Embed Size (px)
Citation preview
2/5/2018
1
COPD 2018
Insights into the Early Detection, Diagnosis, and Management
Brian W. Carlin, MD, FCCP, FAARC, MAACVPRFebruary 2018
Disclosures (Brian Carlin, MD)
▪ Speakers bureaus, advisory panels▪ Sunovion
▪ Philips Respironics
▪ Monaghan Medical
▪ Astra Zeneca
▪ Glaxo Smith Kline
▪ Fiduciary positions▪ National Lung Health Education Program
▪ National Board for Respiratory Care
2
Educational Objectives
Upon completion of this activity, participants should be able to:
3
2/5/2018
2
The Importance of Early Detection and Diagnosis
COPD Definition
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Chronic Obstructive Pulmonary Disease (COPD) is a common, preventable and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar abnormalities usually caused by significant exposure to noxious particles or gases.
Burden of COPD
►4th leading cause of death in the world.1
►COPD projected to be the 3rd leading cause of death by 2020.2
►More than 3 million people died of COPD in 2012 (6% of all deaths globally)
►Globally, the COPD burden is projected to increase in coming decades because of continued exposure to COPD risk factors and aging of the population.
6
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380(9859): 2095-128.2. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med 2006; 3(11): e442.
2/5/2018
3
COPD Costs
Annual costs
▪ Direct: ≈$30 billion1
▪ Indirect ≈$20 billion1
▪ COPD exacerbations account for ≈75% of total costs/y2
▪ ≈13 million office visits/y due to exacerbations3
71. Guarascio AJ, et al. ClinicoEconomics and Outcomes Research: CEOR. 2013;5:235-245. 2. ERS-ATS COPD Guidelines. www.thoracic.org/clinical/copd-guidelines/resources/copddoc.pdf. Accessed 3/29/16. 3. Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2016. www.goldcopd.org. Accessed 3/29/16.
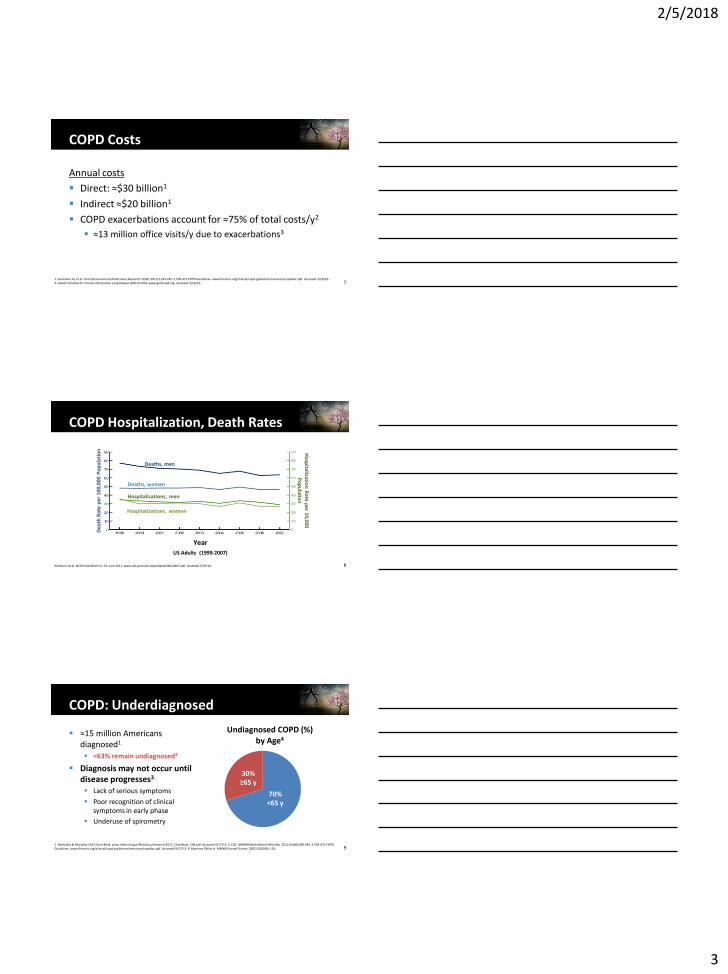
COPD Hospitalization, Death Rates
8
Dea
th R
ate
per
100
,000
Po
pu
lati
on H
osp
italization
Rate p
er 10,000 P
op
ulatio
n
Deaths, men
Deaths, women
Hospitalizations, men
Hospitalizations, women
Year
US Adults (1999-2007)
Akinbai LJ et al. NCHA Data Brief no. 63, June 2011. www.cdc.gov/nchs/data/databriefs/db63.pdf. Accessed 3/29/16.
COPD: Underdiagnosed
9
▪ ≈15 million Americans diagnosed1
▪ ≈63% remain undiagnosed2
▪ Diagnosis may not occur until disease progresses3
▪ Lack of serious symptoms
▪ Poor recognition of clinical symptoms in early phase
▪ Underuse of spirometry
Undiagnosed COPD (%) by Age4
30% ≥65 y
70% <65 y
1. Morbidity & Mortality 2012 Chart Book. www.nhlbi.nih.gov/files/docs/research/2012_ChartBook_508.pdf. Accessed 9/17/13. 2. CDC. MMWR Morb Mortal Wkly Rep. 2012;61(46);938-943. 3. ERS-ATS COPD Guidelines. www.thoracic.org/clinical/copd-guidelines/resources/copddoc.pdf. Accessed 9/17/13. 4. Mannino DM et al. MMWR Surveill Summ. 2002;51(SS06):1-16.
2/5/2018
4
Early Intervention Improves Outcomes
10
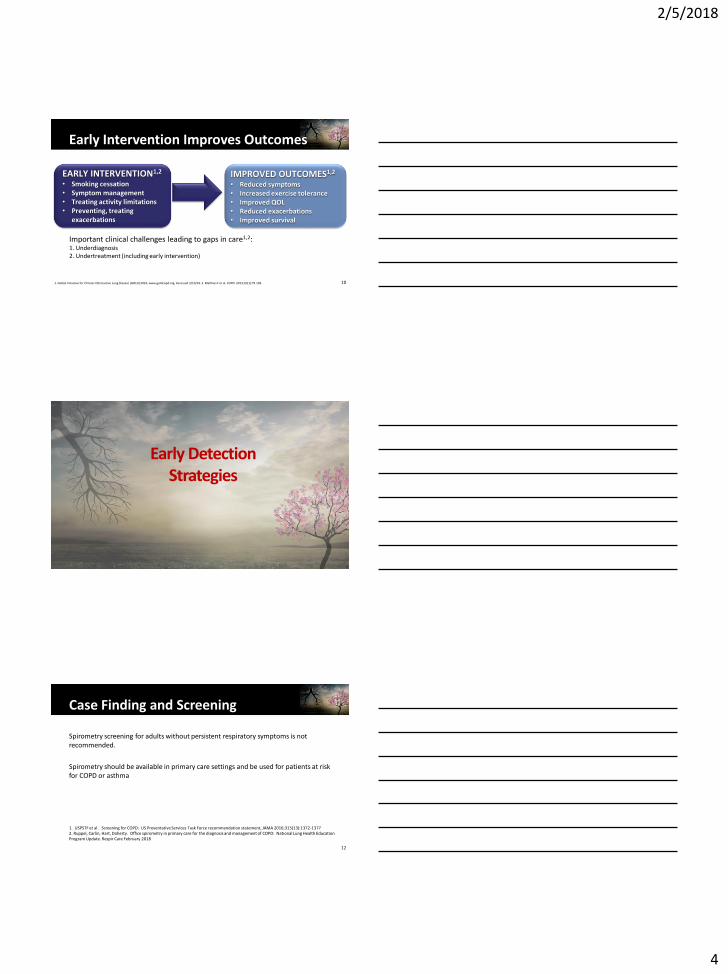
EARLY INTERVENTION1,2
• Smoking cessation• Symptom management• Treating activity limitations• Preventing, treating
exacerbations
IMPROVED OUTCOMES1,2
• Reduced symptoms• Increased exercise tolerance• Improved QOL• Reduced exacerbations• Improved survival
Important clinical challenges leading to gaps in care1,2:1. Underdiagnosis2. Undertreatment (including early intervention)
1. Global Initiative for Chronic Obstructive Lung Disease (GOLD) 2016. www.goldcopd.org. Accessed 3/10/16. 2. Malthais F et al. COPD. 2013;10(1):79-103.
