Embed Size (px)
Citation preview

CDT
RA
Mt
CMssOPwOo
©3
T
CALCINEURIN ANTAGONISTS
onversion of Stable Kidney Transplant Recipients From a Twiceaily Prograf-Based Regimen to a Once Daily Modified Releaseacrolimus-Based Regimen
. Alloway, S. Steinberg, K. Khalil, S. Gourishankar, J. Miller, D. Norman, S. Hariharan, J. Pirsch,
. Matas, J. Zaltzman, K. Wisemandle, W. Fitzsimmons, and M.R. First
ABSTRACT
Modified release (MR) tacrolimus is an extended release formulation administered oncedaily (qD). The purpose of this pharmacokinetic (PK) study was to evaluate tacrolimusexposure in stable kidney transplant recipients converted from Prograf twice a day to MRtacrolimus qD.Methods. This was an open-label, multicenter study with a crossover design. Eligiblepatients were 18 to 65 years of age, more than 6 months posttransplant with stable renalfunction, and received stable Prograf doses more than 2 weeks prior to enrollment.Patients received Prograf twice a day through day 7; 24-hour PK profiles were obtained ondays 1 and 7. Patients were converted to the same milligram-for-milligram daily dose ofMR tacrolimus qD in the morning on day 8; 24-hour PK profiles were obtained for MRtacrolimus on days 8, 14, and 21. Laboratory and safety parameters were also evaluated.Results. Most patients (67 of 70) completed all 5 PK profiles. The 90% confidence intervals(CI) for the MR tacrolimus vs Prograf comparison at steady state (days 14 and 21 vs days 1 and7) were 90.7 and 99.4 for AUC0–24 and 82.7 and 91.9 for Cmin. MR tacrolimus was welltolerated with a safety profile comparable to that of Prograf. AUC0–24 was highly correlated toCmin for Prograf (day 1, r � 0.80; day 7, r � 0.84) and MR tacrolimus (day 14, r � 0.92; day21, r � 0.86). Renal function remained stable after conversion to MR tacrolimus.Conclusion. The steady state PK of MR tacrolimus are equivalent to Prograf after amilligram-for-milligram conversion in stable kidney transplant recipients. The results provide
evidence to support a safe 1:1 conversion from Prograf twice a day to MR tacrolimus.hpM
H(
w(2
oM
ODIFIED RELEASE (MR) tacrolimus is an ex-tended release formulation of tacrolimus adminis-
ered once daily in the morning (qD AM). MR tacrolimus
From the University of Cincinnati, College of Medicine (R.A.),incinnati, Ohio, USA; California Institute of Renal Research, Sharpemorial Hospital (S.S., K.K.), San Diego, California, USA; Univer-
ity of Alberta Hospital, (S.G.), Edmonton, Alberta, Canada; Univer-ity of Miami School of Medicine (J.M.), Miami, Florida, USA;regon Health Sciences University, Department of Medicine (D.N.),ortland, Oregon, USA; Medical College of Wisconsin (S.H.), Mil-aukee, Wisconsin, USA; University of Wisconsin, Division ofrgan Transplantation (J.P.), Madison, Wisconsin, USA; University
f Minnesota (A.M.), Minneapolis, Minnesota, USA; St. Michael’s E2005 by Elsevier Inc. All rights reserved.60 Park Avenue South, New York, NY 10010-1710
ransplantation Proceedings, 37, 867–870 (2005)
as a similar extent of absorption as Prograf with a reducedeak level (Cmax).1 Healthy volunteer data indicate that theR tacrolimus formulation given qD AM and Prograf
ospital (J.Z.), Toronto, Ontario, Canada; Fujisawa Healthcare, Inc.K.W., W.F., M.R.F), Deerfield, Illinois, USA.
This study was supported by Fujisawa Healthcare, Inc. andas also presented in part at the American Transplant Congress
ATC) Annual Meeting in Boston, Massachusetts on May 16,004.Address reprint requests to Rita Alloway, PharmD, University
f Cincinnati, College of Medicine, Department of Surgery,L0558, 231 Albert Sabin Way, Cincinnati, OH 45267-0558.
-mail: [email protected]0041-1345/05/$–see front matterdoi:10.1016/j.transproceed.2004.12.222
867
aa00SapTppts
M
TsaPec2wmrt
ttso1e1Ma1s
(bPA1Pipms11tntcnb
psp9
ulti(i
R
S((cAwi�
epaaedatPwT2r68
Pep
D
D
D
D
868 ALLOWAY, STEINBERG, KHALIL ET AL
dministered twice a day have a similar exposure (AUC)nd trough levels (Cmin; data on file, 2001 company reports0-0-076, 00-0-077, 00-0-078, FG-506-04-21, and FG-506-4-25, Fujisawa Healthcare, Inc., Deerfield, Ill, Unitedtates). Medication compliance remains a serious problemfter transplantation,2,3 and a once daily regimen couldotentially improve compliance while maintaining safety.he aim of this study was to determine the steady stateharmacokinetics (PK) of tacrolimus in stable kidney trans-lant recipients converted from Prograf twice a day to MRacrolimus qD AM. A secondary aim was to determine theafety and tolerability of MR tacrolimus in these patients.
