Embed Size (px)
Citation preview

1/9/14
1
Corneal Manifestations of Systemic Diseases Joseph P. Shovlin, OD, FAAO
Northeastern Eye Institute
Scranton, PA USA
Disclosures
Allergan Pharmacuetical Advisory Panel
Abbott/AMO Global Medical Advisory Panel
-Acanthamoeba Outbreak Panel (ad hoc)
-Consultant
Bausch + Lomb Scientific Advisory Panel
-Global Steering Committee
-Panel On Fusarium Keratitis (ad hoc)
Ciba Vision Post-Market Surveillance Study Group
-Johns Hopkins Adjudication Committee (ad hoc)
Johnson & Johnson Global Professional Advisory Panel
Speaker�s Bureau: Vistakon, Ciba Vision, CooperVision, Bausch + Lomb, AMO, Alcon, Genzyme, and Inspire
Clinical Investigator (FDA): Abbott/AMO, Ciba Vision, Vistakon, Allergan, CooperVision
Topic Outline
I. Classification of Ocular Findings: Metabolic, Immunologic, Infectious
II. Lysosomal Storage Diseases: Recognition and Management
III. Highlighted Cases: Differentials/ Masquerades
IV. Sub-specialty Referrals
V. Summary of Case Reports
Classifications
Metabolic Disorders: systemic metabolic abnormalities lead to an accumulation of an abnormal substance in the cornea
Immunologic/Inflammatory Conditions: systemic immune responses can be found in/on the cornea and surrounding tissues
Infectious Diseases: systemic infections can manifest with corneal signs most often a response to microbial antigens
Metabolic Disorders
Errors in metabolism: storage of protein/
amino acid, carbohydrate, purine/pyrimidine,
and lipid
Often totally asymptomatic
Assorted systemic ramifications are likely
with multiple systems affected.
Early diagnosis is critical for a somewhat
favorable outcome in most cases.

1/9/14
2
Lysosomal Storage Disease
Represents a family of conditions (at least 42)
Enzyme deficiency causes lysosome to become engorged.
Storage in any organ is possible.
Phenotype is determined by location of stored substrate which acts upon an enzyme.
Additional testing should include skeletal survey and MRI of the brain.
Genzyme has four therapies for: Fabry, Pompei, Gaucher and Hunter disease.
Normal Bone Marrow Cell Abnormal Bone Marrow Cell
What are LSDs?
Example: Gaucher
Three are X-linked Fabry, MPS II, Danon Disease Progression
10 months 12 months
22 months 34 months
Photos courtesy of the MPS Society.
Patient with severe MPS I
39 months
Diagnosis of LSD
Leukocyte enzyme analysis
Skin biopsy with electron microscopy
Genetic testing
Newborn screening (approximately 1:5,000 births)
Amniotic enzyme
Hunter and Fabry are X-linked diseases; reflect multiple family members being affected.
NYS requires screening for 6 different LSDs-including Krabbe that responds to bone marrow transplant.
Spingolipidosis
GM gangliosidosis ß-Galactosidase
Krabbe ß-Galactosidase
Tay-Sach Hexosaminidase A
Sandhoff Hexosaminidase B
Gaucher ß-Galactosidase
Fabry â-Galactosidase A
Metachromatic
dystrophy
Arylsulfatase A

1/9/14
3
13
MPS I
Umbilical/inguinal hernia
Cardiovascular disease
Obstructive airway disease
Corneal clouding
Hepatosplenomegaly
Chronic rhinitis/otitis
Joint stiffness
Developmental delay
Hearing loss
Enlarged tongue
Look for unusual symptoms or for clusters of more common symptoms
Carpal tunnel syndrome
Skeletal deformities
Signs & Symptoms
Macrosomia
Neufeld EF, Muenzer J. In: Scriver C,Beaudet A, Sly W, Valle D, eds. The Metabolic and Molecular Bases of Inherited Disease. New York:
McGraw Hill; 2001:3421-3452.
Lysosomal Storage Diseases
Corneal Clouding: GM I Gangliosidosis,
Mucolipidosis II, III, IV, Mucopolysaccharidosis (MPS) I, IV, VI,
VII, Fucosidosis
Corneal Whorling/Opacities: Fabry,
MPS VI, Niemann-Pick, Sialodosis II
Crystal Deposits: Cystinosis
Cherry Red Spot
Tay-Sachs
Sandhoff
Niemann-Pick
Farber
Sialidosis
Galactosialidosis
Gangliosidosis (GM I)
CNS Involvement
Metachromatic Leukodystophy
8%
Sanfilippo A 7%
Hunter Severe 5%
Krabbe 6%
Sandhoff 2% GM 1
Gangliosidosis 2%
Mucolipidosis type II / III 2%
Niemann-Pick A 2%
Niemann-Pick C 4%
Tay-Sachs 4%
Sanfilippo B 4%
Gaucher type 2 & 3 1%
Niemann-Pick B 2%
Maroteaux-Lamy 3%
Cystinosis 4%
Morquio 5%
Pompe 5%
Hurler/Scheie (MPS I) 4%
Gaucher type I 13% Scheie (MPS I)
1%
Hurler (MPS I) 4%
Hunter Mild 1%
Fabry 7%
Significant or severe CNS involvement
(~ 54%)
No or minimal CNS involvement
(~ 46%)
Adapted from Meikle P et al. JAMA. 1999;281:249-254.
Data on file, Genzyme.
Other 2%
a-Mannosidosis
Sanfilippo D
1%
1%
Human Genome Project
Sequence information can be used for:
Mutation analysis
DNA based confirmation of diagnosis
Prenatal diagnosis
Genetic counseling
Population screening
Current Management Options for Some LSDs
Supportive measures
Physical therapy
CPAP
Hearing aids
Surgery
Specific treatments
Organ and stem cell transplantation
Enzyme replacement therapy
Substrate inhibition

