Embed Size (px)
Citation preview

CopingMechanismsofNursesFacingtheDeathofPediatricPatientsALiteratureReviewLindaDindaMelinaEdwardsLilliMikkonenBachelor’sthesisMay2017Socialservices,HealthandSportDegreeProgrammeinNursing
Description
Author(s)Dinda,LindaEdwards,MelinaMikkonen,Lilli
TypeofpublicationBachelor’sthesis
DateMay2017Languageofpublication:English
Numberofpages42
Permissionforwebpubli-cation:x
TitleofpublicationCopingMechanismsofNursesFacingtheDeathofPediatricPatientsALiteratureReview
DegreeprogrammeDegreeProgrammeinNursing
Supervisor(s)Lehto,Siru&Sinivuo,RiikkaAssignedby-
Abstract
In2015,5.9millionchildrendiedworldwide.Althoughnursesfacethedeathofbothyoungandoldpatientsregularly,thedeathofapediatricpatientisoftenperceivedunfairandunexpected.Nursesstruggletodealwiththedeathofachildpatient,asithasphysical,psychological,emotionalandbehavioralimpactsonthem.Additionally,thismayhaveanegativeimpactontheoutcomesofcare.Yet,littleresearchexistsonthecopingmecha-nismsofnurses.Theaimofthisstudywastoexplorenurses’copingmechanismswhenfacingthedeathofapediatricpatient.Thepurposewastoprovideinformationonhowtoencounterthedeathofachildpatientandlearntoacknowledgetheideaofit.Thiswasintendedtopro-videinformationthatcouldbeusedineducatingfuturenursesandnursesworkinginvari-ousfields.Thestudywasimplementedasaliteraturereview.Thedatawassearchedusingthefol-lowingtwodatabases:CinahlandJYKDOK.Overall,elevenarticleswerechosentobere-viewed.Contentanalysiswasappliedintheanalysisofthedata.Threemaincategoriesweregenerated:socialsupport,institutionalsupportandpersonalcopingstrategies.Theapplicabilityoftheseresultsmightvaryaccordingtotheindividualandthenursingsettings.Therefore,theresultsindicatedtheneedforfurtherresearchtodeterminewhatkindsofcopingmechanismswouldbebestapplicableforeachparticularnursingsetting.
Keywords(subjects)nurse,pediatrics,childdeath,copingmechanismMiscellaneous
1
Contents
1 Introduction....................................................................................................3
2 Childmortality................................................................................................4
2.1 Childmortalityrates...................................................................................4
2.2 Majorcausesofchildmortality..................................................................5
3 Pediatricnursing.............................................................................................6
3.1 Challengesinpediatricnursing...................................................................7
3.2 Nurses’experiencesfacingdeathofchildren.............................................9
3.3 Copingmechanisms..................................................................................11
4 Aim,purpose&researchquestion.................................................................12
5 Methodsandimplementationofthestudy....................................................13
5.1 Literaturereview......................................................................................13
5.2 Literaturesearch......................................................................................14
5.3 Dataanalysis.............................................................................................16
6 Results...........................................................................................................17
6.1 Socialsupport...........................................................................................18
6.2 Institutionalsupport.................................................................................20
6.3 Personalcopingstrategies........................................................................22
7 Discussion......................................................................................................26
7.1 Ethicalconsiderations,validityandreliability..........................................26
7.2 Discussionoftheresults...........................................................................28
References............................................................................................................33
Appendices...........................................................................................................40
Appendix1.Thereviewedarticlesinalphabeticalorder...................................40
2
Figures
Figure1.Majorcausesofunder-fivedeathsworldwide(2015)...................................6
Figure2.Inclusioncriteria...........................................................................................15
Figure3.Exampleofdataanalysisprocess.................................................................17
Figure4.Categoriesandsubcategories......................................................................18
Tables
Table1.Datasearch(duplicatesexcluded).................................................................16

3
1 Introduction
Modernmedicineaimstotreatandcure,however,careofthedyingandbereaved
alsoremainsasaroleofhealthcareprofessionals(Reynolds2006).Accordingtothe
WorldHealthOrganization’s(WHO)GlobalHealthObservatory(GHO)data(2017),
5.9millionchildrendiedin2015,mostofwhichhappenedintheWHOAfricaregion.
IntheEuropeanregion,11childrendiedoutofevery1000livebirthsin2015(WHO
2017).Basedonthesestatisticsitcanbededucedthatachilddyinginindustrialized
countriesisuncommon.Nevertheless,whenthisrarephenomenonoccursitisnor-
mallyatthehospitalafterthechildhasreceivedcomplex,andoftenlong-term,med-
icalcareaimedatcuringorcontrollingaseriousdisease(Docherty,Miles&Brandon
2007;Papadatou1997).
Achild’sdeath,ingeneral,isperceivedunfairandunexpected(Furingsten,Sjörgen&
Forsner2015).Comparedtootherhealthcareprofessionals,nursesspendmoretime
withthepatients,especiallyifapatient’shospitalstayisprolonged(Wilson&Kirsh-
baum2011).Hence,takingcareofpatientswhoaredying,andsimultaneouslysup-
portingtheirfamily,canbestressfulandtaskingfornurses.Furthermore,theanxiety
anduneasinessofdeathcanmakenurseslesscomfortablewhenprovidingsuchcare
(Peters,Cant,Payne,O’Connor,McDermott,Hood,Morphet&Shimoinaba2013).
Therefore,nursesinvolvedinthecareofdyingchildrenexperiencevariouschalleng-
esandobstacles.(Furingsten,Sjörgen&Forsner2015.)Duetodeathbeingaregular
occurrenceinanurse’slife,variouscopingmechanismsareessential,andtheability
tocopewhenencounteringdeathisavitalskilltohave.Moreover,inabilitytocope
withthedeathofachildhasbeenproventocauseharmtotheworkingabilitiesof
nurses.(Petersetal.2013.)
Thisresearchaimstoexplorethecopingmechanismsofnurseswhenfacingthe
deathofapediatricpatient.Thepurposeofthisresearchistoprovideinformation
4
onhowtoencounterthedeathofachildpatientandlearntoacknowledgetheidea
ofit.
2 Childmortality
2.1 Childmortalityrates
TheUnitedNation’sConventionontherightsofthechilddefinesachildasaperson
under18yearsold(YK1989).Basedontheirage,childrencanbedividedintodiffer-
entdevelopmentalgroupsasfollows.Logically,asthefirst28-day-periodofachild’s
lifeisreferredtoastheneonatalperiod,childrenagedlessthan28daysarereferred
toasneonates.Predominantly,duringthefirstyearoflife,childrenaredescribedas
infants.Thereafter,they’retoddlersupuntiltheageofthreeyears,andpreschoolers
attheageofthreetosixyears.Childrenfrom7to12yearsofagearedefinedschool
aged,andfinally,adolescentsfrom12to18yearsofage.(Storvik-Sydänmaa,Tal-
vensaari,Kaisvuo&Uotila2012,11.)
AccordingtoWHO(2016)globally,5.9millionchildrendiedbeforereachingtheage
of5in2015.Thenumberisequivalenttoabout16000fatalitieseveryday.Although
under-fivemortalityratesaredecreasingglobally,theratesremainremarkablyun-
balancedbetweenhigh-andlow-incomecountries.Thesub-SaharanAfricaisbattling
thehighestriskforunder-fivemortality,theriskbeingabout14timeshigherthanin
thedeveloped,high-incomeregions(WHO2016).Lookingatthebiggerpicture,in
high-incomecountries7outof10deathsareamong70-year-oldsandolder,with
only1outofevery100deathsamongchildrenunder15years.Incomparison,inlow-
incomecountriesnearly4inevery10deathsareamongchildrenunder15years,and
only2inevery10amongpeopleaged70andolder.(WHOn.d..)
5
Duetosocioeconomicdevelopmentandimplementationofvariousinterventionsfor
thesurvivalofthechildren(Black,Cousens,Johnson,Lawn,Rudan,Bassani,Jha,
Campbell,FischerWalker,Cibulskis,Eisele,Liu&Mathers2010),childmortalityrates
intheAfricanregionhavealsodecreasednotablywithinthelast10years(Ashorn
2016).Eventhoughthispositivechangehasbeenseeninthedevelopingcountries,
therearestillcountriesthathaven’tchanged.Thethreeprinciplefactorsessentialfor
children’shealthareshelter,foodandpotablewater.Nevertheless,thesebasicre-
quirementsarenotfulfilledaswellinthelow-incomecountriesasinthehigh-income
countries.Theabsenceofevenoneofthesefactorscanendangerthehealthofa
child.Withoutshelter,childrenareexposedtoallkindsofenvironmentalhazards
suchascold,radiation,infectionsand,withinwarzones,evenexplosives.Itisbe-
lievedthatabout200millionchildren,undertheageof5,livestarvingandwithout
enoughsourcesforcleanwater,thuspredisposedtovariousmedicalconditions.
(Ashorn2016.)
2.2 Majorcausesofchildmortality
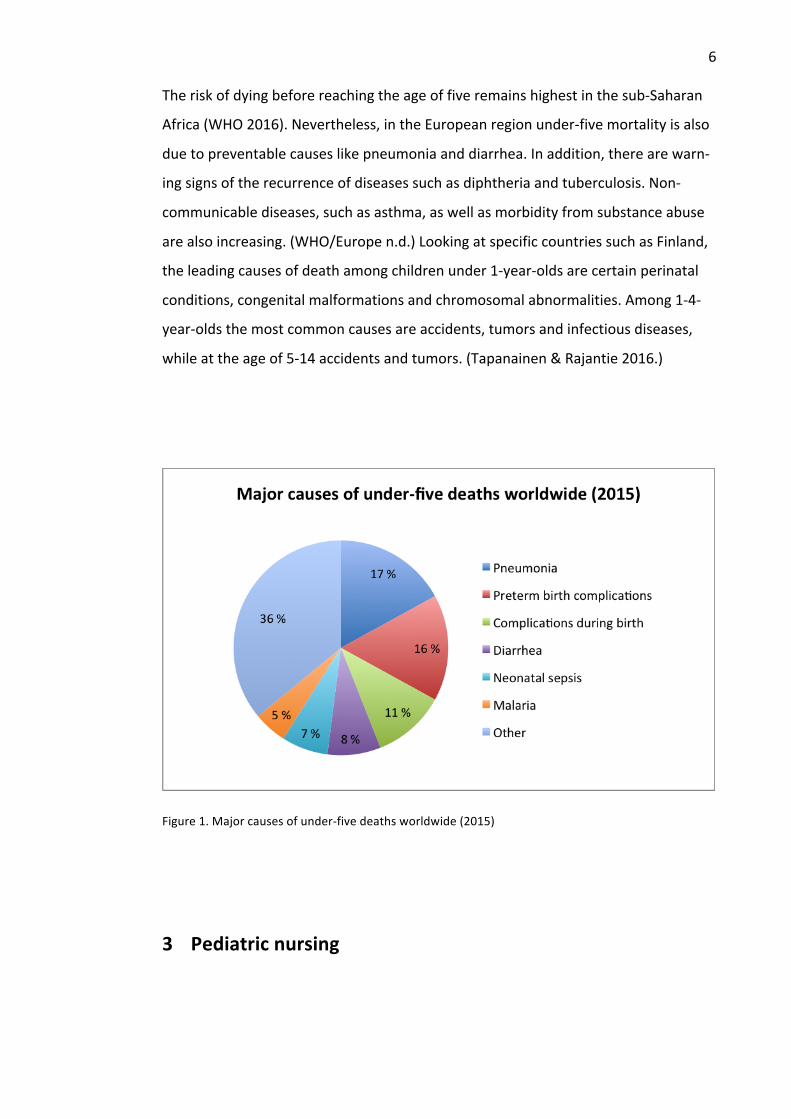
Achild’sriskofdyingishighestduringthefirst28daysoflife,alsoknownasthene-
onatalperiod.Furthermore,45percentofdeathsundertheageof5yearsoccur
withintheneonatalperiod.Mostoftheneonataldeathsareduetoprematurity,
complicationsduringbirthorinfections.Theleadingcausesofdeathamongchildren
agedmorethan28daysbutlessthan5yearsarepneumonia,diarrheaandmalaria.
(WHO2016.)Additionally,nearlyhalfofallunder-fivedeathsareconsequenttoun-
dernutrition.Thus,mostchilddeathsaresubsequenttoconditionsthatareeither
preventableortreatable.Statisticsofthemajorcausesofunder-fivefatalitiesin2015
arepresentedinfigure1.(Levelsandtrendsinchildmortality2015,8.)
