Embed Size (px)
Citation preview

CONVERSION FROM INTRAVENOUS TO ORAL DOSING
K.P. ARUNLECTURER
DEPARTMENT OF PHARMACY PRACTICEJSS COLLGE OF PHARMACY
OOTY
INTRODUCTION The ideal route of administration for any medication is one
that achieves serum concentrations sufficient to produce thedesired effect without producing undesired effects
In the past, patients were switched to oral (PO) therapy tocontinue treatment after an already adequate course ofintravenous (IV) therapy was administered
Today, it is not uncommon to convert a patient to PO therapyas part of the initial treatment course
The available oral formulations on the market are easier toadminister, safe, and achieve desired therapeuticconcentrations, thus making the PO route an ideal choice
INTRODUCTION… Patients are more comfortable if they do not have an IV
catheter in place
Attachment to an IV pole can restrict movement, which canhinder early and/or frequent ambulation
Patients who continue to receive parenteral therapy are at anincreased risk for infusion-related adverse events
In addition, the presence of an IV catheter provides a portalfor bacterial and fungal growth
These secondary infections can lead to additional antibiotictherapy, prosthesis failures, sepsis, and in a small number ofcases, death
Using PO therapy also reduces hidden expenses such as thecost of IV sets and pumps, laboratory monitoring, and nursingand pharmacy personnel time
Most significantly, early use of PO therapy may allow forearlier discharge from the hospital

TYPES OF IV TO PO THERAPY CONVERSIONS There are three types of IV to PO therapy conversions
1. Sequential Therapy
2. Switch Therapy
3. Step-down Therapy
Sequential Therapy:
Refers to the act of replacing a parenteral version of amedication with its oral counterpart
An example is the conversion of famotidine 20 mg IV tofamotidine 20 mg PO
There are many classes of medications that have oral dosageforms that are therapeutically equivalent to the parenteralform of the same medication

TYPES OF IV TO PO THERAPY CONVERSIONS…Switch Therapy:
Used to describe a conversion from an IV medication to the POequivalent that may be within the same class and have thelevel of potency, but is a different compound
An example is the conversion of IV pantoprazole to rapidlydissolving lansoprazole tablets or omeprazole capsules
Step-down Therapy:
Refers to converting from an injectable medication to an oralagent in another class or to a different medication within thesame class where the frequency, dose, and the spectrum ofactivity (in the case of antibiotics) may not be exactly thesame
Converting from ampicillin 3 g IV q 6 hr to amoxicillin 875 mgPO q 12 hr is an example of step-down therapy

SELECTION OF PATIENTS FOR IV TO PO THERAPY CONVERSION
Proper identification of patients, diagnoses, medications, andcontraindications to oral therapy are all essential aspects for asuccessful IV to PO therapy conversion program
It is very important that the pharmacist conduct a thoroughand complete review of these areas so only the mostappropriate patients are converted
Doing so is a benefit to both patient care and professionalcredibility
The criteria used to determine whether or not the patient iseligible for PO therapy vary from hospital to hospital, but theygenerally encompass four key areas:
1. Intact and functioning gastrointestinal (GI) tract
2. Improving clinical status
3. Does not meet any exclusion criteria
4. Others
SELECTION OF PATIENTS FOR IV TO PO THERAPY CONVERSION…
1. Intact and functioning gastrointestinal (GI) tract:
The ability of the GI tract to absorb the medication is criticalfor successful conversion to PO therapy
Factors that influence absorption include gastrointestinal pH,surface area, and permeability
Blood flow to the GI tract is also important, therefore, patientsdisplaying signs and symptoms of shock are not candidates forconversion to oral therapy because blood flow is typicallyshunted away from the GI track secondary to the shock itselfor due to concomitant vasopressor therapy

SELECTION OF PATIENTS FOR IV TO PO THERAPY CONVERSION…
Criteria Indicating Absorption of Oral Medications may beCompromised
NPO status (and no medications are being administeredorally)
NG tube with continuous suction Severe/persistent nausea or vomiting Gastrointestinal transit time too short for absorption
(malabsorption syndromes, partial or total removal of thestomach, short bowel syndrome)
Active gastrointestinal bleeding High doses of vasopressor medications (typically in
presence of shock) Difficulty swallowing or loss of consciousness and no NG
access available Documented ileus or gastrointestinal obstruction Continuous tube feedings that cannot be interrupted and
patient requires a medication known to bind to enteralnutrition formulas

