Embed Size (px)
Citation preview


148
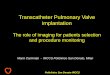
Fig. 10.1:All four heart valves
are seen from abovehere. The pulmonaryvalve is seen on topwith the aortic valve
immediately below it.The two red dots depictwhere the coronary ar-
teries originate in theaorta just above the
aortic valve. The twolower valves are the
tricuspid, on the right,and the mitral valve on the left. The two
illustrations show thevalves during two
stages of the heart cycle.
Mitral Valve
Coronary Arteries Pulmonary Valve
Aortic Valve
Tricuspid Valve
Mitral Valve
Coronary Arteries Pulmonary Valve
Aortic Valve
Tricuspid Valve
Ventricular Systole
Ventricular Dyastole
Fig. 10.1

PICTURE A RED BLOOD CELL TRAV-eling through the venous systemtoward the heart. It enters the heart
through one of two major veins, either thesuperior vena cava or the inferior venacava, and passes into the right atrium. Theone-way tricuspid valve opens, and thecell flows into the right ventricle. The tri-cuspid valve is composed of three leafletsthat are connected on their underside (rightventricle side) to string-like structurescalled chordae tendineae, which are con-nected to muscles called papillary muscles.The papillary muscles are outgrowths ofthe muscular right ventricular wall.
As the right ventricle contracts, thetricuspid valve closes and the pulmonaryvalve opens, allowing the blood cell to bepumped, or propelled, into the pulmonaryartery, which channels unoxygenatedblood containing carbon dioxide to thelungs. Like the tricuspid, the pulmonaryvalve is one-way and composed of threeleaflets (also called cusps), although theleaflets differ from those of the tricuspidvalve in shape. They look like three smallcups. The pulmonary valve does not havechordae tendineae or papillary muscles.
After giving off carbon dioxide andpicking up oxygen in the lungs, the newlyoxygenated red blood cell returns to the
heart through one of the pulmonary veinsand into the left atrium. The two-leaflet mi-tral valve opens, and the cell travels intothe left ventricle. Like the tricuspid, the mi-tral valve has chordae tendineae, whichare attached to papillary muscles. Whenthe mitral and tricuspid valves are closed,the valve leaflets look like a parachute, andthe chordae tendineae resemble the cordsthat connect the parachute to the jumper.The papillary muscle is the jumper.
When the left ventricle contracts, theaortic valve opens, allowing the red bloodcell to stream out the aorta and into thearterial system that nourishes the body(see Fig. 10.1 for cardiac cycle). The twocoronary arteries branch off the base ofthe aorta (aortic root) just above the aor-tic valve leaflets.
Before the Heart-Lung Machine:
Opening Narrowed Valves
The first attempt to open a stenotic(narrowed) heart valve in a human wascarried out by Dr. Theodore Tuffier, aFrench surgeon, on July 13, 1912. Afteropening the patient’s chest, he supposed-ly pushed the wall of the aorta near theheart through the stenotic aortic valve
C H A P T E R T E N
HEART VALVE PROBLEMS
149
Chordae Tendineae:String-like attachmentsthat are part of the mitral and tricuspidvalve apparatus thatconnects the valveleaflets, or flaps, to the papillary muscleson the ventricular wall.
Papillary Muscles:Tiny muscles located in the left and rightventricles that are attached by chordaetendineae to the mitraland tricuspid valves.These muscle structureshelp control the valve function.

S T A T E O F T H E H E A R T
and dilated the valve. The patient survivedand was reported to be improved.
About ten years later, Dr. Elliot Cutler,a surgeon at Harvard Medical School, incollaboration with Boston cardiologistSamuel Levine, worked out a procedure todilate the mitral valve. Their first patientwas a desperately ill twelve-year-old girlwhose mitral valve had been badly dam-aged and narrowed from rheumatic fever.She underwent successful mitral valve di-latation on May 20, 1923. Unfortunately,most of Cutler’s subsequent patients didnot survive the surgery, and he abandonedthe procedure.
These sporadic and mostly unsuc-cessful attempts ceased by 1929, andthings remained quiet until 1945, whenDr. Charles Bailey and his team again at-tempted to treat mitral valve stenosis. Thefirst of their five human patients was athirty-seven-year-old man who was oper-ated on on November 4, 1945. He bled todeath in the operating room during theprocedure. The second patient was atwenty-nine-year-old woman operated onon June 12, 1946. Her condition im-proved for the first thirty hours after the
surgery but suddenly deteriorated, andshe died forty-eight hours after thesurgery. After these two failures, Bailey’shome base, Hahnemann Hospital inPhiladelphia, refused to allow him to at-tempt any more mitral valve dilatations.He even became known as the “butcher”of Hahnemann Hospital.
Their third patient, who was treated ata different hospital, was a thirty-eight-year-old man operated on on March 22, 1948.The surgery seemed to go well, but the pa-tient hemorrhaged into the chest cavity onthe second postoperative day. He died ofcomplications. Patient four was a thirty-two-year-old man who underwent heartsurgery on June 10, 1948. His heartstopped while the incision was being madeto start the surgery. He could not be re-suscitated and died in the operating room.
The surgical team then immediate-ly regrouped and rushed to EpiscopalHospital, where the fifth operation, thisone on a young woman, was started beforethe bad news from that morning wasknown and the hospital administrationcould forbid the procedure. Her mitralvalve dilatation was successfully complet-ed. One week later, Bailey brought thepatient by train one thousand miles toChicago, where he presented her to theAmerican College of Chest Physiciansannual meeting. She was without symp-toms after the surgery and felt betterthan she had been feeling for years.
On June 16, a few days after Bailey’ssuccess, Dr. Dwight Harken in Boston suc-cessfully performed his first mitral valvedilatation. Three months later, SirRussell Brock in England did his firstsuccessful similar procedure but did notreport it until 1950, when he described sixadditional successful attempts.
Targeting the Pulmonary Valve
On December 4, 1947, Dr. ThomasHolmes Sellers, an English surgeon, com-pleted the first successful surgery on a
150
Stenosis:An abnormal narrow-
ing of an orifice, bloodvessel, or heart valve.
Dr. Elliot Cutler (below)performed the first
successful mitral valvedilatation. His patient, a12-year-old girl (right),
had suffered fromrheumatic fever. Her surgery was
successful.

C H A P T E R T E N : H E A R T VA L V E P R O B L E M S
narrowed pulmonary valve. The surgeryoccurred during an operation for a con-genital heart defect called tetralogy ofFallot. In this condition, there is an ob-struction of blood to the lungs and ahole in the heart. This particular pa-tient also suffered from advanced tu-berculosis of both lungs. When Sellersopened the sac around the heart, hecould feel the narrowed pulmonaryheart valve each time the right ventriclecontracted. He passed a special type ofknife through the wall of the right ven-tricle and made slits in the narrowedvalve. The patient made a good recoveryand was markedly improved.
The Development of Valve Replacement Surgery
Like all forms of heart surgery, valvu-lar surgery made great leaps forward asthe heart-lung machine came into use.Doctors who had once only imagined theday when diseased valves could be re-placed began to actually work to developimplantable valves. Artificial valves were
not a novel idea. The first ones had beendeveloped in the 1950s, when Drs.Charles Hufnagel in Washington, D.C.,and J.M. Campbell in Oklahoma indepen-dently developed and implanted artificialvalves in the descending aortas of dogs.This could be done before the heart-lungmachine because the descending aorta isfar enough away from the heart. The sur-geon merely placed clamps several inchesapart on the aorta to interrupt blood flow,opened the aorta, inserted the artificialvalve, and then stitched the aorta closed.
These two valves, which were called“cage-ball valves” because of their design,looked similar. After presenting this mechan-ical heart valve technique in animals atthe American College of Surgeons annualmeeting in 1949, Hufnagel began to usethis procedure in human patients suffer-ing from aortic valve incompetence. Thevalve implantation did not actually replacethe patient’s own leaky aortic valve butacted as a supporting or auxiliary valve.
The Advent of the Heart-Lung Machine
Once the heart-lung machine wasdeveloped, surgeons began to attempt heartvalve replacement with cage-ball valves.The first successful valve replacement wasperformed by Dr. Dwight Harken andhis colleagues at Harvard’s Peter BentBrigham Hospital in Boston. Harken useda cage-ball valve to replace the aorticvalve. Many of the techniques described inhis 1960 report are similar to those usedtoday for aortic valve replacement.
The same year, Dr. Albert Starr suc-cessfully replaced the mitral valve byusing a cage-ball valve.
In 1964, Starr and associates reportedon thirteen patients who had undergonemultiple heart valve replacements. One pa-tient had the aortic, mitral, and tricuspidvalves replaced on February 21, 1963.
By 1967, nearly two thousand Starr-Edwards heart valves had been implant-ed, and the cage-ball prosthesis had gen-
151
In 1960, Dr. DwightHarken (left) performedthe first successfulvalve replacement inthe normal aorticvalve position with an artificial valve. He useda cage-ball valve to replace the aortic valve.
Tetralogy of Fallot:A set of four individualdefects, including: 1) a ventricular septaldefect; 2) an obstructionof blood flow from theright ventricle to thepulmonary arteries; 3) overriding of the aor-tic valve above the ven-tricular septal defect;and 4) an abnormallythickened right ventricle.

