counseled against concurrent use of opioids with other sedating substances,
including alcohol muscle relaxant drugs, and sedative hypnotics including prescription and over-
the-counter sleep aids, etc.
Concurrent use of alcohol, benzodiazepines, and other CNS depressants increases the risk of
respiratory depression, which can potentially cause death. Concurrent use of benzodiazepines
requires explicit medical justification due to the serious risk of respiratory depression. For
putative psychiatric indications, psychiatric consultation should be sought to treat the patient’s
condition with potentially less toxic drug-to-drug interactions. Prescribers should warn patients
of the high-risk interaction of opioids and CNS depressants.
Acute Pain Recommendation 7: Counsel Patients on the Risks of Opioids
The patient should be counseled on the risks of taking opioids that including dependency,
addiction, and death. In addition, patients should be advised of the signs of an opioid overdose
and informed of the availability of naloxone. Patients should be encouraged to securely store
their medications, not share with others, and to dispose of opioids properly when the pain has
resolved to prevent nonmedical use of the medications.
Patients and family/caregivers should learn to recognize the signs of an opioid overdose:
• Extremely pale face and/or feels clammy to the touch
• Body goes limp
• Fingernails or lips have a purple or blue color
• Vomiting or making gurgling noises
• Unable to be awakened or unable to speak
• Breathing or heartbeat slows or stops
Page 32 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
For patient education materials and resources on the risks of taking opioids and signs of an
opioid overdose, visit www.opidemic.org. For information on safe storage and disposal, visit
www.useonlyasdirected.org. For information on naloxone information, visit naloxone.utah.gov/.
Prevent Patient Advancing from Acute to Chronic Pain
( It’s important to recognize and prevent patients from advancing from acute to chronic pain.
Although acute pain is defined differently from chronic pain, they are often closely related,
because most chronic pain begins as acute pain.
There is a growing consensus that if left unresolved, the neuroplastic changes that contribute to
pain progression may become irreversible and ultimately refractory to treatment. Therefore,
healthcare providers’ priorities and standards of therapy for the management of pain should
consider the potential effects on patient health, with the goal of improving long-term outcomes
through early and effective treatment.
Prescribers can reduce the likelihood of a patient developing chronic pain if the appropriate
therapeutic methods to treat acute pain are implemented in a reasonable and coordinated
approach.
Prescribers should identify key factors that predict a transition from acute pain to chronic pain
and intervene with the most appropriate intervention (e.g., medical, cognitive behavioral,
counseling, physical or occupational therapy, etc.).
Key factors predictive of acute pain advancing to chronic pain:
Biomedical (other than ongoing tissue-damaging or inflammatory diseases)
• genetic factors [most studied in migraine and musculoskeletal pain conditions] Note: In the
absence of current genetic marker testing, a family history with positive genetic factors is
considered a risk factor.
• severe pre-operative pain duration and intensity predicts post-operative pain continuing after
usual healing period
• certain surgical procedures (e.g., mastectomy, thoracotomy, inguinal herniorrhaphy,
amputation) and certain types of chemotherapy and antiretroviral therapy
Social/Behavioral/Spiritual
• somatization
• catastrophizing behavior
• poor sleep
• unresolved litigation
• marital/family strife
• job dissatisfaction
• personal beliefs
•
Consider asking the following questions to help determine if the patient is at risk and how to help
the patient reduce the chance of pain advancement.
Page 33 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Disease – What does the patient have? Does the patient have treatable risk factors to reduce the
risk of acute pain becoming chronic?
The patient may have one or more of the following treatable risk factors:
o Major depressive disorder
o Neuropathic pain
o Sensitization that occurs in the nociceptive system
Dimensional – Who is the patient? What are the patient’s intrinsic traits that inhibit response to
treatment or evoke more pain?
The patient may have one or more of the following treatable risk factors:
o Somatosensory amplification, which means the patient has a less efficient system to
suppress nociception when exposed to painful stimuli
o Multiple somatic symptoms
Behavioral – What does the patient do? Does the patient engage in unproductive behaviors that
interfere with recovery?
The patient may have one or more of the following treatable risk factors:
o Fear and avoidance behaviors that result in disuse, disability, and more pain
o Substance abuse
Life Story – What does the patient encounter? Are the patients’ life stressors distracting and
demoralizing?
The patient may have one or more of the following treatable risk factors:
o Hyperarousal by potential threats, (e.g., post-traumatic stress disorder)
o Expecting major negative consequences from having acute pain, which may include
magnification, rumination, and helplessness
In summary, prescribers can minimize the risks and avoid acute pain from advancing to chronic
pain by applying the following principles:
• Repair and cure the patient’s disease
• Guide and strengthen an inherent vulnerability
• Alter patient’s unproductive behaviors into productive habits
• Reframe patient’s interpretations of failure into a positive approach
These resources have contributed to the educational content in this module:
Utah Department of Health (2017). Utah Clinical Guidelines on Prescribing Opioids for
Treatment of Pain. Salt Lake City, UT: Utah Department of Health Centers for Disease Control
and Prevention. [Patients with Mental Health Conditions]. MMWR 2016;65(No. 1)
Fine PG. Long-term consequences of chronic pain: mounting evidence for pain as a neurological
disease and parallels with other chronic disease states. Pain Med, 2011;12(7):996-1004.
Clark, M. R. (2013) How best to prevent acute pain from becoming chronic? Supplement to the
Journal of Family Practice, 62(9), S3
Advance to Module 4 on the next page.
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Controlled Substances: Education for the Prescriber
Presented by the Utah Medical Association Foundation –
“Extending the Reach of the Healer’s Hand.”
MODULE 4
Treating Chronic Pain with Less Risk
Learning Objectives
After completing this module, you should be able to
1. Treat chronic pain using the recommendations for treating chronic pain.
2. Evaluate patient’s need for pain treatment and refer to the chronic pain recommendations
for appropriate treatment.
3. Develop and discuss with patient and caregiver the key elements within the chronic pain
treatment plan.
4. Identify the risk factors that complicate chronic opioid therapy and employ risk-reduction
strategies to reduce opioid misuse, abuse, and death.
5. Recognize when a pain condition is complex or serious enough to warrant multi-
disciplinary pain treatment.
Treating CHRONIC Pain with Less Risk
Prescribers can provide better patient care by methodically evaluating the patient’s need for pain
treatment and referring to the recommendations in this module. Based on national and state data,
opioids continue to be the major problem of controlled substance use, so we’ll primarily focus on
opioid treatment in this module.
Chronic Pain can be defined as pain that persists due to ongoing disease or injury, (e.g. painful
diabetic neuropathy, arthritis, cancer); pain that occurs and persists in the absence of ongoing
tissue damage, (e.g. nociceptive pain or neuropathic pain); and/or pain that lasts longer than 3
months. Treating chronic pain can be complicated necessitating a long-term relationship between
the prescriber and patient. The following recommendations can protect patients and allow
prescribers to more effectively treat chronic pain.
The CDC advises that guidelines are intended for primary care clinicians treating chronic pain
for patients 18 and older. Examples of misapplication include applying the Guideline to patients
in active cancer treatment, patients experiencing acute sickle cell crises, or patients experiencing
post-surgical pain. (CDC Advises Against Misapplication of the Guideline for Prescribing
Opioids for Chronic Pain, April 2019)
mended Records (
The Federation of State Medical Boards Model Policy for the Use of Controlled Substances for
the Treatment of Pain recommends keeping the following patient records:
Page 35 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Medical history and physical examination
• Diagnostic, therapeutic, and laboratory results
• Evaluations and consultations
• Discussion of risks and benefits
• Treatment objectives
• Informed consent
• Treatments
• Medications, including a copy of prescriptions
• Instructions and agreements
• Periodic reviews
• Authorization for release of information
Records should remain current and be maintained in an accessible manner and readily available
for review. (See Module 6 for more information.)
The following recommendations can protect patients and allow prescribers to more effectively
treat chronic pain.
Prior to Prescribing Opioid Treatment for Chronic Pain 1. Chronic Pain Assessment
Prescribers should evaluate the level of pain both at rest and during physical maneuvers and
normative activities, not while the patient is immobile or inactive. The prescriber needs to
determine the reasons for the persistent pain and consider if the condition warrants chronic pain
management. The patient may need to be treated systematically while evaluation is being
completed.
Chronic Pain Recommendation 1.1: Use Non-pharmacologic and Non-opioid
Pharmacologic Therapies as Alternative Treatments to Opioids
Unless contraindicated, non-opioid analgesics, adjuvant analgesics (e.g., anticonvulsants,
antidepressants, non-steroidal anti-inflammatory drugs [NSAIDs], corticosteroids), and non-
pharmacologic therapies (e.g., cognitive behavioral therapy, physical therapy) are the preferred
method of treatment of chronic pain.
Opioid medications are not the appropriate first line of treatment for most patients with chronic
pain. Other measures, such as non-opioid analgesics, non-steroidal anti-inflammatory drugs
(NSAIDs), antidepressants, antiepileptic drugs, and non-pharmacologic therapies (e.g., physical
therapy) should be tried and the outcomes of those therapies documented first. Opioid therapy
should be considered only when other potentially safer and more effective therapies are proven
inadequate.
Non-opioid
NSAIDs are useful treatments for pain; however, they have adverse effects such as GI bleeding
and renal impairment that particularly affect the elderly. Recent studies report significant
Page 36 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
increased risk of myocardial infarction in older patients and others at risk for coronary artery
disease. When the benefit of NSAID use outweighs the risks and a given NSAID is not effective,
consider switching to a different class of NSAID; for example, switching a patient from
ibuprofen to diclofenac.
You may want to refer to the Non-opioid Analgesic Table in the Materials tab for medications
and typical dosages.
