Embed Size (px)
Citation preview

Coronary Artery Disease
Terminal QRS Distortion in ST Elevation
Myocardial Infarction as a Prediction of
Mortality: Systematic Review and Meta-Analysis
Narut Prasitlumkum,1
Natee Sirinvaravong,2
Nath Limpruttidham,1
Pattara Rattanawong,1,4
Elysse Tom,1
Chanavuth Kanitsoraphan,3
Pakawat Chongsathidkiet4,5
and Thosaporn Boondarikpornpant6
Background: Terminal QRS distortion reflects advanced stage and large myocardial infarction predisposing the
heart to adverse outcomes. Recent studies suggest that terminal QRS distortion is associated with morbidity and
mortality in ST elevation myocardial infarction (STEMI). However, a systematic review and meta-analysis of the
literature have not been done.
Objective: We assessed the association between terminal QRS distortion in patients with STEMI and mortality by a
systematic review of the literature and a meta-analysis.
Methods: We comprehensively searched the databases of MEDLINE and EMBASE from inception to September
2017. Included studies were published prospective or retrospective cohort studies that compared all-cause mortality
in subjects with STEMI with QRS distortion versus those without QRS distortion. Data from each study were combined
using the random-effects, generic inverse variance method of DerSimonian and Laird to calculate risk ratios and
95% confidence intervals.
Results: Fifteen studies from January 1993 to May 2015 were included in this meta-analysis involving 7,479
subjects with STEMI (2,906 QRS distortion and 4,573 non-QRS distortion). QRS distortion was associated with
increased mortality (pooled risk ratio = 1.81, 95% confidence interval: 1.37-2.40, p < 0.000, I2
= 41.6%). Considering
the introduction of clopidogrel in 2004, we performed subgroup analyses before and after 2004, and the associated
with higher mortality was still present (before 2004, RR 1.75, 95% CI 1.08-2.82, p = 0.022, I2
= 66.1%; after 2004, RR
1.96, 95% CI 1.44-2.65, p < 0.001, I2
= 0%).
Conclusions: Terminal QRS distortion increased all-cause mortality by 81%. Our study suggests that terminal QRS
distortion is an important tool to assess the risk in patients with STEMI.
Key Words: Mortality � ST elevation � Terminal QRS distortion
INTRODUCTION
Electrocardiography (ECG) is essential in the diagno-
sis of ST-segment elevation myocardial infarction (STEMI),
and it is also used as a prognostic tool for patients with
STEMI.1
Sclarovsky and colleagues developed a grading
system of pre-reperfusion ECG findings in STEMI called
Sclarovsky-Birnbaum’s Grades of Ischemia Score (grade
1: tall peaked T waves in the involved leads, grade 2: ab-
normal T waves and ST elevation, grade 3: abnormal T
waves, ST elevation, and distortion of the terminal por-
445 Acta Cardiol Sin 2019;35:445�458
Original Article doi: 10.6515/ACS.201909_35(5).20180909A
Acta Cardiol Sin 2019;35:445�458
Received: February 23, 2018 Accepted: September 9, 20181University of Hawaii Internal Medicine Residency Program, Honolulu,
HI;2Department of Medicine, Einstein Medical Center, Philadelphia,
PA, USA;3Faculty of Medicine Siriraj Hospital;
4Faculty of Medicine
Ramathibodi Hospital, Mahidol University, Bangkok, Thailand;5Department of Pathology, Duke University Medical Center, Durham,
North Carolina, USA;6Department of Medicine, Faculty of Medicine,
Chulalongkorn University, Bangkok, Thailand.
Corresponding author: Dr. Narut Prasitlumkum, University of Hawaii
Internal Medicine Residency Program, No. 801, South Street, APT
4501, Honolulu, Hawaii, 96813, USA. Tel: (808)-859-3848; E-mail:

tion of the QRS).2,3
Grade 3 ischemia, which is character-
ized by distortion of the terminal portion of the QRS
complexes, has been shown to be a sign of more severe
ischemia and poorer prognosis in STEMI.4,5
The presence
of Grade 3 ischemia has been reported in 19 to 53% of
STEMI patients.6
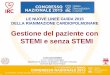
Terminal QRS distortion is defined as a
decrease in S-wave amplitude in leads with a terminal S
wave and an elevation of the J point > 50% of the height
of the R wave amplitude in leads with qR configuration.7
Terminal QRS distortion is not observed in early repo-
larization, and thus it can be useful in distinguishing
STEMI from early repolarization.8
The presence of termi-
nal QRS distortion in STEMI has been associated with a
larger infarct size, impaired myocardial salvage, lower
epicardial reperfusion success, low left ventricular ejec-
tion fraction (LVEF), reperfusion injury, anterior location
of myocardial infarction, higher risk of re-infarction, and
mortality.6,9-11
Terminal QRS distortion has been associ-
ated with increased mortality in STEMI in several stud-
ies.9,10,12,13
However, most of these studies had small co-
horts, and some of the results regarding mortality were
conflicting.14-16
In this study, we aimed to assess the as-
sociation between the presence of terminal QRS distor-
tion in STEMI and mortality in a systematic review and
meta-analysis.