6
Theriskofdyingbeforereachingtheageoffiveremainshighestinthesub-Saharan
Africa(WHO2016).Nevertheless,intheEuropeanregionunder-fivemortalityisalso
duetopreventablecauseslikepneumoniaanddiarrhea.Inaddition,therearewarn-
ingsignsoftherecurrenceofdiseasessuchasdiphtheriaandtuberculosis.Non-
communicablediseases,suchasasthma,aswellasmorbidityfromsubstanceabuse
arealsoincreasing.(WHO/Europen.d.)LookingatspecificcountriessuchasFinland,
theleadingcausesofdeathamongchildrenunder1-year-oldsarecertainperinatal
conditions,congenitalmalformationsandchromosomalabnormalities.Among1-4-
year-oldsthemostcommoncausesareaccidents,tumorsandinfectiousdiseases,
whileattheageof5-14accidentsandtumors.(Tapanainen&Rajantie2016.)
Figure1.Majorcausesofunder-fivedeathsworldwide(2015)
3 Pediatricnursing
7
3.1 Challengesinpediatricnursing
Apediatricnurseisanursewhoisinvolvedinthehealthcareofachildfrominfancy
throughadolescence.Pediatricnurseshaveanoverallgoalofprovidingoptimal
healthcaretotheirclientswhiletakingintoaccounttherolefamiliesplayintheir
client'swellbeing(Kyle2008,Linnard-Palmer&Coats2016,283.)Pediatricnursesare
presentinallthethreemajorlevelsofhealthcare.Intheprimarylevel,theycanpro-
videcareinplaceslikehealthcarecenters,schoolsandevendaycarecenters.Inthe
secondarylevel,pediatricnursescanbefoundprovidingcareinpediatricintensive
units,surgicalunits,andemergencydepartments.Lastly,intertiarycenterstheycan
befoundinrehabilitationcenters,endoflifecareandhomecareagencies(Linnard-
Palmer&Coats2016,284.)Althoughdifferenttypesofnursesinalllevelsofcare
mighthavevariousrolesandresponsibilities,whencaringforachild,allofthem
mustensurethatcommunicationisbasedonthechild’sageanddevelopmentlevel
(Kyle2008).
Communication
Communicationisthemostcommonprocedureinnursing.Itisintimatebecauseof
theveryprivateissues,suchashopes,fears,mentaldisordersandterminalillnesses,
discussed.Itisthefoundationoftherapeuticrelationshipsbetweennursesandtheir
clients.(Levetown2008.)Despitecommunicationbeingacriticalcomponentofcare,
itoftenfaceschallengesespeciallyinpediatriccarewhichrequiresconsideringthe
client’sfamilyaspartoftheholisticcare(Blackstone&Pressman2011).Another
challengeiscommunicatingwiththechildpatientasconsiderationisrequiredon
cultural,ethical,relationalanddevelopmentallevels(Levetown2008).Perhapsthe
mostchallengingpartofcommunicationinpediatricnursingiswhen‘badnews’have
tobegiventoapatient.Discussingtheneedtotakemedicationfortherestofone’s
lifeforachroniccondition,anunanticipatedbloodtestforaneedlephobicchild,or
talkingabouthospiceandpalliativecareforachildmayfeeluncomfortabletoa
nurse,resultingtoemotionaldistress(Berlinger,Barfield&Fleischman2013).
8
Emotionallabor
Maunder(2008)aswellasBailey,MurphyandPorock(2011),refertoHochschild`s
(1983)definitionofemotionallaborastheabilitytodisplayone’swayofworkingina
waythatmakesothersfeelcaredfor,bymanagingone’sownfeelingsandemotions.
Nursesdothisbymakingtheirclientsfeelsafe,comfortableandbybeingavailable
forthem.However,itisofnodoubtthatnursesexperienceemotionalstresswhen
puttingupthisprofessionalwall,especiallyiftheytakecareofachildformanyyears
asinthecaseofpediatricpalliativecare.(Maunder2008.)Thisemotionalstressmay
beaccompaniedbyburnoutandattritionifanurseusesoneofthetwostrategies
usedtoperformemotionallabor,calledsurfaceacting.Surfaceactinginvolvesdis-
playoffakeorganizationallydesiredemotions,whereasdeepactinginvolvesmodifi-
cationofone’srealemotionstoalignwithemotionaldisplayrules.(Golfenshtein&
Drach-Zahavy2014.)
Grief
Itisnotuncommonforpediatricnursestoformaspecialbondwhencaringfortheir
patientsandtheirfamilies.Itisthisuniquecaringrolethatcanexposeapediatric
nursetofrequentandintenseexperienceswithunresolvedlossandgriefwhentheir
patientsdie(Adwan2014).Griefisunderstoodastheemotionalstateofintense
sadnessresultingfromareactiontoalossinitstotality(Hall2011).Duetothecorre-
lationbetweengriefandburnout,nursestendtoexperiencebothemotionaland
physicalchronicexhaustion,depersonalization,andreducedpersonalaccomplish-
ment.Ifthisgriefisnotwelladdressed,itmayleadtofeelingsofdepression,hesita-
tiontoengageoroverinvestmentwithnewpatients,preoccupationwithdeathand
evenresignationfromwork.Consideringthedemandsofprovidingpatientcare,
9
thereislesstimefornursestoworkthroughtheirowngrief,andthustheytendto
adaptinadequatecopingstrategies.(Shinbara2009,17-19.)
3.2 Nurses’experiencesfacingdeathofchildren
Fewstudiesexistontheexperiencesofnursescaringfordyingchildren.Oneinter-
estingarticlethatstandsoutisbyPapadatou,MartinsonandChung(2001)where
theycomparepediatrichospicenurses’experiencesintwodifferentcountries.An-
otherstudybyDocherty,MilesandBrandon(2007)focusesonnurses’experiences
whenthe`dyingpoint`,wherecurativecareendsandpalliativecarebegins,is
reached.
Duetochildrendyingbeingagainsttheorderofnature,nursesaremoreaffectedby
thedeathofchildren,evenifmassiveeffortsandheroicmeasureshavebeentaken
tosavetheirlives(Morgan2009).Withthedeathofachild,thefeelingsoffailureon
thepartofhealthcareprofessionalsareperceivedinthreeparts.Theprovidersof
carefeeltheyhavefailedthechildbecausetheycouldnotsavehislife,andfeelthey
havefailedintheirsocialroleasadultstoprotectthechildfromharm.Lastly,they
feeltheyhavebetrayedtheparentswhotrustedthemwiththemostvaluablebeing
intheirlife.(ibid.)
AccordingtoDunn,Otten&Stephens(2005),issuesthataffectnurses’attitudesto-
wardscaringfordyingpatientsdependsontheirpersonalexperiences(age,race,
religion,attitudestowardsdeath),pastexperiences(levelofeducation,deathtrain-
ing)andprofessionalexperiences(monthsofnursingexperience,percentageoftime
spentincontactwithterminallyillordyingpatients).Moreexperiencedandcompe-
tentnurseshavecopingstrategies,intuitiveawareness,andtheabilitytoprovide
10
holisticcaretotheirdyingpatientswhereasnursesbeginningtheircareersstillrely
onasetofgivenrulesandguidelinestoprovidecare(ibid).
Feelingsoffearandaversionarecommonamongnurses.Theyfeelhelplessanduna-
bletoprovidegoodqualitycare,whentheyareincapabletoalleviatechildren’semo-
tionalandphysicalpainandsufferingaswellastheparents’fearanddistress.They
grieveoverthesufferingexperiencedbyparentsandoverthelossoftheirpersonal
goalsandexpectationsinrelationtothechild’scare.(Papadatouetal.2001.)Along-
sidefearandgrief,nursescanalsofeelangerintertwinedwithguiltandblameofself
andothers,especiallyifthemannerinwhichachilddiesisconsideredtobesense-
lessorpreventable.Theyblamethemselvesfornotspeakingup,fornotdoingwhat
theycouldhavedone,formissingsomethingorfordoingsomethingwrong.(Clem-
ents&Bradley2005;McDevitt2003;Rashotte,Bourbonnais&Chamberlain1997.)
Afterthedeathofapediatricpatient,nursescommonlyfeelintensesorrowbecause
theytendtoformanemotionalattachmentwiththechildandthefamily(Durall
2011).Dissonance,whichisthecontradictionbetweennurses’beliefsorexpecta-
tionstotherealitysurroundingachild’sdeath,greatlyintensifiesthenurse’ssorrow
aswellasthedurationofgrief(Alligood2013,201;Rashotte,Bourbonnais&Cham-
berlain1997).
Deathrelatedactivitieslikecleaningthebodyandtransportingittothemorgueare
partofanurse’sjob.Nursesfinditimmenselydifficulttoleavethechildinacold
barrenenvironment,furthermoreorganization’sproceduresoncaringforthede-
ceased'sbodyrequiresnursestofacethefinalityofthechild'sdeathbeforetheyare
emotionallyreadytodoso.Becauseofthis,nursesareforcedbytherealityoftheir
situationtoperformtaskstheyarenotreadyfor.
“Buttheworst,theworstfeeling,[pause]IhadwaswhenIbroughthimtothe
morgue[shudders].Wewentintothemorguewheretheyputthebodies,andthere
11
wasnobodyinthere,anditwascold.Itwas,[pause]horrific.LikeI,Iput[child's
name]down,andIgavehimagreatbighug,andabigkiss[crying],andhewasgo-
ingtobealoneinthere,[pause]allnight[sniffles].Andtherewasnomorerespect,
therewasnomorelove,therewasnomorefeeling...Itwasruthless.Idon'tknowif
that'sagoodwordtouse,but[sigh].Itwasbad.”(Rashotte,Bourbonnais&Cham-
berlain1997.)
Nevertheless,somenursesfeelsignificantlyrewardedbytheirwork.Theygaindeep
satisfactionfromtheircontributioninthecare,astheyperceivetheworktobeboth
verydifficultandmeaningful.Manyofthenursesdescribetheirroletobe“uniqueor
special”.(Papadatouetal.2001.)
3.3 Copingmechanisms
Thetermcopingcomprehendsalltheeffortsthatapersondoestomanage,accept
orreducetheinternalandexternaldemandsandstressorsthatareperceivedtaxing,
stressingoreventhreatening(Beh&Loo2012).Furthermore,copingisthecapacity
torespondandrecoverfromburdensomeandstressfulevents.Copingmechanisms,
therefore,aretheremedialactionstakenbyapersonwhosesurvivalisendangered.
Copingstrategiesdifferbyaperson'sattitudes,region,community,gender,social
group,age,religion,familyanddifferentseasons.(WHO/EHA,1999.)Additionally,
thelevelofexperience,andtheunitanurseworksinalsoaffectthecopingmecha-
nisms(WahMak,Chiang&Chui2013).
Inhealthcaresettings,nursesaretheoneswhodevelopmorepersonalrelationships
withtheirpatientsduetofrequentandclosecontactwhenprovidingcare(Peterson,
Johnson,Halvorsen,Apmann,Chang,Kershek,Scherr,Ogi&Pincon2010;Wilson&
Kirshbaum2011).Facingdeathcanbeahighlystressful,intenseandchallengingsitu-
ationfornurses(WahMaketal.2013)leadingtovariousphysical,cognitive,behav-
12
ioral,spiritualandemotionalreactions.Copingmechanismsareessentialformanag-
ingwiththenursingprofession.(Wilson&Kirshbaum2011.)
Previousstudiesconcerningcopingmechanismsorstrategiesinnursingconcernonly
adultdeaths.Moreover,moststudiesfocusonfactorssuchasworkrelatedstress,
burnoutandPTSD(Hinderer,VonRuered,Friedmann,McQuillan,Gilmore,Kramer&
Murray2014;Chipas,Cordrey,Floyd,Grubbs,Miller&Tyre2012).Thestudysettings
aremostlyfocusedonhospiceorpalliativecare(ChiHoChan,Fong,LokYWong,
ManWahTse,ShingLau&NgorChan2016;Desbiens&Fillion2007)andcriticalen-
vironments(WahMak,Chiang&Chui,2013;Shariff,Olson,SantosSalas&Cranley
2017).Furthermore,evenwithinthefieldofpediatricnursing,commonlymetpoints
ofviewarethoseofapatient’sfamily,mostlyparents’.Thefamily’scopingwiththe
deathofachild,andthewaysnursesaresupportingthefamilyarealsofrequentsub-
jectsofresearch.(AbibElHalal,Piva,Lago,ElHalal,Cabral,Nilson&Garcia2013.)
Hence,researchconcerningnurses’copingmechanismswhendealingwithchild
deathislacking.
4 Aim,purpose&researchquestion
Theaimofthisstudyistoexplorethecopingmechanismsofnurseswhenfacingthe
deathofapediatricpatient.Thepurposeofthisstudyistoprovideinformationon
howtoencounterthedeathofachildpatientandlearntoacknowledgetheideaof
it.Thisinformationcouldbeusedtoeducatefuturenursesandnursesworkingin
variousfields.
Researchquestion:
• Whatkindsofcopingmechanismsareavailablefornurseswhenfacingthe
deathofapediatricpatient?