Acetaminophen is another effective pain reliever, especially in conjunction with other treatments. Again, like all medications, acetaminophen can have adverse effects, such as liver damage or failure. It is important to limit the total daily dose of acetaminophen to the FDA newly recommended maximum of 3 grams per day. Remember this dose limit when prescribing pain medications that contain any acetaminophen, such as Lortab and Percocet. Also remember, the FDA recommends using caution in prescribing acetaminophen when a
patient drinks 3 or more alcoholic beverages per day due to the increased risk of liver failure.
Treatments
Always consider the inclusion of non-medication-based treatment and self-management tactics to
help reduce chronic pain. The decision to use one or more of these approaches is based on the
practitioner’s expertise; system access to trained and “credentialed” therapists; patient and family
expectations, values, interests, and goals; and patient’s insurance coverage or personal funds for
added service. These treatments may be effective alone or in conjunction with pain medications.
Alternative treatments for chronic pain may include:
• Diet
• Weight Loss
• Cooling or heating techniques
• Sleep hygiene
• Smoking Cessation
• Aerobic and Strengthening Exercises
• Meditation & Relaxation Strategies
• Cognitive Behavioral therapy
• Physical therapy (PT)
• Occupational therapy (OT)
• Massage therapy
• Music therapy
• Aroma therapy
• Acupuncture
• Yoga
• Ultrasound
• Transcutaneous Electrical Nerve Stimulation (TENS) Chronic Pain Recommendation 1.2: Identify if Benefits Outweigh the Risks
Proactively consider initial and ongoing risks associated with opioid exposure based on age of
the patient, history of substance use disorder, or psychiatric, physical, or medical comorbidities.
Prescribers should only consider opioid therapy for a patient when expected benefits of pain
improvement, function, and quality of life are anticipated to outweigh the risks.
Identify if benefits outweigh the risks by completing recommendation sections 2. Comprehensive Evaluation and 3. Screening for Risk of Substance Use Disorder and by determining desired treatment outcomes.
Page 37 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
2. Comprehensive Evaluation
Chronic Pain Recommendation 2.1: Complete a Comprehensive Patient Evaluation
A comprehensive evaluation should be performed before initiating opioid treatment for chronic
pain.
The comprehensive evaluation consists of the patient’s social/work history, medical history,
mental health/substance use history, pain specific history, and physical examination. The goal of
the comprehensive evaluation is to determine the nature of the patient’s pain; evaluate how the
pain is impacting the patient’s job requirements, activities of daily living, and quality of life;
identify other conditions or circumstances that could affect the choice of treatment or the
approach to managing that treatment; assess and evaluate prior approaches to pain management;
and serve as a basis in establishing a treatment plan and evaluation of treatment outcomes.
A comprehensive history and physical examination are critical for both the patient’s physical
health and completion of the patient’s personal history, including social, medical, psychiatric,
psychological, and substance abuse.
The social history should include:
• Employment history and status,
• Social network,
• Marital history, and any
• History of legal problems related to controlled substances.
When gathering a past medical history,
• Assess the pain, emphasizing functional deficits prior to treatment.
• Determine the cause of the pain and the severity of the pain.
• Assess effects of the pain on the patient’s life and function, including the functional
status of the patient during work, home and family activities, and recreational
activities.
• Assess patient’s perceived quality of life using a method/instrument that can be used
later to evaluate treatment effectiveness.
• Assess for the presence of medical conditions that might complicate the treatment of
the pain, including medication allergy, cardiac or respiratory disease, liver disease,
renal disease, and sleep apnea.
When gathering a mental health and substance use history,
• Obtain history of substance use, addiction, or dependence.
• Assess the use of other substances, including alcohol, and illicit drug use such as
marijuana, cocaine, and methamphetamines.
• Identify use of other medications that might interact with medications used to treat
the pain. Particular attention should be given to benzodiazepines and other sedative
medications.
• Identify psychiatric conditions that may affect pain or treatment of pain.
Page 38 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Ask patient about other depressants they are taking, including benzodiazepines and
diphenhydramine, gabapentin/pregabalin, because they may cause drug-drug
interaction that lead to adverse effects potentiating respiratory depression.
• Assess and evaluate prior approaches to the patient’s pain management.
• Assess risk of sleep apnea.
When gathering pain specific information, it can be helpful to use the mnemonic OPQRST.
Onset – When did pain/does pain begin?
Pain – Gets better with_____ or gets worse with_____.
Quality – Does it cause burning/achiness/other symptoms?
Radiation – Where does pain start and where does it spread?
Severity – Use a validated pain rating scale for self-reporting patients. For those unable to
self-report due to dementia, you may use PAINAD© (AMDA), which can be
found in the Material Resources tab.
Temporal Course
- Is there a constant or episodic pattern?
- When is the pain most severe?
- Is there breakthrough pain? What is the frequency, severity, and duration of the
breakthrough pain? Is pain incidental caused by specific activity or action?
Spontaneous pain with no identifiable cause? End-of-dose failure where the pain
returns before next dose of regularly scheduled medicine takes effect?
- It may be helpful for an able patient or caregiver to use a 24-hour pain diary to
help identify many factors and effects of interventions.
Following the comprehensive history, the prescriber needs to complete a physical examination
to:
• Assess the pain, emphasizing functional deficits prior to treatment.
• Determine the cause of the pain as specifically as possible and institute diagnosis-
specific therapy immediately.
• Assess effects of the pain on the patient’s life and function, including the
₋ Functional status of the patient during work, home and family activities, and
recreational activities
₋ Patient’s perceived quality of life and the
₋ Severity of the pain.
• Assess for the presence of medical conditions that might complicate the treatment of
the pain, including medication allergy, cardiac or respiratory disease, liver disease,
renal disease, and sleep apnea or the risk factors for sleep apnea.
This comprehensive evaluation is critical to develop a treatment plan that achieves greater
benefit than harm to the patient and allow the prescriber to assess therapeutic outcome of
chronic pain treatment.
When initiating treatment, remember the patient’s functional ability is more important than
the level of pain relief achieved.
Page 39 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Chronic Pain Recommendation 2.2: Check Disease-Specific Guidelines
Prescribers should refer to disease-specific guidelines for recommendations of treatment for
specific diseases or conditions of chronic pain.
3. Risk of Substance Use Disorder Screening
Chronic Pain Recommendation 3.1: Screen for Risk of Opioid Use Disorder
Use a validated screening tool to assess the patient’s risk of opioid use disorder prior to
prescribing an opioid medication long-term for chronic pain.
Long-term use of opioid medications to treat chronic pain safely requires the commitment of
adequate resources to regularly monitor and evaluate outcomes and identify occurrence of
adverse consequences. The screening tool results are intended to assist the prescriber in
determining whether opioid therapy is appropriate and in determining the level of monitoring
appropriate for the patient’s level of risk.
Prescribers may consider using one of the standardized screening forms to help determine
personal and family risks:
• Patient Health Questionnaire (PHQ-4) or (PHQ-9)
• Opioid Risk Tool (ORT©)
• Screener and Opioid Assessment for Patients with Pain-Revised (SOAPP-R®)
• Current Opioid Misuse Measure (COMM®)
• Alcohol, Smoking, and Substance Screening Test (ASSIST)
• Opioid Abuse Risk Screener (OARS)
These forms can be found in the Material Resources Tab.
Prescribers should consider risk factors for misuse, abuse and addiction before prescribing
controlled substances. The factors that contribute to the onset of drug abuse and addiction may
include:
• Family history of substance use disorder, including illicit and licit (e.g., caffeine, tobacco)
• Current drug and alcohol abuse
• Family and social environment
• Mental disorders, especially mood disorder
• Drug choice and availability
• Mode of administration
• Drug use at early age
• Sleep disorders involving obstructive or central sleep apnea
• Cardiac disorders
• Patients
Medical risks include:
• Sleep disorders involving obstructive or central sleep apnea
Page 40 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Cardiac disorders
• Patients who have major psychiatric disorders such as
- Personality disorder
- Depression
- Anxiety
- Bipolar
- PTSD
Chronic Pain Recommendation 3.2: Obtain a Urine Drug Screen
Urine drug screening is strongly recommended before initiating opioid treatment for chronic
pain.
Research and experience have shown that drug testing can identify problems, such as use of
undisclosed medications, non-use of reported medications (i.e., drug hoarding or diversion),
undisclosed use of alcohol, or use of illicit substances. It is recommended that drug testing be
strongly considered and conducted especially when other factors suggest risk. If the condition
started with acute pain and there is consideration for chronic use, at least one drug screen in
approximately 1-2 months is advised.
A positive drug screen indicates the need for caution, but it does not preclude opioid use for
treatment of pain. Consideration should be given to refer to substance abuse counseling and/or to
a pain management specialist. If urine drug screening is positive for unprescribed or illegal drugs
or the prescribed meds are absent, document this in the patients record and counsel the patient
about adherence to a drug treatment plan or initiating a drug contract.
Chronic Pain Recommendation 3.3: Query the Controlled Substance Database
The prescriber should check Utah’s Controlled Substance Database (CSD) before prescribing
opioids for chronic pain.
The Utah Division of Occupational and Professional Licensing (DOPL) maintains the CSD
Program. Access to the data is provided to authorized individuals by going online at
www.dopl.utah.gov. Individuals who are licensed to prescribe controlled substances in Utah or
staff assigned by the prescriber must register with DOPL to use the CSD. A prescriber can
designate one or more employees who can access the CSD on the prescriber’s behalf.
Utah Code 58-37f-301(2)(i)
Recently passed Utah law requires a prescriber to check the database before prescribing a “high
risk prescription,” defined as a prescription for one or more opiate or benzodiazepine
prescriptions written for longer than 30 days. Prescribers must first check the CSD to determine
if the patient already has any current active high-risk prescriptions. If a high-risk prescription is
in the system, prescriber must contact all other prescribers and document the contact and the
reason the patient needs multiple high-risk prescriptions from different prescribers. Utah Code
58-37-6(11)
A prescriber is also required to periodically check the database or similar records if the
prescriber is repeatedly prescribing Schedule II or III opioids to a patient. The CSD check is not
required 1) in an emergency situation; 2) when the CSD is not working; or 3) when the internet is
not working. Utah Code 58-37f-304(2)
Page 41 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Information from the CSD may be included in a patient’s medical chart or file and shared with
other medical professionals authorized to receive the information pursuant to Utah law and
HIPAA.
