Embed Size (px)
Citation preview

The Journal of Applied Research • Vol. 5, No. 3, 2005 423
Core Strengthening and Balance inthe Geriatric PopulationJerrold S. Petrofsky, PhD*Maria Cuneo, DPT*Russell Dial, DPT*Ashley K. Pawley* Jennifer Hill, BS†
*Department of Physical Therapy, Loma Linda University, Loma Linda, California †Department of Physical Therapy, Azusa Pacific University, Azusa, California
program, showing a correspondingincrease associated with the increasedreach of these subjects. Not only werereach and the critical angle at which thesubject exceeded his or her limit of sta-bility increased, but tremor was reducedsignificantly for these subjects aftertraining.
The results show that even if olderindividuals are engaged in a basic fit-ness program, training is very beneficialto increasing their independence andfunctional activities of daily living.
INTRODUCTIONAging is associated with a loss in musclestrength. This, in itself, would be a limit-ing factor in daily activities, but aging isalso associated with loss of peripheralmotor and sensory nerves,1-3 loss of bothvision and control of the eye throughthe vestibular and visual cortex,4
increased blood pressure during exer-cise,5 and an increase in isometricendurance.6 Peripheral blood flow atrest and during exercise is decreased asis the hyperemia following exercise.7
These disabilities, secondary to the nor-mal aging process, can lead to loss ofbalance and poor gait in the older pop-ulation.8,9
Many types of programs have beendeveloped to increase muscle strengthand balance.8,9 Lifting weights slowly at
KEY WO R D S : e x e r c i s e, e x e r t i o n ,g e r i a t r i c, core strengthening
ABSTRACTAging usually reduces muscle capacityin the core muscles of the body causinga reduction in functional abilities andactivities of daily living. In the presentinvestigation, we evaluated the effect ofan exercise regimen on strength trainingin the core muscles, balance, and reach.Thirteen subjects underwent 20 minutesof exercise per day, 3 days a week, for aperiod of 1 month using a 6 Second Absmachine (Savvier, LP, Carlsbad, CA),eliciting exercise on the rectus abdomin-is, transversus abdominis, and backextensor muscles.
Balance and functional reach wereassessed before and after the exerciseprogram. Before exercise, the averagemaximum reach in the subjects was 15.4± 5.2, 16.9 ± 5.7, and 15.7 ± 4.8 cm forreach in the forward, right, and leftdirections, respectively. After training,reach increased to 22.4 ± 5.9, 20.6 ± 4.0,and 22.5 ± 5.3 cm in the respective direc-tions. Associated with that movement,during maximum reach in the forward,right, and left directions, the reach angleof the body changed from 1.91o ± 2.76o,2.31o ± 0.9o, and 0.9o ± 3.1o before train-ing to 5.33o ± 1.83o, 4.72o ± 1.83o, and2.42o ± 1.1o after the 1-month training
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 423
Vol. 5, No. 3, 2005 • The Journal of Applied Research424
loads set to fatigue the muscle in shortperiods of time, called anaerobic exer-cise,10 can cause muscle enzymes tofavor glycolysis, and DNA is transcribedto build actin and myosin in muscle.10-14
This allows the muscle to build strengthand increase its ability to work withoutoxygen.15 In contrast, light repetitivework (aerobic exercise), which requireshigh blood flow for energy and oxygendelivery, causes the muscle to transcribegenomes on DNA to increase the con-centration of enzymes in the Krebs cycleand for beta oxidation of fats to bettermake use of the muscle’s ability to burnfats.12,16 Aerobic training also elicits anincrease in angiogenesis in capillariesand an increase in mitochondrial surfacearea and density to allow better oxygenand fuel delivery to tissue for aerobicexercise.17 Aerobic exercise training alsoincreases function in the cardiopul-monary system, which lowers triglyc-erides, inflammatory cytokines,C-reactive protein, and increases collat-eral circulation in the heart.18
However, for the older population,while good cardiopulmonary condition-ing is a goal, the most immediate con-cern is simply accomplishing activities ofdaily living (ADL). ADLs are frequentlyimpaired due to weakness in core mus-cles such as the rectus abdominis, trans-versus abdominis, and the internal andexternal oblique muscles.19 This resultsin an inability to reach objects awayfrom the body.
