Embed Size (px)
Citation preview

4/13/21
1
Corrective Measures: Taking a Proactive Approach to Category II FHR Patterns
Rebecca Cypher, MSN, PNNPMaternal-Fetal Solutions, LLC
DisclosuresIn addition to Cypher Maternal-Fetal Solutions LLC offering education and consulting services, I have a professional relationship with ◦ Elsevier: Co-author with royalties◦ Clinical Computer Systems: Education
I may discuss off label medications or productsNot all examples that illustrate a concept will be in your handout

4/13/21
2
Objectives
Discuss the prevalence of intrapartum Category II FHR patternsIdentify optimal management strategies for Category II FHR patternsAnalyze research to support conservative corrective measures
One of the difficult OB challenges we face is to ensure appropriate timing of delivery before injury occurs.

4/13/21
3
ELEMENTS OF EFM STANDARDIZATION
Terminology What is it called
Interpretation What does it mean
Management What do we do about it
ELEMENTS OF EFM STANDARDIZATION
Terminology What is it called
Interpretation What does it mean
Management What do we do about it

4/13/21
4
Category II“Indeterminate”
Please do NOT use Reassuring or Non-Reassuring
”…not predictive of abnormal fetal acid-base status yet we do not have adequate evidence to classify as Category I or Category III”
Frequency of Categories in Labor 20 minutes segments
48,444 patients (10 hospitals; 2007-2009)
ITotal
II III I2 hours
II III
Mean minutes
399.6 113.5 0.02 73.1 46.9 0.01
% of total 77.9 22.1 0.004 60.9 39.1 0.006Median minutes
339.4 74.8 0.0 80 40 0.0
Jackson, Marc, et al. "Frequency of fetal heart rate categories and short-term neonatal outcome." Obstetrics & Gynecology118.4 (2011): 803-808.

4/13/21
5
Frequency of Categories in Labor: 20 minutes segments
ITotal
II III I2 hours
II III
Mean minutes
399.6 113.5 0.02 73.1 46.9 0.01
% of total 77.9 22.1 0.004 60.9 39.1 0.006
Median minutes
339.4 74.8 0.0 80 40 0.0
Jackson, M., Holmgren, C.M., Esplin, M.S., Henry, E. and Varner, M.W., 2011. Frequency of fetal heart rate categories and short-term neonatal outcome. Obstetrics & Gynecology, 118(4), pp.803-808.
48,444 patients (10 hospitals; 2007-2009)
Short Term Neonatal Outcomes: Last 2 Hours
1 -25% 26-50% 51-75% 76-100%Patients 11,676 9,313 9,846 9,4941-min Apgar <7 451 (4.8%) 536 (5.4%) 545 (6.7%) 922 (9.7%)5-min Apgar <7 56 (0.6) 61 (0.6) 69 (0.9) 119 (1.3)NICU admission 363 (3.9) 424 (4.3) 395 (4.9) 691 (7.3)5-min Apgar <7
+NICU
22 (0.2) 27 (0.3) 24 (0.3) 67 (0.7)
Jackson, M., Holmgren, C.M., Esplin, M.S., Henry, E. and Varner, M.W., 2011. Frequency of fetal heart rate categories and short-term neonatal outcome. Obstetrics & Gynecology, 118(4), pp.803-808.

4/13/21
6
Variables lasting longer than 60 seconds with nadir more than 60 bpm below baselineVariables lasting longer than 60 seconds with nadir less than 60 bpm regardless of baselineAny late decelerations of any depthAny prolonged decelerations
Clark SL, et al. Intrapartum management of category II fetal heart rate tracings: towards standardization of care. Am J Obstet Gynecol 2013;209(2):89-97.
Clark SL, et al. Intrapartum management of category II fetal heart rate tracings: towards standardization of care. Am J Obstet Gynecol 2013;209(2):89-97.