METHODS
Search strategy
Two investigators (NL and CK) independently sear-
ched for published studies indexed in MEDLINE and
EMBASE databases from inception to September 2017
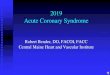
using a search strategy (Figure 1) that included the terms
“terminal QRS distortion”, “grade 3 ischemia”, “ST eleva-
tion”, and “mortality”. Only English language publica-
tions were included. A manual search for additional per-
tinent studies and review articles using references from
the retrieved articles was also completed.
The eligibility criteria included
(1) Studies reporting the incidence of in-hospital mortal-
ity, major cardiovascular events (MACEs), and rein-
farction in patients with STEMI with and without ter-
minal QRS distortion.
(2) Relative risk, hazard ratio, odds ratio, incidence ratio,
or standardized incidence ratio with 95% confidence
interval or sufficient raw data for the calculation were
provided.
(3) Patients with STEMI who did not have terminal QRS
distortion were used as controls.
Study eligibility was independently determined by
two investigators (NL and CK), and differences were re-
solved by mutual consensus. The Newcastle-Ottawa qua-
lity assessment scale was used to evaluate each study in
three domains: recruitment and selection of the partici-
pants, similarity, and comparability between the groups,
and ascertainment of the outcome of interest among
cohort studies.17
Definitions
Terminal QRS distortion was defined according to
QRS morphologies described in each study. STEMI was
defined as typical chest pain with the presence of ST
segment elevation of � 2 mm in 2 contiguous leads or as
defined in each study at the time of STEMI diagnosis.
In-hospital mortality was defined as deaths within the
follow-up time specified in each study. MACEs were de-
Acta Cardiol Sin 2019;35:445�458 446
Narut Prasitlumkum et al.
Figure 1. Search methodology and selection process.

fined as a combination of all-cause mortality readmis-
sions for new congestive heart failure, recurrent infarc-
tion, or as defined in each study (Figure 2).
Data extraction
A standardized data collection form was used to ob-
tain the following information from all studies: title of
the study, name of the first author, year of study, year of
publication, country of origin, number of participants,
demographic data of the participants, method used to
identify cases and controls, method used to diagnose
the outcomes of interest (all-cause mortality), average
duration of follow-up, adjusted and unadjusted risk ra-
tios and their corresponding 95% confidence intervals,
and a list of confounders that were adjusted for multi-
variate analysis.
To ensure accuracy, all investigators independently
performed this data extraction process. Any data dis-
crepancies were resolved by referring back to the origi-
nal articles.
Statistical analysis
Meta-analysis of the included cohort was performed
using a random-effect model with the generic inverse
variance method of DerSimonian and Laird.18
The heter-
ogeneity of effect size estimates across these studies
was quantified using the I2
statistic and Q statistic. For
the Q statistic, substantial heterogeneity was defined as
p < 0.10. The I2
statistic ranges in value from 0 to 100%
(I2
< 25%, low heterogeneity; I2
= 25%-50%, moderate
heterogeneity; and I2
> 50%, substantial heterogeneity).19
Sensitivity analysis was performed to assess the influ-
ence of the individual studies on the overall results by
omitting one study at a time. Publication bias was as-
sessed using a funnel plot and Egger’s regression test20
(p < 0.05 was considered to be significant). All data anal-
yses were performed using Stata SE 14.1 software from
StataCorp LP.
RESULTS
Description of the included studies
Our search strategy yielded 28 potentially relevant
articles (6 articles from EMBASE and 22 articles from
MEDLINE). After excluding 2 duplicate articles, 26 arti-
cles underwent title and abstract review. Four were ex-
cluded at this stage since one was written in Turkish, one
was an abstract presentation, and the other two were ir-
relevant topics, leaving 22 articles for full-length article
review. Six studies were excluded because there was no
outcome of interest, and one was excluded because the
same population was used. Therefore, 7 retrospective
and 8 prospective cohort studies with 2,906 patients
with QRS distortion and 4,573 without QRS distortion
were included in this meta-analysis. The clinical charac-
teristics are described in Table 1.
