Embed Size (px)
Citation preview
Copyright © 2014. F.A. Davis Company
CHAPTER 12CHAPTER 12
SEROUS FLUIDSEROUS FLUID

Copyright © 2014. F.A. Davis Company
Upon completing this chapter, the reader will be able to
1.Describe the normal formation of serous fluid.2.Describe four primary causes of serous effusions.3.Differentiate between a transudate and an exudate, including etiology, appearance, and laboratory tests.4.Differentiate between a hemothorax and a hemorrhagic exudate.5.Differentiate between a chylous and a pseudochylous exudate.
Learning ObjectivesLearning Objectives

Copyright © 2014. F.A. Davis Company
6. State the significance of increased neutrophils, lymphocytes, eosinophils, and plasma cells in pleural fluid.
7. Describe the morphologic characteristics of mesothelial cells and malignant cells.
8. List three common chemistry tests performed on pleural fluid, and state their significance.
9. State the common etiologies of pericardial effusions.10. Discuss the diagnostic significance of peritoneal lavage.
Learning Objectives Learning Objectives (cont’d)(cont’d)

Copyright © 2014. F.A. Davis Company
11. Calculate a serum-ascites gradient, and state its significance.
12. Differentiate between ascitic effusions of hepatic and peritoneal origin.
13. State the clinical significance of the carcinoembryonic antigen and CA 125 tests.
14. List four chemical tests performed on ascitic fluid, and state their significance.
Learning Objectives Learning Objectives (cont’d)(cont’d)

Copyright © 2014. F.A. Davis Company
• Line the closed body cavities– Pleural– Pericardial– Peritoneal
• Two membranes– Parietal: lines cavity wall– Visceral: lines organs in cavity
• Fluid between membranes– Serous fluid: named for each location
Serous MembranesSerous Membranes

Copyright © 2014. F.A. Davis Company
• Purpose: provide lubrication between the two membranes• Ultrafiltrate of plasma• Produced by hydrostatic and oncotic (protein) pressure in
the capillaries lining the membranes• Normally, oncotic pressure is the same on both sides of
the membrane; hydrostatic pressure causes the production
• Small amounts of excess fluid are absorbed by lymphatic capillaries
FormationFormation

Copyright © 2014. F.A. Davis Company
Formation and Absorption Formation and Absorption of Serous Fluidof Serous Fluid

Copyright © 2014. F.A. Davis Company
• Disruption causes fluid buildup; termed effusion– Causes: hydrostatic pressure increased from
congestive heart failure; oncotic pressure decreased from hypoproteinemia; increased capillary permeability from inflammation, infection, malignancy; lymphatic obstruction from tumors
FormationFormation
Copyright © 2014. F.A. Davis Company
• Disruption of the mechanisms of serous fluid formation and reabsorption
• Increased capillary hydrostatic pressure– Congestive heart failure, salt and fluid retention
• Decreased oncotic pressure– Nephrotic syndrome, hepatic cirrhosis– Malnutrition, protein-losing enteropathy
• Increased capillary permeability– Microbial infections, membrane inflammations– Malignancy
• Lymphatic obstruction– Malignant tumors, lymphomas, infection and inflammation, thoracic duct
injury
Pathological Causes of Effusions Pathological Causes of Effusions

Copyright © 2014. F.A. Davis Company
• Collected by needle aspiration– Thoracentesis: pleural cavity– Pericardiocentesis: heart cavity– Paracentesis: peritoneal cavity
• Abundant fluid collected >100 mL• EDTA tube: hematology• Sterile heparinized or polyanethol sulfonate (SPS):
microbiology, cytology• Clotted or heparin: chemistry, serology
Specimen Collection Specimen Collection and Handlingand Handling

Copyright © 2014. F.A. Davis Company
• Specimens for pH must be kept on ice• Concentrate fluid for microbiology and cytology
by centrifuging 100 mL• Chemical tests compared with blood tests drawn
at the same time
Specimen Collection Specimen Collection and Handling (cont'd)and Handling (cont'd)