4/13/21
7
Shields, Laurence E., et al. "A standardized approach for category II fetal heart rate with significant decelerations: Maternal and neonatal outcomes." American journal of perinatology 35.14 (2018): 1405-1410.
Shields, Laurence E., et al. "A standardized approach for category II fetal heart rate with significant decelerations: Maternal and neonatal outcomes." American journal of perinatology 35.14 (2018): 1405-1410.

4/13/21
8
Trial Hospital(6)
PreOct 2015-
March 2016
PostApril 2016-Feb 2017
Non-Trial Hospital
(23)
Pre Post
Total Births 5,208 9,974 Total Births 19, 363 46,839Repeat CD 737 1,459 Repeat CD 2,885 6,933
Eligible 4,471 8,515 Eligible 16,478 39,906
Primary CD-1.5%
p < 0.05
884/4,47119.8%
1,562/8,51518.3%
Primary CD-0.8%
P = 0.02
3,136/16,47819%
7,259/39,90618.2%
VD1.2%
P = 0.13
3,334/4,47174.6%
6,451/8,51575.8%
VD1.3%
P = 0.02
12,296/16,47874.6%
30,305/39,90675.9%
Operative VD0.2%
P = 0.6
253/4,4715.7%
502/8,5155.9%
Operative VD-0.4%P = .02
1,045/16,4786.3%
2,342/39,9065.9%
Shields LE, et al. A Standardized Approach for Category II Fetal Heart Rate with Significant Decelerations: Maternal and Neonatal Outcomes. Am J Perinatol . 2018; 35(14):1405-10.
Trial Hospital(6)
Pre Post Non-Trial (23) Pre Post
5-min Apgar <7-24.6%P <0.05
102/4,4712.3%
146/8,5151.7%
5-min Apgar <7+5.8%
P = 0.08
2,554/16,4781.55%
6,545/39.9061.6%
5-min Apgar <5-26.4%
P = 0.11
474/4,4711.1%
66/8,5150.78%
5-min Apgar <5+12.0%
P = 0.01
1,236/16,4780.53%
227/39,9060.57%
5-min Apgar <30%
P = 0.9
25/4,4710.57%
49/8,5150.57%
5-min Apgar <3+7.5%P = 0.6
87/16,4780.53%
227/39,9060.57%
Severe UNC-27.2%P <0.04
71/4,4711.6%
98/8,5151.2%
Severe UNC-6.7%
P = 0.4
247/16,4781.5%
559/39,9061.4%
UNC: Unexplained Newborn Complications (severe respiratory complications, sepsis, birth trauma, neonatal shock, neuro injury
Shields LE, et al. A Standardized Approach for Category II Fetal Heart Rate with Significant Decelerations: Maternal and Neonatal Outcomes. Am J Perinatol . 2018; 35(14):1405-10.

4/13/21
9
And the subsequent fetal physiologic response if oxygen transfer is
interrupted…decelerations
Fetal oxygenation involves the transfer of oxygen from the environment to the fetus.
Interruptions of oxygen transfer to the fetus can occur at one or more points along the pathway
Miller, L.A., Miller, D. A., & Cypher, R. L. (2021) Mosby’s pocket guide to fetal monitoring: A multidisciplinary approach (9th ed.). Elsevier
• Blood flow to uterine muscle decreased or blocked due to spiral artery compression • Result: Brief periods of anaerobic activity in uterine muscle (normal)
• Relaxation time: oxygenated blood flow returns = lactate cleared

4/13/21
10

4/13/21
11
Recurrent or sustained disruption of oxygenation: Sustain metabolic requirements
Fetal Defense Mechanism Redistribute blood to vital organs
Tissue hypoxia
Anaerobic metabolism
Lactic acidosis
Metabolic acidemia
Direct myocardial depression
Potential Injury
A Standardized Intrapartum FHR Management Model
Four Central Concepts: “ABCD”
A – Assess the oxygen pathway/review differentialsB – Begin conservative corrective measures
C – Clear for delivery D – Decision to delivery time
Miller, L.A., Miller, D. A., & Cypher, R. L. (2021) Mosby’s pocket guide to fetal monitoring: A multidisciplinary approach (9th ed.). Elsevier