S T A T E O F T H E H E A R T
152
Dr. Albert Starr (right)was part of the team
that developed theStarr-Edwards cage-
ball heart valve (facingpage). Starr was thefirst to successfully
replace a mitral valvewith that valve. The
Starr-Edwards valveswent on to become the
world standard.
AFTER GRADUATING FROM Columbia College of Physicians and Surgeons in 1949, Dr. Albert
Starr served a one-year intern-ship at Johns Hopkins Hospital.There, he worked under the world fa-mous surgeon Dr. Alfred Blalock, whohad pioneered the Blalock-Taussigoperation for children with cyanoticheart disease.
When his internship was completed,Starr returned to New York but was soondrafted into the U.S. Army MedicalCorps to serve first as a battalion sur-geon in the First Cavalry Division inKorea, then as a surgeon for a MobileArmy Surgical Hospital (MASH) unit. Ina single year, he performed more thanone thousand major operations.
“Korea was the first war in whichyou had an almost unlimited backupsystem to a limited war,” Starr said ina recent interview. “It was a war inwhich there was almost an unlimit-ed supply of human blood availablefor transfusion on the battlefield. Therewas also the beginning of antibiotics,and helicopter evacuation so that some-one wounded in a firefight in Koreawould be back in a MASH within min-utes of being wounded, rather thanhours or days. The survival rate, ifyou made it back to the MASH hos-pital, was about 95 percent.”
After his tour of duty, he returned tocomplete his surgical training at Bellevueand Presbyterian hospitals in New York.By 1957, Starr had finished his thoracicsurgery residency and moved to theUniversity of Oregon, Portland, to start
an open heart program. This is whereStarr was first exposed to heart valvesurgery and the problems surgeonswere having repairing diseased valves.After experimenting with all sorts ofvalve prostheses, Starr became con-vinced that valve replacement wasnecessary to save many patientswith diseased mitral valves becausethere was no way to repair badly de-formed and diseased mitral valves.
Enter a retired engineer named M.Lowell Edwards. A successful and inde-pendently wealthy engineer, Edwardshad several important inventions to hiscredit and originally approached Starrto help him develop an artificial heart.
“I thought he was overreaching, toput it mildly,” Starr said. “What I dis-covered was that he was a very suc-
ALBERT STARR AND THESTARR-EDWARDS HEART VALVE
Albert Starr

C H A P T E R T E N : H E A R T VA L V E P R O B L E M S
153
cessful engineer, and although he waswearing the typical Oregon golfer’s dress,he was very accomplished and hadnumerous inventions to his credit. Oneof them was a fuel injection system forrapidly climbing aircraft during WorldWar II. The P-38 and many of our fight-er aircraft had his fuel injection system,and a good part of the successful wareffort, at least as far as the air war isconcerned, is credited to his fuel injec-tion system. In the Battle of Britain,the Spitfires had his fuel injection sys-tem, and that enabled them to get upto very high altitudes very rapidly with-out the system failing.”
When Starr pointed out that med-icine didn’t even have artificial valvesyet, much less an artificial heart, the twodecided to begin one valve at a timeand invent prostheses. They startedwith the mitral valve and consideredevery kind of valve known. After driftingfrom valve to valve, they finally hitupon the ball valve, which showed earlypromise because it was not as easilyoccluded by the blood clots that quick-ly formed around the sutures of moreconventional leaflet-type valves.
They quickly learned, however, thatblood clots did form in the ball valves —it just took longer before the clot waslarge enough to block up the free-movingball. At the time, they were performingtheir early experimentation in dogs,many of whom were dying from throm-bosis months after their valves were im-planted. This challenge led Starr andEdwards to the silastic shield, whichwas basically a retractable diaphragmthat covered the sutures and preventedblood clots from forming. This shield cre-ated long-term survivors, and soon Starrhad a kennel full of active dogs that hadundergone mitral valve replacement.
“The chief of cardiology, Dr. HerbertGriswold, knew we had a kennel full of
active dogs and came to visit us in August1960. He looked at all these dogs andsaid, ‘Starr, we have to do this clinical-ly.’ That was the first time we beganto think about that seriously because Ithought it would be a couple years’ pro-ject at least.”
Interestingly, the first valve im-planted in a human did not use thesilastic shield. Starr, knowing thatdog’s blood clots very aggressively, fig-ured he wanted the simplest proce-dure possible and, if the patient’sblood clotted, they could always ad-minister anticoagulant medication.This first operation was done inSeptember 1960 on a young woman inher mid-twenties. The Starr-Edwardscage-ball valve prosthesis quickly be-came established as the gold standardin mechanical heart valve prostheses.
“This generated tremendous ex-citement and put the Oregon HealthSciences University on the map,” Starrsaid. “We had visitors from all overthe world.”
Starr-Edwards cage-ball heart valve

S T A T E O F T H E H E A R T
erated intense excitement and become es-tablished as the gold standard for mechan-ical heart valve prostheses. The valvesmaintained this status for many years,although today newer, low-profile valvesare commonly used. There are, however,still some surgeons implanting theoriginal Starr-Edwards cage-ball valve.
Human Valves Used in Other Humans
Not long after the first heart valveswere implanted, physicians began search-ing for better heart valves — includingbiological valves. Biological valves arevalves from animals or human cadavers orvalves made from other animal tissue.An aortic homograft valve was first used in1962 to replace a mitral valve in one pa-
tient and an aortic valve in another.Survival was short.
That same year, Dr. Donald Ross inEngland reported the first successful aor-tic valve homograft implant. He placedthe valve in the normal position. A monthlater, Sir Brian Barratt-Boyes performedthe same implantation in New Zealand.
Shortly after his success, Dr. Rosswent on to develop another technique. In1967, he used the patient’s own pul-monary valve to replace a malfunction-ing aortic valve. An aortic or pulmonaryvalve homograft was then used to replacethe patient’s pulmonary valve. Thisprocedure, known as the Ross Procedure,is currently recommended for someyounger patients who require aorticvalve replacement.
154
Homograft:A donor graft, or por-
tion of tissue, takenfrom a donor and
placed into a recipientof the same species.
Dr. Donald Ross wasthe first to successfullyreplace an aortic valve
with a tissue valvefrom another human.He also invented the
Ross Procedure, whichis still in use today to
replace a malfunction-ing aortic valve.
DR. DONALD ROSS QUALIFIEDfor his medical degree on thesame day as Dr. Christiaan
Barnard, a fellow SouthAfrican. Although the twowould take divergentpaths — Ross went toEngland to train andBarnard went to theUnited States — they re-mained friends, and bothworked to develop hearttransplantation. Ross re-called in an interview aconversation he had withBarnard before the firsttransplantation.
“Barnard came throughone day and said, ‘I’ve justbeen watching Shumway do the trans-
plant of the heart in an animal and I’mgoing to do that,’” Ross remembered.
Later that same year, a reporterasked Ross when hethought the first hearttransplantation would beperformed. He predictedsometime within the nextfive years. Less than amonth later, Barnard an-nounced he had performedthe first human-to-humantransplant. Shortly after-ward, Ross himself per-formed the first hearttransplant in the UnitedKingdom.
Although his work inheart transplantation was cut-
ting edge, Ross became most famous for
DONALD ROSS: THE VALVE PIONEER
Donald Ross

C H A P T E R T E N : H E A R T VA L V E P R O B L E M S
Other tissues that have been usedfor valve implants include the pericardi-um, fascia lata, or tissue from tendons,and dura mater, which is the tissue thatsurrounds the brain and spinal cord.
In the 1960s, physicians also beganto experiment with valves from other ani-mals, or xenografts. This was first done in1964 by Drs. Carlos Duran and AlfredGunning in England, who replaced anaortic valve in a human by using a valvefrom a pig. The early results were good,but these valves often failed after a fewyears. In France, for instance, Dr. AlainCarpentier and his associates reported ontwelve patients with pig valve replace-ments that all failed by five years. As a re-sult, Carpentier developed a technique tofix the pig valves with a chemical called
glutaraldehyde instead of using theaccepted formaldehyde. In addition,Carpentier mounted his valves on a stent,which allowed the valves to be used to re-place the mitral and tricuspid valves.
Carpentier later wrote:
“It became obvious that the future oftissue valves would depend on the de-velopment of methods of preparation ca-pable of preventing inflammatory cell re-action and penetration into the tissue. Mybackground in chemistry was obviouslyinsufficient. I decided to abandon surgeryfor two days a week to follow the teach-ing program in chemistry at the Faculty ofSciences and prepare a Ph.D. (at theUniversity of Paris). It was certainly noteasy to become a student in chemistry
155
Xenograft:Graft tissue taken from an animal of onespecies and used inanother species. Pigheart valves, which are commonly used to replace heart valves in humans, are oneform of xenograft.
his pioneering work with heart valves.This was an area of interest from thebeginning of his career. In July 1962,Ross implanted the world’s first suc-cessful homograft valve (a tissue valvefrom a human cadaver) only two yearsafter Starr and Harken implanted theirheart valves. Ross recounted this his-torical implantation:
“Lord Brock was my mentor andchief and put me onto repeatingearlier pioneering work in homo-graft implantation [in the animallaboratory]. It was a very excitingtime. We took human valves andhuman aortas and stored them bya process of freeze drying so theycould keep for months.
“One day during surgery while Iwas scratching away at a calcifiedvalve, the whole thing disintegratedand went down the sucker. We didn’thave a valve and there were novalves in England. There were onlyStarr valves in America. So we took
one of those stored human valves,which was freeze dried, reconstitutedit and sewed it in.”
Originally, the valve was supposedto be temporary until the surgical teamcould import a mechanical valve. Thepatient did well, however, and Rossswitched to implanting homograft valvesinstead of artificial valves.
Over the next several years, he foundthat an aortic valve homograft workedwell in the pulmonary valve position.That discovery led to an importantmilestone in valve surgery, the RossProcedure. In this operation, the na-tive pulmonary valve is relocated tothe aortic position, and a homograftvalve replaces the pulmonary valve.
It is a technically difficult opera-tion that took almost two decades togain widespread acceptance but it isperformed today with excellent results.It has the powerful advantage that thenew aortic valve will grow, an especial-ly important quality for small children.