1/9/14
4
Key Points to Remember
Some LSDs are treatable.
Early diagnosis is critical.
Unusual signs and symptoms and clusters of common signs and symptoms aid recognition.
Timely referral to a geneticist +/or metabolic specialist
is crucial.
The Diagnostic Odyssey
Recent Fabry and MPS I market research study data (n = 421)1:
Patients may see 6 to 13 physicians before definitive diagnosis
National Organization for Rare Disorders (NORD) market survey (n=138)2:
68% said 3+ months for diagnosis after first visit to a physician
36% remained undiagnosed for 1+ years
1 in 7 remained undiagnosed for 6+ years
1. Data on file, Genzyme.
2. Krammer M. �The Experience of the Rare Disorder Community� NORD survey,
2003.
Immunologic/Inflammatory Conditions
Surrounding structures are often involved.
Patients are generally symptomatic from an
ocular perspective.
Systemic findings may include:
thyroid and/or parathyroid dysfunction
acoustic neuroma or other tumors
lymphoma or other cancers
renal failure
Infectious Diseases
Immune reaction of the eye may signal systemic infection.
Patients present with non-specific signs and symptoms like phlyctenulosis and interstitial keratitis.
Assorted infections are possible and include viruses, bacteria, fungi and protozoa such as: West Nile and Epstein Barr virus, Lyme disease,
tuberculosis, Bartonella.

1/9/14
5
Corneal Crystals
Cystinosis: an autosomal recessive disorder of cystine storage (deposited in several organs; needle shaped.refractile polychromic crystlas and pigmentary
Lymphoproliferative disorders: associated with variable symptoms, bone pain bruising in monoclonal gammopathy (MGUS, Waldenstrom) and multiple myeloma
Infection: de novo or following refractive or transplant surgery
Medication induced: especially topical fluoroquinolone
Corneal dystrophies: Bietti dystrophy, Schnyder dystrophy
Ochronosis: defect in metabolic tyrosine pathway; �oil droplet� opacity in the peripheral cornea
Dieffenbachia: injury from garden plant (milky latex) causes �blue� crystals
Gold shots: dust-like, glittering granules throughout the anterior surface
Cystinosis
Concern especially in younger patients for severe kidney disease (nephrotic
cystinosis)
Treatment: Oral: cysteamine bitartrate
(Procysbi) and Topical: cysteamine
ophthalmic solution 0.44% (Cystaran)
Plasma Cell Dyscrasia/ Multiple Myeloma
Crystalline keratopathy may signal multiple myeloma.
Crystals are non-reflective and produce a thickened central cornea.
Most often associated with osteolytic lesions, hypercalcemia, anemia, renal failure and increased susceptibility to infection.
Diagnosis: Bence Jones proteinuria (M proteins on serum protein electrophoresis) is diagnostic
Treatment: chemotherapy, radiation and surgery

