Embed Size (px)
Citation preview

ABSTRACT
Objective: To study the relationship between bonemarkers and bone mineral density (BMD) in an effort toidentify their utility in postmenopausal women with osteo-porosis.
Methods: Eighty-two consecutive postmenopausalwomen with untreated osteoporosis were included in thestudy. Forearm, spinal, and femoral BMD by dual-energyx-ray absorptiometry and markers of bone formation(serum osteocalcin and bone-specific alkaline phos-phatase) and bone resorption (urinary free deoxypyridino-line) were measured in all patients. Patients with lowserum vitamin D levels, secondary osteoporosis, or clini-cally significant systemic disease were excluded from thestudy. The patients were classified on the basis of BMD ofthe lumbar spine into the following 3 groups: mild (n = 23)(T score -2.5 through -3), moderate (n = 42) (T score-3.1 through -4), or severe (n = 17) (T score ≤-4.1)osteoporosis. One-way analysis of variance and Pearsoncorrelation were used for statistical analysis, with a Pvalue <.05 being considered significant.
Results: Serum osteocalcin was significantly differ-ent among the 3 study groups (4.1 ± 2.7, 4.5 ± 3.1, and6.7 ± 5.6 ng/mL, respectively; P = .0349) and had asignificant negative correlation with BMD (r2 = -0.0779;P = .0168). Other bone markers such as bone-specificalkaline phosphatase and urinary free deoxypyridinolinedid not correlate with the underlying BMD.
Conclusion: In our study, osteocalcin was signifi-cantly correlated with BMD in postmenopausal womenwith osteoporosis. Other bone markers did not correlatewith BMD. Further large-scale population data and analy-ses are needed to confirm these findings. (Endocr Pract.2008;14:1102-1107)
INTRODUCTION
Osteoporosis is a widely prevalent, often underdiag-nosed public health problem that results in substantialmorbidity and mortality. It is a complex disease of multi-factorial cause with varied bone turnover (1). Poor nutri-tion, inadequate exposure to sunlight, and low vitamin Dstatus contribute to severe osteoporosis in India, and aneed exists for effective measures to diagnose the condi-tion early (2). The current standard approach for diagnos-ing osteoporosis is estimation of bone mineral density(BMD) with use of dual-energy x-ray absorptiometry(DEXA). Nevertheless, lack of definite prescreening vari-ables and poor efficacy of BMD in monitoring theresponse to therapy limit the usefulness of DEXA (3).Hence, investigators have used alternative measures suchas estimation of bone remodeling markers to derive mean-ingful conclusions about the skeletal mineralization.Biochemical markers of bone turnover are released duringbone formation or resorption and can be measured in theblood or urine (or both). The concentrations of boneturnover markers reflect bone remodeling activity and canpotentially be used as surrogate markers of the rate ofbone formation or bone resorption (4-6).
Scientific opinion is divided on the role of biochemi-cal markers of bone turnover as screening tools for diag-nosing osteopenia or osteoporosis (7). Various factorssuch as age, concomitant medication, immobilization, thy-roid function, and comorbidity influence bone metabolismand therefore need to be considered in the interpretation ofbiochemical data and their use in individual patients (8).Markers of bone resorption have been stronger predictorsof future bone loss than markers of bone formation, withstrong correlations in elderly women. On the contrary,predicting bone density may not be possible in an individ-
CORRELATION BETWEEN BONE MARKERSAND BONE MINERAL DENSITY IN
POSTMENOPAUSAL WOMEN WITH OSTEOPOROSIS
K. V. S. Hari Kumar, MD, Jayaraman Muthukrishnan, MD, Abhyuday Verma, MD,and Kirtikumar D. Modi, MD, DM
Submitted for publication June 6, 2008Accepted for publication July 16, 2008From the Department of Endocrinology, Medwin Hospitals, Nampally,Hyderabad, India.Address correspondence and reprint requests to Dr. K. V. S. Hari Kumar,Department of Endocrinology, Medwin Hospitals, Chirag Ali Lane,Nampally, Hyderabad 500001, India.© 2008 AACE.