Quality assessment of the included studies
The Newcastle-Ottawa scale (0 to 9) was used to
evaluate the included studies on 3 domains: selection,
comparability, and outcomes. Higher scores represent
higher study quality. The score of each study ranged
from 7 to 9, which reflected high quality of the included
studies (Supplementary Table 1). Detailed evaluations of
the studies are presented in Table 1.
Meta-analysis results
A total of 15 studies (8 prospective,3,9,12-14,16,21,22
7
retrospective5,6,10,23-26
) with 7,479 participants were in-
cluded in the meta-analysis. The incidence of QRS dis-
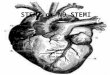
tortion ranged from 19-52%. There was an association
between terminal QRS distortion and all-cause mortality
in the patients with STEMI [relative risk (RR) 1.81; 95%
confidence interval (CI) 1.37-2.40, p < 0.001)] with mod-
erate heterogeneity (I2
= 41.6%) (Figure 3A). We per-
447 Acta Cardiol Sin 2019;35:445�458
Terminal QRS and Mortality
Figure 2. Electrocardiogram showing QRS distortion. An emergence of
J point � 50% of the R wave amplitude in a lead with qR configuration
(III, aVF).





formed subgroup analysis for in-hospital mortality, which
still showed a strong correlation with QRS distortion
(RR 2.05; 95% CI 1.37-3.07, p = 0.001) with high hetero-
geneity (I2
= 55.0%) (Figure 3B). Further subgroup an-
alysis of non-hospital mortality also demonstrated a sub-
stantial association with QRS distortion (RR 1.64; 95%
CI 1.17-2.29, p = 0.004) with no heterogeneity (I2
= 0%)
(Figure 3B). Furthermore, we performed subgroup an-
alysis of patients with anterior infarction and inferior
infarction, which showed that QRS distortion was sig-
nificantly associated with all-cause mortality only in
the anterior group (RR 2.84 95% CI 1.73-4.65, p < 0.001
with I2
= 42.7%) (Supplementary Figure 1). The inferior
infarction group also showed increased all-cause mor-
tality, but the difference was not significant (RR 2.10
95% CI 0.73-6.08, p = 0.169 with I2
= 83.3%) (Supple-
mentary Figure 1).
There have been advancements in treatment such
as the introduction of clopidogrel and major changes in
percutaneous coronary intervention (PCI) and stents
from alternatives to first line from the ACC/AHA Guide-
lines in 2004.27
Since advances in these treatment meth-
ods may have affected outcomes, we conducted other
subgroup analyses, which we subdivided by year (before
or after 2004) and technique [thrombolysis or percu-
taneous transluminal coronary angioplasty (PTCA) and
thrombolysis or stenting]. The results showed a substan-
tial association between QRS distortion and mortality in
both subgroups before 2004 (RR 1.75 CI 1.08-2.82, p =
0.022 with I2
= 66.1%) and after 2004 (RR 1.96 CI 1.44-
2.65, p < 0.001 with I2
= 0%) (Supplementary Figure 2).
There was also a significant association between QRS
distortion and mortality in the thrombolysis (RR 2.94 CI
1.61-5.37, p < 0.001 with I2
= 53.4%) and stenting (RR
1.89 CI 1.39-2.57, p < 0.001 with I2
= 0.0%) groups. How-
ever, there was no difference between the PTCA and
thrombolysis group (RR 1.06 95% CI 0.63-1.80, p = 0.820
with I2
= 39.0%) (Supplementary Figure 3).
We took into account other exploratory outcomes
including MACEs, reinfarction, ventricular arrhythmia
and shock. The analysis of the other outcomes demon-
strated a statistically significant increased risk of MACEs
(RR 1.69; 95% CI 1.31-2.18, p < 0.001 ) and reinfarction
(RR 1.72; 95% CI 1.33-2.24, p < 0.001 ) (Supplementary
Figure 4). There was also an increased rate of shock (RR
1.72; 95% CI 0.91-3.25, p = 0.062) (Supplementary Fig-
ure 5) and ventricular arrhythmia (RR 1.83 95% CI 0.77-
4.63, p = 0.179) (Supplementary Figure 6) in the pati-
Acta Cardiol Sin 2019;35:445�458 452
Narut Prasitlumkum et al.
Figure 3. (A) Forest plot of studies comparing mortality rate in pati-
ents with and without QRS distortion. Horizontal lines represent the 95%
CIs with marker size reflecting the statistical weight of the study using
random-effects model. A diamond data marker represents the overall
adjusted odds ratio (OR) and 95% CI for the outcome of interest. (B) For-
est plot of studies comparing in-hospital and nonhospital mortality rate
in patients with and without QRS distortion. Horizontal lines represent the
95% CIs with marker size reflecting the statistical weight of the study us-
ing random-effects model. A diamond data marker represents the over-
all adjusted odds ratio (OR) and 95% CI for the outcome of interest.