1/9/14
6
Corneal Verticilatta
Represent assorted inclusions within the corneal epithelium: lipid or iodine
Can result from abnormal metabolism pathway disorders or drug toxicity
Differentials include: striate
melanokeratosis, Fabry disease, and drug toxicity from assorted medications
Systemic Medications Associated with Vortex Keratopathy
Amiodarone, Aminoquinolones (chloroquine, hydroxychloroquine, amodiaquine), Chlorpromazine, Clofazimine, Gentamycin (sub-conjunctival), Gold, Ibuprofen, Indomethacin, Mepacrine, Meperidine, Monobenzene (topical skin ointment), Naproxen, Perhexiline maleate, Phenothiazines, Suramin, Tamoxifen, Tilorone hydrochloride
Some cause retinal and optic nerve toxicity and have to be discontinued immediately. (i.e.: ½ life of Amiodarone is weeks. Consult with the cardiologist.)
1/9/14
7
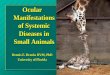
Fabry Disease
Lysosomal storage disorder: deficiency of alpha-galactosidase A or ceramidetrihexosidase
Enzyme cleaves a molecule of galactose from lipid arising from old red blood cells and leads to early myocardial infarction and stroke.
Kidney failure requires dialysis or transplant.
Diagnosis: serum deficiency of alpha-galactosidase A (enzyme assay not as reliable for female carriers), mutation analysis, physical signs
Treatment: infusion enzyme therapy of Fabrazyme (Genzyme) or Replagal (Shire) to prevent renal failure, decreases pain and minimize stroke potential
Fabry Disease
Pathology Inheritance α-galactosidase A (α-GAL) deficiency1
Accumulation of globotriaosylceramide (GL-3)1
X-linked recessive
Onset Incidence May present in childhood or adolescence ~1:40,000 males1
~1:117,000 individuals2
Progression
Often life threatening
Death often due to renal, cardiac, or cerebrovascular complications
Average life expectancy of males ~ 50 years3
Disease-at- a-Glance
1. Desnick RJ et al. In: Scriver C,Beaudet A, Sly W, Valle D, eds. The Metabolic and Molecular Bases of Inherited Disease. 2001;3733-3774.
2. Meikle P et al. JAMA. 1999;281:249-254.
3. MacDermot KD et al. J Med Genet. 2001;38:750-760.
1/9/14
8
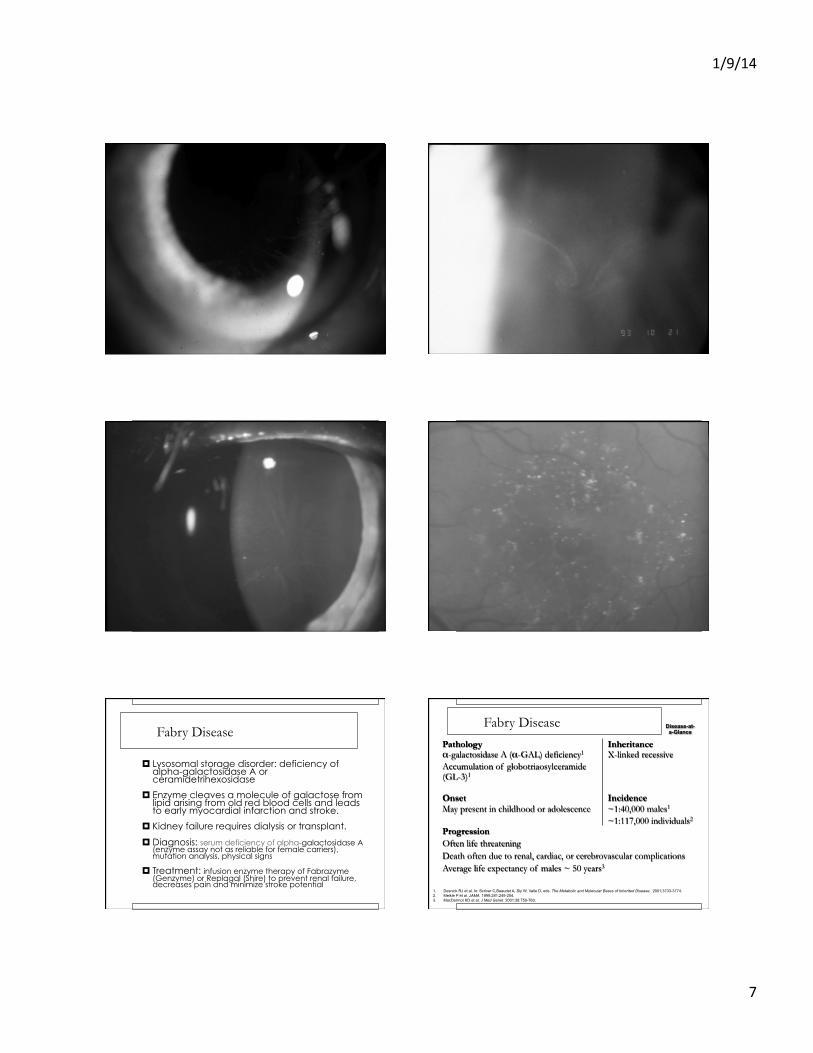
Relative Prevalence
Metachromatic Leukodystophy
8%
Sanfilippo A 7%
Hunter Severe 5%
Krabbe 6%
Sandhoff 2% GM 1
Gangliosidosis 2%
Mucolipidosis type II / III 2%
Niemann-Pick A 2%
Niemann-Pick C 4%
Tay-Sachs 4%
Sanfilippo B 4%
Gaucher type 2 & 3 1%
Niemann-Pick B 2%
Maroteaux-Lamy 3%
Cystinosis 4%
Morquio 5%
Pompe 5%
Hurler/Scheie (MPS I) 4%
Gaucher type I 13% Scheie (MPS I)
1%
Hurler (MPS I) 4%
Hunter Mild 1%
Fabry 7%
Adapted from Meikle P et al. JAMA. 1999;281:249-254.
Other 2%
a-Mannosidosis
Sanfilippo D
1%
1%
1%
Fabry Disease
Left ventricular
hypertrophy
Early ischemic
stroke
Angiokeratomas
Progressive renal
insufficiency Corneal &
lenticular opacities
Hypohidrosis
Acroparesthesia
Psychosocial
manifestations
Recurrent fever
Heat & cold
intolerance
Signs & Symptoms
�Whorllike� or �spokelike�
corneal opacities1
Fabry Disease
Angiokeratomas1 Cardiomyopathy1
Signs & Symptoms
1. Courtesy of R. J. Desnick, PhD, MD