S T A T E O F T H E H E A R T
when you are thirty-five years old and anassociate professor of surgery.
“I began to investigate numerouscross-linking-inducing factors and foundthat glutaraldehyde was able to almosteliminate inflammatory reaction.... Mywife, Sophie, was a tremendous help allthese years.”
Modern Heart Valve Therapy
Rheumatic Fever
Today, surgeons are capable of treat-ing a wide range of heart valve defects,which can be caused by a number of con-ditions. Rheumatic fever is a commoncause of heart valve injury requiringsurgery in adults. People of any age cancontract rheumatic fever, but it’s most
common in children between the ages offive years and fifteen years. It is caused bybacteria known as streptococcus and isusually related to a severe type of sorethroat sometimes called a “strep throat.”Most people who have strep throats do notdevelop rheumatic fever, and appropriatetreatment with antibiotics dramaticallydecreases the risk of developing rheumat-ic fever. Rheumatic fever usually occursfrom two weeks to a month after the strepthroat infection.
Symptoms of rheumatic fever includeaches and pains in the joints. The pain inthe joints tends to migrate from one jointto the next, and it’s not always located inthe same joint. Rashes can occur. Lumps,called subcutaneous nodules, can developunder the skin. Victims sometimes devel-op uncontrolled movements of the legs and
156
Dr. Alain Carpentier(above) was a major
figure in the develop-ment of pig valves for
human hearts. Hisvalves (below) were
mounted on cloth ringsto help physicians sew
them in place.
Cardiomyoplasty: A surgical procedure
using a muscle, usuallythe latissimus dorsi
muscle in the back, towrap around a failingheart. The muscle is
then electrically stimu-lated so it will contractin synchrony with the
failing heart.
DR. ALAIN CARPENTIER DECIDEDto go into medicine after an op-
eration and a month-long stay ina hospital for appendicitis when he wasonly ten years old. At the time, an-tibiotics were not widely available, andhis recovery was very long and painful,inspiring in the young boy a desire tohelp the course of healing. Today, heis best known for three major contri-butions to heart surgery. He developedsurgical techniques to repair the mitralvalve; he developed a practical methodof using heart valves from pigs inhumans; and he pioneered a surgi-cal procedure called cardiomyoplas-ty, which is used in patients with fail-ing heart muscle.
Carpentier began his researchinto heart valve replacement at a timewhen mechanical heart valves, suchas the Starr-Edwards valve, had justrecently become commercially avail-
able. Physicians were also successful-ly using heart valve implants fromhuman cadavers, a technique pioneeredby Ross and Barratt-Boyes. Inspiredby their work, Carpentier began to re-search biological valve replacementsbut ran into a snag in French law.
“My surgical master, Dr. CharlesDuBost, told me if I was interested, Iwould have to collect homograftvalves, just like Barratt-Boyes andRoss did,” he remembered in a 1999interview. “I began to try to collecthomograft valves in Paris; however,French law did not permit one to takepieces from cadavers during the forty-eight hours following death to allowthe family to make an opposition. Ofcourse, after forty-eight hours, most ofthe homograft valves I could collectwere infected.”
After a few months of this, Carpentierbegan researching the use of valves
ALAIN CARPENTIER
Alain Carpentier

C H A P T E R T E N : H E A R T VA L V E P R O B L E M S
arms, called chorea. Patients with rheumat-ic fever can also develop an inflamma-tion of the heart muscle called carditis,which can result in shortness of breathand fatigue. Fever can also be present.
Although it doesn’t always do so,rheumatic fever can cause damage to anyor all of the heart valves. The aortic and mi-tral valves are most commonly affected.
A second episode of rheumatic fevercan further damage the heart, particular-ly the heart valves. Patients with damagedheart valves may need heart surgery rela-tively soon after their rheumatic fever.However, most people who need heartsurgery will require it much later, some-times late in life, even though they con-tracted rheumatic fever as a child. Abouthalf of all patients who require heart valvesurgery as adults because of rheumatic
fever damage do not even know that theyhad rheumatic fever.
Infectious Endocarditis
Bacterial and fungal infections are an-other threat to both the heart and theheart valves (Fig. 10.5). In many cases, theexact reason for the infection is unknown.During a dental procedure, for example,bacteria may gain access to the blood-stream. Antibiotics should be given be-fore a dental procedure to those who havea diseased or artificial heart valve to helpprevent infectious endocarditis, or infec-tion of the heart muscle. Other causesinclude surgery and illicit intravenousdrug use.
In most cases, infections of the heartand heart valves can be treated with
157
Endocarditis: An infection inside the heart.
from other animals, or xenografts. It wasthis effort that led him to his workwith glutaraldehyde and the techniqueto successfully replace any of the fourheart valves with xenografts. He calledthese tissue heart valves, which weremounted on a cloth sewing ring,“bioprostheses,” a term that is stillused today.
At the same time, he also devel-oped what he considers his most im-portant contribution to valve surgery:reconstruction of the mitral valve, asopposed to replacement of it. Thisquestion of valve replacement versusvalve repair used to be answered dur-ing surgery. Today, Carpentier cred-its medical technology like echocar-diography with greatly improvingvalve analysis.
“In the old days, I adopted a policythat I would try to repair the valve for fif-teen minutes and if I was not satisfiedafter fifteen minutes, I would just re-place the valve,” he said. “Progressively,the number of valves I had to replace di-
minished. Today, of course, is very dif-ferent because we see patients at an ear-lier stage and we have the echocardio-graphy technique, which I call thestethoscope of the next century becauseit is so useful.”
Valve repair was a superior optionto replacement, according to Carpentier,because of the drawback of valve pros-theses. “The reason I developed thesetwo techniques almost simultaneouslyis the fact that, in 1966 to 1967, theonly existing solution when a patienthad a valvular problem was replace-ment with a mechanical valve,”Carpentier said. “I was struck by thefact that one of my patients was apainter and was obliged to stop hisartistic activity after the operation. Hewas a well-known artist, and I found ita real tragedy that although the me-chanical valve made it possible to savehundreds of lives, there was this prob-lem of emboli (blood clots breakingaway from the valve) and the need foranticoagulation.”

S T A T E O F T H E H E A R T
antibiotics. In some cases, however, one ormore of the heart valves can be severelydamaged by an infection and may requireheart surgery to repair or replace the valve.
Prolapsed Mitral Valve
Mitral valve prolapse, or MVP, is a con-dition in which the leaflets of the mitralvalve do not meet properly, usually be-cause the chordae tendineae are too long(Fig. 10.2). Sometimes one or both valveleaflets are also abnormally enlarged.When the leaflets do not meet correctly,the heart valve may make an abnormalnoise when it closes. This can be heardwith a stethoscope. If they do not toucheach other when they close, blood from theleft ventricle can leak back into the left atri-um. This can cause a heart murmur.
Some patients may have chest painrelated to mitral valve prolapse. They maydevelop cardiac arrhythmias, or irregularheartbeats, and shortness of breath.Medications may alleviate these symptoms.Fortunately, the great majority of patientswith mitral valve prolapse lead a normallife and do not need a surgical procedure.Some people with diagnosed mitral valveprolapse are also encouraged to under-take an antibiotic regime both before andafter dental work, even teeth cleaning.
The cause of mitral valve prolapse isunknown. It is more common in women.Occasionally, patients require heart surgery,particularly if the chordae tendineae con-necting the prolapsed mitral valve to theheart wall rupture.
Aortic Valve Disease
The aortic valve is responsible forregulating the flow of blood from the leftventricle into the aorta. As time goes byand the valve is subjected to stress, cal-cium may deposit on the leaflets andcause the valve to become stenotic, orconstricted (Fig. 10.3). This process is ac-celerated by rheumatic fever. The leaflets(cusps) become scarred. Over time, thescar tissue increases, and the valve itselfbecomes calcified.
Aortic valve stenosis is also relatedto a condition known as a congenital bi-cuspid valve. In this condition, the aorticvalve, which normally has three leaflets,has only two. The bileaflet valve does notusually cause problems in childhood,but after many years it tends to scar. Aswith rheumatic fever or stenosis, calci-um builds up, and the valve orifice be-comes very narrow. Bicuspid aorticvalves tend to calcify in some people byage twenty years or thirty years. They
158
Fig. 10.2: Mitral valve prolapse,or MVP, occurs when
the valve leaflets donot meet properly. The
mitral valve on the nearright is healthy. The
mitral valve on the farright is prolapsed.
Prolapsed Mitral Valve
Healthy Mitral Valve
Fig. 10.2