Copyright © 2014. F.A. Davis Company
• Primary classification of serous fluids• Transudates: systemic disorder disrupts filtration
and reabsorption, congestive heart failure, nephrotic syndrome
• Exudates: conditions affecting membranes, inflammation, infection, malignancy
• Differentiation important for further testing• Transudates = little further testing
Transudates and ExudatesTransudates and Exudates

Copyright © 2014. F.A. Davis Company
Transudate Exudate
Appearance Clear Cloudy
Fluid:serum protein ratio <0.5 >0.5
Fluid:serum LD ratio <0.6 >0.6
White blood cell count <1000/µL >1000/µL
Spontaneous clotting No Possible
Pleural fluid cholesterol <45 to 60 mg/dL >45 to 60 mg/dL
Pleural fluid:serum cholesterol ratio <0.3 >0.3
Pleural fluid:bilirubin ratio <0.6 >0.6
Serum-ascites albumin gradient >1.1 <1.1
Laboratory Differentiation of Laboratory Differentiation of Transudates and Exudates Transudates and Exudates

Copyright © 2014. F.A. Davis Company
• Appearance• Transudate versus exudate tests first
– Transudates: seldom tested further– Exudates: microbiology, cytology, and tests for
general symptoms– Differentials performed routinely on cytocentrifuged
specimens • White blood cells (WBCs), normal tissue cells, malignant
cells
General Laboratory TestsGeneral Laboratory Tests

Copyright © 2014. F.A. Davis Company
• Additional transudate versus exudate tests– Pleural fluid cholesterol <60 mg/dL versus >60 mg/dL– Fluid-serum cholesterol ratio <0.3 versus >0.3– Fluid-serum bilirubin ratio <0.6 versus >0.6
• Appearance– Normal: clear, pale yellow– Turbid: WBCs, inflammation, infection– Milky: chylous material from thoracic duct leakage,
pseudochylous material from chronic inflammations
Pleural FluidPleural Fluid

Copyright © 2014. F.A. Davis Company
• Bloody: hemothorax (trauma), hemorrhagic effusion (membrane) damage
• Differentiate: do a hematocrit on fluid– >50% blood HCT is hemothorax: more blood– Membrane damage: low blood
• Differentiate chylous and pseudochylous– Chylous is triglycerides; stain with Sudan III– Pseudochylous is cholesterol; polarize and crystals also
seen in wet bright-field view
Pleural Fluid Pleural Fluid (cont’d)(cont’d)

Copyright © 2014. F.A. Davis Company
Appearance Disease
Clear, pale yellow Normal
Turbid, white Microbial infection (tuberculosis)
Bloody Hemothorax, hemorrhagic effusion, pulmonary emboli, tuberculosis, malignancy
Milky Chylous material from thoracic duct leakage Pseudochylous material from chronic inflammation
Brown Rupture of amoebic liver abscess
Black Aspergillus
Viscous Malignant mesothelioma (increased hyaluronic acid)
Correlation of Pleural Fluid Correlation of Pleural Fluid Appearance and Disease Appearance and Disease

Copyright © 2014. F.A. Davis Company
• Differential: primary cells are neutrophils, lymphocytes, macrophages, eosinophils, mesothelial cells, plasma cells, and malignant cells• Macrophages (scavengers) often the highest
• ↑ Neutrophils: bacterial infection, pancreatitis, pulmonary infarction
• ↑ Lymphs: TB, viral infections, autoimmune disorders, malignancy
• Eosinophils: trauma introducing air and blood, allergic reactions, parasites
Hematology TestsHematology Tests

