Embed Size (px)
Citation preview
Case report
Coronary microcirculation in effortischemia: the roar of the rabbit
Paola Capozza and Enrico OrsiniCardiovascular Medicine Division, Cardiac and Thoracic Department, University of Pisa, Pisa, Italy
Correspondence: Paola Capozza, Cardiovascular Medicine Division,Cardiac and Thoracic Department, Via Paradisa 2, 56124 Pisa, Italy.
Tel: +39 050 995307; fax: +39 050 995308; e-mail: [email protected]
Abstract
A 71-year-old man was admitted to our department with a history of effort angina, positive exercise stresstest, and single photon emission computed tomography (SPECT) results indicative of reversible schemiain the left anterior descending artery (LAD) territory. Coronary angiography showed no significantatherosclerotic lesions in either right or left coronary arteries. However, a relevant slow flow in the LADartery was detected. In a traditional interpretation, the SPECT results would be seen as a false positive forcoronary artery disease. In our opinion, the case is instead a true positive for coronary microcirculatorydysfunction. The pathophysiology of myocardial ischemia is not confined to the epicar-dial coronarylevel but globally involves coronary arteries, microcirculation, and myocardium.
Heart Metab. 2011;50:28–31.
Keywords: Coronary angiography, coronary slow flow, myocardial ischemia
History
A 71-year-old man was admitted to our departmentwith a history of effort angina and a diagnosis ofinducible ischemia. As coronary risk factors, he hadessential hypertension and dyslipidemia.
In 2008, because of effort angina, he performed atreadmill exercise test that showed a significant ST-segment depression in V4-V6 leads, so he also under-went an exercise single photon emission computedtomography (SPECT). The examination detected areversible perfu-sion defect in the inferior septum witha normal left ventricular ejection fraction (LVEF).Coronary angiography showed a 50% diameter ste-nosis in the mid left anterior descending coronaryartery (LAD); this lesion was not treated with angio-plasty because the fractional flow reserve FFR)resulted in the normal range (0.87).
In October 2010, a few weeks before admission, thepatient underwent a second exercise est for the per-sistence of effort angina despite medical treatment;the test was positive for nducible ischemia. He alsorepeated an exercise SPECT: the electrocardiogram
28
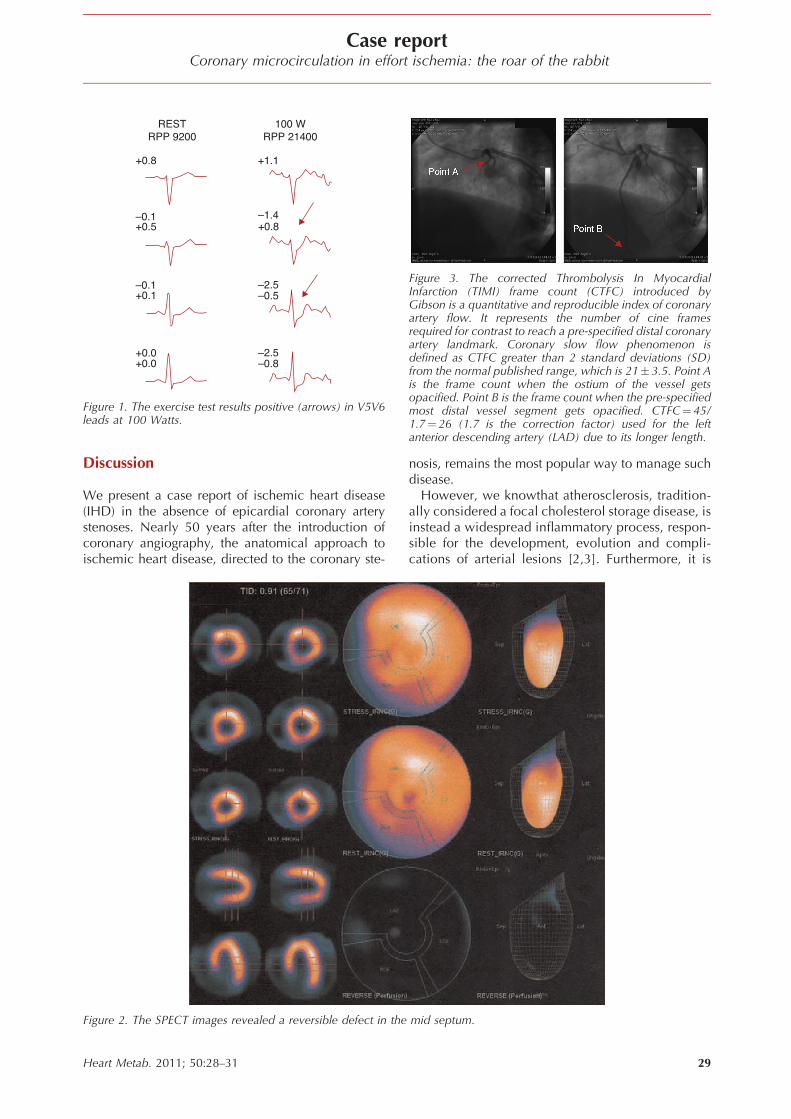