4/13/21
12
Mille
r, L.
A., M
iller,
D.A
. and
Cyp
her,
R.L
., 20
21.M
osby
's P
ocke
t Gui
de to
Fet
al M
onito
ring:
A M
ultid
isci
plin
ary
App
roac
h. E
lsev
ier H
ealth
Sci
ence
s.M
iller,
L.A.
, Mille
r, D
.A. a
nd C
yphe
r, R
.L.,
2021
.Mos
by's
Poc
ket G
uide
to F
etal
Mon
itorin
g: A
Mul
tidis
cipl
inar
y A
ppro
ach.
Els
evie
r Hea
lth S
cien
ces.

4/13/21
13
“B” Begin Corrective Measures
ü Maternal repositioningüOxygen administration üIV fluid bolus üDecrease uterine activityüCorrect hypotensionüAmnioinfusionüTocolytic administrationüAlteration in 2nd stage pushing technique
AWHONN Physiologic Goals
Maximize uterine blood flow
Maximize umbilical circulation
Maximize oxygenation
Maintain appropriate uterine activity
Support maternal coping and labor progress
1. Simpson, K. R. (2021). Physiologic interventions for fetal heart rate patterns. In A. Lyndon & K. Wisner (Eds.), Fetal heart rate monitoring: Principles and practices(6th ed., pp. xxx). Kendall-Hunt Publications
4/13/21
14
The Classic Triad Approach
Maternal Position Change
Oxygen Supplementation
Intravenous Fluid Bolus
Maternal Position ChangeMaximize placental perfusion by avoiding aortocaval compression
Alter relationship between umbilical cord, fetus, uterus or bony pelvis
Aldrich CJ, et al. The effect of maternal posture on fetal cerebral oxygenation during labour. BJOG: An International Journal of Obstetrics & Gynaecology. 1995;102(1):14-9.Carbonne B, et al.. Maternal position during labor: effects on fetal oxygen saturation measured by pulse oximetry. Obstetrics & Gynecology. 1996;88(5):797-800.Clark SL, et al. Position change and central hemodynamic profile during normal third-trimester pregnancy and post partum. American journal of obstetrics and gynecology. 1991;164(3):883-7.

4/13/21
15
Lateral PositioningImproves cardiac return and output◦ Position off vena cava or aorta◦⬇ risk of maternal hypotension◦ Maximizes blood flow to uterus
Improves fetal oxygenation◦ Mean FSp02: ◦ LL = 53.2%, RL – 50.5%, Supine = 46.7%
Carbonne, Bruno, et al. "Maternal position during labor: effects on fetal oxygen saturation measured by pulse oximetry." Obstetrics & Gynecology 88.5 (1996): 797-800
Lateral Positioning12 women: 35-38 weeks gestation
MRI: supine and left lateral Phase-contrast images measurements◦ Cardiac output◦ Flow through azygos vein, abdominal aorta
and IVC◦ Deoxygenated blood back to superior vena cava
Humphries, Aimee, et al. "The effect of supine positioning on maternal hemodynamics during late pregnancy." The Journal of Maternal-Fetal & Neonatal Medicine (2018): 1-8.