Studies show that strengtheningcore muscles does aid in functional abili-ties.20,21 Using large exercise machines tostrengthen the abdominal and lowerback muscles can allow someone in awheelchair to have more effective boweland bladder programs, to sit straighter inthe chair, get less scoliosis, and to havebetter reach without losing his or herbalance.22 This increase in functionalitytranslates into better performance inADLs. This in turn leads to great psy-
chological gains by allowing a person tobe more independent.
However, with ever-rising costs inrehabilitation and even health spas, itbecomes important to develop exercisetechniques and devices to allow individ-uals who are disabled to exercise athome.23 One such device is the 6 SecondAbs machine (Savvier, LP, Carlsbad,CA). This machine provides a progres-sive increase in resistance with a built-intimer so that individuals can exercisetheir abdominal muscles and lower backmuscles from the sitting position.24,25
These devices are marketed at mostsports stores in the United States and,for those who are not disabled, haveoffered a unique way to build abdominalmuscle strength that is more effectivethan conventional sit ups.24,25 The pur-pose of this investigation was to see ifthe device would help older peopleachieve better balance. Because thedevice allows people to exercise in theseated position, it allows safer exercisethan lying on the floor or standing in apopulation with limited mobility.
SUBJECTSThirteen subjects participated in thisstudy; the average age of the subjects asshown in Table 1 was 73.1 ± 7.3 years.The average height was 65.6 ± 3.8 cm,and the average weight was 68.2 ± 12.7kg. Twelve of the subjects were womenand one was a man. The oldest subject inthe group was 82, and the youngest was61. All subjects in the studies wereengaged in a fitness program thatincluded the 6 Second Abs machineworkout at the La Fetra Senior Centerin Glendora, California, 2 days a weekand did 1 additional day of exercise withthe machine independently.
All protocols and procedures wereapproved by the committee on humanexperimentation at Azusa PacificUniversity, and all subjects signed astatement of informed consent.
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 424
The Journal of Applied Research • Vol. 5, No. 3, 2005 425
METHODS6 Second Abs MachineThe 6 Second Abs machine is a commer-cial exercise device that consists of arectangular plastic frame with rubberbands on the inside to adjust resistance.Resistance can be increased in a numberof different stages so that it becomesincreasingly difficult to compress therectangle.
As the machine is compressed to thefirst, second, and third clicks positionwith 3 different resistance bands, there isa linear increase in load. The upper partof the rectangle is placed under the sub-ject’s arms (under the triceps musclesbilaterally) or held in the subject’s arms
against the chest while the base of therectangle is placed on of the middle ofthe quadriceps muscles. Both the upperand lower rectangles are padded.
Measurement of Muscle StrengthMuscle strength was measured in theabdominal and back muscles. The sub-jects were in the seated position withtheir backs at 90o in reference to thehips. A strap was placed around the sub-ject’s chest just below the axilla and con-nected to a strain gauge force sensor.Strength was then assessed for flexionand extension as the highest of 3 maxi-mal efforts in each muscle group; 1minute separated the contractions. Acomplete description is given else-where.24,25
Assessing Balance during FunctionalDaily ActivitiesBalance was assessed by a balance plat-form similar to the Smart BalanceMaster (NeuroCom Internation, Inc.,Clackamas, OR). However, a similardevice was built from two sheets of ply-wood and a ramp. The 1-inch plywoodplates (Figure 1) were separated by fourmetal bars connected to strain gauges.Each bar was positioned at 90o with ref-erence to the other bar. As such, straingauges were placed at 0o, 90o, 180o, and270o. With the subject standing in thecenter of the platform, leaning in anydirection was then transduced throughstrain gauges mounted on the metal barsto an electrical output, so that the devia-tion and center of gravity could beassessed. The output of the strain gaugeswas connected to four strain gaugeamplifiers (Biopac Inc., Santa Barbara,CA) and digitized with a 12-bit A/Dconverter (Biopac Inc.). The digitized
Table 1. General Characteristics of Subjects
Age (years) Height (cm) Weight (kg)Mean ± SD 73.1 ± 7.3 65.6 ± 3.8 68.2 ± 12.7
Figure 1. A typical patient standing quietlyon the center of the balance platform.
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 425
Vol. 5, No. 3, 2005 • The Journal of Applied Research426
data were sorted on a computer for lateranalysis.