(ECG) showed a downsloping ST-segment depression(2 mm) in V5-V6 leads (Figure 1), while the perfusionscan documented a moderate and reversible defect inthe mid septum (Figure 2).
When the patient was admitted, he had a normalsinus rhythm. Echocardiography showed normal leftventricular volumes, wall thickness and LVEF (58%),without wall-motion abnormali-ies. Due to his highFramingham Risk Score and the positive SPECTresults, we decided to perform a second coronaryangiography. Coronary arteriography showed theabsence of lesions in the right coronary and circum-flex arteries and a non-critical stenosis (<50% luminaldiameter narrowing) in the mid-LAD (Figure 3). Themost important finding was the delayed progression ofthe contrast agent in the whole LAD artery thatresulted in a Thrombolysis In Myocardial Infarction(TIMI) 2 flow (45 frames to opacify the distal vascu-lature, against 5 beats for the right coronary andcircumflex artery). The corrected TIMI frame countfor LAD (CTFC) was 26 [1]. The left ventriculographyconfirmed the absence of wall-motion abnormalitiesand a good LVEF (56%).
Heart Metab. 2011; 50:28–31
Case reportCoronary microcirculation in effort ischemia: the roar of the rabbit
+0.8 +1.1
–1.4
–2.5
+0.8
–0.8–2.5
–0.5
–0.1
–0.1+0.1
+0.0+0.0
+0.5
RESTRPP 9200
100 WRPP 21400
Figure 1. The exercise test results positive (arrows) in V5V6leads at 100 Watts.
Figure 3. The corrected Thrombolysis In MyocardialInfarction (TIMI) frame count (CTFC) introduced byGibson is a quantitative and reproducible index of coronaryartery flow. It represents the number of cine framesrequired for contrast to reach a pre-specified distal coronaryartery landmark. Coronary slow flow phenomenon isdefined as CTFC greater than 2 standard deviations (SD)from the normal published range, which is 21�3.5. Point Ais the frame count when the ostium of the vessel getsopacified. Point B is the frame count when the pre-specifiedmost distal vessel segment gets opacified. CTFC¼45/1.7¼ 26 (1.7 is the correction factor) used for the leftanterior descending artery (LAD) due to its longer length.
Discussion
We present a case report of ischemic heart disease(IHD) in the absence of epicardial coronary arterystenoses. Nearly 50 years after the introduction ofcoronary angiography, the anatomical approach toischemic heart disease, directed to the coronary ste-
Figure 2. The SPECT images revealed a reversible defect in the
Heart Metab. 2011; 50:28–31
nosis, remains the most popular way to manage suchdisease.