The following controlled substances are not required to be reported in the CSD:
• Prescriptions filled at federal facilities, such as military. The Veteran’s Administration
provides data in accordance to Public Law 115-86 115th Congress.
• Prescriptions filled for individuals located outside the State of Utah.
• Controlled substances administered in an inpatient setting.
• Methadone maintenance clinics.
Establish Treatment Goals and Written Treatment Plan 4. Treatment Plan
Prescribers should have patients sign a treatment agreement once they understand and agree on
the treatment plan. This detailed agreement between the patient and prescriber documents the
requirements for chronic pain management and assists the prescriber in monitoring the patient’s
compliance with the treatment plan.
Chronic Pain Recommendation 4.1: Establish a Written Treatment Plan
A patient-provider collaborative written opioid treatment plan should be established before
opioid therapy and be reviewed and updated on a regular basis.
Prescribers should tailor the treatment plan to the patient’s circumstances and cultural
differences and to the characteristics and pathophysiology of the pain. The pathophysiologic
basis of the pain can help establish a prognosis for future improvement (or worsening) in
function and pain and should influence the treatment goals. Non-opioid treatment modalities
should be included in the treatment plan whenever possible to maximize the likelihood of
achieving treatment goals.
Patient responsibilities include properly obtaining, filling, and using prescriptions as directed,
and adherence to the treatment plan. The agreement is usually combined with the Informed
Consent. See Recommendation 5.1 for more information.
Treatment agreement outlines the joint responsibilities of the clinician and patient and are
indicated for opioid or other medications with potential for substance use disorder. It is strongly
recommended that treatment agreements include:
• Unforeseen problems and to prescribe scheduled refills. Treatment goals in terms of pain
management, restoration of function and safety
• Patient’s responsibility for safe medication use (not taking more than prescribed; dangers
of using in combination with alcohol, cannabis, or other substances like benzodiazepines
unless closely monitored by the prescriber, etc.)
• Secure storage and safe disposal
• Patient’s responsibility to obtain prescribed opioids from only one clinician or practice
Page 42 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Patient’s responsibility of getting the prescriptions filled at only one pharmacy
• Patient’s agreement to periodic drug testing
• Clinician’s responsibility to be available or to have a covering clinician available to care
for patient
A sample Treatment Plan can be found in the Material Resources Tab.
Chronic Pain Recommendation 4.2: Identify Measurable Treatment Goals
Treatment goals should include measurable goals for function, quality of life, and improved pain
control and should be developed jointly by patient and prescriber.
Prescribers have observed and adherence literature confirms that when patients are engaged in
their own healthcare and assume responsibility for their rehabilitation, they are more likely to
improve; and that when they participate in goal setting, they are more likely to achieve their
goals. As with any other chronic illness (e.g., diabetes or heart disease), the prescriber should
focus not just on pain control, but also on treating the patient’s underlying diseases and
encouraging them to engage in the full spectrum of their health.
These measures of improvement or worsening can be reported by the patient, family members,
and/or employer. Permission to discuss the patient’s condition with these persons should have
previously been obtained and documented.
Informed consent should also include explaining to the patient that they shouldn’t expect
complete relief of their pain. Improved function is the main criterion for continuing opioid
treatment.
Chronic Pain Recommendation 4.3: Maintain Accurate Patient Records
Prescribers should obtain and document information about the patient’s treatment and history.
Prescribers should document the treatment, interactions, and findings throughout your
professional relationship with the patient. Providing thorough documentation throughout the
treatment plan is essential for patient safety and prescriber protection. According to ruling R156-
37-603(9), each prescription for a controlled substance and the number of refills authorized shall
be documented in the patient records by the prescribing practitioner. In addition, ruling R156-37-
602(5) requires all records relating to Schedule II controlled substances received, purchased,
administered, or dispensed by the practitioner shall be maintained separately from all other records
of the pharmacy or practice.
Chronic Pain Recommendation 4.4: Plan to Modify or Discontinue Opioid Therapy
The treatment plan and goals should explicitly include a plan to modify or discontinue opioid
therapy when benefits do not outweigh the risks and when patient fails to adhere to the agreed
upon treatment plan.
Prescribers should evaluate benefits and harms with patient within 1 to 4 weeks of starting opioid
therapy or of dose escalation; then continue to evaluate the benefits and harms of therapy with
Page 43 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
patient every 3 months or more frequently. If benefits do not outweigh the harms of continued
opioid therapy, prescribers should optimize other therapies and work with the patient to taper
opioids to lower dosages or to taper and discontinue opioids. (See Chronic Recommendation
10.2 for additional information.)
When tapering or discontinuing opioids, the CDC announces, “The [CDC] Guideline does not
support abrupt tapering or sudden discontinuation of opioids. These practices can result in
severe opioid withdrawal symptoms including pain and psychological distress, and some patients
might seek other sources of opioids. In addition, policies that mandate hard limits conflict with
the Guideline’s emphasis on individualized assessment of the benefits and risks of opioids given
the specific circumstances and unique needs of each patient.”
5. Informed Consent
Chronic Pain Recommendation 5.1: Obtain Signed Informed Consent Form
Prescribers should discuss with patients the known risks and realistic benefits of opioid therapy
and patient and prescriber responsibilities for managing therapy, including any conditions for
continuation of opioid treatment. This discussion should be documented using a written and
signed informed consent form, which is often combined with the treatment agreement.
Before issuing an initial opiate prescription*, a prescriber must discuss with the patient, or the
patient's parent or guardian:
• the risks of addiction and overdose associated with opiate drugs;
• the dangers of taking opiates with alcohol, benzodiazepines, and other central nervous
system depressants;
• the reasons why the prescription is necessary;
• alternative treatments that may be available; and
• the risks associated with the use of the drugs being prescribed.
* “Initial opiate prescription” includes a prescription for a patient who was last prescribed an
opiate more than a year ago.
This discussion is not required for:
• a patient who is currently in active treatment for cancer;
• a patient who is receiving hospice care from a licensed hospice; or
• a medication that is being prescribed to a patient for the treatment of the
patient's substance abuse or opiate dependence.
Utah Code 58-37-19
The informed consent document typically includes:
• Potential risks and benefits of controlled substance use, including the risk of misuse,
dependence, addiction, overdose, and death
• Adverse effects, both short-term and long-term, such as cognitive impairment and
constipation
• Likelihood of tolerance and dependence developing
• Possible drug interactions and over-sedation
• Limited evidence of the benefit of long-term opioid therapy
Page 44 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Risk of impairment in operating motor vehicles or equipment or performing other tasks
• Prescriber’s policies and expectations
• Specific reasons for adapting or discontinuing drug therapy
Chronic Pain Recommendation 5.2: Educate Patient and Family/Caregivers
Educational material about the patient’s opioid treatment plan should be provided in written form
and discussed in person with the patient and, when applicable, the family or caregivers.
For patient education materials and resources on the risks of taking opioids and signs of an opioid
overdose, visit www.opidemic.org. For information on safe storage and disposal, visit
www.useonlyasdirected.org. For information on naloxone information, visit naloxone.utah.gov/.
Discuss with the patient the involvement of family and caregivers in the patient’s care and
receive written permission from the patient to involve the family or caregivers. This is best done
before starting to treat the patient, because it can be more difficult to obtain consent after an
issue occurs.
Note: Consultation with others, in the absence of consent, must be done within the guidelines and
constraints of HIPAA.
Utah Code 58-37f-301(5) allows a patient with a controlled substance prescription to designate a
third party who will be notified by DOPL when a controlled substance is dispensed to the
patient. The controlled substance is not identified in the notification. When the patient tells the
division to stop providing information to the designated party, the designee will be notified of the
change. Prescribers should discuss this designation with patients.
Initiate and Adjust Opioid Treatment
6. Opioid Treatment Trial
When non-opioid treatments don’t lead to improved therapeutic goals and outcomes in patients
with debilitating pain, a trial of opioid therapy should be considered if potential benefits
outweigh risks.
Chronic Pain Recommendation 6.1: Combine Therapy
When opioid treatment is indicated, non-opioid analgesics, adjuvant analgesics and non-
pharmacologic therapies should be used in combination with opioid treatment as appropriate for
the patient.
Combination products with opioid and non-opioid analgesics may result in better pain relief than either drug alone, but the opioid dose is limited by the non-opioid. The use of adjunctive
medications, as well as other therapies, such as physical therapy, exercise, stretching, and other
alternative therapies, can reduce the dose of opioid needed for adequate pain relief; and
consequently, improve a patient’s functionality.
Page 45 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Chronic Pain Recommendation 6.2: Initiate Short-term Treatment Trial
Opioid medication should be initiated as a short-term trial to assess the effects of opioid
treatment on pain intensity, function, and quality of life.
The prescriber should clearly explain to the patient that initiation of opioid treatment is not a
commitment to long-term opioid treatment and that treatment will be stopped if the trial is
determined to be unsuccessful. The trial should be for a specific time period with pre-determined
evaluation points as defined in the treatment plan measures. The decision to continue opioid
medication treatment beyond the trial period should be based on the balance between benefits
gained in function and quality of life, and adverse effects experienced. Criteria for cessation
should be considered before treatment begins.
When a new patient has already been receiving opioid therapy for a chronic condition, the same
recommendations apply: assess the patient’s chronic pain, complete a comprehensive evaluation,
screen for risk of substance use disorder, perform random drug screens, establish a treatment
plan and informed consent, initiate treatment trial, mitigate risks, and consider a multi-
disciplinary approach. The evaluation process may require more time than the initial
appointment, so the prescriber must use their professional judgement if opioids are deemed
necessary. If opioid treatment is necessary, it is suggested that the dose be limited and only long
enough to complete an adequate evaluation and to seek consultation, as needed.