ProceduresSubjects exercised 3 days a week for aperiod of 4 weeks. On any exercise day,10 minutes of passive stretching wasaccomplished before the test exercise tominimize any chance of soft-tissueinjury. Four different exercises werethen accomplished to exercise the rectusabdominis muscles; subjects placed the 6Second Abs machine equally across themid thigh of both legs and flexed theabdominals by leaning forward, usingthe rectus abdominis muscles. Theweight was set such that with repetitivecontraction of the muscles over 6-secondcycles of contraction, the musclefatigued in 5 minutes. If, on any one day,5 minutes of exercise was accomplished
in any one exercise position, the work-load was increased by 5 pounds suchthat on the next day they fatigued withinthe 5-minute period. In this manner,having accomplished exercise over aperiod of 30 days, the workload was pro-gressively increased
In addition to this 5-minute bout ofexercise, with the subject in the sittingposition facing forward, two other boutsof exercise were accomplished with thesubject facing 45o to the left and 45o tothe right. In these cases, the machinewas placed on one knee, such that theexternal oblique muscles were exercised.Once again, the workload was progres-sively increased over the 1-month peri-od. For the final 5 minutes of exerciseeach day, subjects, again seated, placedthe 6 Second Abs machine against theirupper back and leaned backward andpushed against a wall from their seats toexercise their lower back muscles.
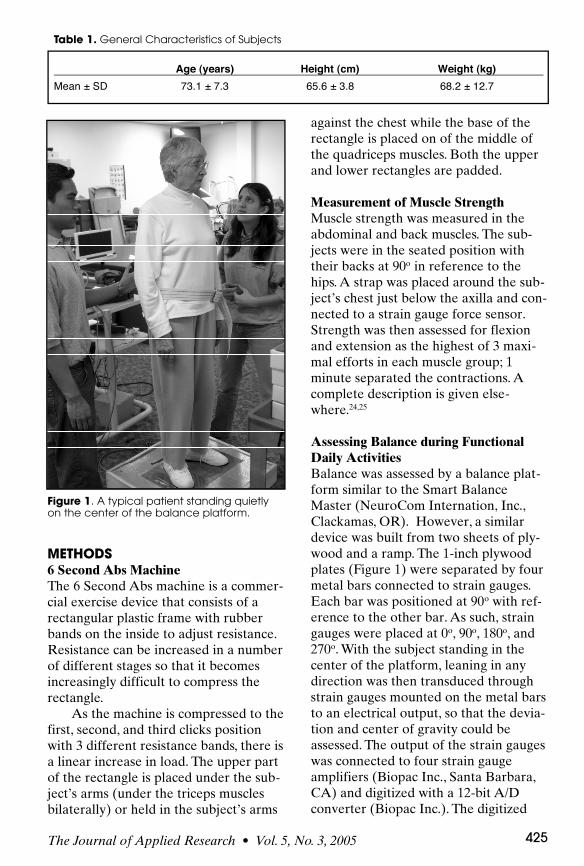
At the start and end of the month,strength was measured in the rectusabdominis and lower back muscles asdescribed in the Methods section. Onboth occasions, balance was assessed.Subjects stood in the middle of the bal-ance platform and reached at eye levelto the furthest extent of their reach inthe forward, left, and right directions(Figure 2). A gait belt was worn, and aphysical therapist guarded the patientsso they could not fall. A completedescription of the technique is givenelsewhere.26
Figure 2. A typical subject reaching to theright but not to the fully extended positionwhile standing on the balance platform. Agait belt was used for safety but was nottouched by the investigators during reach.
