Embed Size (px)
Citation preview

ARTICLE OPEN ACCESS
Cortical topological network changes followingoptic neuritisYael Backner MSc Ido Ben-Shalom BMedSc Joseph Kuchling MD Nadja Siebert MD Michael Scheel MD
Klemens Ruprecht MD Alexander Brandt MD Friedemann Paul MD and Netta Levin MD PhD
Neurol Neuroimmunol Neuroinflamm 20207e687 doi101212NXI0000000000000687
Correspondence
Dr Levin
nettahadassahorgil
AbstractObjectiveTo differentiate between visual cortical network topology changes following optic neuritis(ON) stemming from different inflammatory disease types we used mathematical graphtheoryndashbased tools to analyze functional imaging data
MethodsSixty-two patients were recruited into this cross-sectional study 23 of whom had neuromyelitisoptica spectrum disorder (NMOSD) with ON 18 with clinically isolated syndrome (CIS)-ONand 21 with other CIS episodes Twenty-six healthy controls (HCs) were also recruited Allparticipants underwent resting-state functional MRI Visual networks were defined using 50visual regions of interest Analysis included graph theory metrics including degree densitymodularity and local and global efficiency
ResultsVisual network density shows decreased connectivity in all patient groups compared with con-trols A higher degree of connections is seen in both ON groups (CIS and NMOSD) comparedwith the the non-ON group This pattern is most pronounced in dorsal-lateral regions In-formation transfer efficiency and modularity were reduced in both CIS groups but not in theNMOSD group compared with the HC group
ConclusionsVisual network density appears affected by the neurologic deficit sustained (ON) and connec-tivity changes are more evident in dorsal-lateral regions Efficiency and modularity appear to beassociated with the specific disease type (CIS vs NMOSD) Thus topological cortical changes inthe visual system are associated with the type of neurologic deficit within the limits set on them bythe underlying pathophysiologyWe suggest that cortical patterns of activity should be consideredin the outcome of the patients despite the localized nature of ON
These authors are equally contributing last authors
From the fMRI Unit (YB IB-S NL) Neurology Department Hadassah-Hebrew University Medical Center Jerusalem Israel Experimental and Clinical Research Center (JK NSAB FP) Max Delbrueck Center for Molecular Medicine and CharitendashUniversitatsmedizin Berlin Germany NeuroCure Clinical Research Center (JK NS MS AB FP)CharitendashUniversitatsmedizin Berlin Freie Universitat Berlin Humboldt-Universitat zu Berlin and Berlin Institute of Health Department of Neurology (JK KR FP) CharitendashUniversitatsmedizin Berlin Freie Universitat Berlin Humboldt-Universitat zu Berlin and Berlin Institute of Health Germany Department of Neuroradiology (MS) CharitendashUniversitatsmedizin Berlin Germany and Department of Neurology (AB) University of California Irvine
Go to NeurologyorgNN for full disclosures Funding information is provided at the end of the article
The Article Processing Charge was funded by the authors
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License 40 (CC BY-NC-ND) which permits downloadingand sharing the work provided it is properly cited The work cannot be changed in any way or used commercially without permission from the journal
Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the American Academy of Neurology 1
Following an MS episode recovery involves the resolving ofinflammation and remyelination However other processessuch as functional cortical network changes may also havea role to play1 Whether such changes are driven by the spe-cific neurologic deficit experienced by the patient or by theunderlying disease pathophysiology and are they specific tocertain regions are questions that remain unanswered
The visual system is a suitable model to address this Althoughoptic neuritis (ON) is a shared neurologic deficit of both MSand neuromyelitis optica spectrum disorder (NMOSD) 2distinct CNS inflammatory diseases in patients with MS thesame underlying pathophysiology may or may not involve theoptic nerve23
NMOSD and MS differ in their pathophysiologic mecha-nisms while in MS demyelination is the primary damagemechanism in NMOSD it is secondary to astrocytopathyand thus the damage is considered more severe4 Further-more as NMOSD is antibody mediated it is more localized toregions containing the antibody target (aquaporin-4)5 Thesedifferences in severity and damage distribution suggest thatcortical network changes following ON may differ in the 2disease types
Moreover our previous works have emphasized the impor-tance of activity along the visual dorsal stream in patients withON6ndash10 but our works on connectivity have used whole-network resolution1011 Therefore to examine whether thereare specific connectivity changes within the visual network weherein used graph theory methods1213 focusing on its regionalmeasures to pinpoint which visual regions are more affected
MethodsParticipantsSixty-two patients were prospectively recruited into this cross-sectional study at the NeuroCure Clinical Research CenterCharite-Universitatsmedizin Berlin including 18 patients withON in context of clinically isolated syndrome (CIS) 21patients with CIS with nonvisual episodes (CISndashnonopticneuritis [nON]) and 23 patients with NMOSD and previousON Since enrollment in the study 3 patients with CIS-ONand 5 patients with CIS-nON have been diagnosed with earlyrelapsing-remitting MS according to the 2010 revised McDo-nald criteria14 Patients with NMOSD met the internationalconsensus diagnostic criteria for NMOSD15 In addition 26healthy controls (HCs) were also recruited (table 1) Data fromthese cohorts have been previously published101617
Standard protocol approvals registrationsand patient consentsThe study was approved by the Charite-UniversitatsmedizinBerlin ethics committee and was conducted in accordancewith the Declaration of Helsinki18 Written informed consentwas obtained for each participant
Data acquisition and analysisMRI data were acquired on a 3T scanner (Magnetom TrioSiemens Erlangen Germany) using a 12-channel head coilAnatomic sequences included high-resolution T1-weightedimages (MPRAGE sequence repetition time [TR]echo time[TE] = 1900303 ms field-of-view [FOV] 256 times 256 mm2matrix 256 times 256 176 slices slice thickness 1 mm) and fluid-attenuated inversion recovery (FLAIR)-weighted images 3DFLAIR images (3D FLAIRTETR = 60002100388 msFOV240times 240mm2matrix 240 times 240 176 slices slice thickness1 mm) of all patients were checked and verified for T2 lesions by3 expert raters under the supervision of a board-certified radi-ologist Whole-brain segmentation and quantification of lesionsof FLAIR images were performed using ITK-SNAP (itksnaporg)19 Further lesion analysis was performed using the mrVistasoftware package (VISTA Lab Stanford University)
Resting-state functional MRI (RS-fMRI) measurements wereobtained with an echo-planar imaging sequence (TRTE =225030 ms FOV = 218 times 218 mm2 matrix 64 times 64 37 slicesslice thickness 34 mm sequence duration 9 minutes) Subjectswere instructed to lie still with their eyes closed Functionalimaging data preprocessing and analysis were performed usingthe BrainVoyager software package version 206 (Brain In-novation) Data underwent slice scan time correction motioncorrection and high-pass temporal filtering by BrainVoyagerdefault parameters to remove drift and improve the signal-to-noise ratio Functional images were coregistered to the anatomicimages using trilinear interpolation and transformed intoMontreal Neurological Institute space Each participantrsquos scanwas verified to include the entire brain with particular attentionto the occipital lobe Each scanwasmanually checked for quality
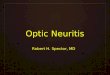
Network constructionComplex network analysis is based on graph theory a mathe-matical approach to networks Briefly the method requiresdefinition of brain regions as nodes and the search for con-nections or edges between those nodes These connectionsanatomic or functional can then be thresholded and binarizedinto connectivity matrices representing the existence or lack ofconnection between any 2 nodes in the network From thesematrices various measures can be extracted to quantify net-work topology and organization (figure 1)
GlossaryCIS = clinically isolated syndrome EDSS = Expanded Disability Status Scale FEF = frontal eye field FLAIR = fluid-attenuatedinversion recoveryHC = healthy controlNMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritisON =optic neuritis ROI = region of interest RS-fMRI = resting-state functional MRI
2 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
Visual network node definitionAs we focus in our studies on the visual system visual networknodes were defined using the probabilistic atlas ofWang et al20
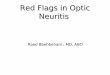
created in Montreal Neurological Institute space and used invisual systemndashrelated studies21ndash24 which afforded us the levelof detail we needed The constructed networks included 50regions of interest (ROIs) (25 per hemisphere 8 ventral-temporal regions 9 dorsal-lateral regions and 8 parietal-frontalregions figure 2A table e-1A linkslwwcomNXIA207) eachrepresenting a node Because of the variety in ROI sizeswishing to minimize bias of variations in ROI size on estimatesof connectivity and signal-to-noise ratio differences the ROIswere arbitrarily constricted to a set size of 5 times 5 times 5 voxelspositioned at the center of each atlas-defined ROI The specificsize was set so that all constricted regions would be within theborders of their respective original ROIs
Motor network node definitionIn addition to the visual network we wished to examinewhether similar changes to those in the visual network ofpatients with ON may also be found in other networksin patients with corresponding CIS episodes As many of thepatients withCIS-nONhave experiencedmotor symptoms themotor network was also defined based on the Harvard-Oxfordcortical and subcortical structural atlas included in FMRIBSoftware Library25 and on several motor networkndashrelatedstudies26ndash28 The constructed networks included 12 ROIs (6per hemisphere figure 2B table e-1B linkslwwcomNXIA207) The selected ROIs were pure motor regions to provideus with a clean cutoff between networks and participants andno overlap existed between the 2 networks used ROIs wereconstricted to 125 voxels as in the visual network Because ofthe variety of CIS episodes included in the CIS-nON group for
Table 1 Study cohort description
HC CIS-ON CIS-nON NMOSD
Subjects (n) 26 18 21 23
Sex (f [m]) 22 (4) 11 (7) 11 (10) 20 (3)
Age (y mean plusmn SD) 437 plusmn 157 312 plusmn 77ab 334 plusmn 86ab 467 plusmn 145
Disease duration (mo mean plusmn SD) NA 463 plusmn 515a 540 plusmn 667a 9417 plusmn 9572
EDSS score (median range) NA 15 (0ndash35)a 15 (0ndash40)a 40 (0ndash65)
RRMS NA 3 5 NA
AQP4-ab-positive (n) NA NA NA 19
Bilateral ON NA NA NA 4
High-contrast visual acuity 102 plusmn 032 091 plusmn 034 101 plusmn 034 075 plusmn 047
Global lesion volume and number(cm3 n mean plusmn SD)
NA 252 plusmn 312 2144 plusmn 2266 369 plusmn 553 2323 plusmn 2235 258 plusmn 394 1674 plusmn 1937
Abbreviations AQP4 = aquaporin-4 CIS = clinically isolated syndrome EDSS = Expanded Disability Status Scale HC = healthy control NA = not applicableNMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritis ON = optic neuritis RRMS = relapsing-remitting MSa Significantly different than the NMOSD group p lt 001b Significantly different than the HC group p lt 001
Figure 1 Visualization of the translation process from atlas to brain network
(A) Original Wang et al20 atlas as transformed into BrainVoyager (B) Creating thresholded and binarized matrices representing all the connections in bothhemispheres (C) A visual network graph representation (healthy control group)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 3
the motor network analyses we have further divided the CIS-nON group into patients with motor symptoms (CIS-nON-motor n = 10) and with other nonmotor symptoms mainlysensory (CIS-nON-other n = 11)
Matrix preparationThe average RS-fMRI time course of all voxels within eachROI was extracted and Pearson correlation coefficientsrepresenting connectivity strength between regions werecalculated between each pair of ROIs in each hemisphereresulting in two 25 times 25 hemispheric visual matrices for eachsubject and two 6 times 6 motor matrices Each correlationmatrix was thresholded and binarized at a range of corre-lation thresholds (01ndash05 for the visual network and01ndash02 for the motor network at increments of 005) Thehighest correlation threshold was set as the last threshold inwhich all subjects still had any connection between ROIsFour patients with CIS-ON and 2 patients with CIS-nONdid not have connections in the highest threshold of themotor network Analyses have been performed with andwithout these patients and no significant differences werefound
Network analysisBoth local and global network properties were studied usingthe MATLAB Brain Connectivity Toolbox12 Here we brieflylist the network analysis metrics chosen to characterize thenetworks All parameters were integrated over the variousthresholds used to create a single value for analysis Graphspresenting the metrics used over the entire range of correla-tion thresholds are presented in figure e-1 (linkslwwcomNXIA207) It should be noted that most metrics chosencould not be used in the motor network because of the smallnumber of regions used and the largely disconnected net-works obtained
Basic network topology analysisTo characterize the general structure of the network in thelocal (nodal) level the nodal degree of the various ROIs wasexplored The group mean degree of each given ROI wascompared between groups to examine changes followingON and verify whether any region or subdivision of regionsshowed greater change Network density the proportion ofexisting connections in the network out of all possibleconnections based on the entire networkrsquos degree was also
Figure 2 Regions of interest (ROIs) used
(A) Visual network ROIs color coded according to classification in Wang et al20mdashventral-temporal (red) dorsal-lateral (blue) and parietal-frontal (green) (B)Motor network ROIs Visualization created using Xia M et al55 d = dorsal FEF = frontal eye field hMT = human middle temporal region hV4 = human visualregion V4 IFG = inferior frontal gyrus IPS = intraparietal sulcus LO = lateral occipital cortexM1 = primarymotor cortexMST =medial superior temporal areaPO = pars opercularis PT = pars triangularis SMA = supplementary motor area SPL = superior parietal lobule v = ventral VO = ventral occipital cortex V1 =primary visual cortex V2 = secondary visual cortex V3 = visual area V3
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
calculated and compared to examine the global networkdifferences between groups
Global network analysisTo examine the topological organization of the studiednetworks 6 global network metrics were explored Becausethis study explored only nodes within the visual system wewere interested in seeing whether small-worldness a ubiq-uitous trait reported in brain networks also exists within thevisual network To that end we included 4 parameters usedto calculate small-worldnessmdashclustering coefficient Cpharmonic mean of shortest path lengths Lp and their nor-malized counterparts These were defined as in references 29and 30 A typical small-world network should exhibit γ gt 1and λ asymp 1 The harmonic mean was chosen rather than themore commonly used characteristic path length becausemost of the networks in our study are at least partially dis-connected and therefore have infinite characteristic pathlength31
To examine segregation and integration within the visualnetwork we first looked at the 2 efficiency metrics the globaland local efficiency parameters Global efficiency is the re-ciprocal of the harmonic mean thought to represent howefficiently information is exchanged within the networkLocal (or nodal) efficiency is defined for the single nodelocalizing global efficiency effects to specific nodes givinga measure of how well that region is integrated within thenetwork32
To further examine segregation and integration we alsocalculated modularity33 This measure of network segrega-tion quantifies the degree to which the network may besubdivided into nonoverlapping groups of ROIs whichare densely interconnected within and sparsely connectedwithout
Statistical analysisData were examined for normality using QQ-plots andShapiro-Wilk tests The results variables were non-normallydistributed and thus for univariate comparisons betweengroups we used the Kruskal-Wallis test To assess the in-dependent effect of group designation on the result varia-bles after checking compliance with model assumptionsmultivariate linear models were built using age sex andExpanded Disability Status Scale (EDSS) score as cova-riates Statistical significance was assessed at p lt 005 levelTo control the false discovery rate multiple comparisoncorrection was performed using the Benjamini-Hochbergmethod All calculations were performed using R version351 (R Foundation for Statistical Computing ViennaAustria)
Data availabilityThe data sets generated for this study are available on requestfrom the corresponding author
ResultsResearch cohort characteristicsA summary of demographic and clinical measures is presentedin table 1 Differences were found in age disease duration andEDSS score between the 2 CIS groups and the HC andNMOSD groups (p lt 001 for all comparisons) Malefemaleratios were also different between those groups Thereforeage sex and EDSS score were added as covariates to allanalyses and were found to have no effect on the resultsDisease duration was not included as a covariate because itwas highly correlated with age of patients (p = 0007) Visualacuity did not significantly differ between any of the groupsand therefore was not included as covariate either
No significant differences were found in lesion numbervolume or specific location in the 3 patient groups Nosignificant differences were found between hemispheres inany of the metrics However significant results betweengroups were more pronounced in the left hemisphere andtherefore only these results are presented For the motornetwork significant results were found only in the righthemisphere and those are the results presented Results forthe unpresented hemispheres can be seen in the supple-mental materials (linkslwwcomNXIA207)
Visual network results
Small-worldness apparent in visual networksBy the criteria defined for small-worldness the healthy visualnetwork appears to display a small-world structure All theparticipants in the HC group have shown properties within thecriteria (λ values were nearly 1 in all participants and thresholdsγ values were mostly higher than 1 barring a few inconsistentexceptions) The same was shown in the patient groups ex-cluding 1 patient with CIS-ON and 1 patient with CIS-nONwho failed to meet the γ gt 1 criterion To verify whether thisdeviation from criteria somehow influences our group resultsanalyses were performed with and without these patients andno significant differences were found so both were included inthe results The small-world criteria curves for each group arepresented in figure e-2 (linkslwwcomNXIA207)
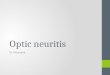
Basic network topology patternsFigure 3 presents a visualization of the visual network for the 4groups The normal network displayed by the HC cohort(figure 3A) appears to be more connected than all 3 patientgroups (figure 3 BndashD) in all 3 region subdivisions (ventral-temporal in red dorsal-lateral in blue and parietal-frontal ingreen) The NMOSD group (figure 3B) and the CIS-ONgroup (figure 3C) are quite similar in appearance and betterconnected than the CIS-nON group (figure 3D) which dis-plays the highest disconnection
This connectivity pattern according to which HCs gt NMOSDCIS-ONgtCIS-nON is seen globally using the densitymetricHC density (028 plusmn 009) is higher than CIS-nON density (019
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 5
plusmn 01 p = 00009) and it is higher though not significantly sothan the density of theCIS-ONgroup (022 plusmn 01 p= 005) TheNMOSD group (024 plusmn 01) density was higher than that of theCIS-nON group but not significantly so (p = 006) No signif-icant differences were found between the CIS-ON andNMOSDgroups or between the NMOSD and HC groups
Themean degree of theHC groupwas significantly higher thanthat of the CIS-nONgroup in all visual regions although not allsurvived multiple comparison correction Most survivingcomparisons were in low-order and dorsal-lateral regions(lower-ventral V1v and V2v lower-dorsal V1d V2d and V3ddorsal-lateral MST hMT and V3b frontal-parietal IPS0IPS1 and IPS2)
In addition the pattern found using the density metric bywhich HCs gt NMOSD CIS-ON gt CIS-nON exists mostlyin the dorsal-lateral region subdivision The ventral-temporalsubdivision (excluding the very early regions V1v and V2v)generally shows no significant differences between groups Theparietal-frontal subdivision shows either no significant differ-ences between groups at all (IPS3 IPS4 and IPS5) or a patternwhere the 2 CIS groups show no difference between them butlower mean degree than both the HC and NMOSD groups(SPL1 frontal eye field [FEF] p = 006) Figure 4 shows anexample from each subdivision displaying the emerging pat-terns The average degrees for each ROI can be found in tablee-2 (linkslwwcomNXIA207)
Network segregation and integration patternsAll segregation and integration metrics reveal connectivitydifferences unlike those for the basic network topologyshowing a pattern by which HC NMOSD gt CIS-ON CIS-nON This is in contrast to the basic topology pattern(achieved using the degree and density metrics) which high-lighted the similarity in topology in different diseases sharingthe same neurologic deficit (HC gt NMOSD CIS-ON gtCIS-nON)
Modularity results (figure 5A) show differences between theHC and CIS-nON groups (039 plusmn 005 and 03 plusmn 008 re-spectively p = 0004) as well as between the NMOSD (037 plusmn005) and CIS-nON groups (p = 0016) but no significantdifferences between the HC and NMOSD groups Themodularity result of the CIS-ON group (033 plusmn 009) is notsignificantly different from any of the other groups but isquantitatively closer to the CIS-nON group
The harmonizedmean of the characteristic path length (figure5B) shows a difference between the HC and CIS-nON groups(075 plusmn 044 and 256 plusmn 291 respectively p = 001) Althoughthe difference between the CIS-nON and NMOSD groups(083 plusmn 037 p = 0087) is not significant the NMOSD groupdisplays a shorter path length The harmonized mean of theCIS-ON group (211 plusmn 279) was not significantly differentfrom any of the groups and no significant difference wasfound between the HC and NMOSD groups
Figure 3 Visualization of the visual system for the 4 subject groups
Considered at correlation threshold r = 05 shown in the coronal (back view top) sagittal (lateral left hemisphere viewmiddle) and axial (dorsal view bottom)planes Nodes (regions of interest) are color coded according to their classification inWang et al20mdashventral-temporal (red) dorsal-lateral (blue) and parietal-frontal (green) The size of nodes reflects the relative degree of a given region in the network Disconnected regions are presented using an arbitrarily selectedsize for visualization purposes Visualization created using reference 55 CIS = clinically isolated syndrome NMOSD = neuromyelitis optica spectrumdisordernON = nonoptic neuritis ON = optic neuritis
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
Similarly global efficiency (figure 5C) shows change betweenthe HC and CIS-nON groups (035 and 025 respectively p =0008) Again no significant difference was found betweenthe NMOSD (031) and CIS-nON groups (p = 0093) butthe NMOSD group quantitatively shows higher efficiencyThe CIS-ON group once again shows no significant differ-ences (028) from any group but is between the NMOSD andCIS-nON groups in terms of global efficiency
Local efficiency showed similar results with differences foundbetween the CIS-nON group and the HC and NMOSDgroups though mostly in high-order regions particularly in thedorsal-lateral and parietal-frontal region subdivisions (lower-ventral V1v CIS-nONvsHCs only lower-dorsal V3d dorsal-lateral MST hMT V3a CIS-nON vs HCs only LO1 LO2V3b CIS-nON vs HCs and NMOSD frontal-parietal IPS3IPS4 IPS5 SPL1 vs HCs only IPS2 FEF vs HCs andNMOSD regions V3b IPS3 IPS5 have also shown significant
differences between HCs and CIS-ON) Details on local effi-ciency for each ROI can be seen in table e-3 (linkslwwcomNXIA207)
Motor network resultsDifferences between groups were found using the degreemetric in the motor putamen between the HC group whichwas most connected (054) and all patient groups (CIS-ON028 CIS-nON-motor 0225 CIS-nON-other 028 p lt 001for all) except for the NMOSD group (038 p = 01 aftermultiple comparison correction) No significant differenceswere found between any patient groups
In the pars opercularis (inferior frontal gyrusndashpars opercularis)differences were found between the CIS-nON-motor group(025) and the HC (057 p = 0004) and NMOSD (049p = 003) groups Density and global efficiency metrics alsoshow differences between the HC group and the CIS-nON-
Figure 4 Average degree of all 4 subject groups for selected regions of the 3 region subdivisions
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) hMT (dorsal-lateral subdivision) (B) VO1 (ventral-temporal subdivision) (C) FEF(frontal eye field parietal-frontal subdivision) Significantly different than HC CIS = clinically isolated syndrome HC = healthy control hMT = humanmiddletemporal region NMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritis ON = optic neuritis
Figure 5 Segregation and integration metrics for all 4 subject groups