Chronic Pain Recommendation 6.3: Begin with Immediate Release/Short-Acting (IR/SA)
The trial should begin with Immediate Release/Short-Acting (IR/SA) opioid medication.
Immediate-release, short-acting (IR/SA) opioid medications are generally safer and easier to
titrate to an effective dose. CDC experts agreed that for patients not already receiving opioids,
prescribers should not initiate opioid treatment with extended-release or long-acting opioids
(ER/LA) and should not prescribe ER/LA opioids for intermittent use.
ER/LA opioids should be reserved for severe continuous pain and should be considered only for
patients who have received IR/SA opioids daily for at least 1 week. Initial treatment should avoid
the use of methadone, fentanyl, or the combination of opioids and benzodiazepines.
When Schedule II opioids are being prescribed, prescribers or patients may request that a
Schedule II prescription be partially filled and then, if more is needed, the patient may pick up
the rest of the prescription within the time period allowed for that prescription. The intent is to
help keep unused prescriptions out of medicine cabinets. Utah Code 58-17b-610.7
Schedule II controlled substances may not be refilled; a new prescription must be issued. A
practitioner may issue more than one prescription at the same time for the same Schedule II
controlled substance, but only under the following conditions:
• No more than three prescriptions for the same Schedule II controlled substance may be
issued at the same time,
• No one prescription may exceed a 30-day supply; and
• A second or third prescription shall include the date of issuance and the date for
dispensing. Utah Code 58-7(f)(vii)
Page 46 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Nurse Practitioners in independent solo practice and who 1) have been licensed less than a year
or 2) have less than 2000 hours of practice experience, may prescribe or administer Schedule II
or III Controlled Substances after nurse practitioner:
1. Receives a board certification from a nationally recognized organization;
2. Completes at least 30 hours of instruction in advanced pharmacology;
3. Demonstrate at least 7 hours of continuing medical education on prescribing opioids; and
4. Participate in and document a prescribing mentorship with a physician or experienced
nurse practitioner for 1000 hours of clinical experience.
Utah Code 58-31b-803
Chronic Pain Recommendation 6.4: Prescribe the Lowest Effective Dose
When opioids are started, prescribers should prescribe the lowest effective dosage. Prescribers
should use caution when prescribing opioids at any dosage, should carefully re-assess evidence
of individual benefits and risks when increasing dosage to > 50 morphine milligram equivalents
(MME)/day, and should avoid increasing dosage to > 90 or carefully justify a decision to titrate
dosage to > 90 MME/day.
CDC states that although there is not a single dosage threshold below which overdose risk is
eliminated, holding dosages below 50 MME/day would likely reduce risk among most patients
who would experience fatal overdose at higher prescribed dosages. The recommendation does
not suggest the discontinuation of opioids already prescribed at higher dosages. Utilization of
any dose should be based on incremental functional gains.
Benefits of high-dose opioids for chronic pain are not established. At the same time, risks for
serious harm increase at higher opioid doses. Opioid overdose risk increases in a dose-response
manner. Dosages of 50-100 MME/day increase risks for opioid overdose by 1.9-4.6 times, and
dosages > 100 MME increase risk by 2.0-8.9 times as compared with the risk at 1-20 MME/day.
Any individual who knows of a practitioner or employee involved in diversion of a Schedule II
or III opiate >500 MME is required to report the diversion to a peace officer or law enforcement
agency. Failing to report is a class B misdemeanor. Utah Code 76-10-2204(2)
Chronic Pain Recommendation 6.5: Prevent Prescription Fraud
The prescription for opioid therapy should be written on tamper-resistant prescription paper or e-
prescribed to prevent prescription fraud.
To reduce the chance of tampering with the prescription, write legibly, and keep a copy in your
records. According to the DEA, all records related to controlled substances must be maintained
and be available for inspection for a minimum of two years.
Chronic Pain Recommendation 6.6: Implement Dose Titration and Re-evaluation
Regular face-to-face visits with evaluation of progress against goals should be scheduled during
the period when the opioid dosage is being adjusted. The opioid trial or long-term treatment
should be continually evaluated for functional benefit and achievement of treatment goals, using
appropriate tracking tools.
Page 47 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Clinically meaningful improvement has been defined as a 30% improvement in scores for both
pain and function. Monitoring progress toward patient-centered functional goals (e.g., walking
the dog or walking around the block, returning to part-time work, attending family sports or
recreational activities) can also contribute to the assessment of functional improvement.
Prescribing providers should use these goals in assessing benefits of opioid therapy for
individual patients and in weighing benefits against risks of continued opioid therapy.
If the patient’s pain is not effectively treated by increasing the opioid dose, the patient may be
non-responsive to opioids. Non-response to one opioid often means patients will be non-
responsive to other opioids, especially for chronic non-cancer pain patients. For example,
myofascial pain and fibromyalgia are seldom responsive to opioid treatment.
When opioids are initially effective, but only remain effective with frequent increases in dose,
the opioid may only be affecting mood or anxiety. This is an inappropriate indication for opioids
and the prescriber should discontinue treatment. Refer to Chronic Recommendation 10.1 for
more information about treatment discontinuation.
There are a variety of tracking tools that can be used to set and monitor treatment goals:
• Pain Assessment and Documentation Tool (PADT™)
• Patient Pain and Medication Tracking Chart, ©Utah Department of Health
• Brief Pain Inventory (BPI©)
• Treatment agreement
• Patient Health Questionnaire (PHQ-4 or PHQ-9)
Forms can be found in the Material Resources Tab.
Chronic Pain Recommendation 6.7: Avoid Parenteral Opioids
Parenteral (intravenous, intramuscular, subcutaneous) administration of opioids for chronic pain
is strongly discouraged, unless prescribing within an inpatient or palliative care setting.
Any circumstance warranting parenteral administration should be clearly justified by clinical
exigencies (e.g., bowel obstruction; terminal care).
These guidelines do not consider intrathecal administration and this recommendation was not
intended to discourage trained and qualified physicians from using intrathecal opioid
medications when indicated.
Daily IM or SC injections should be avoided except in a highly supervised environment, such as
during an admission to the hospital or hospice.
Risk Mitigation
7. Risk Mitigation
Considering the current epidemic of opioid-related deaths, prescribers must employ risk-
Page 48 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
reduction strategies to reduce opioid misuse, abuse, and death. Prescribers can take measures to
protect patients from these risks through implementing screening and monitoring processes
before and during opioid treatment.
Chronic Pain Recommendation 7.1: Avoid Combining Opioids with CNS Depressants
Avoid prescribing, and counsel against, concurrent use of opioids and benzodiazepines. Patients
should be counseled against concurrent use of opioids with other sedating substances, including
alcohol, muscle relaxant drugs, and sedative hypnotics, including prescription and over-the-
counter sleep aids.
Concurrent use of alcohol, benzodiazepines, and other CNS depressants increases the risk of
respiratory depression, which can potentially cause death. Concurrent use of benzodiazepines
requires explicit medical justification due to the serious risk of respiratory depression. For
putative psychiatric indications, psychiatric consultation should be sought to treat the patient’s
condition with potentially less toxic drug-to-drug interactions. Prescribers should warn patients
of the high-risk interaction.
Chronic Pain Recommendation 7.2: Evaluate Risks Associated with Sleep Apnea
Prescribers should assess the patient’s risk for sleep apnea and consider formal screening.
Risk factors for sleep-disordered breathing include congestive heart failure, and obesity. Careful
monitoring and cautious dose titration should be used if opioids are prescribed for patients with
mild sleep-disordered breathing. Prescribers should avoid prescribing opioids to patients with
moderate or severe sleep-disordered breathing whenever possible to minimize risks for opioid
overdose.
Patients who are taking more than 100mg of oral morphine a day, or an equivalent analgesic dose
of other opioids, are at a higher risk of central sleep apnea. Patients who are obese and those who
experience loud snoring, shallow or irregular breathing while asleep are also at a higher risk.
Consider sleep screening studies for all patients on moderate or high doses of any long-acting
opioid and those on moderate to high doses of other depressants, such as benzodiazepines and
sleep medications.
Naloxone rescue medication should be provided to family members/caregivers, who should
receive education on when to administer if patient has risk of sleep apnea, regardless of total
daily dose of MME used.
Educating the family about the signs of opioid overdose may help detect problems before they
lead to a serious complication. Patients and family/caregivers should learn to recognize the
danger signs of respiratory depression and know to how to offer help and summon medical help
immediately if a person demonstrates any of the following signs while on opioids:
• Episodic cessation of breathing;
• Periods of irregular or other sleep disordered breathing;
• Extreme drowsiness and difficulty being awakened;
Page 49 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Slow, shallow breathing with little chest movement;
• Increased or decreased heartbeat or palpitations; or
• Feeling faint, dizzy, confused.
Chronic Pain Recommendation 7.3: Obtain Urine Drug Screens
Prescribers should perform drug screening on randomly selected visits and any time aberrant
behavior is suspected.
A good practice is to give all patients taking chronic controlled substance prescriptions at least
annual urine tests and high-risk patients more frequent random urine tests with no advance
notice. Drug testing has been shown to identify the presence of illegal drugs, unreported
prescribed medication, unreported alcohol use, or the absence of the patient’s prescribed
medication, which could indicate diversion or non-adherence to the treatment plan. This assists the prescriber in determining whether the opioid therapy is appropriate and in
determining the required frequency of monitoring. It also provides an opportunity to discuss the
risks with opioid treatment. As another cautionary measure, a prescriber may request random pill counts to determine if the patient is using the appropriate amount of medication.