C H A P T E R T E N : H E A R T VA L V E P R O B L E M S
usually become symptomatic betweenages thirty years and sixty years.
Stenotic aortic valves cause stress onthe left ventricle, which is forced to workharder to push blood through the nar-rowed opening. As a result, the ventric-ular heart muscle will thicken, or hyper-trophy, until it actually outgrows its bloodsupply. Finally, the left ventricle will nolonger be able to force enough blood pastthe valve.
In this case, the heart itself maybegin to fail, and patients usuallystart to develop symptoms includinglightheadedness, or they may even passout because not enough blood is gettingto the brain. Irregular heartbeats andangina pectoris are also symptoms. Thiskind of angina occurs not only becausethe heart muscle outgrew its blood sup-ply but also because not enough blood isgetting past the narrowed aortic valveand into the coronary arteries that sup-ply the heart.
Heart failure, signaled by shortness ofbreath and fatigue, is also associated withaortic valve stenosis. These symptoms aremore commonly brought on by exercise,which increases the body’s demand foroxygen. The severity of symptoms of aorticstenosis does not always correlate with theseverity of the blockage. Sometimes thefirst sign of severe aortic stenosis is sud-den death.
Diagnosing Aortic Stenosis
This condition can be diagnosed byusing a number of different techniques.The first clue is frequently obtained with astethoscope, which reveals a heart mur-mur that is rather typical of aortic steno-sis. Further testing will be performed, in-cluding the two definitive tests that revealaortic stenosis: echocardiography andcardiac catheterization. If the aortic steno-sis is severe enough to warrant heartsurgery, the patient will frequently under-go both tests.
Aortic Valve Incompetence
Aortic valve incompetence, also calledinsufficiency or regurgitation, usually oc-curs when the three leaflets of the aorticvalve do not come in contact with eachother when the valve closes. Some of theblood that has just been pumped into theaorta leaks back into the left ventricle. Thismakes the left ventricle much less efficientbecause it pumps the same blood twice.
159
Fig. 10.3:Aortic Valve Stenosis: A condition in which theaortic valve is narrowed, which stresses the leftventricle because it hasto work harder to getblood through the valve.
Angina Pectoris:Chest pain that occurswhen the heart is notgetting enough blood.Often described as pres-sure, like a band tighten-ing around the chest, ora dull, aching pain overthe front left side of thechest. It can also be apain radiating down theleft arm or, occasionally,it can radiate into theneck or jaw.
Aortic Valve
Aorta
Fig. 10.3

S T A T E O F T H E H E A R T
Aortic valve incompetence can becaused by rheumatic fever (Fig. 10.4). Italso can result from infective endocardi-tis or a number of other causes.
Aortic valve incompetence ranges inseverity from mild to severe. Mild to mod-erate aortic valve incompetence is general-ly well tolerated. Most patients with mildor moderate aortic incompetence can leada normal life and have a normal life ex-pectancy. If the leakage becomes great,however, the left ventricle will start to di-late and fail. Patients can develop signsand symptoms of congestive heart failure,including shortness of breath and fatigue,and their ankles may become swollen. Adefinitive diagnosis is made with echocar-diography and/or cardiac catheterization.
In some cases, aortic incompetencecan appear rather quickly and be severe.This could be related to an infection inwhich one of the heart valve leaflets is de-stroyed, or it can happen as a result oftrauma sustained in an automobile acci-dent when the chest strikes the steeringwheel. There can be other causes. Inthese situations, emergency heart surgerywith heart valve replacement is necessary.
Aortic Valve Stenosis and Incompetence
A combination of aortic valve steno-sis and incompetence is usually relatedto rheumatic heart valve disease but can
also be due to bicuspid aortic valve oraging. In either case, as the valve becomesdeformed, narrowed, and stenotic,the leaflets no longer come together. Notonly is the blood obstructed as it tries toleave the left ventricle, but when the leftventricle relaxes, some of the bloodleaks back into the chamber. Heartvalve surgery may be needed.
Mitral Valve Disease
Mitral Stenosis
Mitral valve stenosis is usuallycaused by rheumatic fever. In thiscondition, the two leaflets of the mitralvalve gradually fuse together, making itdifficult for the blood traveling into theleft atrium from the lungs to passthrough the mitral valve and into the leftventricle. As this condition becomesmore severe, shortness of breath devel-
160
To correct aortic valvestenosis with a porcinevalve, physicians remove
the diseased aorticvalve (above) and sewin a xenograft (below).
The final illustration(above right) shows
the aorta incisionstitched closed.
DiseasedAortic Valve
Pig Valve
RejoinedAorta
with NewValve

ops because blood backs up into thelungs. Fatigue is also a common symp-tom. Also, some babies are born withan abnormally narrowed mitral valve
In some cases, the patient may coughup blood. (However, there are many othercauses of coughing up blood [hemoptysis].)Depending on the degree of mitral valvestenosis, some form of intervention may benecessary. This might involve using a bal-loon catheter to dilate the stenotic mitralvalve and could also mean heart surgery.
Mitral Valve Incompetence
Mitral valve incompetence, which isalso referred to as mitral valve regurgita-tion or insufficiency, occurs when the twoleaflets of the mitral valve no longer meeteach other when the valve is closed.Because the leaflets do not meet, some ofthe blood that should be ejected into theaorta is squeezed through the faulty mitral
valve backwards into the left atrium as theleft ventricle contracts. The resulting high-er pressure in the left atrium sendsblood backwards into the lungs.
This condition can cause shortness ofbreath and fatigue. The heart also has towork harder because some of the bloodthat’s being pumped is going backwards.As a result, the left ventricle will dilate andbegin to fail, adding to the shortness ofbreath. Patients also have swollen ankles.If this problem becomes severe, heartsurgery will most likely be required.
Another condition is called myxoiddegeneration, in which some of the tis-sues in the heart are weakened, and thevalve is prone to incompetence. Thiscondition can affect varying parts of themitral valve. For example, the chordae,which attach the valve to the underlyingmuscles, can rupture (Fig. 10.4). Likewise,the papillary muscles can rupture.Papillary muscle rupture is usually re-lated to a heart attack. This condition re-quires emergency heart surgery.
Mitral Valve Stenosis and Incompetence
As with the aortic valve, the mitralvalve may deform so that it obstructs theflow of blood into the left ventricle andprevents it from closing normally be-cause the two mitral leaflets no longertouch each other. In this condition, thevalve is narrowed and incompetent,sending some of the blood back throughthe deformed valve. Depending on theseverity of this problem, heart surgerymay be required.
Tricuspid Valve Disease
Tricuspid Valve Stenosis
The tricuspid valve may becomestenotic as a result of rheumatic fever, or itmay be narrow at birth (Fig. 10.5). Tricuspidvalve stenosis from rheumatic fever,particularly that which is severe enough
C H A P T E R T E N : H E A R T VA L V E P R O B L E M S
161
Myxoid Degeneration: Degeneration of themiddle layer of tissuein blood vessels andheart valves.
Fig. 10.4: The mitral valve is at-tached to the ventricu-lar wall by chordae. Ifthese rupture, the mi-tral valve becomes in-competent. The sur-geon removes that por-tion of the valve wherethe ruptured chordaeis located (above), thensews the valve togetherand places a support-ing ring (below).
RupturedChordae
RepairedIncision
SupportingRing
Fig. 10.4

S T A T E O F T H E H E A R T
162
Ascites:An abnormal accumu-
lation of serum-likefluid in the abdomen.
Fig. 10.5: This illustration shows
four possible valve dis-orders. The pulmonary
valve (top) suffersfrom congenital steno-
sis. The aortic valve(middle) suffers from
stenosis and incompe-tence resulting fromrheumatic fever. The
tricuspid valve (farright) suffers from
stenosis and incompe-tence. The mitral valve
(near right) suffersfrom incompetence
due to bacterial infec-tion. The growths on
the valve’s surface areclumps of bacteria, and
a hole has been eatenthrough the valve leaflet.
to require heart surgery, is relativelyuncommon.
If the valve is severely stenotic, bloodreturning from the veins to the heart willhave difficulty getting into the right ventri-cle. As a result, the liver may become en-gorged, and fluid can build up in the ab-domen. This fluid buildup is known asascites. The legs and ankles may swell.If there’s a small hole in the heart be-tween the right and the left atrium, someunoxygenated blood may pass throughthis hole, and a patient may appear blue(cyanotic). Heart surgery may be requiredto correct this problem.
Tricuspid Valve Incompetence
Tricuspid valve incompetence is rela-tively common and usually related to di-latation of the tricuspid valve annulus, or
the ring around the tricuspid valve thatanchors the valve. This is commonly re-lated to either long-standing mitral valvedisease or pulmonary arterial and/or pulmonary venous hypertension, mean-ing the pressure in the pulmonary arter-ies and veins is elevated, forcing the rightventricle to work harder.
Over time, the right ventricle en-larges and begins to fail. As it does, theannulus may dilate and cause the tri-cuspid valve to leak blood back into theright atrium, causing similar signs andsymptoms as in tricuspid valve steno-sis (narrowed valve).
During an episode of endocarditis,bacteria or fungi can destroy the leafletsof the tricuspid valve. Depending on theseverity of the condition, heart surgerymay be required, and the valve may berepaired or replaced.
Mitral Valve,Incompetent dueto BacterialEndocarditis
Pulmonary Valve, Congenital Stenosis
Stenotic andIncompetent Aortic Valve
Stenotic andIncompetent
Tricuspid ValveFig. 10.5