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) Modularity (B) harmonizedmean of characteristic path length (C) global efficiencySignificantly different thanHC Significantly different thanNMOSD CIS = clinically isolated syndrome HC = healthy control NMOSD = neuromyelitis opticaspectrum disorder nON = nonoptic neuritis ON = optic neuritis
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 7
motor group (density HCs 012 CIS-nON-motor 007 p =0005 efficiencyHCs 014 CIS-nON-motor 009 p = 0001)Density also shows difference between the HC group and theCIS-ON group (011 p = 004) Other comparisons did notsurvive correction but surprisingly the general pattern remainshere similarly to the visual network HCs gt NMOSD gt CIS-ON CIS-nON-other gt CIS-nON-motor Results are pre-sented in figure e-3 (linkslwwcomNXIA207)
DiscussionIn this study we addressed visual cortical network patterns ininflammatory diseases following ON To that end we included2 prototypic autoimmune CNS diseases with distinct un-derlying pathophysiology MS and NMOSD3435 These dis-eases both share visual dysfunction caused by ON as clinicalcommonality Through these 2 disease types we haveattempted to discover whether changes to the visual systemfollowing ON are driven just by the specific neurologic visualdeficit or also by the underlying pathophysiology We usedgraph analysis methods to investigate topological and localchanges in resting-state visual networks of patients in those 2disease groups further dividing theMS group into patients withand without ON
Our main findings showed 2 distinct patterns of change in thevisual networks of the patient groups First the highly con-nected normal visual network is affected in all 3 diseasegroups showing reduced density and changes in topologyThese differences from HCs however are most pronouncedin the CIS-nON group The 2ON groups (NMOSD and CIS-ON) showed remarkably similar results in density and degreedistribution particularly in lower and dorsal-lateral regionsboth higher than those of patients with CIS-nON This sug-gests changes unique to the directly affected system (visualinput) We cautiously suggest that these changes may reflectan attempt to compensate for the damage incurred lastingeven when the underlying pathology has existed for yearsconsidering the relatively long disease durations displayed bythe NMOSD compared with the CIS-ON group
Second measures of network segregation and integration de-fining efficiency of information transfer and local structureshowed similarity between the MS-background groups (CIS-ON and CIS-nON) whereas the NMOSD group showedresults closer to those of the HCs This suggests that networksegregation and integration may be more affected by type ofunderlying pathophysiology rather than the specific neurologicdeficit
The question of whether cortical reorganization plays a role inrecovery from ON has long been discussed Early studies fo-cused mainly on cortical activity patterns in response to visualtasks presented to the affected eye Some studies have sug-gested that adaptive cortical plasticity following ON involvesincreased activity in higher visual areas assisting in overcoming
visual insult36ndash39 However later studies suggested that corticalactivation reflects the visual percept rather than demonstratesplasticity8 In recent years the importance of considering cor-tical networks rather than regional activity has emergedFunctional connectivity assessing the synchronized fluctua-tions in the fMRI signal between regions has shown sensitivityto neurologic damage and so it was suggested that connectivityrather than activity may play a role in clinical outcome How-ever as this is a cross-sectional study and no clinical measureswere included this remains hypothetical
InMS andNMOSDmuch emphasis has been given to changesin functional connectivity in sensorimotor networks Func-tional connectivity within the motor network was found toreflect motor function40 and to change in response to re-habilitative intervention41 in patients with MS Whether suchchanges reflect compensatory mechanisms or loss of function isstill a matter of debate4243 It has been suggested that theinterpretation of such observations depends on lesion load anddisease duration44
Our motor network results show no compensatory changes inthe subgroup of nON patients with motor symptoms On thecontrary specific clinical motor involvement resulted in re-duced connectivity within the motor cortex These results areparticularly prominent in view of the opposite results obtainedin the visual network where the relevant neurologic deficitseemed to be associated with elevated connectivity We suggestthat this may be the result of lesions located close to motorregions compared with the more peripheral damage sustainedthrough ON causing greater direct damage to the systemAnother piece of evidence supporting this suggestion is thedenser motor network seen in the NMOSD group who almostall had myelitis in addition to ON (19 of 23 patients) Thisfinding may be the motor networkrsquos equivalent of response todistant damage However because of the small numbers ofpatients included in the nonmotor subgroup and of patientswith nonmyelitis NMOSD these speculations should be takenwith caution
Although much attention has been given to the motor net-works in recent years the visual system has received less at-tention usually as a small part of a wider study4345 A studyfocusing on the visual system of patients with NMOSD andprevious ON has shown increase in the functional connectivityof the primary visual network compared with those withoutON11 These findings were also associated with greater retinaldamage and reduced visual acuity suggesting an attempt atcortical reorganization Similar findings were seen in our pre-vious work showing an increase in visual network connectivityin patients with CIS-ON compared with CIS-nON10 AMEGOCT study of the visual system in patients with MS has suc-ceeded in differentiating between patients with and withoutON based on a unique pattern of connectivity that specificallyinvolves the visual system46 These studies mostly focus on theneurologic deficit as the driving force behind the effects ob-served in MS and NMOSD connectivity and are congruent
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
with the general connectivity patterns presented in our currentstudy
However another cause for connectivity change may be thespecific type of disease Very few studies have tried to compareconnectivity between these 2 similar yet dissimilar diseasegroups Of these one has studied the functional and structuralconnectivity of the thalamus finding structural changes inboth diseases but functional disconnection only in MS47
Another study used a wide array of tests to differentiate be-tween the 2 disease types showing that the top 2 modalitiesuseful in this were white matter lesion load and functionalconnectivity48 In our results the white matter lesion elementappears negligible because both groups exhibit similar lesionnumber and volume and even lesion distribution was notlocalized in any of the groups And yet the segregation andintegration patterns of the functional visual network differedbetween MS and NMOSD with those of the latter moreclosely resembling that of HCs We suggest that this markeddifference may stem from differences in normal-appearingwhite matter Diffusion tensor imaging studies have showndiffusion abnormalities in both disease types but patientswith MS display widespread and more severe degree ofabnormality49ndash51 This may explain the difference in the seg-regation and integration properties of functional connectivitybetween the 2 groups
The use of graph-based analysis has enabled us to explore boththese driving forces of connectivity alterations the specificneurologic deficit and the disease type itself that appear to beassociated with different types of change Another advantageof this method is its ability to examine connectivity not only ina holistic manner In a work from 2015 the advantage ofgraph-based analysis inMS was presented Although emphasiswas on cognitive changes it was suggested that graph theoryshould be used to overcome the simplistic and incompleteinterpretations of previous methods52 Work on functionalconnectivity of the visual network in MS over the years hasmainly examined the network as a single entity using in-dependent component analysis1053 or seed-region analysis54
However the introduction of graph theory methods12 hasopened new possibilities in studying the affected network InMS the different works report both decreased global con-nectivity attributed to disease course and adaptation patternswith increased local connectivity and modularity13 Our cur-rent findings highlighting reorganization in dorsal-lateralregions known to be involved in dynamic perception pro-cesses are consistent with our previous works that emphasizedpersistent motion perception impairment following ON78
Based on our previous works in the field we suggest that thedorsal stream-specific increase in connectivity in our currentstudy may be part of a recovery process involving functionalmodifications Because bothON groups exhibit such a patternthis supports the notion that the neurologic deficit elicits thesechanges As this is a cross-sectional study this remains onlya suggestion
This study has several limitations First graph theorymethods are often used on larger subject groups Howeverthe significance of the results and their consistency with ourprevious findings convince us that our current findings aretrue Second the differences in age in all groups and indisease duration between the disease groups are problem-atic but these measures were factored into the variousanalyses and had no significant influence on the resultsThird our assumptions regarding the existence of com-pensatory mechanisms are based on the patterns emergingand former findings of our research Further light could havebeen shed on the matter had behavioral measures beenincluded as well as a longitudinal design It should be fur-ther noted that this study analyzed only functional con-nections within the visual system without the addedinformation that could have been gleaned from the com-plementing structural connectome limiting the ability todisentangle compensatory changes from structural damageFurthermore although the differences between groups mayindeed be interpreted as reorganizational changes of thevisual network in response to damage they may also reflectdifferential level of damage between individuals This issueshould be further investigated using a different study designbecause it could not be covered under the scope of thecurrent study
To conclude the visual network highly connected inHCs is made less connected by disease be it MS orNMOSD However a higher degree of connections wasobserved in the ON groups (CIS-ON and NMOSD)compared with the nON group This suggests that thesystem responds to specific damage caused to the anteriorvisual pathway bringing connectivity closer to that ofa normal network regardless of disease type On the otherhand network segregation and integration and the effi-ciency of information transfer appear more affected bydisease type altered in the MS groups but not inNMOSD particularly in higher regions Therefore wesuggest that the response to damage is dependent on thetype of neurologic deficit within the limitations of theunderlying pathophysiology
Study fundingSupported by the National Multiple Sclerosis Society (researchgrant RG-1802-30165) and the Applebaum Foundation FPaul was supported by Deutsche Forschungsgemeinschaft(DFG Exc 257)
DisclosureY Backner I Ben-Shalom J Kuchling N Siebert M ScheelK Ruprecht A Brandt F Paul and N Levin report no dis-closures Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationOctober 11 2019 Accepted in final form January 10 2020
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 9
References1 Schoonheim MM Filippi M Functional plasticity in MS Friend or foe Neurology
2012791418ndash14192 Costello F Vision disturbances in multiple sclerosis Semin Neurol 201636185ndash1953 Abel AMcClelland C LeeMS Critical review typical and atypical optic neuritis Surv
Ophthalmol 201964770ndash7794 Chen JJ Pittock SJ Flanagan EP Lennon VA Bhatti MT Optic neuritis in the era of
biomarkers Surv Ophthalmol 20206512ndash175 Lennon VA Wingerchuk DM Kryzer TJ et al A serum autoantibody marker of neu-
romyelitis optica distinction from multiple sclerosis Lancet 20043642106ndash21126 Raz N Chokron S Ben-Hur T Levin N Temporal reorganization to overcome
monocular demyelination Neurology 201381702ndash7097 Raz N Dotan S Chokron S Ben‐Hur T Levin N Demyelination affects temporal
aspects of perception an optic neuritis study Ann Neurol 201271531ndash5388 Raz N Dotan S Benoliel T Chokron S Ben-Hur T Levin N Sustained motion
perception deficit following optic neuritis Behavioral and cortical evidence Neurology2011762103ndash2111
9 Benoliel T Raz N Ben-Hur T Levin N Cortical functional modifications followingoptic neuritis Mult Scler 201723220ndash227
10 Backner Y Kuchling JMassarwa S et al Anatomical wiring and functional networkingchanges in the visual system following optic neuritis JAMANeurol 201875287ndash295
11 Finke C Zimmermann H Pache F et al Association of visual impairment in neu-romyelitis optica spectrum disorder with visual network reorganization JAMANeurol201875296ndash303
12 Rubinov M Sporns O Complex network measures of brain connectivity uses andinterpretations Neuroimage 2010521059ndash1069
13 Fleischer V Radetz A Ciolac D et al Graph theoretical framework of brain networksin multiple sclerosis a review of concepts Neuroscience 201940335ndash53
14 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
15 Wingerchuk DM Banwell B Bennett JL et al International consensus diagnosticcriteria for neuromyelitis optica spectrum disorders Neurology 201585177ndash189
16 Kuchling J Backner Y Oertel FC et al Comparison of probabilistic tractography andtract-based spatial statistics for assessing optic radiation damage in patients withautoimmune inflammatory disorders of the central nervous system Neuroimage Clin201819538ndash550
17 Oertel FC Kuchling J Zimmermann H et al Microstructural visual system changes inAQP4-antibodyndashseropositive NMOSD Neurol Neuroimmunol Neuroinflamm 20174e334 doi 101212NXI0000000000000334
18 Association WM World Medical Association Declaration of Helsinki ethical prin-ciples for medical research involving human subjects JAMA 20133102191
19 Yushkevich PA Piven J Hazlett HC et al User-guided 3D active contour segmen-tation of anatomical structures significantly improved efficiency and reliabilityNeuroimage 2006311116ndash1128
20 Wang L Mruczek RE Arcaro MJ Kastner S Probabilistic maps of visual topographyin human cortex Cereb Cortex 2014253911ndash3931
21 Hindy NC Ng FY Turk-Browne NB Linking pattern completion in the hippo-campus to predictive coding in visual cortex Nat Neurosci 201619665
22 Cichy RM Khosla A Pantazis D Torralba A Oliva A Comparison of deep neuralnetworks to spatio-temporal cortical dynamics of human visual object recognitionreveals hierarchical correspondence Sci Rep 2016627755
23 Cichy RM Pantazis D Oliva A Similarity-based fusion of MEG and fMRI revealsspatio-temporal dynamics in human cortex during visual object recognition CerebCortex 2016263563ndash3579
24 Mackey WE Winawer J Curtis CE Visual field map clusters in human frontoparietalcortex Elife 20176e22974
25 Smith SM Jenkinson M Woolrich MW et al Advances in functional and structuralMR image analysis and implementation as FSL Neuroimage 200423S208ndashS219
26 Pool E-M Rehme AK Eickhoff SB Fink GR Grefkes C Functional resting-stateconnectivity of the humanmotor network differences between right-and left-handersNeuroimage 2015109298ndash306
27 Hardwick RM Rottschy C Miall RC Eickhoff SB A quantitative meta-analysis andreview of motor learning in the human brain Neuroimage 201367283ndash297
28 Rocca MA Meani A Riccitelli GC et al Abnormal adaptation over time of motornetwork recruitment in multiple sclerosis patients with fatigue Mult Scler J 2016221144ndash1153
29 Watts DJ Strogatz SH Collective dynamics of ldquosmall-worldrdquonetworks Nature 1998393440ndash442
30 Maslov S Sneppen K Specificity and stability in topology of protein networks Sci-ence 2002296910ndash913
31 Newman ME The structure and function of complex networks SIAM Rev 200345167ndash256
32 Latora V Marchiori M Efficient behavior of small-world networks Phys Rev Lett200187198701
33 Newman ME Modularity and community structure in networks Proc Natl Acad SciUSA 20061038577ndash8582
34 Zamvil SS Slavin AJ Does MOG Ig-posit ive AQP4-seronegative opti-cospinal inflammatory disease justify a diagnosis of NMO spectrumdisorder Neurol Neuroimmunol Neuroinflamm 20152e62 doi 101212NXI0000000000000062
35 Zekeridou A Lennon VA Aquaporin-4 autoimmunity Neurol NeuroimmunolNeuroinflamm 20152e110 doi 101212NXI0000000000000110
36 Toosy AT Hickman SJ Miszkiel KA et al Adaptive cortical plasticity in higher visualareas after acute optic neuritis Ann Neurol 200557622ndash633
37 Jenkins TM Toosy AT Ciccarelli O et al Neuroplasticity predicts outcome of opticneuritis independent of tissue damage Ann Neurol 20106799ndash113
38 Werring DJ Bullmore ET Toosy AT et al Recovery from optic neuritis is associatedwith a change in the distribution of cerebral response to visual stimulation a func-tional magnetic resonance imaging study J Neurol Neurosurg Psychiatry 200068441ndash449
39 Levin N Orlov T Dotan S Zohary E Normal and abnormal fMRI activation patternsin the visual cortex after recovery from optic neuritis Neuroimage 2006331161ndash1168
40 Cordani C Meani A Esposito F et al Imaging correlates of hand motor performancein multiple sclerosis a multiparametric structural and functional MRI study MultScler 20191352458518822145
41 Fling BW Martini DN Zeeboer E Hildebrand A Cameron M Neuroplasticity of thesensorimotor neural network associated with walking aid training in people withmultiple sclerosis Mult Scler Relat Disord 2019311ndash4
42 Tommasin S De Giglio L Ruggieri S et al Relation between functional connectivityand disability in multiple sclerosis a non-linear model J Neurol 20182652881ndash2892
43 Castellazzi G Debernard L Melzer TR et al Functional connectivity alterationsreveal complex mechanisms based on clinical and radiological status in mild relapsingremitting multiple sclerosis Front Neurol 20189690
44 Tewarie P Steenwijk MD Brookes MJ et al Explaining the heterogeneity of func-tional connectivity findings in multiple sclerosis an empirically informed modelingstudy Hum Brain Mapp 2018392541ndash2548
45 Rocca MA Savoldi F Valsasina P et al Cross-modal plasticity among sensory net-works in neuromyelitis optica spectrum disorders Mult Scler 201925968ndash979
46 Tewarie P Balk LJ Hillebrand A et al Structure‐function relationships in the visualsystem in multiple sclerosis an MEG and OCT study Ann Clin Transl Neurol 20174614ndash621
47 Liu Y Duan Y Huang J et al Multimodal quantitative MR imaging of the thalamus inmultiple sclerosis and neuromyelitis optica Radiology 2015277784ndash792
Appendix Authors
Name Location Contribution
YaelBacknerMSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Designed andconceptualized the studyanalyzed the data draftedthe figures and draftedthe manuscript forintellectual content
Ido Ben-ShalomBMedSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Analyzed the motornetwork data
JosephKuchlingMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
NadjaSiebert MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
MichaelScheel MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
KlemensRuprechtMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
AlexanderBrandt MD
CharitendashUniversitatsmedizinBerlin Germany Universityof California
Major role in dataacquisition
FriedemannPaul MD
CharitendashUniversitatsmedizinBerlin Germany
Supervised the study andrevised the manuscript forintellectual content
Netta LevinMD PhD
Hadassah-HebrewUniversity Medical CenterJerusalem Israel
Conceptualized anddesigned the studysupervised the studyand drafted themanuscript forintellectual content
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

Following an MS episode recovery involves the resolving ofinflammation and remyelination However other processessuch as functional cortical network changes may also havea role to play1 Whether such changes are driven by the spe-cific neurologic deficit experienced by the patient or by theunderlying disease pathophysiology and are they specific tocertain regions are questions that remain unanswered
The visual system is a suitable model to address this Althoughoptic neuritis (ON) is a shared neurologic deficit of both MSand neuromyelitis optica spectrum disorder (NMOSD) 2distinct CNS inflammatory diseases in patients with MS thesame underlying pathophysiology may or may not involve theoptic nerve23
NMOSD and MS differ in their pathophysiologic mecha-nisms while in MS demyelination is the primary damagemechanism in NMOSD it is secondary to astrocytopathyand thus the damage is considered more severe4 Further-more as NMOSD is antibody mediated it is more localized toregions containing the antibody target (aquaporin-4)5 Thesedifferences in severity and damage distribution suggest thatcortical network changes following ON may differ in the 2disease types
Moreover our previous works have emphasized the impor-tance of activity along the visual dorsal stream in patients withON6ndash10 but our works on connectivity have used whole-network resolution1011 Therefore to examine whether thereare specific connectivity changes within the visual network weherein used graph theory methods1213 focusing on its regionalmeasures to pinpoint which visual regions are more affected
MethodsParticipantsSixty-two patients were prospectively recruited into this cross-sectional study at the NeuroCure Clinical Research CenterCharite-Universitatsmedizin Berlin including 18 patients withON in context of clinically isolated syndrome (CIS) 21patients with CIS with nonvisual episodes (CISndashnonopticneuritis [nON]) and 23 patients with NMOSD and previousON Since enrollment in the study 3 patients with CIS-ONand 5 patients with CIS-nON have been diagnosed with earlyrelapsing-remitting MS according to the 2010 revised McDo-nald criteria14 Patients with NMOSD met the internationalconsensus diagnostic criteria for NMOSD15 In addition 26healthy controls (HCs) were also recruited (table 1) Data fromthese cohorts have been previously published101617
Standard protocol approvals registrationsand patient consentsThe study was approved by the Charite-UniversitatsmedizinBerlin ethics committee and was conducted in accordancewith the Declaration of Helsinki18 Written informed consentwas obtained for each participant
Data acquisition and analysisMRI data were acquired on a 3T scanner (Magnetom TrioSiemens Erlangen Germany) using a 12-channel head coilAnatomic sequences included high-resolution T1-weightedimages (MPRAGE sequence repetition time [TR]echo time[TE] = 1900303 ms field-of-view [FOV] 256 times 256 mm2matrix 256 times 256 176 slices slice thickness 1 mm) and fluid-attenuated inversion recovery (FLAIR)-weighted images 3DFLAIR images (3D FLAIRTETR = 60002100388 msFOV240times 240mm2matrix 240 times 240 176 slices slice thickness1 mm) of all patients were checked and verified for T2 lesions by3 expert raters under the supervision of a board-certified radi-ologist Whole-brain segmentation and quantification of lesionsof FLAIR images were performed using ITK-SNAP (itksnaporg)19 Further lesion analysis was performed using the mrVistasoftware package (VISTA Lab Stanford University)
Resting-state functional MRI (RS-fMRI) measurements wereobtained with an echo-planar imaging sequence (TRTE =225030 ms FOV = 218 times 218 mm2 matrix 64 times 64 37 slicesslice thickness 34 mm sequence duration 9 minutes) Subjectswere instructed to lie still with their eyes closed Functionalimaging data preprocessing and analysis were performed usingthe BrainVoyager software package version 206 (Brain In-novation) Data underwent slice scan time correction motioncorrection and high-pass temporal filtering by BrainVoyagerdefault parameters to remove drift and improve the signal-to-noise ratio Functional images were coregistered to the anatomicimages using trilinear interpolation and transformed intoMontreal Neurological Institute space Each participantrsquos scanwas verified to include the entire brain with particular attentionto the occipital lobe Each scanwasmanually checked for quality
Network constructionComplex network analysis is based on graph theory a mathe-matical approach to networks Briefly the method requiresdefinition of brain regions as nodes and the search for con-nections or edges between those nodes These connectionsanatomic or functional can then be thresholded and binarizedinto connectivity matrices representing the existence or lack ofconnection between any 2 nodes in the network From thesematrices various measures can be extracted to quantify net-work topology and organization (figure 1)
GlossaryCIS = clinically isolated syndrome EDSS = Expanded Disability Status Scale FEF = frontal eye field FLAIR = fluid-attenuatedinversion recoveryHC = healthy controlNMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritisON =optic neuritis ROI = region of interest RS-fMRI = resting-state functional MRI
2 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
Visual network node definitionAs we focus in our studies on the visual system visual networknodes were defined using the probabilistic atlas ofWang et al20
created in Montreal Neurological Institute space and used invisual systemndashrelated studies21ndash24 which afforded us the levelof detail we needed The constructed networks included 50regions of interest (ROIs) (25 per hemisphere 8 ventral-temporal regions 9 dorsal-lateral regions and 8 parietal-frontalregions figure 2A table e-1A linkslwwcomNXIA207) eachrepresenting a node Because of the variety in ROI sizeswishing to minimize bias of variations in ROI size on estimatesof connectivity and signal-to-noise ratio differences the ROIswere arbitrarily constricted to a set size of 5 times 5 times 5 voxelspositioned at the center of each atlas-defined ROI The specificsize was set so that all constricted regions would be within theborders of their respective original ROIs