13
5 Methodsandimplementationofthestudy
5.1 Literaturereview
Areviewofliteratureisawrittendocumentpresentedinalogicallyarguedmanner
leadingtoacomprehensiveunderstandingofthecurrentstateofknowledgeabouta
particulartopicofstudy.Itinvolvesinterpretingaselectionofdocumentsfromvari-
oussources,bothpublishedandunpublished,withtheaimofansweringresearch
questions(Wiliams&Vogt2011,184)andprovidingasoundbaseonwhichnewre-
searchideascanbefounded.(Oliver2012,1.)
Thismethodwaschosenforthisreviewtodevelopinsightsonthecopingmecha-
nismsofpediatricnurseswhentheirclientsdie.Thedecisiontonotlimitthisstudyto
aparticularcountryallowsfortheresultsoftheresearchtobeusedinevidenced
basedpracticeuniversally.Thisalsoprovidesthereadersofthisstudyalargerbody
ofanalyzedresearchinonetext(Aveyard2007,4).
Anevidencebasedliteraturereviewshouldbedoneinasystematicexplicitmanner
withareproduciblemethodforidentifying,evaluatingandsynthesizingexistingwork
producedbypreviousresearches(Fink2010,3).Unlikethenarrativereviewthatis
likelytobeinfluencedbyaresearcher`sinterest(Saks&Allsop2007,34;Bettany-
Saltikov2012,9),asystematicreviewrequiresarigorousresearchmethodologywith
limitedbiasinallaspectsofthereview(Bettany-Saltikov2012,5-9).Asystematic
reviewcallsforastringentmeta-analysisofdataandrequiresresearcherstoinclude
detailsofbothusedandnotusedstudiesthatstayrelevantwiththeresearchques-
tions(Gaerish&Lathlean2015).
14
AsoutlinedbyMachiandMcEvoy(2012),theprocessofaliteraturereviewconsists
ofsixbasicsteps.First,selectionofatopic,followedbysearchingtheliterature,then
developinganargument,andsurveyingtheliterature.Critiquingtheliteraturecomes
nextandfinally,writingthereview.Asthefirststep,asubjectthatoriginatedfrom
theinterestsoftheresearcherswasformulatedintoatopicofresearch.Asthese-
condstep,theliteraturewassearchedbymanagingdata,scanningandskimming
literature,mappingmaterialandcreatingsubjectmemorandathatleadtorefining
theresearchtopic.
Thethirdstep,developinganargument,includedbuildingthecasefortheliterature
reviewbyunderstandingclaims,buildingevidenceandlogicallyconnectingevidence
andclaim.Thus,multipleclaimargumentswereformedtobeusedinwritingthe
review.Thefourthstepconsistedofimplicativereasoning,formulatingargument
patternsandbackingtheargumentsinordertoavoidfallacies.Finally,thelaststep,
writingthereview,involvedtwoprinciplesofwriting:tounderstandandtobeun-
derstood.(4-159.)
5.2 Literaturesearch
TheliteraturesearchwasconductedduringlateFebruaryandearlyMarch2017,af-
terdefiningtheresearchquestion,searchtermsandtheinclusionandexclusioncri-
teria.Theliteraturewasreviewedbythreeindividualresearcherstominimizebias.
Theprocessofselectingtherelevantstudiesforareviewconsistsoftwophases(Bet-
tany-Saltikov2012,84).Accordingly,thesearchresultswerefirstprocessedbasedon
titleandabstracttoexcludeirrelevantresults.Inthesecondphase,fulltextsofthe
resultspassingthefirstphasewerereadtofurtherdeterminewhethertheinclusion
criteriawasmet.Figure2demonstratestheinclusioncriteriaforthisliteraturere-
view.Theinclusioncriteriawasselectedinordertofindcurrent,relevantandhigh

15
qualityresearchmaterial.Theresultsnotfulfillingtheinclusioncriteriawereauto-
maticallyexcluded.
Inclusioncriteria:
• Freefulltextaccessforstudents
• Scientificpublication
• Peerreviewed
• Publishedbetween2010-2017
• StudyinEnglish
• Answerstheresearchquestion
Figure2.Inclusioncriteria
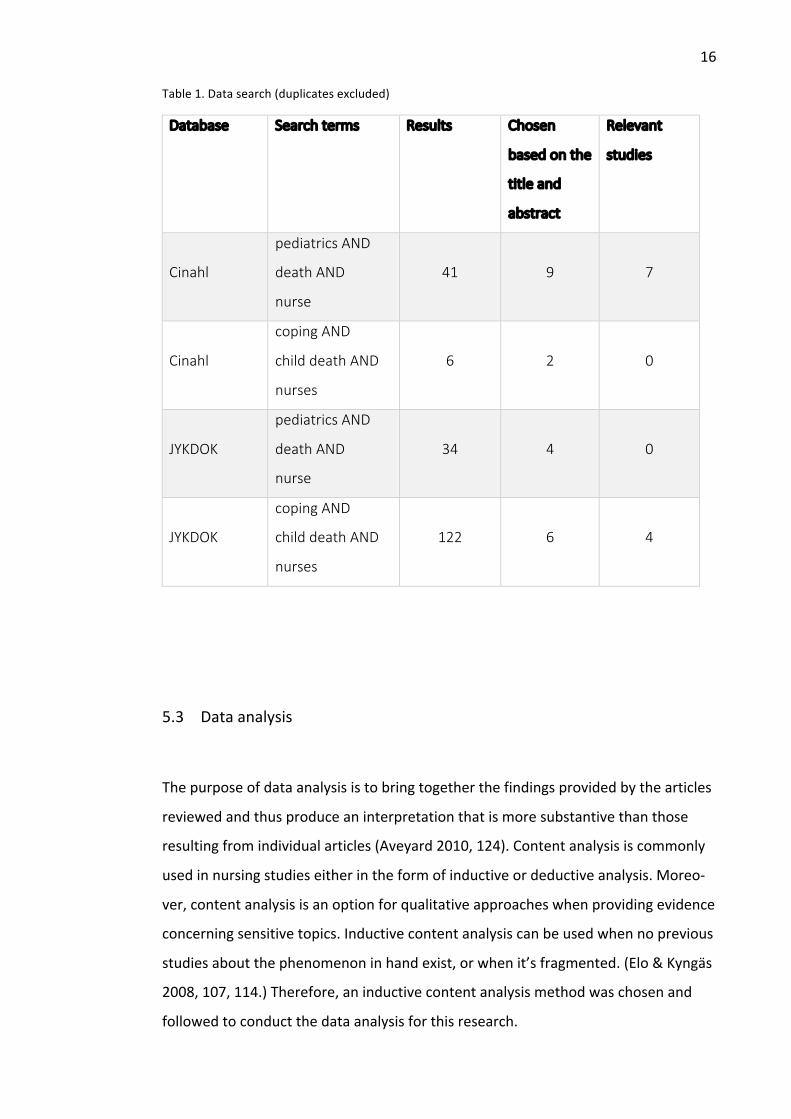
Thedatafortheliteraturereviewwasgatheredusingthefollowingtwodatabases:
CinahlandJYKDOK.ThesearchtermsusedwerepediatricsANDdeathANDnurse,
andcopingANDchilddeathANDnurses.Booleansearchwasused.Twooptionsof
searchwordswerechosenandappliedinordertogainmoreresultswithinthedif-
ferentdatabases.Bothoptionsofsearchtermswereusedtoconductasearchin
eachdatabase.Basedonthesearch,atotalof11articleswerechosentobere-
viewed.Duplicateswereexcludedfromthefinalnumberofarticles.Table1demon-
stratesthedatasearch.AtableofallthereviewedarticlescanbefoundinAppendix
1.
16
Table1.Datasearch(duplicatesexcluded)
Database Searchterms Results Chosen
basedonthe
titleand
abstract
Relevant
studies
Cinahl
pediatricsAND
deathAND
nurse
41
9
7
Cinahl
copingAND
childdeathAND
nurses
6
2
0
JYKDOK
pediatricsAND
deathAND
nurse
34
4
0
JYKDOK
copingAND
childdeathAND
nurses
122
6
4
5.3 Dataanalysis
Thepurposeofdataanalysisistobringtogetherthefindingsprovidedbythearticles
reviewedandthusproduceaninterpretationthatismoresubstantivethanthose
resultingfromindividualarticles(Aveyard2010,124).Contentanalysisiscommonly
usedinnursingstudieseitherintheformofinductiveordeductiveanalysis.Moreo-
ver,contentanalysisisanoptionforqualitativeapproacheswhenprovidingevidence
concerningsensitivetopics.Inductivecontentanalysiscanbeusedwhennoprevious
studiesaboutthephenomenoninhandexist,orwhenit’sfragmented.(Elo&Kyngäs
2008,107,114.)Therefore,aninductivecontentanalysismethodwaschosenand
followedtoconductthedataanalysisforthisresearch.
17
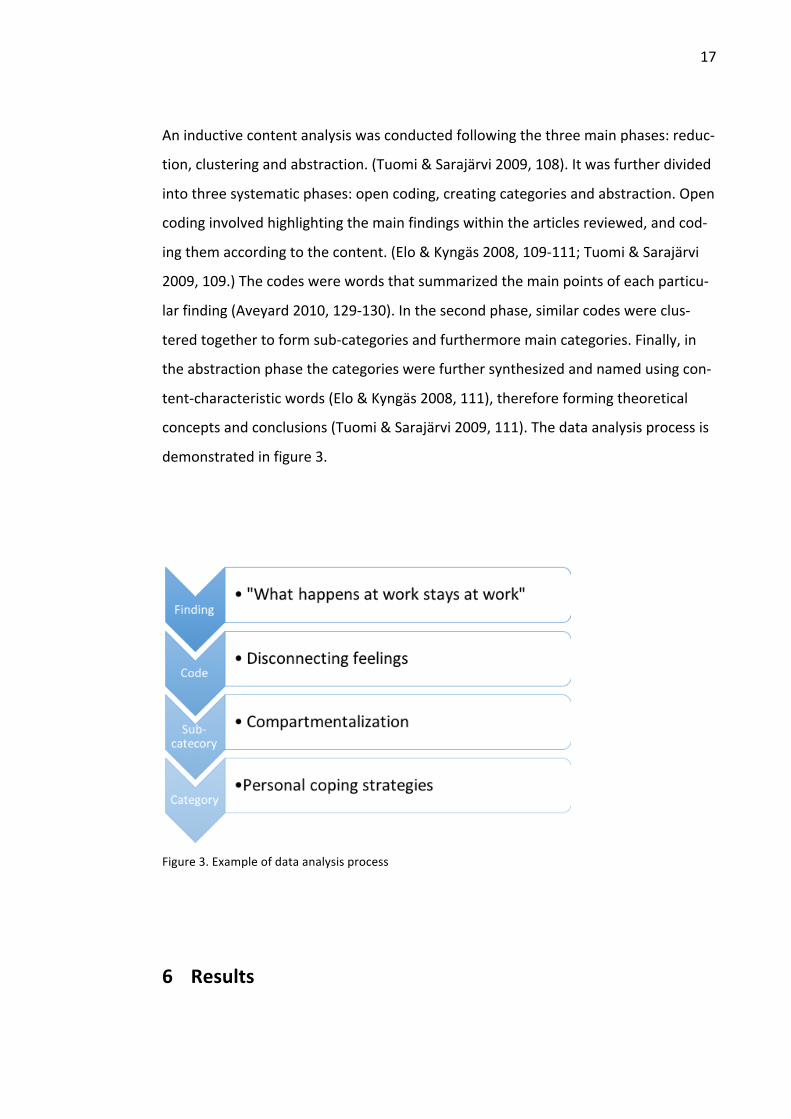
Aninductivecontentanalysiswasconductedfollowingthethreemainphases:reduc-
tion,clusteringandabstraction.(Tuomi&Sarajärvi2009,108).Itwasfurtherdivided
intothreesystematicphases:opencoding,creatingcategoriesandabstraction.Open
codinginvolvedhighlightingthemainfindingswithinthearticlesreviewed,andcod-
ingthemaccordingtothecontent.(Elo&Kyngäs2008,109-111;Tuomi&Sarajärvi
2009,109.)Thecodeswerewordsthatsummarizedthemainpointsofeachparticu-
larfinding(Aveyard2010,129-130).Inthesecondphase,similarcodeswereclus-
teredtogethertoformsub-categoriesandfurthermoremaincategories.Finally,in
theabstractionphasethecategorieswerefurthersynthesizedandnamedusingcon-
tent-characteristicwords(Elo&Kyngäs2008,111),thereforeformingtheoretical
conceptsandconclusions(Tuomi&Sarajärvi2009,111).Thedataanalysisprocessis
demonstratedinfigure3.