Immunoassays can be done in the office. These screening tests determine if opioids are present
but do not identify specific ones, which can subsequently be determined by confirmatory
laboratory testing. However, in many cases, confirmation testing can be eliminated by carefully
going over the results of the initial in-office test with the patient. Prescribers need to recognize
that immunoassays have both false positive and false negative results. Over-the-counter
medication, for example, can cause a positive result. Many synthetic opioids are not detected by
urine immunoassay screening and require confirmation testing when there is suspected use. The
prescriber may want to consider confirmatory testing or consultation with a Certified Medical
Review Officer if drug test results are unclear.
An abnormal drug screen should be specified in the treatment agreement as a possible reason to
cease treatment.
Chronic Pain Recommendation 7.4: Query the Controlled Substance Database
During treatment of chronic pain with opioid medications, the Utah Controlled Substance
Database (CSD) should be checked at least quarterly.
Prescribers should review the patient’s history of controlled substance prescriptions to determine
whether the patient is receiving opioid dosages or dangerous combinations that put them at high risk
for overdose. Prescribers should communicate with others managing the patient or prescribing
controlled substances to coordinate care and to improve patient’s safety.
Aberrant findings in the CSD (or from urine drug screening) necessitate a frank conversation
with the patient. Such findings, based upon the treatment agreement, may be cause for
tapering/discontinuing controlled substances, referring the patient to a pain management
specialist, or developing a new treatment plan.
Page 50 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Chronic Pain Recommendation 7.5: Co-prescribe Naloxone
As an intervention to prevent a potential opioid overdose death, consider co-prescribing an
approved naloxone delivery kit for patients receiving opioids for treatment of chronic pain.
Prescribers should mitigate risk of overdose by offering naloxone when increased opioid
overdose risk factors are present. Risks factors may include: patient has a history of overdose or
a substance use disorder, patient is taking higher opioid dosages (≥50 MME/day), or patient is
concurrently using a benzodiazepine. Naloxone administration is intended to reverse life-
threatening respiratory depression. Naloxone is commercially available by prescription for
emergency use in autoinjector and intranasal administration forms.
See Chronic Pain Recommendation 7.6 for the duration of action and additional information.
A prescriber-patient relationship is not required for a prescriber to prescribe or dispense an opiate
antagonist to an at-risk person, a concerned person in a position to help, or an overdose outreach
provider. According to Utah law, lay persons who administer an opiate antagonist are protected
from civil liability when acting in good faith. Utah Code 26-55-104
As provided by this law, on December 8, 2016, the physician-executive director of the Utah
Department of Health issued a standing order allowing pharmacists to dispense naloxone to
concerned family members, caregivers, friends, and patients without a written prescription.
However, pharmacies are not required to participate in the standing order.
Chronic Pain Recommendation 7.6: Provide Overdose Education and Counseling
Provide the patient and caregivers information on the signs and symptoms of opioid overdose,
how to obtain naloxone, and the timely and proper administration of naloxone.
Patients and family/caregivers should learn to recognize the danger signs of opioid overdose:
• Extremely pale face and/or feels clammy to the touch
• Body goes limp
• Fingernails or lips have a purple or blue color
• Vomiting or making gurgling noises
• Unable to be awakened or unable to speak
• Breathing or heartbeat slows or stops
Educating the family about the signs of opioid overdose may help detect problems before they
lead to a serious complication. Patients and family/caregivers should also learn to recognize the
danger signs of respiratory depression (see Recommendation 7.2) and know how to offer help
and summon medical help immediately. Counseling about administration of naloxone for
suspected overdose should be provided in those cases where naloxone is co-prescribed.
Naloxone can be prescribed by a healthcare provider or by a pharmacist, as per the Utah
Department of Health standing order.
Once naloxone is administered, professional emergency care needs to be provided by calling
911. Naloxone wears off in 30-90 minutes, so naloxone administration may need to be repeated.
Meanwhile, CPR or mouth-to-mouth resuscitation may also need to be administered, so family
Page 51 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
and caregivers should receive training in both when naloxone is prescribed. Warning: The
standard IV dosage of naloxone is 0.4 mg and the intranasal dose is 2-4 mg. Administering an
excessive amount of naloxone by repeating doses too frequently or using a high dose preparation
can cause the patient to experience acute opioid withdrawal symptoms which can cause seizures
or even be life threatening.
Naloxone may not be effective if opioids are misused in combination with other sedatives or
stimulants. It is not effective in treating overdoses of benzodiazepines or stimulant overdoses
involving cocaine and amphetamines.
See Instructions for Naloxone Administration in the Material Resources Tab. Additional
information for the public, prescribers, pharmacists, and first responders can be found at
https://naloxone.utah.gov/.
Chronic Pain Recommendation 7.7: Counsel Patients on Safe Storage, Disposal, and
Diversion
Patients should be encouraged to securely store their medications, not share with others, and to
dispose of opioids properly when the pain has resolved to prevent non-medical use of the
medications.
For patient education materials and resources on safe storage and disposal, visit
www.useonlyasdirected.org.
Treatment Management
8. Monitoring Treatment and Dose Adjustments
Chronic Pain Recommendation 8.1: Monitor Opioid Therapy
Once a stable dose has been established, regular monitoring should be conducted at face-to-face
visits. During these visits, treatment goals, affect and mood, analgesia, activity and level of
function, adverse effects, and aberrant behaviors should be monitored.
These assessments can be remembered as the “5 A’s.”
5 A’s Opioid Therapy Monitoring Tool
1. Affect: determine if pain has impacted patient’s mood
2. Analgesia: inquire about level of pain (current, recent, trends, etc.)
3. Activity: assess both the patient’s function and overall quality of life
4. Adverse events: determine whether the patient is having medication side effects
5. Aberrant behavior: regularly evaluate for substance use disorder related behavior
Also, it is recommended to consider the patient’s airway and sleep apnea status.
Chronic Pain Recommendation 8.2: Evaluate Patient Progress
Continuation or modification of therapy should depend on the prescriber’s evaluation of progress
towards stated treatment goals.
Page 52 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Prescribers should evaluate benefits and harms of continued therapy with patients every 3
months or more frequently. If benefits do not outweigh harms of continued opioid therapy,
prescribers should optimize other therapies and work with patients to taper opioids to lower
dosages or to taper and discontinue opioids.
Chronic Pain Recommendation 8.3: Adjust and Prescribe Medication During Clinic Visit
Medication adjustments should generally be made and prescriptions provided during a clinic
visit.
Face-to-face follow-up visits should occur at least every 2-4 weeks during any period when
dosages are being adjusted. More frequent follow-up visits may be advisable when prescribing
opioid medication to a patient with a known addiction problem, suspected aberrant behavior, or
co-existing psychiatric or medical problems.
Options for medication adjustments include reducing medication or rotating opioid medication.
Opioid rotation can be an effective means of reducing opioid dose, reducing adverse side effects
or improving efficacy. However, when switching from one opioid to another, extreme caution is
required due to incomplete cross-tolerance among various opioids. Refer to opioid rotation
guidelines (in Module 2) before attempting an opioid switch (opioid rotation). When it is
documented that the patient is compliant with agreed-upon recommendations, the prescriber may
consider adding supplemental immediate-release/short-acting (IR/SA) medications for control of
break-through pain exacerbation to facilitate increases in activity.
In general, if the patient’s underlying medical condition is chronic and unchanging and if opioid-
associated problems (hyperalgesia, substantial tolerance, important adverse effects) have not
developed, it is recommended that the effective dose achieved through titration not be lowered
once the patient has reached a plateau of adequate pain relief and functional level.
9. Multi-Disciplinary Approach
Chronic Pain Recommendation 9.1: Obtain a Second Opinion or Consultation
Prescriber should obtain a consultation for a patient with complex pain conditions or serious
comorbidities.
A multidisciplinary approach for chronic pain may result in a better outcome compared to
medical management alone. The results generally indicate a reduction in pain, better functional
restoration, reduced healthcare costs, higher return-to-work rates, and reduced disability costs.
This approach involves a range of healthcare professionals specializing in pain management.
Often involved in a multidisciplinary approach are medicine, nursing, physical therapy,
pharmacy, psychology, and social work. These disciplines are integrated to address a problem
that reflects a complex web of biological, neurological, psychological, physical, and social
dysfunctions.
Page 53 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Patients with serious comorbidities may benefit from a Palliative Care consultation if the goal is
to improve a person’s quality of life while living with chronic or serious illness. These patients
usually have exhausted other traditional therapies for their illnesses (congestive heart failure,
COPD, advanced cancer) or live with a high symptom burden during treatment of their
illness. They are not hospice eligible, because they live longer than a traditional hospice patient
or may have aggressive medical goals. Patients that receive Palliative Care may have less
frequent hospitalizations, improved quality of life, and improved physical function. (April
Krutka, Palliative Care Medical Director, McKay Dee Hospital)
Chronic Pain Recommendation 9.2: Refer to a Substance Use Disorder Specialist for
Treatment
Patients at high risk for Substance Use Disorder (SUD) or those exhibiting behaviors of abuse,
diversion, or addiction should be considered for referral to a SUD specialist for treatment.
Reasons to refer patients include:
• The prescriber has reached a limit of what he or she feels comfortable prescribing.
• The treatment needs a multi-disciplinary approach.
• The pain has progressed to a complex level.
• Significant risk factors for substance use disorder are identified.
• There is a need to re-evaluate the patient’s diagnosis and/or confirm the continued
diagnosis.
Find Substance Abuse Agencies by county at https://dsamh.utah.gov/substance-use-disorders/.
Also, see Material Resources Tab for a list of Opioid Use Disorder Providers.
Offering, soliciting, paying, or promising to pay, or receiving remuneration for the referral of an
individual for substance use disorder treatment is a third-degree felony. Remuneration includes any
commission, bonus, kickback, bribe or rebate, directly or indirectly, overtly or covertly, in cash or
in-kind, or engaging in any split-fee arrangement. Some exceptions apply. Utah Code 62A-2-116(5)
Chronic Pain Recommendation 9.3: Offer Medication-Assisted Treatment
Prescribers should offer or arrange evidence-based treatment for a patient with opioid use
disorder, which usually includes medication-assisted treatment with buprenorphine, naltrexone
or methadone in combination with behavioral therapies.