Table 2. Average Strength of Subjects
Average Strength (kg)Flexion Extension
pre 31.8 34.2post 43.2 45.6difference 11.4 11.4t-Test 0.001 0.001
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 426
The Journal of Applied Research • Vol. 5, No. 3, 2005 427
RESULTSPrior to exercise, the strength of the
subjects, as shown in Table 2, for exten-sion was 34.2 ± 10.2 kg while duringflexion the average strength of the
group was 31.8 ± 11.1 kg. After the 1-month training period, strengthincreased to 45.6 ± 16.9 kg for extensionand 43.2 ± 14.6 kg for flexion. Thisincrease in strength for both abdominal
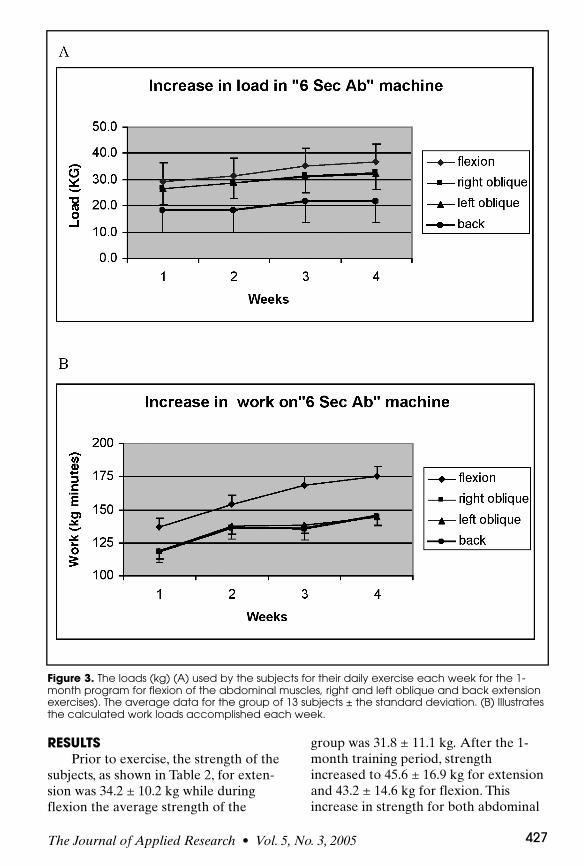
Figure 3. The loads (kg) (A) used by the subjects for their daily exercise each week for the 1-month program for flexion of the abdominal muscles, right and left oblique and back extensionexercises). The average data for the group of 13 subjects ± the standard deviation. (B) Illustratesthe calculated work loads accomplished each week.
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 427
Vol. 5, No. 3, 2005 • The Journal of Applied Research428
flexors and extensors was 11.4 kg andwas significant (P<0.01). The increase instrength was not surprising since, asshown in Figure 3A, there was progres-sive increase in the work and the loadthe subjects could tolerate on theabdominal machine for 5 minutes ofexercise throughout the 1-month period.The average compliance for the exercisewas 93% ± 19% for the group over 1month. As shown in Figure 3B, theincrease in work was 28.3% ± 7.2%,23.3% ± 6.8%, 21.2% ± 5.9%, and21.9% ± 5.8% for flexion, right oblique,left oblique, and back extension exercis-es, respectively. Whereas the maximumreach for the subjects averaged 15.38 ±5.23, 16.92 ± 5.74, and 15.73 ± 4.87 cmfor the forward, right, and left directionsbefore the 1-month exercise programand, after the program, the respectivereach was 22.4 ± 5.4, 20.7 ± 4.0, and 22.5± 5.3 cm. The increase in reach associat-ed with the training averaged over 7 cmand was significant (P<0.01). Thisincrease in reach is expressed as a per-cent of initial reach.
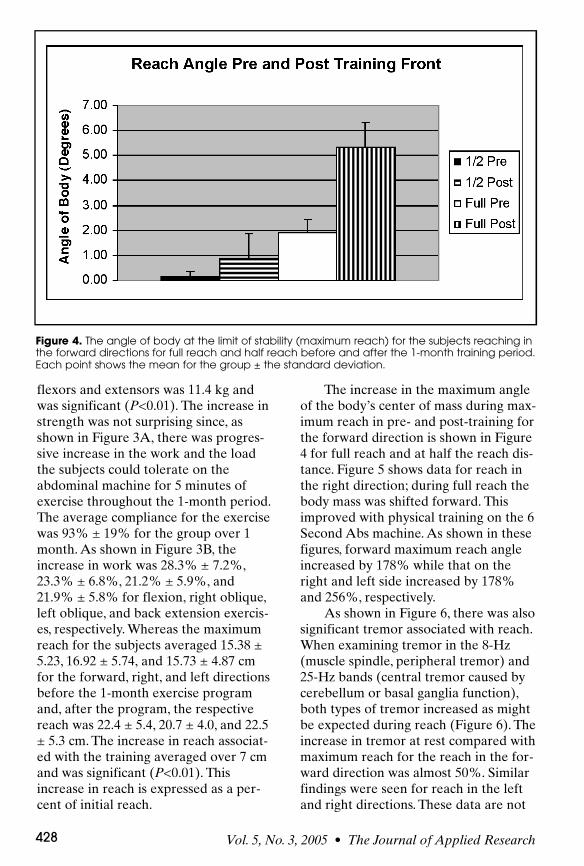
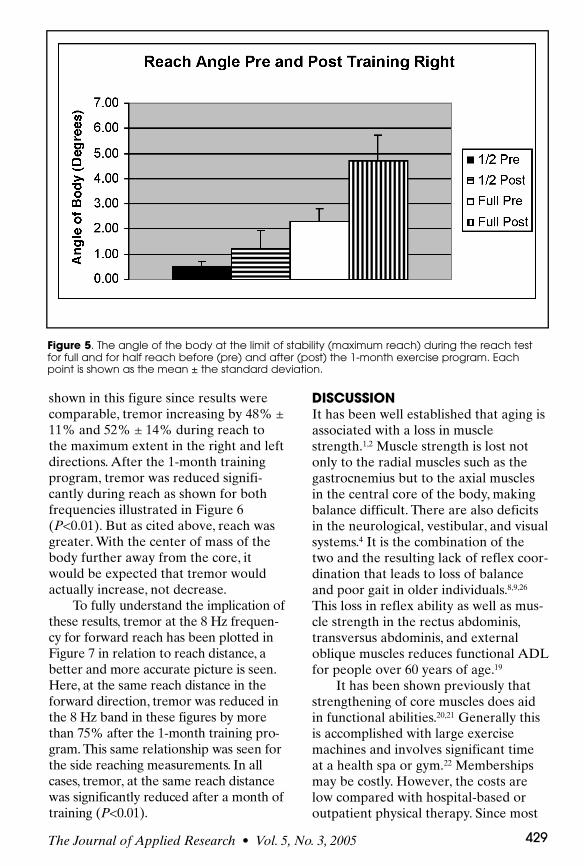
The increase in the maximum angleof the body’s center of mass during max-imum reach in pre- and post-training forthe forward direction is shown in Figure4 for full reach and at half the reach dis-tance. Figure 5 shows data for reach inthe right direction; during full reach thebody mass was shifted forward. Thisimproved with physical training on the 6Second Abs machine. As shown in thesefigures, forward maximum reach angleincreased by 178% while that on theright and left side increased by 178%and 256%, respectively.
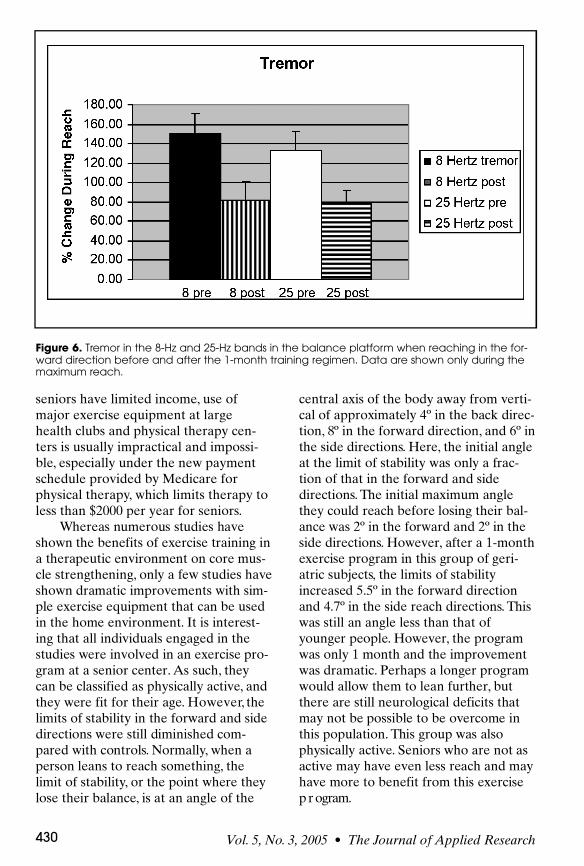
As shown in Figure 6, there was alsosignificant tremor associated with reach.When examining tremor in the 8-Hz(muscle spindle, peripheral tremor) and25-Hz bands (central tremor caused bycerebellum or basal ganglia function),both types of tremor increased as mightbe expected during reach (Figure 6). Theincrease in tremor at rest compared withmaximum reach for the reach in the for-ward direction was almost 50%. Similarfindings were seen for reach in the leftand right directions. These data are not
Figure 4. The angle of body at the limit of stability (maximum reach) for the subjects reaching inthe forward directions for full reach and half reach before and after the 1-month training period.Each point shows the mean for the group ± the standard deviation.