Figure3.Exampleofdataanalysisprocess
6 Results
18
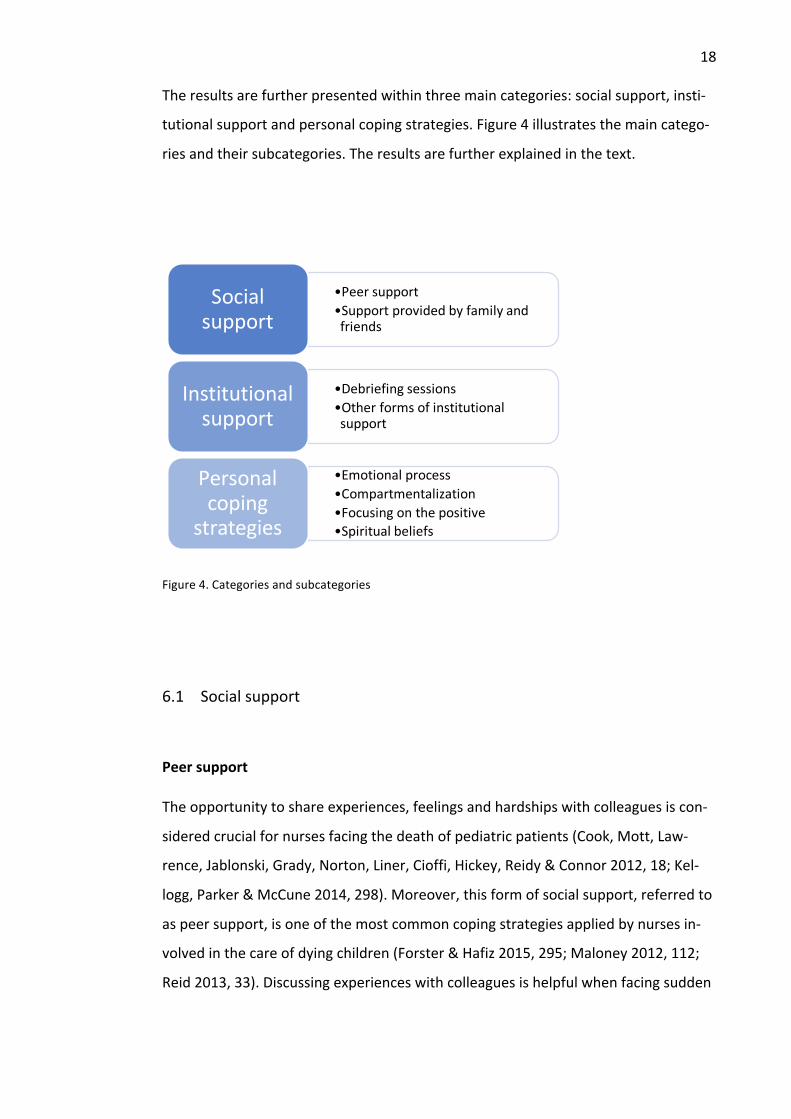
Theresultsarefurtherpresentedwithinthreemaincategories:socialsupport,insti-
tutionalsupportandpersonalcopingstrategies.Figure4illustratesthemaincatego-
riesandtheirsubcategories.Theresultsarefurtherexplainedinthetext.
Figure4.Categoriesandsubcategories
6.1 Socialsupport
Peersupport
Theopportunitytoshareexperiences,feelingsandhardshipswithcolleaguesiscon-
sideredcrucialfornursesfacingthedeathofpediatricpatients(Cook,Mott,Law-
rence,Jablonski,Grady,Norton,Liner,Cioffi,Hickey,Reidy&Connor2012,18;Kel-
logg,Parker&McCune2014,298).Moreover,thisformofsocialsupport,referredto
aspeersupport,isoneofthemostcommoncopingstrategiesappliedbynursesin-
volvedinthecareofdyingchildren(Forster&Hafiz2015,295;Maloney2012,112;
Reid2013,33).Discussingexperienceswithcolleaguesishelpfulwhenfacingsudden
•Peersupport•Supportprovidedbyfamilyandfriends
Socialsupport
•Debriefingsessions•Otherformsofinstitutionalsupport
Institutionalsupport
•Emotionalprocess•Compartmentalization•Focusingonthepositive•Spiritualbeliefs
Personalcoping
strategies

19
overwhelmingemotions,andduringtheprocessofgrievingthelosses(Cholette&
Gephart2012,17;Kelloggetal.2014,298;Pardoe2011,27).
Peersupportallowspediatricnursesto,informally,sharetheirexperiences,andfur-
thermoreexpresstheirfeelingsrelatedtoparticularcasesinvolvingchilddeath(Kel-
loggetal.2014,298;Maloney2012,112;Reid2013,33).Colleaguesareseenasa
valuablesourceofsupportduetotheiruniqueabilitytorelatetotheexperiences.
Furthermore,peersareperceivedtohavegonethroughthesamethings,tobefamil-
iarwiththeenvironmentandto‘beinitwithyou’.(Cooketal.2012,18;Forster&
Hafiz2015,295;Kelloggetal.2014,300;Stayer&Lockhart2016,354.)Thestudyby
Reid(2013,33)suggeststhatcolleaguesarehelpfulin“figuringthingsout”,whereas
StayerandLockhart(2016,354)identifysituationswhere“colleaguestrytocheer
youup”.Additionally,Kelloggetal.(2014,300)introduceaphysicalformofcollegial
support:“somepeoplewillfallapart--theyareasobbingmess,andsomebodygoes
intheretohugthemandtalktothem”.
Asaresultofthesenseofsharedexperience,thecomfortgainedfrompeersupport
isseentohavethemeanstoprovidetheaffected,grievingnurseswithpositivevali-
dation,closure,senseofpurpose,enhancedself-confidenceandthustheabilityto
continueworkingintheirunits(Forster&Hafiz2015,296;Stayer&Lockhart2016,
354).Finally,thisformofsocialsupportcanlessenwork-relatedstress(Maloney
2012,112)andasdescribedbyÅngström-Brännström,Dahlqvist,Strandbergand
Norberg(2014,7),thepositiveeffectcanalsobeseenhelpfulinbeingpresentfor
thedyingchildandthefamily.Inspiteofthevariouspositiveeffectsfound,Forster
andHafiz(2015,295-296)explainthatapossiblenegativeimpactofpeersupportis
thatthedistressratherexacerbatesasaresult.
Supportprovidedbyfamilyandfriends
20
Fewofthestudiesrevieweddescribethatsomenursesfindcomfortintheirfamilies
whencaringforadyingchild(Forster&Hafiz2015,297;Kellogg,Barker&McCune
2014,300;Pardoe2011,28;Stayer&Lockhart2016,354).Althoughnotencountered
inthereviewasoftenaspeersupport,somenursesalsoseeksocialsupport,and
furthermorecomfort,byconfidingintheirpartners.Thisformofsocialsupportis
describedforexampleasdebriefingwithsupportivepartners,talkingtospouses
aboutbadcasesandhavingone’sfamilymemberstheretolistenandtalkwith.(For-
ster&Hafiz2015,297,300;Kelloggetal.2014,300;Stayer&Lockhart2016,354.)A
spouse’sexperiencefromsimilarsettingsandthusabilitytorelatecanalsobefound
useful(Kelloggetal.2014,300).
Furthermore,thestudybyKelloggetal.(2014,300)alsospecifieschildrenasa
sourceofcomfortasfollows:“thefirstthingIwanttodo[afteracaseofpatient
death]isclimbintobedandhugmyownchild”.Finally,oneofthearticlesreviewed
alsogivesinsightintoharnessingsupportbytalkingwithone’sfriends(Pardoe2011,
28).Althoughfamilycanbeconsideredasatoolforcoping,nurses’professionalcon-
fidentialityremainsanissuewiththistypeofsocialsupport(ForsterandHafiz2015,
297).
6.2 Institutionalsupport
Debriefingsessions
Oneinstitutionalresource,createdbyapediatricpalliativecareprogram(Harriet
LaneCompassionateCare)inJohnsHopkinsChildren’sCenter,isthebereavement
debriefingsession,whichaimstoprovideemotionalsupport,increasetheabilityto
manageone’sgriefandfindmeaningwhencaringforchildrenwithlife-threatening
conditions.Thesevoluntarydebriefingsessionsareofferedforallhealthcareprovid-
ersaftereachpatientdeath,andcanbeheldwithinaweekaftertheincidentina
privatesetting.Thepurposeofthesesessionsistocompareandsharedifferent
21
healthcareproviders’emotions,experiencesandresponsestodeathand,further-
more,copingmethods.Ultimately,thesedebriefingsessionsleadtoprovidingsup-
portandsharingwisdomfrommoreexperiencedcolleaguestothenewerones.
(Keene,Hutton,Hall&Rushton2010,185-186.)
Anotherquitesimilar,structuredprocessisCriticalIncidentStressDebriefing(CISD),
whichwasspecificallydesignedforthehealthcareprofessionalsencounteringtrau-
matizingeventsandemergencies(Maloney2012,111).CISDcanbeappliedafter
variouskindsofevents,notonlythosedealingwithapatientdeath(Keeneetal.
2010,185).Therefore,thisdebriefingmethodsupportsdealingwiththephysicaland
psychologicalsymptomsevokedbyatraumaticincident(Maloney2012,111).The
timingforCISDshouldbewithinhoursaftertheincident,andlocatedneartothesite
ofthetraumaincident.Thus,comparedtoBereavementDebriefingsessions,the
CISDsessionsaremoreacute.CISDisconsideredareviewoftheincidentsbefore,
duringandafterthecrisis.Itallowsthehealthcareprofessionalstoprocessandre-
flecttheincident,andfurthermoreallowstoventilatethoughtsandemotionsassoci-
atedwiththetraumatizingevent,thussupportingthehealingprocessofthestaff.
(ibid,110-111.)
Otherformsofinstitutionalsupport
Someinstitutionsoffermentoringprograms,whereanewlygraduatednurseis
matchedwithanexperiencednurseforsupportandlearningcopingmechanisms
(Maloney2012,111).Additionally,othermentoringprograms,peerorteamsupport
meetingsandclinicalsupervisionarementioned(Maloney2012,112-113;Pardoe
2011,28).AstudybyCook,Mott,Lawrence,Jablonski,Grady,Norton,Liner,Cioffi,
Hickey,ReidyandConnor(2012)introducesthePediatricAdvancedCareTeam
(PACT)asamajorformofsupportinthepediatricsetting,whendealingwithdying
childrenandtheirfamilies.Theteamassistsboththefamiliesandtheprofessionals.
PACTiscomposedofanursepractitioner,physicians,asocialworkerandacoordina-
22
tor,whohaveallreceivedadditionaltrainingforpalliativeandend-of-lifecare.PACT
facilitatesdiscussionsaboutdeath,andassiststhehealthcareteamwithdecision-
makingandexploringtreatmentoptionsandgoals.Moreover,PACTprovidesaguide
toqualityandmeaningfulend-of-lifecareandassessingproperpainandsymptom
managementforthechild.Asaresult,manynursesexpressfeelingsofreliefanddi-
minishmentofpressureincare,becauseofthepresenceandsupportofthePACT.
(18.)
Finally,anissuethatispointedoutaslackinginmanysystemsiseducation.Never-
theless,someofthearticlesalsodiscusseducationprovidedforhealthcareprofes-
sionals.Palliativecareeducation(Keenan&MacDermott2016,22;Keene,Hutton,
Hall&Rushton2010,186),forumsandconferencesforclinicalsupportandritualsfor
remembrance(Keeneetal.2010,186),arementionedaseducationalresources.Psy-
chologicalsupportaswellassessionswiththehospital’spsychologistarealso
sourcesforsupportingnursescoping(Pardoe2011,28).
Someinstitutionsalsoprovidedifferentkindsofrelaxationmethods,suchastran-
quilityrooms,therapies(aromatherapy)andmassagechairs.Somearrangements
requestedbynursesthemselves,suchasreflexologyandothertypeoftherapiesare
alsomentionedinthereviewedarticles.(Forster&Hafiz2015,297;Maloney2012,
112).Nevertheless,workingintensivelywithfamiliesandtheirdyingchildrenhasa
highinfluenceonsomeoftheprofessionals,leadingtotheneedofsickleave.This
personalcopingstrategyprovidedbytheinstitutionisvitalforsomehealthcarepro-
fessionals.(Forster&Hafiz2015,297.)
6.3 Personalcopingstrategies
Emotionalprocess
23
Theneedtotakecareofoneselfisexpressedbymanynurses.Somenursesdothisby
exercisingafterexperiencingalossoftheirpatients,somebyrelaxing,eatingwell
andbasicallypamperingthemselves.(Kelloggetal.2014,300;Pardoe2011,29.)
Knowingthattheyhavedonealltheycouldfortheirpatientsandhavinghadestab-
lishedatrustfulrelationshipwiththechildandtheirfamilyalsohelpsnursestoper-
sonallycopewiththedeathoftheirclients.Inthecasethatthistrustisestablished
throughoutthecourseoftreatmentthenursefeelscomfortedbecausesheknows
thathercarehasmadeadifferenceandshehashelpedalleviatethechild'spain.
(Ångström-Brännströmetal.2014,6.)