SELECTION OF PATIENTS FOR IV TO PO THERAPY CONVERSION…
The following guidelines are provided to help manage theconversion from IV to PO therapy in the presence of continuoustube feeding
Select the most appropriate oral formulation of themedication for NG tube administration
Solutions or suspensions are preferred over tablets
If this is not available, a tablet can be crushed as long as itis not an extended-release or enteric-coated formulation
Dissolve the tablet in a small amount of liquid to make aslurry, and then draw the preparation into an oral syringefor administration
Once the medication has been administered, allequipment used in preparation and administration shouldbe rinsed, and those washings administered

SELECTION OF PATIENTS FOR IV TO PO THERAPY CONVERSION…
IV to PO therapy in the presence of continuous tube feeding –guidelines…
Feeding tubes should be flushed with water both beforeand after medication administration to avoid blockage
For medications considered to be compatible with tubefeeding, stop the feeding and administer the medicationas specified above
For oral fluoroquinolones, stop the tube feeding for atleast 2 hours before and 2 hours after administration
For phenytoin, which is dosed more than once a day, tubefeedings can be stopped approximately 1 hour before and1 hour after medication administration
Medications should never be added directly into the tubefeedings
SELECTION OF PATIENTS FOR IV TO PO THERAPY CONVERSION…
2. Improving Clinical Status:
Signs and symptoms of the condition for which themedication is prescribed should be improving or resolving inpatients being converted to PO therapy
The patient should be clinically stable and deteriorationshould not be expected
Following observations normally made to assess theappropriate clinical status for conversion of IV to PO
Patients with active infections who are receivingantibiotics should be afebrile or have had a maximumtemperature of less than 100.4o F in the previous 24hours
WBC count should be trending downward, indicatesthe patient’s inflammatory response associated withthe infection is declining

SELECTION OF PATIENTS FOR IV TO PO THERAPY CONVERSION…
Observations to assess clinical status for conversion of IV to PO…
It is important to examine the patient’s medicationtherapy for other medications that can cause anincrease or sustained high WBC count, such as steroids
In this case, if the patient meets all other criteria, asafe conversion to PO therapy can still be made
Conversely, patients who are neutropenic (commonlydefined as an absolute neutrophil count of less than 500cells/mm3) are typically excluded from IV to PO therapyconversion, but this can vary from institution toinstitution
It is also important to review the cultured pathogen(bacteria, fungus, etc.) and ensure that it is susceptibleto the oral medication

SELECTION OF PATIENTS FOR IV TO PO THERAPY CONVERSION…
Observations to assess clinical status for conversion of IV to PO…
If no pathogen is identified, the oral agent shouldcover commonly suspected pathogens based upon localsensitivities and/or infection type
When converting from IV to PO therapy, the selectedoral medication should have activity against theseorganisms in the absence of a positive bacterial culture
If gastrointestinal bleeding is present, documentationthat the bleeding has stopped should be verified beforeconverting to PO therapy
For cardiovascular medications, the patient shouldhave stable blood pressure and heart rate
For anticonvulsant medications, the patient shouldbe stable and not be actively seizing
If in doubt, review the chart or discuss with thepatient’s nurse

SELECTION OF PATIENTS FOR IV TO PO THERAPY CONVERSION…
3. Exclusion Criteria:
Antibiotics:
Oral therapy can be commonly used to treat a variety ofinfections
However, there are certain infections that should be treatedwith parenteral therapy due to the severity or location ofinfection
These include endocarditis, meningitis, brain abscess, orbitalcellulitis, other central nervous system infections,osteomyelitis, and endophthalmitis
Patients with multiple antibiotic allergies may be restricted totherapy choices that may only be available parenterally

SELECTION OF PATIENTS FOR IV TO PO THERAPY CONVERSION…
3. Exclusion Criteria…
Antiepileptic Medications:
Patients who are at risk for actively seizing or are unable totolerate oral medications without risk of aspiration are notappropriate candidates for PO therapy
Cardiovascular Medications:
Patients with unstable cardiac conditions or for whomfrequent dose changes are occurring (e.g., through IV driptitration) are not good candidates for PO therapy
4. Others:
Some hospitals may require that patients have received atleast one dose of intravenous medication or have beenhospitalized for at least 24 hours
PHARMACOECONOMICS OF IV TO PO THERAPY CONVERSION
Changing the route of administration from intravenous to oralresults in direct cost reductions (medication costs, supplycosts)
Personnel time spent preparing and administering doses isgreatly reduced
Proactive conversion to the oral formulation reduce the lengthof stay and save medication/supply costs and total hospitalcosts