1/9/14
9
Fabry Disease
Supportive care
- Pain management
- Valve replacement
- Dialysis or renal transplantation
Enzyme replacement therapy
Agalsidase beta (Fabrazyme, Genzyme Corp.)
Agalsidase alfa (Replagal, Shire Human Genetic
Therapies)
Treatment Strategies Enzyme Infusion Therapy

1/9/14
10
Corneal Dendriform
Herpes simplex dendrite
Herpes zoster keratopathy
Thygeson superficial keratopathy
Protozoan keratitis
Contact lens induced �pseudo-dendrite�
Tyrosinemia
Superficial hypertrophic dendriform epitheliopathy
Other corneal fascinations: edematous corneal formation, healing abrasion, verticillate, stromal dystrophy.
Both Stains ?? Additional Value Case 14 - painless Herpes Simplex (not a classic dendrite)
Prevention Through Vaccination
Controversies…..
Should healthcare providers be vaccinated?
When is vaccination appropriate after having the shingles?
When should one stop antivirals before/after vaccination?
Should patients with active kerato-uveitis or corneal
dendriform be vaccinated?

1/9/14
11
Antiviral Resistance
Rare event overall, but definitely more common in immuno-compromised individuals. Any resistance does raise the concern for immuno-compromised states (i.e CA).
TK mutants (encodes for key enzyme) are responsible. Some concern for prolonged prophylaxis and emerging resistance as in bacterial disease.