C H A P T E R T E N : H E A R T VA L V E P R O B L E M S
Dr. Agustin Arbulu, a heart surgeonat Wayne State University in Detroit, hasshown that when a tricuspid valve is se-verely damaged because of antibiotic-re-sistant infection and the infection is theresult of illicit intravenous drug abuse, agood method of treatment is to removethe infected tricuspid valve and not re-place it. This removes the source of theinfection. If an artificial valve is put in, ittoo will likely become infected since thepatient frequently resumes the illicitdrug use.
Tricuspid Valve Stenosis and Incompetence
This combination is usually related torheumatic heart disease, and the problemis similar to mitral and aortic valveincompetence/stenosis in which the valveis both leaky and narrow. Depending onits severity, this condition may requireheart surgery.
Pulmonary Valve Disease
Pulmonary Valve Stenosis
Pulmonary valve stenosis (narrowing)is most commonly of congenital origin inthe United States (Fig. 10.5). Although itmay occur as a result of rheumatic fever,this is relatively uncommon in the UnitedStates. Pulmonary valve stenosis can betreated with a balloon catheter, which isused to dilate the valve. Sometimes, how-ever, heart valve surgery is needed.
Pulmonary Valve Incompetence
Pulmonary valve leakage (incom-petence) is usually related to abnor-mally high pressure in the pulmonaryarteries or pulmonary veins. This, inturn, may be due to a problem with thepulmonary blood vessels or with theaortic or mitral valves. In this case, theright ventricle may fail, causing thepulmonary valve annulus to dilate and
leak. The pulmonary artery may alsodilate and cause the valve to leak. It isuncommon to need heart surgery forthis condition.
The pulmonary valve may also becomeincompetent as a result of bacterial endo-carditis. Sometimes, the valve may needto be replaced.
Heart Valve Balloon Dilatation
When heart valves, including the pul-monary valve, the mitral valve, or even theaortic valve, are narrow (stenotic), they cansometimes be dilated with a balloon. Theballoon is attached to a catheter and in-serted into the bloodstream through anartery or vein. After the catheter is placedwithin the narrowed heart valve, the bal-loon is inflated, which dilates the valve. Ifthe valve is both stenotic and incompetent,however, physicians generally do not try todilate the valve with the balloon catheter.Although the obstruction may be relievedto some degree, the valve would likely be-come more incompetent, thus trading onetype of heart valve problem for another.
Mitral valves that are narrowed fromrheumatic fever can sometimes be openedsuccessfully with balloon catheters, simi-larly to the treatment of pulmonary valvestenosis. In fact, Dr. Zoltan Turi, a cardi-ologist at Wayne State University inDetroit, has shown in two randomizedstudies (published in the journal Circulationand The New England Journal of Medicine)that in certain patients, balloon cathetertreatment for rheumatic mitral valve steno-sis yields results that are as good as or bet-ter than surgery.
Balloon catheter therapy for congeni-tal aortic valve stenosis can sometimesbe life saving. This technique can buy timeand delay heart valve surgery in someinfants until they are in better conditionto undergo elective heart valve surgery.
Balloon catheter therapy can also beused for rheumatic aortic stenosis or bi-cuspid aortic stenosis. However, the
163

S T A T E O F T H E H E A R T
longer-term results tend to be unsatis-factory. Aortic valve balloon catheter ther-apy is used in some adult patients whoare desperately ill, perhaps even beingtreated with a mechanical ventilator. It isdesigned to improve their condition anddecrease the risk of the aortic valve oper-ation. It is also sometimes used in pa-tients more than eighty years old whohave numerous other serious medicalproblems, in hopes that their symptomswill improve, even though in most casesthe improvement is short lived.
Heart Valve Surgery Repair versusReplacement
Most heart surgeons believe that if aheart valve can be repaired with the like-lihood of relatively good long-term results,repair should be attempted rather thanvalve replacement. Although many excel-lent artificial heart valves are currentlyavailable, the perfect heart valve substi-tute has yet to be developed. If any oneof the four valves is stenotic, physiciansmay be able to open the closed valve witha scalpel by carefully opening the fusedleaflets, or commissures. This is calledcommissurotomy or valvotomy (Fig. 10.6). Itis most commonly done in patients whorequire heart surgery for congenital pul-monary stenosis and those requiring mi-tral valve surgery for mitral valvestenosis related to rheumatic fever. Theshort-term and long-term results in bothcases are quite good.
For mitral valve incompetence andtricuspid valve incompetence, there arenumerous repair techniques that can beused depending on the circumstances.
Heart Valve Replacement
If the heart valve cannot be re-paired, physicians will most likely rec-ommend heart valve replacement witheither a mechanical heart valve or a tis-sue (biological) heart valve.
When it comes to mechanical heartvalves, some surgeons still use the orig-inal cage-ball valves. These valves have agood, long-term track record. Some pa-tients have had the cage-ball valves formore than thirty years.
The newer mechanical heart valvesare made from carbon. They tend to below profile so they take up less space andhave better flow characteristics. Thesetypes of valves have been put on pulseduplicators with which accelerated wearcan be tested. Tests of one hundred sim-ulated years of use show very little actu-al wear on the valve. These tests indicatethat, in most cases, satisfactory functioncan be expected for many years.
164
Fig. 10.6: During a valvotomy, a surgeon can treat
a narrowed valve bywidening the valve with
a scalpel (above). Thecorrected valve (below)
will allow blood tomove through morefreely and thereforeplace less stress on
the heart. Fig. 10.6

C H A P T E R T E N : H E A R T VA L V E P R O B L E M S
The biggest disadvantage of the me-chanical heart valves is that most pa-tients need to take an anticoagulant,also referred to as a “blood thinner,” toprevent blood clots from forming on thevalve itself. The most common anticoag-ulant is coumadin, otherwise known aswarfarin. Patients who take coumadinneed to get their blood tested periodical-ly. When coumadin treatment is firststarted, the blood is tested every day ortwo, but after a few weeks, it is usuallytested every couple of months to makesure the level of anticoagulation is ap-propriate. If the anticoagulation is toogreat, the patient is more prone to devel-op bleeding problems, which can includebleeding into the stomach, intestines,brain, or kidneys. A person with bleed-ing ulcers would be prone to bleed more.If you were cut, you would have aproblem with abnormal bleeding. Thecoumadin treatment can be reversed inan emergency situation if necessary.
Another problem related to mechani-cal heart valves is blood clots that occureven if the anticoagulation level is appro-priate. These clots can form on or near theartificial valve and travel to various partsof the body, causing strokes and otherproblems. Fortunately, the incidence ofthis is small. It is somewhat more com-mon in patients who have mechanical ar-tificial heart valves than in those with tis-sue heart valves. The biggest advantage of
the mechanical valves is that the currentmodels tend not to wear out.
Both mechanical and tissue heartvalves are more prone to become infectedthan your own normal heart valves.Currently, the most commonly used tis-sue valves come from a pig. The pig valvecan be used to replace any of the fourhuman heart valves. Another type of tis-sue valve is made from the pericardium ofa cow. The results with this valve seemcomparable to those with the pig valve.
The problem with tissue valves is thatthey wear out, which occurs more rapidlyin children and young adults. The degen-eration of these tissue valves is slower inolder adults, particularly those more thanseventy years of age. In patients less thanseventy years old, about 15 percent to 30percent of the tissue valves wear out with-in ten years. The rate of valve deteriorationincreases greatly after the valves havebeen in place for ten years.
Another type of tissue valve is the aor-tic homograft valve, which is used to re-place the aortic valve and sometimes thepulmonary valve. These valves come froma human donor and are removed right
165
Above: A modern, bi-leaflet, low-profile heartvalve made of carbon.
Left: A tilting disc me-chanical heart valvemade by Medtronic.