Copyright © 2014. F.A. Davis Company
Hematology Tests Hematology Tests (cont’d)(cont’d)
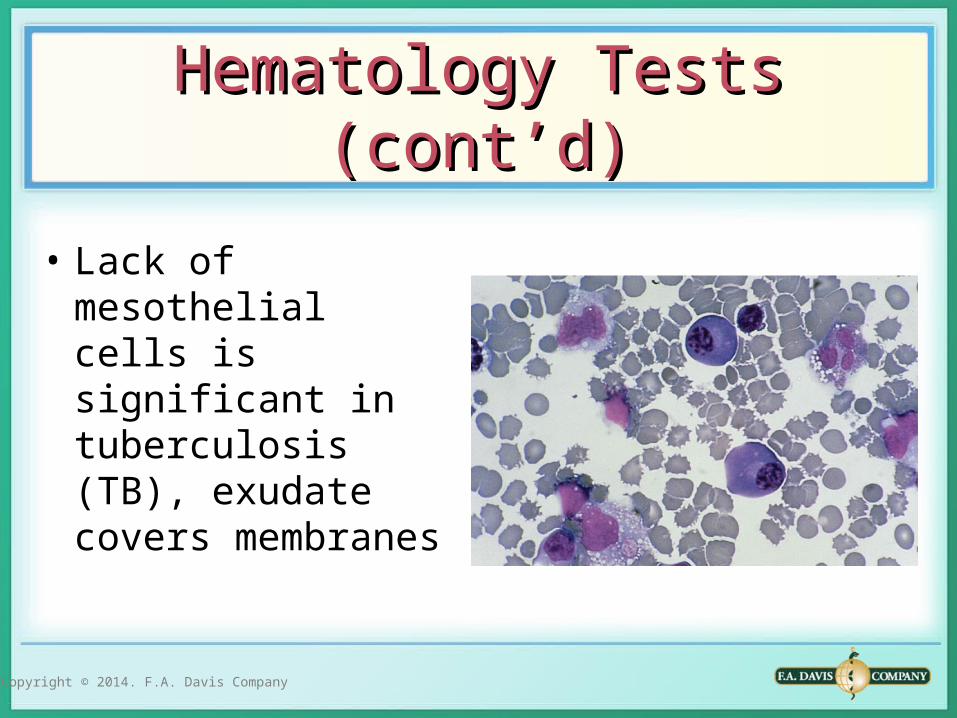
• Mesothelial cells: single cell layer lines membranes, common to see in serous fluid, pleomorphic, dark blue cytoplasm, round nuclei, normal and reactive; “fried egg appearance”
• Reactive cells may be multinucleated
Copyright © 2014. F.A. Davis Company
Hematology Tests Hematology Tests (cont’d)(cont’d)
• Lack of mesothelial cells is significant in tuberculosis (TB), exudate covers membranes

Copyright © 2014. F.A. Davis Company
Hematology Tests Hematology Tests (cont’d)(cont’d)
• Pleural fluid: primary cancer cells
• Adenocarcinoma cells are large and irregular; small cell or oat cell carcinoma cells are small like lymph cells, mesothelioma cells are large

Copyright © 2014. F.A. Davis Company
Hematology Tests Hematology Tests (cont’d)(cont’d)
• Metastatic breast carcinoma cells seen in clumps
• Small cell carcinoma
Copyright © 2014. F.A. Davis Company
• Glucose: decreased in inflammations and infections, have blood comparison
• pH: <7.0 indicates need for chest tubes, <6.0 indicates esophageal rupture (gastric fluid)
• Adenosine deaminase elevated in TB and malignancy
• Amylase: elevated in esophageal rupture and malignancy
Chemistry TestsChemistry Tests

Copyright © 2014. F.A. Davis Company
Test Significance
Glucose Decreased in rheumatoid inflammation
Decreased in purulent infection
Lactate Elevated in bacterial infection
Triglyceride Elevated in chylous effusions
pH Decreased in pneumonia not responding to antibiotics
Markedly decreased with esophageal rupture
ADA Elevated in tuberculosis and malignancy
Amylase Elevated in pancreatitis, esophageal rupture, and malignancy
Significance of Chemical Testing Significance of Chemical Testing of Pleural Fluidof Pleural Fluid