Early Detection Strategies
Case Finding and Screening
Spirometry screening for adults without persistent respiratory symptoms is not recommended.
Spirometry should be available in primary care settings and be used for patients at risk for COPD or asthma
12
1. USPSTF et al . Screening for COPD: US Preventative Services Task Force recommendation statement, JAMA 2016;315(13):1372-13772. Ruppel, Carlin, Hart, Doherty. Office spirometry in primary care for the diagnosis and management of COPD: National Lung Health Education Program Update. Respir Care February 2018
2/5/2018
5
Case Finding and Screening
Spirometry should be used for patients:
> 40 years of age who are current or former smokers and
have one or more of the following
chronic cough
excess sputum production
wheezing
dyspnea out of proportion to age or activity
131. Office spirometry in primary care for the diagnosis and management of COPD: National Lung Health Education Program Update. Ruppel, Carlin, Hart, Doherty, Respir Care February 2018
Other Methods
Questionnaires and PEF measurements to select patients for diagnostic spirometry
COPD-population screener (COPD-PS)
Diagnostic score for COPD (DS-COPD)
International Primary Care Airways Guidelines questionnaire (IPAG)
Cost-effective approach
Reduces number of spirometry studies needed
141. Nelson, LaVange, Nie, Walsh, Enright. Questionnaire and pocket spirometers provide an alternative approach for COPD screening in the general population. Chest 2012;142:358-366.2. Soriano, Molina, Miravittlles. Int J TB and Lung Disease 2018;22:106-111.
Diagnosis
2/5/2018
6
Diagnosis and Initial Assessment
© 2017 Global Initiative for Chronic Obstructive Lung Disease
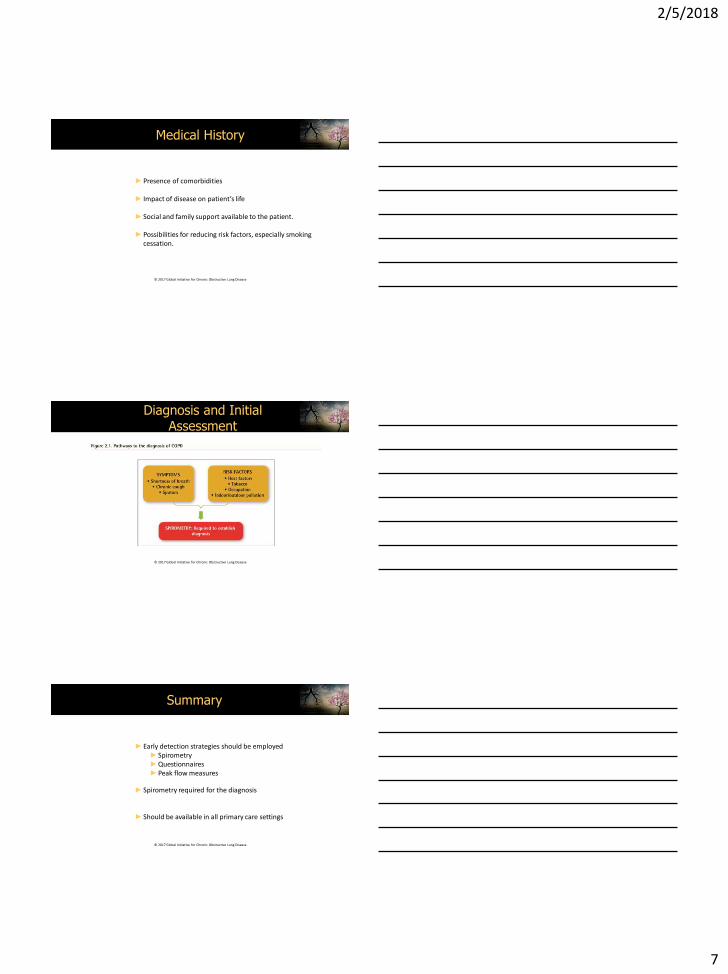
►COPD should be considered in any patient who has dyspnea, chronic cough or sputum production, and/or a history of exposure to risk factors for the disease.
►Spirometry is required to make the diagnosis
►The goals of COPD assessment are to determine ► the level of airflow limitation► the impact of disease on the patient’s health status,► the risk of future events
Diagnosis and Initial Assessment
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Symptoms of COPD
➢ Chronic and progressive dyspnea➢ Cough➢ Sputum production➢ Wheezing and chest tightness➢ Others – including fatigue, weight
loss, anorexia, syncope, rib fractures, ankle swelling, depression, anxiety.
Medical History
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Patient’s exposure to risk factors
►Past medical history
► Family history of COPD or other chronic respiratory disease.
►Pattern of symptom development
►History of exacerbations or previous hospitalizations for respiratory disorder
2/5/2018
7
Medical History
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Presence of comorbidities
► Impact of disease on patient’s life
►Social and family support available to the patient.
►Possibilities for reducing risk factors, especially smoking cessation.
Diagnosis and Initial Assessment
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Summary
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Early detection strategies should be employed►Spirometry►Questionnaires►Peak flow measures
►Spirometry required for the diagnosis
►Should be available in all primary care settings
2/5/2018
1
GOLD STANDARDS: WHAT YOU NEED TO KNOW
Gerard J. Criner, M.D.
Professor and Chair, Department of Thoracic
Medicine and Surgery
Temple University
Philadelphia, PA
PRESENTER DISCLOSURES
(1) The following relationships with commercial interests related to this presentation existed during the past 60 months:
Gerard J. Criner, M.D.
Honoraria: None
Grants received: NIH-NHLBI, PA-DOH,GSK, Boehringer- Ingelheim,
Novartis, Astra Zeneca, Respironics, Pearl, PneumRx, Pulmonx,
ResMed, Mereo,Probioterix, Broncus, Spiration
Grants pending: NIH-NHLBI, Fisher Paykel,
Consultation: Amirall, Holaira, Boehringer –Ingelheim, Astra
Zeneca, Respironics, Mereo, Patara
Equity Interest: HGE Health Care Solutions, Inc.
GOLD 2017: Most Significant Changes
➢ Assessment of COPD has been refined to separate the spirometric assessment from symptom evaluation
➢ ABCD groups are now proposed to be derived exclusively from patient symptoms and their history of exacerbations
➢ For each group A to D, escalation strategies for pharmacological treatments are proposed
➢ The concept of de-escalation of therapy is introduced in the treatment assessment scheme
➢ Non-pharmacologic therapies are comprehensively presented
➢ The importance of comorbid conditions in managing COPD is reviewed.
2/5/2018
2
COPD Definition
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Chronic Obstructive Pulmonary Disease
(COPD) is a common, preventable and
treatable disease that is characterized by
persistent respiratory symptoms and airflow
limitation that is due to airway and/or
alveolar abnormalities usually caused by
significant exposure to noxious particles or
gases.