Motor network node definitionIn addition to the visual network we wished to examinewhether similar changes to those in the visual network ofpatients with ON may also be found in other networksin patients with corresponding CIS episodes As many of thepatients withCIS-nONhave experiencedmotor symptoms themotor network was also defined based on the Harvard-Oxfordcortical and subcortical structural atlas included in FMRIBSoftware Library25 and on several motor networkndashrelatedstudies26ndash28 The constructed networks included 12 ROIs (6per hemisphere figure 2B table e-1B linkslwwcomNXIA207) The selected ROIs were pure motor regions to provideus with a clean cutoff between networks and participants andno overlap existed between the 2 networks used ROIs wereconstricted to 125 voxels as in the visual network Because ofthe variety of CIS episodes included in the CIS-nON group for
Table 1 Study cohort description
HC CIS-ON CIS-nON NMOSD
Subjects (n) 26 18 21 23
Sex (f [m]) 22 (4) 11 (7) 11 (10) 20 (3)
Age (y mean plusmn SD) 437 plusmn 157 312 plusmn 77ab 334 plusmn 86ab 467 plusmn 145
Disease duration (mo mean plusmn SD) NA 463 plusmn 515a 540 plusmn 667a 9417 plusmn 9572
EDSS score (median range) NA 15 (0ndash35)a 15 (0ndash40)a 40 (0ndash65)
RRMS NA 3 5 NA
AQP4-ab-positive (n) NA NA NA 19
Bilateral ON NA NA NA 4
High-contrast visual acuity 102 plusmn 032 091 plusmn 034 101 plusmn 034 075 plusmn 047
Global lesion volume and number(cm3 n mean plusmn SD)
NA 252 plusmn 312 2144 plusmn 2266 369 plusmn 553 2323 plusmn 2235 258 plusmn 394 1674 plusmn 1937
Abbreviations AQP4 = aquaporin-4 CIS = clinically isolated syndrome EDSS = Expanded Disability Status Scale HC = healthy control NA = not applicableNMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritis ON = optic neuritis RRMS = relapsing-remitting MSa Significantly different than the NMOSD group p lt 001b Significantly different than the HC group p lt 001
Figure 1 Visualization of the translation process from atlas to brain network
(A) Original Wang et al20 atlas as transformed into BrainVoyager (B) Creating thresholded and binarized matrices representing all the connections in bothhemispheres (C) A visual network graph representation (healthy control group)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 3
the motor network analyses we have further divided the CIS-nON group into patients with motor symptoms (CIS-nON-motor n = 10) and with other nonmotor symptoms mainlysensory (CIS-nON-other n = 11)
Matrix preparationThe average RS-fMRI time course of all voxels within eachROI was extracted and Pearson correlation coefficientsrepresenting connectivity strength between regions werecalculated between each pair of ROIs in each hemisphereresulting in two 25 times 25 hemispheric visual matrices for eachsubject and two 6 times 6 motor matrices Each correlationmatrix was thresholded and binarized at a range of corre-lation thresholds (01ndash05 for the visual network and01ndash02 for the motor network at increments of 005) Thehighest correlation threshold was set as the last threshold inwhich all subjects still had any connection between ROIsFour patients with CIS-ON and 2 patients with CIS-nONdid not have connections in the highest threshold of themotor network Analyses have been performed with andwithout these patients and no significant differences werefound
Network analysisBoth local and global network properties were studied usingthe MATLAB Brain Connectivity Toolbox12 Here we brieflylist the network analysis metrics chosen to characterize thenetworks All parameters were integrated over the variousthresholds used to create a single value for analysis Graphspresenting the metrics used over the entire range of correla-tion thresholds are presented in figure e-1 (linkslwwcomNXIA207) It should be noted that most metrics chosencould not be used in the motor network because of the smallnumber of regions used and the largely disconnected net-works obtained
Basic network topology analysisTo characterize the general structure of the network in thelocal (nodal) level the nodal degree of the various ROIs wasexplored The group mean degree of each given ROI wascompared between groups to examine changes followingON and verify whether any region or subdivision of regionsshowed greater change Network density the proportion ofexisting connections in the network out of all possibleconnections based on the entire networkrsquos degree was also
Figure 2 Regions of interest (ROIs) used
(A) Visual network ROIs color coded according to classification in Wang et al20mdashventral-temporal (red) dorsal-lateral (blue) and parietal-frontal (green) (B)Motor network ROIs Visualization created using Xia M et al55 d = dorsal FEF = frontal eye field hMT = human middle temporal region hV4 = human visualregion V4 IFG = inferior frontal gyrus IPS = intraparietal sulcus LO = lateral occipital cortexM1 = primarymotor cortexMST =medial superior temporal areaPO = pars opercularis PT = pars triangularis SMA = supplementary motor area SPL = superior parietal lobule v = ventral VO = ventral occipital cortex V1 =primary visual cortex V2 = secondary visual cortex V3 = visual area V3
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
calculated and compared to examine the global networkdifferences between groups
Global network analysisTo examine the topological organization of the studiednetworks 6 global network metrics were explored Becausethis study explored only nodes within the visual system wewere interested in seeing whether small-worldness a ubiq-uitous trait reported in brain networks also exists within thevisual network To that end we included 4 parameters usedto calculate small-worldnessmdashclustering coefficient Cpharmonic mean of shortest path lengths Lp and their nor-malized counterparts These were defined as in references 29and 30 A typical small-world network should exhibit γ gt 1and λ asymp 1 The harmonic mean was chosen rather than themore commonly used characteristic path length becausemost of the networks in our study are at least partially dis-connected and therefore have infinite characteristic pathlength31
To examine segregation and integration within the visualnetwork we first looked at the 2 efficiency metrics the globaland local efficiency parameters Global efficiency is the re-ciprocal of the harmonic mean thought to represent howefficiently information is exchanged within the networkLocal (or nodal) efficiency is defined for the single nodelocalizing global efficiency effects to specific nodes givinga measure of how well that region is integrated within thenetwork32
To further examine segregation and integration we alsocalculated modularity33 This measure of network segrega-tion quantifies the degree to which the network may besubdivided into nonoverlapping groups of ROIs whichare densely interconnected within and sparsely connectedwithout
Statistical analysisData were examined for normality using QQ-plots andShapiro-Wilk tests The results variables were non-normallydistributed and thus for univariate comparisons betweengroups we used the Kruskal-Wallis test To assess the in-dependent effect of group designation on the result varia-bles after checking compliance with model assumptionsmultivariate linear models were built using age sex andExpanded Disability Status Scale (EDSS) score as cova-riates Statistical significance was assessed at p lt 005 levelTo control the false discovery rate multiple comparisoncorrection was performed using the Benjamini-Hochbergmethod All calculations were performed using R version351 (R Foundation for Statistical Computing ViennaAustria)
Data availabilityThe data sets generated for this study are available on requestfrom the corresponding author
ResultsResearch cohort characteristicsA summary of demographic and clinical measures is presentedin table 1 Differences were found in age disease duration andEDSS score between the 2 CIS groups and the HC andNMOSD groups (p lt 001 for all comparisons) Malefemaleratios were also different between those groups Thereforeage sex and EDSS score were added as covariates to allanalyses and were found to have no effect on the resultsDisease duration was not included as a covariate because itwas highly correlated with age of patients (p = 0007) Visualacuity did not significantly differ between any of the groupsand therefore was not included as covariate either
No significant differences were found in lesion numbervolume or specific location in the 3 patient groups Nosignificant differences were found between hemispheres inany of the metrics However significant results betweengroups were more pronounced in the left hemisphere andtherefore only these results are presented For the motornetwork significant results were found only in the righthemisphere and those are the results presented Results forthe unpresented hemispheres can be seen in the supple-mental materials (linkslwwcomNXIA207)
Visual network results
Small-worldness apparent in visual networksBy the criteria defined for small-worldness the healthy visualnetwork appears to display a small-world structure All theparticipants in the HC group have shown properties within thecriteria (λ values were nearly 1 in all participants and thresholdsγ values were mostly higher than 1 barring a few inconsistentexceptions) The same was shown in the patient groups ex-cluding 1 patient with CIS-ON and 1 patient with CIS-nONwho failed to meet the γ gt 1 criterion To verify whether thisdeviation from criteria somehow influences our group resultsanalyses were performed with and without these patients andno significant differences were found so both were included inthe results The small-world criteria curves for each group arepresented in figure e-2 (linkslwwcomNXIA207)
Basic network topology patternsFigure 3 presents a visualization of the visual network for the 4groups The normal network displayed by the HC cohort(figure 3A) appears to be more connected than all 3 patientgroups (figure 3 BndashD) in all 3 region subdivisions (ventral-temporal in red dorsal-lateral in blue and parietal-frontal ingreen) The NMOSD group (figure 3B) and the CIS-ONgroup (figure 3C) are quite similar in appearance and betterconnected than the CIS-nON group (figure 3D) which dis-plays the highest disconnection
This connectivity pattern according to which HCs gt NMOSDCIS-ONgtCIS-nON is seen globally using the densitymetricHC density (028 plusmn 009) is higher than CIS-nON density (019
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 5
plusmn 01 p = 00009) and it is higher though not significantly sothan the density of theCIS-ONgroup (022 plusmn 01 p= 005) TheNMOSD group (024 plusmn 01) density was higher than that of theCIS-nON group but not significantly so (p = 006) No signif-icant differences were found between the CIS-ON andNMOSDgroups or between the NMOSD and HC groups
Themean degree of theHC groupwas significantly higher thanthat of the CIS-nONgroup in all visual regions although not allsurvived multiple comparison correction Most survivingcomparisons were in low-order and dorsal-lateral regions(lower-ventral V1v and V2v lower-dorsal V1d V2d and V3ddorsal-lateral MST hMT and V3b frontal-parietal IPS0IPS1 and IPS2)
In addition the pattern found using the density metric bywhich HCs gt NMOSD CIS-ON gt CIS-nON exists mostlyin the dorsal-lateral region subdivision The ventral-temporalsubdivision (excluding the very early regions V1v and V2v)generally shows no significant differences between groups Theparietal-frontal subdivision shows either no significant differ-ences between groups at all (IPS3 IPS4 and IPS5) or a patternwhere the 2 CIS groups show no difference between them butlower mean degree than both the HC and NMOSD groups(SPL1 frontal eye field [FEF] p = 006) Figure 4 shows anexample from each subdivision displaying the emerging pat-terns The average degrees for each ROI can be found in tablee-2 (linkslwwcomNXIA207)
Network segregation and integration patternsAll segregation and integration metrics reveal connectivitydifferences unlike those for the basic network topologyshowing a pattern by which HC NMOSD gt CIS-ON CIS-nON This is in contrast to the basic topology pattern(achieved using the degree and density metrics) which high-lighted the similarity in topology in different diseases sharingthe same neurologic deficit (HC gt NMOSD CIS-ON gtCIS-nON)
Modularity results (figure 5A) show differences between theHC and CIS-nON groups (039 plusmn 005 and 03 plusmn 008 re-spectively p = 0004) as well as between the NMOSD (037 plusmn005) and CIS-nON groups (p = 0016) but no significantdifferences between the HC and NMOSD groups Themodularity result of the CIS-ON group (033 plusmn 009) is notsignificantly different from any of the other groups but isquantitatively closer to the CIS-nON group
The harmonizedmean of the characteristic path length (figure5B) shows a difference between the HC and CIS-nON groups(075 plusmn 044 and 256 plusmn 291 respectively p = 001) Althoughthe difference between the CIS-nON and NMOSD groups(083 plusmn 037 p = 0087) is not significant the NMOSD groupdisplays a shorter path length The harmonized mean of theCIS-ON group (211 plusmn 279) was not significantly differentfrom any of the groups and no significant difference wasfound between the HC and NMOSD groups
Figure 3 Visualization of the visual system for the 4 subject groups
Considered at correlation threshold r = 05 shown in the coronal (back view top) sagittal (lateral left hemisphere viewmiddle) and axial (dorsal view bottom)planes Nodes (regions of interest) are color coded according to their classification inWang et al20mdashventral-temporal (red) dorsal-lateral (blue) and parietal-frontal (green) The size of nodes reflects the relative degree of a given region in the network Disconnected regions are presented using an arbitrarily selectedsize for visualization purposes Visualization created using reference 55 CIS = clinically isolated syndrome NMOSD = neuromyelitis optica spectrumdisordernON = nonoptic neuritis ON = optic neuritis
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
Similarly global efficiency (figure 5C) shows change betweenthe HC and CIS-nON groups (035 and 025 respectively p =0008) Again no significant difference was found betweenthe NMOSD (031) and CIS-nON groups (p = 0093) butthe NMOSD group quantitatively shows higher efficiencyThe CIS-ON group once again shows no significant differ-ences (028) from any group but is between the NMOSD andCIS-nON groups in terms of global efficiency
Local efficiency showed similar results with differences foundbetween the CIS-nON group and the HC and NMOSDgroups though mostly in high-order regions particularly in thedorsal-lateral and parietal-frontal region subdivisions (lower-ventral V1v CIS-nONvsHCs only lower-dorsal V3d dorsal-lateral MST hMT V3a CIS-nON vs HCs only LO1 LO2V3b CIS-nON vs HCs and NMOSD frontal-parietal IPS3IPS4 IPS5 SPL1 vs HCs only IPS2 FEF vs HCs andNMOSD regions V3b IPS3 IPS5 have also shown significant
differences between HCs and CIS-ON) Details on local effi-ciency for each ROI can be seen in table e-3 (linkslwwcomNXIA207)
Motor network resultsDifferences between groups were found using the degreemetric in the motor putamen between the HC group whichwas most connected (054) and all patient groups (CIS-ON028 CIS-nON-motor 0225 CIS-nON-other 028 p lt 001for all) except for the NMOSD group (038 p = 01 aftermultiple comparison correction) No significant differenceswere found between any patient groups
In the pars opercularis (inferior frontal gyrusndashpars opercularis)differences were found between the CIS-nON-motor group(025) and the HC (057 p = 0004) and NMOSD (049p = 003) groups Density and global efficiency metrics alsoshow differences between the HC group and the CIS-nON-
Figure 4 Average degree of all 4 subject groups for selected regions of the 3 region subdivisions
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) hMT (dorsal-lateral subdivision) (B) VO1 (ventral-temporal subdivision) (C) FEF(frontal eye field parietal-frontal subdivision) Significantly different than HC CIS = clinically isolated syndrome HC = healthy control hMT = humanmiddletemporal region NMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritis ON = optic neuritis
Figure 5 Segregation and integration metrics for all 4 subject groups
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) Modularity (B) harmonizedmean of characteristic path length (C) global efficiencySignificantly different thanHC Significantly different thanNMOSD CIS = clinically isolated syndrome HC = healthy control NMOSD = neuromyelitis opticaspectrum disorder nON = nonoptic neuritis ON = optic neuritis
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 7
motor group (density HCs 012 CIS-nON-motor 007 p =0005 efficiencyHCs 014 CIS-nON-motor 009 p = 0001)Density also shows difference between the HC group and theCIS-ON group (011 p = 004) Other comparisons did notsurvive correction but surprisingly the general pattern remainshere similarly to the visual network HCs gt NMOSD gt CIS-ON CIS-nON-other gt CIS-nON-motor Results are pre-sented in figure e-3 (linkslwwcomNXIA207)
DiscussionIn this study we addressed visual cortical network patterns ininflammatory diseases following ON To that end we included2 prototypic autoimmune CNS diseases with distinct un-derlying pathophysiology MS and NMOSD3435 These dis-eases both share visual dysfunction caused by ON as clinicalcommonality Through these 2 disease types we haveattempted to discover whether changes to the visual systemfollowing ON are driven just by the specific neurologic visualdeficit or also by the underlying pathophysiology We usedgraph analysis methods to investigate topological and localchanges in resting-state visual networks of patients in those 2disease groups further dividing theMS group into patients withand without ON
Our main findings showed 2 distinct patterns of change in thevisual networks of the patient groups First the highly con-nected normal visual network is affected in all 3 diseasegroups showing reduced density and changes in topologyThese differences from HCs however are most pronouncedin the CIS-nON group The 2ON groups (NMOSD and CIS-ON) showed remarkably similar results in density and degreedistribution particularly in lower and dorsal-lateral regionsboth higher than those of patients with CIS-nON This sug-gests changes unique to the directly affected system (visualinput) We cautiously suggest that these changes may reflectan attempt to compensate for the damage incurred lastingeven when the underlying pathology has existed for yearsconsidering the relatively long disease durations displayed bythe NMOSD compared with the CIS-ON group
Second measures of network segregation and integration de-fining efficiency of information transfer and local structureshowed similarity between the MS-background groups (CIS-ON and CIS-nON) whereas the NMOSD group showedresults closer to those of the HCs This suggests that networksegregation and integration may be more affected by type ofunderlying pathophysiology rather than the specific neurologicdeficit
The question of whether cortical reorganization plays a role inrecovery from ON has long been discussed Early studies fo-cused mainly on cortical activity patterns in response to visualtasks presented to the affected eye Some studies have sug-gested that adaptive cortical plasticity following ON involvesincreased activity in higher visual areas assisting in overcoming
visual insult36ndash39 However later studies suggested that corticalactivation reflects the visual percept rather than demonstratesplasticity8 In recent years the importance of considering cor-tical networks rather than regional activity has emergedFunctional connectivity assessing the synchronized fluctua-tions in the fMRI signal between regions has shown sensitivityto neurologic damage and so it was suggested that connectivityrather than activity may play a role in clinical outcome How-ever as this is a cross-sectional study and no clinical measureswere included this remains hypothetical
InMS andNMOSDmuch emphasis has been given to changesin functional connectivity in sensorimotor networks Func-tional connectivity within the motor network was found toreflect motor function40 and to change in response to re-habilitative intervention41 in patients with MS Whether suchchanges reflect compensatory mechanisms or loss of function isstill a matter of debate4243 It has been suggested that theinterpretation of such observations depends on lesion load anddisease duration44
Our motor network results show no compensatory changes inthe subgroup of nON patients with motor symptoms On thecontrary specific clinical motor involvement resulted in re-duced connectivity within the motor cortex These results areparticularly prominent in view of the opposite results obtainedin the visual network where the relevant neurologic deficitseemed to be associated with elevated connectivity We suggestthat this may be the result of lesions located close to motorregions compared with the more peripheral damage sustainedthrough ON causing greater direct damage to the systemAnother piece of evidence supporting this suggestion is thedenser motor network seen in the NMOSD group who almostall had myelitis in addition to ON (19 of 23 patients) Thisfinding may be the motor networkrsquos equivalent of response todistant damage However because of the small numbers ofpatients included in the nonmotor subgroup and of patientswith nonmyelitis NMOSD these speculations should be takenwith caution
Although much attention has been given to the motor net-works in recent years the visual system has received less at-tention usually as a small part of a wider study4345 A studyfocusing on the visual system of patients with NMOSD andprevious ON has shown increase in the functional connectivityof the primary visual network compared with those withoutON11 These findings were also associated with greater retinaldamage and reduced visual acuity suggesting an attempt atcortical reorganization Similar findings were seen in our pre-vious work showing an increase in visual network connectivityin patients with CIS-ON compared with CIS-nON10 AMEGOCT study of the visual system in patients with MS has suc-ceeded in differentiating between patients with and withoutON based on a unique pattern of connectivity that specificallyinvolves the visual system46 These studies mostly focus on theneurologic deficit as the driving force behind the effects ob-served in MS and NMOSD connectivity and are congruent
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
with the general connectivity patterns presented in our currentstudy
However another cause for connectivity change may be thespecific type of disease Very few studies have tried to compareconnectivity between these 2 similar yet dissimilar diseasegroups Of these one has studied the functional and structuralconnectivity of the thalamus finding structural changes inboth diseases but functional disconnection only in MS47
Another study used a wide array of tests to differentiate be-tween the 2 disease types showing that the top 2 modalitiesuseful in this were white matter lesion load and functionalconnectivity48 In our results the white matter lesion elementappears negligible because both groups exhibit similar lesionnumber and volume and even lesion distribution was notlocalized in any of the groups And yet the segregation andintegration patterns of the functional visual network differedbetween MS and NMOSD with those of the latter moreclosely resembling that of HCs We suggest that this markeddifference may stem from differences in normal-appearingwhite matter Diffusion tensor imaging studies have showndiffusion abnormalities in both disease types but patientswith MS display widespread and more severe degree ofabnormality49ndash51 This may explain the difference in the seg-regation and integration properties of functional connectivitybetween the 2 groups
The use of graph-based analysis has enabled us to explore boththese driving forces of connectivity alterations the specificneurologic deficit and the disease type itself that appear to beassociated with different types of change Another advantageof this method is its ability to examine connectivity not only ina holistic manner In a work from 2015 the advantage ofgraph-based analysis inMS was presented Although emphasiswas on cognitive changes it was suggested that graph theoryshould be used to overcome the simplistic and incompleteinterpretations of previous methods52 Work on functionalconnectivity of the visual network in MS over the years hasmainly examined the network as a single entity using in-dependent component analysis1053 or seed-region analysis54
However the introduction of graph theory methods12 hasopened new possibilities in studying the affected network InMS the different works report both decreased global con-nectivity attributed to disease course and adaptation patternswith increased local connectivity and modularity13 Our cur-rent findings highlighting reorganization in dorsal-lateralregions known to be involved in dynamic perception pro-cesses are consistent with our previous works that emphasizedpersistent motion perception impairment following ON78
Based on our previous works in the field we suggest that thedorsal stream-specific increase in connectivity in our currentstudy may be part of a recovery process involving functionalmodifications Because bothON groups exhibit such a patternthis supports the notion that the neurologic deficit elicits thesechanges As this is a cross-sectional study this remains onlya suggestion