A
B

ents with QRS distortion. In particular, statistical hetero-
geneity was not found (I2
= 0%) in the secondary analyses
of MACEs and reinfarction. Nevertheless, there was sub-
stantial heterogeneity in the analysis of shock (I2
= 55.4%)
and ventricular arrhythmia (I2
= 85.9%). No publication
bias was found in any of these analyses in either the
funnel plot or Egger’s test (Figure 4). Sensitivity analysis
to explore heterogeneity showed no significant change
in our findings after omitting each study.
DISCUSSION
General
In this study, the incidence of QRS distortion ranged
from 19-52% in the STEMI patients before undergoing
either PCI or thrombolysis. Our meta-analysis demon-
strated that the presence of terminal QRS distortion was
associated with increased combined all-cause mortality,
including in-hospital mortality, 30-day mortality, and
mortality within 1 year. Additionally, our exploratory
analysis suggested associations between the presence
of QRS distortion and increased risks of reinfarction,
MACEs, ventricular arrhythmia, and shock.
Regardless of the technique and changes in treat-
ment according to the ACC/AHA Guidelines in 2004,27
the risk of all-cause mortality was still statistically sig-
nificant among the patients with QRS distortion in both
the stenting and thrombolysis groups. However, there
was no difference in mortality between the PTCA and
thrombolysis groups, which could be explained by the
difference in treatment techniques.
Is QRS distortion still useful in the current era?
In addition to recent shifts in acute myocardial in-
farction treatment, many ECG parameters including ter-
minal QRS distortion have been investigated for their
prognostic ability. For example, Valle-Caballero et al.28
reported that QRS distortion was associated with a
higher risk, extent and size of myocardial infarction.
Likewise, Tanrivedi et al.29
demonstrated that a combi-
nation of QRS distortion and fragmented QRS was corre-
lated with higher mortality, poor LVEF, high levels of car-
diac biomarkers and low rate of ST resolution after PCI.
We believe that these ECG parameters are still useful
and applicable to any circumstance, especially in the
setting of limited resources. In addition, our subgroup
analyses showed that terminal QRS distortion was still
associated with an equivalently increased risk of all-
cause mortality both before and after 2004.
QRS distortion equivalency to other contemporary
modalities
QRS distortion is thought to be an old-fashioned
marker compared to other modern modalities including
signal averaged ECG and cardiac imaging. However, it is
still a useful tool to stratify the risk of morbidity and
mortality among STEMI patients. Recently, signal aver-
aged ECG has been recognized as a promising tool for
prognostication. However, the predictive value com-
pared to QRS distortion may not be as equivalent as it
should. Bauer et al.30
demonstrated that ventricular late
potentials (VLPs) were not predictive of long-term seri-
ous cardiac events. VLPs were also of limited use for very
long-term risk stratification according to Shturman et
al.31
Despite these unsatisfactory results, VLPs are par-
ticularly recommended to determine the risk of devel-
oping sustained ventricular tachycardia in patients re-
covering from myocardial infarction without bundle
branch block.32
Regarding cardiovascular imaging, various modalities
have been developed to help identify high-risk patients
with STEMI. LVEF from echocardiography is currently the
most important risk stratification tool, strongly recom-
mended by the ACCF/AHA STEMI guidelines and ESC
STEMI guidelines for further therapy including implant-
able cardioverter-defibrillator (ICD) implantation and
453 Acta Cardiol Sin 2019;35:445�458
Terminal QRS and Mortality
Figure 4. Funnel plot of QRS distortion and mortality. Circles represent
published studies.

biventricular pacing.33,34
This could be inferred that ec-
hocardiography is superior to ECG parameters. However,
measurements during acute myocardial infarction can
be misleading, since the LVEF may significantly improve
after optimal revascularization. In addition, cardiac mag-
netic resonance imaging (MRI) has been shown to be a
promising modality which may play a greater role in the
cardiovascular field in the future. Eitel et al.35
conducted
a prospective multicenter study to evaluate the prog-
nostic impact of cardiac MRI, and found that only micro-
vascular obstructions were associated with an up to
3-fold risk of MACEs. Another study36
suggested that in-
farct characteristics in cardiac MRI could provide addi-
tional prognostic value, especially mortality. Despite
the high predictive value, more studies are required to
verify the results since there were few participants,
stringent inclusion and exclusion criteria, need of re-
sourceful setting, and the generalizability of the results
is still questionable. Taken together, ECG is still the best
method given its convenience, simplicity and cost-effec-
tiveness.