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 428
shown in this figure since results werecomparable, tremor increasing by 48% ±11% and 52% ± 14% during reach tothe maximum extent in the right and leftdirections. After the 1-month trainingprogram, tremor was reduced signifi-cantly during reach as shown for bothfrequencies illustrated in Figure 6(P<0.01). But as cited above, reach wasgreater. With the center of mass of thebody further away from the core, itwould be expected that tremor wouldactually increase, not decrease.
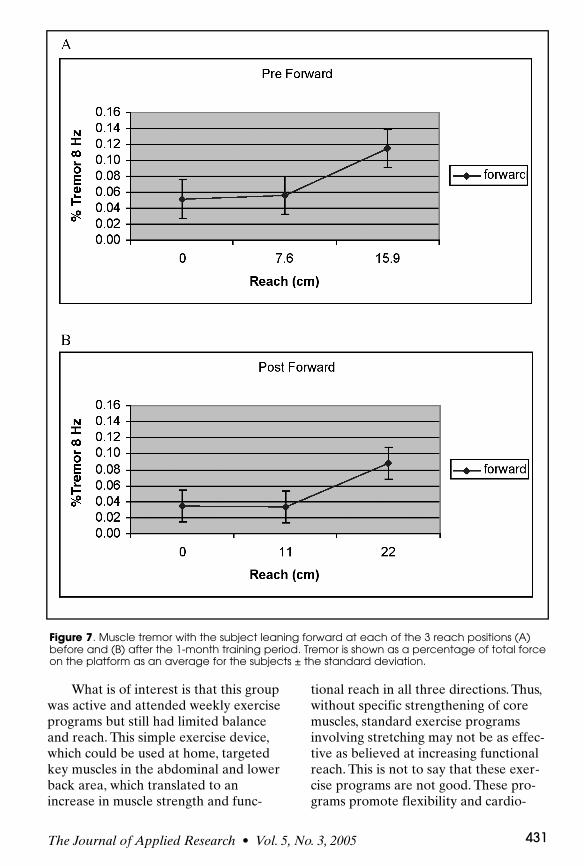
To fully understand the implication ofthese results, tremor at the 8 Hz frequen-cy for forward reach has been plotted inFigure 7 in relation to reach distance, abetter and more accurate picture is seen.H e r e, at the same reach distance in theforward direction, tremor was reduced inthe 8 Hz band in these figures by morethan 75% after the 1-month training pro-g r a m . This same relationship was seen forthe side reaching measurements. In allc a s e s, t r e m o r, at the same reach distancewas significantly reduced after a month oftraining (P< 0 . 0 1 ) .
DISCUSSIONIt has been well established that aging isassociated with a loss in musclestrength.1,2 Muscle strength is lost notonly to the radial muscles such as thegastrocnemius but to the axial musclesin the central core of the body, makingbalance difficult. There are also deficitsin the neurological, vestibular, and visualsystems.4 It is the combination of thetwo and the resulting lack of reflex coor-dination that leads to loss of balanceand poor gait in older individuals.8,9,26
This loss in reflex ability as well as mus-cle strength in the rectus abdominis,transversus abdominis, and externaloblique muscles reduces functional ADLfor people over 60 years of age.19
It has been shown previously thatstrengthening of core muscles does aidin functional abilities.20,21 Generally thisis accomplished with large exercisemachines and involves significant timeat a health spa or gym.22 Membershipsmay be costly. However, the costs arelow compared with hospital-based oroutpatient physical therapy. Since most
The Journal of Applied Research • Vol. 5, No. 3, 2005 429
Figure 5. The angle of the body at the limit of stability (maximum reach) during the reach testfor full and for half reach before (pre) and after (post) the 1-month exercise program. Eachpoint is shown as the mean ± the standard deviation.
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 429
Vol. 5, No. 3, 2005 • The Journal of Applied Research430
seniors have limited income, use ofmajor exercise equipment at largehealth clubs and physical therapy cen-ters is usually impractical and impossi-ble, especially under the new paymentschedule provided by Medicare forphysical therapy, which limits therapy toless than $2000 per year for seniors.