COPD Etiology, Pathobiology & Pathology
Etiology
• Smoking and pollutants
• Host factors
Pathobiology
• Impaired lung growth
• Accelerated decline
• Lung injury
• Lung & systemic inflammation
Pathology
• Small airway disorders
• Emphysema
• Systemic effects
Airflow limitation
• Persistent airflow limitationClinical manifestations
• Symptoms & Exacerbations
• Comorbidities
Keys to the Diagnosis of COPD
Assessment of
Clinical
History and
Respiratory
Symptoms *
Physical
Examination*
Presence of
Airflow
obstruction
* Clinical history and physical examination are compatible with COPD and exclude
competing comorbid conditions as the major cause of current symptoms
2/5/2018
3
Classification of Airflow Limitation Severity in
COPD
GOLD Class Severity FEV1 % predicted
I Mild FEV1 > 80%
II Moderate 50% < FEV1 < 80%
III Severe 30% < FEV1 < 50%
IV Very Severe FEV1 < 30%
Classifying Symptoms: MRC or CAT
0 I only get breathless with strenuous
exercise
1 I get short of breath when hurrying on
the level or walking up a slight hill
2 I walk slower than people of the same
age on the level because of
breathlessness, or I have to stop for
breath when walking on my own pace on
the level
3 I stop for breath after walking about 100
meters or after a few minutes on the
level
4 I am too breathless to leave the house
or I am breathless when dressing or
undressing
Modified MRC Dyspnea Scale COPD Assessment Test (CAT)
Assessment of Exacerbation Risk
➢ Defined as acute worsening of
respiratory symptoms that
results in additional therapy
➢ Severity of events are
characterized as
Mild- treated with SABDs only
Moderate- treated with steroids +
antibiotics
Severe—ER or hospitalized
➢ Higher prevalence of
Exacerbations
Greater airflow limitation
Hospitalization
Prior exacerbations
Number of Exacerbations
Factor Odds Ratio p
AECOPD
prior yr.
5.72 <0.001
GERD 2.07 <0.001
FEV1 1.11 <0.001
WBC 1.08 0.002
SGRQ 1.07 <0.001
Hurst, NEJM, 2010
2/5/2018
4
Exa
ce
rba
tio
ns p
er
yea
r
0
CAT < 10
mMRC 0-1
GOLD 4
CAT > 10
mMRC > 2
GOLD 3
GOLD 2
GOLD 1
SAMA prn
or
SABA prn
LABA
or
LAMA
ICS + LABA
or
LAMA
GOLD RECOMMENDATIONS TO MANAGE STABLE COPD:
PHARMACOLOGIC THERAPY RECOMMENDED FIRST CHOICE
A B
DC
ICS + LABA
and/or
LAMA
© 2015 Global Initiative for Chronic Obstructive Lung Disease
2 or more or
> 1 leadingto hospitaladmission
1 (not leadingto hospitaladmission)
ABCD classification
➢ Pluses➢ “ABCD” assessment tool
of the 2011 GOLD update was a major advancement from the simple spirometricgrading system of earlier GOLD versions
➢ Incorporated patient-reported symptoms
➢ Highlighted the importance of exacerbation prevention in the management of COPD
➢ Minuses➢ Performed no better than
spirometric grades for mortality prediction or other important health outcomes
➢ Unable to assess the individual contributions of severity of airflow limitation from exacerbation frequency or severity
➢ Hindered initial ABCD assessment in subjects without spirometry (ER, hospitalized patient, initial outpatient assessment)
Diagnosis
C D
A B
mMRC 0-1CAT < 10CCQ < 1
mMRC 2+CAT 10+ CCQ 1+
> 2 or >1 leading
to hospitalization
0 or 1 (not leadingto hospitaladmission)
ExacerbationHistory
Grade FEV1
(% pred.)
1 ≥80
2 50-79
3 30-49
4 <30
FEV1/FVC<0.7
Assessment of airflowlimitation
Assessment ofsymptoms/risk of
exacerbations+=
The GOLD Refined ABCD Assessment Tool
2/5/2018
5
Example: Consider Two Patients
Both with FEV1 < 30% and CAT scores of 18
• No AECOPDs
• 3 AECOPDs
Both labelled GOLD D in prior
classification scheme
C D
A B
• No AECOPDs
• 3 AECOPDs
Grade FEV1 (% pred.)
1 ≥80
2 50-79
3 30-49
4 <30
A B
C D
• 3 AECOPDs - GOLD 4, Category D
• No AECOPDs- GOLD 4, Category B
Recommended Pharmacological Pathway Treatment
Algorithms by GOLD Grade
Exa
ce
rba
tio
ns
Sxs
Management of Stable COPD
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Smoking cessation
r/o AATD
Vaccination (flu, pneumococcal pneumonia)
Exercise
Goal weight
Manage comorbid conditions
Inhaled medications Short acting bronchodilators
Long acting bronchodilators
Inhaled steroids
2/5/2018
6
Treatment of Stable COPD
© 2017 Global Initiative for Chronic Obstructive Lung Disease
Manage and prevent exacerbations
Assess for exacerbation risk
Past history
Presence of Chronic bronchitis
Bronchiectasis
Emphysema
Treat promptly
Increased short acting bronchodilators
Antibiotics
Oral steroids
Hospitalization
Prevent exacerbations
Long acting bronchodilators
Inhaled steroids
Chronic azithromycin
Roflumilast
? N-acetylcysteine
? Theophyline
Non-Pharmacologic Treatment
© 2017 Global Initiative for Chronic Obstructive Lung Disease
►Education and self-
management
►Physical activity
►Pulmonary rehabilitation
programs
►Exercise training
►Self-management
education
► Nutritional support
► Vaccination
► Oxygen therapy
► Interventional
procedures
► Comorbidities
► End of life and
palliative care
Summary
➢ The diagnosis and treatments of COPD is changing
➢ New data suggests patients develop COPD along different paths
➢ Ultralong bronchodilators and ICS and their combinations may allow us to refine our current treatment paradigms
➢ Additional Tools (HRCT) now enable us to diagnose patients at an earlier stage
➢ New biological characterization schemes (EOS,PMNs) have promise to personalize treatment with novel therapies (IL-5 antagonists)
➢ GOLD continues to use new data to enhance our understanding of the management of patients with COPD
2/5/2018
1
Strategies to Relieve Dyspnea
Donald A. Mahler, M.D., FCCP
Emeritus Professor of Medicine
Geisel School of Medicine at Dartmouth
Director of Respiratory Services
Valley Regional Hospital
Claremont, NH
Conflicts of Interest
Advisory Boards – AZ; BI; GSK; Mylan;
Sunovion; Theravance
Royalties
CRC Press – Dyspnea 3rd Edition (2014)
Hillcrest Media – COPD: Answers to
Your Questions (2015)
MAPI and pharma – use of BDI/TDI
Speaker’s Bureau: BI, Grifols, Sunovion
Website: http://www.donaldmahler.com
an educational website for those with COPD and their families
Can you help me breathe easier?