However, we knowthat atherosclerosis, tradition-ally considered a focal cholesterol storage disease, isinstead a widespread inflammatory process, respon-sible for the development, evolution and compli-cations of arterial lesions [2,3]. Furthermore, it is
mid septum.
29

Case reportPaola Capozza and Enrico Orsini
now recognized that most atherosclerotic lesionsgrow outward, so a consistent burden of atheroscle-rosis can exist in the absence of stenoses. Finally, inthe setting of acute coronary syndromes (ACS), Riofolet al demonstrated that vulnerable plaques are pre-sent throughout the coronary tree, regardless of theculprit lesion [4].
In reality, the pathophysiology of ischemic heartdisease is not confined to epicardial coronary stenosis,but is much more complicated and invariablyinvolves both coronary microcirculation and themyocardium.
Several published series have demonstrated that alarge number of patients with symptoms and signs ofischemic heart disease have no stenoses at coronaryangiography. In the setting of ACS, the Global Use ofStrategies to Open Occluded Coronary Arteries inAcute Coronary Syndromes (GUSTO) IIb trial demon-strated in a large cohort that about 30% of patients hadno culprit lesions [5]. The same result was recentlyconfirmed by the Coronary Artery Spasm in PatientsWith Acute Coronary Syndrome (CASPER) study,which also documented that epicardial coronaryvasospasm was responsible of the ACS in the half ofthe cases [6].
As regards stable angina, the Coronary ArterySurgery Study (CASS), involving 21,487 angiograms,showed that 18.8% of patients had non-obstructivecoronary artery disease [7] and, among women, thispercentage raises up to 50%, as documented by theWomen’s Ischemia Syndrome Evaluation (WISE)study [8].
Likoff et al [9] and Kemp [10] reported two studiesin which patients with ST-segment depression or T-wave inversion at rest accentuated such ECG changesduring exercise despite normal coronary angiography.Abnormalities in coronary flow and metabolicresponses to stress were reported over the years byseveral groups, all findings consistent with a micro-vascular etiology for ischemia and symptoms [11,12],the so-called microvascular angina.
The coronary slow-flow phenomenon (CSFP), docu-mented in our case report, is defined as an abnormalcondition in which (micro)vascular resistances areinappropriately high, causing a slow anterograde pro-gression of the contrast medium [13]. CSFP waswidely recognized as a marker of myocardial ische-mia [14]. The overall incidence of CSFP has beenreported as 1 % among patients undergoing coronaryangiography, especially in patients presenting withacute coronary syndromes [15]. In the TIMI-IIIA study,the incidence of CSFP was approximately 4% amongpatients presenting with unstable angina and withoutsignificant epicardial coronary artery disease [16].Myocardial perfusion scintigraphy shows reversibleperfusion abnormalities in 28–75% of patients withCSFP [17,18].
30
Different theories have been postulated about thecause of small-vessel dysfunction, including micro-vascular tone alteration, small-vessel wall thickening[19], patchy fibrosis [20], and impaired endothelialrelease of nitric oxide (NO) [21]. In any case, struc-tural or functional alterations of coronary microcir-culation have been documented in several clinicalconditions, such as stable and unstable angina[22–27]. In these conditions, endothelial and micro-vascular dysfunction play a pathophysiological roleboth in the precipitation and maintenance of myo-cardial ischemia, also in the absence of coronaryatherosclerosis.
The discussion of our case report should focus ontwo main questions. The first issue is whether or notour patient suffered from IHD despite the absence ofcoronary artery disease (CAD). The second isthe significance of a positive stress test in absenceof CAD.
The answer to the first question is undoubtedly yes.Our patient had not only a long history of stable,reproducible, and typical angina on effort but alsounequivocal signs of myocardial ischemia documen-ted by both electrocardiographic and myocardialperfusion markers. The patient had moderate per-fusion defects on stress imaging SPECT. We knowthat, regardless of the diagnostic approach, 5% ormore of ischemic myocardium is an importantmeasure of 2-year risk of death or MI [28].