S T A T E O F T H E H E A R T
after death. Like pig valves, they tend notto last as long in younger people and lastlonger in patients fifty years of age orolder. The incidence of blood clot problemswith these tissue valves is generally quitelow. Most patients with tissue valves donot need to be anticoagulated.
Some patients who undergo aorticvalve replacement have a procedure calledthe Ross Procedure. During this opera-tion, patients have their own pulmonary
valve removed and used to replace theaortic valve. The pulmonary valve is thenreplaced with a human pulmonary or aor-tic valve homograft. This seems to be aparticularly good operation for children, inwhom the valve may grow with the child.Some groups have reported excellent re-sults with this procedure, whereas othersare less enthusiastic about it. Centersthat have considerable experience withthe Ross Procedure tend to have thebest results.
The Heart Valve Operation
Many aspects of heart valve operationsare similar to those of other forms of car-diac surgery. The patient is usually admit-ted to the hospital the morning of the op-eration. The procedure is performed aftergeneral anesthesia is induced. Operationsare performed through a midline chest in-cision (from the base of the neck to theupper abdomen) through the breastbone,although some surgeons prefer to use otherincisions depending on the circumstances.
The pericardium is opened, and thepatient is connected to the heart-lungmachine. The heart or a major blood ves-sel is opened, and the heart valve is re-paired or replaced. After that, the heartor blood vessel is sutured closed, and thepatient is disconnected from the heart-lung machine. The chest incisions areclosed in layers with stitches, and theskin is closed with stitches or staples.
Afterward, the patient is transferredfrom the operating room to the intensivecare unit (ICU). At this point, a mechan-ical respirator is breathing for him orher, and will for at least several hours.The patient is typically in the ICU for aday or two. Discharge from the hospitaltypically occurs from four days to ninedays after the surgery.
When the patient returns home, he orshe will be able to go out for walks. It willbe about a month before driving a car isrecommended. By then, many patients are
166
A pig valve without a stent (inset) can be
used to correct variousabnormalities of the
aortic valve.

C H A P T E R T E N : H E A R T VA L V E P R O B L E M S
walking a mile or two a day. Some cardiol-ogists feel that all of their patients shouldbe enrolled in a cardiac rehabilitation pro-gram, whereas others feel that only moresedentary people need a formal rehabilita-tion program. Professional athletes mightbe able to resume normal strenuousactivities, depending on a number ofvariables, about three months after heartsurgery. Cardiologists determine whenand what level of activity can be re-sumed and when it can be started afterheart surgery.
The midline incision (through thebreast bone) that is currently used formost valve replacement surgeries is notvery painful for most people. Patients areusually discharged with a prescriptionfor a relatively mild pain medicine.
So how many heart valves can be re-placed in the same person? The aorticvalve is the most commonly replaced. Thesecond most commonly replaced is themitral valve. Third is replacement of boththe aortic and mitral valves during the
same operation. Sometimes the aortic, mi-tral, and tricuspid valves are all replacedat the same time. More typically, the aor-tic and mitral valves are replaced, and thetricuspid valve is repaired. This treatmentis usually reserved for long-standing aor-tic and mitral valve disease in which thetricuspid valve has become incompetentas a result of the other two valves causingstress on the right ventricle and tricuspidvalve. Occasionally, the mitral and tricus-pid valves are both replaced. Rarely, theaortic and tricuspid valves are replaced atthe same time.
I am aware of one patient, a younggirl, who had stenosis of all four valvesrelated to rheumatic fever. All four valveswere opened at surgery with a commis-surotomy procedure. She was alive andwell one year later. I am also aware ofone patient who underwent replacementof all four valves. This was at the MayoClinic. The patient survived for aboutsix months and then died of unrelatedcomplications.
167

168
ROBOTIC HEART VALVE SURGERY:IS THIS REALITY OR MYTH?
ByRandolph Chitwood, M.D.
Cardiothoracic SurgeonProfessor and Chairman, Department of Surgery
East Carolina University School of MedicineGreenville, North Carolina
IN THE LAST SEVERALyears, the public has becomeentranced by the idea of
reducing both the psychologicaland the physical effects of heartsurgery. Minimally invasive tech-niques have recently emerged asone way to speed patient recov-ery, reduce discomfort, and re-duce the economic impact ofthese expensive operations.Unfortunately, despite rapid,multiple advances in other surgi-cal specialties and interventionalcardiology, heart surgery haslagged behind in the developmentof less invasive methods.
Cardiac surgeons have beenafraid of accepting the added riskof performing major heart oper-ations through tiny incisionsand obtaining less-than-excellentresults. In fact, our surgical teach-ers, many of whom are featuredin this book, taught that expo-sure of the entire heart and greatvessels was central to performingsafe, technically excellent surgery.
In the early 1960s, it was afeat to have patients survive evensimple heart valve operations.
Most patients were at the endstages of their cardiac disease,the heart-lung machines werecrude, and heart valve prostheseswere in early evolution. Moreover,these were uncharted waters forsurgeons regarding techniqueand postoperative care. In spiteof these impediments, pioneersin heart surgery took the neces-sary first steps.
Years later, minimally inva-sive cardiac surgery is emergingwith no less skepticism andcriticism. However, simultaneousnear-meteoric advances have been
made in both Europe and theUnited States. After just threeyears, we are beginning to seeimprovements in our specialty andwhat may be a renaissance in car-diac care. Evolving technology hasafforded us opportunities to makethese changes safely.
Many of us think it is time tomake bold steps in cardiac care.Advances in heart-lung perfusion,surgical mini-cameras (endo-scopes), “smart” instruments androbotics, and cardiac cellular pro-tection have catapulted us to abetter position. Moreover, stan-dard heart operations are saferthan ever. For example, both coro-nary bypass and heart valve oper-ations in uncomplicated cases canbe performed with only a 1 per-cent to 2 percent operative mor-tality, even in the elderly.
Why should we try to improveon these outstanding results?Technology has allowed some sur-geons to envision ways to im-prove heart operations. Still, mostheart surgeons perform opera-tions through large breastboneincisions. Patient recovery is slow

169
R O B O T I C H E A R T VA L V E S U R G E R Y : I S T H I S R E A L I T Y O R M Y T H ?
because of muscular and skele-tal tissue trauma rather thanthe operation on the heart itself.Thus, surgeons are now askingthemselves: Can quality coronarybypass and valve operations bedone through tiny access portsusing endoscopes and minia-turized instruments, and evenrobotic assistance?
Minimally Invasive Valve Surgery— The Beginnings
The trek to a completelyclosed chest heart operation maybe compared to a Mt. Everest as-cent. There are multiple levels ofaccomplishment established be-fore reaching the summit. Thissurgical trek began at a “basecamp” that was the conventionalvalve operation with a breast-bone incision. All new proce-dures are being compared tothis gold standard.
Although widespread adop-tion has been slow, many cardiacsurgeons already have learned touse less invasive techniques toreplace and repair valves and placecoronary artery grafts. They cando this safely, with demonstratedexpertise and improved outcomes.
The first minimally invasivevalve operations were done in1996 through smaller incisionsyet under direct vision. Clinicalresults in the last three years havebeen excellent. Dr. Delos Cosgroveof the Cleveland Clinic Foundationand Dr. Lawrence Cohn ofBrigham and Women’s Hospitalpioneered much of this early work.
Operative results have beenexcellent in hundreds of patientswho had both aortic and mitralvalves repaired and replacedthrough smaller chest incisions
(four to five inches) with a 1 per-cent operative mortality.
Others have followed andshown that these results can bereproduced in many local hospi-tals. Using more expensive aor-tic balloon occlusion devices,namely the Port-Access™ device(Heartport, Inc., Redwood City,California), the Stanford Universityand New York University groupshave operated through evensmaller chest incisions (3 inchesto 3.5 inches) to repair and re-place mitral valves effectivelywith a 2 percent mortality.
Video-Assisted Minimally InvasiveMitral Valve Surgery:
Trekking to Robotic Heart Surgery
Once these valve operations,performed under direct visionthrough a smaller incision, wereaccomplished, the door was
opened to the use of tiny camerasfor secondary vision. This allowedsurgeons to operate through evensmaller incisions. Ultimately andhopefully, physicians will be ableto perform true closed-chestcardiac surgery by using a mon-itor or head-mounted visual dis-play to see the inside of thechest. The use of computer-assistance and robotic tech-niques may one day allow a com-pletely endoscopic heart valve op-eration. These devices continueto evolve at a very rapid pace.
Dr. Alain Carpentier in Parisperformed the first video-assistedmitral valve operation in February1996. Three months later, ourgroup at East Carolina Universityperformed the first videoscopicmitral valve replacement in NorthAmerica. Since then, more thanninety minimally invasive video-assisted mitral valve replace-
Using robotic technology, surgeons are able to perform heart operationsthrough much smaller incisions in the side of the chest.