GENERAL PHARMACOKINETIC AND PHARMACODYNAMIC ISSUES
Pharmacokinetic Considerations:
Bioavailability is a commonly referenced pharmacokineticparameter
For oral medications, bioavailability may be less due to thevariability in the rate and extent of dissolution of the oral formand the total amount that is absorbed into the systemiccirculation
When IV infusion is stopped, the serum concentrationdecreases according to first order elimination kinetics
Therefore, if the patient starts the dosage regimen with theoral drug product at the same time as the IV infusion isstopped, then the exponential decline of serum levels form IVinfusion should be matched by the exponential increase inserum drug levels from the oral drug product
GENERAL PHARMACOKINETIC AND PHARMACODYNAMIC ISSUES
Pharmacokinetic Considerations…
Following two methods can be used to calculate anappropriate oral dosage regimen for a patient whose conditionhas been stabilized by an IV drug infusion
Both methods assume that the patient’s plasma drugconcentration is at steady state
Method-I:
where S is the salt form of the drug and D0 / τ is the dosing rate
C∞av = SFD0 / k Vd τ
D0 / τ = C∞av k Vd / SF
GENERAL PHARMACOKINETIC AND PHARMACODYNAMIC ISSUES
Method-II:
This method assumes that the rate of intravenous infusion (mg/hr) isthe same desired rate of oral dosage
EXAMPLE:
An adult male asthmatic patient (age 55, 78 kg) has beenmaintained on an IV infusion of aminophylline at a rate of 34 mg/hr. Thesteady state theophylline drug concentration was 12 µg/mL and totalbody clearance was calculated as 3.0 L/hr. Calculate an appropriate oraldosage regimen of theophylline for this patient.
Given: Aminophylline is a soluble salt of theophylline and contains 85%theophylline (S=0.85)
Theophylline is 100% bioavailable (F = 1)after an oral dose

GENERAL PHARMACOKINETIC AND PHARMACODYNAMIC ISSUES
Solution:
Method - I
But, total body clearance (Cl T) = k Vd
Therefore,
D0 / τ = C∞av ClT/ SF
The dose rate (34 mg/hr) was calculated on the basis ofaminophylline
The patient however will be given theophylline orally To convert to oral theophylline, S and F should be considered
D0 / τ = C∞av k Vd / SF
GENERAL PHARMACOKINETIC AND PHARMACODYNAMIC ISSUES
Oral theophylline dose rate = SFD0 / τ = (0.85) (1) (34) / 1
= 28.9 mg / hr Therefore the total daily dose is 28.9 mg/hr x 24 hr or 693.6
mg/day Possible theophylline schedules might be 700 mg/day The dose of 350 mg every 12 hours could be given in
sustained-release form to avoid any excessive high drugconcentration in the body
Method-II
Rate of IV infusion is 34 mg/hr and so the daily dose is 34 mg/hrx 24 = 816 mg/day
The equivalent dose in terms of theophylline is 816 x 0.85 =693.6 mg
Thus the patient should receive approximately 700 mg oftheophylline per day or 350 mg every 12 hours

GENERAL PHARMACOKINETIC AND PHARMACODYNAMIC ISSUES
Pharmacodynamic Considerations:
The ideal oral medication should possess properties that resultin minimal disruption to the treatment course
The medication should have recognized activity toward theinfection or condition being treated and its use should besupported by clinical trials
To improve patient compliance, the medication should beavailable in dosage forms that do not limit the patient’s abilityto tolerate the medication
Ingesting large tablets or capsules or having to take multipledoses per day is not desirable

GENERAL PHARMACOKINETIC AND PHARMACODYNAMIC ISSUES
Specific Medication Class Considerations:
Fluoroquinolones are ideal for conversion because of highbioavailability, rapid absorption, and good distribution withinthe body
But their absorption may be affected by concurrentadministration of products containing divalent and trivalentcations such as calcium, calcium containing antacids, iron andzinc salts
Hence administration of these compounds couple of ourbefore or after is preferred
Triazole antifungals especially Itraconazole is unique amongthe triazoles in that it requires an acidic gastric pH forabsorption
Antacids, H2 receptor antagonists, and proton-pumpinhibitors can significantly reduce itraconazole’s bioavailability
GENERAL PHARMACOKINETIC AND PHARMACODYNAMIC ISSUES
Specific Medication Class Considerations…
Vancomycin is unique because it is one of the few medicationswhere the oral and IV formulations have different uses
The IV formulation is used to treat gram positive bacterialinfections
However, the oral formulation is poorly absorbed and istypically only used in the treatment of Clostridium difficilecolitis
This medication should not be included in an IV to PO therapyconversion program
Because of their mechanism of action, the proton pumpinhibitors (PPIs) are most effective when administered on anempty stomach or at least 30 minutes to 1 hour prior to meals