1102 ENDOCRINE PRACTICE Vol 14 No. 9 December 2008
Original Article
Abbreviations:BMD = bone mineral density; DEXA = dual-energy x-ray absorptiometry; DPD = deoxypyridinoline; 25-OHD = 25-hydroxyvitamin D; PTH = parathyroidhormone

ual patient because of the high variability in markers ofbone turnover (9). None of the biochemical markers ofbone turnover has proved useful as a single diagnosticindex of osteoporosis. In clinical practice, however, boneturnover markers help in decision making in patients withborderline risk and in serial monitoring of patients receiv-ing therapy for osteoporosis. Data regarding the correla-tion of bone turnover markers with underlying osteo-porosis or osteopenia are limited. An increase in boneturnover markers suggests underlying increased bone loss;however, the direct relationship between levels of boneturnover markers and severity of bone loss as assessed byBMD is unclear. Hence, in an attempt to ascertain the rela-tionship between bone turnover markers and osteoporosis,we performed this cross-sectional study in post-menopausal women already diagnosed with osteoporosison the basis of BMD determined by DEXA.
PATIENTS AND METHODS
Study SubjectsThe study cohort consisted of 82 consecutive post-
menopausal (defined as at least 2 years after last menstru-al period) Indian women with untreated osteoporosis(defined as T score at least 2.5 SDs below the young adultmean). The patients did not have clinically significantpostmenopausal symptoms at the time of evaluation. Adetailed history was elicited regarding features of osteo-porosis, personal history and family history of fractures,loss of height, bone pains, and other complaints. Otherimportant assessment included the amount of milk con-sumption and exposure to sunlight per day. The patientswith secondary osteoporosis, prolonged glucocorticoidintake (defined as use of prednisolone in a dosage of morethan 5 mg/d for at least 3 months), or significant renal,hepatic, or thyroid dysfunction were excluded from thestudy. Similarly, patients with low serum vitamin D levels(defined as less than 30 ng/mL) or elevated levels ofparathyroid hormone (PTH) (more than 65 pg/mL) oralkaline phosphatase (more than 110 U/L) were excludedfrom the study. No patients were receiving calcium or vi-tamin D supplements before the study. All participants inthe study were nonsmokers, denied alcohol consumption,were ambulatory, and were not receiving hormonereplacement therapy. Moreover, they were not using anyconcomitant medication that would appreciably affect theestimation of bone turnover markers.
Of the 240 patients who were screened for the study,82 qualified for inclusion in the analysis. The reasons forexclusion of the other 158 patients were vitamin D defi-ciency (80%), systemic disorder (10%), glucocorticoidintake (5%), elevated PTH level (2%), and other factors(3%). The patients were grouped on the basis of BMD ofthe lumbar spine into mild (T score -2.5 through -3),moderate (T score -3.1 through -4), or severe (T score≤-4.1) osteoporosis. The stratification of the groups wasfor comparative statistical analysis and was based on pre-
vious studies that indicated a higher fracture risk associat-ed with worsening BMD value (10,11).
Biochemical MeasurementsSerum and urine samples were collected from all
patients before 9 AM after an overnight fast. The sampleswere immediately processed and kept frozen at -80°Cuntil the assays were performed. Biochemical tests includ-ing serum calcium, 25-hydroxyvitamin D (25-OHD),intact PTH, and thyroid-stimulating hormone (thy-rotropin) as well as fasting urine collection for measure-ment of calcium and creatinine were performed on allparticipants. Markers of bone formation (bone-specificalkaline phosphatase and osteocalcin) and markers of boneresorption (urinary free deoxypyridinoline [DPD] cross-links) were measured in all study subjects. Serum calciumand serum phosphorus were determined by spectrophoto-metric analysis, serum 25-OHD was measured by radioim-munoassay, and intact PTH was determined bychemiluminescence assay. All bone turnover markerswere measured by highly specific enzyme-linkedimmunosorbent assay (kits provided by Metra Biosystems,Quidel Corporation, Mountain View, California).
BMD MeasurementsThe T score, bone mineral content, and BMD were
determined at 3 anatomic sites—the hip, the lumbar spine,and the forearm—with use of DEXA (Lunar Corp.,Madison, Wisconsin; coefficient of variation, 0.64%).Values of the BMD at the lumbar spine were expressed asthe mean of those at the L1 through L4 vertebrae. The Tscores and Z scores were calculated on the basis of normalreference values for age- and sex-matched subjects (pro-vided by the DEXA manufacturer). The estimation ofBMD was done with use of the same machine for allpatients participating in the study.