Regarding the second issue, many stress tests havebeen evaluated to clarify their diagnostic and predic-tive accuracy [29,30]. In our case, the SPECT resultwould be conventionally rated as a false positiveresult for CAD, even in the presence of typical symp-toms and other unequivocal signs of inducible ische-mia. In reality, our case report demonstrates thatexercise stress test and SPECT results must be regardedas a true positive result for coronary microcirculatorydysfunction and microvascular ischemia. Patel et al[31], in a recently published paper, show that,although a positive test is highly predictive of coron-ary obstructions, significant coronary stenoses arepresent in >30% of patients with negative exercisetest, both symptomatic and asymptomatic. Therefore,CAD does not necessarily imply IHD, since ischemicsyndromes often manifest in absence of coronaryatherosclerosis and, vice versa, even a severe coron-ary atherosclerosis frequently occurs in the absence ofdocumentable ischemia.
Conclusion
IHD is a multi-factorial syndrome, with a complexpathophysiology that goes far beyond coronary ste-nosis and involves both coronary microcirculation
and the myocardium.Heart Metab. 2011; 50:28–31
Case reportCoronary microcirculation in effort ischemia: the roar of the rabbit
References
1. Gibson CM, et al. TIMI frame count: a quantitative methodof assessing coronary artery flow. Circulation. 1996;93 (5):879–888.
2. Orsini E, Zito GB. Matching pathophysiology and evidence-based medicine for optimal management of ischemic heartdisease. J Cardiovasc Med (Hagerstown). 2010;11 (6):469–479.
3. Falk E. Pathogenesis of atherosclerosis. J Am Coll Car- diol.2006;47 (8 Suppl):C7–C12.
4. Rioufol G, et al. Multiple atherosclerotic plaque rupture inacute coronary syndrome: a three-vessel intravascular ultra-sound study. Circulation. 2002;106 (7):804–808.
5. Hochman JS, et al. Sex, clinical presentation, and outcome inpatients with acute coronary syndromes. Global Use of Strate-gies to Open Occluded Coronary Arteries in Acute CoronarySyndromes IIb Investigators. N Engl J Med. 1999;341 (4):226–232.
6. Ong P, et al. Coronary artery spasm as a frequent cause ofacute coronary syndrome: The CASPAR (Coronary ArterySpasm in Patients With Acute Coronary Syndrome) Study.J Am Coll Cardiol. 2008;52 (7):523–527.
7. Kemp HG, et al. Seven-year survival of patients with normal ornear normal coronary arteriograms: a CASS registry study.J Am Coll Cardiol. 1986;7 (3):479–483.
8. Pepine CJ, et al. Coronary microvascular reactivity to adeno-sine predicts adverse outcome in women evaluated for sus-pected ischemia results from the National Heart, Lung andBlood Institute WISE (Women’s Ischemia Syndrome Evalua-tion) study. J Am Coll Cardiol. 2010;55 (25):2825–2832.
9. Likoff W, Segal BL, Kasparian H. Paradox of normal selectivecoronary arteriograms in patients considered to have unmis-takable coronary heart disease. N Engl J Med. 1967;276 (19):1063–1066.
10. Kemp HG, Elliott WC, Gorlin R. The anginal syndrome withnormal coronary arteriography. Trans Assoc Am Physicians.1967;80:59–70.
11. Cannon RO 3rd. Chest pain with normal coronary angio-grams. N Engl J Med. 1993;328 (23):1706–1708.
12. Cannon RO 3rd. The Conundrum of Cardiovascular SyndromeX. Cardiol Rev. 1998;6 (4):213–220.
13. Fineschi M, Gori T. Coronary slow flow: description of a new‘‘cardiac Y’’ syndrome. Int J Cardiol. 2009;137 (3):308–310.