2/5/2018
2
Treatment of COPD
GOLD Strategy
↓
Assess for Oxygen
↓
Pulmonary Rehabilitation
↓
Treat Psychosocial Factors
↓
Persistent Dyspnea
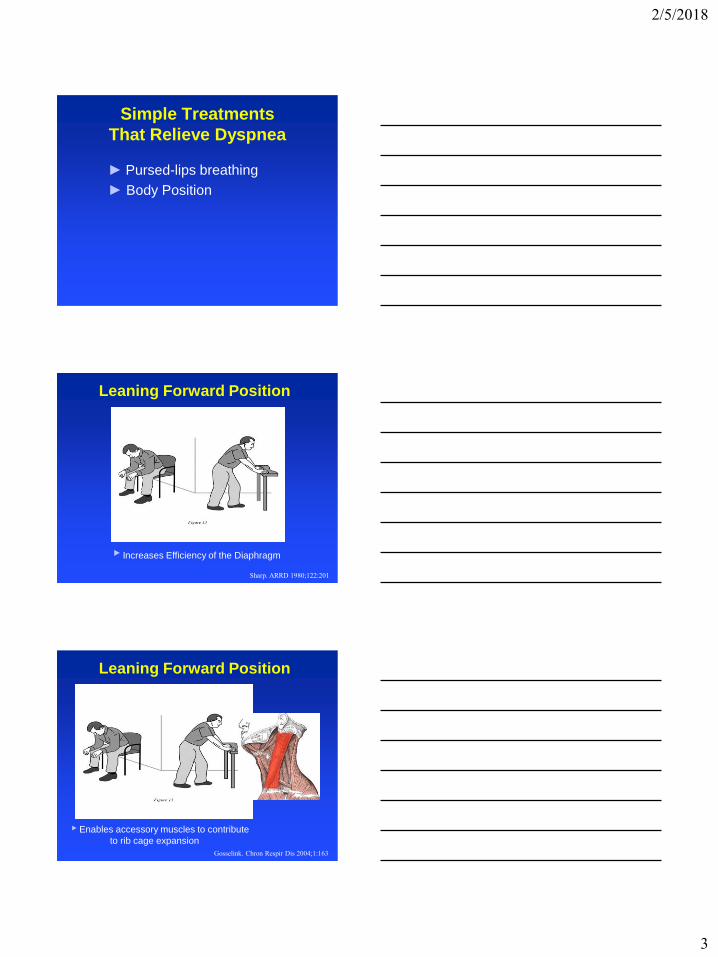
Simple Treatments
That Relieve Dyspnea
► Pursed-lips breathing
Pursed-Lips Breathing
Inhale thru nose Purse Lips Exhale thru mouth
► Creates Pressure At The Mouth To Keep
Airways Open Longer and Prolongs Exhalation
↑ SpO2; altered recruitment of respir muscles;
↓ chest wall volume; sense of breathing control
2/5/2018
3
Simple Treatments
That Relieve Dyspnea
► Pursed-lips breathing
► Body Position
Leaning Forward Position
► Increases Efficiency of the Diaphragm
Sharp. ARRD 1980;122:201
Leaning Forward Position
► Enables accessory muscles to contribute
to rib cage expansion
Gosselink. Chron Respir Dis 2004;1:163
2/5/2018
4
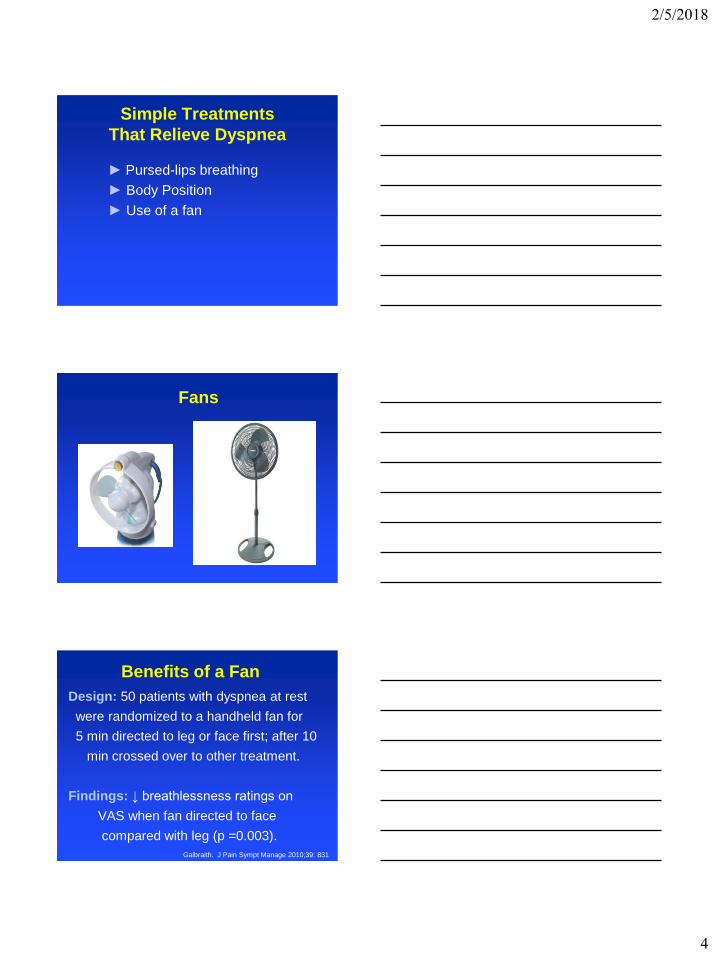
Simple Treatments
That Relieve Dyspnea
► Pursed-lips breathing
► Body Position
► Use of a fan
Fans
Benefits of a Fan
Design: 50 patients with dyspnea at rest
were randomized to a handheld fan for
5 min directed to leg or face first; after 10
min crossed over to other treatment.
Findings: ↓ breathlessness ratings on
VAS when fan directed to face
compared with leg (p =0.003).
Galbraith. J Pain Sympt Manage 2010;39: 831
2/5/2018
5
Simple Treatments
That Relieve Dyspnea
► Pursed-lips breathing
► Body Position
► Use of a fan
► Music (distracting stimulus)
► Activites that promote release
of endorphins
Activities that Promote
Release of Endorphins
► Exercise – “runner’s high”
► Laughter
► Listening to soothing music
► Eating chocolate
► Eating hot peppers – capsaicin
► Alcohol – light to moderate
► Acupuncture and massage
Mahler. Breathe Easy 2017;p.128
Simple and Inexpensive
Specific Patient Characteristics
2/5/2018
6
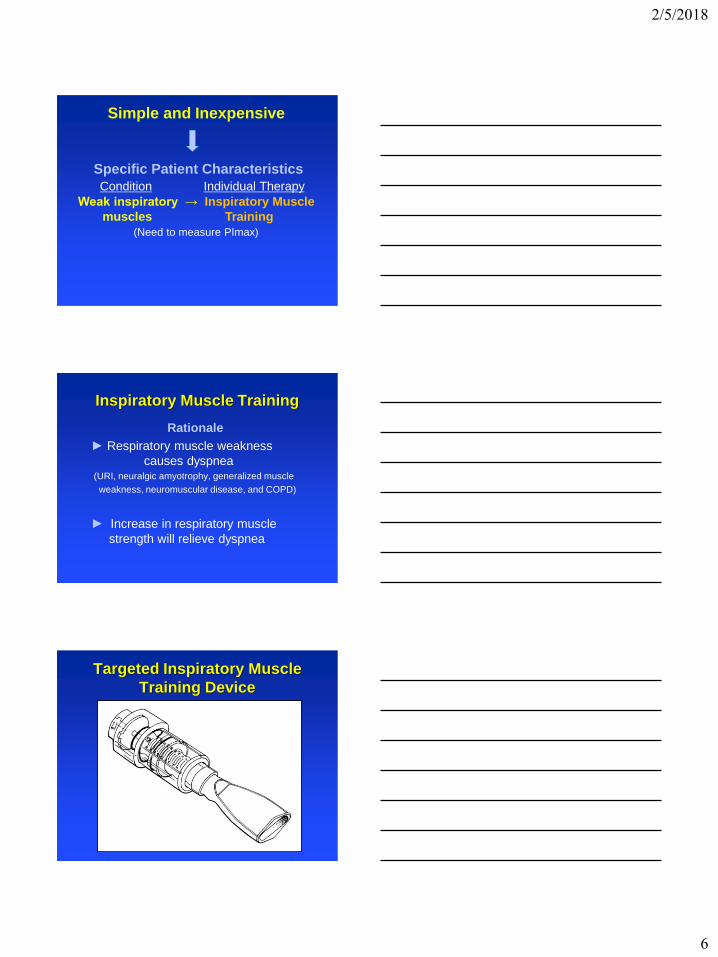
Simple and Inexpensive
Specific Patient Characteristics
Condition Individual Therapy
Weak inspiratory → Inspiratory Muscle
muscles Training
(Need to measure PImax)
Inspiratory Muscle Training
Rationale
► Respiratory muscle weakness
causes dyspnea (URI, neuralgic amyotrophy, generalized muscle
weakness, neuromuscular disease, and COPD)
► Increase in respiratory muscle
strength will relieve dyspnea
Targeted Inspiratory Muscle
Training Device