Acknowledgementoflosswhileexpressinggriefandsorrowisusedbynursestocope
withthedeathoftheirchildpatients.Acceptingthatdeathispartofanurse`slife
allowsnursestofacetherealityandmoveontocaringfornewpatients.(Cholette&
Gephart2012,298.)Somenursesexpresstheirsorrowopenlybycryingwhenthey
loseachildpatient,andsomeevencrywiththebereavedfamilies(Kelloggetal.
2014,299).ItisnotedbyKelloggetal.(2014)thatalthoughnursesarepreparedto
dealwithfamiliesduringillnessesandloss,theirreleaseofemotionswhentheylose
achildpatientisminimalandthismayleadtofrustrationandcareerfatigue.Forthis
reason,nursesshouldhavetheabilitytomanagetheirgrieftoavoidnegativeimpli-
cationsontheirprofessionalpractice(298).
Compartmentalization
Compartmentalizationisdonetomaintainanoutwardprofessionaldemeanorandto
continuecaringforthebereavedfamilies.Itinvolvessettingone'sfeelingsasidein
ordertogoonwiththejob,butthenworkingonthosefeelingslater.Nursesfeelthat
thiscopingskillaffordsthemtimetoworkthroughtheiremotionsandconflicting
feelingsofthedeathofachildatalatertime(Forster&Hafiz2015,296-297,300;
Kelloggetal.2014,299-300.)Compartmentalizationisdifferentfromdisconnecting
whichinvolvesturningoffone'semotionalsideanddoingone'sjobofcaringand
24
supportingtheliving,thebereavedfamilies,andnotworkingonthoseemotions
(Cholette&Gephart2012,17-18;Cooketal.2012,17).Tosomenurses,thiscoping
skillisextendedhomeastheyavoidtakingworkhomewiththemandthusemploy
strategiessuchaslabellingtoprotecttheirfamilies.Therefore,theyanswertoques-
tionssuchas‘howwaswork’by,forexample,sayingtheyhadabaddayinsteadof
sayingtheylosttheirpatients(Cooketal.2012,18.)
Finally,settingprofessionalboundaries,byplacingtheprofessionalandpersonalline
betweenfamilymembersandstaff,isalsoawaysomeofthenursescope.Nurses
usethislineasaguideonhowinvolvedtheyshouldbe.Furthermore,theyusethisto
maintainanemotionalseparationthusavoidingburnout.Nevertheless,thesenurses
acknowledgethattheprofessionallineissomewhatfluid,asthelevelofinvolvement
changesfromonepatienttoanother.Thetermprofessionalboundariesisdescribed
asuncomfortableforsomenurses,astothemthetermimplies‘notcaring’.There-
fore,thisissimplynotanoptiontoallnurses.(Cooketal.2012,15-18.)
Focusingonthepositive
Whenpersonallydealingwiththedeathofapediatricpatient,nursesfindfocusing
onthepositivetobeausefulcopingmechanism(Keenan&MacDermott2016,21-
22).Somenursesdescribetheneedtomakesomegoodoutofabadsituation,even
beforeachildpasseson.Theydothisbyprovidingasmuchcomforttothechildand
thechild'sfamilyastheycan.(Stayer&Lockhart2016,353.)Furthermore,nurses
describetheneedtocreateapeacefulendingforthechildandthefamily,asthis
helpsthemfindandmakemeaningofthedeathofapediatricpatient(ibid.,354-
355).
Tosomenurses,focusingonthepositivemeansthattheytakeituponthemselvesto
studyaboutpalliativecare,ortodeveloptheirpracticeoncaringforthedying(Kee-
nan&MacDermott2016,19).Thesenursesacknowledgethatalthoughthese
25
measuresdonotchangetheirpreviousexperiences,itenablesthemtoknowthat
theyhavetheabilitytopreventsimilarsituationsfromhappeningand,hence,both
reducestheirpotentialguiltandbuildstheirconfidence(ibid.,21).
Focusingonmemoriesbyusingbedsidephotosofachildpatientisdescribedhelpful
bysomenurseswhencopingwiththedeathoftheirpatients.However,somenurses
findtheuseofbedsidephotosmoredistressingthanhelpfulasseeingthecomplete
transformationtheirpatienthasmadefromahappychildtoadyingchildmakes
themsad.(Cooketal.2012,17.)Finally,thepromiseoftomorrowbringingwithita
cleanslate,anewchildtocarefor,anopportunitytogetbackonandtokeeptrying
isdescribedbysomenursesasanewbeginning,awaytofocusonthepositive
(Cholette&Gephart2012,16-17).
Spiritualbeliefs
Spiritualitycanbeseenasaformofpersonalcopingstrategy.Spiritualbeliefs,reli-
gionandattendingthechild’sfuneralforclosurearerecognizedascopingmecha-
nismwhenfacingthedeathandlossofachildpatient.(Forster&Hafiz2015,298;
Keenan&MacDermott2016,21-22;Reid2013,33,35-36.)Forsomenurses,spiritu-
alityishelpfulwhencopingwithpatientdeath,asmeaningmakingandexistential
questionsaboutlife’spurposearereviewed(Forster&Hafiz2015,297-298).Like-
wise,meditationisusedasacopingmechanismbysomenursestoprocessthe
death,andfindmeaningandcomfort(Kellogg,Barker&McCune2014,300).
Religionandfaith,beingapartofsomenurses’everydaylife,arealsoseenasacom-
fortingcopingstrategy(Keenan&MacDermott2016,22).Religiousbeliefsandre-
sources,Godandprayer,areusedascopingmethodswhensupportandmeaning
makingafterachild’sdeathisneeded(Forster&Hafiz2015,298;Keenan&Mac
Dermott2016,21-22).Finally,forsomenurses,funeralscontributetotheemotional
coping(Reid,2013,35).Therearecaseswherethenursesarenotpresentwhena
26
childpatientdies,andthustheyfeeltheyarenottheretosupportthechildandthe
family.Thiscanleadtonotgettingthesenseofpersonalclosure.Inthesesituations,
thesupportfromtheinstitutionfornursestoattendthepatient’sfuneralisveryval-
uable.(Keenan&MacDermott2016,21.)Moreover,funeralsareseenasritualsand
settingswherenursescouldgrieveopenly,acknowledgethedeathofthechildand
getthesenseofclosure.(Keenan&MacDermott2016,21;Reid2013,33,35.)
7 Discussion
7.1 Ethicalconsiderations,validityandreliability
Ethicsinresearchisdescribedasthenormsforconductsthatguidesmethods,pro-
ceduresorperspectiveswhenanalyzingandpresentingcomplexproblemsandissues
(Resnik2011).Mainprinciplesofethicsincluderespectforhumandignity,privacy
andautonomy.Theseprinciplesalsoincludehonestyinreportingdata,resultsand
proceduresandavoidingmisrepresentation,fabricationorfalsificationofdata.One
hastobecarefuloftheirownworkandkeepgoodrecordsofresearchactivities
(ibid).
Asthisstudywasbasedonthemethodologyofliteraturereviewwhereprevious
studieswereusedasrawmaterials,onemajorethicalissuearosearoundinterview-
ingchildren(Ångström-Brännströmetal.2014).Theauthorsofthisresearchdebated
theethicsofinterviewingadyingchildandthemother.Theyalsowonderedifitwas
sufficienttoconsiderthechild'sconsenttotheoriginalresearchers(Ångström-
Brännströmetal.2014)asapermissionforthemtousethedata.However,because
thisstudywasdonefromanurse`sperspective,thisdidnotpresentachallenge.
27
Byensuringappropriatereferencingandavoidingmisrepresentationofotherau-
thor`sworksastheirown,thewritersofthisresearchpracticedtheprincipleofhon-
estythroughavoidingplagiarismandfabrication(Price2014,46).Presentationof
dataandresultsthatarosefromthisresearchwasdoneinanhonestandcareful
manner,andrecordsoftheresearchprocesswaskeptintheformofphotographs.
Thiswasdonetoavoidanyclaimsoffalsification.
Thedegreetowhicharesearchislikelytobefreeofbias,believableandtrueiswhat
definesvalidity(Buckingham,Fisher&Saunders2008).Inordertoadheretothis
principleandavoidbias,theauthorsscrupulouslyresearchedliteratureandaccurate-
lydocumentedresearchdataandresults.Thiswasdonetoallowforreviewal,evalu-
ationandreproducibilityoftheresearch.Althoughunintentional,publicationbiasis
evidentinthisresearch,astheauthorsbeingstudentshadlimitedaccesstoexisting
literature.
Theliteraturereviewedinthisstudyisfromsixcountries:TheUnitedStates,Austral-
ia,NewZealand,Scotland,Ireland,andtheUK.ThelanguageusedisEnglishandthe
researchmethodswereallqualitative.Thislimitsthegeneralizationoftheresults
takingintoaccountthesimilaritiesinculturethatthe6countriesshare.Themeth-
odologybeingthesameinallthereviewedliterature,presentsalimitationinthe
variationswithinthestudiesthemselves.
Thearticlesreviewedinthisstudyhadbeenresearchedondifferentsettings:pediat-
ricintensivecareunits,pediatricpalliativecareunits,oncologycaresettings,perina-
talcareunits,pediatricburncareunits,emergency,traumaunits,andgeneralacute
careunits.ThestudybyKeenanandMacDermott(2016)wasopentonurseswork-
inginanyfieldwhohadcaredforachildwhohaddiedinthepastsevenyears.This
varietyofsettingsallowfortheresultsofthisresearchtobeappliedindifferent
fieldsofnursingandincreasesitscredibility.
28
Thisresearchwasdonewiththethemeofstabilityinmind.Carewastakentoensure
thatthestepsoftheresearchwereclearenoughtoallowforduplicationofthere-
sultsbyanotherresearcherifalltheotherfactorsremainedconstant.Literaturein-
clusioncriteriawasplainlyoutlined,ideasandthoughtspreciselycredited,andre-
viewedliteratureswereputunderthesameethicalguidelinesaprimaryresearch
studywouldhavebeenputthrough.Thiswasdonetoemploytheprincipleofrelia-
bilityinresearch.(Houser2008;Roberts,Priest&Traynor2006,41.)
Thenumberofauthorsofthisresearchbeingthreealsoincreasesthereliabilityof
thestudyasopennessintermsofdatasharing,discussionsandcriticisms(Resnik
2011)wasemployed.Thisallowedforreviewevenduringtheresearchperiod.How-
ever,allthreeauthorsbeingbeginnersinconductingaresearchmayaffectthequali-
tyofthestudyintermsofdatapresentationandreliability.
7.2 Discussionoftheresults
Nursesworkinginpediatricpalliativeorcriticalcarewherechildrendieeveryday,
someunexpectedlyandsomeafteralongend-of-lifecare,oftenhaveoverwhelming
experiences.Encounteringthesesituationsdailyhasanemotional,physical,spiritual,
behavioralandcognitiveimpactonnurses(Cui,Shen,Ma&Zhao2011,403;Keene,
Hutton,Hall&Rushton2010,185).Iftheseexperiencesarenotdealtwith,thenurs-
es’professionalpracticeandoutcomesofcarecanbeaffectednegatively(Cui,Shen,
Ma&Zhao2011,403;Keeneetal.2010,185;Maloney2012,111).Therefore,death
asaneventshouldbeconfrontedratherthanavoided(Cui,Shen,Ma&Zhao2011).
Nevertheless,asoftheseresults,itwasagreedbytheauthorsofthisstudythatallof
thecopingmechanismsintroducedmaynotbeapplicabletoeverypracticingnurse.
Simplythefactthateverynurseisdifferentfromage,genderornationalityalone
makesdiversityinthecopingbehaviors.Additionally,thestudybyCook,Mott,Law-
29
rence,Jablonski,Grady,Norton,Liner,Cioffi,Hickey,ReidyandConnor(2012),ana-
lyzedsomespecificfactorsthatinfluencethecopingbehaviorsofnurses.Afewmain
componentspointedoutwerethelevelofexperienceofnurses’,theyearsofprac-
ticeinaparticularunit,andthelengthoftimetheyhadcaredforaparticularpatient.
(18.)Basedontheresults,itseemsthathavingmoreexperiencemightcorrelateto
havingmoretoolsforcoping.Thenagain,eventhoughonecanlearntoacceptdeath,
itseemsunlikelytogetfullyaccustomedtoit.Religionandone’sownspiritualitywas
seentobothsupportanddisturbcoping.Anotherfactoraffectingnurses’copingwas
iftheyhadchildrenoftheirown(ibid.).Yet,beingawareofone’sownneeds,
strengthsandlimitationsisthekeytofindingthemostsuitablecopingmechanisms
(Furingsten,Sjörgen&Forsner2015,180).