14. Goel PK, et al. Slow coronary flow: a distinct angio- graphicsubgroup in syndrome X. Angiology. 2001;52 (8):507–514.
15. Singh S, Kothari SS, Bahl VK. Coronary slow flow phenom-enon: an angiographic curiosity. Indian Heart J. 2004;56(6):613–617.
16. Diver DJ, et al. Clinical and arteriographic characterization ofpatients with unstable angina without critical coronary arterialnarrowing (from the TIMI-IIIA Trial). Am J Cardiol. 1994;74(6):531–537.
Heart Metab. 2011; 50:28–31
17. Cesar LA, et al. Slow coronary run-off in patients with anginapectoris: clinical significance and thallium-201 scinti- graphicstudy. Braz J Med Biol Res. 1996;29 (5):605–613.
18. Demirkol MO, Yaymaci B, Mutlu B. Dipyridamole myo-cardial perfusion single photon emission computed tomo-graphy in patients with slow coronary flow. Coron Artery Dis.2002;13 (4):223–229.
19. Mangieri E, et al. Slow coronary flow: clinical and histo-pathological features in patients with otherwise normal epi-car- dial coronary arteries. Cathet Cardiovasc Diagn. 1996;37(4):375–381.
20. Mosseri M, et al. Histologic evidence for small-vessel coron-ary artery disease in patients with angina pectoris and patentlarge coronary arteries. Circulation. 1986;74 (5):964–972.
21. Sezgin AT, et al. Vascular endothelial function in patients withslow coronary flow. Coron Artery Dis. 2003;14 (2):155–161.
22. Sambuceti G, et al. Coronary vasoconstriction during myo-cardial ischemia induced by rises in metabolic demand inpatients with coronary artery disease. Circulation. 1997;95 (12):2652–2659.
23. Sambuceti G, L’Abbate A, Marzilli M. Why should westudy the coronary microcirculation? Am J Physiol Heart CircPhysiol. 2000;279 (6):H2581–H2584.
24. Marzilli M, et al. Coronary microcirculatory vasoconstrictionduring ischemia in patients with unstable angina. J Am CollCardiol. 2000;35 (2):327–334.
25. Sambuceti G, et al. Paradoxical increase in microvascularresistance during tachycardia downstream from a severestenosis in patients with coronary artery disease: reversal byangioplasty. Circulation. 2001;103 (19):2352–2360.
26. Marzilli M, et al. Platelet glycoprotein IIb/IIIa receptor block-ade and coronary resistance in unstable angina. J Am CollCardiol. 2002;40 (12):2102–2109.
27. Sambuceti G, et al. Coronary microcirculatory vasoconstric-tion is heterogeneously distributed in acutely ischemicmyocardium. Am J Physiol Heart Circ Physiol. 2005;288 (5):H2298–H2305.
28. Shaw LJ, et al. Cardiovascular imaging research at the cross-roads. JACC Cardiovasc Imaging. 2010;3 (3):316–324.
29. Schwitter J, et al. MR-IMPACT: comparison of perfusion-cardiac magnetic resonance with single-photon emissioncomputed tomography for the detection of coronary arterydisease in a multicentre, multivendor, randomized trial. EurHeart J. 2008;29 (4):480–489.
30. Metz LD, et al. The prognostic value of normal exercisemyocardial perfusion imaging and exercise echocardiogra-phy: a meta-analysis. J Am Coll Cardiol. 2007;49 (2):227–237.
31. Patel MR, et al. Low diagnostic yield of elective coronaryangiography. N Engl J Med. 2010;362 (10):886–895.
31
![Shunting of the Microcirculation After Mesenteric Ischemia and ... · terial blood pressure [SAP, MAP, DAP], heart rate [HR], abdominal blood flow) were recorded using System 6 (Triton](https://img.pdfslide.net/doc/110x75/5e80b881a297cd7cd3039627/shunting-of-the-microcirculation-after-mesenteric-ischemia-and-terial-blood.jpg)