2/5/2018
7
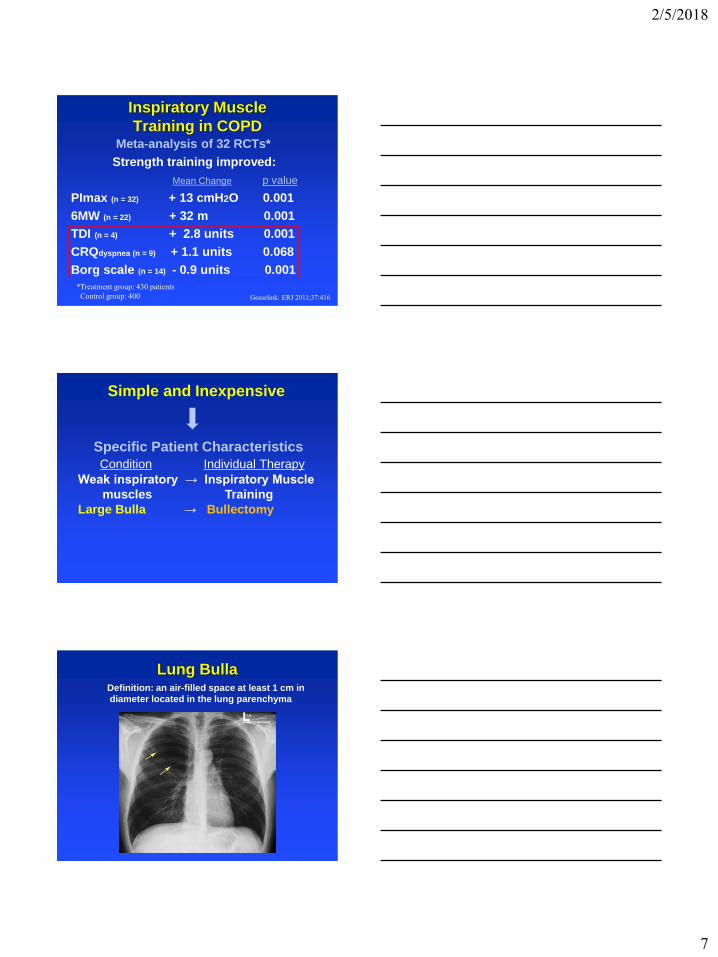
Inspiratory Muscle
Training in COPDMeta-analysis of 32 RCTs*
Strength training improved:
Mean Change p value
PImax (n = 32) + 13 cmH2O 0.001
6MW (n = 22) + 32 m 0.001
TDI (n = 4) + 2.8 units 0.001
CRQdyspnea (n = 9) + 1.1 units 0.068
Borg scale (n = 14) - 0.9 units 0.001
Gosselink. ERJ 2011;37:416
*Treatment group: 430 patients
Control group: 400
Simple and Inexpensive
Specific Patient Characteristics
Condition Individual Therapy
Weak inspiratory → Inspiratory Muscle
muscles Training
Large Bulla → Bullectomy
Lung BullaDefinition: an air-filled space at least 1 cm in
diameter located in the lung parenchyma
2/5/2018
8
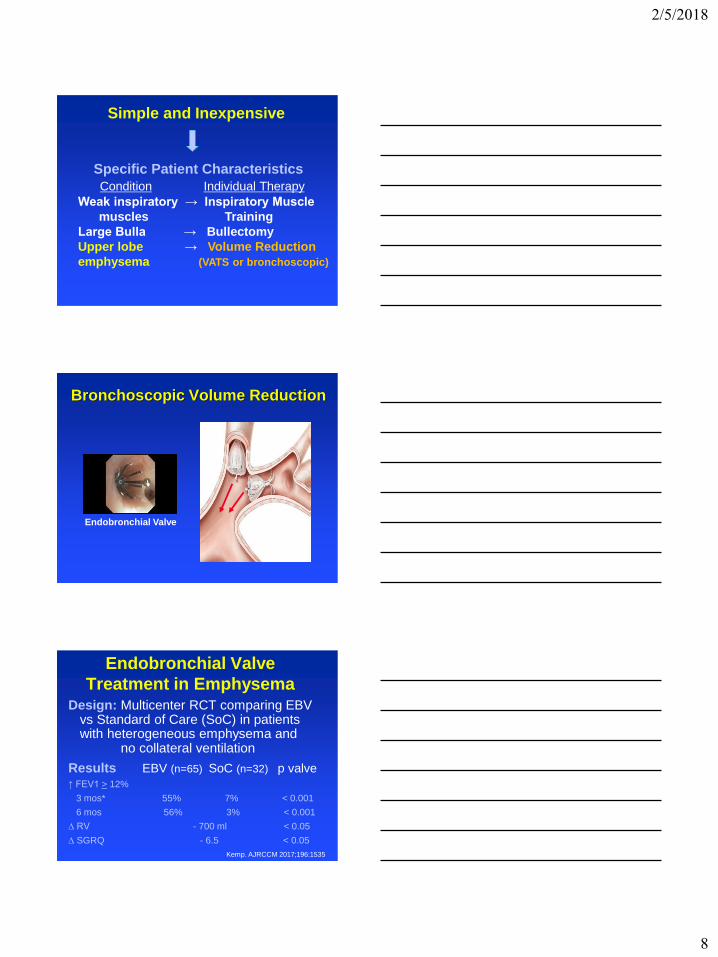
Simple and Inexpensive
Specific Patient Characteristics
Condition Individual Therapy
Weak inspiratory → Inspiratory Muscle
muscles Training
Large Bulla → Bullectomy
Upper lobe → Volume Reduction
emphysema (VATS or bronchoscopic)
Bronchoscopic Volume Reduction
Endobronchial Valve
Endobronchial Valve
Treatment in EmphysemaDesign: Multicenter RCT comparing EBV
vs Standard of Care (SoC) in patients with heterogeneous emphysema and
no collateral ventilation
Results EBV (n=65) SoC (n=32) p valve
↑ FEV1 > 12%
3 mos* 55% 7% < 0.001
6 mos 56% 3% < 0.001
∆ RV - 700 ml < 0.05
∆ SGRQ - 6.5 < 0.05
Kemp. AJRCCM 2017;196:1535
2/5/2018
9
Opioids
Effect of Opioids for
Relief of Dyspnea
In systematic review of 26 studies in
526 patients with a variety of advanced
diseases, “there is some low quality
evidence that shows benefit with
oral or parenteral opioids to
palliate breathlessness.”
(mean ∆ = - 0.28)
Barnes. Cochrane Database Syst Rev 2016 Mar 31:3
Opioid Prescription for Dyspnea
Dyspnea Opioid
Episodic IR or short-acting
Constant Sustained-release
► Start with low dose
► Titrate to achieve lowest effective dose
based on patient ratings of dyspnea
► Discontinue opioid if unsatisfactory response
or if adverse effect develops
2/5/2018
10
Therapies Receptors
► Inhaled Lung
furosemide (↑ SARs and ↓ RARs;
reflex bronchodilation;
? ↓ mucoasl edema)
► Chest Wall Chest wall
Vibration (muscle spindles in intercostal mm)
► Acupuncture Opioid (↑ β-endorphin in blood and CSF)
Investigational Therapies
Can you help me breathe easier?