Socialsupportwasintroducedasausefulcopingmechanismin9outofthe11arti-
clesreviewed.Basedontheresultsgainedwithinthisstudy,socialsupportcouldbe
perceivedasthemostcommonlyusedformofcoping,duetoitsextensiveavailabil-
ity.Furthermore,evenforundergraduates,peersupportseemstobethemostnatu-
ral,althoughsometimessubconscious,copingstrategy.However,surprisingly,oneof
thearticlesalsogaveinsighttoapossiblenegativeimpactofit.Forster&Hafiz(2015,
295-296)explainedthatpeersupport,asindiscussingwithcolleagues,mightactually
exacerbatethefeelingsofanxietyanddistress.Indemandingworkenvironments,
socialsupportmight,insomecases,contributetodistressratherthanrelief.Moreo-
ver,inadequateorpoorsupportmayevencauseadditionalstress.(Button2008,
509-510.)
Anotherissueraisedwithinsocialsupportwasmaintainingprofessionalconfidentiali-
tywhileapplyingfamilysupport(Forster&Hafiz2015,297).Confidentialityinhealth
careisexplainedastheactofkeepingpatientinformationprivateorsecret.Thus,
onlynecessarypatientinformationcanbesharedwithotherhealthcareprofessionals
whoneedtheinformationinordertoprovidecare.Inrelationtotheconceptofchild
death,itshouldalsobenotedthatapatient’srighttoconfidentialityremainsafter
30
death.(NMC2015.)Discussingpatientcasesathomemightbreachtoofarfromthe-
seregulations,andthereforeoneshouldbecarefulwhensharingtheseexperiences.
Withinthecategoryofinstitutionalsupport,twoUSA-basedarticlesexplainedthe
useofdebriefingsessions,criticalincidentstressdebriefing(Maloney2012)andbe-
reavementdebriefing(Keene,Hutton,Hall&Rushton2010).Thesetwoformsofde-
briefing,whenaccessibletodistressednurses,areausefultoolforcopingwiththe
casesofchilddeath.However,incomparisontosocialsupport,theavailabilityand
applicationofthesesessionsremainedaquestiontotheauthorsofthisstudy.
Thelackofeducationandthuspreparednessconsideringthedeathofapediatric
patientwasbroughtupbymanyofthearticlesreviewed(Forster&Hafiz2015;Kee-
nan&MacDermott2016;Kellogg,Barker&McCune2014;Reid2013).Overall,nurs-
eslackformaleducationinbothundergraduatecurriculumsandduringworkinglife.
Sufficienteducationthatconsidersdeathfromvarious,holistic,pointsofviewcould
helpnursestoconfrontdeathasaphenomenonmorenaturallyandtoprovidegood
qualitycare.(Ciu,Shen,Ma&Zhao2011,403-404;Edo-Gual,Tomas-Sabado,Bar-
dallo-Porras&Monforte-Royo2014.)AccordingtothearticlebyKelloggetal.(2014,
300),thephysicalaspectofcaringforthedeadmighthavebeendiscussed,butcop-
ingwiththepsychologicalaspectwasnotprocessed.Furthermore,insomecases,
thedeathofadultpatientswasaddressed,butinpediatricstheprocessofdyingwas
overlooked(Kelloggetal.2014,300).Thus,theresearchhighlightedtheneedfor
moreeducationinthisparticular,sensitiveareaofnursing.
Intermsofpersonalcopingstrategies,anissuediscussedbytheauthorswasthatin
somecasessettingstrictprofessionalboundariesmightcomeacrossasnotcaring.
Furthermore,assaidinthearticlebyCook,Mott,Lawrence,Jablonski,Grady,Nor-
ton,Liner,Cioffi,Hickey,Reidy&Connor(2012,15)“thedaywestopfeelingisthe
daythatweneedtoquit...ifwedon’tgetaffectedbyachild’sdeath,that’swhenyou
needtorethinkyourprofession”.It’svitaltodrawthelinebetweenoneselfasaper-
31
sonandasaprofessional.Therefore,it’salsoessentialtoknowthedifferencebe-
tweentherealfeelingof“notcaring”andthedismissalofone’sfeelingsduetopro-
fessionalboundaries.Secondly,asintensepersonalfeelingssuchasgriefandanxiety
areconsideredanaturalresponsetodeath(Cui,Shen,Ma&Zhao2011,403)it
seemsvitalfornursestorecognizeandacceptsuchfeelings,eventhoughitmight
sometimesbeperceivedunprofessional.
Anotherdilemmaariseswhenthefamiliesofthedyingchildexpectthenursetoem-
pathizeandgrievewiththem,whilethenursetriestomaintainprofessionalism
(Cholette&Gephart2012,14).Hence,tosupporttheparents,nursesmustbalance
theirownemotionalexpressionsaccordingtoeachuniquesituationandthefamily’s
wishes(Furingsten,Sjörgen&Forsner2015,179-180).Thequalityoftherelationship
formedwiththedyingchildandthefamilymightalsoinfluencethecopingofboth
partiesinvolved.
Finally,pediatricnursingalwaysrevolvesaroundthewholefamily,andthusthephe-
nomenonofachildpassingencompassestheemotionalprocessofboththefamily
andthenurse.Althoughthedeathofachildisdevastating,itcouldalsobeseenasa
reliefforasufferingchild.Interestingly,theremaybeconsiderabledifferencesto
howachild’sdeathiscopedwithwhenit’sduetoalong-termillnessandwhenit’s
sudden.Therefore,copingwithsuchoverwhelmingexperiencesisnotonlyvitalfor
thefamilybutalsoforthenursesinvolved.Thefamily’scopinghasbeenstudiedbe-
fore,whereaslessfocushasbeengiventothenurses’pointofview.Basedonthis
research,variouscopingmechanismsareavailablefornursesfacingthedeathofpe-
diatricpatients,butnotallofthemaresuitableforeachindividual.Theseresults
couldbeappliedtovariousnursingsettingsandforeducationalpurposesforunder-
graduates.
Theauthorsagreedthattheavailabilityandqualityofinstitution-basedcoping
mechanismsshouldberesearchedfurther.Additionally,toallowforefficientcoping

32
indifferentnursingsettings,furtherresearchisneededtodeterminewhatkindsof
copingmechanismswouldbebestapplicableforeachparticularsetting.Asanexam-
ple,inthecurrentworldnursesmightalsoworkinareasofconflictanddisaster
wheredeathofchildrencanbearegularoccurrence.Therefore,furtherresearch
shouldbeconductedonwhatkindsofcopingstrategiesareapplicableforsuchde-
mandingsettings.
33
References
AbibElHalal,G.MC.,Piva,J.F.,Lago,P.M.,ElHalal,M.GS.,Cabral,F.C.,Nilson,C.&Garcia,P.CR.2013.Parents’perspectivesonthedeathsoftheirchildrenintwoBrazil-ianpaediatricintensivecareunits.InternationalJournalofPalliativeNursing,19(10).
Adwan,J.2014.PediatricNurses'GriefExperience,BurnoutandJobSatisfaction.JournalofPediatricNursing,29(4),329–336.
Alligood,M.R.2013.NursingTheory:Utilization&Application.5thEdition.ElsevierHealthSciences.
Ashorn,P.2016.Historiallinenkehitysjakuolleisuudenennustetekijät.Lastentaudit.Duodecim/Oppiportti.KustannusoyDuodecim2016.
Aveyard,H.2010.DoingaLiteratureReviewinHealthandSocialCare:APracticalGuide.2ndEdition.OpenUniversityPress.England.McGraw-HillCompanies.
Bailey,C.,Murphy,R.&Porock,D.2011.Professionaltears:developingemotionalintelligencearounddeathanddyinginemergencywork.Journalofclinicalnursing,20(23-24),3364–3372.
Beh,L-S.2012.JobStressandCopingMechanismsamongNursingStaffinPublicHealthServices.InternationalJournalofAcademicResearchinBusinessandSocialSciences,2(7).Accessedon14February2017.Retrievedfromhttp://www.hrmars.com/admin/pics/912.pdf
Berlinger,N.,Barfield,R.&Fleischman,A.2013.FacingPersistentChallengesinPedi-atricDecision-Making:NewHastingsCenterGuidelines.AmericanAcademyofPedi-atrics,132(5).
Bettany-Saltikov,J.2012.HowToDoASystematicliteratureReviewinNursing:AStepbyStepGuide.Mcgraw-HillEducation.UK
Blackstone,S.&Pressman,H.2011.EffectiveCommunicationinChildren’sHospitals:AHandbookofResourcesforParents,Patients,andPractitioners.CentralCoastChil-dren’sFoundation.AugmentativeCommunicationInc.RehabilitationEngineeringResearchCenteronCommunicationEnhancement(AACRERC).Accessedon30Janu-ary2017.Retrievedfromhttp://www.patientprovidercommunication.org/pdf/25.pdf
Black,R.E.,Cousens,S.,Johnson,H.L.,Lawn,J.E.,Rudan,I.,Bassani,D.G.,Jha,P.,Campbell,H.,FischerWalker,C.,Cibulskis,R.,Eisele,T.,Liu,L.&Mathers,C.2010.
34
Global,regional,andnationalcausesofchildmortalityin2008:asystematicanalysis.TheLancet.Accessedon29January2017.Retrievedfromhttp://cdrwww.who.int/immunization/monitoring_surveillance/resources/Lancet_2010_withAppendix.pdf
Buckingham,J.,Fisher,B.&Saunders,D.2008.ClinicalEpidemiologyGlossary:Validi-ty.EvidenceBasedMedicineToolkit.Accessed17April2017.Retrievedfromhttp://www.ebm.med.ualberta.ca/Glossary.html
Button,L.A.2008.Effectofsocialsupportandcopingstrategiesontherelationshipbetweenhealthcare-relatedoccupationalstressandhealth.JournalofResearchinNursing,13(6),498-524.
ChiHoChan,W.,Fong,A.,LokYWong,K.,ManWahTse,D.,ShingLau,K.&NgorChan,L.2016.ImpactofDeathWorkonSelf:ExistentialandEmotionalChallengesandCopingofPalliativeCareProfessionals.Health&SocialWork,41(1).
Chipas,A.,Cordrey,D.,Floyd,D.,Grubbs,L.,Miller,S.&Tyre,B.2012.Stress:Percep-tions,Manifestations,andCopingMechanismsofStudentRegisteredNurseAnesthe-tists.AANAJournal,80(4).
Cholette,M.&Gephart,S.M.2012.AModelfortheDynamicsofBereavementCare-giving.InternationalJournalofChildbirthEducation,27(2),14-18.
Clements,P.&Bradley,J.2005.Whenayoungpatientdies.RN,68(4)40-45.
Cook,K.A.,Mott,S.,Lawrence,P.,Jablonski,J.,Grady,M.R.,Norton,D.,Liner,K.P.,Cioffi,J.,Hickey,P.,Reidy,S.&Connor,J.A.2012.CopingWhileCaringfortheDyingChild:Nurses'ExperiencesinanAcuteCareSetting.JournalofPediatricNursing,27,e11–e21.
Cui,J.,Shen,F.,Ma,X.&Zhao,J.2011.WhatDoNursesWanttoLearnFromDeatheducation?ASurveyofTheirNeeds.OncologyNursingForum,38(6),402-408.
Desbiens,J-F.&Fillion,L.2007.Copingstrategies,emotionaloutcomesandspiritualqualityoflifeinpalliativecarenurses.InternationalJournalofPalliativeNursing,13(6).
Docherty,S.L.,MilesM.S.,&Brandon,D.2007SearchingFor"TheDyingPoint:"Pro-viders'ExperienceswithPalliativeCareinPediatricAcuteCare.PediatricNursing,33(4),335-341.
35
Dunn,K.S.,Otten,C.&Stephens,E.2005.NursingExperienceandtheCareofDyingPatients.OncologyNursingForum,32(1).Accessedon22March2017.Retrievedfromhttp://www.researchgate.net/profile/Karen_Dunn3/publication/8071591_Nursing_experience_and_the_care_of_dying_patients/links/0fcfd50aa5cc831c84000000.pdf
Durall,A.2011.CareoftheCaretaker:ManagingtheGriefProcessofHealthCareProfessionals.PediatricAnnals,40(5).CME.
Edo-Gual,M.,Tomas-Sabado,J.,Bardallo-Porras,D.&Monforte-Royo,C.2014.Theimpactofdeathanddyingonnursingstudents:anexplanatorymodel.JournalofClin-icalNursing,23,3501-3512.
Elo,S.&Kyngäs,H.2008.Thequalitativecontentanalysisprocess.JournalofAd-vancedNursing62(1),107-115.2007BlackwellPublishingLtd.
Fink,A.2010.ConductingResearchLiteratureReviews:FromInternettopaper.3rdEdition.USA:SagePublicationsltd.
Forster,E.&Hafiz,A.2015.Paediatricdeathanddying:exploringcopingstrategiesofhealthprofessionalsandperceptionsofsupportprovision.InternationalJournalofPalliativeNursing,21(6),294-301.
Furingsten,L.,Sjörgen,R.&Forsner,M.2015.Ethicalchallengeswhencaringfordy-ingchildren.NursingEthics,22(2),176-187.
Gerrish,K.&Lathlean,J.2015.TheResearchProcessinNursing.7thEdition.Black-wellPublishingLtd.