ETHODS
his was an open-label, multicenter, PK, safety, and tolerabilitytudy. To be eligible, patients had to be between 18 and 65 years ofge, more than 6 months post–kidney transplant taking stablerograf doses twice a day for at least 2 weeks prior to studynrollment, and they had to have stable renal function (serumreatinine less than 3.0 mg/dL and variation less than 0.5 mg/dL forlevels drawn at least 6 days apart). Patients were excluded if theyere receiving any drugs known to interfere with tacrolimusetabolism, if they had a rejection within 90 days, or if they
equired antibody therapy for rejection within 6 months prior tohe study.
This was a single-sequence, crossover study design. During thereatment phases of the study, patients were continued on Prografwice a day dosing through day 7. Patients were converted to theame milligram-for-milligram daily dose of MR tacrolimus qD AMn day 8 and were maintained with tacrolimus trough levels of 5 to5 ng/mL throughout the study. Twenty-four-hour tacrolimus PKvaluations were performed under steady state conditions on daysand 7 for the Prograf treatment and on days 8, 14, and 21 for theR tacrolimus treatment. Tacrolimus trough levels and clinical
ssessments for safety and rejection were completed on days 1, 7, 8,1, 14, 21, 28, and 35. In this study design, patients were able toerve as their own controls.
AUC0–24 was derived from the concentration-time curves. Cmin
trough) values were determined by using the tacrolimus wholelood concentration values at the 24-hour time point on days whenK profiles were obtained. The primary measure of exposure wasUC0–24. Descriptive statistics were provided for AUC0–24 at days
, 7, 8, 14, and 21. Statistical comparisons of AUC0–24 and Cmin forrograf and MR tacrolimus were assessed using a 90% confidence
nterval (CI) approach, analogous to Schuirmann’s 2 one-sided testrocedure.4 The method of analysis of variance with repeatedeasures was used for the comparisons of AUC0–24. Exposure at
teady state was used for Prograf (steady state was defined as daysand 7) and for MR tacrolimus (steady state was defined as days
4 and 21). The 90% CI was constructed for the natural logarithm–ransformed PK parameters. If the 90% CI for the ratio of theatural logarithm–transformed PK parameters fell within an 80%o 125% range, then the exposure between the 2 formulations wasonsidered to be equivalent.5,6 The PK parameters that wereatural logarithm–transformed prior to analyses were transformedack to the original scale for the presentation of results.All PK sample analyses (Prograf and MR tacrolimus) were
erformed using a validated LC/MS/MS assay at Fujisawa Re-earch Institute, Inc., Evanston, Ill, United States. Statistical com-arisons of AUC were assessed using a 90% CI approach. The
0–240% CI was constructed for natural logarithm–transformed and
ntransformed PK data. The PK parameters that were naturalogarithm–transformed prior to analyses were transformed back tohe original scale for the presentation of results. Equality ofntrasubject variability between the 2 formulations was also testedsmaller intrasubject variability is an indication of better reproduc-bility in PK profiles).
ESULTS
eventy patients were enrolled in the study; 67 patients95.7%) completed all 5 PK profiles; and 66 patients94.2%) completed all 5 PK profiles without a dosingonversion error and were considered for PK evaluation.mong these patients, there were 42 men (63.6%), 24omen (36.4%), 53 Caucasian (80.3%), 12 African Amer-
cans (18.2%), and 1 Asian (1.5%). The mean age was 46.912.37 years.The mean total daily dose of Prograf at baseline upon
nrollment was 5.7 � 3.47 mg. Approximately 70% ofatients converted to MR tacrolimus did not require a dosedjustment during the PK study. Twenty patients had dosesdjusted during the PK period for dosing errors, adversevents, trough level maintenance, or at the physician’siscretion. Of those adjusted for trough level maintenance,ll 3 patients were maintained at the lower end of theherapeutic range (�5 ng/mL). The mean daily dose ofrograf on days 1 and 7 was 5.8 � 3.5 mg. The median doseas 5.0 mg at both time points with a range of 1 to 19 mg.he mean daily doses of MR tacrolimus on days 8, 14, and1 were 5.8 � 3.5 mg, 5.9 � 3.3 mg, and 6.1 � 3.5 mg,espectively. The median doses were 5.0 mg on day 8 and.0 mg on days 14 and 21. The ranges were 1 to 19 mg (day), 1 to 17 mg (day 14), and 1 to 18 mg (day 21).A summary of the untransformed MR tacrolimus and
rograf PK parameters is given in Table 1. The meanxposure (ln AUC0–24, ng h/mL) of tacrolimus on PKrofile days 1 and 7 was 202.5 (Prograf) and on days 14 and
Table 1. Summary of the Tacrolimus PharmacokineticParameters
TreatmentAUC0–24
(ng · h/mL)Cmin
(ng/mL)
ay 1, PrografMean � SD 215.1 � 59.4 6.96 � 1.90Median 216.4 6.97Range 98.4–333.2 2.80–13.00
ay 7, MR tacrolimusMean � SD 206.6 � 58.4 6.73 � 1.99Median 200.9 6.83Range 87.9–355.6 3.03–11.90
ay 14, PrografMean � SD 200.7 � 57.5 6.08 � 1.80Median 200.8 5.89Range 92.8–364.7 2.69–10.40
ay 21, MR tacrolimusMean � SD 197.6 � 47.5 5.83 � 1.63Median 195.6 5.47Range 117.0–286.5 2.88–9.73
AUC0–24, exposure; Cmin, trough level.