Acyclovir resistance are often resistant to valacyclovir and cross-resistance to famciclovir; 45% of resistant strains are resistant to ganciclovir. ACV efficacy may have reduced therapeutic effect in lactose intolerant patients.
In vitro resistance assays and molecular characterization of isolates should be performed in refractory cases.
1/9/14
12
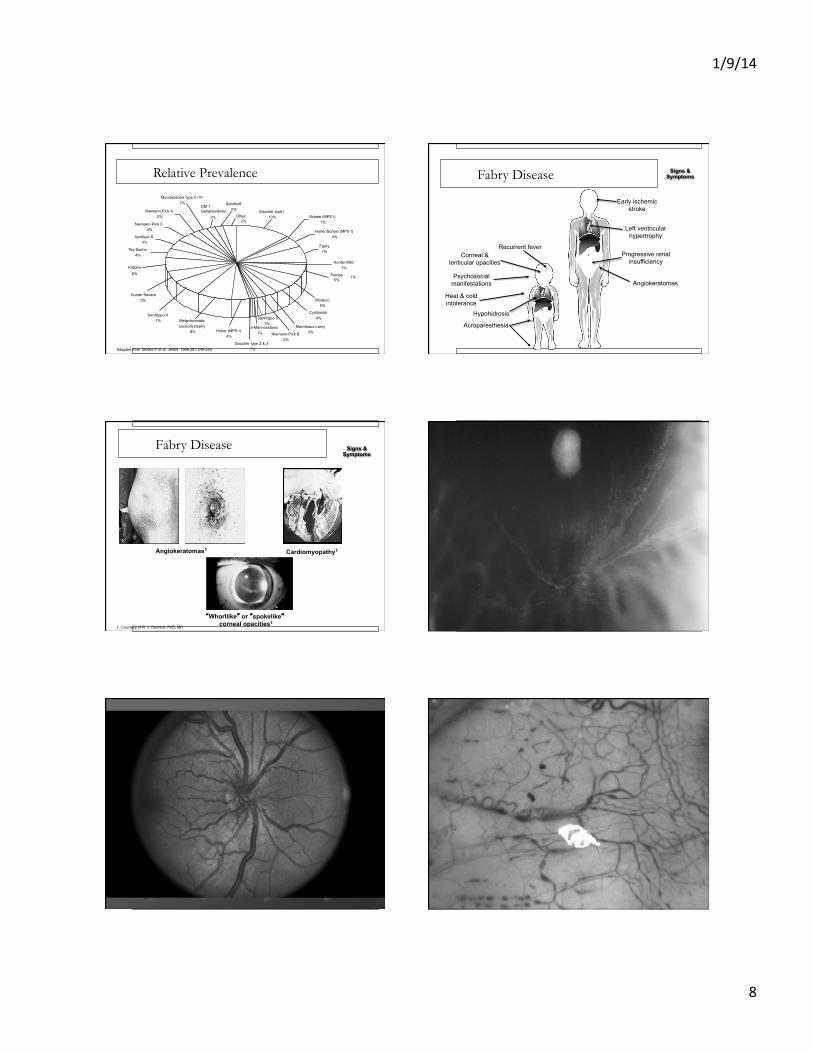
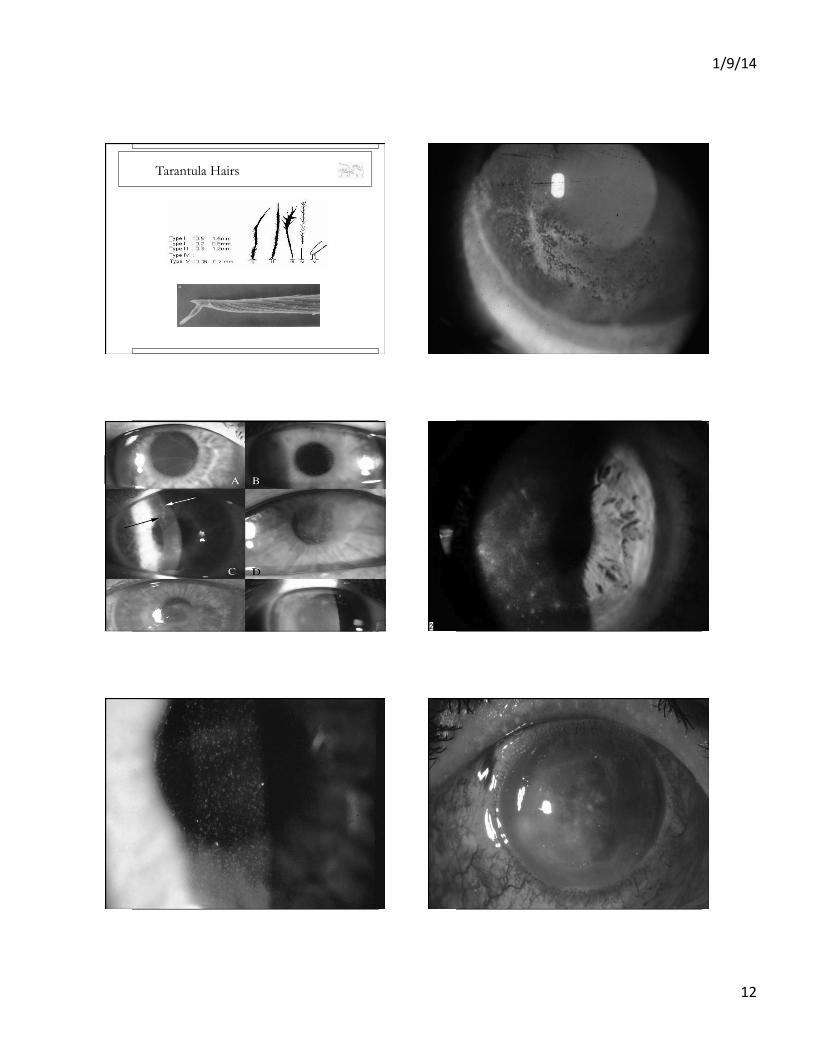
Tarantula Hairs

1/9/14
13
Tyrosinemia (Type II)
Richner-Hanhart syndrome: rare protein and
amino acid metabolic disorder.
Characterized by: corneal dendriform
lesions, painful planar and plantar
hyperkerotosis and retardation.
Treatment: dietary restrictions of tyrosine
and phenyalanine

1/9/14
14
Darrier Disease
Keratosis follicularis: a disorder of keratinization
Skin lesions are brown-yellow and are found on
the face, neck and scalp.
Corneal lesions are characterized by peripheral
opacity and central corneal irregularity in
radiating or cob-web patterns that pool fluorescein.
Indolent Ulcerations of the Cornea
Sterile ulcerations: vitamin A deficiency, vernal shield ulcers, HSV, other corneal irritants
Must be differentiated from an infectious process
Often difficult to manage without surgical intervention that includes flaps, tarsorrhaphy, autologous serum, or amniotic membrane transplant.