Golfenshtein,N.&Drach-Zahavy,A.2014.Anattributiontheoryperspectiveonemo-tionallabourinnurse-patientencounters:anestedcross-sectionalstudyinpaediatricsettings.JournalofAdvancedNursing,71(5),1123-1134.
Hall,C.2011.BeyondKübler-Ross:Recentdevelopmentsinourunderstandingofgriefandbereavement.AustralianPsychologicalSociety.Accessedon1February2017.Retrievedfromhttps://www.psychology.org.au/publications/inpsych/2011/december/hall/
Hinderer,K.A.,VonRuered,K.T.,Friedmann,E.,McQuillan,K.A.,Gilmore,R.,Kra-mer,B.&Murray,M.2014.Burnout,CompassionFatigue,CompassionSatisfaction,andSecondaryTraumaticStressinTraumaNurses.JournalofTraumaNursing,21(4).
36
Houser,J.2008.Precision,Reliability,andValidity:EssentialElementsofMeasure-mentinNursingResearch.JournalsforSpecialistsinPaediatricNursing,13(4).
Keenan,P.&MacDermott,C.M.2016.HOWNURSESGRIEVEFORCHILDRENWHODIEINTHEIRCARE.LearningDisabilityPractice,19(3),16-22.
Keene,E.A.,Hutton,N.,Hall,B.&Rushton,C.2010.BereavementDebriefingSes-sions:AnInterventiontoSupportHealthCareProfessionalsinManagingTheirGriefAftertheDeathofaPatient.PEDIATRICNURSING,36(4),185-189.
Keidel,G.C.2002Burnoutandcompassionfatigueamonghospicecaregivers.Ameri-canJournalofHospice&PalliativeCare,19(3).Accessedon22March2017.Re-trievedfromhttp://ajh.sagepub.com/content/19/3/200.full.pdf+html
Kellogg,M.B.,Barker,M.&McCune,N.2014.TheLivedExperienceofPediatricBurnNursesFollowingPatientDeath.PEDIATRICNURSING,40(6),297-300.
Kyle,T.2008.EssentialsofpediatricNursing.WoltersKluwerhealth.Lippincott,Wil-liams&Wilkins.
Levelsandtrendsinchildmortality.2015.UNInter-agencygroupforchildmortalityestimation.Accessedon29January2017.Retrievedfromhttp://www.childmortality.org/files_v20/download/IGME%20Report%202015_9_3%20LR%20Web.pdf
Levetown,M.2008.CommunicatingwithChildrenandFamilies:FromEverydayIn-teractionstoSkillinConveyingDistressingInformation.AmericanAcademyofPediat-rics,121(5).Accessedon29January2017.Retrievedfromhttps://pediatrics.aappublications.org/content/pediatrics/121/5/e1441.full.pdf
Linnard-Palmer,L.&Coats,G.2016.SafeMaternityandPediatricNursingCare.F.A.Davispublishers.283-284.
Machi,L.A.&McEvoy,B.T.2012.Theliteraturereview:SixStepstoSuccess.USA:CorwinPress
Maloney,C.2012.CriticalIncidentStressDebriefingandPediatricNurses:AnAp-proachtoSupportTheWorkEnvironmentandMitigateNegativeConsequences.PEDIATRICNURSING,38(2)110-113.
Maunder,E.2008.Emotionmanagementinchildren'spalliativecarenursing.IndianJournalofPalliativeCare,14(1),45-50.
37
McDevitt,C.M.2003.Withoutwarning:sometimes,thingsgowrongdespiteourbestefforts.Nursingcentre.
Morgan,D.2009.CaringforDyingChildren:AssessingtheNeedsofthePediatricPal-liativeCareNurse.PediatricNursing,35(2).Accessedon22March2017.Retrievedfrom:http://www.pediatricnursing.net/ce/2011/article35086090.pdfNMC.2015.TheCode:Professionalstandardsofpracticeandbehaviourfornursesandmidwives.NursingandMidwiferyCouncilUK.Accessedon10April2017.Re-trievedfromhttps://www.nmc.org.uk/globalassets/sitedocuments/nmc-publications/nmc-code.pdfOliver,P.2012.SucceedingwithyourLiteratureReview:AHandbookforStudents.McgrawHillEducation.UK.
Papadatou,D.1997.TRAININGHEALTHPROFESSIONALSINCARINGFORDYINGCHILDRENANDGRIEVINGFAMILIES,DeathStudies,21:6,575-600.Accessedon22March2017.Retrievedfromhttp://www.tandfonline.com/doi/pdf/10.1080/074811897201787
Papadatou,D.,Martinson,I.M.&Chung,P.M.2001.CaringforDyingChildren:AComparativeStudyofNurses’ExperiencesinGreeceandHongKong.CancerNursing,24(5),402-412.
Pardoe,P.2011.Psychologicalsupportfornursesonpaediatricintensivecareunits.NURSINGCHILDRENANDYOUNGPEOPLE,23(8)27-29.Payne,N.2001.Occupationalstressorsandcopingasdeterminantsofburnoutinfe-malehospicenurses.Journalofadvancednursing33(3),396-405.Accessedon22March2017.Retrievedfromhttp://onlinelibrary.wiley.com/doi/10.1046/j.1365-2648.2001.01677.x/epdf
Peters.L.,Cant,R.,Payne,S.,O’Connor,M.,McDermott,F.,Hood,K.,Morphet,J.&Shimoinaba,K.2013.HowDeathAnxietyImpactsNurses’CaringforPatientsattheEndofLife:AReviewofLiterature.TheOpenNursingJournal.Accessedon4April2017.Retrievedfromhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC3565229/Peterson,J.,Johnson,M.,Halvorsen,B.,Apmann,L.,Chang,P-C.,Kershek,S.,Scherr,C.,Ogi,M.&Pincon,D.2010.Wheredonursesgoforhelp?Aqualitativestudyofcopingwithdeathanddying.InternationalJournalofPalliativeNursing,16(9).
Price,B.2014.Avoidingplagiarism:guidancefornursingstudents.NursingStandard28(26),45-51.
38
Rashotte,J.Bourbonnais,F.&Chamberlain,M.1997.Pediatricintensivecarenursesandtheirgriefexperiences:Aphenomenologicalstudy.Mosbyyearbookinc.
Resnik,D.B.2011.WhatisethicsinResearch&whyisitimportant?NationalInstituteofenvironmentalhealthsciences.Accessedon17April2017.Retrievedfromhttp://www.niehs.nih.gov/research/resources/bioethics/whatis/
Reynolds,F.2006.Howdoctorscopewithdeath.ArchivesofDiseaseinChildhood.Accessedon4April2017.Retrievedfromhttps://www.ncbi.nlm.nih.gov/pmc/articles/PMC2082912/
Reid,F.2013.Griefandtheexperiencesofnursesprovidingpalliativecaretochildrenandyoungpeopleathome.NURSINGCHILDRENANDYOUNGPEOPLE,25(9),31-36.
Roberts,P.,Priest,H.&Traynor,M.2006.Reliabilityandvalidityinresearch.NursingStandard,20(44),41-45.
Saks,M.&Allsop,J.2007.ResearchingHealthQualitative,QuantitativeandMixedMethods.30-124.SagePublications.
Shariff,A.,Olson,J.,SantosSalas,A.&Cranley,L.2017.Nurses’experiencesofprovidingcaretobereavedfamilieswhoexperienceunexpecteddeathinintensivecareunits:Anarrativeoverview.TheCanadianJournalofCriticalCareNursing,28(1).
Shinbara,C.2009.GriefSupportforNurses:AnAssessmentofNeeds.Proquest.17-19.
Stayer,D.&Lockhart,J.S.2016.LivingwithDyinginthePediatricIntensiveCareUnit:ANursingPerspective.AMERICANJOURNALOFCRITICALCARE,25(4),350-356.
Storvik-Sydänmaa,S.,Talvensaari,H.,Kaisvuo,T.&Uotila,N.2012.Lapsenjanuorenhoitotyö.SanomaProOyHelsinki.
Tapanainen,P.&Rajantie,J.2016.Kuolleisuus.Lastentaudit.Duodecim/Oppiportti.KustannusOyDuodecim2016.
Tuomi,J.&Sarajärvi,A.2009.Laadullinentutkimusjasisällönanalyysi.Helsinki.KustannusosakeyhtiöTammi.
WahMak,Y.,Chiang,V.C.L.&Chui,W.T.2013.Experiencesandperceptionsofnursescaringfordyingpatientsandfamiliesintheacutemedicaladmissionsetting.InternationalJournalofPalliativeNursing,19(9).
39
Wilson,J.&Kirshbaum,M.2011Effectsofpatientdeathonnursingstaff:aliteraturereview.PubmedGov.Accessedon4April2017.Retrievedfromhttps://www.ncbi.nlm.nih.gov/pubmed/21647017
WHO/EHA.1999.CopingMechanisms.EMERGENCYHEALTHTRAININGPROGRAMMEFORAFRICA.WorldHealthOrganization/EmergencyHumanitarianAction.Accessedon14February2017.Retrievedfromhttp://apps.who.int/disasters/repo/5517.pdf
WHO/Europe.n.d.Childandadolescenthealth.WorldHealthOrganization,RegionalofficeforEurope.Accessedon29January2017.Retrievedfromhttp://www.euro.who.int/en/health-topics/Life-stages/child-and-adolescent-health/child-and-adolescent-health
WHO.n.d.Thetop10causesofdeath:Majorcausesofdeath.Mediacentre.WorldHealthOrganization.Accessedon27January2017.Retrievedfromhttp://www.who.int/mediacentre/factsheets/fs310/en/index2.html
WHO.2016.Children:reducingmortality.Factsheet.WorldHealthOrganization.Ac-cessedon30January2017.Retrievedfromhttp://www.who.int/mediacentre/factsheets/fs178/en/
WHO.2017.Under-fivemortality.WorldHealthOrganization.Accessedon30Janu-ary2017.Retrievedfromhttp://www.who.int/gho/child_health/mortality/mortality_under_five_text/en/
Williams,M.&Vogt,P.2011.ThehandbookofInnovationsinSocialResearchMeth-ods.Sagepublications.
YK.1989.YK:nyleissopimuslastenoikeuksista.Unicef.Accessedon28January2017.Retrievedfromhttps://unicef.studio.crasman.fi/pub/public/pdf/LOS_A5fi.pdf
Ångström-Brännström,C.,Dahlqvist,V.,Strandberg,G.&Norberg,A.2014.Descrip-tionsofcomfortinthesocialnetworkssurroundingadyingchild.VårdINorden,34,4-8.
40
Appendices
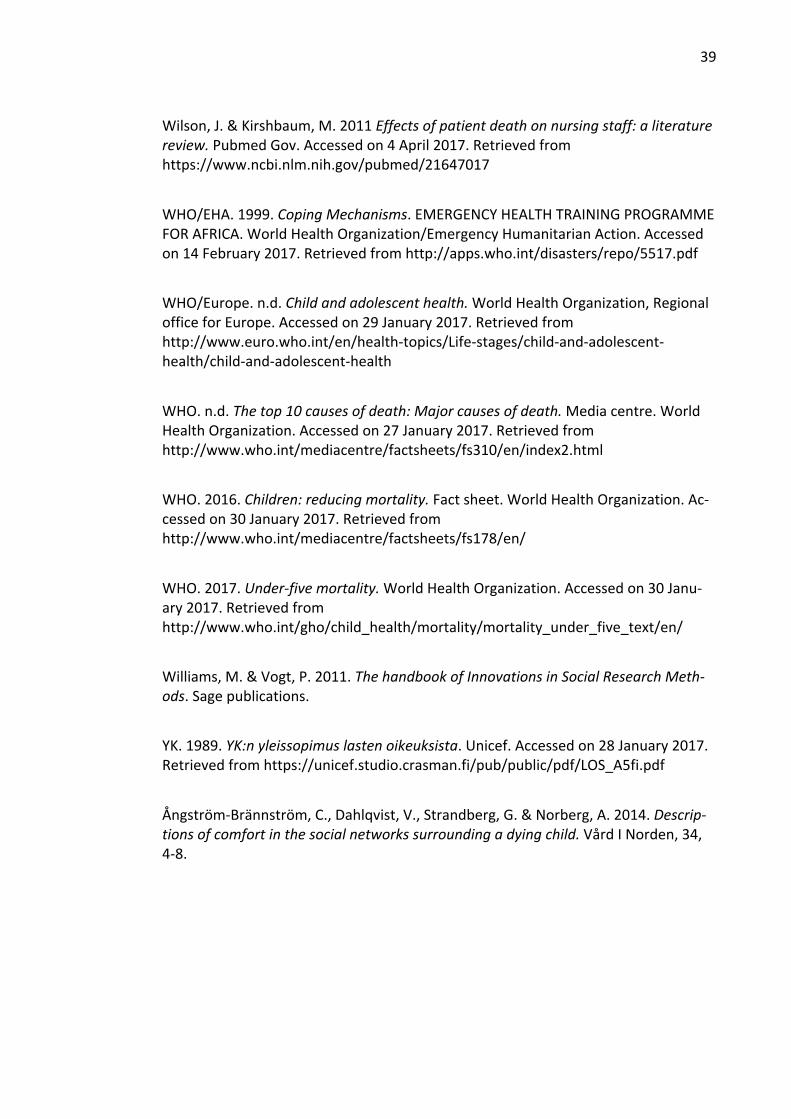
Appendix1.Thereviewedarticlesinalphabeticalorder
Author(s) Publishing
yearand
country
Title Researchmethod Mainfindings
Cholette,M.,Gephart,S.M.
