Embed Size (px)
Citation preview

Cooper Longitudinal Clinical Clerkship for Primary Care
Dyanne P. Westerberg, DONirandra Mahamitra, MD
Brian Gable, MDJenny Melle, MD

3rd year rotations
• students work with mentors in core specialties on their principal clinical year and follow cases from beginning to end.
– David Hirsh, MD
– Cambridge Health System




Humanism
• Research suggests that as students progress through medical school, med students become more cynical, with a resulting decline in patient centeredness.
• Hirsh--graduating from an LIC can give a future doctor a better grounding in the humanism necessary to her or his profession, Hirsh says.


Cooper Medical School of Rowan University

Cooper Longitudinal Integrated Clerkship
Overview of the M3 year

Orientation week
6 immersion weeks
40 CLIC weeks
Inpatient “burst” weeks
Burst Weeks
Ob/gyn
Surgery
Psychiatry
Internal Medicine
Neurology
Pediatrics

Exams
• Last 2 weeks of the year.
• Family Medicine will be last
• OSKE
– Formative in December
– Summative in June

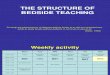
CLIC Sample Weekly Schedule
Sunday Monday Tuesday Wednesday Thursday Friday Saturday
7:00 AM
OFF
PATIENT ROUNDS AS NEEDED
OFF
8:00 AM
SDL
OB/GYN
or
SDL
SURGERY
ADULT
PRIMARY
CARE
SURGERY
OR TIME
9:00 AM
10:00 AM
11:00 AM
12:00 PM L U N C H
1:00 PM
PEDS
SCHOLAR’S
WORKSHOP NEURO
or
PSYCH
SDL DIDACTICS2:00 PM
3:00 PMSDL
4:00 PM
5:00 PM
PATIENT ROUNDS AS NEEDED 6:00 PM
7:00 PM

Sample M3 CLIC Month

Evaluations
• Monthly by the Preceptor
• Quarterly by the Clerkship Director
• Is this a good idea?
– Pros: Keeps the physicians focused
– Cons: May only see the student one time between evaluations

Preceptors were paid!!
As long as evaluations received on time!

Committee Thoughts
• Not enough time in Primary Care
• Teach or make RVU’s ??? Not enough time to teach.
• Not enough Administrative Support
• Not enough protected time to meet with students quarterly
• Not enough attendance at Faculty Development

Thoughts continued
• Feedback has not been valuable.
• Less didactic time
• Too much time with the specialists.

Summary of CLIC student narrative comments

Strengths:
• Longitudinal experience with preceptors and patients• Opportunity to learn about all core disciplines from
very early in the M3 year• Great variety of outpatient experiences• Great variety of settings• Individualized curriculum via SDL time• 1:1 preceptor relationship• Enthusiastic preceptors• Opportunity for integration of knowledge and skills
across disciplines• Abundance of OR time

Weaknesses:
• Not enough inpatient time to adequately prepare for M4 year and GME
• Inadequate exposure to patients with acute, serious illness
• Excessively narrow practice focus of preceptors in some disciplines (Neuro, Ob-Gyn, Peds)
• Mandatory plenary sessions; too “didactic”
• Drive time = wasted time
• Discontinuity in the outpatient venues due to Bursts
• Not enough true continuity patients

Big Problems
• Not enough generalist
• Example:
• 1 student saw 60 aneurysm patients and 0 patients with Gall Bladder Disease.
• Instead of pediatric generalist one student is following the allergist.

Evaluation Competencies• Medical Knowledge
• Patient Care
• Professionalism
• Interpersonal and Communication skills
• Practiced Based Learning and Improvement
• Systems Based Practice
• Scholarly Inquiry
• Health Partnership
• Learning and working in teams.