4/13/21
16
Cardiac Output⇓ 16.4 %
IVC flow⇓ 85.3 % (Origin)
⇓ 44.4 % (Renal veins)
Azygos Vein⇑ 220%
Aortic Bifurcation⇓ 32.3%
SUPINE
Let’s Talk About Oxygen
HypoxemiaHypoxia
Maternal Oxygen10L/min
Anaerobic Metabolism
Metabolic Acidosis
Potential Injury
4/13/21
17
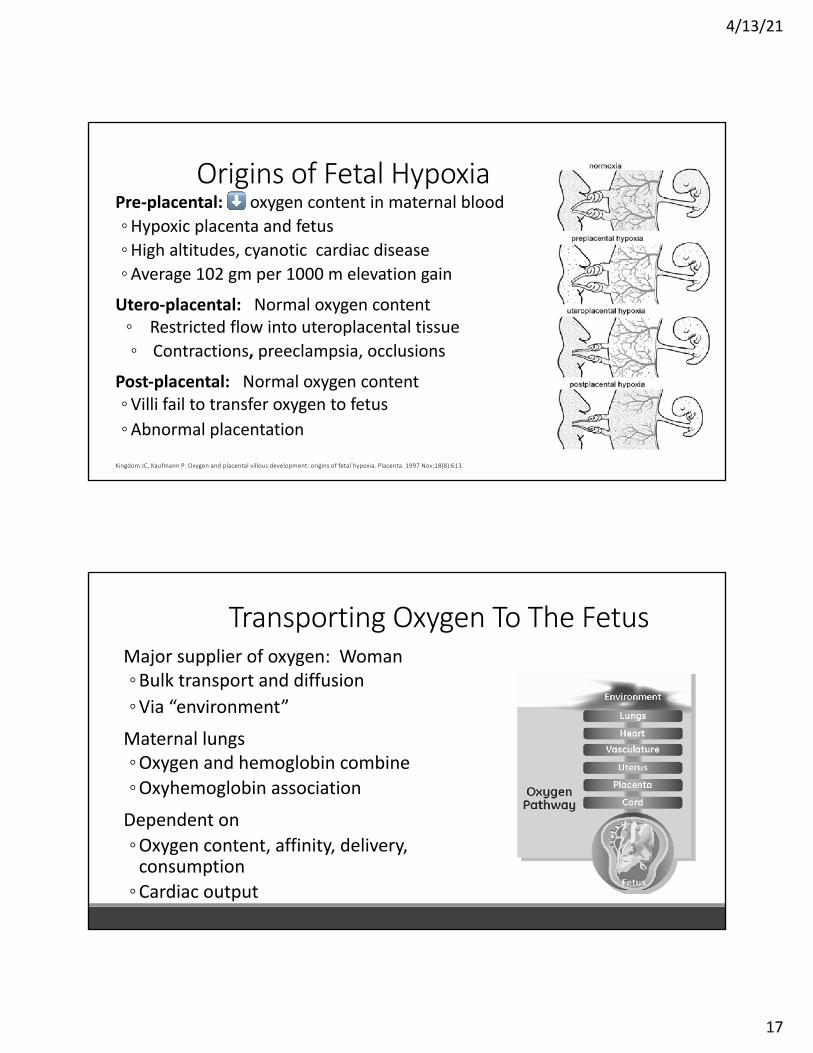
Origins of Fetal HypoxiaPre-placental: ⬇ oxygen content in maternal blood ◦ Hypoxic placenta and fetus◦ High altitudes, cyanotic cardiac disease◦ Average 102 gm per 1000 m elevation gain
Utero-placental: Normal oxygen content ◦ Restricted flow into uteroplacental tissue◦ Contractions, preeclampsia, occlusions
Post-placental: Normal oxygen content ◦ Villi fail to transfer oxygen to fetus◦ Abnormal placentation
Kingdom JC, Kaufmann P. Oxygen and placental villous development: origins of fetal hypoxia. Placenta. 1997 Nov;18(8):613.
Major supplier of oxygen: Woman ◦ Bulk transport and diffusion ◦ Via “environment”
Maternal lungs ◦ Oxygen and hemoglobin combine◦ Oxyhemoglobin association
Dependent on ◦ Oxygen content, affinity, delivery,
consumption◦ Cardiac output
Transporting Oxygen To The Fetus