Statistical AnalysisThe summary data are expressed as mean values ±
SD, and comparisons between groups were done by usingthe one-way analysis of variance test. Relationshipsbetween continuous variables were assessed by Pearsoncorrelation, and the distribution of all variables was con-sidered to be derived from the population following agaussian distribution. P values were reported for all statis-tical tests, and values <.05 were considered significant.
RESULTS
The clinical and biochemical data of the 3 groups ofpatients are presented in Table 1. Overall, the mean age ofthe study population was 62.4 ± 6.4 years, and the meanbody mass index was 25.76 ± 4.01 kg/m2. The mean ageof the patients in the 3 study groups was not significantlydifferent. For the overall study cohort, the mean durationof postmenopausal years was 16.04 ± 6.4 years. The cor-relation between body mass index and BMD in the entire
Bone Markers and Bone Density, Endocr Pract. 2008;14(No. 9) 1103
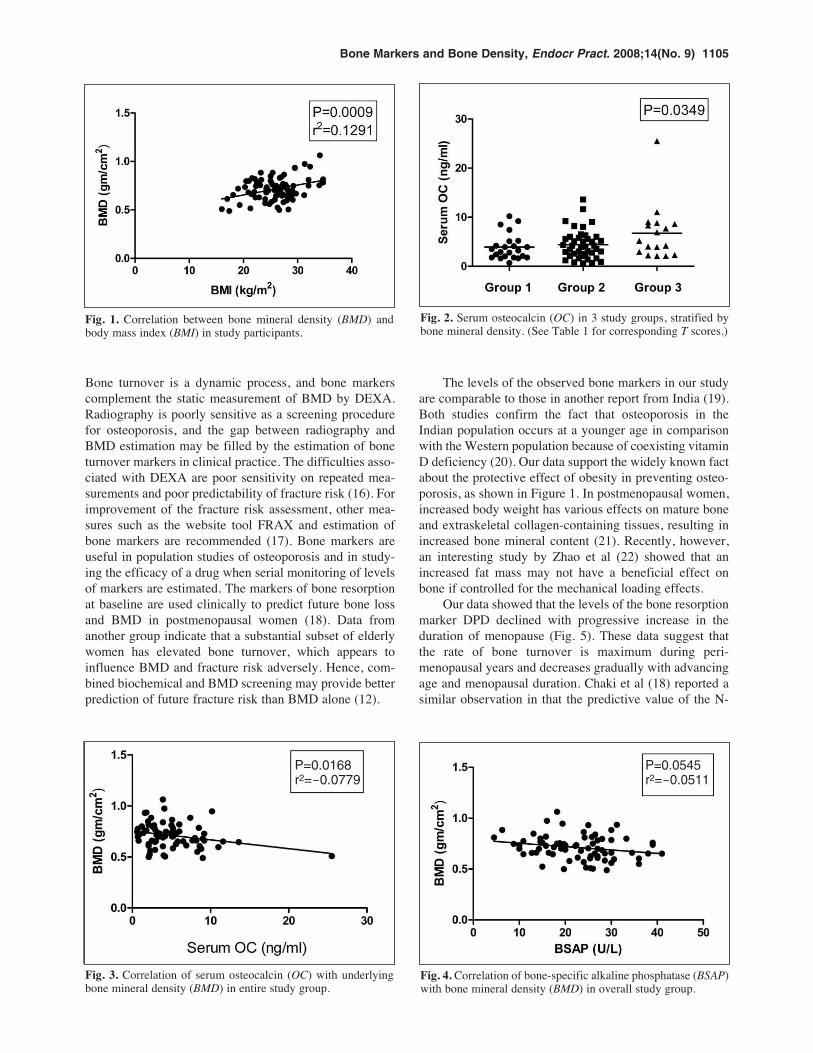
study population is depicted in Figure 1. All groups hadcomparable mean baseline values of 25-OHD and intactPTH levels.
Serum osteocalcin was significantly different amongthe 3 study groups, as shown in Figure 2 (4.1 ± 2.7, 4.5 ±3.1, and 6.7 ± 5.6 ng/mL; P = .0349); the highest valueswere observed in the group with severe osteoporosis.The correlation of serum osteocalcin with underlyingBMD demonstrated a significant negative relationship(r2 = -0.0779; P = .0168) (Fig. 3). Bone-specific alkalinephosphatase, the other bone formation marker studied,showed a similar trend, but it was not statistically signifi-cant (r2 = -0.0511; P = .0545) (Fig. 4). The bone resorp-tion marker DPD did not correlate with BMD (P = .6871).