Copyright © 2014. F.A. Davis Company
• Gram stains and aerobic and anaerobic cultures on fluid, TB smears, and cultures
• Serology tests for autoimmune disorders• Tumor markers for metastatic malignancy
– Carcinoembryonic antigen: gastrointestinal malignancy
– CA125: uterine and ovarian malignancy
Microbiology and Serology TestsMicrobiology and Serology Tests

Copyright © 2014. F.A. Davis Company
Pleural Fluid Testing AlgorithmPleural Fluid Testing Algorithm

Copyright © 2014. F.A. Davis Company
• Normally small amount: 10 to 50 mL• Permeability of membranes from infection
(pericarditis, endocarditis), malignancy, trauma produces exudates
• Transudates: hypothyroidism, uremia, immune disorders
• Detect by cardiac tamponade (compression) heard by physician
Pericardial FluidPericardial Fluid

Copyright © 2014. F.A. Davis Company
• Appearance: normal clear, pale yellow• Turbid: infection, malignancy (also blood
streaked)• Bloody: accidental puncture, anticoagulants• Milky: chylous and pseudochylous material• Fluid-serum protein and LD ratios for transudate
versus exudate differentiation• WBCs >1000/μL is bacterial endocarditis
Pericardial Fluid Pericardial Fluid (cont’d)(cont’d)

Copyright © 2014. F.A. Davis Company
• Malignant cells are metastatic from lung and breast
• Gram stains and cultures for endocarditis often caused by previous respiratory infections
• TB smears and cultures done in AIDS
Pericardial Fluid Pericardial Fluid (cont’d)(cont’d)

Copyright © 2014. F.A. Davis Company
Pericardial Fluid Pericardial Fluid (cont’d)(cont’d)
• Metastatic giant mesothelioma cell also seen in pleural fluid as a primary malignancy in persons with asbestos contact

Copyright © 2014. F.A. Davis Company
Test Significance
Appearance
Clear, pale yellow Normal, transudate
Blood streaked Infection, malignancy
Grossly bloody Cardiac puncture, anticoagulants
Milky Chylous and pseudochylous material
Differential
Increased neutrophils Bacterial endocarditis
Malignant cells Metastatic carcinoma
Carcinoembryonic antigen Metastatic carcinoma
Gram stain and culture Bacterial endocarditis
Acid-fast stain Tubercular effusion
Adenosine deaminase Tubercular effusion
Significance of Pericardial Significance of Pericardial Fluid Testing Fluid Testing

Copyright © 2014. F.A. Davis Company
• Effusion between the peritoneal membranes is called ascites
• Fluid is often called ascitic fluid• Transudates: hepatic origin (cirrhosis)• Exudates: bacterial peritonitis from intestinal
perforation, ruptured appendix, and malignancy
Peritoneal FluidPeritoneal Fluid

Copyright © 2014. F.A. Davis Company
• Performed to detect early abdominal bleeding and need for surgery
• Blunt trauma injuries• Normal saline injected into cavity, withdrawn,
and red blood cell (RBC) count performed• RBC count >100,000 indicates blunt trauma case• Radiographic procedures also available
Peritoneal LavagePeritoneal Lavage

Copyright © 2014. F.A. Davis Company
• More difficult than pleural and pericardial fluids• Serum-ascites gradient is best differentiation• Serum and fluid albumin levels are measured;
fluid level is subtracted from serum level; difference (gradient) > than 1.1 is a transudate (hepatic origin)
• Serum albumin 3.8 – fluid albumin 1.2 = 2.6 = hepatic transudate
Transudates and ExudatesTransudates and Exudates

Copyright © 2014. F.A. Davis Company
• Normal: clear, pale yellow• Turbid: bacterial and fungal infections• Green-brown color = bile• Milky: chylous and pseudochylous with trauma and
lymphatic blockage• WBC count: normal 350 cells/μL• Absolute neutrophil count: >50% of total WBC count or
greater than 250 cells indicates infection• Lymphocytes elevated in TB
AppearanceAppearance