1/9/14
15
Crack Keratopathy
Neurotrophic ulcer results from: hypesthesia and reduced tearing (inherent), chemical burn
(alkali), direct toxic irritant to the cornea (smoke), and mechanical rubbing due to eye irritation.
Ulceration is oval with smooth, rolled edge.
Diagnosis by exclusion when suppuration is present and pain is not proportional.
Persistent ulcers may continue even after cessation.
Treatment: tarsorrhaphy, amniotic membrane transplant or Pro-Kera graft, support for chemical dependency
Recurrent Herpes Zoster
Recurrent episodes (different locations) are somewhat atypical and practitioners must consider a
sinister etiology.
Patients should be worked up for occult malignancy
or other reduced cell mediated immunity concerns
(body scans, T4 and T8 subsets may be needed).
HIV/CMV titers are suggested.
4.5X greater risk of stroke the 1st yr.

1/9/14
16
Thymoma
Thymus is a lymphoid organ located in the anterior mediastinum and is responsible for the development and maturation of cell mediated function.
Many thymoma patients experience symptoms of myasthenia gravis and are associated with many other systemic syndromes like Cushing disease and lupus.
May represent thymic cancer
Diagnosis: chest CT scan with contrast, thoracoscopic biopsy
Treatment: chemotherapy (induction), surgical excision, radiotherapy
Theodore Superior Limbic Keratoconjunctivitis
Characterized by superior bulbar conjunctival
redness and laxity, petechial hemorrhage on the
palpebral conjunctiva, and superior corneal
involvement (localized form of Conj.-CH)
Contact lens analog exists which manifests with
desquamation and keratinization of the ocular
surface (fibrovascular variant may be present).
Interesting thyroid dysfunction link (anti-thyroid
antibody panel is suggested)
OCT: Conjunctivochalasis

1/9/14
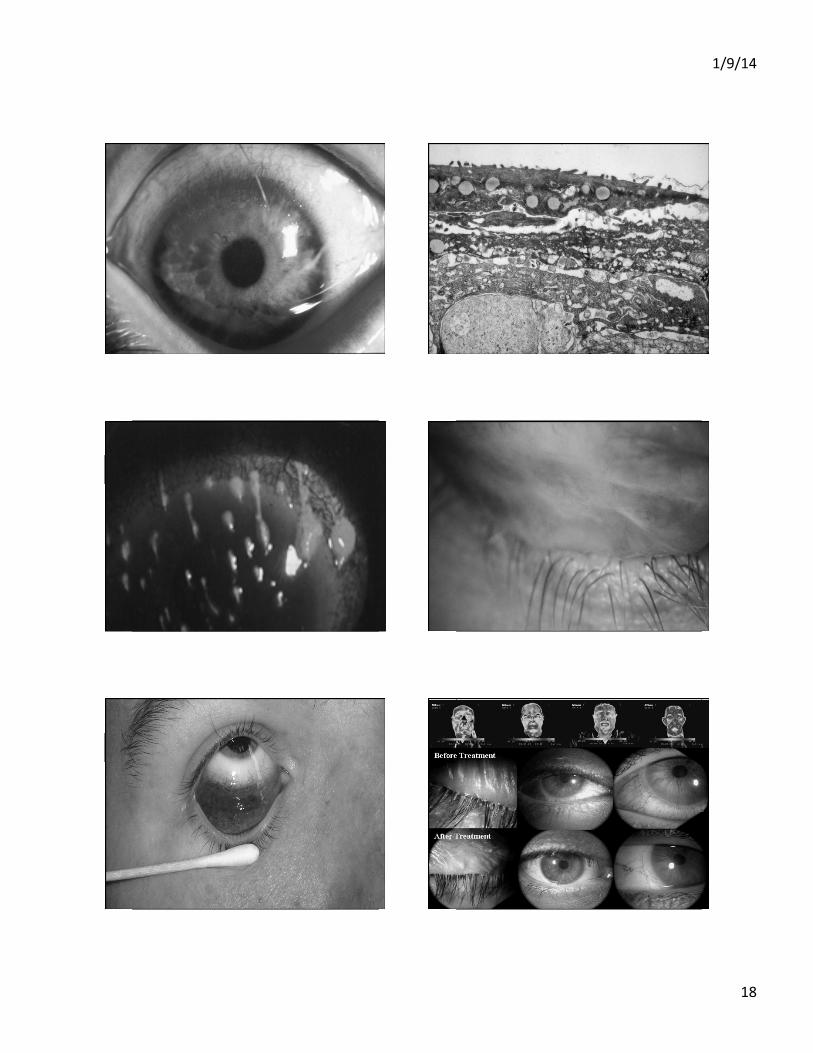
17
Conjunctival Chemosis
LID WIPER EPITHELIOPATHY
LWE rose bengal staining approaching the staining of Line of Marx
Line of Marx
Line of Marx
subtarsal fold
1/9/14
18