Pathophysiology
Many previous studies have demonstrated that the
presence of QRS distortion or grade 3 ischemia is associ-
ated with increased morbidity and mortality.3,9,12,13,21,25
The mechanism of terminal QRS distortion has yet to be
clearly elucidated. Myocardial ischemia has been shown
to lead to delayed conduction in Purkinje fibers.37
This
decreases the degree of cancellation, which causes an
increase in R-wave and decrease in S-wave amplitudes
on surface ECG.38
Since Purkinje cells are less sensitive
to ischemia than contracting myocytes,39
an alteration
at the terminal portion of the QRS complex, also known
as terminal QRS distortion, will occur in the setting of
profound ischemia.40
Based on these possible explana-
tions, an association has also been reported between
terminal QRS distortion and evidence of the significant
extent of ischemia, supported by single-photon emis-
sion computed tomography (SPECT) findings,41
and less
myocardial salvage as well as a rapid progression of ne-
crosis.42
Previous studies have shown that terminal QRS
distortion is associated with a more advanced stage of
myocardial infarction, higher in-hospital mortality, higher
risk of reinfarction, and poor prognosis of STEMI.43
With
respect to ventricular arrhythmogenesis, the relation-
ship between QRS distortion and ventricular arrhythmia
is still unclear. Taken together, we hypothesize that QRS
distortion is an indicator of poor ventricular substrate.
Interestingly, our results showed that QRS distortion was
only associated with higher overall mortality in the sub-
jects with anterior infarction but not with inferior in-
farction, which is consistent with a previous study by
Fakhei et al. that described the applicability of ECG indi-
ces of severity, and showed that acuteness of myocar-
dial ischemia is only confined to anterior myocardial in-
farction.44
To the best of our knowledge, this is the first meta-
analysis to examine the association between QRS dis-
tortion and increased mortality in STEMI patients un-
dergoing either thrombolysis or PCI. We believe that
QRS distortion may be integrated as part of a risk strati-
fication tool in STEMI. Given our exploratory findings,
further studies are warranted to determine the associa-
tion between QRS distortion and MACEs, reinfarction
and shock.
Limitations
There are several limitations to this meta-analysis.
Studies with different methodologies and populations
were included as well as variations in QRS definition in
each study. The primary outcome of our study was a
combination of all-cause mortality, which was defined
differently in each study, from in-hospital mortality to
one-year mortality. Our analysis only showed the out-
come at 1 year at most from the beginning of each study.
Therefore, we could not analyze the long-term outcomes.
The proportion of patients with anterior infarction was
different in each study, which could have impacted the
incidence of mortality, shock, reinfarction, ventricular
arrhythmia and MACEs in patients with QRS distortion.
Nevertheless, we performed subgroup analysis between
anterior and inferior infarction groups, which suggested
that the location of infarction may have affected the
outcome. Additionally, differences in follow-up time be-
tween studies may have resulted in a differences in the
incidence of adverse outcomes. These factors may have
introduced potential sources of moderate heterogeneity
in our study. Nonetheless, we used sensitivity analysis
methods in the random-effects model and found no dif-
ference in the imputed risk ratio and its 95% confidence
interval.
Acta Cardiol Sin 2019;35:445�458 454
Narut Prasitlumkum et al.

CONCLUSIONS
In conclusion, our meta-analysis demonstrated an
association between terminal QRS distortion and mor-
tality in patients with STEMI undergoing PCI or throm-
bolysis. Terminal QRS distortion should be added as an
additional tool for risk stratification in STEMI patients.
Our findings suggest that further research is warranted
to determine the utility of QRS distortion as an indicator
of high-risk STEMI.
FINANCIAL SUPPORT
None.
ACKNOWLEDGEMENT
We would like to thank Elysse Tom, MD., for critical
reading.
CONFLICT OF INTEREST
None to declare.
AUTHOR CONTRIBUTION
Narut Prasitlumkum, conception design, data inter-
pretation, draft manuscript, corresponding; Natee Sirin-
varavong, data acquisition, draft manuscript; Nath Lim-
pruttidham, data acquisition, data interpretation; Cha-
navuth Kanitsoraphan, data acquisition, draft manu-
script; Elysse Tom, draft manuscript; Pattara Rattana-
wong, data acquisition, statistical analysis; Pakawat
Chongsathidkiet, data acquisition; Thosaporn Boonda-
rikpornpant, data acquisition.
REFERENCES
1. Bren GB, Wasserman AG, Ross AM. The electrocardiogram in
patients undergoing thrombolysis for myocardial infarction.
Circulation 1987;76:II18-24.