The prescriber may consider opioid medication for pain when monitoring is performed during the
titration and maintenance phase and the patient understands and consents to the risks, even if the
patient has a self-reported or documented previous problem with opioids. Opioid treatment in this
case requires more structured ongoing assessment for loss of control and nonadherence. Co-
management with or a referral to an addiction medicine specialist is recommended. The specialist is
required to have a special registration to provide medication-assisted treatment; otherwise, there is a
provision in the Controlled Substance Act in which the provider may apply to receive a waiver of
the special registration requirements to treat with buprenorphine. This can be done through the
Substance Abuse Mental Health Services Administration Buprenorphine Waiver Management at
https://www.samhsa.gov/medication-assisted-treatment/training-materials-resources/buprenorphine-
waiver.
Page 54 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Note: The 2017 CDC Guideline’s recommendation about dosage applies to use of opioids in the
management of chronic pain, not to the use of medication-assisted treatment for opioid use
disorder. The Guideline strongly recommends offering medication-assisted treatment for patients
with opioid use disorder.
Chronic Pain Recommendation 9.4: Refer to Mental Health Services
Patients with co-existing psychiatric disorders should receive ongoing mental health support and
treatment while being treated for chronic pain.
Unless the prescriber treating the patient is qualified to provide the appropriate care and
evaluation of the coexisting psychiatric disorder, consultation should be obtained to assist in
formulating the treatment plan and establishing a plan for coordinated care of both the chronic
pain and psychiatric conditions.
Because psychological distress frequently interferes with improvement of pain and function in
patients with chronic pain, use validated instruments such as the Generalized Anxiety Disorder
(GAD)-7, the Patient Health Questionnaire (PHQ)-9 or PHQ-4, and Opioid Abuse Risk Screener
(OARS) to assess for anxiety, post-traumatic stress disorder, and/or depression.
Opioid therapy should not be initiated during acute psychiatric instability or uncontrolled suicide
risk, and prescribers should consider behavioral health specialist consultation for any patient
with a history of suicide attempt or psychiatric disorder. In addition, patients with anxiety
disorders and other mental health conditions are more likely to receive benzodiazepines, which
can exacerbate opioid-induced respiratory depression and increase risk for overdose. For
treatment of chronic pain in patients with depression, prescribers should strongly consider using
tricyclic or SNRI antidepressants for analgesic as well as antidepressant effects.
10. Discontinuing Opioid Treatment
Chronic Pain Recommendation 10.1: Discontinue Treatment
Opioid treatment should be discontinued when pain problems have been resolved, treatment
goals are not being met, adverse effects outweigh benefits, or dangerous or illegal behaviors are
demonstrated.
Dangerous or illegal behaviors may include frequent request for refills prior to expected use date,
positive urine drug screens for non-prescribed medications, negative urine drug screens for
opiates that have been prescribed and the patient states they are taking, and suspicion of diverting
medications to others.
The decision to discontinue opioid treatment should ideally be made jointly with the patient and
the family/caregivers when appropriate. This decision requires careful consideration of the
treatment outcomes and the need to provide ongoing monitoring.
When the patient is discharged, the prescriber is obliged to offer continued monitoring for 30
days post-discharge. Once a provider-patient relationship is established, the prescriber owes a
Page 55 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
continuing duty to provide care until that relationship is appropriately terminated. Prescribers
should adhere to the standard of care for their specific discipline when dismissing a patient. The
failure to do so may constitute neglect or abandonment.
When it is beneficial or necessary to discontinue opioid or controlled substance treatment, the
prescriber needs to develop a treatment plan to taper the medication. Using a documented taper
plan can help prescribers safely discontinue treatment by gradually and methodically weaning
patients off the medication. A treatment plan will allow time for the patient to adjust to the
physical and psychological changes. It is often useful to allow the patient to help create the
tapering schedule, so the patient feels more confident in achieving the desired outcome.
A rapid decrease of any opioid or controlled substance medication may cause withdrawal
symptoms, including cramps, diarrhea, fast heartbeat, sweating, and body aches. Withdrawal
risks are higher with longer treatment and higher doses. Some patients may require
pharmaceutical management, (e.g. clonidine) to mitigate withdrawal symptoms Some patients
may experience severe and potentially life-threatening signs and symptoms during controlled
substance withdrawal, requiring acute care.
Chronic Pain Recommendation 10.2: Safely Taper and Refer to Treatment
When a patient chooses to stop treatment or has been discharged for agreement violations, offer
assistance to safely taper medications or obtain appropriate treatment.
When tapering a patient from opioid treatment, the rate of taper will depend on the patient’s
medical, social and mental health factors. Medicine should be dispensed in small increments, no
more than a weekly supply.
When tapering or discontinuing opioids, the CDC announces, “The [2017 CDC] Guideline does
not support abrupt tapering or sudden discontinuation of opioids. These practices can result in
severe opioid withdrawal symptoms including pain and psychological distress, and some patients
might seek other sources of opioids. In addition, policies that mandate hard limits conflict with
the Guideline’s emphasis on individualized assessment of the benefits and risks of opioids given
the specific circumstances and unique needs of each patient.” A CDC Clinical Pocket Tapering
Guide is available and can be found in the Material Resources Tab.
For prescribers who are not familiar with opioid tapering within the context of pain care (i.e., no
opioid use disorder co-morbidity), consultation with a pain medicine specialist is recommended.
If opioid use disorder is suspected, consultation with a SUD specialist is recommended.
Patients receiving both benzodiazepines and opioids require tapering to reduce risk for fatal
respiratory depression. It might be safer and more practical to taper opioids first, because there is
a greater risk of benzodiazepine withdrawal relative to opioid withdrawal and tapering opioids
can be associated with anxiety. Prescribers should taper benzodiazepines gradually, because if
discontinued abruptly, this may cause withdrawal with rebound anxiety, hallucinations, seizures,
delirium tremens, and, in rare cases, death. A commonly used benzodiazepine tapering schedule
that has been used safely and with moderate success is a reduction of the benzodiazepine dose by
25% every 1–2 weeks.
Page 56 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
11. Methadone
Chronic Pain Recommendation 11: Avoid Methadone Unless Trained
Methadone should not be used for pain unless the prescriber has extensive training or experience
in its use and when the benefits outweigh the known risks.
Methadone has highly complex and variable pharmacokinetics and pharmacodynamics, making
it unsuitable as a preferred (1st or 2nd line) extending-release/long-acting (ER/LA) opioid
analgesic for the management of chronic pain when around-the-clock opioids are indicated. Its
use for this indication has been associated with a disproportionately high incidence of
prescription opioid-related deaths.
Methadone is one option for maintenance therapy for opioid addicted patients who have been
transitioned from their other opioid medications, and under a frequent urine drug screening plan.
The DEA requires special registration as a Narcotic Treatment Program (NTP) for prescribers to
use methadone for this purpose. Buprenorphine is another option for long-term therapy of opioid
use disorder.
An ECG screening should be performed on patients who will be receiving methadone.
Caution: Anti-depressants may prolong the QT interval and increase the risk of cardiac death
when taken with methadone.
According to the methadone packaging information, Life-Threatening QT Prolongation Cases of
QT interval prolongation and serious arrhythmia (torsades de pointes) have been observed during
treatment with methadone. These cases appear to be more commonly associated with, but not
limited to, higher dose treatment (> 200 mg/day). The evidence strongly suggests that methadone
possesses the potential for adverse cardiac conduction effects in some patients.
Opioid therapy used effectively and responsibly should improve a patient’s function and quality
of life. However, patients should not expect absolute relief from pain when using opioid therapy.
Prescribers should only continue opioid prescribing as long as the patient’s function and pain
improve.
Summary of Module These resources have contributed to the educational content in this module:
Utah Department of Health (2018). Utah Clinical Guidelines on Prescribing Opioids for
Treatment of Pain. Salt Lake City, UT: Utah Department of Health
Centers for Disease Control and Prevention. [Patients with Mental Health Conditions]. MMWR
2016;65(No. 1)
Federation of State Medical Boards of the United States, Inc. (2004). Model Policy for the Use of
Controlled Substances for the Treatment of Pain.
Federation of State Medical Boards of the United States, Inc. (July 2013). Model Policy on the
Use of Opioid Analgesics in the Treatment of Chronic Pain.
Federation of State Medical Boards of the United States, Inc. (July 2017). Guidelines for the
Chronic Use of Opioid Analgesics.
The Extended-Release and Long-Acting Opioid Analgesics Risk Evaluation and Mitigation
Strategy Program, http://www.er-la-opioidrems.com/IwgUI/rems/home.action.

Page 57 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved.
No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Substance Abuse and Mental Health Services Administration. [Naloxone]. (2016, March 03).
Retrieved June 28, 2017, from https://www.samhsa.gov/medication-assisted-
treatment/treatment/naloxone
Substance Abuse and Mental Health Services Administration. [Buprenorphine Waiver
Management]. (2017, February 09). Retrieved October 30, 2017, from
https://www.samhsa.gov/medication-assisted-treatment/buprenorphine-waiver-management
Department of Veterans Affairs, Department of Defense. (2003) VA/DoD Clinical Practice
Guideline for the Management of Opioid Therapy for Chronic Pain
Advance to Module 5 on the next page.
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Controlled Substances: Education for the Prescriber
Presented by the Utah Medical Association Foundation –
“Extending the Reach of the Healer’s Hand.”
MODULE 5
Patient Education
Learning Objectives
After completing this module, you should be able to
1. List the topics that should be discussed with patients receiving controlled substances.
2. Incorporate required discussions with patient or guardian/caregiver before issuing initial opiate
prescription as specified in Utah Code 58-37-19.
3. Explain patient expectations for controlled substance use regarding pain relief vs. improved
function.
4. Instruct patients and/or caregivers on how to recognize a suspected overdose and administer
Naloxone in an overdose crisis.