4/13/21
18
Transporting Oxygen To The FetusCirculated to uterus ◦ Pulmonary arteries◦ Left atrium and left ventricles◦ Aorta◦ Uterine arteries
Uterine perfusion◦ 700-800 mL/min at term◦ 10-15% of maternal CO
Why Give Oxygen In LaborPhysiologically◦Normal oxygen supply to fetus exceeds demand◦Fetal oxygen uptake ◦Not affected until oxygen delivery ⇓ by half
Indeterminate and Abnormal FHR characteristics (Lates)◦Apply 02◦Intervention to ⇑ fetal P02
James LS, Morishima HO, Daniel SS, Bowe ET, Cohen H, Niemann WH. Mechanism of late deceleration of the fetal heart rate. Am J Obstet Gynecol 1972;113:578-82.Murata Y, Martine CB, Ikenoue T, et al. Fetal heart rate accelerations and late decelerations during the course of intrauterine death in chronically catheterized rhesus monkeys. Am JObstet Gynecol 1982;144:218-23.
4/13/21
19
Hamel MS, Anderson BL, Rouse DJ. Oxygen for intrauterine resuscitation: of unproved benefit and potentially harmful. AJOG 2014;211(2):124-7.
Can Oxygen Improve Fetal Metabolic Status?
1960’s-1970’s (animal and human data)Data supporting oxygen to correct FHR decelerations only
Althabe et al., Effects on fetal heart rate and fetal pO2 of oxygen administration to the mother. Am J Obstet Gynecol 1967;98:858-70◦ 100% 02 via face mask (21 women in labor)◦ Corrected fetal tachycardia and ⇓ late decels◦ Correlated with fetal muscle PO2 levels

4/13/21
20
Can Oxygen Improve Fetal Metabolic Status? Maybe
Limited mixed results data◦ Mostly nonrandomized trials◦ Not exclusive to laboring women◦ Animal data
◦ 0xygen ⇑ maternal-fetal oxygen levels ◦ ⇓ Frequency of late decelerations◦ No improvement in fetal pH
Morishima HO, Daniel SS, Richards RT, James LS. The effect of increased maternal PaO2 upon the fetus during labor. Am J Obstet Gynecol 1975;123:257-64.
Thorp JA, et al. The effect of maternal oxygen administration during the second stage of labor on umbilical cord blood gas values: a randomized controlled prospective trial. Am J Obstet Gynecol 1995;172:465-74.◦ Room air versus 10 L/min face mask◦ No difference in umbilical artery pH◦ Oxygen group: ⇑ number of pH values <7.20
Sirimai K, et al. The correlation of intrapartum maternal oxygen administration and umbilical cord blood gas values. Acta Obstet Gynecol Scand 1997;76:90.◦ Similar results

4/13/21
21
⇑ Need for neonatal resuscitationMaternal hyperoxia = ⇑ free radical activity
3 markers of free radical activity ◦ Malondialdehyde (MDA), isoprostane, organic hydroperoxides
Limited Data of Oxygen and Fetal Acid-Base Status
Nesterenko TH, Acun C, Mohamed MA, et al. Is it a safe practice to administer oxygen during uncomplicated delivery? A randomized controlled trial. Early Human Dev 2012;88: 677-81.Yamada T, Yoneyama Y, Sawa R, Araki T. Effects of maternal oxygen supplementation on fetal oxygenation and lipid peroxidation following a single umbilical cod occlusion in fetal goats.J Nippon Med Sch 2003;70:165-71.Suzuki S, Yoneyama Y, Sawa R, Murata T, Araki T, Power GG. Changes in fetal plasma adenosine and xanthine concentrations during fetal asphyxia with maternal oxygen administration in ewes. Tohoku J Exp Med 2000;192:275-81.
Aerobic to anaerobic • ATP depleted
ATP breakdown product
accumulate• Increases cell permeability
Reoxygenation
• Calcium flows into cells• Disrupted ATP production • Cellular molecules breakdown
Oxygen Free Radicals
• Unstable molecules that damage cell membrane.
• Potential edema and hemorrhage to fetal brain and heart
Klinger G, Beyene J, Shah P, Perlman M. Do hyperoxemia and hypocapnia add to the risk of brain injury after ntrapartum asphyxia? Arch Dis Child FetalNeonatal Ed 2005;90:F49-52.