1/9/14
19
Demodex Keratitis

1/9/14
20
Case 7 -- corneal haze

1/9/14
21
Thyroid Disease
Thyroid dysfunction should be explored including the possibility of thyroid cancer.
Standard thyroid profile will often be normal (Wills series-40% prevalence).
Order anti-thyroid antibody panel: thyroid peroxidase (TPO) and thyroid antithyroglobulin (Tg).
The antibodies (especially TPO) will often be exceedingly high.
Corneal Pigmentation
Assorted pigment with various locations and configurations are possible.
-Fleischer (arcuate/KCN), Henle (trauma), Ferry
(filtering bleb), Stocker (pterygium),
Commonly found in post refractive surgery patients
due to altered corneal profile
Important differential with Kayser-Fleischer ring by
location and color

1/9/14
22
Keyser Fleischer Ring
Formed by copper deposition and complexes with sulfur to become visible.
Copper NOT pathognomonic for Wilson disease (also found with other hepatic conditions)
Pigmented rings are seen in many metabolic conditions and in multiple myeloma.
Present in nearly all patients with Wilson disease and neurologic symptoms.
Other ophthalmic conditions associated with Wilson disease: night blindness, strabismus, and xerophthalmia
Wilson Disease
Typically presents the first two decades of life: liver dysfunction, icterus, and hemolytic anemia.
Neurologic signs include: loss of coordination, dysarthria and abnormal muscle tone, behavioral disturbance, and loss of memory.
Joint changes and renal dysfunction are commonly found.
Diagnosis: reduced ceruloplasmin and serum copper levels, increased urinary excretion of copper and increased hepatic copper levels
Treatment: D-penicillamine
Herpes Simplex Keratitis Manifests with many different ocular
presentations
Periocular involvement (early) is possible.