This study has several limitations First graph theorymethods are often used on larger subject groups Howeverthe significance of the results and their consistency with ourprevious findings convince us that our current findings aretrue Second the differences in age in all groups and indisease duration between the disease groups are problem-atic but these measures were factored into the variousanalyses and had no significant influence on the resultsThird our assumptions regarding the existence of com-pensatory mechanisms are based on the patterns emergingand former findings of our research Further light could havebeen shed on the matter had behavioral measures beenincluded as well as a longitudinal design It should be fur-ther noted that this study analyzed only functional con-nections within the visual system without the addedinformation that could have been gleaned from the com-plementing structural connectome limiting the ability todisentangle compensatory changes from structural damageFurthermore although the differences between groups mayindeed be interpreted as reorganizational changes of thevisual network in response to damage they may also reflectdifferential level of damage between individuals This issueshould be further investigated using a different study designbecause it could not be covered under the scope of thecurrent study
To conclude the visual network highly connected inHCs is made less connected by disease be it MS orNMOSD However a higher degree of connections wasobserved in the ON groups (CIS-ON and NMOSD)compared with the nON group This suggests that thesystem responds to specific damage caused to the anteriorvisual pathway bringing connectivity closer to that ofa normal network regardless of disease type On the otherhand network segregation and integration and the effi-ciency of information transfer appear more affected bydisease type altered in the MS groups but not inNMOSD particularly in higher regions Therefore wesuggest that the response to damage is dependent on thetype of neurologic deficit within the limitations of theunderlying pathophysiology
Study fundingSupported by the National Multiple Sclerosis Society (researchgrant RG-1802-30165) and the Applebaum Foundation FPaul was supported by Deutsche Forschungsgemeinschaft(DFG Exc 257)
DisclosureY Backner I Ben-Shalom J Kuchling N Siebert M ScheelK Ruprecht A Brandt F Paul and N Levin report no dis-closures Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationOctober 11 2019 Accepted in final form January 10 2020
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 9
References1 Schoonheim MM Filippi M Functional plasticity in MS Friend or foe Neurology
2012791418ndash14192 Costello F Vision disturbances in multiple sclerosis Semin Neurol 201636185ndash1953 Abel AMcClelland C LeeMS Critical review typical and atypical optic neuritis Surv
Ophthalmol 201964770ndash7794 Chen JJ Pittock SJ Flanagan EP Lennon VA Bhatti MT Optic neuritis in the era of
biomarkers Surv Ophthalmol 20206512ndash175 Lennon VA Wingerchuk DM Kryzer TJ et al A serum autoantibody marker of neu-
romyelitis optica distinction from multiple sclerosis Lancet 20043642106ndash21126 Raz N Chokron S Ben-Hur T Levin N Temporal reorganization to overcome
monocular demyelination Neurology 201381702ndash7097 Raz N Dotan S Chokron S Ben‐Hur T Levin N Demyelination affects temporal
aspects of perception an optic neuritis study Ann Neurol 201271531ndash5388 Raz N Dotan S Benoliel T Chokron S Ben-Hur T Levin N Sustained motion
perception deficit following optic neuritis Behavioral and cortical evidence Neurology2011762103ndash2111
9 Benoliel T Raz N Ben-Hur T Levin N Cortical functional modifications followingoptic neuritis Mult Scler 201723220ndash227
10 Backner Y Kuchling JMassarwa S et al Anatomical wiring and functional networkingchanges in the visual system following optic neuritis JAMANeurol 201875287ndash295
11 Finke C Zimmermann H Pache F et al Association of visual impairment in neu-romyelitis optica spectrum disorder with visual network reorganization JAMANeurol201875296ndash303
12 Rubinov M Sporns O Complex network measures of brain connectivity uses andinterpretations Neuroimage 2010521059ndash1069
13 Fleischer V Radetz A Ciolac D et al Graph theoretical framework of brain networksin multiple sclerosis a review of concepts Neuroscience 201940335ndash53
14 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
15 Wingerchuk DM Banwell B Bennett JL et al International consensus diagnosticcriteria for neuromyelitis optica spectrum disorders Neurology 201585177ndash189
16 Kuchling J Backner Y Oertel FC et al Comparison of probabilistic tractography andtract-based spatial statistics for assessing optic radiation damage in patients withautoimmune inflammatory disorders of the central nervous system Neuroimage Clin201819538ndash550
17 Oertel FC Kuchling J Zimmermann H et al Microstructural visual system changes inAQP4-antibodyndashseropositive NMOSD Neurol Neuroimmunol Neuroinflamm 20174e334 doi 101212NXI0000000000000334
18 Association WM World Medical Association Declaration of Helsinki ethical prin-ciples for medical research involving human subjects JAMA 20133102191
19 Yushkevich PA Piven J Hazlett HC et al User-guided 3D active contour segmen-tation of anatomical structures significantly improved efficiency and reliabilityNeuroimage 2006311116ndash1128
20 Wang L Mruczek RE Arcaro MJ Kastner S Probabilistic maps of visual topographyin human cortex Cereb Cortex 2014253911ndash3931
21 Hindy NC Ng FY Turk-Browne NB Linking pattern completion in the hippo-campus to predictive coding in visual cortex Nat Neurosci 201619665
22 Cichy RM Khosla A Pantazis D Torralba A Oliva A Comparison of deep neuralnetworks to spatio-temporal cortical dynamics of human visual object recognitionreveals hierarchical correspondence Sci Rep 2016627755
23 Cichy RM Pantazis D Oliva A Similarity-based fusion of MEG and fMRI revealsspatio-temporal dynamics in human cortex during visual object recognition CerebCortex 2016263563ndash3579
24 Mackey WE Winawer J Curtis CE Visual field map clusters in human frontoparietalcortex Elife 20176e22974
25 Smith SM Jenkinson M Woolrich MW et al Advances in functional and structuralMR image analysis and implementation as FSL Neuroimage 200423S208ndashS219
26 Pool E-M Rehme AK Eickhoff SB Fink GR Grefkes C Functional resting-stateconnectivity of the humanmotor network differences between right-and left-handersNeuroimage 2015109298ndash306
27 Hardwick RM Rottschy C Miall RC Eickhoff SB A quantitative meta-analysis andreview of motor learning in the human brain Neuroimage 201367283ndash297
28 Rocca MA Meani A Riccitelli GC et al Abnormal adaptation over time of motornetwork recruitment in multiple sclerosis patients with fatigue Mult Scler J 2016221144ndash1153
29 Watts DJ Strogatz SH Collective dynamics of ldquosmall-worldrdquonetworks Nature 1998393440ndash442
30 Maslov S Sneppen K Specificity and stability in topology of protein networks Sci-ence 2002296910ndash913
31 Newman ME The structure and function of complex networks SIAM Rev 200345167ndash256
32 Latora V Marchiori M Efficient behavior of small-world networks Phys Rev Lett200187198701
33 Newman ME Modularity and community structure in networks Proc Natl Acad SciUSA 20061038577ndash8582
34 Zamvil SS Slavin AJ Does MOG Ig-posit ive AQP4-seronegative opti-cospinal inflammatory disease justify a diagnosis of NMO spectrumdisorder Neurol Neuroimmunol Neuroinflamm 20152e62 doi 101212NXI0000000000000062
35 Zekeridou A Lennon VA Aquaporin-4 autoimmunity Neurol NeuroimmunolNeuroinflamm 20152e110 doi 101212NXI0000000000000110
36 Toosy AT Hickman SJ Miszkiel KA et al Adaptive cortical plasticity in higher visualareas after acute optic neuritis Ann Neurol 200557622ndash633
37 Jenkins TM Toosy AT Ciccarelli O et al Neuroplasticity predicts outcome of opticneuritis independent of tissue damage Ann Neurol 20106799ndash113
38 Werring DJ Bullmore ET Toosy AT et al Recovery from optic neuritis is associatedwith a change in the distribution of cerebral response to visual stimulation a func-tional magnetic resonance imaging study J Neurol Neurosurg Psychiatry 200068441ndash449
39 Levin N Orlov T Dotan S Zohary E Normal and abnormal fMRI activation patternsin the visual cortex after recovery from optic neuritis Neuroimage 2006331161ndash1168
40 Cordani C Meani A Esposito F et al Imaging correlates of hand motor performancein multiple sclerosis a multiparametric structural and functional MRI study MultScler 20191352458518822145
41 Fling BW Martini DN Zeeboer E Hildebrand A Cameron M Neuroplasticity of thesensorimotor neural network associated with walking aid training in people withmultiple sclerosis Mult Scler Relat Disord 2019311ndash4
42 Tommasin S De Giglio L Ruggieri S et al Relation between functional connectivityand disability in multiple sclerosis a non-linear model J Neurol 20182652881ndash2892
43 Castellazzi G Debernard L Melzer TR et al Functional connectivity alterationsreveal complex mechanisms based on clinical and radiological status in mild relapsingremitting multiple sclerosis Front Neurol 20189690
44 Tewarie P Steenwijk MD Brookes MJ et al Explaining the heterogeneity of func-tional connectivity findings in multiple sclerosis an empirically informed modelingstudy Hum Brain Mapp 2018392541ndash2548
45 Rocca MA Savoldi F Valsasina P et al Cross-modal plasticity among sensory net-works in neuromyelitis optica spectrum disorders Mult Scler 201925968ndash979
46 Tewarie P Balk LJ Hillebrand A et al Structure‐function relationships in the visualsystem in multiple sclerosis an MEG and OCT study Ann Clin Transl Neurol 20174614ndash621
47 Liu Y Duan Y Huang J et al Multimodal quantitative MR imaging of the thalamus inmultiple sclerosis and neuromyelitis optica Radiology 2015277784ndash792
Appendix Authors
Name Location Contribution
YaelBacknerMSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Designed andconceptualized the studyanalyzed the data draftedthe figures and draftedthe manuscript forintellectual content
Ido Ben-ShalomBMedSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Analyzed the motornetwork data
JosephKuchlingMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
NadjaSiebert MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
MichaelScheel MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
KlemensRuprechtMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
AlexanderBrandt MD
CharitendashUniversitatsmedizinBerlin Germany Universityof California
Major role in dataacquisition
FriedemannPaul MD
CharitendashUniversitatsmedizinBerlin Germany
Supervised the study andrevised the manuscript forintellectual content
Netta LevinMD PhD
Hadassah-HebrewUniversity Medical CenterJerusalem Israel
Conceptualized anddesigned the studysupervised the studyand drafted themanuscript forintellectual content
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

Visual network node definitionAs we focus in our studies on the visual system visual networknodes were defined using the probabilistic atlas ofWang et al20
created in Montreal Neurological Institute space and used invisual systemndashrelated studies21ndash24 which afforded us the levelof detail we needed The constructed networks included 50regions of interest (ROIs) (25 per hemisphere 8 ventral-temporal regions 9 dorsal-lateral regions and 8 parietal-frontalregions figure 2A table e-1A linkslwwcomNXIA207) eachrepresenting a node Because of the variety in ROI sizeswishing to minimize bias of variations in ROI size on estimatesof connectivity and signal-to-noise ratio differences the ROIswere arbitrarily constricted to a set size of 5 times 5 times 5 voxelspositioned at the center of each atlas-defined ROI The specificsize was set so that all constricted regions would be within theborders of their respective original ROIs
Motor network node definitionIn addition to the visual network we wished to examinewhether similar changes to those in the visual network ofpatients with ON may also be found in other networksin patients with corresponding CIS episodes As many of thepatients withCIS-nONhave experiencedmotor symptoms themotor network was also defined based on the Harvard-Oxfordcortical and subcortical structural atlas included in FMRIBSoftware Library25 and on several motor networkndashrelatedstudies26ndash28 The constructed networks included 12 ROIs (6per hemisphere figure 2B table e-1B linkslwwcomNXIA207) The selected ROIs were pure motor regions to provideus with a clean cutoff between networks and participants andno overlap existed between the 2 networks used ROIs wereconstricted to 125 voxels as in the visual network Because ofthe variety of CIS episodes included in the CIS-nON group for
Table 1 Study cohort description
HC CIS-ON CIS-nON NMOSD
Subjects (n) 26 18 21 23
Sex (f [m]) 22 (4) 11 (7) 11 (10) 20 (3)
Age (y mean plusmn SD) 437 plusmn 157 312 plusmn 77ab 334 plusmn 86ab 467 plusmn 145
Disease duration (mo mean plusmn SD) NA 463 plusmn 515a 540 plusmn 667a 9417 plusmn 9572
EDSS score (median range) NA 15 (0ndash35)a 15 (0ndash40)a 40 (0ndash65)
RRMS NA 3 5 NA
AQP4-ab-positive (n) NA NA NA 19
Bilateral ON NA NA NA 4
High-contrast visual acuity 102 plusmn 032 091 plusmn 034 101 plusmn 034 075 plusmn 047
Global lesion volume and number(cm3 n mean plusmn SD)
NA 252 plusmn 312 2144 plusmn 2266 369 plusmn 553 2323 plusmn 2235 258 plusmn 394 1674 plusmn 1937
Abbreviations AQP4 = aquaporin-4 CIS = clinically isolated syndrome EDSS = Expanded Disability Status Scale HC = healthy control NA = not applicableNMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritis ON = optic neuritis RRMS = relapsing-remitting MSa Significantly different than the NMOSD group p lt 001b Significantly different than the HC group p lt 001
Figure 1 Visualization of the translation process from atlas to brain network
(A) Original Wang et al20 atlas as transformed into BrainVoyager (B) Creating thresholded and binarized matrices representing all the connections in bothhemispheres (C) A visual network graph representation (healthy control group)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 3
the motor network analyses we have further divided the CIS-nON group into patients with motor symptoms (CIS-nON-motor n = 10) and with other nonmotor symptoms mainlysensory (CIS-nON-other n = 11)
Matrix preparationThe average RS-fMRI time course of all voxels within eachROI was extracted and Pearson correlation coefficientsrepresenting connectivity strength between regions werecalculated between each pair of ROIs in each hemisphereresulting in two 25 times 25 hemispheric visual matrices for eachsubject and two 6 times 6 motor matrices Each correlationmatrix was thresholded and binarized at a range of corre-lation thresholds (01ndash05 for the visual network and01ndash02 for the motor network at increments of 005) Thehighest correlation threshold was set as the last threshold inwhich all subjects still had any connection between ROIsFour patients with CIS-ON and 2 patients with CIS-nONdid not have connections in the highest threshold of themotor network Analyses have been performed with andwithout these patients and no significant differences werefound
Network analysisBoth local and global network properties were studied usingthe MATLAB Brain Connectivity Toolbox12 Here we brieflylist the network analysis metrics chosen to characterize thenetworks All parameters were integrated over the variousthresholds used to create a single value for analysis Graphspresenting the metrics used over the entire range of correla-tion thresholds are presented in figure e-1 (linkslwwcomNXIA207) It should be noted that most metrics chosencould not be used in the motor network because of the smallnumber of regions used and the largely disconnected net-works obtained
Basic network topology analysisTo characterize the general structure of the network in thelocal (nodal) level the nodal degree of the various ROIs wasexplored The group mean degree of each given ROI wascompared between groups to examine changes followingON and verify whether any region or subdivision of regionsshowed greater change Network density the proportion ofexisting connections in the network out of all possibleconnections based on the entire networkrsquos degree was also
Figure 2 Regions of interest (ROIs) used
(A) Visual network ROIs color coded according to classification in Wang et al20mdashventral-temporal (red) dorsal-lateral (blue) and parietal-frontal (green) (B)Motor network ROIs Visualization created using Xia M et al55 d = dorsal FEF = frontal eye field hMT = human middle temporal region hV4 = human visualregion V4 IFG = inferior frontal gyrus IPS = intraparietal sulcus LO = lateral occipital cortexM1 = primarymotor cortexMST =medial superior temporal areaPO = pars opercularis PT = pars triangularis SMA = supplementary motor area SPL = superior parietal lobule v = ventral VO = ventral occipital cortex V1 =primary visual cortex V2 = secondary visual cortex V3 = visual area V3
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
calculated and compared to examine the global networkdifferences between groups
Global network analysisTo examine the topological organization of the studiednetworks 6 global network metrics were explored Becausethis study explored only nodes within the visual system wewere interested in seeing whether small-worldness a ubiq-uitous trait reported in brain networks also exists within thevisual network To that end we included 4 parameters usedto calculate small-worldnessmdashclustering coefficient Cpharmonic mean of shortest path lengths Lp and their nor-malized counterparts These were defined as in references 29and 30 A typical small-world network should exhibit γ gt 1and λ asymp 1 The harmonic mean was chosen rather than themore commonly used characteristic path length becausemost of the networks in our study are at least partially dis-connected and therefore have infinite characteristic pathlength31
To examine segregation and integration within the visualnetwork we first looked at the 2 efficiency metrics the globaland local efficiency parameters Global efficiency is the re-ciprocal of the harmonic mean thought to represent howefficiently information is exchanged within the networkLocal (or nodal) efficiency is defined for the single nodelocalizing global efficiency effects to specific nodes givinga measure of how well that region is integrated within thenetwork32
To further examine segregation and integration we alsocalculated modularity33 This measure of network segrega-tion quantifies the degree to which the network may besubdivided into nonoverlapping groups of ROIs whichare densely interconnected within and sparsely connectedwithout
Statistical analysisData were examined for normality using QQ-plots andShapiro-Wilk tests The results variables were non-normallydistributed and thus for univariate comparisons betweengroups we used the Kruskal-Wallis test To assess the in-dependent effect of group designation on the result varia-bles after checking compliance with model assumptionsmultivariate linear models were built using age sex andExpanded Disability Status Scale (EDSS) score as cova-riates Statistical significance was assessed at p lt 005 levelTo control the false discovery rate multiple comparisoncorrection was performed using the Benjamini-Hochbergmethod All calculations were performed using R version351 (R Foundation for Statistical Computing ViennaAustria)
Data availabilityThe data sets generated for this study are available on requestfrom the corresponding author
ResultsResearch cohort characteristicsA summary of demographic and clinical measures is presentedin table 1 Differences were found in age disease duration andEDSS score between the 2 CIS groups and the HC andNMOSD groups (p lt 001 for all comparisons) Malefemaleratios were also different between those groups Thereforeage sex and EDSS score were added as covariates to allanalyses and were found to have no effect on the resultsDisease duration was not included as a covariate because itwas highly correlated with age of patients (p = 0007) Visualacuity did not significantly differ between any of the groupsand therefore was not included as covariate either
No significant differences were found in lesion numbervolume or specific location in the 3 patient groups Nosignificant differences were found between hemispheres inany of the metrics However significant results betweengroups were more pronounced in the left hemisphere andtherefore only these results are presented For the motornetwork significant results were found only in the righthemisphere and those are the results presented Results forthe unpresented hemispheres can be seen in the supple-mental materials (linkslwwcomNXIA207)
Visual network results
Small-worldness apparent in visual networksBy the criteria defined for small-worldness the healthy visualnetwork appears to display a small-world structure All theparticipants in the HC group have shown properties within thecriteria (λ values were nearly 1 in all participants and thresholdsγ values were mostly higher than 1 barring a few inconsistentexceptions) The same was shown in the patient groups ex-cluding 1 patient with CIS-ON and 1 patient with CIS-nONwho failed to meet the γ gt 1 criterion To verify whether thisdeviation from criteria somehow influences our group resultsanalyses were performed with and without these patients andno significant differences were found so both were included inthe results The small-world criteria curves for each group arepresented in figure e-2 (linkslwwcomNXIA207)
Basic network topology patternsFigure 3 presents a visualization of the visual network for the 4groups The normal network displayed by the HC cohort(figure 3A) appears to be more connected than all 3 patientgroups (figure 3 BndashD) in all 3 region subdivisions (ventral-temporal in red dorsal-lateral in blue and parietal-frontal ingreen) The NMOSD group (figure 3B) and the CIS-ONgroup (figure 3C) are quite similar in appearance and betterconnected than the CIS-nON group (figure 3D) which dis-plays the highest disconnection
This connectivity pattern according to which HCs gt NMOSDCIS-ONgtCIS-nON is seen globally using the densitymetricHC density (028 plusmn 009) is higher than CIS-nON density (019
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 5
plusmn 01 p = 00009) and it is higher though not significantly sothan the density of theCIS-ONgroup (022 plusmn 01 p= 005) TheNMOSD group (024 plusmn 01) density was higher than that of theCIS-nON group but not significantly so (p = 006) No signif-icant differences were found between the CIS-ON andNMOSDgroups or between the NMOSD and HC groups
Themean degree of theHC groupwas significantly higher thanthat of the CIS-nONgroup in all visual regions although not allsurvived multiple comparison correction Most survivingcomparisons were in low-order and dorsal-lateral regions(lower-ventral V1v and V2v lower-dorsal V1d V2d and V3ddorsal-lateral MST hMT and V3b frontal-parietal IPS0IPS1 and IPS2)
In addition the pattern found using the density metric bywhich HCs gt NMOSD CIS-ON gt CIS-nON exists mostlyin the dorsal-lateral region subdivision The ventral-temporalsubdivision (excluding the very early regions V1v and V2v)generally shows no significant differences between groups Theparietal-frontal subdivision shows either no significant differ-ences between groups at all (IPS3 IPS4 and IPS5) or a patternwhere the 2 CIS groups show no difference between them butlower mean degree than both the HC and NMOSD groups(SPL1 frontal eye field [FEF] p = 006) Figure 4 shows anexample from each subdivision displaying the emerging pat-terns The average degrees for each ROI can be found in tablee-2 (linkslwwcomNXIA207)
Network segregation and integration patternsAll segregation and integration metrics reveal connectivitydifferences unlike those for the basic network topologyshowing a pattern by which HC NMOSD gt CIS-ON CIS-nON This is in contrast to the basic topology pattern(achieved using the degree and density metrics) which high-lighted the similarity in topology in different diseases sharingthe same neurologic deficit (HC gt NMOSD CIS-ON gtCIS-nON)
Modularity results (figure 5A) show differences between theHC and CIS-nON groups (039 plusmn 005 and 03 plusmn 008 re-spectively p = 0004) as well as between the NMOSD (037 plusmn005) and CIS-nON groups (p = 0016) but no significantdifferences between the HC and NMOSD groups Themodularity result of the CIS-ON group (033 plusmn 009) is notsignificantly different from any of the other groups but isquantitatively closer to the CIS-nON group
The harmonizedmean of the characteristic path length (figure5B) shows a difference between the HC and CIS-nON groups(075 plusmn 044 and 256 plusmn 291 respectively p = 001) Althoughthe difference between the CIS-nON and NMOSD groups(083 plusmn 037 p = 0087) is not significant the NMOSD groupdisplays a shorter path length The harmonized mean of theCIS-ON group (211 plusmn 279) was not significantly differentfrom any of the groups and no significant difference wasfound between the HC and NMOSD groups
Figure 3 Visualization of the visual system for the 4 subject groups
Considered at correlation threshold r = 05 shown in the coronal (back view top) sagittal (lateral left hemisphere viewmiddle) and axial (dorsal view bottom)planes Nodes (regions of interest) are color coded according to their classification inWang et al20mdashventral-temporal (red) dorsal-lateral (blue) and parietal-frontal (green) The size of nodes reflects the relative degree of a given region in the network Disconnected regions are presented using an arbitrarily selectedsize for visualization purposes Visualization created using reference 55 CIS = clinically isolated syndrome NMOSD = neuromyelitis optica spectrumdisordernON = nonoptic neuritis ON = optic neuritis
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