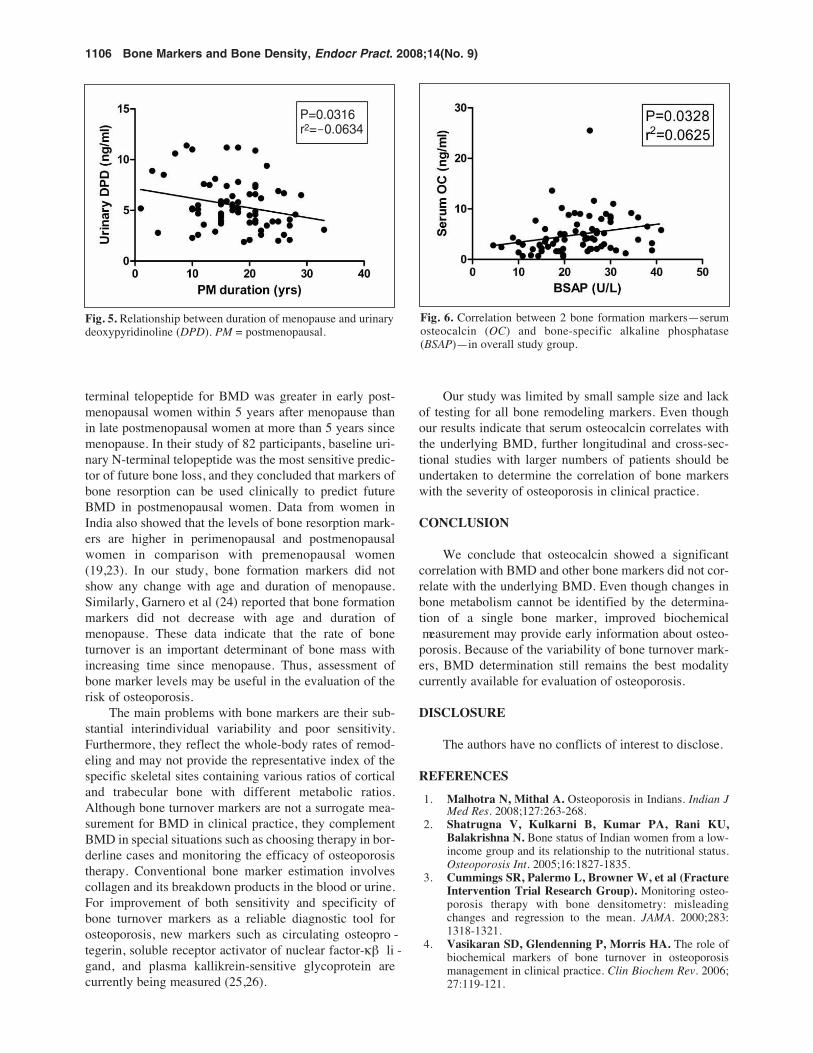
Of 3 bone turnover markers measured, the resorptionmarker (DPD) showed a significant negative correlationwith the duration of postmenopausal years (P = .0316)(Fig. 5). Bone-specific alkaline phosphatase (P = .1951)and osteocalcin (P = .8048) did not change with the dura-tion of menopause. In the entire study population, osteo-calcin levels showed no correlation with vitamin Dconcentrations (r2 = 0.0207; P = .2238).
DISCUSSION
In this study, we have analyzed the correlationbetween markers of bone turnover and underlying osteo-porosis. Our data showed that levels of bone formationmarkers such as osteocalcin have a significant correlationwith the underlying BMD. The data suggest that anincrease in osteocalcin levels is associated with moresevere osteoporosis. This finding highlights the fact that
high bone turnover rates are associated with more rapidand severe bone loss in postmenopausal women (12). Onepatient in the severe osteoporosis group (group 3) had anextremely high osteocalcin value (25.5 ng/mL) (Fig. 2).This outlier value emphasizes the variability and poorstandardization of the osteocalcin assay. In the analysisafter exclusion of this outlier value, osteocalcin did notshow a correlation with the underlying BMD (P = .08).Bone-specific alkaline phosphatase, the other bone forma-tion marker studied, demonstrated a similar (but statisti-cally nonsignificant) trend in relationship to BMD (P =.0545). This result highlights the biologic and laboratoryvariability of bone marker assays, limiting their clinicalapplication. In our study, however, there was a linear cor-relation between 2 bone formation markers (osteocalcinand bone-specific alkaline phosphatase), as shown inFigure 6.