Patient Education
The Utah Department of Health recommends that all patient education be provided in written
form and discussed in person and, when applicable, with the family or caregivers. However,
prescribers must remain within the constraints of the Health Insurance Portability and
Accountability Act, commonly called (HIPAA).
Informed consent is important when treating all patients, especially those receiving controlled
substance therapy. As mentioned in the previous module, the informed consent is usually
combined with the treatment agreement.
The informed consent document typically includes:
• potential risks and benefits of controlled substance use, including the risk of misuse,
dependence, addiction, overdose, and death;
• adverse effects;
• likelihood of tolerance and dependence developing;
• possible drug interactions and over-sedation, particularly the dangers of taking opiates
with alcohol, benzodiazepines, and other central nervous system depressants;
• limited evidence of the benefit of long-term opioid therapy;
• impairment in operating motor vehicles or equipment or performing other tasks;
• prescriber’s policies and expectations; and
• specific reasons for adapting or discontinuing drug therapy.
Informed
Informed consent should also include explaining to patients that they should not expect complete
relief of their pain. Improved function is the main criterion for continuing controlled substance
treatment.
Page 59 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Before issuing an initial opiate prescription*, a prescriber must discuss with the patient, or the
patient's parent or guardian:
• the risks of addiction and overdose associated with opiate drugs;
• the dangers of taking opiates with alcohol, benzodiazepines, and other central nervous
system depressants;
• the reasons why the prescription is necessary;
• alternative treatments that may be available; and
• the risks associated with the use of the drugs being prescribed.
* “Initial opiate prescription” includes a prescription for a patient who was last prescribed an
opiate more than a year ago.
This discussion is not required for:
• a patient who is currently in active treatment for cancer;
• a patient who is receiving hospice care from a licensed hospice; or
• a medication that is being prescribed to a patient for the treatment of the
patient's substance abuse or opiate dependence.
Utah Code 58-37-19
To ensure the safety of patients, educate patients and their caregivers on the correct use, storage,
and disposal of drugs.
Patient and Caregiver
Set clear rules about drug use. Clearly explain exactly what they are receiving and how to safely
take the medications. Also, explain that medications are not meant to be shared, and patients
should always follow the prescriber’s advice and dosage. Warn patients that medications should
never be broken, chewed or crushed and patches should not be cut or torn prior to use. and
Caregiver Education (
As recommended, co-prescribe naloxone and educate on the proper administration of naloxone.
Explain naloxone may reverse an overdose of opiate drugs. Naloxone may not be effective if
opioids are misused in combination with other sedatives or stimulants. It is not effective in
treating overdoses of benzodiazepines or stimulant overdoses involving cocaine and
amphetamines.
See Instructions for Naloxone Administration in the Tools and Resources section. These
instructions may be printed and given to the patient when naloxone is co-prescribed. Additional
information and patient materials can be found at naloxone.utah.gov in addition to a list of
pharmacies that stock and dispense naloxone.
Explain that lost or stolen medication will not be replaced or refilled early. The only exception to
this rule would be when the patient is experiencing serious withdrawal symptoms.
Patient and Caregiver Education (
Ensure the patient and caregivers understand that medications should never be mixed with
sedative hypnotics, alcohol or other medications like sleep aids or anti-anxiety medications. A
missed dose may be taken at a later time if the pain merits the dose. However, the patient must
maintain the prescribed interval between doses.
Page 60 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Under no circumstance should a patient increase their dose of pain medication. Patients should
contact their prescriber if pain is not controlled or patient experiences troublesome adverse
effects.
Documenting Patient
Stop the Opidemic is a public awareness campaign designed to prevent and reduce misuse,
abuse, and overdose of opioids in Utah. The campaign focuses on opioid risks, signs of an
overdose, and naloxone. The website, http://www.opidemic.org/, offers information about
treatment facilities in addition to provider resources and tools.
Use Only As Directed is a public awareness campaign focused on the areas of Opt Out, Throw
Out, and Speak Out. The campaign encourages the public to opt out of taking opioids to manage
pain, dispose of prescriptions properly, and to engage in conversations with their provider about
alternative treatments to pain.
Storage and Diversion Reduction of Controlled Substances
It is imperative that prescribers remind patients to keep controlled substance medications in a
secure location. Prescribers should provide information to patients and their caregivers on ways
to dispose of their extra medication. The preferred method for disposing of unused controlled
substances is dropping the medication off at a collection site. The website
https://useonlyasdirected.org/throw-out/, offers information on drop box locations.
Controlled substances can be effective, yet they have a high-risk factor. Therefore, prescribers
must educate the patient and the caregivers in each step of the treatment and ensure all involved
parties understand that improvement in function and quality of life are the goals.
These resources have contributed to the educational content in this module:
Federation of State Medical Boards of the United States, Inc. (2004). Model Policy for the Use of
Controlled Substances for the Treatment of Pain.
Federation of State Medical Boards of the United States, Inc. (July 2013). Model Policy on the
Use of Opioid Analgesics in the Treatment of Chronic Pain.
Use Only as Directed http://useonlyasdirected.org
Utah Department of Health (2009). Utah Clinical Guidelines on Prescribing Opioids for
Treatment of Pain. Salt Lake City, UT: Utah Department of Health
Hall AJ, et al. JAMA 2008;300:2613
Intermountain Healthcare. (n.d.). Managing chronic pain: Reclaiming your life. Patient and
Family Education
Castillo, M. and Tirado, M.D., C. (2013, February 20), With Drug Overdose Deaths on Rise,
Experts Push to Recognize Signs of Addiction. CBS News. http://www.cbsnews.com/8301-
204_162-57570385/with-drug-overdose-deaths-on-rise-experts-push-to-recognize-signs-of-
addiction/
Advance to Module 6 on the next page.
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Controlled Substances: Education for the Prescriber
Presented by the Utah Medical Association Foundation –
“Extending the Reach of the Healer’s Hand.”
MODULE 6
Utah Medical Cannabis
Learning Objectives
After completing this module, you should be able to
1. Describe the difference between delta-9-tetrahydrocannabinol (THC) and cannabidiol
(CBD).
2. Define the types of medical cannabis providers and their requirements and restrictions.
3. Be familiar with the qualifying medical conditions for cannabis treatment in Utah and
any associated restrictions.
4. Explain the contraindications of cannabis treatment.
Marijuana is the most commonly used addictive drug after tobacco and alcohol. The rates of use
have increased, especially by adolescents, because the perception of risk has declined over the
last two decades. Emergency department visits have also increased. It is uncertain whether it is
due to increased use, increased potency of the marijuana, or other factors. The State of Utah,
through legislation, has limited marijuana use for medicinal purposes only and has defined what
constitutes a qualified medical condition. As a Utah provider, there are requirements and
limitations in recommending medical cannabis.
For complete and comprehensive information about the Utah Medical Cannabis Program, you
may go to: https://medicalcannabis.utah.gov/.
The Endocannabinoid System
Human beings have receptors that are specific for cannabinoids, known as CB1 and CB2. In
fact, humans produce two chemicals that interact with this system that are nearly identical to
THC; and two chemicals that interact with this system that are nearly identical to CBD.
Medicinal cannabis preparations are intended to interact with this system to address specific
diseases and/or symptoms. These preparations can range from CBD products with essentially no
THC (see below), to products with varying mixtures of THC and CBD. The cannabis plant can
produce up to 114 physiologically active compounds (cannabinoids); but to date, there is only
information about the effects of THC and CBD. Some patients benefit from a product containing
several other, minor cannabinoids and terpenes (chemicals that impart flavor and smell, along
with other effects, in addition to whatever CBD and THC is present. This has been called the
“entourage” effect.
THC and CBD
The two primary elements of marijuana are delta-9-tetrahydrocannabinol (THC) and cannabidiol
(CBD). THC is the main psychotropic ingredient of marijuana that leads to intoxication and to
Page 62 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
potential substance abuse disorder (addiction). THC can have important therapeutic effects at
doses that will not cause an abuse disorder. When CBD is taken in conjunction with THC, the
CBD can block most, if not all, of the psychotropic effects. CBD is not intoxicating and does not
lead to addiction. It was the first form of cannabis approved in the state of Utah to treat seizure
disorders.
Subsequently, an FDA approved form of CBD (Epidiolex) has been approved for two, specific
types of seizures. For some patients, CBD can prove helpful for other types of seizures. CBD
products do not have to be sold in medical cannabis pharmacies as long as those products contain
less than 0.3% of THC. The Utah licensed medical cannabis pharmacies ensure that the contents
of their products, THC and CBD, are pure (without any additives).
Medical Cannabis Delivery Methods
Cannabis products come in many forms. There are oils that can be used for vaporization, or
sublingually, or ingested. There are tablets, capsules, liquid suspensions and cubes that are for
ingestion. There are also topical preparations, such as balms and lotions. One of the most
popular forms is unprocessed cannabis flower that can be ingested or vaporized. Smoking is
prohibited in Utah, and smoking destroys 20% of the cannabinoids present in the flower. A
major appeal of cannabis flower is the “entourage” effect, since this unprocessed form will
contain numerous cannabinoids and terpenes in addition to the THC and CBD content.
Patients need the correct dosage for maximum effect. The Start Low, Go Slow approach applies
to medical cannabis as well. Higher dosages do not necessarily lead to better results; in fact, it
can have the opposite effect. If the prescriber is uncomfortable recommending the dosage type or
amount of medical cannabis, the registered pharmacy medical provider is qualified to
recommend the form and dosage based on the prescriber’s recommendation. By law, the
pharmacy should label the content in mg of both the THC and CBD in the package received.
This will help the prescriber to follow-up with the patient on the efficacy of the treatment and
what adjustments may be needed.
Common dosage amounts:
CBD: 2.5 – 10 mg/kg p.o. in 2 divided doses
THC: 2-10 mg p.o.q8h
Greater than 30 mg/day of THC is associated with increased adverse effects.