Similarly global efficiency (figure 5C) shows change betweenthe HC and CIS-nON groups (035 and 025 respectively p =0008) Again no significant difference was found betweenthe NMOSD (031) and CIS-nON groups (p = 0093) butthe NMOSD group quantitatively shows higher efficiencyThe CIS-ON group once again shows no significant differ-ences (028) from any group but is between the NMOSD andCIS-nON groups in terms of global efficiency
Local efficiency showed similar results with differences foundbetween the CIS-nON group and the HC and NMOSDgroups though mostly in high-order regions particularly in thedorsal-lateral and parietal-frontal region subdivisions (lower-ventral V1v CIS-nONvsHCs only lower-dorsal V3d dorsal-lateral MST hMT V3a CIS-nON vs HCs only LO1 LO2V3b CIS-nON vs HCs and NMOSD frontal-parietal IPS3IPS4 IPS5 SPL1 vs HCs only IPS2 FEF vs HCs andNMOSD regions V3b IPS3 IPS5 have also shown significant
differences between HCs and CIS-ON) Details on local effi-ciency for each ROI can be seen in table e-3 (linkslwwcomNXIA207)
Motor network resultsDifferences between groups were found using the degreemetric in the motor putamen between the HC group whichwas most connected (054) and all patient groups (CIS-ON028 CIS-nON-motor 0225 CIS-nON-other 028 p lt 001for all) except for the NMOSD group (038 p = 01 aftermultiple comparison correction) No significant differenceswere found between any patient groups
In the pars opercularis (inferior frontal gyrusndashpars opercularis)differences were found between the CIS-nON-motor group(025) and the HC (057 p = 0004) and NMOSD (049p = 003) groups Density and global efficiency metrics alsoshow differences between the HC group and the CIS-nON-
Figure 4 Average degree of all 4 subject groups for selected regions of the 3 region subdivisions
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) hMT (dorsal-lateral subdivision) (B) VO1 (ventral-temporal subdivision) (C) FEF(frontal eye field parietal-frontal subdivision) Significantly different than HC CIS = clinically isolated syndrome HC = healthy control hMT = humanmiddletemporal region NMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritis ON = optic neuritis
Figure 5 Segregation and integration metrics for all 4 subject groups
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) Modularity (B) harmonizedmean of characteristic path length (C) global efficiencySignificantly different thanHC Significantly different thanNMOSD CIS = clinically isolated syndrome HC = healthy control NMOSD = neuromyelitis opticaspectrum disorder nON = nonoptic neuritis ON = optic neuritis
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 7
motor group (density HCs 012 CIS-nON-motor 007 p =0005 efficiencyHCs 014 CIS-nON-motor 009 p = 0001)Density also shows difference between the HC group and theCIS-ON group (011 p = 004) Other comparisons did notsurvive correction but surprisingly the general pattern remainshere similarly to the visual network HCs gt NMOSD gt CIS-ON CIS-nON-other gt CIS-nON-motor Results are pre-sented in figure e-3 (linkslwwcomNXIA207)
DiscussionIn this study we addressed visual cortical network patterns ininflammatory diseases following ON To that end we included2 prototypic autoimmune CNS diseases with distinct un-derlying pathophysiology MS and NMOSD3435 These dis-eases both share visual dysfunction caused by ON as clinicalcommonality Through these 2 disease types we haveattempted to discover whether changes to the visual systemfollowing ON are driven just by the specific neurologic visualdeficit or also by the underlying pathophysiology We usedgraph analysis methods to investigate topological and localchanges in resting-state visual networks of patients in those 2disease groups further dividing theMS group into patients withand without ON
Our main findings showed 2 distinct patterns of change in thevisual networks of the patient groups First the highly con-nected normal visual network is affected in all 3 diseasegroups showing reduced density and changes in topologyThese differences from HCs however are most pronouncedin the CIS-nON group The 2ON groups (NMOSD and CIS-ON) showed remarkably similar results in density and degreedistribution particularly in lower and dorsal-lateral regionsboth higher than those of patients with CIS-nON This sug-gests changes unique to the directly affected system (visualinput) We cautiously suggest that these changes may reflectan attempt to compensate for the damage incurred lastingeven when the underlying pathology has existed for yearsconsidering the relatively long disease durations displayed bythe NMOSD compared with the CIS-ON group
Second measures of network segregation and integration de-fining efficiency of information transfer and local structureshowed similarity between the MS-background groups (CIS-ON and CIS-nON) whereas the NMOSD group showedresults closer to those of the HCs This suggests that networksegregation and integration may be more affected by type ofunderlying pathophysiology rather than the specific neurologicdeficit
The question of whether cortical reorganization plays a role inrecovery from ON has long been discussed Early studies fo-cused mainly on cortical activity patterns in response to visualtasks presented to the affected eye Some studies have sug-gested that adaptive cortical plasticity following ON involvesincreased activity in higher visual areas assisting in overcoming
visual insult36ndash39 However later studies suggested that corticalactivation reflects the visual percept rather than demonstratesplasticity8 In recent years the importance of considering cor-tical networks rather than regional activity has emergedFunctional connectivity assessing the synchronized fluctua-tions in the fMRI signal between regions has shown sensitivityto neurologic damage and so it was suggested that connectivityrather than activity may play a role in clinical outcome How-ever as this is a cross-sectional study and no clinical measureswere included this remains hypothetical
InMS andNMOSDmuch emphasis has been given to changesin functional connectivity in sensorimotor networks Func-tional connectivity within the motor network was found toreflect motor function40 and to change in response to re-habilitative intervention41 in patients with MS Whether suchchanges reflect compensatory mechanisms or loss of function isstill a matter of debate4243 It has been suggested that theinterpretation of such observations depends on lesion load anddisease duration44
Our motor network results show no compensatory changes inthe subgroup of nON patients with motor symptoms On thecontrary specific clinical motor involvement resulted in re-duced connectivity within the motor cortex These results areparticularly prominent in view of the opposite results obtainedin the visual network where the relevant neurologic deficitseemed to be associated with elevated connectivity We suggestthat this may be the result of lesions located close to motorregions compared with the more peripheral damage sustainedthrough ON causing greater direct damage to the systemAnother piece of evidence supporting this suggestion is thedenser motor network seen in the NMOSD group who almostall had myelitis in addition to ON (19 of 23 patients) Thisfinding may be the motor networkrsquos equivalent of response todistant damage However because of the small numbers ofpatients included in the nonmotor subgroup and of patientswith nonmyelitis NMOSD these speculations should be takenwith caution
Although much attention has been given to the motor net-works in recent years the visual system has received less at-tention usually as a small part of a wider study4345 A studyfocusing on the visual system of patients with NMOSD andprevious ON has shown increase in the functional connectivityof the primary visual network compared with those withoutON11 These findings were also associated with greater retinaldamage and reduced visual acuity suggesting an attempt atcortical reorganization Similar findings were seen in our pre-vious work showing an increase in visual network connectivityin patients with CIS-ON compared with CIS-nON10 AMEGOCT study of the visual system in patients with MS has suc-ceeded in differentiating between patients with and withoutON based on a unique pattern of connectivity that specificallyinvolves the visual system46 These studies mostly focus on theneurologic deficit as the driving force behind the effects ob-served in MS and NMOSD connectivity and are congruent
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
with the general connectivity patterns presented in our currentstudy
However another cause for connectivity change may be thespecific type of disease Very few studies have tried to compareconnectivity between these 2 similar yet dissimilar diseasegroups Of these one has studied the functional and structuralconnectivity of the thalamus finding structural changes inboth diseases but functional disconnection only in MS47
Another study used a wide array of tests to differentiate be-tween the 2 disease types showing that the top 2 modalitiesuseful in this were white matter lesion load and functionalconnectivity48 In our results the white matter lesion elementappears negligible because both groups exhibit similar lesionnumber and volume and even lesion distribution was notlocalized in any of the groups And yet the segregation andintegration patterns of the functional visual network differedbetween MS and NMOSD with those of the latter moreclosely resembling that of HCs We suggest that this markeddifference may stem from differences in normal-appearingwhite matter Diffusion tensor imaging studies have showndiffusion abnormalities in both disease types but patientswith MS display widespread and more severe degree ofabnormality49ndash51 This may explain the difference in the seg-regation and integration properties of functional connectivitybetween the 2 groups
The use of graph-based analysis has enabled us to explore boththese driving forces of connectivity alterations the specificneurologic deficit and the disease type itself that appear to beassociated with different types of change Another advantageof this method is its ability to examine connectivity not only ina holistic manner In a work from 2015 the advantage ofgraph-based analysis inMS was presented Although emphasiswas on cognitive changes it was suggested that graph theoryshould be used to overcome the simplistic and incompleteinterpretations of previous methods52 Work on functionalconnectivity of the visual network in MS over the years hasmainly examined the network as a single entity using in-dependent component analysis1053 or seed-region analysis54
However the introduction of graph theory methods12 hasopened new possibilities in studying the affected network InMS the different works report both decreased global con-nectivity attributed to disease course and adaptation patternswith increased local connectivity and modularity13 Our cur-rent findings highlighting reorganization in dorsal-lateralregions known to be involved in dynamic perception pro-cesses are consistent with our previous works that emphasizedpersistent motion perception impairment following ON78
Based on our previous works in the field we suggest that thedorsal stream-specific increase in connectivity in our currentstudy may be part of a recovery process involving functionalmodifications Because bothON groups exhibit such a patternthis supports the notion that the neurologic deficit elicits thesechanges As this is a cross-sectional study this remains onlya suggestion
This study has several limitations First graph theorymethods are often used on larger subject groups Howeverthe significance of the results and their consistency with ourprevious findings convince us that our current findings aretrue Second the differences in age in all groups and indisease duration between the disease groups are problem-atic but these measures were factored into the variousanalyses and had no significant influence on the resultsThird our assumptions regarding the existence of com-pensatory mechanisms are based on the patterns emergingand former findings of our research Further light could havebeen shed on the matter had behavioral measures beenincluded as well as a longitudinal design It should be fur-ther noted that this study analyzed only functional con-nections within the visual system without the addedinformation that could have been gleaned from the com-plementing structural connectome limiting the ability todisentangle compensatory changes from structural damageFurthermore although the differences between groups mayindeed be interpreted as reorganizational changes of thevisual network in response to damage they may also reflectdifferential level of damage between individuals This issueshould be further investigated using a different study designbecause it could not be covered under the scope of thecurrent study
To conclude the visual network highly connected inHCs is made less connected by disease be it MS orNMOSD However a higher degree of connections wasobserved in the ON groups (CIS-ON and NMOSD)compared with the nON group This suggests that thesystem responds to specific damage caused to the anteriorvisual pathway bringing connectivity closer to that ofa normal network regardless of disease type On the otherhand network segregation and integration and the effi-ciency of information transfer appear more affected bydisease type altered in the MS groups but not inNMOSD particularly in higher regions Therefore wesuggest that the response to damage is dependent on thetype of neurologic deficit within the limitations of theunderlying pathophysiology
Study fundingSupported by the National Multiple Sclerosis Society (researchgrant RG-1802-30165) and the Applebaum Foundation FPaul was supported by Deutsche Forschungsgemeinschaft(DFG Exc 257)
DisclosureY Backner I Ben-Shalom J Kuchling N Siebert M ScheelK Ruprecht A Brandt F Paul and N Levin report no dis-closures Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationOctober 11 2019 Accepted in final form January 10 2020
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 9
References1 Schoonheim MM Filippi M Functional plasticity in MS Friend or foe Neurology
2012791418ndash14192 Costello F Vision disturbances in multiple sclerosis Semin Neurol 201636185ndash1953 Abel AMcClelland C LeeMS Critical review typical and atypical optic neuritis Surv
Ophthalmol 201964770ndash7794 Chen JJ Pittock SJ Flanagan EP Lennon VA Bhatti MT Optic neuritis in the era of
biomarkers Surv Ophthalmol 20206512ndash175 Lennon VA Wingerchuk DM Kryzer TJ et al A serum autoantibody marker of neu-
romyelitis optica distinction from multiple sclerosis Lancet 20043642106ndash21126 Raz N Chokron S Ben-Hur T Levin N Temporal reorganization to overcome
monocular demyelination Neurology 201381702ndash7097 Raz N Dotan S Chokron S Ben‐Hur T Levin N Demyelination affects temporal
aspects of perception an optic neuritis study Ann Neurol 201271531ndash5388 Raz N Dotan S Benoliel T Chokron S Ben-Hur T Levin N Sustained motion
perception deficit following optic neuritis Behavioral and cortical evidence Neurology2011762103ndash2111
9 Benoliel T Raz N Ben-Hur T Levin N Cortical functional modifications followingoptic neuritis Mult Scler 201723220ndash227
10 Backner Y Kuchling JMassarwa S et al Anatomical wiring and functional networkingchanges in the visual system following optic neuritis JAMANeurol 201875287ndash295
11 Finke C Zimmermann H Pache F et al Association of visual impairment in neu-romyelitis optica spectrum disorder with visual network reorganization JAMANeurol201875296ndash303
12 Rubinov M Sporns O Complex network measures of brain connectivity uses andinterpretations Neuroimage 2010521059ndash1069
13 Fleischer V Radetz A Ciolac D et al Graph theoretical framework of brain networksin multiple sclerosis a review of concepts Neuroscience 201940335ndash53
14 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
15 Wingerchuk DM Banwell B Bennett JL et al International consensus diagnosticcriteria for neuromyelitis optica spectrum disorders Neurology 201585177ndash189
16 Kuchling J Backner Y Oertel FC et al Comparison of probabilistic tractography andtract-based spatial statistics for assessing optic radiation damage in patients withautoimmune inflammatory disorders of the central nervous system Neuroimage Clin201819538ndash550
17 Oertel FC Kuchling J Zimmermann H et al Microstructural visual system changes inAQP4-antibodyndashseropositive NMOSD Neurol Neuroimmunol Neuroinflamm 20174e334 doi 101212NXI0000000000000334
18 Association WM World Medical Association Declaration of Helsinki ethical prin-ciples for medical research involving human subjects JAMA 20133102191
19 Yushkevich PA Piven J Hazlett HC et al User-guided 3D active contour segmen-tation of anatomical structures significantly improved efficiency and reliabilityNeuroimage 2006311116ndash1128
20 Wang L Mruczek RE Arcaro MJ Kastner S Probabilistic maps of visual topographyin human cortex Cereb Cortex 2014253911ndash3931
21 Hindy NC Ng FY Turk-Browne NB Linking pattern completion in the hippo-campus to predictive coding in visual cortex Nat Neurosci 201619665
22 Cichy RM Khosla A Pantazis D Torralba A Oliva A Comparison of deep neuralnetworks to spatio-temporal cortical dynamics of human visual object recognitionreveals hierarchical correspondence Sci Rep 2016627755
23 Cichy RM Pantazis D Oliva A Similarity-based fusion of MEG and fMRI revealsspatio-temporal dynamics in human cortex during visual object recognition CerebCortex 2016263563ndash3579
24 Mackey WE Winawer J Curtis CE Visual field map clusters in human frontoparietalcortex Elife 20176e22974
25 Smith SM Jenkinson M Woolrich MW et al Advances in functional and structuralMR image analysis and implementation as FSL Neuroimage 200423S208ndashS219
26 Pool E-M Rehme AK Eickhoff SB Fink GR Grefkes C Functional resting-stateconnectivity of the humanmotor network differences between right-and left-handersNeuroimage 2015109298ndash306
27 Hardwick RM Rottschy C Miall RC Eickhoff SB A quantitative meta-analysis andreview of motor learning in the human brain Neuroimage 201367283ndash297
28 Rocca MA Meani A Riccitelli GC et al Abnormal adaptation over time of motornetwork recruitment in multiple sclerosis patients with fatigue Mult Scler J 2016221144ndash1153
29 Watts DJ Strogatz SH Collective dynamics of ldquosmall-worldrdquonetworks Nature 1998393440ndash442
30 Maslov S Sneppen K Specificity and stability in topology of protein networks Sci-ence 2002296910ndash913
31 Newman ME The structure and function of complex networks SIAM Rev 200345167ndash256
32 Latora V Marchiori M Efficient behavior of small-world networks Phys Rev Lett200187198701
33 Newman ME Modularity and community structure in networks Proc Natl Acad SciUSA 20061038577ndash8582
34 Zamvil SS Slavin AJ Does MOG Ig-posit ive AQP4-seronegative opti-cospinal inflammatory disease justify a diagnosis of NMO spectrumdisorder Neurol Neuroimmunol Neuroinflamm 20152e62 doi 101212NXI0000000000000062
35 Zekeridou A Lennon VA Aquaporin-4 autoimmunity Neurol NeuroimmunolNeuroinflamm 20152e110 doi 101212NXI0000000000000110
36 Toosy AT Hickman SJ Miszkiel KA et al Adaptive cortical plasticity in higher visualareas after acute optic neuritis Ann Neurol 200557622ndash633
37 Jenkins TM Toosy AT Ciccarelli O et al Neuroplasticity predicts outcome of opticneuritis independent of tissue damage Ann Neurol 20106799ndash113
38 Werring DJ Bullmore ET Toosy AT et al Recovery from optic neuritis is associatedwith a change in the distribution of cerebral response to visual stimulation a func-tional magnetic resonance imaging study J Neurol Neurosurg Psychiatry 200068441ndash449
39 Levin N Orlov T Dotan S Zohary E Normal and abnormal fMRI activation patternsin the visual cortex after recovery from optic neuritis Neuroimage 2006331161ndash1168
40 Cordani C Meani A Esposito F et al Imaging correlates of hand motor performancein multiple sclerosis a multiparametric structural and functional MRI study MultScler 20191352458518822145
41 Fling BW Martini DN Zeeboer E Hildebrand A Cameron M Neuroplasticity of thesensorimotor neural network associated with walking aid training in people withmultiple sclerosis Mult Scler Relat Disord 2019311ndash4
42 Tommasin S De Giglio L Ruggieri S et al Relation between functional connectivityand disability in multiple sclerosis a non-linear model J Neurol 20182652881ndash2892
43 Castellazzi G Debernard L Melzer TR et al Functional connectivity alterationsreveal complex mechanisms based on clinical and radiological status in mild relapsingremitting multiple sclerosis Front Neurol 20189690
44 Tewarie P Steenwijk MD Brookes MJ et al Explaining the heterogeneity of func-tional connectivity findings in multiple sclerosis an empirically informed modelingstudy Hum Brain Mapp 2018392541ndash2548
45 Rocca MA Savoldi F Valsasina P et al Cross-modal plasticity among sensory net-works in neuromyelitis optica spectrum disorders Mult Scler 201925968ndash979
46 Tewarie P Balk LJ Hillebrand A et al Structure‐function relationships in the visualsystem in multiple sclerosis an MEG and OCT study Ann Clin Transl Neurol 20174614ndash621
47 Liu Y Duan Y Huang J et al Multimodal quantitative MR imaging of the thalamus inmultiple sclerosis and neuromyelitis optica Radiology 2015277784ndash792
Appendix Authors
Name Location Contribution
YaelBacknerMSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Designed andconceptualized the studyanalyzed the data draftedthe figures and draftedthe manuscript forintellectual content
Ido Ben-ShalomBMedSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Analyzed the motornetwork data
JosephKuchlingMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
NadjaSiebert MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
MichaelScheel MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
KlemensRuprechtMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
AlexanderBrandt MD
CharitendashUniversitatsmedizinBerlin Germany Universityof California
Major role in dataacquisition
FriedemannPaul MD
CharitendashUniversitatsmedizinBerlin Germany
Supervised the study andrevised the manuscript forintellectual content
Netta LevinMD PhD
Hadassah-HebrewUniversity Medical CenterJerusalem Israel
Conceptualized anddesigned the studysupervised the studyand drafted themanuscript forintellectual content
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

the motor network analyses we have further divided the CIS-nON group into patients with motor symptoms (CIS-nON-motor n = 10) and with other nonmotor symptoms mainlysensory (CIS-nON-other n = 11)
Matrix preparationThe average RS-fMRI time course of all voxels within eachROI was extracted and Pearson correlation coefficientsrepresenting connectivity strength between regions werecalculated between each pair of ROIs in each hemisphereresulting in two 25 times 25 hemispheric visual matrices for eachsubject and two 6 times 6 motor matrices Each correlationmatrix was thresholded and binarized at a range of corre-lation thresholds (01ndash05 for the visual network and01ndash02 for the motor network at increments of 005) Thehighest correlation threshold was set as the last threshold inwhich all subjects still had any connection between ROIsFour patients with CIS-ON and 2 patients with CIS-nONdid not have connections in the highest threshold of themotor network Analyses have been performed with andwithout these patients and no significant differences werefound
Network analysisBoth local and global network properties were studied usingthe MATLAB Brain Connectivity Toolbox12 Here we brieflylist the network analysis metrics chosen to characterize thenetworks All parameters were integrated over the variousthresholds used to create a single value for analysis Graphspresenting the metrics used over the entire range of correla-tion thresholds are presented in figure e-1 (linkslwwcomNXIA207) It should be noted that most metrics chosencould not be used in the motor network because of the smallnumber of regions used and the largely disconnected net-works obtained
Basic network topology analysisTo characterize the general structure of the network in thelocal (nodal) level the nodal degree of the various ROIs wasexplored The group mean degree of each given ROI wascompared between groups to examine changes followingON and verify whether any region or subdivision of regionsshowed greater change Network density the proportion ofexisting connections in the network out of all possibleconnections based on the entire networkrsquos degree was also
Figure 2 Regions of interest (ROIs) used
(A) Visual network ROIs color coded according to classification in Wang et al20mdashventral-temporal (red) dorsal-lateral (blue) and parietal-frontal (green) (B)Motor network ROIs Visualization created using Xia M et al55 d = dorsal FEF = frontal eye field hMT = human middle temporal region hV4 = human visualregion V4 IFG = inferior frontal gyrus IPS = intraparietal sulcus LO = lateral occipital cortexM1 = primarymotor cortexMST =medial superior temporal areaPO = pars opercularis PT = pars triangularis SMA = supplementary motor area SPL = superior parietal lobule v = ventral VO = ventral occipital cortex V1 =primary visual cortex V2 = secondary visual cortex V3 = visual area V3
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
calculated and compared to examine the global networkdifferences between groups
Global network analysisTo examine the topological organization of the studiednetworks 6 global network metrics were explored Becausethis study explored only nodes within the visual system wewere interested in seeing whether small-worldness a ubiq-uitous trait reported in brain networks also exists within thevisual network To that end we included 4 parameters usedto calculate small-worldnessmdashclustering coefficient Cpharmonic mean of shortest path lengths Lp and their nor-malized counterparts These were defined as in references 29and 30 A typical small-world network should exhibit γ gt 1and λ asymp 1 The harmonic mean was chosen rather than themore commonly used characteristic path length becausemost of the networks in our study are at least partially dis-connected and therefore have infinite characteristic pathlength31