Whereas numerous studies haveshown the benefits of exercise training ina therapeutic environment on core mus-cle strengthening, only a few studies haveshown dramatic improvements with sim-ple exercise equipment that can be usedin the home environment. It is interest-ing that all individuals engaged in thestudies were involved in an exercise pro-gram at a senior center. As such, t h e ycan be classified as physically active, a n dthey were fit for their age. H o w e v e r, t h elimits of stability in the forward and sidedirections were still diminished com-pared with controls. N o r m a l l y, when aperson leans to reach something, t h elimit of stability, or the point where theylose their balance, is at an angle of the
central axis of the body away from verti-cal of approximately 4º in the back direc-t i o n , 8º in the forward direction, and 6º inthe side directions. H e r e, the initial angleat the limit of stability was only a frac-tion of that in the forward and sided i r e c t i o n s. The initial maximum anglethey could reach before losing their bal-ance was 2º in the forward and 2º in theside directions. H o w e v e r, after a 1-monthexercise program in this group of geri-atric subjects, the limits of stabilityincreased 5.5º in the forward directionand 4.7º in the side reach directions. Th i swas still an angle less than that ofyounger people. H o w e v e r, the programwas only 1 month and the improvementwas dramatic. Perhaps a longer programwould allow them to lean further, b u tthere are still neurological deficits thatmay not be possible to be overcome inthis population. This group was alsophysically active. Seniors who are not asactive may have even less reach and mayhave more to benefit from this exercisep r ogram.
Figure 6. Tremor in the 8-Hz and 25-Hz bands in the balance platform when reaching in the for-ward direction before and after the 1-month training regimen. Data are shown only during themaximum reach.
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 430
The Journal of Applied Research • Vol. 5, No. 3, 2005 431
What is of interest is that this groupwas active and attended weekly exerciseprograms but still had limited balanceand reach. This simple exercise device,which could be used at home, targetedkey muscles in the abdominal and lowerback area, which translated to anincrease in muscle strength and func-
tional reach in all three directions. Thus,without specific strengthening of coremuscles, standard exercise programsinvolving stretching may not be as effec-tive as believed at increasing functionalreach. This is not to say that these exer-cise programs are not good. These pro-grams promote flexibility and cardio-
Figure 7. Muscle tremor with the subject leaning forward at each of the 3 reach positions (A)before and (B) after the 1-month training period. Tremor is shown as a percentage of total forceon the platform as an average for the subjects ± the standard deviation.
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 431
Vol. 5, No. 3, 2005 • The Journal of Applied Research432
vascular fitness, which are critical for thegeriatric population, but for maintainingfunctional ADL, an exercise device suchas the one described here would be agreat adjunct to therapy. Furthermore,the reduction in tremor after trainingand the greater reach should translateinto less falls, a leading killer of the geri-atric population.8
Tremor is associated with droppingobjects and frustration with simple taskssuch as reaching in a cabinet to get a canof food. The sharp reduction in tremorafter core training is logical. If the coremuscles are stronger, then it is easier tosteady the limbs during a reach. Betterreach with less tremor could make lifeless frustrating and can lead to increasedquality of life in this population. Thereduction in both tremor bands showsthat motor control is improved at thecentral and peripheral level with corestrengthening, probably leading to fewerfalls.
REFERENCES1. Resnick HE, Vinik AI, Schwartz AV, et al.
Independent effects of peripheral nerve dys-function on lower-extremity physical functionin old age: the Women’s Health and AgingStudy. Diabetes Care. 2000;23:1642-1647.
2. Resnick HE, Stansberry KB, Harris TB, et al.Diabetes, peripheral neuropathy, and old agedisability. Muscle Nerve. 2002;25:43-50.
3. Hof PR, Morrison JH. The aging brain: mor-phomolecular senescence of cortical circuits.Trends Neurosci. 2004;27:607-613.
4. West CG, Gildengorin G, Haegerstrom-Portnoy G, et al. Is vision function related tophysical functional ability in older adults? JAm Geriatr Soc. 2002;50:136-145.
5. Petrofsky JS, Lind AR. Aging, isometricstrength and endurance and the cardiovascu-lar responses to static effort. J Appl Physiol.1975;38:91-95.
6. Petrofsky JS, Laymon M. The effect of agingin spinal cord injured individuals on theblood pressure and heart rate responses dur-ing fatiguing isometric exercise. Eur J ApplPhysiol. 2002;86:479-486.