Our data suggest that the bone resorption marker DPDdid not correlate with the severity of the underlying BMD.Bone loss is characterized by increased turnover andresorption. Therefore, it was surprising that DPD did notemulate the results of bone formation markers. The uri-nary free DPD assay is not sufficiently sensitive to distin-guish between normal and low bone mass inpostmenopausal women (13). Moreover, the laboratoryassay varies for measurement of free DPD and total DPD;the latter has enhanced sensitivity and specificity (14). Astudy by Kitatani et al (15), however, showed that theresponse to bisphosphonate therapy is better assessed byfree DPD than by total DPD estimation.
Early diagnosis of osteoporosis is the key to successin prevention, and bone markers are helpful in this regard.
1104 Bone Markers and Bone Density, Endocr Pract. 2008;14(No. 9)
Table 1Clinical and Biochemical Characteristics of Study Patientsa
Patients stratified by T scoreGroup 1: Group 2: Group 3: P
Factor --2.5 to --3 --3.1 to --4 ≤--4.1 value
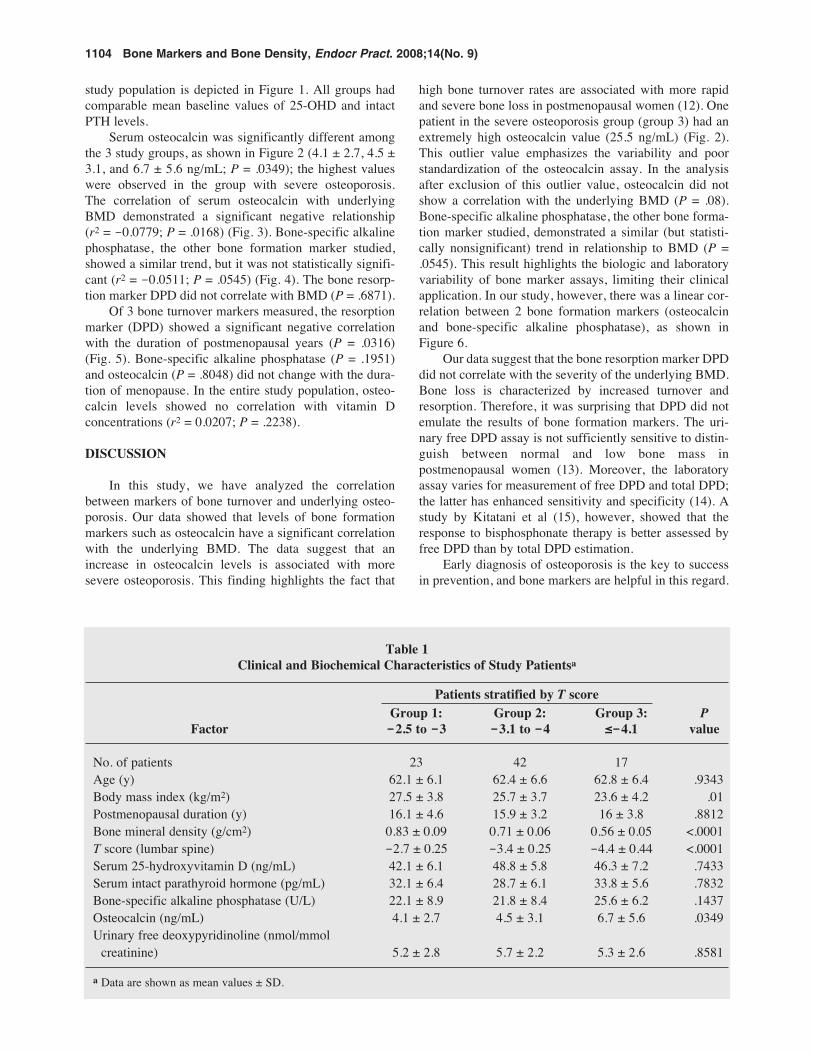
No. of patients 23 42 17Age (y) 62.1 ± 6.1 62.4 ± 6.6 62.8 ± 6.4 .9343Body mass index (kg/m2) 27.5 ± 3.8 25.7 ± 3.7 23.6 ± 4.2 .01Postmenopausal duration (y) 16.1 ± 4.6 15.9 ± 3.2 16 ± 3.8 .8812Bone mineral density (g/cm2) 0.83 ± 0.09 0.71 ± 0.06 0.56 ± 0.05 <.0001T score (lumbar spine) -2.7 ± 0.25 -3.4 ± 0.25 -4.4 ± 0.44 <.0001Serum 25-hydroxyvitamin D (ng/mL) 42.1 ± 6.1 48.8 ± 5.8 46.3 ± 7.2 .7433Serum intact parathyroid hormone (pg/mL) 32.1 ± 6.4 28.7 ± 6.1 33.8 ± 5.6 .7832Bone-specific alkaline phosphatase (U/L) 22.1 ± 8.9 21.8 ± 8.4 25.6 ± 6.2 .1437Osteocalcin (ng/mL) 4.1 ± 2.7 4.5 ± 3.1 6.7 ± 5.6 .0349Urinary free deoxypyridinoline (nmol/mmol
creatinine) 5.2 ± 2.8 5.7 ± 2.2 5.3 ± 2.6 .8581
a Data are shown as mean values ± SD.
Bone turnover is a dynamic process, and bone markerscomplement the static measurement of BMD by DEXA.Radiography is poorly sensitive as a screening procedurefor osteoporosis, and the gap between radiography andBMD estimation may be filled by the estimation of boneturnover markers in clinical practice. The difficulties asso-ciated with DEXA are poor sensitivity on repeated mea-surements and poor predictability of fracture risk (16). Forimprovement of the fracture risk assessment, other mea-sures such