170
ments or repairs have been doneat our center. Details of the re-sults in the first thirty-one pa-tients were published, as wasthe technique.
To perform these operations,an even smaller (2.5-inch) chestincision was used, and intracar-diac instrument manipulationwas performed using videoscop-ic vision. There were no operativedeaths, and midterm results wereexcellent. Both transfusion andICU requirements were markedlyless than with the breastbone in-cision, and the length of stay av-eraged 3.5 days. There have beenfew major complications. Eachvideoscopic operation is now per-formed with an effort similar tothat in a conventional operation.Overseas doctors have also pio-neered videoscopic mitral valvesurgery, working through tiny,two-inch incisions, and have hadexcellent results in more thantwo hundred patients.
Robotics: The Final Ascent
Surgeons and patients review-ing this emerging area of heartsurgery will have to judge whetherwidespread, truly endoscopic oreven robotic (computer-assisted)valve operations are possible. Inthe past, three-dimensional visionwas not possible unless the sur-geon viewed the operation withhis or her eyes. Recently, how-ever, new video devices havebeen developed that are very
promising. Using both three-di-mensional Zeiss™ and Vista™systems, doctors in Germany,as well as our group, have per-formed “video-directed,” or com-pletely endoscopic, mitral valvereplacements.
Each surgeon worked witheither a head-mounted display ora television monitor. Currently,three-dimensional intracardiaccameras are somewhat large (10to 15 mm); however these areevolving rapidly toward the 5-mmsize. These three-dimensionaldevices give us a look inside theheart as never seen before — thesmall papillary muscles look liketrees, the fine chords to the valve
now appear as ropes, and thevalve itself looks like a parachuterather than a small (about 1.5-inch) potato-chip-like structure.
Many of us have worked withevolving robotic methods. Earlycosts have been great and video-dexterity expertise difficult todevelop. However, it is clear thatnew technology will allow voice-activated camera manipulation,scaling and tremor eliminationof instrument motion, cameratracking of the operative field,flexible intracardiac articulationof small instrument tips, andthree-dimensional vision.
During computer-assistedor robotic cardiac surgery, the
R O B O T I C H E A R T VA L V E S U R G E R Y : I S T H I S R E A L I T Y O R M Y T H ?
The robotic operating room at theLeipzig Heart Center in Germany.
Inset: The wrist-like robotic instrument is capable of intricate movement.

171
R O B O T I C H E A R T VA L V E S U R G E R Y : I S T H I S R E A L I T Y O R M Y T H ?
surgeon moves the instrumentwithin the chest by manipulatinginstrument-like electronic sen-sors. The robotic unit requires a“master” and a “slave” unit. Thesurgeon sits at a master consolelocated a distance from thepatient, and the slave unit iswithin the patient’s chest. Thephysician’s hand and wristmotions are translated directlyto the robotic instruments,which are inserted through thechest wall.
There are two effector com-ponents common to all surgicalrobotic systems. Advanced com-puter technology has enableddirect translation of electronic datafrom the master console into finemechanical motion in the slaveunit. The camera tracks the oper-ative site, and instrument tips arecontrolled by complex slidinginternal cables within mechani-cal arms.
Unfortunately, complexinstruments can be made onlyso small and still function well.Moreover, mechanical limita-tions and chest anatomic varia-tions have caused intrathoracicinstrument conflicts (much likesword fighting). Despite theselimitations, massive progress inrobotic cardiac surgery has beenmade in the last two years. Todate, we have done thirty mitraloperations using the Aesop™(Computer Motion, Inc., SantaBarbara, California) voice-ac-tivated camera-directing robot.This device has made the oper-ation easier for surgeons and re-duced operative time but hasnot decreased costs or improved
operative quality. However, it hasprovided the first step in ro-botic cardiac surgery.
On May 21, 1998, Carpentierand Dr. Didier Loulmet atBroussais Hospital in Paris suc-cessfully performed the world’sfirst truly robotic-assisted heartoperations in mitral valve pa-tients. In these cases, intracar-diac “wrist” instruments weremanipulated from outside thechest. The surgeon, sitting at amaster console, “drove” the in-strument in the heart using theslave robot. This device providestrue telemanipulation of a vari-ety of coronary and valve instru-ments within the chest.
One week later, Dr. Friedrich-Wilhelm Mohr’s group in Leipzigsuccessfully performed five mi-tral repairs using the samesystem. This latter group hasperformed more than twenty mi-tral repairs totally endoscopi-cally using a DaVinci™ device(Intuitive Surgical, Inc., MountainView, California).
Recently, I had the opportu-nity to be the first American toperform a true robotic mitral valverepair while working in Leipzigwith Mohr’s group. The operativefacility and translated hand move-ments with this device are superb;however, other challenges surelyawait us. The Leipzig group hasbrought the field of robotic coro-nary and valve surgery from fan-tasy to reality and to the forefront.
Other groups in France,Belgium, and Germany are begin-ning to apply this device to car-diac operations. To date, both theDaVinci™ and Zeus™ surgical
robots await FDA approval in theUnited States. Early results usingthese true robots appear to par-allel those of both prior videoscop-ic operations and of convention-al mitral valve operations.
Thus, within the last threeyears, cardiac minimally invasivesurgery has developed from aconcept to a working applica-tion. The current enthusiasm ofsurgeons worldwide, combinedwith rapid technological develop-ment and communications, ap-pears to be moving us towardeven less traumatic and maybe“microinvasive” cardiac operations.Yes, the spirit of innovation forbetter patient care is in the air!Yet many techniques are evolv-ing so rapidly that large multipa-tient series have not been done.However, data from series of pa-tients are beginning to be col-lected, and analysis of these datashould be enlightening.
Surgeons always will askthemselves: Is this new methodreally offering our patients re-duced trauma, fewer complica-tions, more rapid recovery, andbetter long-term results, com-pared with traditional opera-tions? A healthy mix of scientif-ic skepticism and wisdom mustbe exercised. The public must askpenetrating questions regardingefficacy and outcomes. Yes —some of us believe that micro-invasive reconstructive cardiacsurgery will be a reality, and ro-botic cardiac surgery will proba-bly be a reality rather than a fan-tasy. But the trek up Mt. Everestis not over — we have just ar-rived at a new base camp.

172
MINIMALLY INVASIVEHEART VALVE SURGERY
ByDelos M. Cosgrove, M.D.Chief of Cardiothoracic Surgery
andA. Marc Gillinov, M.D.
Staff Cardiothoracic Surgery
The Cleveland Clinic FoundationCleveland, Ohio
THOUSANDS OF PEOPLEbenefit from heart valverepair or replacement every
year. Heart valves require surgi-cal correction when they becomenarrowed (stenotic) or when theybegin to leak (become regurgitant).Although there are four heartvalves, surgery is most oftennecessary for diseases of themitral valve and the aorticvalve. When these two valvesbecome severely dysfunctionaland cause symptoms, valve re-pair or replacement is indicat-ed; there are no effective non-surgical treatments.
Traditionally, during heartvalve surgery with the heart-lung machine, the heart wasapproached through a longincision down the middle of thechest. The breastbone, or ster-num, was split in two, allowingaccess to the entire heart andthe great vessels. This incisionis called a median sternotomy.Recently, however, it has becomeapparent that heart valve surgerycan be accomplished through afar smaller incision.
When a patient needs valvu-lar heart surgery and does notrequire a coronary artery bypassgraft, a variety of smaller inci-sions allow the mitral and aorticvalves to be seen. These incisionsgenerally fall into two categories:thoracotomy, or an incision inthe side of the chest between theribs, and partial sternotomy, oran incision in the middle of thechest that divides only a portionof the sternum. Using thesesmaller incisions to accomplishheart valve surgery is called min-imally invasive heart valvesurgery. At the Cleveland ClinicFoundation, heart valve surgeryis performed through a 2.5-inchto 3.5-inch skin incision and apartial upper sternotomy. A largeportion of the sternum is left in-tact, decreasing postoperativepain and hastening healing.
Since 1996, we have per-formed more than one thousandheart valve operations using thisincision. The average patient agewas fifty-six years, and the old-est patient was eighty-four yearsold. More than six hundred
Delos M. Cosgrove, M.D.
A. Marc Gillinov, M.D.

173
M I N I M A L L Y I N VA S I V E H E A R T VA L V E S U R G E R Y
patients had mitral valve surgery,and nearly 90 percent of thesepatients had mitral valve repair.Three hundred patients hadaortic valve procedures, in-cluding valve replacements witha variety of artificial valves anda considerable number of aorticvalve repairs.
Overall, operative mortali-ty was less than 1 percent, andwound infections occurred inonly 0.3 percent of patients.
The average length of stay inintensive care was one day, andthe average hospital stay wassix days.
These results demonstratethat minimally invasive heart valvesurgery can be performed verysafely with a low risk of compli-cations. There are many advan-tages to minimally invasive heartvalve surgery. There is less bloodloss, and patients generally reportless postoperative discomfort.
Less time is spent in the inten-sive care unit and in the hospi-tal, and recovery at home tendsto be rapid.
The next decade is likely tobring even more ingenious ap-proaches, including roboticallyassisted cardiac valve surgery.These advances promise refine-ments to minimally invasiveheart valve surgery, further re-ducing hospital stays and in-creasing patient satisfaction.