4/13/21
22
Neonatal Resuscitation100% oxygen no longer recommended◦ Oxygen induced cellular damage
◦ Bronchopulmonary dysplasia◦ Neurodevelopmental complications◦ Retinopathy
Room air: decreased neonatal mortalityNo difference in HIE or changes in neurodevelopmental outcomes
Aziz, K.,et al., (2020). 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and
Emergency Cardiovascular Care. Pediatrics.Welsford, Michelle, et al. "Room air for initiating term newborn resuscitation: a systematic review with meta-analysis." Pediatrics 143.1 (2019).
Impact of HyperoxygenationAdult (AVOID trial)◦ Supplemental oxygen with ST-elevation–myocardial infarction without hypoxia ◦ ⇑ early myocardial injury = larger myocardial infarct size at 6 months
Adult◦ 02 to maintain PaO2 and SpO2 values◦ Conservative oxygen therapy vs conventional therapy resulted in lower ICU mortality
◦ Maintain Pao2 between 70 and 100 mm Hg or Spo2 94% - 98%
Stub, Dion, et al. "A randomized controlled trial of oxygen therapy in acute myocardial infarction Air Verses Oxygen In myocarDial infarction study (AVOID Study)." American heart journal 163.3 (2012): 339-345.Stub D, et al.. Air versus oxygen in ST-segment elevation myocardial infarction. Circulation. 2015 May 22:circulationaha-114.Girardis, Massimo, et al. "Effect of conservative vs conventional oxygen therapy on mortality among patients in an intensive care unit: the oxygen-ICU randomized clinical trial." Jama 316.15 (2016): 1583-1589.

4/13/21
23
Hemodynamics of Hyperoxygenation
46 pregnant women and 20 nonpregnant women◦ Median EGA: 35 weeks (33 to 37 weeks)
Continuous hemodynamic monitoringHyperoxygenation: 02 100% at 12L/min by partial non-breather maskMeasurements before, immediately after completion, 10 minutes after◦ Cardiac index, SVR, stroke volume, HR, BL◦ Significant ⇓ cardiac index and ⇑ SVR without
return to BL◦ ? Impact on oxygen delivery
McHugh A, et al.. Hyperoxygenation in pregnancy exerts a more profound effect on cardiovascular hemodynamics than is observed in the nonpregnant state. Am J Obstet Gynecol 2019;220:397.e1-8.
Study Population N Groups Findings
Lawes et al, 1988RCT
Elective CD 35 02 50% vs 33% ND: Cord gasesApgars
Perreault et al, 1992RCT
Elective CD 20 02 50% vs 100% ND: Cord gases5 minute Apgars
Thorp et al, 1995RCT
2nd stage labor 86 02 10L face mask vs no 02
⬆ abnormal cord gases prolonged 02
Sirimai et al, 1997RCT
2nd stage labor 80 02 vs no 02 ND: cord gases
Jozwik et al, 2000Prospective Cohort
Elective CD 41 02 60% at 15L x15 min vs 02 via face mask
ND: Fetal acid base status
Qian et al, 2017RCT
2nd stage laborNo EFM
abnormalities
443 02 2L/min nasal cannula vs placebo
ND: Cord gasesFHR changes
Raghuraman et al, 2017Retrospective Cohort
1st and 2nd stage 7,789 02 vs no 02 02 : ⬆ neo morbidity in acidemic neonates
Ankumah, Nana-Ama E., et al. "Liberal versus Indicated Maternal Oxygen Supplementation in Labor: A Before-and-After Trial." American journal of perinatology (2018).35 (11) 1057-1064

4/13/21
24
Among patients with category II fetal heart tracings, intrauterine resuscitation with room air is noninferior to oxygen in improving umbilical artery lactate. The results of this trial challenge the efficacy of a ubiquitous obstetric practice and suggest that room air may be an acceptable alternative.
Raghuraman, Nandini, et al. "Effect of oxygen vs room air on intrauterine fetal resuscitation: a randomized noninferiority clinical trial." JAMA pediatrics 172.9 (2018): 818-823.