GENERAL PHARMACOKINETIC AND PHARMACODYNAMIC ISSUES
Oral Bioavailability of Selected Medications Available in Both IVand PO Formulations:
BIOAVAILABILITY
< 50 % 50 % TO 80 % 80 % TO 100 %
AcyclovirAzithromycinCefuroximeDiltiazemFamotidineGanciclovirRanitidine
CefiximeCefpodoximeCimetidineCiprofloxacinDexamethasoneDigoxinItraconazoleLevothyroxineMetoprololPantoprazole
AmoxicillinCephalexinClindamycinDoxycyclineEsomeprazoleFluconazoleHydrocortisoneKetorolacLansoprazoleLevetiracetamLevofloxacinLinezolidMethylprednisoloneMetronidazoleMoxifloxacinPhenytoinSulfamethoxaxole/trimethoprimWarfarin

Medications That Can Be Included in IV to PO Therapy ConversionPrograms:
Category Sequential / Switch Therapy Step-down Therapy(Oral Equivalent)
Antibacterials Azithromycin, cefuroxime,ciprofl oxacin, clindamycin,doxycycline, levofl oxacin,linezolid, metronidazole,moxifloxacin, sulfamethoxazole/trimethoprim
Ampicillin (amoxicillin), ampicillin / sulbactam (amoxicillin / clavulanate),Piperacillin / tazobactam(multiple options), ticarcillin / clavulanic acid(multiple options), aztreonam (ciprofloxacin or levofl oxacin), cefazolin(cephalexin), cefotaxime/ ceftriaxone (cefpodoxime orcefuroxime), ceftazidimeor cefepime (ciprofl oxacin orlevofloxacin)
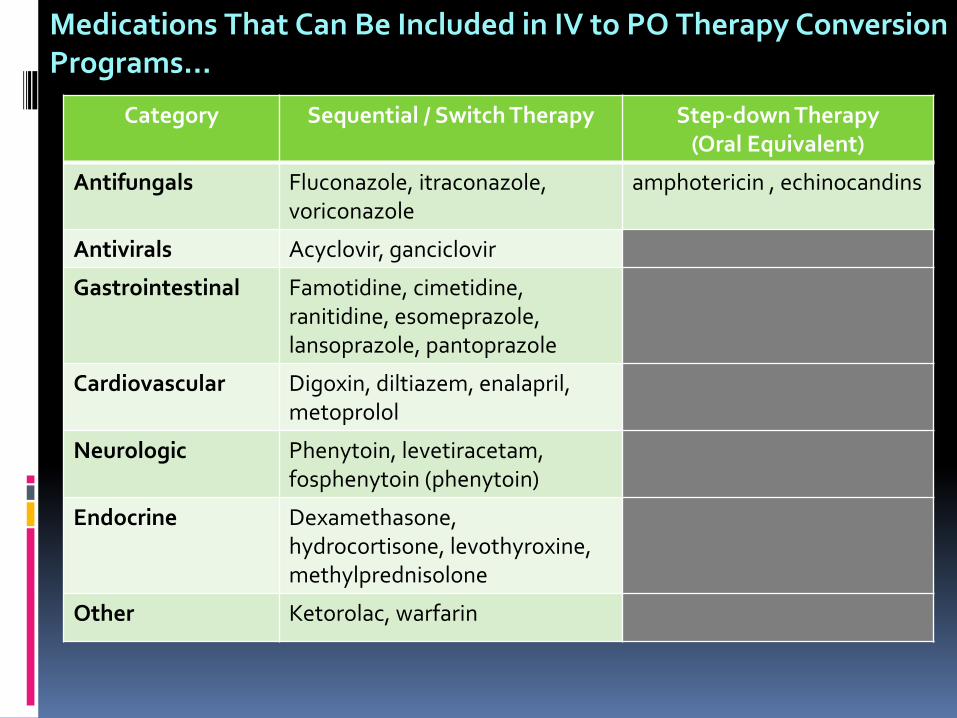
Medications That Can Be Included in IV to PO Therapy ConversionPrograms…
Category Sequential / Switch Therapy Step-down Therapy(Oral Equivalent)
Antifungals Fluconazole, itraconazole,voriconazole
amphotericin , echinocandins
Antivirals Acyclovir, ganciclovir
Gastrointestinal Famotidine, cimetidine,ranitidine, esomeprazole,lansoprazole, pantoprazole
Cardiovascular Digoxin, diltiazem, enalapril,metoprolol
Neurologic Phenytoin, levetiracetam,fosphenytoin (phenytoin)
Endocrine Dexamethasone,hydrocortisone, levothyroxine,methylprednisolone
Other Ketorolac, warfarin