2. Sclarovsky S, Mager A, Kusniec J, et al. Electrocardiographic clas-
sification of acute myocardial ischemia. Isr J Med Sci 1990;26:
525-31.
3. Birnbaum Y, Sclarovsky S, Blum A, et al. Prognostic significance of
the initial electrocardiographic pattern in a first acute anterior
wall myocardial infarction. Chest 1993;103:1681-7.
4. Birnbaum Y, Sclarovsky S. The grades of ischemia on the pres-
enting electrocardiogram of patients with ST elevation acute
myocardial infarction. J Electrocardiol 2001;34 Suppl:17-26.
5. Birnbaum Y, Kloner RA, Sclarovsky S, et al., Distortion of the ter-
minal portion of the QRS on the admission electrocardiogram in
acute myocardial infarction and correlation with infarct size and
long-term prognosis (Thrombolysis in Myocardial Infarction 4
Trial). Am J Cardiol 1996;78:396-403.
6. Rommel KP, Badarnih H, Desch S, et al. QRS complex distortion
(Grade 3 ischaemia) as a predictor of myocardial damage as-
sessed by cardiac magnetic resonance imaging and clinical prog-
nosis in patients with ST-elevation myocardial infarction. Eur
Heart J Cardiovasc Imaging 2016;17:194-202.
7. Nikus K, Birnbaum Y, Eskola M, et al. Updated electrocardio-
graphic classification of acute coronary syndromes. Curr Cardiol
Rev 2014;10:229-36.
8. Lee DH, Walsh B, Smith SW. Terminal QRS distortion is present in
anterior myocardial infarction but absent in early repolarization.
Am J Emerg Med 2016;34:2182-5.
9. Mulay DV, Mukhedkar SM. Prognostic significance of the dis-
tortion of terminal portion of QRS complex on admission elec-
trocardiogram in ST segment elevation myocardial infarction.
Indian Heart J 2013;65:671-7.
10. Birnbaum Y, Herz I, Sclarovsky S, et al. Prognostic significance of
the admission electrocardiogram in acute myocardial infarction.
J Am Coll Cardiol 1996;27:1128-32.
11. Lee CW, Hong MK, Yang HS, et al. Determinants and prognostic
implications of terminal QRS complex distortion in patients
treated with primary angioplasty for acute myocardial infarction.
Am J Cardiol 2001;88:210-3.
12. Postma S, Heestermans T, Ten Berg JW, et al. Predictors and out-
come of grade 3 ischemia in patients with ST-segment elevation
myocardial infarction undergoing primary percutaneous coro-
nary intervention. J Electrocardiol 2011;44:516-22.
13. Sejersten M, Birnbaum Y, Ripa RS, et al. Influences of electro-
cardiographic ischaemia grades and symptom duration on out-
comes in patients with acute myocardial infarction treated with
thrombolysis versus primary percutaneous coronary interven-
tion: results from the DANAMI-2 trial. Heart 2006;92:1577-82.
14. Garcia-Rubira JC, Garcia-Borbolla R, Nunez-Gil I, et al. Distortion
of the terminal portion of the QRS is predictor of shock after
primary percutaneous coronary intervention for acute myocar-
dial infarction. Int J Cardiol 2008;130:241-5.
15. Garcia-Rubira JC, Molano F, Trujillo F, et al. A new classification of
lower infarcts with important prognostic significance. Rev Port
Cardiol 1996;15:793-7, 772.
16. Hasdai D, Sclarovsky S, Solodky A, et al. Prognostic significance of
the initial electrocardiographic pattern in patients with inferior
455 Acta Cardiol Sin 2019;35:445�458
Terminal QRS and Mortality

wall acute myocardial infarction. Clin Cardiol 1996;19:31-6.
17. Stang A. Critical evaluation of the Newcastle-Ottawa scale for the
assessment of the quality of nonrandomized studies in meta-
analyses. Eur J Epidemiol 2010;25:603-5.
18. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control
Clin Trials 1986;7:177-88.
19. Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsis-
tency in meta-analyses. BMJ 2003;327:557-60.
20. Sterne JA, Egger M. Funnel plots for detecting bias in meta-analysis:
guidelines on choice of axis. J Clin Epidemiol 2001;54:1046-55.
21. Garcia-Rubira JC, Perez-Leal I, Garcia-Martinez JT, et al. The initial
electrocardiogram pattern is a strong predictor of outcome in
acute myocardial infarction. Int J Cardiol 1995;51:301-5.
22. Wolak A, Yaroslavtsev S, Amit G, et al. Grade 3 ischemia on the admis-
sion electrocardiogram predicts failure of ST resolution and of ade-
quate flow restoration after primary percutaneous coronary inter-
vention for acute myocardial infarction. Am Heart J 2007;153:410-7.