174
TISSUE ENGINEERING OFCARDIAC VALVES AND ARTERIES
ByJohn Mayer, M.D.
Professor of SurgeryHarvard Medical School
Senior Associate in Cardiac SurgeryBoston Children’s Hospital
Boston, Massachusetts
T ISSUE ENGINEERINGunites engineering andbiology in an attempt to
develop replacement tissues.Normal tissues draw much oftheir strength and flexibilityfrom specialized proteins andpolysaccharide-protein com-plexes that are produced bytheir cells. Although it has beenpossible to grow specific types ofcells in the lab for some time, itis difficult to cause these cells toorganize into the complex struc-tures that are found in normaltissues or to produce normalstructural proteins in an orga-nized fashion.
To overcome this challenge,we are attempting to “grow” heartvalves and large arteries byusing biodegradable polymersas temporary scaffolds. Thesepolymer scaffolds provide thestructure and stability neces-sary for tissues to develop.Ideally, these scaffolds woulddegrade as the cells producenormal structural proteins andbegin to replicate normal, orga-nized tissue structures.
Diseases of the heart valvesand large arteries account forabout sixty thousand surgerieseach year in the United States,including many replacementsurgeries with synthetic substi-tutes. Ideally, any valve or arterysubstitute would function likethe normal valve or artery, allow-ing blood to pass through it with-out narrowing or leakage, but itwould also have the followingcharacteristics: 1) durability, 2)growth potential, 3) compatibilitywith blood so that blood clots will
not form on its surface, and 4) re-sistance to infection.
None of the currently avail-able devices constructed fromprosthetic or biological materi-als meets these criteria. Ourconcept, however, was to devel-op new valves or arteries fromindividual cells in the hope thatthese new tissues will have thesedesirable characteristics. Thepotential for growth is of partic-ular importance to children withmalformed or diseased valvesor arteries.
Several projects have beenundertaken in our laboratory toconstruct a heart valve leafletand large arteries by using tissueengineering. We used cells fromnormal arteries that could be re-moved and separated into thevarious cell components. Wefound it was important to usethe animal’s own tissue as thesource of the cells, thereby elim-inating the possibility of immunerejection once the tissues werereimplanted. The cells were “ex-panded” in cultures by allowingthem to divide, and then suspen-

175
T I S S U E E N G I N E E R I N G O F C A R D I A C VA L V E S A N D A R T E R I E S
sions of the cells were mixed withthe polymer scaffolds. The cell-polymer constructs were then in-cubated in culture for severalmore days before they were im-planted as a valve replacementor an artery replacement. Valveleaflets and segments of large ar-teries functioned well for up tofour months without structuralfailure or formation of blood clotson their surfaces. Importantly,when these structures were im-planted into growing animals,they demonstrated growth. Thetissues appeared to have rela-tively normal structure, and theyproduced the normal matrixproteins.
Despite these encouragingresults, many questions remainto be resolved.
♥ First, all of these exper-iments have been carriedout in animals, and it re-mains to be determined ifhuman cells could be usedto develop tissues in thesame way.
♥ Second, the polymer usedas the scaffold in theseinitial experiments is stiff,biodegradable polymer thatmay or may not have ac-ceptable strength and flex-ibility (“handling”) charac-teristics while still provid-ing a hospitable environ-
ment for the cells to de-velop into tissues.
♥ Third, the ideal source ofthe cells for the developing“tissues” has not beendetermined. In patients,it would be preferable touse veins rather than arter-ies as the initial source ofthe cells because veins aremore plentiful and theirremoval does not compro-mise blood supply to nor-mal tissues. We have someevidence that heart valvesdeveloped by using cellsfrom the skin do not func-tion as well as those de-veloped with cells from thewall of the artery, but veinwall cells seem to workreasonably well.
♥ Fourth, because all of ourexperiments have beencarried out in immaturegrowing animals, it is notclear whether the cells thatare used to form these “tis-sues” must be from imma-ture animals. There is somereason to believe that fetalcells would be preferable.Because it is now possibleto diagnose many forms ofcongenital heart diseasewhile the embryo is still inutero, one might imagineusing fetal cells to developreplacement valves or ar-
teries while gestation iscontinuing. At birth, thesereplacement valves or ar-teries could be ready to beimplanted.
♥ Fifth, it is not clear whetherthe “tissues” should beimplanted while they arestill dependent on thepolymer scaffold for theirphysical integrity or if theyshould be allowed to devel-op further in culture be-fore implantation intothe body. One of our cur-rent ideas is that if thedeveloping tissues are sub-jected to physical forcesand/or chemical signalswhile in the laboratory, itmay be possible to guidetheir development furtherbefore implantation into thebody. Our understandingof how these developingtissues will respond to anynumber of physical andchemical signals remainsvery limited.
Tissue engineering is one newapproach to solving the problemof creating replacement tissuesfor use as heart valves or arteries.Although initial animal studieshave been encouraging, numer-ous questions must be resolvedbefore we embark on clinical tri-als in humans.

176
DIET PILLS ANDHEART VALVE PROBLEMS
ByLarry Stephenson, M.D.
ON OCTOBER 8, 1999, AN article appeared on the
front page of The New YorkTimes with the headline, “Fen-Phen Maker to Pay Billions inSettlement of Diet-Injury Cases.”This article is hopefully the finalchapter in the story of the pop-ular diet drugs, which were re-moved from the market afterthey were linked to heart valveproblems. According to TheNew York Times, anybody witha pill-related heart valve in-jury could receive as much as$1.5 million.
“Some six million peopletook the diet drugs, Pondimin,American Home Products brandname for fenfluramine, the‘fen’ in Fen-Phen, and Redux,a similar drug.
“The drugs were hailed earli-er in the decade as miracle pillsfor obesity, as an alternative topure diet and exercise. Diet cen-ters actively promoted the pillsto the obese and even to peoplewho wanted to lose a fewpounds. In 1996, doctors wrote
eighteen million prescriptions forthe two drugs.
“But in September 1997, thecompany removed the drugs fromthe market at the request of theFood and Drug Administrationafter studies linked them to heartvalve damage.”
What is the specific prob-lem caused by these drugs?
In the August 28, 1997, issueof The New England Journal ofMedicine, a group of doctors fromthe Mayo Clinic reported on twen-ty-four women who had taken
Fen-Phen and had no previoushistory of heart disease. Thesewomen were evaluated at an av-erage of one year after their initialtreatment with Fen-Phen. All hadleaky heart valves. Two requiredsurgical repair of their mitralvalves, two, replacement of theirmitral valves, and one patient, re-placement of her aortic valve andmitral valve and repair of her tri-cuspid valve.
In their report, the doctorsfrom the Mayo Clinic concluded,“These cases arouse concern thattherapy may be associated withvalvular heart disease. Candidatesfor fenfluramine-phenteraminetherapy should be informedabout serious potential adverseeffects, including pulmonaryhypertension and valvularheart disease.”
The following year, anotherarticle appeared in The NewEngland Journal of Medicine bya group of doctors fromMinneapolis who had studiedmore than two hundred pa-tients who had received Fen-Phen therapy compared with a

177
D I E T P I L L S A N D H E A R T VA L V E P R O B L E M S
group who had not. They foundthat a greater percentage of thepatients receiving Fen-Phenhad cardiac valve abnormali-ties than those who had nottaken the drug.
In the same issue of The NewEngland Journal of Medicine, agroup of doctors from GeorgetownUniversity in Washington, D.C.,reported on a study of patientstaking dexfenfluramine (a relateddrug) in which they found a smallincrease in the prevalence ofaortic and mitral valve leakage.
Over the next year, twelveadditional articles and letters tothe editors appeared in The NewEngland Journal of Medicine deal-ing with a possible link betweenappetite suppressants and valvu-lar heart disease as well as a re-lation between high blood pres-sure in the pulmonary arteriesand these drugs. There was con-siderable controversy amongthese doctors as to what thechances were of developing heartvalve disease problems after Fen-Phen therapy.
Perhaps Dr. Richard B.Devereux from New York Hospital-
Cornell Medical Center summedit up best by stating:
“What advice should we offerpatients based on these findings?
“First, all patients who receivefenfluramine or dexfenfluramineshould be examined clinically.Echocardiography should berecommended for those whohave a heart murmur or otherevidence of valvular disease,as well as those who receivedone of the drugs for three or moremonths or at high doses....
“Second, standard prophy-laxis against endocarditis (heartinfections) should be recom-mended to patients with a heartmurmur, those with ‘silent’moderate or severe regurgi-tation ... and those with mildregurgitation....
“Third, in view of the delayin recognizing the associationbetween the use of appetitesuppressants and cardiac-valve abnormalities, cautionshould be urged in the long-term use of other agents thatact on serotonergic mecha-nisms, albeit by different
pathways [meaning drugsthat have similarities in theway they work].
“Finally, it is important toremember that in patientswho meet the FDA criteria forcardiac-valve abnormalitieson echocardiography per-formed soon after the discon-tinuation of appetite suppres-sants, there is a possibility(ranging from as low as 5 per-cent to as high as 67 percent)that the abnormality is a nat-urally occurring phenomenonand not a consequence ofdrug use.”
The bottom line is, anyonewho has taken these drugsshould be checked by their doc-tor for symptoms of heart valvedisease and/or pulmonary arteryhypertension. If symptoms arepresent, a cardiologist will do afurther evaluation.
The good news at this pointis that the majority of patients whohave taken these drugs seem tobe doing quite well and havetrivial, if any, heart problems.