Embed Size (px)
Citation preview

Vol. 102, No. 2 Letters to The Journal 279
upon hemagglutination of sensitized sheeperythrocytes rather than fluorescence.
References
1. O'Connor, G. R.: Uveitis of microbial origin.Current and future trends. Trans. Pacific Coast OtoOphthalmol. Soc. 57:223, 1976.
2. Mendelsohn, A. D., and [ampol, L. M.: Syphilitic retinitis. A cause of necrotizing retinitis. Retina4:221, 1984.
3. Morgan, C. M., Webb, R. M., and O'Connor,G. R.: Atypical syphilitic chorioretinitis and vasculitis. Retina 4:225, 1984.
4. Hunter, E. F., Deacon, W. E., and Meyer, P. E.:An improved FTA test for syphilis, the absorptionprocedure (FTA-ABS). Pub. Health Rep. 79:410, 1964.
Corneal Subepithelial Deposits AfterUse of Sodium Chondroitin
Mark R. Coffman, M.D.,and Paul Michael Mann, M.D.Mann Eye Clinic.Inquiries to Mark R. Coffman, M.D., Mann Eye Clinic,18850 S. Memorial Blvd., Humble, TX 77338.
We used sodium chondroitin in cataract extraction and intraocular lens surgery in 21 eyesof 19 patients from November 1985 throughJanuary 1986. In six of these eyes, white deposits in the corneal stroma were noted within 24hours of surgery. These deposits appeared tomigrate anteriorly within the stroma during thefirst one or two postoperative weeks and assumed a subepithelial position. The depositshad fairly distinct borders but varied in density(Figure). There was no subepithelial edema orstromal edema.
Of these six eyes, two had undergonephacoemulsification with implantation of aposterior chamber lens and four had undergone secondary intraocular lens implantation.Regular BSS was used in all cases. Acetylcholine was used in only one eye. The postoperative medications used were prednisolone (fiveeyes), neomycin sulfate-polymyxin B (one eye),and gentamicin (one eye). In three eyes, thesodium chondroitin came from the same lot butin the other three eyes, the sodium chondroitincame from three separate lots. The sodium
Figure (Coffman and Mann). Subepithelial cornealdeposits after intraocular surgery using sodiumchondroitin.
chondroitin was not aspirated from the eye atthe end of the operation because the manufacturer suggests that leaving the sodium chondroitin in the anterior chamber is not deleterious. Intraocular pressure measurements wereobtained on the first postoperative day in all sixeyes and in no case exceeded 30 mm Hg.
The longest follow-up at this point is 20weeks. The subepithelial deposits initially appeared to fade slowly, but have stabilized during the last four to eight weeks. Visual acuity,which ranged from 20/50 to 20/200 one weekpostoperatively in the eyes with the subepithelial deposits, improved at eight weeks to 20/20to 20/30 in all but one patient. This patient hascystoid macular edema.
The University of Oregon Drug ReactionCenter has received two reports regardingchondroitin sulfate and corneal deposits. Onereport included 20 cases but minimal additionalinformation. The second report included twocases in which a "calcific band keratopathy"appeared immediately postoperatively wheresodium chondroitin touched the endothelialdeposits. Another investigator reported similarchanges in one patient referred to him (J.Rowsey, oral communication, January 1986).
280 AMERICAN JOURNAL OF OPHTHALMOLOGY August, 1986
According to the manufacturer (Cilco), the subepithelial corneal changes have been noted inapproximately 0.5% of cases. Of the surgeonsinvolved as investigators, 4.9% have noted thecorneal changes. Research has shown that thesubepithelial white deposits are probably calcium phosphate precipitates. The calcium phosphate tends to precipitate if BSS+ or sodiumcitrate is used with the sodium chondroitin.The precipitate is least likely to occur if BSS isused and at least 50% of the sodium chondroitin is aspirated or irrigated from the anteriorchamber. Six months to two years may berequired for the subepithelial deposits to resolve. The manufacturer recommends no treatment if the deposits are outside the visual axisand do not affect visual acuity. If visual acuityis effected, topical EDTA may be used for chelation.
References
1. Barron, B. A., Busin, M., Page, c., Bergsma,D. R., and Kaufman, H. E.: Comparison of the effects of Viscoat and Healon on postoperative intraocular pressure. Am. J. Ophthalmol. 100:337, 1985.
2. Wilson, M. F. II: Adverse external ocular effectsof topical ophthalmic medications. Surv. Ophthalmol. 24:47, 1979.
Palmar-Plantar HyperkeratosisAssociated With BilateralKeratopathy
Saul Ullman, M.D.,Leonard B. Nelson, M.D.,and Ming-liang Lee, M.D.Department of Pediatric Ophthalmology, Wills EyeHospital (S.U. and L.B.N.) and Department of Pediatrics, Division of Medical Genetics, Rutgers MedicalSchool (M.L.).Inquiries to Leonard B. Nelson, M.D., Wills Eye Hospital, Ninth and Walnut Sts., Philadelphia, PA 19107.