4/13/21
25
FHR Pattern OxygenN-57
Room AirN=57
P-value
Ever variable deceleration 34 (59.7%) 29 (50.9%) 0.35Recurrent variable deceleration 4 (7%) 2 (3.5%) 0.40Ever late deceleration 40 (70.2%) 41 (71.9%) 0.84Recurrent late deceleration 2 (3.5%) 5 (8.8%) 0.24Ever tachycardia 0 2 (3.3%) 0.50Ever minimal variability 5 (8.3%) 11 (8.3%) 0.18Ever prolonged deceleration 18 (31.6%) 17 (29.8%) 0.56
60 Minutes Prior to Randomization
Ever: present at any point within 60 minutes as analyzed in 10 minute segmentsRecurrent: present with more than 50% of contractions within 60 minutes as analyzed in 10 minute segments
Oxygen (N=48) Room Air (n=51) P-ValueUmbilical Artery Gas
pHBase ExcesspCO2
7.26 (7.24-7.28)-3.62 (-4.3-2.9)55.9 (53.5-58.2)
7.25 (7.23-7.27)-3.6 (4.3-2.9)
57.4 (54.2-60.6)
0.550.990.44
Mode of BirthCesareanCesarean for FHROperative Vaginal Birth
2 (3.9%)0
6 (11.8%)
6 (12.5%)2 (4.2%)1 (2.1%)
0.14N/A0.10
Raghuraman, Nandini, et al. "Effect of oxygen vs room air on intrauterine fetal resuscitation: a randomized noninferiority clinical trial." JAMA pediatrics 172.9 (2018): 818-823.

4/13/21
26
Mean Umbilical Artery Lactate
Blue line: non-inferiority marginBlack dot: mean and error for 95% CI
Mean lactate difference: 0.9 mg/dL
Raghuraman, Nandini, et al. "Effect of oxygen vs room air on intrauterine fetal resuscitation: a randomized noninferiority clinical trial." JAMA pediatrics 172.9 (2018): 818-823.
Today’s Take Home PointsAsk yourself if oxygen is necessary as a first line responseTry other corrective measures initially◦ Moderate variability
Discontinue as soon as fetal response warrantsKeep reading the journals

4/13/21
27
Raghuraman, Nandini, et al. "Maternal Oxygen Supplementation Compared With Room Air for Intrauterine Resuscitation: A Systematic Review and Meta-analysis." JAMA pediatrics (2021).
Question: Is maternal oxygen supplementation at the time of birth associated with improved umbilical artery gas measures and neonatal outcomes?
Key Point: ◦ Maternal oxygen supplementation was associated with improved UA PaO2 but
no significant difference in UA pH compared with room air. ◦ Similar UA gas measures, NICU admissions, and Apgar scores between the
oxygen and room air groups.
What does this mean to you? No association between maternal oxygen supplementation and a clinically relevant improvement in UA pH or other neonatal outcomes.

4/13/21
28
Maximize Maternal Intravascular Volume
Improved cardiac output by
Increasing circulatory volume
Increasing venous return
Increasing left ventricular end-diastolic pressure
Increasing ventricular preload
Increased stroke volume
⬆ Intravascular Volume Improves Uteroplacental Perfusion
Simpson, K.R. and James, D.C., 2005. Efficacy of intrauterine resuscitation techniques in improving fetal oxygen status during labor. Obstetrics & Gynecology, 105(6), pp.1362-1368.

4/13/21
29
57Miller NR, Cypher RL, Nielsen PE, Foglia LM. Maternal pulse pressure at admission is a risk factor for fetal heart rate changes after initial dosing of a labor epidural: a retrospective cohort study. AJOG. 2013;209(4):382-e1.
Objective
Is decreased maternal pulse pressure a risk factor for new onset post-epidural FHR abnormalities
◦<45 mmHg◦FHR abnormalities in first 60 minutes after dosing◦Recurrent late decelerations and/or prolonged decelerations
58

4/13/21
30
Admission PP ≥45 mmHg
N=95
Admission PP <45 mmHg
N=95
OR (95% CI P value
FHR Abnormalities
6 (6) 26 (27) 5.6 (2.1 -14.3) < .001
After initial labor epidural dosing, new onset FHR abnormalities occur more frequently in women with low admission PP compared to those with normal admission PP
Lappen, J.R., Chien, E.K. and Mercer, B.M., 2018. Contraction-associated maternal heart rate decelerations: a pragmatic marker of intrapartum volume status. Obstetrics & Gynecology, 132(4), pp.1011-1017.
Contraction Associated Maternal Heart Rate Decelerations