2taCwr
omsPlT(Pfs
r(ftA9fscP
PTra
aPcpwmcfnaPf
S
Tacocaie
lll
Fm
POSTTRANSPLANTATION REGIMEN CONVERSION 869
1 was 192.3 (MR tacrolimus). The ratio of the MRacrolimus/Prograf exposure (ln AUC0–24) was 94.97% with90% CI of 90.7, 99.4. As this is contained within the 90%I of 80, 125, equivalent tacrolimus exposure was achievedith both tacrolimus formulations. These data are summa-
ized in Table 2During the Prograf and MR tacrolimus treatment peri-
ds, tacrolimus trough levels (Cmin) were analyzed. Theean log-transformed tacrolimus trough levels at steady
tate were 5.7 ng/mL for MR tacrolimus and 6.6 ng/mL forrograf. The ratio of the MR tacrolimus/Prograf for trough
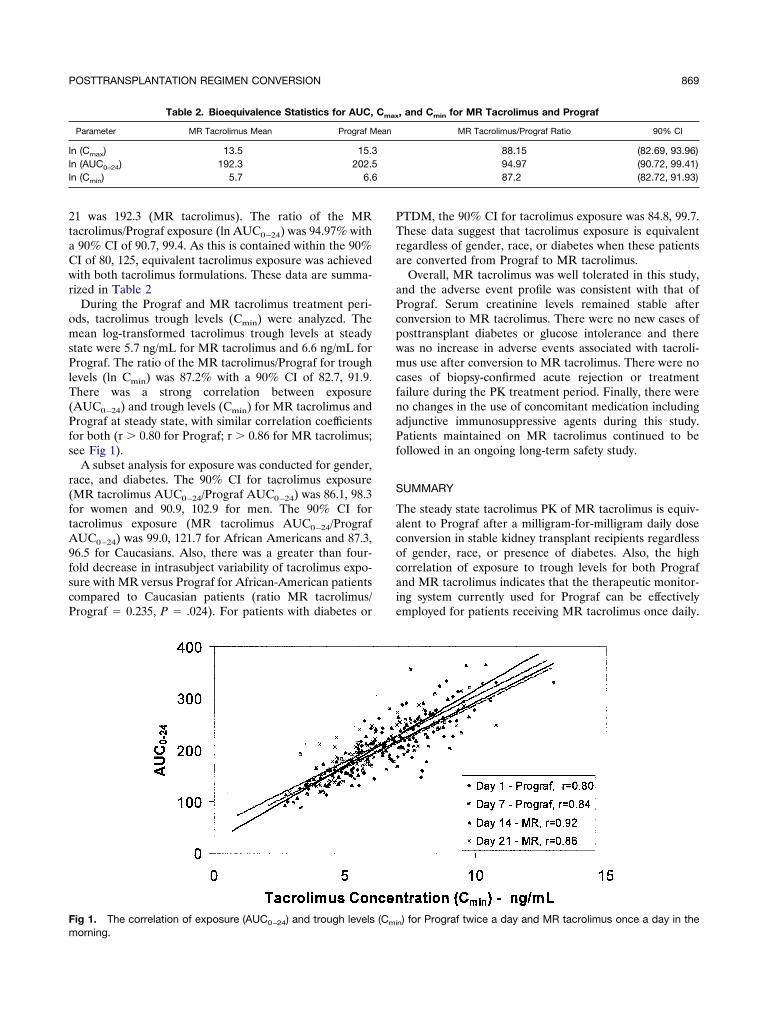
evels (ln Cmin) was 87.2% with a 90% CI of 82.7, 91.9.here was a strong correlation between exposure
AUC0–24) and trough levels (Cmin) for MR tacrolimus andrograf at steady state, with similar correlation coefficients
or both (r � 0.80 for Prograf; r � 0.86 for MR tacrolimus;ee Fig 1).