2/5/2018
1
COPD GOLD GuidelinesChallenges for the Future
Sidney S. Braman MD Master FCCPProfessor of Medicine
Disclosures
• Non-promotional lectures on lung inflammation- Genentech
• Non-Promotional educational Video on respiratory compromise- Covidien
• Consultant on research directions-AstraZeneca and Sunovion
Learning Objectives
1. Assess the implications of a new definition of COPD
2. List phenotypes of COPD that will have implications for future care of COPD
3. Discuss new directions in the treatment of COPD patients
2/5/2018
2
What’s Going to be New ?Outline
• Definition of COPD changed!!
• GOLD Stage 0 and 1-should they be treated?
• “De-escalation” refined Will Inhaled corticosteroid controversy be resolved?
GOLD Definition of COPD-Changed
n COPD, a common preventable and treatable disease, is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases. Exacerbations and comorbidities contribute to the overall severity in individual patients
GOLD 2015
n “COPD is a common, preventable and treatable disease that is characterized by persistent respiratory symptoms and airflow limitation that is due to airway and/or alveolar
abnormalities usually caused by significant exposure to noxious particles or gases.”
GOLD 2017
n
……..an abnormal inflammatory responseof the lungs to noxious particles or gases
2/5/2018
3
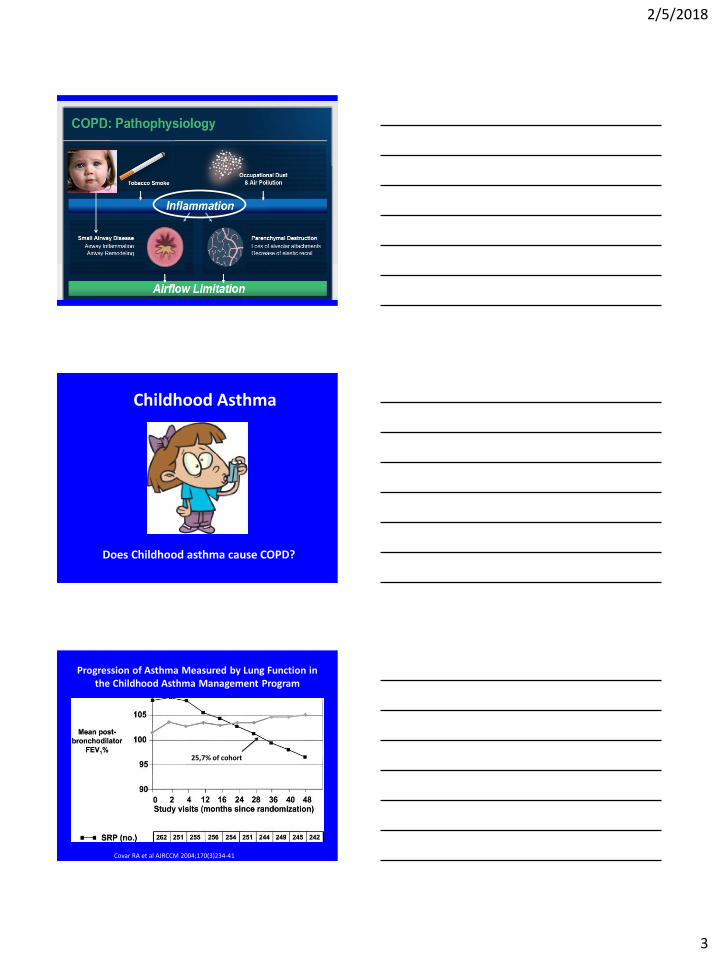
Childhood Asthma
Does Childhood asthma cause COPD?
Progression of Asthma Measured by Lung Function in the Childhood Asthma Management Program
25,7% of cohort
Covar RA et al AJRCCM 2004;170(3)234-41
2/5/2018
4
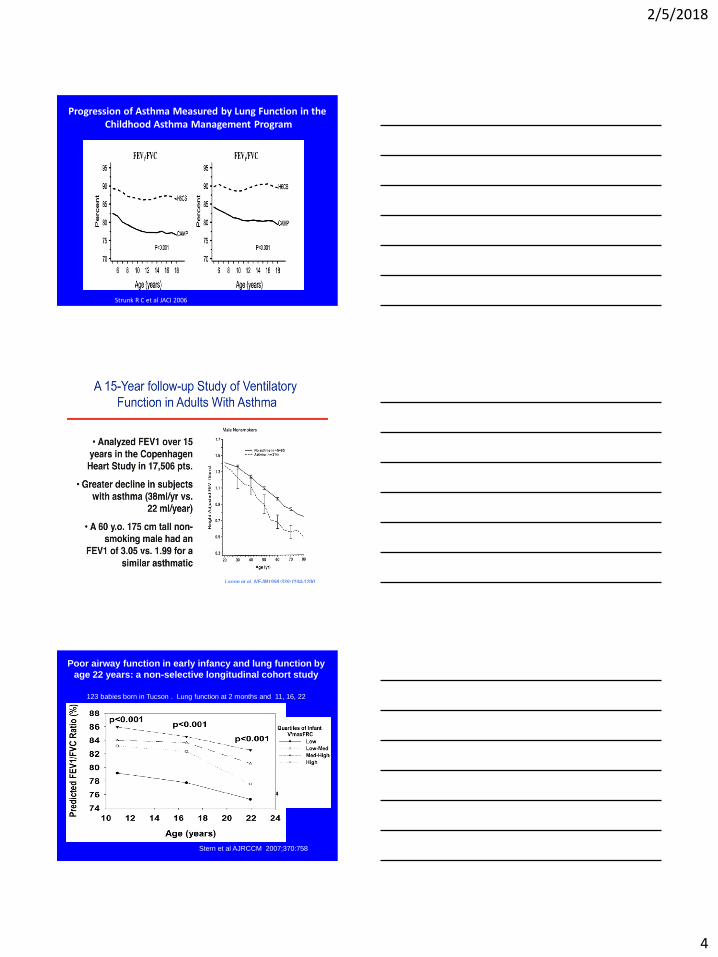
Progression of Asthma Measured by Lung Function in theChildhood Asthma Management Program
Strunk R C et al JACI 2006
Poor airway function in early infancy and lung function by
age 22 years: a non-selective longitudinal cohort study
123 babies born in Tucson . Lung function at 2 months and 11, 16, 22
Stern et al AJRCCM 2007;370:758
2/5/2018
5
Conclusions
• Low lung function “Early” in life is as
important a risk for COPD development
• Asthma at an early age may be associated
with a rapid decline in lung function and a
combination of asthma and starting at low
lung function may lead to severe fixed
airflow obstruction.
No known risk factors and...
1. low lung function starting early in
life resulting in fixed airflow
obstruction later in live.
2. asthma resulting in fixed airflow
obstruction later in live.
Is this COPD?
What’s Going to be New ?Outline
• GOLD Stage “0” and 1-should they be treated?
• “De-escalation” refined Will Inhaled corticosteroid controversy be resolved?