23. Birnbaum Y, Goodman S, Barr A, et al. Comparison of primary
coronary angioplasty versus thrombolysis in patients with ST-
segment elevation acute myocardial infarction and grade II and
grade III myocardial ischemia on the enrollment electrocardio-
gram. Am J Cardiol 2001;88:842-7.
24. McGehee JT, Rangasetty UC, Atar S, et al. Grade 3 ischemia on
admission electrocardiogram and chest pain duration predict
failure of ST-segment resolution after primary percutaneous
coronary intervention for acute myocardial infarction. J Elec-
trocardiol 2007;40:26-33.
25. Tanriverdi Z, Dursun H, Simsek MA, et al. The predictive value of
fragmented QRS and QRS distortion for high-risk patients with
STEMI and for the reperfusion success. Ann Noninvasive Elec-
trocardiol 2015;20:578-85.
26. Zalenski RJ, Grzybowski M, Ross MA, et al. ECG scores for a triage
of patients with acute myocardial infarction transported by the
emergency medical system. J Electrocardiol 2000;33 Suppl:245-9.
27. Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines
for the management of patients with ST-elevation myocardial
infarction--executive summary. A report of the American Col-
lege of Cardiology/American Heart Association Task Force on
Practice Guidelines (Writing Committee to revise the 1999 guide-
lines for the management of patients with acute myocardial
infarction). J Am Coll Cardiol 2004;44:671-719.
28. Valle-Caballero MJ, Fernandez-Jimenez R, Diaz-Munoz R, et al.
QRS distortion in pre-reperfusion electrocardiogram is a bedside
predictor of large myocardium at risk and infarct size (a ME-
TOCARD-CNIC trial substudy). Int J Cardiol 2016;202:666-73.
29. Tanriverdi Z, Colluoglu T, Unal B, et al. The prognostic value of the
combined use of QRS distortion and fragmented QRS in patients
with acute STEMI undergoing primary percutaneous coronary
intervention. J Electrocardiol 2018;51:210-7.
30. Bauer A, Guzik P, Barthel P, et al. Reduced prognostic power of
ventricular late potentials in post-infarction patients of the re-
perfusion era. Eur Heart J 2005;26:755-61.
31. Shturman A, Vardi S, Bickel A, et al. Ventricular late potentials
immediately post ST-elevation myocardial infarction, and very
long-term mortality. Isr Med Assoc J 2017;19:246-50.
32. Breithardt G, Cain ME, el-Sherif N, et al. Standards for analysis of
ventricular late potentials using high-resolution or signal-aver-
aged electrocardiography. A statement by a Task Force Commit-
tee of the European Society of Cardiology, the American Heart
Association, and the American College of Cardiology. Circulation
1991;83:1481-8.
33. O'Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guide-
line for the management of ST-elevation myocardial infarction:
executive summary: a report of the American College of Car-
diology Foundation/American Heart Association Task Force on
Practice Guidelines. Circulation 2013;127:529-55.
34. Task Force on the management of ST-segment elevation acute
myocardial infarction of the European Society of Cardiology (ESC),
Steg PG, James SK, et al. ESC Guidelines for the management of
acute myocardial infarction in patients presenting with ST-seg-
ment elevation. Eur Heart J 2012;33:2569-619.
35. Eitel I, de Waha S, Wohrle J, et al. Comprehensive prognosis
assessment by CMR imaging after ST-segment elevation myo-
cardial infarction. J Am Coll Cardiol 2014;64:1217-26.
36. Yan AT, Shayne AJ, Brown KA, et al. Characterization of the peri-
infarct zone by contrast-enhanced cardiac magnetic resonance
imaging is a powerful predictor of post-myocardial infarction
mortality. Circulation 2006;114:32-9.
37. Lewis CT, Naumann DN, Crombie N, et al. Prehospital point-of-
care lactate following trauma: a systematic review. J Trauma
Acute Care Surg 2016;81:748-55.
38. Holland RP, Brooks H. The QRS complex during myocardial is-
chemia. An experimental analysis in the porcine heart. J Clin In-
vest 1976;57:541-50.
39. Dehaan RL. Differentiation of the atrioventricular conducting
system of the heart. Circulation 1961;24:458-70.
40. Spekhorst H, SippensGroenewegen A, David GK, et al. Body sur-
face mapping during percutaneous transluminal coronary angio-
plasty. QRS changes indicating regional myocardial conduction
delay. Circulation 1990;81:840-9.