To examine segregation and integration within the visualnetwork we first looked at the 2 efficiency metrics the globaland local efficiency parameters Global efficiency is the re-ciprocal of the harmonic mean thought to represent howefficiently information is exchanged within the networkLocal (or nodal) efficiency is defined for the single nodelocalizing global efficiency effects to specific nodes givinga measure of how well that region is integrated within thenetwork32
To further examine segregation and integration we alsocalculated modularity33 This measure of network segrega-tion quantifies the degree to which the network may besubdivided into nonoverlapping groups of ROIs whichare densely interconnected within and sparsely connectedwithout
Statistical analysisData were examined for normality using QQ-plots andShapiro-Wilk tests The results variables were non-normallydistributed and thus for univariate comparisons betweengroups we used the Kruskal-Wallis test To assess the in-dependent effect of group designation on the result varia-bles after checking compliance with model assumptionsmultivariate linear models were built using age sex andExpanded Disability Status Scale (EDSS) score as cova-riates Statistical significance was assessed at p lt 005 levelTo control the false discovery rate multiple comparisoncorrection was performed using the Benjamini-Hochbergmethod All calculations were performed using R version351 (R Foundation for Statistical Computing ViennaAustria)
Data availabilityThe data sets generated for this study are available on requestfrom the corresponding author
ResultsResearch cohort characteristicsA summary of demographic and clinical measures is presentedin table 1 Differences were found in age disease duration andEDSS score between the 2 CIS groups and the HC andNMOSD groups (p lt 001 for all comparisons) Malefemaleratios were also different between those groups Thereforeage sex and EDSS score were added as covariates to allanalyses and were found to have no effect on the resultsDisease duration was not included as a covariate because itwas highly correlated with age of patients (p = 0007) Visualacuity did not significantly differ between any of the groupsand therefore was not included as covariate either
No significant differences were found in lesion numbervolume or specific location in the 3 patient groups Nosignificant differences were found between hemispheres inany of the metrics However significant results betweengroups were more pronounced in the left hemisphere andtherefore only these results are presented For the motornetwork significant results were found only in the righthemisphere and those are the results presented Results forthe unpresented hemispheres can be seen in the supple-mental materials (linkslwwcomNXIA207)
Visual network results
Small-worldness apparent in visual networksBy the criteria defined for small-worldness the healthy visualnetwork appears to display a small-world structure All theparticipants in the HC group have shown properties within thecriteria (λ values were nearly 1 in all participants and thresholdsγ values were mostly higher than 1 barring a few inconsistentexceptions) The same was shown in the patient groups ex-cluding 1 patient with CIS-ON and 1 patient with CIS-nONwho failed to meet the γ gt 1 criterion To verify whether thisdeviation from criteria somehow influences our group resultsanalyses were performed with and without these patients andno significant differences were found so both were included inthe results The small-world criteria curves for each group arepresented in figure e-2 (linkslwwcomNXIA207)
Basic network topology patternsFigure 3 presents a visualization of the visual network for the 4groups The normal network displayed by the HC cohort(figure 3A) appears to be more connected than all 3 patientgroups (figure 3 BndashD) in all 3 region subdivisions (ventral-temporal in red dorsal-lateral in blue and parietal-frontal ingreen) The NMOSD group (figure 3B) and the CIS-ONgroup (figure 3C) are quite similar in appearance and betterconnected than the CIS-nON group (figure 3D) which dis-plays the highest disconnection
This connectivity pattern according to which HCs gt NMOSDCIS-ONgtCIS-nON is seen globally using the densitymetricHC density (028 plusmn 009) is higher than CIS-nON density (019
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 5
plusmn 01 p = 00009) and it is higher though not significantly sothan the density of theCIS-ONgroup (022 plusmn 01 p= 005) TheNMOSD group (024 plusmn 01) density was higher than that of theCIS-nON group but not significantly so (p = 006) No signif-icant differences were found between the CIS-ON andNMOSDgroups or between the NMOSD and HC groups
Themean degree of theHC groupwas significantly higher thanthat of the CIS-nONgroup in all visual regions although not allsurvived multiple comparison correction Most survivingcomparisons were in low-order and dorsal-lateral regions(lower-ventral V1v and V2v lower-dorsal V1d V2d and V3ddorsal-lateral MST hMT and V3b frontal-parietal IPS0IPS1 and IPS2)
In addition the pattern found using the density metric bywhich HCs gt NMOSD CIS-ON gt CIS-nON exists mostlyin the dorsal-lateral region subdivision The ventral-temporalsubdivision (excluding the very early regions V1v and V2v)generally shows no significant differences between groups Theparietal-frontal subdivision shows either no significant differ-ences between groups at all (IPS3 IPS4 and IPS5) or a patternwhere the 2 CIS groups show no difference between them butlower mean degree than both the HC and NMOSD groups(SPL1 frontal eye field [FEF] p = 006) Figure 4 shows anexample from each subdivision displaying the emerging pat-terns The average degrees for each ROI can be found in tablee-2 (linkslwwcomNXIA207)
Network segregation and integration patternsAll segregation and integration metrics reveal connectivitydifferences unlike those for the basic network topologyshowing a pattern by which HC NMOSD gt CIS-ON CIS-nON This is in contrast to the basic topology pattern(achieved using the degree and density metrics) which high-lighted the similarity in topology in different diseases sharingthe same neurologic deficit (HC gt NMOSD CIS-ON gtCIS-nON)
Modularity results (figure 5A) show differences between theHC and CIS-nON groups (039 plusmn 005 and 03 plusmn 008 re-spectively p = 0004) as well as between the NMOSD (037 plusmn005) and CIS-nON groups (p = 0016) but no significantdifferences between the HC and NMOSD groups Themodularity result of the CIS-ON group (033 plusmn 009) is notsignificantly different from any of the other groups but isquantitatively closer to the CIS-nON group
The harmonizedmean of the characteristic path length (figure5B) shows a difference between the HC and CIS-nON groups(075 plusmn 044 and 256 plusmn 291 respectively p = 001) Althoughthe difference between the CIS-nON and NMOSD groups(083 plusmn 037 p = 0087) is not significant the NMOSD groupdisplays a shorter path length The harmonized mean of theCIS-ON group (211 plusmn 279) was not significantly differentfrom any of the groups and no significant difference wasfound between the HC and NMOSD groups
Figure 3 Visualization of the visual system for the 4 subject groups
Considered at correlation threshold r = 05 shown in the coronal (back view top) sagittal (lateral left hemisphere viewmiddle) and axial (dorsal view bottom)planes Nodes (regions of interest) are color coded according to their classification inWang et al20mdashventral-temporal (red) dorsal-lateral (blue) and parietal-frontal (green) The size of nodes reflects the relative degree of a given region in the network Disconnected regions are presented using an arbitrarily selectedsize for visualization purposes Visualization created using reference 55 CIS = clinically isolated syndrome NMOSD = neuromyelitis optica spectrumdisordernON = nonoptic neuritis ON = optic neuritis
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
Similarly global efficiency (figure 5C) shows change betweenthe HC and CIS-nON groups (035 and 025 respectively p =0008) Again no significant difference was found betweenthe NMOSD (031) and CIS-nON groups (p = 0093) butthe NMOSD group quantitatively shows higher efficiencyThe CIS-ON group once again shows no significant differ-ences (028) from any group but is between the NMOSD andCIS-nON groups in terms of global efficiency
Local efficiency showed similar results with differences foundbetween the CIS-nON group and the HC and NMOSDgroups though mostly in high-order regions particularly in thedorsal-lateral and parietal-frontal region subdivisions (lower-ventral V1v CIS-nONvsHCs only lower-dorsal V3d dorsal-lateral MST hMT V3a CIS-nON vs HCs only LO1 LO2V3b CIS-nON vs HCs and NMOSD frontal-parietal IPS3IPS4 IPS5 SPL1 vs HCs only IPS2 FEF vs HCs andNMOSD regions V3b IPS3 IPS5 have also shown significant
differences between HCs and CIS-ON) Details on local effi-ciency for each ROI can be seen in table e-3 (linkslwwcomNXIA207)
Motor network resultsDifferences between groups were found using the degreemetric in the motor putamen between the HC group whichwas most connected (054) and all patient groups (CIS-ON028 CIS-nON-motor 0225 CIS-nON-other 028 p lt 001for all) except for the NMOSD group (038 p = 01 aftermultiple comparison correction) No significant differenceswere found between any patient groups
In the pars opercularis (inferior frontal gyrusndashpars opercularis)differences were found between the CIS-nON-motor group(025) and the HC (057 p = 0004) and NMOSD (049p = 003) groups Density and global efficiency metrics alsoshow differences between the HC group and the CIS-nON-
Figure 4 Average degree of all 4 subject groups for selected regions of the 3 region subdivisions
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) hMT (dorsal-lateral subdivision) (B) VO1 (ventral-temporal subdivision) (C) FEF(frontal eye field parietal-frontal subdivision) Significantly different than HC CIS = clinically isolated syndrome HC = healthy control hMT = humanmiddletemporal region NMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritis ON = optic neuritis
Figure 5 Segregation and integration metrics for all 4 subject groups
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) Modularity (B) harmonizedmean of characteristic path length (C) global efficiencySignificantly different thanHC Significantly different thanNMOSD CIS = clinically isolated syndrome HC = healthy control NMOSD = neuromyelitis opticaspectrum disorder nON = nonoptic neuritis ON = optic neuritis
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 7
motor group (density HCs 012 CIS-nON-motor 007 p =0005 efficiencyHCs 014 CIS-nON-motor 009 p = 0001)Density also shows difference between the HC group and theCIS-ON group (011 p = 004) Other comparisons did notsurvive correction but surprisingly the general pattern remainshere similarly to the visual network HCs gt NMOSD gt CIS-ON CIS-nON-other gt CIS-nON-motor Results are pre-sented in figure e-3 (linkslwwcomNXIA207)
DiscussionIn this study we addressed visual cortical network patterns ininflammatory diseases following ON To that end we included2 prototypic autoimmune CNS diseases with distinct un-derlying pathophysiology MS and NMOSD3435 These dis-eases both share visual dysfunction caused by ON as clinicalcommonality Through these 2 disease types we haveattempted to discover whether changes to the visual systemfollowing ON are driven just by the specific neurologic visualdeficit or also by the underlying pathophysiology We usedgraph analysis methods to investigate topological and localchanges in resting-state visual networks of patients in those 2disease groups further dividing theMS group into patients withand without ON
Our main findings showed 2 distinct patterns of change in thevisual networks of the patient groups First the highly con-nected normal visual network is affected in all 3 diseasegroups showing reduced density and changes in topologyThese differences from HCs however are most pronouncedin the CIS-nON group The 2ON groups (NMOSD and CIS-ON) showed remarkably similar results in density and degreedistribution particularly in lower and dorsal-lateral regionsboth higher than those of patients with CIS-nON This sug-gests changes unique to the directly affected system (visualinput) We cautiously suggest that these changes may reflectan attempt to compensate for the damage incurred lastingeven when the underlying pathology has existed for yearsconsidering the relatively long disease durations displayed bythe NMOSD compared with the CIS-ON group
Second measures of network segregation and integration de-fining efficiency of information transfer and local structureshowed similarity between the MS-background groups (CIS-ON and CIS-nON) whereas the NMOSD group showedresults closer to those of the HCs This suggests that networksegregation and integration may be more affected by type ofunderlying pathophysiology rather than the specific neurologicdeficit
The question of whether cortical reorganization plays a role inrecovery from ON has long been discussed Early studies fo-cused mainly on cortical activity patterns in response to visualtasks presented to the affected eye Some studies have sug-gested that adaptive cortical plasticity following ON involvesincreased activity in higher visual areas assisting in overcoming
visual insult36ndash39 However later studies suggested that corticalactivation reflects the visual percept rather than demonstratesplasticity8 In recent years the importance of considering cor-tical networks rather than regional activity has emergedFunctional connectivity assessing the synchronized fluctua-tions in the fMRI signal between regions has shown sensitivityto neurologic damage and so it was suggested that connectivityrather than activity may play a role in clinical outcome How-ever as this is a cross-sectional study and no clinical measureswere included this remains hypothetical
InMS andNMOSDmuch emphasis has been given to changesin functional connectivity in sensorimotor networks Func-tional connectivity within the motor network was found toreflect motor function40 and to change in response to re-habilitative intervention41 in patients with MS Whether suchchanges reflect compensatory mechanisms or loss of function isstill a matter of debate4243 It has been suggested that theinterpretation of such observations depends on lesion load anddisease duration44
Our motor network results show no compensatory changes inthe subgroup of nON patients with motor symptoms On thecontrary specific clinical motor involvement resulted in re-duced connectivity within the motor cortex These results areparticularly prominent in view of the opposite results obtainedin the visual network where the relevant neurologic deficitseemed to be associated with elevated connectivity We suggestthat this may be the result of lesions located close to motorregions compared with the more peripheral damage sustainedthrough ON causing greater direct damage to the systemAnother piece of evidence supporting this suggestion is thedenser motor network seen in the NMOSD group who almostall had myelitis in addition to ON (19 of 23 patients) Thisfinding may be the motor networkrsquos equivalent of response todistant damage However because of the small numbers ofpatients included in the nonmotor subgroup and of patientswith nonmyelitis NMOSD these speculations should be takenwith caution
Although much attention has been given to the motor net-works in recent years the visual system has received less at-tention usually as a small part of a wider study4345 A studyfocusing on the visual system of patients with NMOSD andprevious ON has shown increase in the functional connectivityof the primary visual network compared with those withoutON11 These findings were also associated with greater retinaldamage and reduced visual acuity suggesting an attempt atcortical reorganization Similar findings were seen in our pre-vious work showing an increase in visual network connectivityin patients with CIS-ON compared with CIS-nON10 AMEGOCT study of the visual system in patients with MS has suc-ceeded in differentiating between patients with and withoutON based on a unique pattern of connectivity that specificallyinvolves the visual system46 These studies mostly focus on theneurologic deficit as the driving force behind the effects ob-served in MS and NMOSD connectivity and are congruent
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
with the general connectivity patterns presented in our currentstudy
However another cause for connectivity change may be thespecific type of disease Very few studies have tried to compareconnectivity between these 2 similar yet dissimilar diseasegroups Of these one has studied the functional and structuralconnectivity of the thalamus finding structural changes inboth diseases but functional disconnection only in MS47
Another study used a wide array of tests to differentiate be-tween the 2 disease types showing that the top 2 modalitiesuseful in this were white matter lesion load and functionalconnectivity48 In our results the white matter lesion elementappears negligible because both groups exhibit similar lesionnumber and volume and even lesion distribution was notlocalized in any of the groups And yet the segregation andintegration patterns of the functional visual network differedbetween MS and NMOSD with those of the latter moreclosely resembling that of HCs We suggest that this markeddifference may stem from differences in normal-appearingwhite matter Diffusion tensor imaging studies have showndiffusion abnormalities in both disease types but patientswith MS display widespread and more severe degree ofabnormality49ndash51 This may explain the difference in the seg-regation and integration properties of functional connectivitybetween the 2 groups
The use of graph-based analysis has enabled us to explore boththese driving forces of connectivity alterations the specificneurologic deficit and the disease type itself that appear to beassociated with different types of change Another advantageof this method is its ability to examine connectivity not only ina holistic manner In a work from 2015 the advantage ofgraph-based analysis inMS was presented Although emphasiswas on cognitive changes it was suggested that graph theoryshould be used to overcome the simplistic and incompleteinterpretations of previous methods52 Work on functionalconnectivity of the visual network in MS over the years hasmainly examined the network as a single entity using in-dependent component analysis1053 or seed-region analysis54
However the introduction of graph theory methods12 hasopened new possibilities in studying the affected network InMS the different works report both decreased global con-nectivity attributed to disease course and adaptation patternswith increased local connectivity and modularity13 Our cur-rent findings highlighting reorganization in dorsal-lateralregions known to be involved in dynamic perception pro-cesses are consistent with our previous works that emphasizedpersistent motion perception impairment following ON78
Based on our previous works in the field we suggest that thedorsal stream-specific increase in connectivity in our currentstudy may be part of a recovery process involving functionalmodifications Because bothON groups exhibit such a patternthis supports the notion that the neurologic deficit elicits thesechanges As this is a cross-sectional study this remains onlya suggestion
This study has several limitations First graph theorymethods are often used on larger subject groups Howeverthe significance of the results and their consistency with ourprevious findings convince us that our current findings aretrue Second the differences in age in all groups and indisease duration between the disease groups are problem-atic but these measures were factored into the variousanalyses and had no significant influence on the resultsThird our assumptions regarding the existence of com-pensatory mechanisms are based on the patterns emergingand former findings of our research Further light could havebeen shed on the matter had behavioral measures beenincluded as well as a longitudinal design It should be fur-ther noted that this study analyzed only functional con-nections within the visual system without the addedinformation that could have been gleaned from the com-plementing structural connectome limiting the ability todisentangle compensatory changes from structural damageFurthermore although the differences between groups mayindeed be interpreted as reorganizational changes of thevisual network in response to damage they may also reflectdifferential level of damage between individuals This issueshould be further investigated using a different study designbecause it could not be covered under the scope of thecurrent study
To conclude the visual network highly connected inHCs is made less connected by disease be it MS orNMOSD However a higher degree of connections wasobserved in the ON groups (CIS-ON and NMOSD)compared with the nON group This suggests that thesystem responds to specific damage caused to the anteriorvisual pathway bringing connectivity closer to that ofa normal network regardless of disease type On the otherhand network segregation and integration and the effi-ciency of information transfer appear more affected bydisease type altered in the MS groups but not inNMOSD particularly in higher regions Therefore wesuggest that the response to damage is dependent on thetype of neurologic deficit within the limitations of theunderlying pathophysiology
Study fundingSupported by the National Multiple Sclerosis Society (researchgrant RG-1802-30165) and the Applebaum Foundation FPaul was supported by Deutsche Forschungsgemeinschaft(DFG Exc 257)
DisclosureY Backner I Ben-Shalom J Kuchling N Siebert M ScheelK Ruprecht A Brandt F Paul and N Levin report no dis-closures Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationOctober 11 2019 Accepted in final form January 10 2020
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 9
References1 Schoonheim MM Filippi M Functional plasticity in MS Friend or foe Neurology
2012791418ndash14192 Costello F Vision disturbances in multiple sclerosis Semin Neurol 201636185ndash1953 Abel AMcClelland C LeeMS Critical review typical and atypical optic neuritis Surv
Ophthalmol 201964770ndash7794 Chen JJ Pittock SJ Flanagan EP Lennon VA Bhatti MT Optic neuritis in the era of
biomarkers Surv Ophthalmol 20206512ndash175 Lennon VA Wingerchuk DM Kryzer TJ et al A serum autoantibody marker of neu-
romyelitis optica distinction from multiple sclerosis Lancet 20043642106ndash21126 Raz N Chokron S Ben-Hur T Levin N Temporal reorganization to overcome
monocular demyelination Neurology 201381702ndash7097 Raz N Dotan S Chokron S Ben‐Hur T Levin N Demyelination affects temporal
aspects of perception an optic neuritis study Ann Neurol 201271531ndash5388 Raz N Dotan S Benoliel T Chokron S Ben-Hur T Levin N Sustained motion
perception deficit following optic neuritis Behavioral and cortical evidence Neurology2011762103ndash2111
9 Benoliel T Raz N Ben-Hur T Levin N Cortical functional modifications followingoptic neuritis Mult Scler 201723220ndash227
10 Backner Y Kuchling JMassarwa S et al Anatomical wiring and functional networkingchanges in the visual system following optic neuritis JAMANeurol 201875287ndash295
11 Finke C Zimmermann H Pache F et al Association of visual impairment in neu-romyelitis optica spectrum disorder with visual network reorganization JAMANeurol201875296ndash303
12 Rubinov M Sporns O Complex network measures of brain connectivity uses andinterpretations Neuroimage 2010521059ndash1069
13 Fleischer V Radetz A Ciolac D et al Graph theoretical framework of brain networksin multiple sclerosis a review of concepts Neuroscience 201940335ndash53
14 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
15 Wingerchuk DM Banwell B Bennett JL et al International consensus diagnosticcriteria for neuromyelitis optica spectrum disorders Neurology 201585177ndash189
16 Kuchling J Backner Y Oertel FC et al Comparison of probabilistic tractography andtract-based spatial statistics for assessing optic radiation damage in patients withautoimmune inflammatory disorders of the central nervous system Neuroimage Clin201819538ndash550
17 Oertel FC Kuchling J Zimmermann H et al Microstructural visual system changes inAQP4-antibodyndashseropositive NMOSD Neurol Neuroimmunol Neuroinflamm 20174e334 doi 101212NXI0000000000000334
18 Association WM World Medical Association Declaration of Helsinki ethical prin-ciples for medical research involving human subjects JAMA 20133102191
19 Yushkevich PA Piven J Hazlett HC et al User-guided 3D active contour segmen-tation of anatomical structures significantly improved efficiency and reliabilityNeuroimage 2006311116ndash1128
20 Wang L Mruczek RE Arcaro MJ Kastner S Probabilistic maps of visual topographyin human cortex Cereb Cortex 2014253911ndash3931
21 Hindy NC Ng FY Turk-Browne NB Linking pattern completion in the hippo-campus to predictive coding in visual cortex Nat Neurosci 201619665
22 Cichy RM Khosla A Pantazis D Torralba A Oliva A Comparison of deep neuralnetworks to spatio-temporal cortical dynamics of human visual object recognitionreveals hierarchical correspondence Sci Rep 2016627755
23 Cichy RM Pantazis D Oliva A Similarity-based fusion of MEG and fMRI revealsspatio-temporal dynamics in human cortex during visual object recognition CerebCortex 2016263563ndash3579
24 Mackey WE Winawer J Curtis CE Visual field map clusters in human frontoparietalcortex Elife 20176e22974
25 Smith SM Jenkinson M Woolrich MW et al Advances in functional and structuralMR image analysis and implementation as FSL Neuroimage 200423S208ndashS219
26 Pool E-M Rehme AK Eickhoff SB Fink GR Grefkes C Functional resting-stateconnectivity of the humanmotor network differences between right-and left-handersNeuroimage 2015109298ndash306