2/5/2018
6
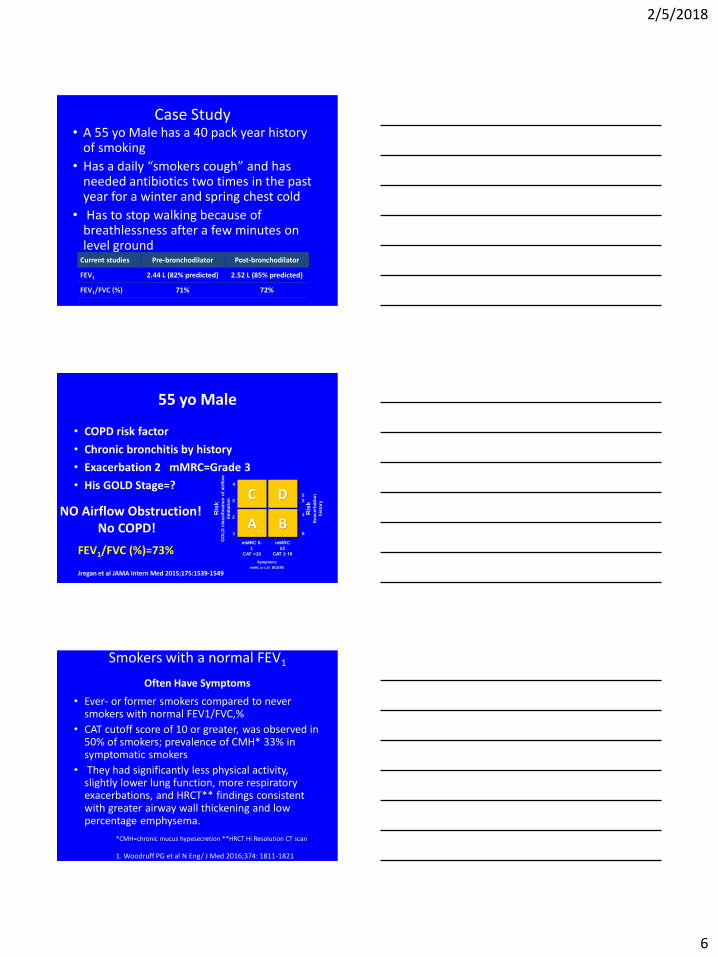
Case Study• A 55 yo Male has a 40 pack year history
of smoking
• Has a daily “smokers cough” and has needed antibiotics two times in the past year for a winter and spring chest cold
• Has to stop walking because of breathlessness after a few minutes on level ground
Current studies Pre-bronchodilator Post-bronchodilator
FEV1 2.44 L (82% predicted) 2.52 L (85% predicted)
FEV1/FVC (%) 71% 72%
55 yo Male
• COPD risk factor
• Chronic bronchitis by history
• Exacerbation 2 mMRC=Grade 3
• His GOLD Stage=?
Jregan et al JAMA Intern Med 2015;175:1539-1549
C D
A B
4
3
2
1
≥
2
1
0
mMRC 0-
1
CAT <10
Symptoms
mMRC or CAT score
Ris
kE
xacerb
ati
on
his
tory
mMRC
≥2
CAT ≥ 10
Ris
kG
OL
D c
lassif
icati
on
of
air
flo
w
lim
itati
on
NO Airflow Obstruction!No COPD!
FEV1/FVC (%)=73%
Smokers with a normal FEV1
Often Have Symptoms
• Ever- or former smokers compared to never smokers with normal FEV1/FVC,%
• CAT cutoff score of 10 or greater, was observed in 50% of smokers; prevalence of CMH* 33% in symptomatic smokers
• They had significantly less physical activity, slightly lower lung function, more respiratory exacerbations, and HRCT** findings consistent with greater airway wall thickening and low percentage emphysema.
*CMH=chronic mucus hypesecretion **HRCT Hi Resolution CT scan
1. Woodruff PG et al N Eng/ J Med 2016;374: 1811-1821
2/5/2018
7
C D
A B
4
3
2
1
≥
2
1
0
mMRC 0-
1
CAT <10
Symptoms
mMRC or CAT score
Ris
kE
xacerb
ati
on
his
tory
mMRC
≥2
CAT ≥ 10
Ris
kG
OL
D c
lassif
icati
on
of
air
flo
w
lim
itati
on
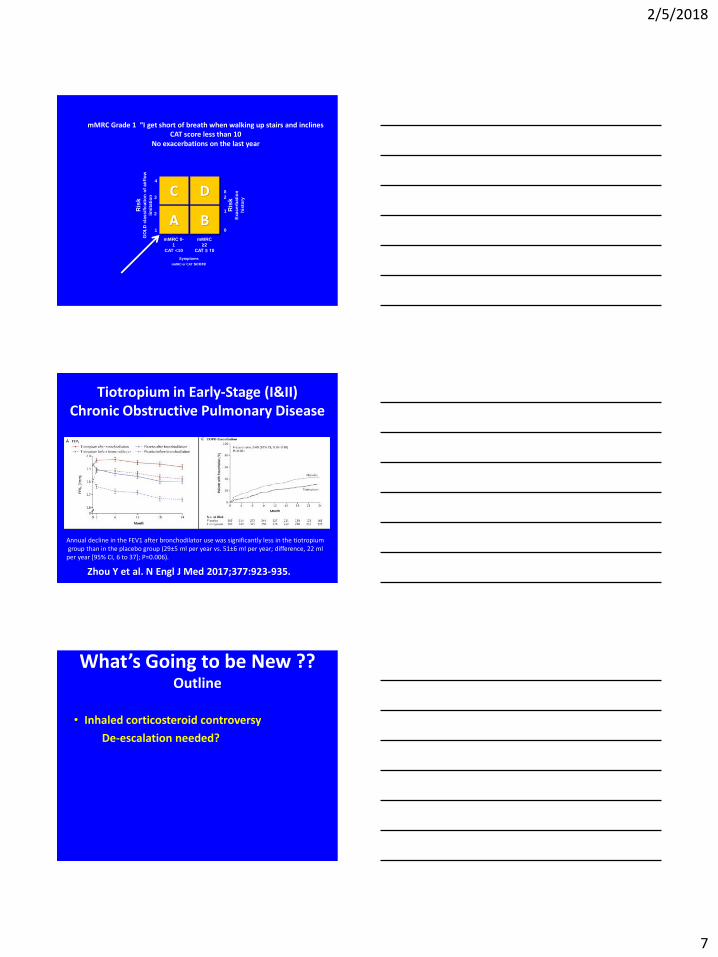
mMRC Grade 1 “I get short of breath when walking up stairs and inclinesCAT score less than 10
No exacerbations on the last year
Zhou Y et al. N Engl J Med 2017;377:923-935.
Tiotropium in Early-Stage (I&II) Chronic Obstructive Pulmonary Disease
Annual decline in the FEV1 after bronchodilator use was significantly less in the tiotropiumgroup than in the placebo group (29±5 ml per year vs. 51±6 ml per year; difference, 22 ml
per year [95% CI, 6 to 37]; P=0.006).
What’s Going to be New ??Outline
• Inhaled corticosteroid controversy
De-escalation needed?