41. Yang HS, Lee CW, Hong MK, et al. Terminal QRS complex distor-
tion on the admission electrocardiogram in anterior acute myo-
cardial infarction and association with residual flow and infarct
size after primary angioplasty. Korean J Intern Med 2005;20:21-5.
42. Billgren T, Maynard C, Christian TF, et al. Grade 3 ischemia on the
admission electrocardiogram predicts rapid progression of ne-
crosis over time and less myocardial salvage by primary angio-
plasty. J Electrocardiol 2005;38:187-94.
43. Birnbaum Y, Herz I, Sclarovsky S, et al. Admission clinical and
electrocardiographic characteristics predicting an increased risk
for early reinfarction after thrombolytic therapy. Am Heart J
1998;135:805-12.
44. Fakhri Y, Sejersten M, Schoos MM, et al. Electrocardiographic
scores of severity and acuteness of myocardial ischemia predict
myocardial salvage in patients with anterior ST-segment ele-
vation myocardial infarction. J Electrocardiol 2018;51:195-202.
Acta Cardiol Sin 2019;35:445�458 456
Narut Prasitlumkum et al.

457 Acta Cardiol Sin 2019;35:445�458
Terminal QRS and Mortality
SUPPLEMENT
Supplementary Figure 1. Forest plot of studies comparing anterior ver-
sus inferior infarction and overall mortality in patients with and without
QRS distortion. Horizontal lines represent the 95% CIs with marker size
reflecting the statistical weight of the study using random-effects
model. A diamond data marker represents the overall adjusted odds ra-
tio (OR) and 95% CI for the outcome of interest.
Supplementary Figure 2. Forest plot of studies comparing period and
overall mortality in patients with and without QRS distortion. Horizontal
lines represent the 95% CIs with marker size reflecting the statistical
weight of the study using random-effects model. A diamond data
marker represents the overall adjusted odds ratio (OR) and 95% CI for
the outcome of interest.
Supplement Table 1. Newcastle-Ottawa quality assessment scale of included studies in meta-analysis
Selection Comparability Outcome
Study Represent-ativeness
Selectionof the non-
exposedcohort
Ascertainmentof exposure
Endpointnot present
at start
Comparability(Confounding)
Assessmentof outcome
Follow-upduration
Adequacyfollow-up
Totalscore
Birnbaum (1995) * * * * ** * * * 9Birnbaum (1993) * * * * * * * 7Birnbaum (2001) * * * * ** * * * 9Birnbaum (1996) * * * * ** * * * 9Mulay (2013) * * * * * * * * 8Garcia-Rubira (1995) * * * * * * * * 8Garcia-Rubira (2007) * * * * ** * * * 9Hasdai (1996) * * * * * * * * 8Mcgehee (2007) * * * * ** * * * 9Postma (2011) * * * * ** * * * 9Rommel (2015) * * * * ** * * * 9Sejersten (2006) * * * * ** * * * 9Tanriverdi (2015) * * * * * * * * 8Wolak (2007) * * * * ** * * * 9Zalenski (2000) * * * ** * * 7
Notes: The Newcastle-Ottawa scale uses a star system (0 to 9) to evaluate included studies on 3 domains: selection, comparability,and outcomes. Star (*) = item presents. Maximum 1 star (*) for selection and outcome components and 2 stars (**) forcomparability components. Higher scores represent higher study quality.

Acta Cardiol Sin 2019;35:445�458 458
Narut Prasitlumkum et al.
Supplementary Figure 4. Forest plot of studies comparing reinfarction
rate and MACE in patients with and without QRS distortion. Horizontal
lines represent the 95% CIs with marker size reflecting the statistical
weight of the study using random-effects model. A diamond data mar-
ker represents the overall adjusted odds ratio (OR) and 95% CI for the
outcome of interest.
Supplementary Figure 5. Forest plot of studies comparing shock rate
in patients with and without QRS distortion. Horizontal lines represent the
95% CIs with marker size reflecting the statistical weight of the study us-
ing random-effects model. A diamond data marker represents the over-
all adjusted odds ratio (OR) and 95% CI for the outcome of interest.
Supplementary Figure 6. Forest plot of studies comparing QRS distor-
tion and fatal arrhythmia. Horizontal lines represent the 95% CIs with
marker size reflecting the statistical weight of the study using random-
effects model. A diamond data marker represents the overall adjusted
odds ratio (OR) and 95% CI for the outcome of interest.
Supplementary Figure 3. Forest plot of studies comparing technique
and overall mortality in patients with and without QRS distortion. Hori-
zontal lines represent the 95% CIs with marker size reflecting the statis-
tical weight of the study using random-effects model. A diamond data
marker represents the overall adjusted odds ratio (OR) and 95% CI for
the outcome of interest.