7. Petrofsky JS, Besonis C, Rivera D, et al. Heattolerance in patients with diabetes. J ApplRes. 2003;3:28-34.
8. Stevens JA, Olson S. Reducing falls andresulting hip fractures among older women.MMWR Recomm Rep. 2000;49(BR-2):3-12.
9. Jensen J, Nyberg L, Rosendahl E, et al.Effects of a fall prevention program includingexercise on mobility and falls in frail olderpeople living in residential care facilities.Aging Clin Exp Res. 2004;16:283-292.
10. Astrand PO, Rodhal K. Physiology of WorkCapacity and Fatigue. New York, NY:McGraw Hill; 1970.
11. Nuhr M, Crevenna R, Gohlsch B, et al.Functional and biochemical properties ofchronically stimulated human skeletal muscle.Eur J Appl Physiol. 2003;89:202-208.
12. Radda GK, Gadian DG, Ross BD. Energymetabolism and cellular pH in normal andpathological conditions. A new look through31phosphorus nuclear magnetic resonance.Ciba Found Symp. 1982;87:36-57.
13. Taunton JE, Maron H, Wilkinson JG.Anaerobic performance in middle and longdistance runners. Can J Appl Sport Sci.1981;6:109-113.
14. Rusko H, Rahkila P, Karvinen E. Anaerobicthreshold, skeletal muscle enzymes and fibercomposition in young female cross-countryskiers. Acta Physiol Scand. 1980;108:263-268.
15. Carrithers JA, Tesch PA, Trieschmann J, et al.Skeletal muscle protein composition follow-ing 5 weeks of ULLS and resistance exercisecountermeasures. J Gravit Physiol. 2002;9:P155-P156.
16. Langfort J, Viese M, Ploug T, Dela F. Timecourse of GLUT4 and AMPK protein expres-sion in human skeletal muscle during onemonth of physical training. Scand J Med SciSports. 2003;13:169-174.
17. Scheinowitz M, Kessler-Icekson G, FreimannS, et al. Short- and long-term swimming exer-cise training increases myocardial insulin-likegrowth factor-I gene expression. GrowthHorm IGF Res. 2003;13:19-25.
18. Nicklas BJ, Ambrosius W, Messier SP, et al.Diet-induced weight loss, exercise, and chron-ic inflammation in older, obese adults: a ran-domized controlled clinical trial. Am J ClinNutr. 2004;79:544-551.
19. Fujiwara T, Hara Y, Chino N. Expiratoryfunction in complete tetraplegics: study ofspirometry, maximal expiratory pressure, andmuscle activity of pectoralis major and latis-simus dorsi muscles. Am J Phys Med Rehabil.1999;78:464-469.
20. Seelen HA, Potten YJ, Drukker J, et al.Development of new muscle synergies in pos-tural control in spinal cord injured subjects. JElectromyogr Kinesiol. 1998;8:23-34.
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 432
The Journal of Applied Research • Vol. 5, No. 3, 2005 433
21. Chen CL, Yeung KT, Bih LI, et al. The rela-tionship between sitting stability and func-tional performance in patients withparaplegia. Arch Phys Med Rehabil.2003;84:1276-1281.
22. Ryerson S. Hemiplegia resulting from vascu-lar insult. In Umphred D, ed. NeurologicalRehabilitation. St. Louis, MO: Mosby Inc.;1995;619-658.
23. Ostelo RW, Goossens ME, de Vet HC, vanden Brandt PA. Economic evaluation of abehavioral-graded activity program comparedto physical therapy for patients followinglumbar disc surgery. Spine. 2004;29:615-622.
24. Petrofsky JS, Morris A, Bonacci J, et al.Aerobic training on a portable abdominalmachine. J Appl Res. 2003;3:402-415.
25. Petrofsky JS, Morris A, Bonacci J, et al.Comparison between an abdominal curl withtimes curls on a portable abdominal machine.J Appl Res. 2003;3:394-401.
26. Petrofsky JS, Lee S, Cuneo M. Effects ofaging and type 2 diabetes on resting and postocclusive hyperemia of the forearm; impactof rosiglitazone. BMC Endocr Disord.2005;5:4-16.
13Petrofsky-vol5no3 2/5/70 10:06 AM Page 433