While most medications delivered to ambulatory patients are delivered in oral form (capsule,
tablet, liquid), medical cannabis preparations come in several forms. It is important to understand
the time to onset of the preparation and the duration of the effects.
Inhalation: onset in seconds to minutes, peak blood level in 30 minutes; duration 2-4 hours.
Sublingual or oromucosal: onset in 15-45 minutes; duration 90 minutes to several hours.
Oral/edible: onset in 1-3 hours, duration 6-8 hours.
Topical: variable onset and duration.
Suppositories: onset in 15-45 minutes; duration 2-4 hours.
Page 63 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Provider Types
Qualified Medical Provider (QMP), including physicians, nurse practitioners, physician
assistants, and podiatrists, may recommend up to 275 active cardholders. Becoming a QMP
(QMP) requires an initial 4-hour training that has been approved by the Utah Department of
Health. Continuing education is required each license renewal period. Providers must hold a
Utah Controlled Substance License.
Qualified Medical Provider (QMP) with Board Certification in certain sub-specialties,
including anesthesiology, gastroenterology, neurology, oncology, pain, hospice and palliative
medicine, physical medicine and rehabilitation, rheumatology, endocrinology, or psychiatry, may
recommend up to 600 cardholders. The same initial training and continuing education is
required, and providers must hold a Utah Controlled Substance License.
Limited Medical Provider (LMP)
New legislation allows physicians, nurse practitioners, physician assistants, and podiatrists to
recommend medical cannabis treatment for up to 15 patients without being a QMP. This
provides a way for patients to remain with existing practitioner when patient could benefit from
medical cannabis without having to find a QMP. Providers must hold a Utah Controlled
Substance License.
LMP can only recommend for patients 21 years and older and the patient must have a qualifying
condition.
Provider-Patient Relationship
Initial in-person visit is required to recommend cannabis treatment. QMP/LMP may only
recommend medical cannabis treatment to a patient in the course of the provider-patient
relationship after completing and documenting in the patient’s record a thorough assessment of
the patient’s condition and medical history. This assessment must include a check of the Utah
Controlled Substances Database to identify possible concerns with adding medical cannabis to
the patient’s treatment plan.
Legal Protections for Medical Providers
Although Federal law has not changed, the Utah Department of Occupational and Professional
Licensing (DOPL) or Utah law enforcement will not penalize a provider when following Utah
Cannabis law.
Medical Cannabis Cards
A patient seeking medical cannabis treatment must obtain a medical cannabis card from the State
of Utah. The card application must be completed using the online Electronic Verification System
(EVS). The medical cannabis card is valid at any of the fourteen licensed pharmacies located in
Utah. See below for explanation of the Compassionate Use Board.
Patient Card – Patient must be 21 years and older when the provider certifies the patient has a
qualifying condition and provider is willing to make a recommendation for medical cannabis
treatment. If a patient is under 21 years of age, the Qualified Medical Provider (QMP) must
Page 64 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
submit a petition to the Compassionate Use Board (CUB) with detailed medical information that
justifies the use of a product containing THC.
Caregiver Card – Caregiver must be 21 years or older and pass a federal criminal background
check. Facilities may be designated as a caregiver, including assisted living facility, nursing care
facility, or general acute hospital. Patients less than 21 years of age with designated caregiver
must be approved through the Compassionate Use Board.
Provisional Patient Card/Guardian Card (issued simultaneously) – Patients under the age of 18
will receive a provisional patient card if: 1) minor has qualifying condition, 2) QMP
recommends medical cannabis treatment, 3) petition is approved by the Compassion Use Board
and 4) minor’s guardian is eligible for the guardian card. Guardian of patients under 18 years of
age must obtain a guardian card in which the process will include a background check.
Non-Resident Patient Card – Non-Utah residents may obtain a card for no more than two visits
of 21 days or less and must have existing medical cannabis card or equivalent from another state,
district territory, commonwealth, or insular possession of the US for qualifying conditions.
Qualifying Medical Conditions
Medical Providers may recommend a medical cannabis card for patients with the following
qualifying medical conditions:
• Chronic Pain -lasting longer than two weeks and that is not adequately managed despite
treatment attempts using conventional medications or physical interventions.
• HIV or AIDS
• Alzheimer’s Disease
• Amyotrophic Lateral Sclerosis (ALS)
• Cancer
• Cachexia
• Persistent nausea under certain conditions
• Crohn’s Disease / Ulcerative Colitis
• Epilepsy / Debilitating seizures
• Multiple Sclerosis (MS) or persistent muscle spasms
• Post Traumatic Stress Disorder (PTSD) which must be diagnosed and treated by a
licensed mental health therapist and has been diagnosed by either the VA or through an
evaluation by a psychiatrist, or a Master’s level psychologist, LCSW, or a Psych-APRN.
• Autism
• Terminal illness with less than 6 months to live
• A condition resulting in the patient receiving hospice care
• A rare condition or disease that affects less than 200,000 individuals in the US and is not
adequately managed by a non-opioid or physical intervention.
For guidance on the suggested use of medical cannabis for these conditions, go to
https://medicalcannabis.utah.gov/resources/provider-resources/medical-cannabis-guidance/
Contraindications
Providers must take precautions when working with a patient using or desiring to use medical
cannabis.
Page 65 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
Pregnancy– There is conclusive evidence marijuana use by a pregnant woman is associated with
a low birth weight infant, 2.3 times more risk of still birth, increase the chance of a child with
autism, and negatively affecting the fetus’ brain development.
Breastfeeding – One study suggests a nursing mother can expose an her infant to THC through
breast milk. This can result in decreased motor developments at one year of age and can
adversely affect brain development.
Psychiatric – Marijuana increases risk of psychosis, particularly schizophrenia, in vulnerable
populations, and this risk is influenced by the frequency of use and the levels of THC. The
greatest concern is for patients with a prior history of schizophrenia, those currently being treated
for schizophrenia, or those having a family history of schizophrenia.
Hypomanic symptoms and PTSD – Marijuana use may increase the risk of developing
psychiatric disorders.
Blood Thinning – Marijuana inhibits the metabolism, thus increasing the anticoagulant effect of
warfarin (Coumadin) and Direct Oral Anticoagulants (DOACs).
Substance Use Disorder – Marijuana increases dopamine levels. THC stimulates neurons in the
reward system to release the signaling chemical dopamine at levels higher than typically
observed in response to natural rewarding stimuli. The surge of dopamine “teaches” the brain to
repeat the rewarding behavior, helping account for marijuana’s addictive properties.
Low Blood Pressure – Immediately after consumption blood pressure usually rises and then will
soon drop.
Heart Conditions – Heart rate may increase by 20 to 50 beats per minute. Because marijuana
increases the heart rate and blood pressure, this effect can also adversely impact patients with
existing heart disease.
Compassionate Use Board (CUB)
Individuals who do not have a “qualifying condition” may request that their QMP provider
submit a petition to the Compassionate Use Board (CUB) for review and recommendation for
department approval. To be considered, a patient must have a qualifying and intractable
condition which substantially impairs the individual’s quality of life and has not adequately
responded to conventional treatments. All patients under the age of 21, regardless of their
medical condition, must have their application reviewed by the Board.
QMPs will need to complete the petition and upload to the Electronic Verification System
(EVS). The following information is required:
• Petition Form, including details of the condition or symptoms for which the medical
cannabis will treat, and history of the standard treatment modalities, including the results
of the previously tried treatments;
• A Subjective Objective Assessment and Plan (SOAP) note from the face-to-face
evaluation with the Qualified Medical Provider. See sample Cannabis SOAP template in
the material resources tab. Telehealth visits are not accepted;
• An evaluation of any current or past cannabis treatment as related to the condition;
• For PTSD, documentation of this diagnosis by a licensed mental health provider;
confirmation of current treatment under the care of a licensed mental health provider;
and a letter from the mental health provider indicating the diagnosis and that they are
aware of the decision to seek medical cannabis; and
Page 66 of 66
Copyright ©2021 The Utah Medical Association Foundation. All rights reserved. No copyright is claimed in text and data from government and other sources quoted within this work. Submit requests for permission to copy
material to The Utah Medical Association Foundation, 310 East 4500 South, Suite 500, Salt Lake City, UT 84107, telephone 801-747-3500.
• Any past treatment records from previous primary care physicians and or specialty
providers that provide a record of the condition’s past treatments of symptoms.
Electronic Verification System (EVS)
The electronic verification system (EVS) is Utah State’s system for tracking medical cannabis
recommendation and dispensing and for communicating medical cannabis dispensing
information to the controlled substance database (CSD). (The exchange system from the EVS to
the CSD still needs to be developed.)
These resources have contributed to the educational content in this module.
Utah Department of Health (2021). Utah Medical Cannabis Program.
https://medicalcannabis.utah.gov/ Salt Lake City, UT: Utah Department of Health
National Institute on Drug Abuse (2020), Marijuana Research Report – What is the scope of
Marijuana Use in the United States?, https://www.drugabuse.gov/publications/research-
reports/marijuana/what-scope-marijuana-use-in-united-states
U.S. Surgeon General Advisory, 2019, Marijuana Use and the Developing Brain
What’s Next
As a prescriber, you should carefully consider your own prescribing practices and determine if
you are appropriately assessing your patients for pain treatment and providing the appropriate
choice, the proper strength, and the correct amounts of controlled substances to your patients.
It is your responsibility to provide the patient with appropriate care and educate patients of the
risks, proper use, storage, and disposal of controlled substances.
Appropriately applying the recommendations and guidelines from this education into your
prescribing practices can help protect your practice, offer your patients safe and effective pain
management, and reduce the negative effects of controlled substances in Utah.
Congratulations on completing the Controlled Substances: Education for the Prescriber series.
In order to be awarded participation or credit for this course, you must complete each module
exam and the program evaluation. Then, a Certificate of Completion can be generated by going
to the next “component” of the course, where you may print the certificate for your records.