2012USA
AModelfortheDynamicsofBereavementCaregiving
Qualitativere-search:casestudy
Importanceofacknowledgementoflosses,strongsupportiveteams,asafevenuetoexpressandsharefeelings,andset-tingtimeasideforself-careandin-trapersonalre-flection.
Cook,K.A.,Mott,S.,Lawrence,P.,Jablonski,J.,Grady,M.R.,Norton,D.,Liner,K.B.,Cioffi,J.,Hickey,P.,Reidy,S.&Connor,J.A.
2012USA
CopingWhileCaringfortheDyingChild:Nurses’Experi-encesinanAcuteCareSetting
Qualitativere-search:focusgroups
Nurses’specificneedswhilecar-ingfordyingpa-tientsandim-portanceofsup-portivecolleaguesandotheravaila-bleresources.
Forster,E.&Hafiz,A.
2015Australia
Paediatricdeathanddy-ing:exploringcopingstrate-giesofhealthprofessionalsandperceptionsofsupportpro-vision
Qualitativere-search:socialcon-structionism
Nursescopebyusingpeersup-port,personalcopingstrategies,familysupport,andspiritualbe-liefs.
Keenan,P.&Dermott,K.M.ORisitPaterson,J.G.
2016Ireland
HowNursesGrieveForChil-drenWhoDieInTheirCare
Qualitativere-search:descriptivestudy
Nursesvaryinthewaytheyexperi-enceandmanagetheirgrief.
41
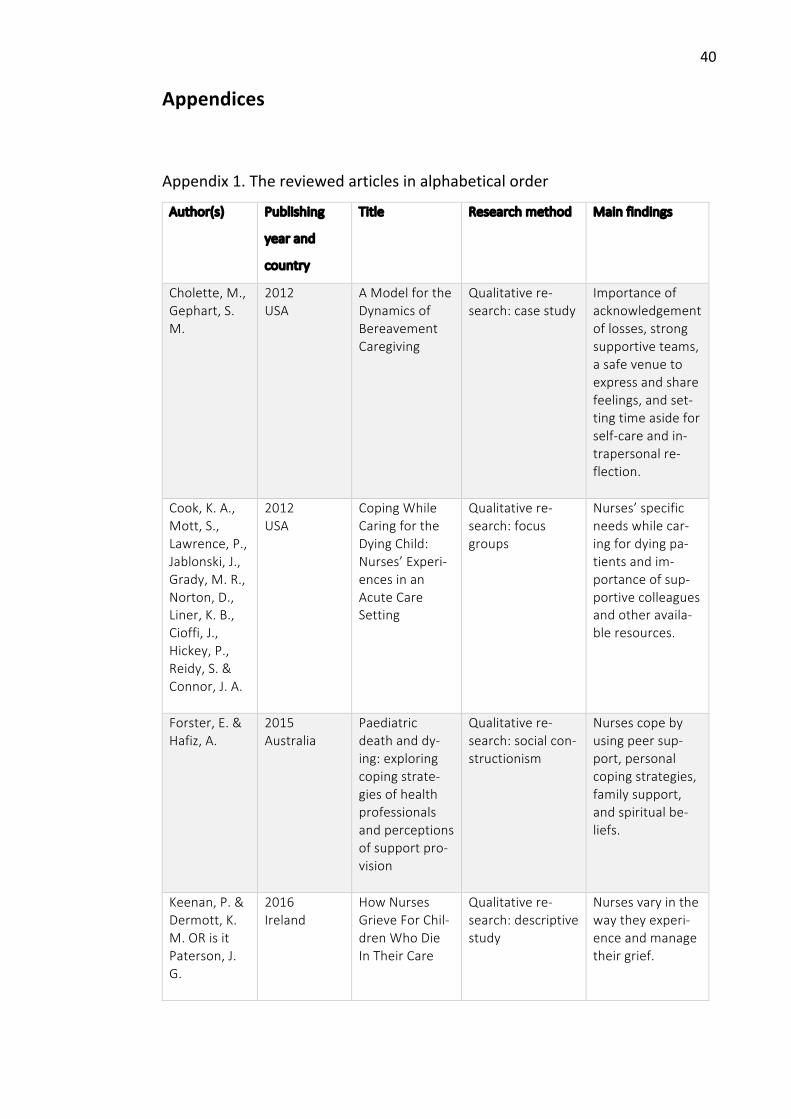
Keene,E.A.,Hutton,N.,Hall,B.&Rushton,C.
2010USA
BereavementDebriefingSes-sions:AnInter-ventiontoSup-portHealthCareProfes-sionalsinMan-agingTheirGriefAftertheDeathofaPa-tient
Qualitativere-search:ethno-graphic
Opportunitiesforexpressionofgriefandreflectionallowsnursestocontinuetopro-videcareeffec-tively.
Kellogg,M.B.,Barker,M.&McCune,N.
2014USA
TheLivedExpe-rienceofPedi-atricBurnNursesFollow-ingPatientDeath
Qualitativere-search:phenome-nologicaldesign
Nursesdevelopindividualcopingmechanismsandseekpeersupportwhendealingwithalossofapatient.
Maloney,C. 2012USA
CriticalIncidentStressDebrief-ingandPediat-ricNurses:AnApproachtoSupporttheWorkEnviron-mentandMiti-gateNegativeConsequences
Qualitativere-search:casestudy
Debriefingisamodelofcopingtosupportstaffhealingfollowingacriticalincident.
Pardoe,P. 2011UK
Psychologicalsupportfornursesonpae-diatricintensivecareunits
Qualitativere-search:casestudy
Nursesshouldbeentitledtoseeknumerouspsy-chologicalsupportwhendealingwithgrief,andit’sim-portantthatnurs-esacknowledgetheirfeelings.
Reid,F. 2013Scotland
Griefandtheexperiencesofnursesprovid-ingpalliativecaretochildrenandyoungpeo-pleathome
Qualitativere-search
Nursesrequireconsiderableskillsandreflectiontomanagetheirowncopingstrategies,inordertocon-tinuecaringforotherpatients.
Stayer,D.&LockhartJ.S.
2016USA
LivingwithDy-inginthePedi-atricIntensiveCareUnit:A
Qualitativere-search:herme-neuticphenome-nologicalstudy
Nursesfindpro-fessionalsatisfac-tioninprovidingpalliativecare,
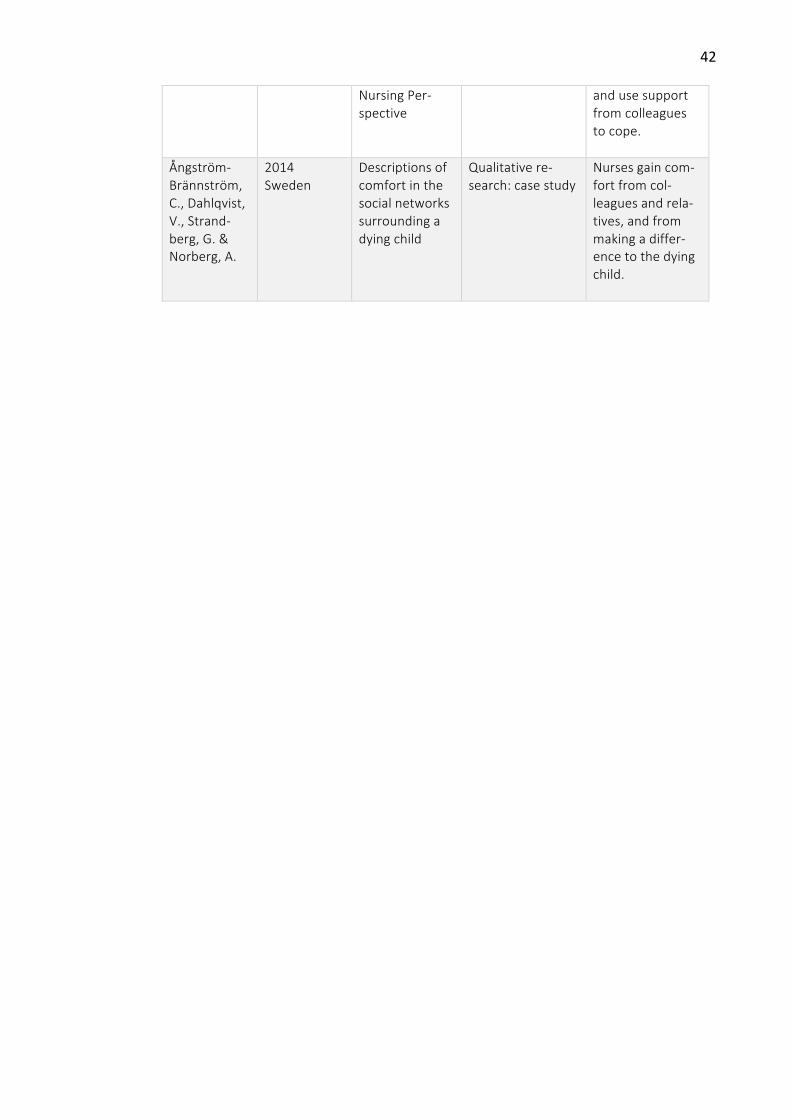
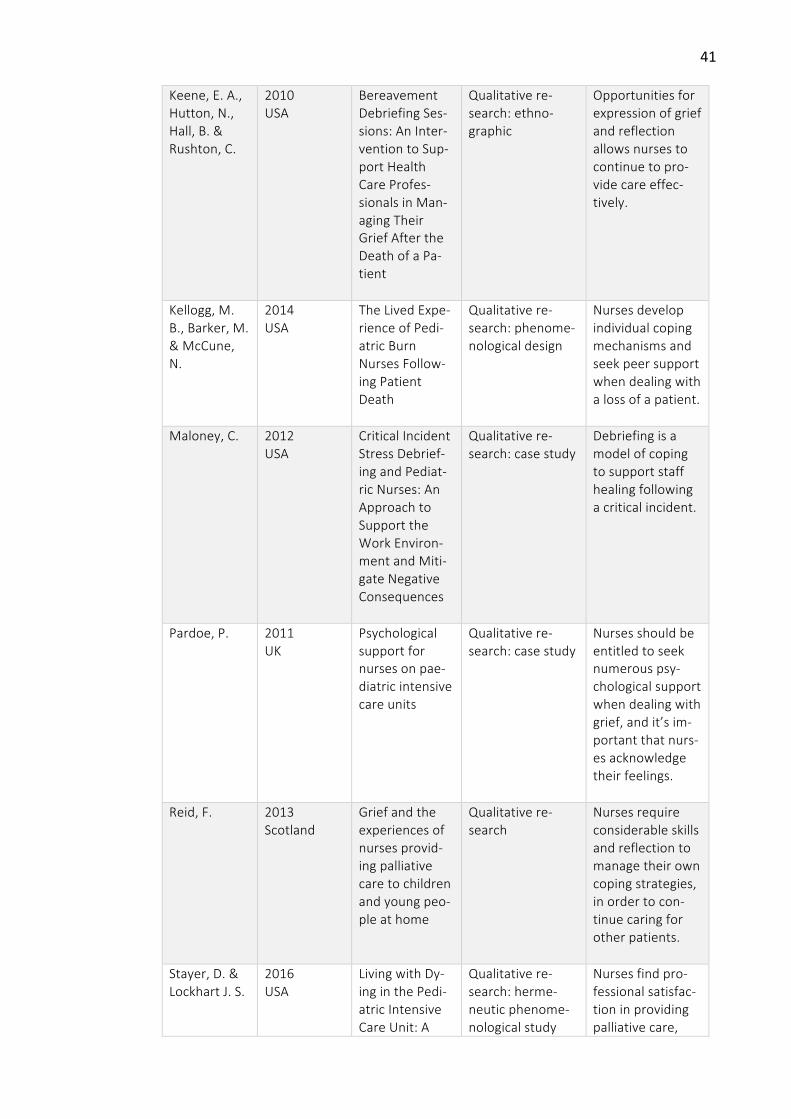
42
NursingPer-spective
andusesupportfromcolleaguestocope.
Ångström-Brännström,C.,Dahlqvist,V.,Strand-berg,G.&Norberg,A.
2014Sweden
Descriptionsofcomfortinthesocialnetworkssurroundingadyingchild
Qualitativere-search:casestudy
Nursesgaincom-fortfromcol-leaguesandrela-tives,andfrommakingadiffer-encetothedyingchild.