Copyright © 2014. F.A. Davis Company
Cellular Examination Cellular Examination
• Cells: WBCs, mesothelial cells, macrophages (lipophages)
• Yeast cells and Toxoplasma gondii
• Malignant cells, often contain mucin vacuoles

Copyright © 2014. F.A. Davis Company
Cellular Examination Cellular Examination (cont’d)(cont’d)
• Malignant cells of prostate, gastrointestinal, and ovarian origin
Copyright © 2014. F.A. Davis Company
Cellular Examination Cellular Examination (cont’d)(cont’d)
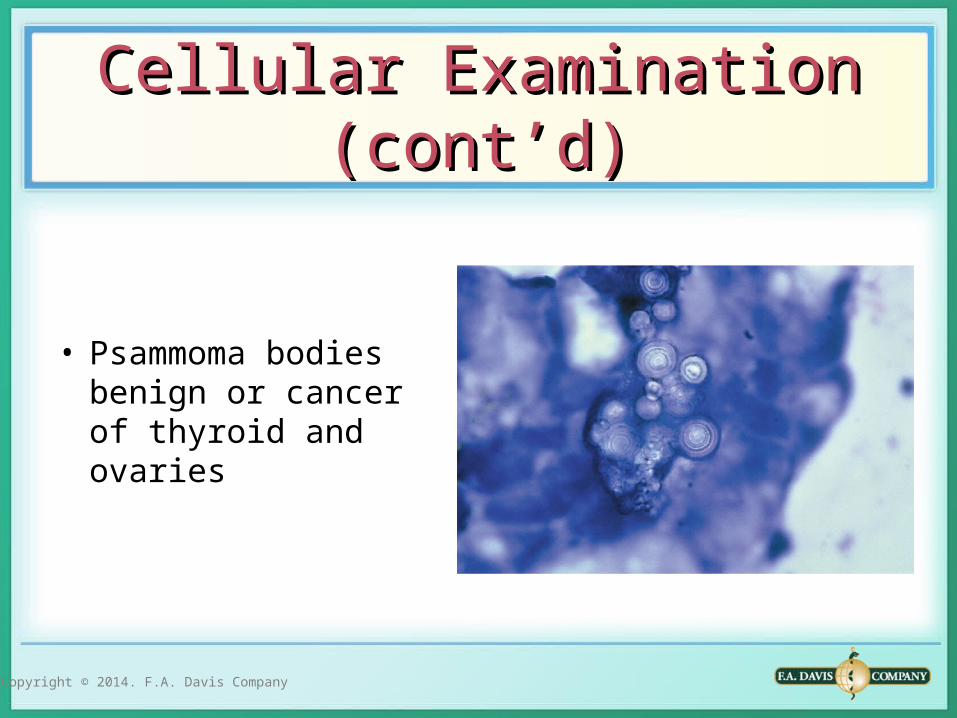
• Psammoma bodies benign or cancer of thyroid and ovaries
Copyright © 2014. F.A. Davis Company
• Glucose: below plasma levels = peritonitis and malignancy
• ↑ Amylase: pancreatitis, gastrointestinal perforation
• ↑ Alkaline phosphatase: intestinal perforation• ↑ BUN, creatinine: ruptured bladder, accidental
perforation
Chemical TestsChemical Tests

Copyright © 2014. F.A. Davis Company
• Gram stains and aerobic and anaerobic cultures• Anaerobic cultures: inoculate blood culture
bottle at bedside• Acid-fast smear, adenosine deaminase and
culture for TB
Microbiology TestsMicrobiology Tests

Copyright © 2014. F.A. Davis Company
• Tumor markers – CEA – CA 125
• Presence of CA 125 antigen with a negative CEA suggests the source is from the ovaries, fallopian tubes, or endometrium
• Presence of CEA antigen suggests source is gastrointestinal
Serological TestsSerological Tests