A subset analysis for exposure was conducted for gender,ace, and diabetes. The 90% CI for tacrolimus exposureMR tacrolimus AUC0–24/Prograf AUC0–24) was 86.1, 98.3or women and 90.9, 102.9 for men. The 90% CI foracrolimus exposure (MR tacrolimus AUC0–24/PrografUC0–24) was 99.0, 121.7 for African Americans and 87.3,
6.5 for Caucasians. Also, there was a greater than four-old decrease in intrasubject variability of tacrolimus expo-ure with MR versus Prograf for African-American patientsompared to Caucasian patients (ratio MR tacrolimus/rograf � 0.235, P � .024). For patients with diabetes or
Table 2. Bioequivalence Statistics for AUC,
Parameter MR Tacrolimus Mean Prograf M
n (Cmax) 13.5 15.3n (AUC0–24) 192.3 202.5n (Cmin) 5.7 6.6
ig 1. The correlation of exposure (AUC ) and trough levels
0–24 miorning.
TDM, the 90% CI for tacrolimus exposure was 84.8, 99.7.hese data suggest that tacrolimus exposure is equivalent
egardless of gender, race, or diabetes when these patientsre converted from Prograf to MR tacrolimus.
Overall, MR tacrolimus was well tolerated in this study,nd the adverse event profile was consistent with that ofrograf. Serum creatinine levels remained stable afteronversion to MR tacrolimus. There were no new cases ofosttransplant diabetes or glucose intolerance and thereas no increase in adverse events associated with tacroli-us use after conversion to MR tacrolimus. There were no
ases of biopsy-confirmed acute rejection or treatmentailure during the PK treatment period. Finally, there wereo changes in the use of concomitant medication includingdjunctive immunosuppressive agents during this study.atients maintained on MR tacrolimus continued to be
ollowed in an ongoing long-term safety study.
UMMARY
he steady state tacrolimus PK of MR tacrolimus is equiv-lent to Prograf after a milligram-for-milligram daily doseonversion in stable kidney transplant recipients regardlessf gender, race, or presence of diabetes. Also, the highorrelation of exposure to trough levels for both Prografnd MR tacrolimus indicates that the therapeutic monitor-ng system currently used for Prograf can be effectivelymployed for patients receiving MR tacrolimus once daily.
, and Cmin for MR Tacrolimus and Prograf
MR Tacrolimus/Prograf Ratio 90% CI
88.15 (82.69, 93.96)94.97 (90.72, 99.41)87.2 (82.72, 91.93)
) for Prograf twice a day and MR tacrolimus once a day in the
Cmax
ean
(C
n
Tapbtmrw
R
o
pr
ns
da
Set2
Set
870 ALLOWAY, STEINBERG, KHALIL ET AL
here is significantly less intrasubject variability in exposurefter conversion to MR tacrolimus for African-Americanatients. In conclusion, stable kidney transplant recipients cane safely converted from standard Prograf twice-a-day dosingo the same milligram-for-milligram daily dose of MR tacroli-us once daily in the morning. Hopefully a once daily dosing
egimen of MR tacrolimus can improve patient compliancehile maintaining effective immunosuppression.
EFERENCES
1. First MR, Fitzsimmons WE: New drugs to improve transplantutcomes. Transplantation 77:S88, 20042. Didlake RH, Dreyfus K, Kerman RH, et al: Patient noncom-
liance: a major cause of late graft failure in cyclosporine-treatedenal transplants. Transplant Proc 20:63, 1998 2
3. Butler JA, Roderick P, Mullee, et al: Frequency and impact ofonadherence to immunosuppressants after transplantation: aystematic review. Transplantation 77:769, 2004
4. Schuirmann DJ: A comparison of the two-sided tests proce-ure and the power approach for assessing the equivalence ofverage bioavailability. J Pharmacokin Biopharm 15:657, 1987
5. Guidance for Industry. Bioavailability and Bioequivalencetudies for Orally Administered Drug Products-General Consid-rations. U.S. Department of Health, Food and Drug Administra-ion, Center for Drug Evaluation and Research (CDER); July002.6. Guidance for Industry. Bioavailability and Bioequivalence
tudies for Orally Administered Drug Products-General Consid-rations. U.S. Department of Health, Food and Drug Administra-ion, Center for Drug Evaluation and Research (CDER); March
003; BP Revision 1.




