2/5/2018
8
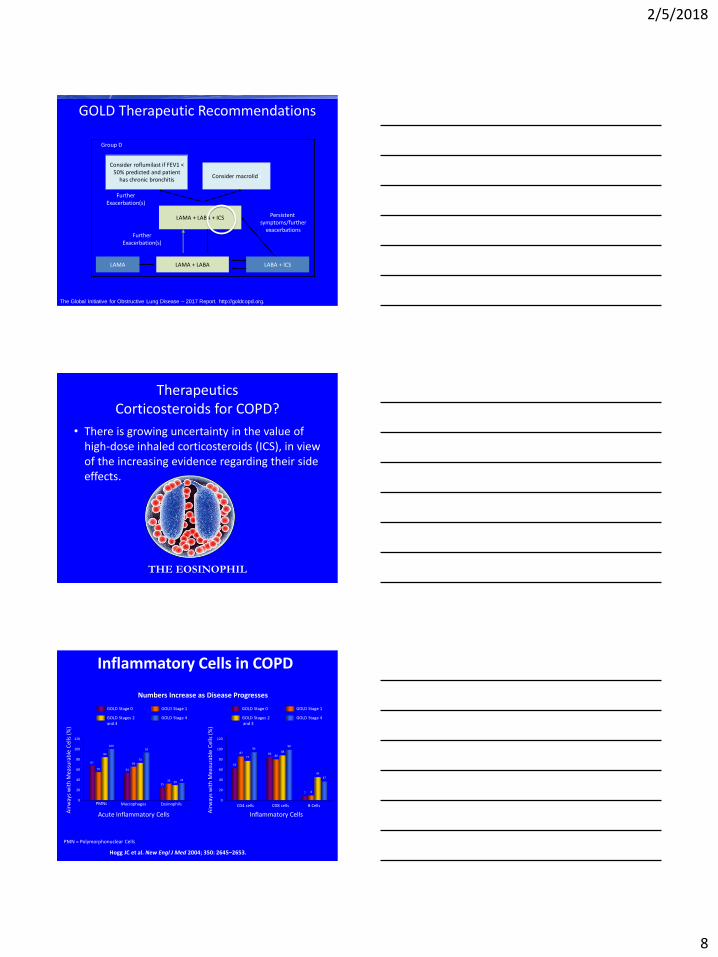
GOLD Therapeutic Recommendations
The Global Initiative for Obstructive Lung Disease – 2017 Report. http://goldcopd.org.
Group D
LAMA + LABA
Consider roflumilast if FEV1 < 50% predicted and patient
has chronic bronchitis
FurtherExacerbation(s)
Consider macrolide
LAMA LABA + ICS
LAMA + LABA + ICS
FurtherExacerbation(s)
Persistent symptoms/further
exacerbations
TherapeuticsCorticosteroids for COPD?
• There is growing uncertainty in the value of high-dose inhaled corticosteroids (ICS), in view of the increasing evidence regarding their side effects.
THE EOSINOPHIL
Numbers Increase as Disease Progresses
120
100
80
60
40
20
0PMNs Macrophages Eosinophils
Acute Inflammatory Cells
67
55
84
100
54
6673
92
2533 29
32
Air
way
s w
ith
Mea
sura
ble
Cel
ls (
%)
120
100
80
60
40
20
0
CD4 cells CD8 cells B Cells
Inflammatory Cells
GOLD Stage 0
GOLD Stages 2and 3
GOLD Stage 1
GOLD Stage 4
63
87
77
94
8580
88
98
7 8
45
37
Air
way
s w
ith
Mea
sura
ble
Cel
ls (
%)
Hogg JC et al. New Engl J Med 2004; 350: 2645–2653.
GOLD Stage 0
GOLD Stages 2 and 3
GOLD Stage 1
GOLD Stage 4
PMN = Polymorphonuclear Cells
Inflammatory Cells in COPD
2/5/2018
9
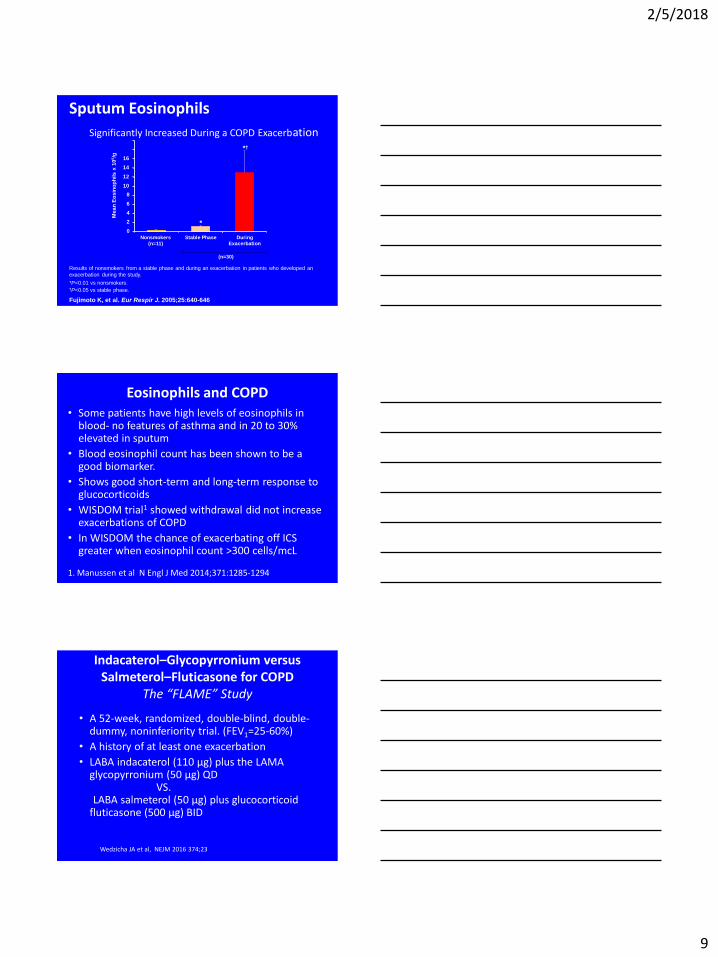
Significantly Increased During a COPD Exacerbation
Fujimoto K, et al. Eur Respir J. 2005;25:640-646.
Results of nonsmokers from a stable phase and during an exacerbation in patients who developed an
exacerbation during the study.
*P<0.01 vs nonsmokers.†P<0.05 vs stable phase.
Me
an
Eo
sin
op
hils
x 1
05/g
0
2
4
6
8
10
12
14
16
Stable Phase During
Exacerbation
*
Nonsmokers
(n=11)
(n=30)
*
†
Sputum Eosinophils
Eosinophils and COPD• Some patients have high levels of eosinophils in
blood- no features of asthma and in 20 to 30% elevated in sputum
• Blood eosinophil count has been shown to be a good biomarker.
• Shows good short-term and long-term response to glucocorticoids
• WISDOM trial1 showed withdrawal did not increase exacerbations of COPD
• In WISDOM the chance of exacerbating off ICS greater when eosinophil count >300 cells/mcL
1. Manussen et al N Engl J Med 2014;371:1285-1294
Indacaterol–Glycopyrronium versus Salmeterol–Fluticasone for COPD
The “FLAME” Study
• A 52-week, randomized, double-blind, double-dummy, noninferiority trial. (FEV1=25-60%)
• A history of at least one exacerbation
• LABA indacaterol (110 μg) plus the LAMA glycopyrronium (50 μg) QD
VS.LABA salmeterol (50 μg) plus glucocorticoid
fluticasone (500 μg) BID
Wedzicha JA et al, NEJM 2016 374;23
2/5/2018
10
Indacaterol–Glycopyrronium versus Salmeterol–Fluticasone for COPD
The “FLAME” Study
• Indacaterol–glycopyrronium was more effective than salmeterol–fluticasone in preventing COPD exacerbations in patients with a history of exacerbation during the previous year with 11% lower rate.
• Also greater decrease in the use of rescue medication and the greater improvement in health status (decrease in SGRQ-C score) and lung function.
• No difference in results if blood eosinophil count< 2% or>2%
Wedzicha JA et al, NEJM 2016 374;23
TherapeuticsCorticosteroids for COPD
• Blood eosinophil counts may predict the efficacy of ICS in preventing exacerbations in patients with COPD, but prospective studies are needed.
• In patients with lower blood eosinophil counts (< 2%) there is evidence for a poor response to ICS and an increased risk of pneumonia.
Thanks for your attention.





