27 Hardwick RM Rottschy C Miall RC Eickhoff SB A quantitative meta-analysis andreview of motor learning in the human brain Neuroimage 201367283ndash297
28 Rocca MA Meani A Riccitelli GC et al Abnormal adaptation over time of motornetwork recruitment in multiple sclerosis patients with fatigue Mult Scler J 2016221144ndash1153
29 Watts DJ Strogatz SH Collective dynamics of ldquosmall-worldrdquonetworks Nature 1998393440ndash442
30 Maslov S Sneppen K Specificity and stability in topology of protein networks Sci-ence 2002296910ndash913
31 Newman ME The structure and function of complex networks SIAM Rev 200345167ndash256
32 Latora V Marchiori M Efficient behavior of small-world networks Phys Rev Lett200187198701
33 Newman ME Modularity and community structure in networks Proc Natl Acad SciUSA 20061038577ndash8582
34 Zamvil SS Slavin AJ Does MOG Ig-posit ive AQP4-seronegative opti-cospinal inflammatory disease justify a diagnosis of NMO spectrumdisorder Neurol Neuroimmunol Neuroinflamm 20152e62 doi 101212NXI0000000000000062
35 Zekeridou A Lennon VA Aquaporin-4 autoimmunity Neurol NeuroimmunolNeuroinflamm 20152e110 doi 101212NXI0000000000000110
36 Toosy AT Hickman SJ Miszkiel KA et al Adaptive cortical plasticity in higher visualareas after acute optic neuritis Ann Neurol 200557622ndash633
37 Jenkins TM Toosy AT Ciccarelli O et al Neuroplasticity predicts outcome of opticneuritis independent of tissue damage Ann Neurol 20106799ndash113
38 Werring DJ Bullmore ET Toosy AT et al Recovery from optic neuritis is associatedwith a change in the distribution of cerebral response to visual stimulation a func-tional magnetic resonance imaging study J Neurol Neurosurg Psychiatry 200068441ndash449
39 Levin N Orlov T Dotan S Zohary E Normal and abnormal fMRI activation patternsin the visual cortex after recovery from optic neuritis Neuroimage 2006331161ndash1168
40 Cordani C Meani A Esposito F et al Imaging correlates of hand motor performancein multiple sclerosis a multiparametric structural and functional MRI study MultScler 20191352458518822145
41 Fling BW Martini DN Zeeboer E Hildebrand A Cameron M Neuroplasticity of thesensorimotor neural network associated with walking aid training in people withmultiple sclerosis Mult Scler Relat Disord 2019311ndash4
42 Tommasin S De Giglio L Ruggieri S et al Relation between functional connectivityand disability in multiple sclerosis a non-linear model J Neurol 20182652881ndash2892
43 Castellazzi G Debernard L Melzer TR et al Functional connectivity alterationsreveal complex mechanisms based on clinical and radiological status in mild relapsingremitting multiple sclerosis Front Neurol 20189690
44 Tewarie P Steenwijk MD Brookes MJ et al Explaining the heterogeneity of func-tional connectivity findings in multiple sclerosis an empirically informed modelingstudy Hum Brain Mapp 2018392541ndash2548
45 Rocca MA Savoldi F Valsasina P et al Cross-modal plasticity among sensory net-works in neuromyelitis optica spectrum disorders Mult Scler 201925968ndash979
46 Tewarie P Balk LJ Hillebrand A et al Structure‐function relationships in the visualsystem in multiple sclerosis an MEG and OCT study Ann Clin Transl Neurol 20174614ndash621
47 Liu Y Duan Y Huang J et al Multimodal quantitative MR imaging of the thalamus inmultiple sclerosis and neuromyelitis optica Radiology 2015277784ndash792
Appendix Authors
Name Location Contribution
YaelBacknerMSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Designed andconceptualized the studyanalyzed the data draftedthe figures and draftedthe manuscript forintellectual content
Ido Ben-ShalomBMedSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Analyzed the motornetwork data
JosephKuchlingMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
NadjaSiebert MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
MichaelScheel MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
KlemensRuprechtMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
AlexanderBrandt MD
CharitendashUniversitatsmedizinBerlin Germany Universityof California
Major role in dataacquisition
FriedemannPaul MD
CharitendashUniversitatsmedizinBerlin Germany
Supervised the study andrevised the manuscript forintellectual content
Netta LevinMD PhD
Hadassah-HebrewUniversity Medical CenterJerusalem Israel
Conceptualized anddesigned the studysupervised the studyand drafted themanuscript forintellectual content
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

calculated and compared to examine the global networkdifferences between groups
Global network analysisTo examine the topological organization of the studiednetworks 6 global network metrics were explored Becausethis study explored only nodes within the visual system wewere interested in seeing whether small-worldness a ubiq-uitous trait reported in brain networks also exists within thevisual network To that end we included 4 parameters usedto calculate small-worldnessmdashclustering coefficient Cpharmonic mean of shortest path lengths Lp and their nor-malized counterparts These were defined as in references 29and 30 A typical small-world network should exhibit γ gt 1and λ asymp 1 The harmonic mean was chosen rather than themore commonly used characteristic path length becausemost of the networks in our study are at least partially dis-connected and therefore have infinite characteristic pathlength31
To examine segregation and integration within the visualnetwork we first looked at the 2 efficiency metrics the globaland local efficiency parameters Global efficiency is the re-ciprocal of the harmonic mean thought to represent howefficiently information is exchanged within the networkLocal (or nodal) efficiency is defined for the single nodelocalizing global efficiency effects to specific nodes givinga measure of how well that region is integrated within thenetwork32
To further examine segregation and integration we alsocalculated modularity33 This measure of network segrega-tion quantifies the degree to which the network may besubdivided into nonoverlapping groups of ROIs whichare densely interconnected within and sparsely connectedwithout
Statistical analysisData were examined for normality using QQ-plots andShapiro-Wilk tests The results variables were non-normallydistributed and thus for univariate comparisons betweengroups we used the Kruskal-Wallis test To assess the in-dependent effect of group designation on the result varia-bles after checking compliance with model assumptionsmultivariate linear models were built using age sex andExpanded Disability Status Scale (EDSS) score as cova-riates Statistical significance was assessed at p lt 005 levelTo control the false discovery rate multiple comparisoncorrection was performed using the Benjamini-Hochbergmethod All calculations were performed using R version351 (R Foundation for Statistical Computing ViennaAustria)
Data availabilityThe data sets generated for this study are available on requestfrom the corresponding author
ResultsResearch cohort characteristicsA summary of demographic and clinical measures is presentedin table 1 Differences were found in age disease duration andEDSS score between the 2 CIS groups and the HC andNMOSD groups (p lt 001 for all comparisons) Malefemaleratios were also different between those groups Thereforeage sex and EDSS score were added as covariates to allanalyses and were found to have no effect on the resultsDisease duration was not included as a covariate because itwas highly correlated with age of patients (p = 0007) Visualacuity did not significantly differ between any of the groupsand therefore was not included as covariate either
No significant differences were found in lesion numbervolume or specific location in the 3 patient groups Nosignificant differences were found between hemispheres inany of the metrics However significant results betweengroups were more pronounced in the left hemisphere andtherefore only these results are presented For the motornetwork significant results were found only in the righthemisphere and those are the results presented Results forthe unpresented hemispheres can be seen in the supple-mental materials (linkslwwcomNXIA207)
Visual network results
Small-worldness apparent in visual networksBy the criteria defined for small-worldness the healthy visualnetwork appears to display a small-world structure All theparticipants in the HC group have shown properties within thecriteria (λ values were nearly 1 in all participants and thresholdsγ values were mostly higher than 1 barring a few inconsistentexceptions) The same was shown in the patient groups ex-cluding 1 patient with CIS-ON and 1 patient with CIS-nONwho failed to meet the γ gt 1 criterion To verify whether thisdeviation from criteria somehow influences our group resultsanalyses were performed with and without these patients andno significant differences were found so both were included inthe results The small-world criteria curves for each group arepresented in figure e-2 (linkslwwcomNXIA207)
Basic network topology patternsFigure 3 presents a visualization of the visual network for the 4groups The normal network displayed by the HC cohort(figure 3A) appears to be more connected than all 3 patientgroups (figure 3 BndashD) in all 3 region subdivisions (ventral-temporal in red dorsal-lateral in blue and parietal-frontal ingreen) The NMOSD group (figure 3B) and the CIS-ONgroup (figure 3C) are quite similar in appearance and betterconnected than the CIS-nON group (figure 3D) which dis-plays the highest disconnection
This connectivity pattern according to which HCs gt NMOSDCIS-ONgtCIS-nON is seen globally using the densitymetricHC density (028 plusmn 009) is higher than CIS-nON density (019
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 5
plusmn 01 p = 00009) and it is higher though not significantly sothan the density of theCIS-ONgroup (022 plusmn 01 p= 005) TheNMOSD group (024 plusmn 01) density was higher than that of theCIS-nON group but not significantly so (p = 006) No signif-icant differences were found between the CIS-ON andNMOSDgroups or between the NMOSD and HC groups
Themean degree of theHC groupwas significantly higher thanthat of the CIS-nONgroup in all visual regions although not allsurvived multiple comparison correction Most survivingcomparisons were in low-order and dorsal-lateral regions(lower-ventral V1v and V2v lower-dorsal V1d V2d and V3ddorsal-lateral MST hMT and V3b frontal-parietal IPS0IPS1 and IPS2)
In addition the pattern found using the density metric bywhich HCs gt NMOSD CIS-ON gt CIS-nON exists mostlyin the dorsal-lateral region subdivision The ventral-temporalsubdivision (excluding the very early regions V1v and V2v)generally shows no significant differences between groups Theparietal-frontal subdivision shows either no significant differ-ences between groups at all (IPS3 IPS4 and IPS5) or a patternwhere the 2 CIS groups show no difference between them butlower mean degree than both the HC and NMOSD groups(SPL1 frontal eye field [FEF] p = 006) Figure 4 shows anexample from each subdivision displaying the emerging pat-terns The average degrees for each ROI can be found in tablee-2 (linkslwwcomNXIA207)
Network segregation and integration patternsAll segregation and integration metrics reveal connectivitydifferences unlike those for the basic network topologyshowing a pattern by which HC NMOSD gt CIS-ON CIS-nON This is in contrast to the basic topology pattern(achieved using the degree and density metrics) which high-lighted the similarity in topology in different diseases sharingthe same neurologic deficit (HC gt NMOSD CIS-ON gtCIS-nON)
Modularity results (figure 5A) show differences between theHC and CIS-nON groups (039 plusmn 005 and 03 plusmn 008 re-spectively p = 0004) as well as between the NMOSD (037 plusmn005) and CIS-nON groups (p = 0016) but no significantdifferences between the HC and NMOSD groups Themodularity result of the CIS-ON group (033 plusmn 009) is notsignificantly different from any of the other groups but isquantitatively closer to the CIS-nON group
The harmonizedmean of the characteristic path length (figure5B) shows a difference between the HC and CIS-nON groups(075 plusmn 044 and 256 plusmn 291 respectively p = 001) Althoughthe difference between the CIS-nON and NMOSD groups(083 plusmn 037 p = 0087) is not significant the NMOSD groupdisplays a shorter path length The harmonized mean of theCIS-ON group (211 plusmn 279) was not significantly differentfrom any of the groups and no significant difference wasfound between the HC and NMOSD groups
Figure 3 Visualization of the visual system for the 4 subject groups
Considered at correlation threshold r = 05 shown in the coronal (back view top) sagittal (lateral left hemisphere viewmiddle) and axial (dorsal view bottom)planes Nodes (regions of interest) are color coded according to their classification inWang et al20mdashventral-temporal (red) dorsal-lateral (blue) and parietal-frontal (green) The size of nodes reflects the relative degree of a given region in the network Disconnected regions are presented using an arbitrarily selectedsize for visualization purposes Visualization created using reference 55 CIS = clinically isolated syndrome NMOSD = neuromyelitis optica spectrumdisordernON = nonoptic neuritis ON = optic neuritis
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
Similarly global efficiency (figure 5C) shows change betweenthe HC and CIS-nON groups (035 and 025 respectively p =0008) Again no significant difference was found betweenthe NMOSD (031) and CIS-nON groups (p = 0093) butthe NMOSD group quantitatively shows higher efficiencyThe CIS-ON group once again shows no significant differ-ences (028) from any group but is between the NMOSD andCIS-nON groups in terms of global efficiency
Local efficiency showed similar results with differences foundbetween the CIS-nON group and the HC and NMOSDgroups though mostly in high-order regions particularly in thedorsal-lateral and parietal-frontal region subdivisions (lower-ventral V1v CIS-nONvsHCs only lower-dorsal V3d dorsal-lateral MST hMT V3a CIS-nON vs HCs only LO1 LO2V3b CIS-nON vs HCs and NMOSD frontal-parietal IPS3IPS4 IPS5 SPL1 vs HCs only IPS2 FEF vs HCs andNMOSD regions V3b IPS3 IPS5 have also shown significant
differences between HCs and CIS-ON) Details on local effi-ciency for each ROI can be seen in table e-3 (linkslwwcomNXIA207)
Motor network resultsDifferences between groups were found using the degreemetric in the motor putamen between the HC group whichwas most connected (054) and all patient groups (CIS-ON028 CIS-nON-motor 0225 CIS-nON-other 028 p lt 001for all) except for the NMOSD group (038 p = 01 aftermultiple comparison correction) No significant differenceswere found between any patient groups
In the pars opercularis (inferior frontal gyrusndashpars opercularis)differences were found between the CIS-nON-motor group(025) and the HC (057 p = 0004) and NMOSD (049p = 003) groups Density and global efficiency metrics alsoshow differences between the HC group and the CIS-nON-
Figure 4 Average degree of all 4 subject groups for selected regions of the 3 region subdivisions
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) hMT (dorsal-lateral subdivision) (B) VO1 (ventral-temporal subdivision) (C) FEF(frontal eye field parietal-frontal subdivision) Significantly different than HC CIS = clinically isolated syndrome HC = healthy control hMT = humanmiddletemporal region NMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritis ON = optic neuritis
Figure 5 Segregation and integration metrics for all 4 subject groups
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) Modularity (B) harmonizedmean of characteristic path length (C) global efficiencySignificantly different thanHC Significantly different thanNMOSD CIS = clinically isolated syndrome HC = healthy control NMOSD = neuromyelitis opticaspectrum disorder nON = nonoptic neuritis ON = optic neuritis
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 7
motor group (density HCs 012 CIS-nON-motor 007 p =0005 efficiencyHCs 014 CIS-nON-motor 009 p = 0001)Density also shows difference between the HC group and theCIS-ON group (011 p = 004) Other comparisons did notsurvive correction but surprisingly the general pattern remainshere similarly to the visual network HCs gt NMOSD gt CIS-ON CIS-nON-other gt CIS-nON-motor Results are pre-sented in figure e-3 (linkslwwcomNXIA207)
DiscussionIn this study we addressed visual cortical network patterns ininflammatory diseases following ON To that end we included2 prototypic autoimmune CNS diseases with distinct un-derlying pathophysiology MS and NMOSD3435 These dis-eases both share visual dysfunction caused by ON as clinicalcommonality Through these 2 disease types we haveattempted to discover whether changes to the visual systemfollowing ON are driven just by the specific neurologic visualdeficit or also by the underlying pathophysiology We usedgraph analysis methods to investigate topological and localchanges in resting-state visual networks of patients in those 2disease groups further dividing theMS group into patients withand without ON
Our main findings showed 2 distinct patterns of change in thevisual networks of the patient groups First the highly con-nected normal visual network is affected in all 3 diseasegroups showing reduced density and changes in topologyThese differences from HCs however are most pronouncedin the CIS-nON group The 2ON groups (NMOSD and CIS-ON) showed remarkably similar results in density and degreedistribution particularly in lower and dorsal-lateral regionsboth higher than those of patients with CIS-nON This sug-gests changes unique to the directly affected system (visualinput) We cautiously suggest that these changes may reflectan attempt to compensate for the damage incurred lastingeven when the underlying pathology has existed for yearsconsidering the relatively long disease durations displayed bythe NMOSD compared with the CIS-ON group
Second measures of network segregation and integration de-fining efficiency of information transfer and local structureshowed similarity between the MS-background groups (CIS-ON and CIS-nON) whereas the NMOSD group showedresults closer to those of the HCs This suggests that networksegregation and integration may be more affected by type ofunderlying pathophysiology rather than the specific neurologicdeficit
The question of whether cortical reorganization plays a role inrecovery from ON has long been discussed Early studies fo-cused mainly on cortical activity patterns in response to visualtasks presented to the affected eye Some studies have sug-gested that adaptive cortical plasticity following ON involvesincreased activity in higher visual areas assisting in overcoming
visual insult36ndash39 However later studies suggested that corticalactivation reflects the visual percept rather than demonstratesplasticity8 In recent years the importance of considering cor-tical networks rather than regional activity has emergedFunctional connectivity assessing the synchronized fluctua-tions in the fMRI signal between regions has shown sensitivityto neurologic damage and so it was suggested that connectivityrather than activity may play a role in clinical outcome How-ever as this is a cross-sectional study and no clinical measureswere included this remains hypothetical
InMS andNMOSDmuch emphasis has been given to changesin functional connectivity in sensorimotor networks Func-tional connectivity within the motor network was found toreflect motor function40 and to change in response to re-habilitative intervention41 in patients with MS Whether suchchanges reflect compensatory mechanisms or loss of function isstill a matter of debate4243 It has been suggested that theinterpretation of such observations depends on lesion load anddisease duration44
Our motor network results show no compensatory changes inthe subgroup of nON patients with motor symptoms On thecontrary specific clinical motor involvement resulted in re-duced connectivity within the motor cortex These results areparticularly prominent in view of the opposite results obtainedin the visual network where the relevant neurologic deficitseemed to be associated with elevated connectivity We suggestthat this may be the result of lesions located close to motorregions compared with the more peripheral damage sustainedthrough ON causing greater direct damage to the systemAnother piece of evidence supporting this suggestion is thedenser motor network seen in the NMOSD group who almostall had myelitis in addition to ON (19 of 23 patients) Thisfinding may be the motor networkrsquos equivalent of response todistant damage However because of the small numbers ofpatients included in the nonmotor subgroup and of patientswith nonmyelitis NMOSD these speculations should be takenwith caution
Although much attention has been given to the motor net-works in recent years the visual system has received less at-tention usually as a small part of a wider study4345 A studyfocusing on the visual system of patients with NMOSD andprevious ON has shown increase in the functional connectivityof the primary visual network compared with those withoutON11 These findings were also associated with greater retinaldamage and reduced visual acuity suggesting an attempt atcortical reorganization Similar findings were seen in our pre-vious work showing an increase in visual network connectivityin patients with CIS-ON compared with CIS-nON10 AMEGOCT study of the visual system in patients with MS has suc-ceeded in differentiating between patients with and withoutON based on a unique pattern of connectivity that specificallyinvolves the visual system46 These studies mostly focus on theneurologic deficit as the driving force behind the effects ob-served in MS and NMOSD connectivity and are congruent
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
with the general connectivity patterns presented in our currentstudy
However another cause for connectivity change may be thespecific type of disease Very few studies have tried to compareconnectivity between these 2 similar yet dissimilar diseasegroups Of these one has studied the functional and structuralconnectivity of the thalamus finding structural changes inboth diseases but functional disconnection only in MS47
Another study used a wide array of tests to differentiate be-tween the 2 disease types showing that the top 2 modalitiesuseful in this were white matter lesion load and functionalconnectivity48 In our results the white matter lesion elementappears negligible because both groups exhibit similar lesionnumber and volume and even lesion distribution was notlocalized in any of the groups And yet the segregation andintegration patterns of the functional visual network differedbetween MS and NMOSD with those of the latter moreclosely resembling that of HCs We suggest that this markeddifference may stem from differences in normal-appearingwhite matter Diffusion tensor imaging studies have showndiffusion abnormalities in both disease types but patientswith MS display widespread and more severe degree ofabnormality49ndash51 This may explain the difference in the seg-regation and integration properties of functional connectivitybetween the 2 groups
The use of graph-based analysis has enabled us to explore boththese driving forces of connectivity alterations the specificneurologic deficit and the disease type itself that appear to beassociated with different types of change Another advantageof this method is its ability to examine connectivity not only ina holistic manner In a work from 2015 the advantage ofgraph-based analysis inMS was presented Although emphasiswas on cognitive changes it was suggested that graph theoryshould be used to overcome the simplistic and incompleteinterpretations of previous methods52 Work on functionalconnectivity of the visual network in MS over the years hasmainly examined the network as a single entity using in-dependent component analysis1053 or seed-region analysis54
However the introduction of graph theory methods12 hasopened new possibilities in studying the affected network InMS the different works report both decreased global con-nectivity attributed to disease course and adaptation patternswith increased local connectivity and modularity13 Our cur-rent findings highlighting reorganization in dorsal-lateralregions known to be involved in dynamic perception pro-cesses are consistent with our previous works that emphasizedpersistent motion perception impairment following ON78
Based on our previous works in the field we suggest that thedorsal stream-specific increase in connectivity in our currentstudy may be part of a recovery process involving functionalmodifications Because bothON groups exhibit such a patternthis supports the notion that the neurologic deficit elicits thesechanges As this is a cross-sectional study this remains onlya suggestion
This study has several limitations First graph theorymethods are often used on larger subject groups Howeverthe significance of the results and their consistency with ourprevious findings convince us that our current findings aretrue Second the differences in age in all groups and indisease duration between the disease groups are problem-atic but these measures were factored into the variousanalyses and had no significant influence on the resultsThird our assumptions regarding the existence of com-pensatory mechanisms are based on the patterns emergingand former findings of our research Further light could havebeen shed on the matter had behavioral measures beenincluded as well as a longitudinal design It should be fur-ther noted that this study analyzed only functional con-nections within the visual system without the addedinformation that could have been gleaned from the com-plementing structural connectome limiting the ability todisentangle compensatory changes from structural damageFurthermore although the differences between groups mayindeed be interpreted as reorganizational changes of thevisual network in response to damage they may also reflectdifferential level of damage between individuals This issueshould be further investigated using a different study designbecause it could not be covered under the scope of thecurrent study