Hyperkeratosis of the volar aspects of thehands and feet is a rare condition that may beassociated with inborn errors of metabolismand ophthalmic disease;' We studied a patientwith palmar-plantar hyperkeratosis associated
with severe corneal epithelial disease and developmental delay.
The patient, a 25-month-old girl, was theproduct of an uneventful full-term pregnancy.When she was first examined at the age of 22months, it was found that she had had severephotophobia, tearing, and blepharospasmsince the age of 6 weeks. The child was beingmonitored for developmental delay and wastaking no medications. The family history wasnoncontributory for ophthalmic or dermatologic disorders.
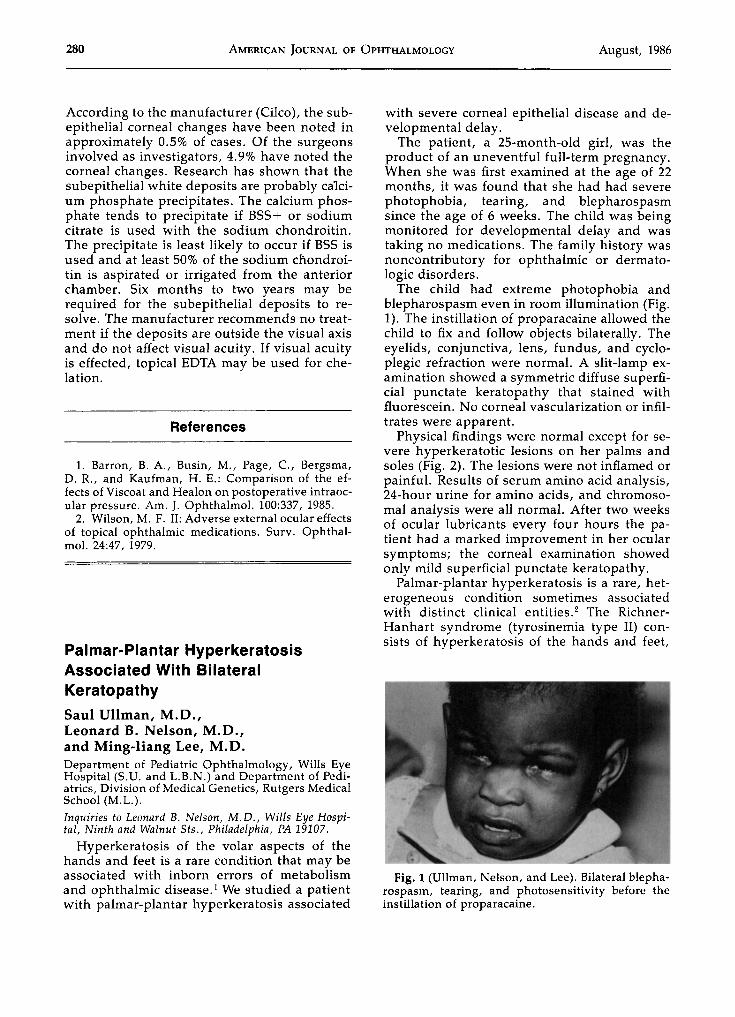
The child had extreme photophobia andblepharospasm even in room illumination (Fig.1). The instillation of proparacaine allowed thechild to fix and follow objects bilaterally. Theeyelids, conjunctiva, lens, fundus, and cycloplegic refraction were normal. A slit-lamp examination showed a symmetric diffuse superficial punctate keratopathy that stained withfluorescein. No corneal vascularization or infiltrates were apparent.
Physical findings were normal except for severe hyperkeratotic lesions on her palms andsoles (Fig. 2). The lesions were not inflamed orpainful. Results of serum amino acid analysis,24-hour urine for amino acids, and chromosomal analysis were all normal. After two weeksof ocular lubricants every four hours the patient had a marked improvement in her ocularsymptoms; the corneal examination showedonly mild superficial punctate keratopathy.
Palmar-plantar hyperkeratosis is a rare, heterogeneous condition sometimes associatedwith distinct clinical entities." The RichnerHanhart syndrome (tyrosinemia type II) consists of hyperkeratosis of the hands and feet,
Fig. 1 (Ullman, Nelson, and Lee). Bilateral blepharospasm, tearing, and photosensitivity before theinstillation of proparacaine.





![Fu abutment stabilization technique (FAST): A simple ...Subepithelial connective tissue graft (CTG) [24-27] Subepithelial Connective Tissue Graft (CTG) is commonly harvested from the](https://img.pdfslide.net/doc/110x75/601a275155ed9c309b1586a7/fu-abutment-stabilization-technique-fast-a-simple-subepithelial-connective.jpg)