Vital stains are helpful, but some have antiviral potential.
Bilateral disease is possible especially with immunocompromised or suppressed individuals, especially in occult CA and adolescent atopy.
1/9/14
23
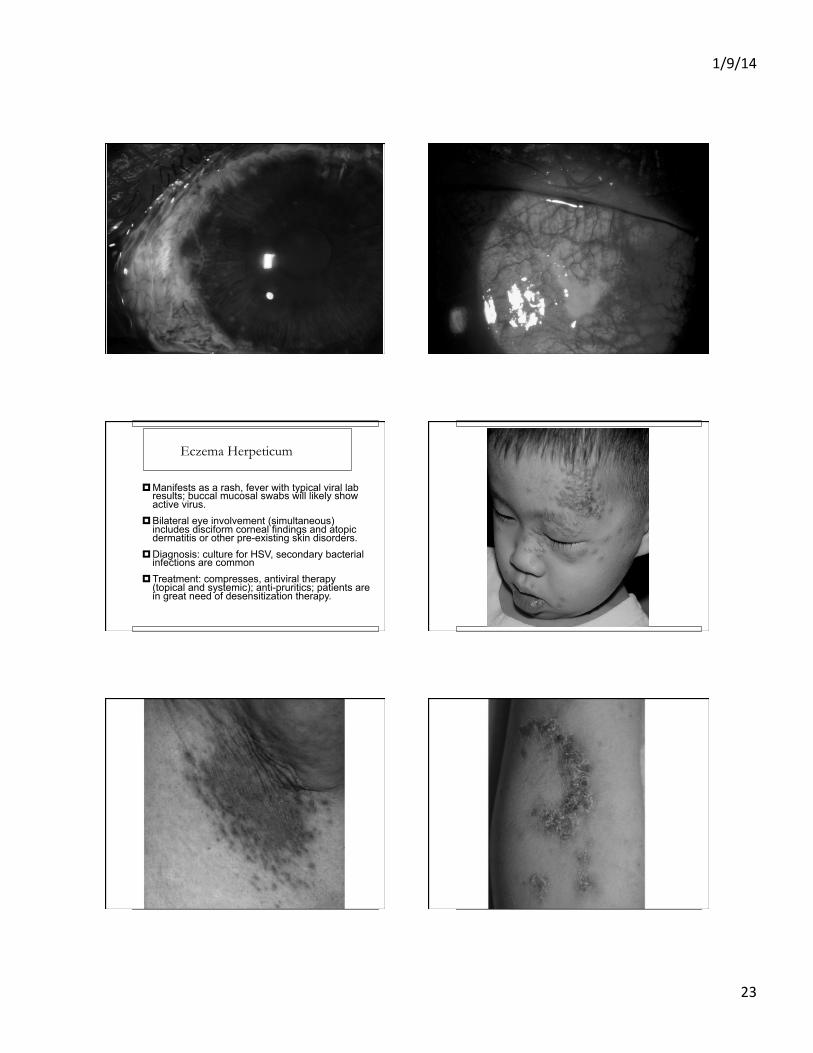
Eczema Herpeticum
Manifests as a rash, fever with typical viral lab results; buccal mucosal swabs will likely show active virus.
Bilateral eye involvement (simultaneous) includes disciform corneal findings and atopic dermatitis or other pre-existing skin disorders.
Diagnosis: culture for HSV, secondary bacterial infections are common
Treatment: compresses, antiviral therapy (topical and systemic); anti-pruritics; patients are in great need of desensitization therapy.
1/9/14
24
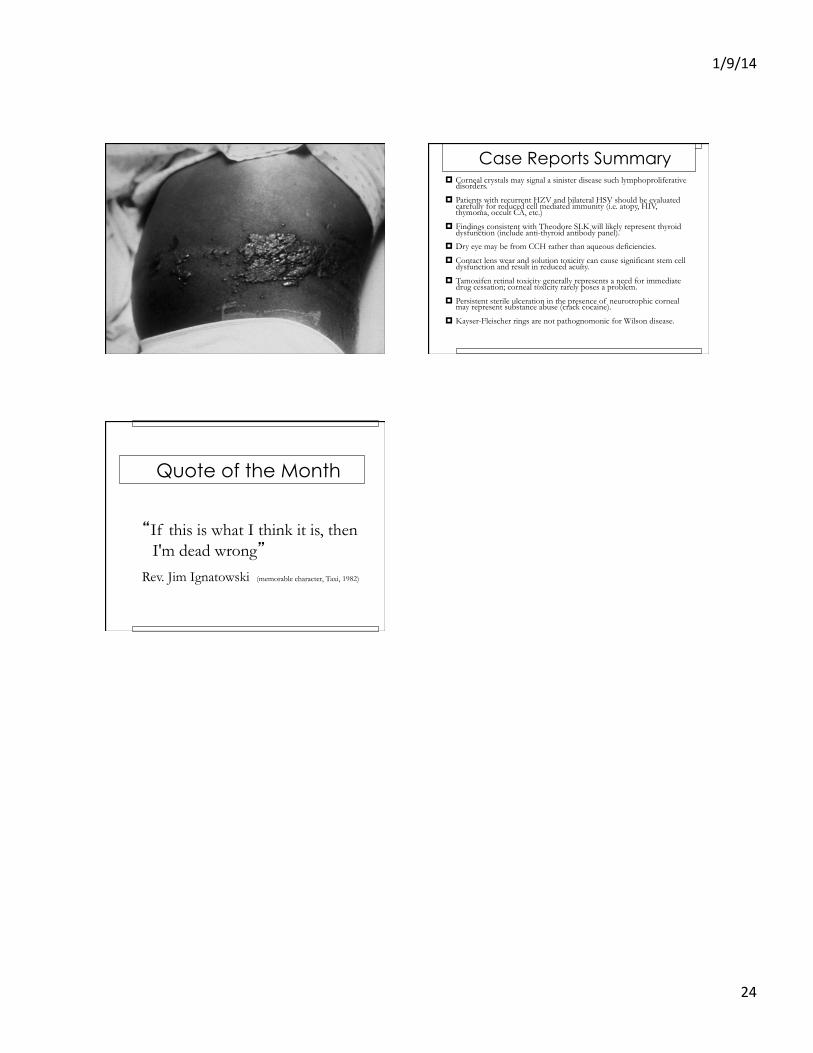
Case Reports Summary Corneal crystals may signal a sinister disease such lymphoproliferative
disorders.
Patients with recurrent HZV and bilateral HSV should be evaluated carefully for reduced cell mediated immunity (i.e. atopy, HIV, thymoma, occult CA, etc.)
Findings consistent with Theodore SLK will likely represent thyroid dysfunction (include anti-thyroid antibody panel).
Dry eye may be from CCH rather than aqueous deficiencies.
Contact lens wear and solution toxicity can cause significant stem cell dysfunction and result in reduced acuity.
Tamoxifen retinal toxicity generally represents a need for immediate drug cessation; corneal toxicity rarely poses a problem.
Persistent sterile ulceration in the presence of neurotrophic corneal may represent substance abuse (crack cocaine).
Kayser-Fleischer rings are not pathognomonic for Wilson disease.
Quote of the Month
�If this is what I think it is, then
I'm dead wrong��
Rev. Jim Ignatowski (memorable character, Taxi, 1982)