as the website tool FRAX and estimation ofbone markers are recommended (17). Bone markers areuseful in population studies of osteoporosis and in study-ing the efficacy of a drug when serial monitoring of levelsof markers are estimated. The markers of bone resorptionat baseline are used clinically to predict future bone lossand BMD in postmenopausal women (18). Data fromanother group indicate that a substantial subset of elderlywomen has elevated bone turnover, which appears toinfluence BMD and fracture risk adversely. Hence, com-bined biochemical and BMD screening may provide betterprediction of future fracture risk than BMD alone (12).
The levels of the observed bone markers in our studyare comparable to those in another report from India (19).Both studies confirm the fact that osteoporosis in theIndian population occurs at a younger age in comparisonwith the Western population because of coexisting vitaminD deficiency (20). Our data support the widely known factabout the protective effect of obesity in preventing osteo-porosis, as shown in Figure 1. In postmenopausal women,increased body weight has various effects on mature boneand extraskeletal collagen-containing tissues, resulting inincreased bone mineral content (21). Recently, however,an interesting study by Zhao et al (22) showed that anincreased fat mass may not have a beneficial effect onbone if controlled for the mechanical loading effects.
Our data showed that the levels of the bone resorptionmarker DPD declined with progressive increase in theduration of menopause (Fig. 5). These data suggest thatthe rate of bone turnover is maximum during peri-menopausal years and decreases gradually with advancingage and menopausal duration. Chaki et al (18) reported asimilar observation in that the predictive value of the N-
Bone Markers and Bone Density, Endocr Pract. 2008;14(No. 9) 1105
Fig. 1. Correlation between bone mineral density (BMD) andbody mass index (BMI) in study participants.
Fig. 2. Serum osteocalcin (OC) in 3 study groups, stratified bybone mineral density. (See Table 1 for corresponding T scores.)
Fig. 3. Correlation of serum osteocalcin (OC) with underlyingbone mineral density (BMD) in entire study group.
Fig. 4. Correlation of bone-specific alkaline phosphatase (BSAP)with bone mineral density (BMD) in overall study group.