4/13/21
31
Contraction Associated DecelerationsHypovolemic (<45 mmHg) vs euvolemic (≥ 50 mmHg)◦ 41.1% vs 13.6%
CAHRD◦⬆ Post-epidural FHR abnormalities (43.5% vs 31.1%)◦⬆ Diastolic hypotension (63.7% vs 50.0%)◦⬆ Need for resuscitative interventions (33.9% vs 23.1%)◦Our goal: Intrapartum maternal heart rate assessment
Intrapartum fluid management
Lappen, J.R., Chien, E.K. and Mercer, B.M., 2018. Contraction-associated maternal heart rate decelerations: a pragmatic marker of intrapartum volume status. Obstetrics & Gynecology, 132(4), pp.1011-1017.
The “So What” Factor
Evaluate for intravascular volume reductionBleeding or dehydration
Co-load versus pre-load for regional anesthesia
Consider pretreatment with vasoconstricting agent

4/13/21
32
IV Fluid Maintenance RateIncrease IV fluid maintenance rate◦125 cc/hr designed to replace loss in resting patient
◦Labor = active metabolically and physiologically◦Consider 200-250 cc/hr in healthy patient
Five studies: LROne study: D5NSOne study: Not defined

4/13/21
33
IV Fluid: 250 cc/hr vs 125 cc/hr7 clinical trials
Lower incidence of cesarean for any indication: 12.5 vs 18.1%Lower incidence of cesarean for labor dystocia: 4.9 vs 7.7%Shorter mean duration of labor: mean difference 64 minutes“Shorter” mean length 2nd stage: ~ 3 minutes
Normal saline versus D5NS versus D10NS 125 mL/hr
Shrivastava, Vineet K., et al. "A randomized, double-blinded, controlled trial comparing parenteral normal saline with and without dextrose on the course of labor in nulliparas." American journal of obstetrics and gynecology 200.4 (2009): 379-e1.

4/13/21
34
Labor OutcomesNS
N=84D5NSN=76
D10NSN=72
P Value
IVF start to 10 cm 360 min(95-1203)
299 minutes(82-1091)
328 minutes(61-672)
.10
2nd stage 106 minutes(24-266)
69 minutes(17-227)
62 minutes(14-191)
.01
IVF start to birth 464 minutes(185-1336)
392 minutes(100-1157)
393 minutes(97-827)
.02
Prolonged labor>12 hours
18 (22%) 7 (9.3%) 5 (6.8%) .01
Shrivastava, Vineet K., et al. "A randomized, double-blinded, controlled trial comparing parenteral normal saline with and without dextrose on the course of labor in nulliparas." American journal of obstetrics and gynecology 200.4 (2009): 379-e1.
Thank You



![RAPID EVALUATION OF MAINTENANCE PROCESS USING … · Table I: Maintenance terminology by [21]. Action Corrective/ reactive Predictive, preventive and proactive Policy Failure based](https://img.pdfslide.net/doc/110x75/5ed4261c15afd8270936f088/rapid-evaluation-of-maintenance-process-using-table-i-maintenance-terminology-by.jpg)




















![Taking a Proactive Approach to Combat Ransomware [Druva Webinar]](https://img.pdfslide.net/doc/110x75/58d19c991a28ab6f6b8b500f/taking-a-proactive-approach-to-combat-ransomware-druva-webinar.jpg)




![mechanical fault diagnosis part 1 · 2019. 5. 17. · Ch 1 [2] Prepared by: Dr. Essam Bahgat essbahgat@gmail.com 4) Proactive-Centred Maintenance (PCM) 1.2.1 CORRECTIVE OR REACTIVE](https://img.pdfslide.net/doc/110x75/61482ac3cee6357ef9252d83/mechanical-fault-diagnosis-part-1-2019-5-17-ch-1-2-prepared-by-dr-essam.jpg)