P=0.0168r2=-0.0779
P=0.0545r2=-0.0511
terminal telopeptide for BMD was greater in early post-menopausal women within 5 years after menopause thanin late postmenopausal women at more than 5 years sincemenopause. In their study of 82 participants, baseline uri-nary N-terminal telopeptide was the most sensitive predic-tor of future bone loss, and they concluded that markers ofbone resorption can be used clinically to predict futureBMD in postmenopausal women. Data from women inIndia also showed that the levels of bone resorption mark-ers are higher in perimenopausal and postmenopausalwomen in comparison with premenopausal women(19,23). In our study, bone formation markers did notshow any change with age and duration of menopause.Similarly, Garnero et al (24) reported that bone formationmarkers did not decrease with age and duration ofmenopause. These data indicate that the rate of boneturnover is an important determinant of bone mass withincreasing time since menopause. Thus, assessment ofbone marker levels may be useful in the evaluation of therisk of osteoporosis.
The main problems with bone markers are their sub-stantial interindividual variability and poor sensitivity.Furthermore, they reflect the whole-body rates of remod-eling and may not provide the representative index of thespecific skeletal sites containing various ratios of corticaland trabecular bone with different metabolic ratios.Although bone turnover markers are not a surrogate mea-surement for BMD in clinical practice, they complementBMD in special situations such as choosing therapy in bor-derline cases and monitoring the efficacy of osteoporosistherapy. Conventional bone marker estimation involvescollagen and its breakdown products in the blood or urine.For improvement of both sensitivity and specificity ofbone turnover markers as a reliable diagnostic tool forosteoporosis, new markers such as circulating osteopro -tegerin, soluble receptor activator of nuclear factor-κβ li -gand, and plasma kallikrein-sensitive glycoprotein arecurrently being measured (25,26).
Our study was limited by small sample size and lackof testing for all bone remodeling markers. Even thoughour results indicate that serum osteocalcin correlates withthe underlying BMD, further longitudinal and cross-sec-tional studies with larger numbers of patients should beundertaken to determine the correlation of bone markerswith the severity of osteoporosis in clinical practice.
CONCLUSION
We conclude that osteocalcin showed a significantcorrelation with BMD and other bone markers did not cor-relate with the underlying BMD. Even though changes inbone metabolism cannot be identified by the determina-tion of a single bone marker, improved biochemical measurement may provide early information about osteo -porosis. Because of the variability of bone turnover mark-ers, BMD determination still remains the best modalitycurrently available for evaluation of osteoporosis.
DISCLOSURE
The authors have no conflicts of interest to disclose.
REFERENCES1. Malhotra N, Mithal A. Osteoporosis in Indians. Indian J
Med Res. 2008;127:263-268.2. Shatrugna V, Kulkarni B, Kumar PA, Rani KU,
Balakrishna N. Bone status of Indian women from a low-income group and its relationship to the nutritional status.Osteoporosis Int. 2005;16:1827-1835.
3. Cummings SR, Palermo L, Browner W, et al (FractureIntervention Trial Research Group). Monitoring osteo-porosis therapy with bone densitometry: misleadingchanges and regression to the mean. JAMA. 2000;283:1318-1321.
4. Vasikaran SD, Glendenning P, Morris HA. The role ofbiochemical markers of bone turnover in osteoporosismanagement in clinical practice. Clin Biochem Rev. 2006;27:119-121.
1106 Bone Markers and Bone Density, Endocr Pract. 2008;14(No. 9)
Fig. 5. Relationship between duration of menopause and urinarydeoxypyridinoline (DPD). PM = postmenopausal.
Fig. 6. Correlation between 2 bone formation markers—serumosteocalcin (OC) and bone-specific alkaline phosphatase(BSAP)—in overall study group.
P=0.0316r2=-0.0634

5. Seibel MJ. Clinical application of biochemical markers ofbone turnover. Arq Bras Endocrinol Metabol. 2006;50:603-620.
6. Kushida K, Takahashi M, Kawana K, Inoue T.Comparison of markers for bone formation and resorptionin premenopausal and postmenopausal subjects, and osteo-porosis patients. J Clin Endocrinol Metab. 1995;80:2447-2450.
7. Seibel MJ. Biochemical markers of bone metabolism inthe assessment of osteoporosis: useful or not? J EndocrinolInvest. 2003;26:464-471.
8. Stepan JJ. Clinical utility of bone markers in the evalua-tion and follow-up of osteoporotic patients: why are themarkers poorly accepted by clinicians? J EndocrinolInvest. 2003;26:458-463.
9. Seibel MJ, Lang M, Geilenkeuser WJ. Interlaboratoryvariation of biochemical markers of bone turnover. ClinChem. 2001;47:1443-1450.
10. Abrahamsen B, Vestergaard P, Rud B, et al. Ten-yearabsolute risk of osteoporotic fractures according to BMD Tscore at menopause: the Danish Osteoporosis PreventionStudy. J Bone Miner Res. 2006;21:796-800.
11. Johnell O, Kanis JA, Oden A, et al. Predictive value ofBMD for hip and other fractures [published correctionappears in J Bone Miner Res. 2007;22:774]. J Bone MinerRes. 2005;20:1185-1194.
12. Majima T, Shimatsu A, Komatsu Y, et al. Associationbetween baseline values of bone turnover markers andbone mineral density and their response to raloxifene treat-ment in Japanese postmenopausal women with osteoporo-sis. Endocr J. 2008;55:41-48.
13. Yu SL, Ho LM, Lim BC, Sim ML. Urinary deoxypyridin -oline is a useful biochemical bone marker for the manage-ment of postmenopausal osteoporosis. Ann Acad MedSingapore. 1998;27:527-529.
14. Vesper HW, Audain C, Woolfitt A, et al. High-perfor-mance liquid chromatography method to analyze free andtotal urinary pyridinoline and deoxypyridinoline. AnalBiochem. 2003;318:204-211.
15. Kitatani K, Nakatsuka K, Naka H, Miki T, Morii H,Nishizawa Y. Clinical usefulness of measurements of uri-nary deoxypyridinoline (DPD) in patients with post-menopausal osteoporosis receiving intermittent cyclicaletidronate: advantage of free form of DPD over total DPD
in predicting treatment efficacy. J Bone Miner Metab.2003;21:217-224.
16. Seibel MJ. Biochemical markers of bone turnover, part I:biochemistry and variability. Clin Biochem Rev. 2005;26:97-122.
17. Kanis JA, Johnell O, Oden A, Johansson H, McCloskeyE. FRAX and the assessment of fracture probability in menand women from the UK. Osteoporos Int. 2008;19:385-397.
18. Chaki O, Yoshikata I, Kikuchi R, et al. The predictivevalue of biochemical markers of bone turnover for bonemineral density in postmenopausal Japanese women. JBone Miner Res. 2000;15:1537-1544.
19. Desai MP, Bhanuprakash KV, Khatkhatay MI, DondeUM. Age-related changes in bone turnover markers andovarian hormones in premenopausal and postmenopausalIndian women. J Clin Lab Anal. 2007;21:55-60.
20. Harinarayan CV, Ramalakshmi T, Venkataprasad U.High prevalence of low dietary calcium and low vitamin Dstatus in healthy south Indians. Asia Pac J Clin Nutr. 2004;13:359-364.
21. Papakitsou EF, Margioris AN, Dretakis KE, et al. Bodymass index (BMI) and parameters of bone formation andresorption in postmenopausal women. Maturitas. 2004;47:185-193.
22. Zhao LJ, Liu YJ, Liu PY, Hamilton J, Recker RR,Deng HW. Relationship of obesity with osteoporosis. JClin Endocrinol Metab. 2007;92:1640-1646.
23. Desai Meena P, Khatkhatay MI, Bhanu Prakash KV,Savardekar LS, Shah RS, Ansari Z. Hormonal profilesand biochemical indices of bone turnover in Indian women.Osteoporos Int. 2007;18:923-929.
24. Garnero P, Sornay-Rendu E, Chapuy MC, Delmas PD.Increased bone turnover in late postmenopausal women isa major determinant of osteoporosis. J Bone Miner Res.1996;11:337-349.
25. Uemura H, Yasui T, Miyatani Y, et al. Circulating pro-files of osteoprotegerin and soluble receptor activator ofnuclear factor kappaB ligand in post-menopausal women.J Endocrinol Invest. 2008;31:163-168.
26. Bhattacharyya S, Siegel ER, Achenbach SJ, Khosla S,Suva LJ. Serum biomarker profile associated with highbone turnover and BMD in postmenopausal women. JBone Miner Res. 2008;23:1106-1117.
Bone Markers and Bone Density, Endocr Pract. 2008;14(No. 9) 1107