To conclude the visual network highly connected inHCs is made less connected by disease be it MS orNMOSD However a higher degree of connections wasobserved in the ON groups (CIS-ON and NMOSD)compared with the nON group This suggests that thesystem responds to specific damage caused to the anteriorvisual pathway bringing connectivity closer to that ofa normal network regardless of disease type On the otherhand network segregation and integration and the effi-ciency of information transfer appear more affected bydisease type altered in the MS groups but not inNMOSD particularly in higher regions Therefore wesuggest that the response to damage is dependent on thetype of neurologic deficit within the limitations of theunderlying pathophysiology
Study fundingSupported by the National Multiple Sclerosis Society (researchgrant RG-1802-30165) and the Applebaum Foundation FPaul was supported by Deutsche Forschungsgemeinschaft(DFG Exc 257)
DisclosureY Backner I Ben-Shalom J Kuchling N Siebert M ScheelK Ruprecht A Brandt F Paul and N Levin report no dis-closures Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationOctober 11 2019 Accepted in final form January 10 2020
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 9
References1 Schoonheim MM Filippi M Functional plasticity in MS Friend or foe Neurology
2012791418ndash14192 Costello F Vision disturbances in multiple sclerosis Semin Neurol 201636185ndash1953 Abel AMcClelland C LeeMS Critical review typical and atypical optic neuritis Surv
Ophthalmol 201964770ndash7794 Chen JJ Pittock SJ Flanagan EP Lennon VA Bhatti MT Optic neuritis in the era of
biomarkers Surv Ophthalmol 20206512ndash175 Lennon VA Wingerchuk DM Kryzer TJ et al A serum autoantibody marker of neu-
romyelitis optica distinction from multiple sclerosis Lancet 20043642106ndash21126 Raz N Chokron S Ben-Hur T Levin N Temporal reorganization to overcome
monocular demyelination Neurology 201381702ndash7097 Raz N Dotan S Chokron S Ben‐Hur T Levin N Demyelination affects temporal
aspects of perception an optic neuritis study Ann Neurol 201271531ndash5388 Raz N Dotan S Benoliel T Chokron S Ben-Hur T Levin N Sustained motion
perception deficit following optic neuritis Behavioral and cortical evidence Neurology2011762103ndash2111
9 Benoliel T Raz N Ben-Hur T Levin N Cortical functional modifications followingoptic neuritis Mult Scler 201723220ndash227
10 Backner Y Kuchling JMassarwa S et al Anatomical wiring and functional networkingchanges in the visual system following optic neuritis JAMANeurol 201875287ndash295
11 Finke C Zimmermann H Pache F et al Association of visual impairment in neu-romyelitis optica spectrum disorder with visual network reorganization JAMANeurol201875296ndash303
12 Rubinov M Sporns O Complex network measures of brain connectivity uses andinterpretations Neuroimage 2010521059ndash1069
13 Fleischer V Radetz A Ciolac D et al Graph theoretical framework of brain networksin multiple sclerosis a review of concepts Neuroscience 201940335ndash53
14 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
15 Wingerchuk DM Banwell B Bennett JL et al International consensus diagnosticcriteria for neuromyelitis optica spectrum disorders Neurology 201585177ndash189
16 Kuchling J Backner Y Oertel FC et al Comparison of probabilistic tractography andtract-based spatial statistics for assessing optic radiation damage in patients withautoimmune inflammatory disorders of the central nervous system Neuroimage Clin201819538ndash550
17 Oertel FC Kuchling J Zimmermann H et al Microstructural visual system changes inAQP4-antibodyndashseropositive NMOSD Neurol Neuroimmunol Neuroinflamm 20174e334 doi 101212NXI0000000000000334
18 Association WM World Medical Association Declaration of Helsinki ethical prin-ciples for medical research involving human subjects JAMA 20133102191
19 Yushkevich PA Piven J Hazlett HC et al User-guided 3D active contour segmen-tation of anatomical structures significantly improved efficiency and reliabilityNeuroimage 2006311116ndash1128
20 Wang L Mruczek RE Arcaro MJ Kastner S Probabilistic maps of visual topographyin human cortex Cereb Cortex 2014253911ndash3931
21 Hindy NC Ng FY Turk-Browne NB Linking pattern completion in the hippo-campus to predictive coding in visual cortex Nat Neurosci 201619665
22 Cichy RM Khosla A Pantazis D Torralba A Oliva A Comparison of deep neuralnetworks to spatio-temporal cortical dynamics of human visual object recognitionreveals hierarchical correspondence Sci Rep 2016627755
23 Cichy RM Pantazis D Oliva A Similarity-based fusion of MEG and fMRI revealsspatio-temporal dynamics in human cortex during visual object recognition CerebCortex 2016263563ndash3579
24 Mackey WE Winawer J Curtis CE Visual field map clusters in human frontoparietalcortex Elife 20176e22974
25 Smith SM Jenkinson M Woolrich MW et al Advances in functional and structuralMR image analysis and implementation as FSL Neuroimage 200423S208ndashS219
26 Pool E-M Rehme AK Eickhoff SB Fink GR Grefkes C Functional resting-stateconnectivity of the humanmotor network differences between right-and left-handersNeuroimage 2015109298ndash306
27 Hardwick RM Rottschy C Miall RC Eickhoff SB A quantitative meta-analysis andreview of motor learning in the human brain Neuroimage 201367283ndash297
28 Rocca MA Meani A Riccitelli GC et al Abnormal adaptation over time of motornetwork recruitment in multiple sclerosis patients with fatigue Mult Scler J 2016221144ndash1153
29 Watts DJ Strogatz SH Collective dynamics of ldquosmall-worldrdquonetworks Nature 1998393440ndash442
30 Maslov S Sneppen K Specificity and stability in topology of protein networks Sci-ence 2002296910ndash913
31 Newman ME The structure and function of complex networks SIAM Rev 200345167ndash256
32 Latora V Marchiori M Efficient behavior of small-world networks Phys Rev Lett200187198701
33 Newman ME Modularity and community structure in networks Proc Natl Acad SciUSA 20061038577ndash8582
34 Zamvil SS Slavin AJ Does MOG Ig-posit ive AQP4-seronegative opti-cospinal inflammatory disease justify a diagnosis of NMO spectrumdisorder Neurol Neuroimmunol Neuroinflamm 20152e62 doi 101212NXI0000000000000062
35 Zekeridou A Lennon VA Aquaporin-4 autoimmunity Neurol NeuroimmunolNeuroinflamm 20152e110 doi 101212NXI0000000000000110
36 Toosy AT Hickman SJ Miszkiel KA et al Adaptive cortical plasticity in higher visualareas after acute optic neuritis Ann Neurol 200557622ndash633
37 Jenkins TM Toosy AT Ciccarelli O et al Neuroplasticity predicts outcome of opticneuritis independent of tissue damage Ann Neurol 20106799ndash113
38 Werring DJ Bullmore ET Toosy AT et al Recovery from optic neuritis is associatedwith a change in the distribution of cerebral response to visual stimulation a func-tional magnetic resonance imaging study J Neurol Neurosurg Psychiatry 200068441ndash449
39 Levin N Orlov T Dotan S Zohary E Normal and abnormal fMRI activation patternsin the visual cortex after recovery from optic neuritis Neuroimage 2006331161ndash1168
40 Cordani C Meani A Esposito F et al Imaging correlates of hand motor performancein multiple sclerosis a multiparametric structural and functional MRI study MultScler 20191352458518822145
41 Fling BW Martini DN Zeeboer E Hildebrand A Cameron M Neuroplasticity of thesensorimotor neural network associated with walking aid training in people withmultiple sclerosis Mult Scler Relat Disord 2019311ndash4
42 Tommasin S De Giglio L Ruggieri S et al Relation between functional connectivityand disability in multiple sclerosis a non-linear model J Neurol 20182652881ndash2892
43 Castellazzi G Debernard L Melzer TR et al Functional connectivity alterationsreveal complex mechanisms based on clinical and radiological status in mild relapsingremitting multiple sclerosis Front Neurol 20189690
44 Tewarie P Steenwijk MD Brookes MJ et al Explaining the heterogeneity of func-tional connectivity findings in multiple sclerosis an empirically informed modelingstudy Hum Brain Mapp 2018392541ndash2548
45 Rocca MA Savoldi F Valsasina P et al Cross-modal plasticity among sensory net-works in neuromyelitis optica spectrum disorders Mult Scler 201925968ndash979
46 Tewarie P Balk LJ Hillebrand A et al Structure‐function relationships in the visualsystem in multiple sclerosis an MEG and OCT study Ann Clin Transl Neurol 20174614ndash621
47 Liu Y Duan Y Huang J et al Multimodal quantitative MR imaging of the thalamus inmultiple sclerosis and neuromyelitis optica Radiology 2015277784ndash792
Appendix Authors
Name Location Contribution
YaelBacknerMSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Designed andconceptualized the studyanalyzed the data draftedthe figures and draftedthe manuscript forintellectual content
Ido Ben-ShalomBMedSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Analyzed the motornetwork data
JosephKuchlingMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
NadjaSiebert MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
MichaelScheel MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
KlemensRuprechtMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
AlexanderBrandt MD
CharitendashUniversitatsmedizinBerlin Germany Universityof California
Major role in dataacquisition
FriedemannPaul MD
CharitendashUniversitatsmedizinBerlin Germany
Supervised the study andrevised the manuscript forintellectual content
Netta LevinMD PhD
Hadassah-HebrewUniversity Medical CenterJerusalem Israel
Conceptualized anddesigned the studysupervised the studyand drafted themanuscript forintellectual content
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

plusmn 01 p = 00009) and it is higher though not significantly sothan the density of theCIS-ONgroup (022 plusmn 01 p= 005) TheNMOSD group (024 plusmn 01) density was higher than that of theCIS-nON group but not significantly so (p = 006) No signif-icant differences were found between the CIS-ON andNMOSDgroups or between the NMOSD and HC groups
Themean degree of theHC groupwas significantly higher thanthat of the CIS-nONgroup in all visual regions although not allsurvived multiple comparison correction Most survivingcomparisons were in low-order and dorsal-lateral regions(lower-ventral V1v and V2v lower-dorsal V1d V2d and V3ddorsal-lateral MST hMT and V3b frontal-parietal IPS0IPS1 and IPS2)
In addition the pattern found using the density metric bywhich HCs gt NMOSD CIS-ON gt CIS-nON exists mostlyin the dorsal-lateral region subdivision The ventral-temporalsubdivision (excluding the very early regions V1v and V2v)generally shows no significant differences between groups Theparietal-frontal subdivision shows either no significant differ-ences between groups at all (IPS3 IPS4 and IPS5) or a patternwhere the 2 CIS groups show no difference between them butlower mean degree than both the HC and NMOSD groups(SPL1 frontal eye field [FEF] p = 006) Figure 4 shows anexample from each subdivision displaying the emerging pat-terns The average degrees for each ROI can be found in tablee-2 (linkslwwcomNXIA207)
Network segregation and integration patternsAll segregation and integration metrics reveal connectivitydifferences unlike those for the basic network topologyshowing a pattern by which HC NMOSD gt CIS-ON CIS-nON This is in contrast to the basic topology pattern(achieved using the degree and density metrics) which high-lighted the similarity in topology in different diseases sharingthe same neurologic deficit (HC gt NMOSD CIS-ON gtCIS-nON)
Modularity results (figure 5A) show differences between theHC and CIS-nON groups (039 plusmn 005 and 03 plusmn 008 re-spectively p = 0004) as well as between the NMOSD (037 plusmn005) and CIS-nON groups (p = 0016) but no significantdifferences between the HC and NMOSD groups Themodularity result of the CIS-ON group (033 plusmn 009) is notsignificantly different from any of the other groups but isquantitatively closer to the CIS-nON group
The harmonizedmean of the characteristic path length (figure5B) shows a difference between the HC and CIS-nON groups(075 plusmn 044 and 256 plusmn 291 respectively p = 001) Althoughthe difference between the CIS-nON and NMOSD groups(083 plusmn 037 p = 0087) is not significant the NMOSD groupdisplays a shorter path length The harmonized mean of theCIS-ON group (211 plusmn 279) was not significantly differentfrom any of the groups and no significant difference wasfound between the HC and NMOSD groups
Figure 3 Visualization of the visual system for the 4 subject groups
Considered at correlation threshold r = 05 shown in the coronal (back view top) sagittal (lateral left hemisphere viewmiddle) and axial (dorsal view bottom)planes Nodes (regions of interest) are color coded according to their classification inWang et al20mdashventral-temporal (red) dorsal-lateral (blue) and parietal-frontal (green) The size of nodes reflects the relative degree of a given region in the network Disconnected regions are presented using an arbitrarily selectedsize for visualization purposes Visualization created using reference 55 CIS = clinically isolated syndrome NMOSD = neuromyelitis optica spectrumdisordernON = nonoptic neuritis ON = optic neuritis
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
Similarly global efficiency (figure 5C) shows change betweenthe HC and CIS-nON groups (035 and 025 respectively p =0008) Again no significant difference was found betweenthe NMOSD (031) and CIS-nON groups (p = 0093) butthe NMOSD group quantitatively shows higher efficiencyThe CIS-ON group once again shows no significant differ-ences (028) from any group but is between the NMOSD andCIS-nON groups in terms of global efficiency
Local efficiency showed similar results with differences foundbetween the CIS-nON group and the HC and NMOSDgroups though mostly in high-order regions particularly in thedorsal-lateral and parietal-frontal region subdivisions (lower-ventral V1v CIS-nONvsHCs only lower-dorsal V3d dorsal-lateral MST hMT V3a CIS-nON vs HCs only LO1 LO2V3b CIS-nON vs HCs and NMOSD frontal-parietal IPS3IPS4 IPS5 SPL1 vs HCs only IPS2 FEF vs HCs andNMOSD regions V3b IPS3 IPS5 have also shown significant
differences between HCs and CIS-ON) Details on local effi-ciency for each ROI can be seen in table e-3 (linkslwwcomNXIA207)
Motor network resultsDifferences between groups were found using the degreemetric in the motor putamen between the HC group whichwas most connected (054) and all patient groups (CIS-ON028 CIS-nON-motor 0225 CIS-nON-other 028 p lt 001for all) except for the NMOSD group (038 p = 01 aftermultiple comparison correction) No significant differenceswere found between any patient groups
In the pars opercularis (inferior frontal gyrusndashpars opercularis)differences were found between the CIS-nON-motor group(025) and the HC (057 p = 0004) and NMOSD (049p = 003) groups Density and global efficiency metrics alsoshow differences between the HC group and the CIS-nON-
Figure 4 Average degree of all 4 subject groups for selected regions of the 3 region subdivisions
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) hMT (dorsal-lateral subdivision) (B) VO1 (ventral-temporal subdivision) (C) FEF(frontal eye field parietal-frontal subdivision) Significantly different than HC CIS = clinically isolated syndrome HC = healthy control hMT = humanmiddletemporal region NMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritis ON = optic neuritis
Figure 5 Segregation and integration metrics for all 4 subject groups
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) Modularity (B) harmonizedmean of characteristic path length (C) global efficiencySignificantly different thanHC Significantly different thanNMOSD CIS = clinically isolated syndrome HC = healthy control NMOSD = neuromyelitis opticaspectrum disorder nON = nonoptic neuritis ON = optic neuritis
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 7
motor group (density HCs 012 CIS-nON-motor 007 p =0005 efficiencyHCs 014 CIS-nON-motor 009 p = 0001)Density also shows difference between the HC group and theCIS-ON group (011 p = 004) Other comparisons did notsurvive correction but surprisingly the general pattern remainshere similarly to the visual network HCs gt NMOSD gt CIS-ON CIS-nON-other gt CIS-nON-motor Results are pre-sented in figure e-3 (linkslwwcomNXIA207)
DiscussionIn this study we addressed visual cortical network patterns ininflammatory diseases following ON To that end we included2 prototypic autoimmune CNS diseases with distinct un-derlying pathophysiology MS and NMOSD3435 These dis-eases both share visual dysfunction caused by ON as clinicalcommonality Through these 2 disease types we haveattempted to discover whether changes to the visual systemfollowing ON are driven just by the specific neurologic visualdeficit or also by the underlying pathophysiology We usedgraph analysis methods to investigate topological and localchanges in resting-state visual networks of patients in those 2disease groups further dividing theMS group into patients withand without ON
Our main findings showed 2 distinct patterns of change in thevisual networks of the patient groups First the highly con-nected normal visual network is affected in all 3 diseasegroups showing reduced density and changes in topologyThese differences from HCs however are most pronouncedin the CIS-nON group The 2ON groups (NMOSD and CIS-ON) showed remarkably similar results in density and degreedistribution particularly in lower and dorsal-lateral regionsboth higher than those of patients with CIS-nON This sug-gests changes unique to the directly affected system (visualinput) We cautiously suggest that these changes may reflectan attempt to compensate for the damage incurred lastingeven when the underlying pathology has existed for yearsconsidering the relatively long disease durations displayed bythe NMOSD compared with the CIS-ON group
Second measures of network segregation and integration de-fining efficiency of information transfer and local structureshowed similarity between the MS-background groups (CIS-ON and CIS-nON) whereas the NMOSD group showedresults closer to those of the HCs This suggests that networksegregation and integration may be more affected by type ofunderlying pathophysiology rather than the specific neurologicdeficit
The question of whether cortical reorganization plays a role inrecovery from ON has long been discussed Early studies fo-cused mainly on cortical activity patterns in response to visualtasks presented to the affected eye Some studies have sug-gested that adaptive cortical plasticity following ON involvesincreased activity in higher visual areas assisting in overcoming
visual insult36ndash39 However later studies suggested that corticalactivation reflects the visual percept rather than demonstratesplasticity8 In recent years the importance of considering cor-tical networks rather than regional activity has emergedFunctional connectivity assessing the synchronized fluctua-tions in the fMRI signal between regions has shown sensitivityto neurologic damage and so it was suggested that connectivityrather than activity may play a role in clinical outcome How-ever as this is a cross-sectional study and no clinical measureswere included this remains hypothetical
InMS andNMOSDmuch emphasis has been given to changesin functional connectivity in sensorimotor networks Func-tional connectivity within the motor network was found toreflect motor function40 and to change in response to re-habilitative intervention41 in patients with MS Whether suchchanges reflect compensatory mechanisms or loss of function isstill a matter of debate4243 It has been suggested that theinterpretation of such observations depends on lesion load anddisease duration44
Our motor network results show no compensatory changes inthe subgroup of nON patients with motor symptoms On thecontrary specific clinical motor involvement resulted in re-duced connectivity within the motor cortex These results areparticularly prominent in view of the opposite results obtainedin the visual network where the relevant neurologic deficitseemed to be associated with elevated connectivity We suggestthat this may be the result of lesions located close to motorregions compared with the more peripheral damage sustainedthrough ON causing greater direct damage to the systemAnother piece of evidence supporting this suggestion is thedenser motor network seen in the NMOSD group who almostall had myelitis in addition to ON (19 of 23 patients) Thisfinding may be the motor networkrsquos equivalent of response todistant damage However because of the small numbers ofpatients included in the nonmotor subgroup and of patientswith nonmyelitis NMOSD these speculations should be takenwith caution
Although much attention has been given to the motor net-works in recent years the visual system has received less at-tention usually as a small part of a wider study4345 A studyfocusing on the visual system of patients with NMOSD andprevious ON has shown increase in the functional connectivityof the primary visual network compared with those withoutON11 These findings were also associated with greater retinaldamage and reduced visual acuity suggesting an attempt atcortical reorganization Similar findings were seen in our pre-vious work showing an increase in visual network connectivityin patients with CIS-ON compared with CIS-nON10 AMEGOCT study of the visual system in patients with MS has suc-ceeded in differentiating between patients with and withoutON based on a unique pattern of connectivity that specificallyinvolves the visual system46 These studies mostly focus on theneurologic deficit as the driving force behind the effects ob-served in MS and NMOSD connectivity and are congruent
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
with the general connectivity patterns presented in our currentstudy
However another cause for connectivity change may be thespecific type of disease Very few studies have tried to compareconnectivity between these 2 similar yet dissimilar diseasegroups Of these one has studied the functional and structuralconnectivity of the thalamus finding structural changes inboth diseases but functional disconnection only in MS47
Another study used a wide array of tests to differentiate be-tween the 2 disease types showing that the top 2 modalitiesuseful in this were white matter lesion load and functionalconnectivity48 In our results the white matter lesion elementappears negligible because both groups exhibit similar lesionnumber and volume and even lesion distribution was notlocalized in any of the groups And yet the segregation andintegration patterns of the functional visual network differedbetween MS and NMOSD with those of the latter moreclosely resembling that of HCs We suggest that this markeddifference may stem from differences in normal-appearingwhite matter Diffusion tensor imaging studies have showndiffusion abnormalities in both disease types but patientswith MS display widespread and more severe degree ofabnormality49ndash51 This may explain the difference in the seg-regation and integration properties of functional connectivitybetween the 2 groups
The use of graph-based analysis has enabled us to explore boththese driving forces of connectivity alterations the specificneurologic deficit and the disease type itself that appear to beassociated with different types of change Another advantageof this method is its ability to examine connectivity not only ina holistic manner In a work from 2015 the advantage ofgraph-based analysis inMS was presented Although emphasiswas on cognitive changes it was suggested that graph theoryshould be used to overcome the simplistic and incompleteinterpretations of previous methods52 Work on functionalconnectivity of the visual network in MS over the years hasmainly examined the network as a single entity using in-dependent component analysis1053 or seed-region analysis54
However the introduction of graph theory methods12 hasopened new possibilities in studying the affected network InMS the different works report both decreased global con-nectivity attributed to disease course and adaptation patternswith increased local connectivity and modularity13 Our cur-rent findings highlighting reorganization in dorsal-lateralregions known to be involved in dynamic perception pro-cesses are consistent with our previous works that emphasizedpersistent motion perception impairment following ON78
Based on our previous works in the field we suggest that thedorsal stream-specific increase in connectivity in our currentstudy may be part of a recovery process involving functionalmodifications Because bothON groups exhibit such a patternthis supports the notion that the neurologic deficit elicits thesechanges As this is a cross-sectional study this remains onlya suggestion
This study has several limitations First graph theorymethods are often used on larger subject groups Howeverthe significance of the results and their consistency with ourprevious findings convince us that our current findings aretrue Second the differences in age in all groups and indisease duration between the disease groups are problem-atic but these measures were factored into the variousanalyses and had no significant influence on the resultsThird our assumptions regarding the existence of com-pensatory mechanisms are based on the patterns emergingand former findings of our research Further light could havebeen shed on the matter had behavioral measures beenincluded as well as a longitudinal design It should be fur-ther noted that this study analyzed only functional con-nections within the visual system without the addedinformation that could have been gleaned from the com-plementing structural connectome limiting the ability todisentangle compensatory changes from structural damageFurthermore although the differences between groups mayindeed be interpreted as reorganizational changes of thevisual network in response to damage they may also reflectdifferential level of damage between individuals This issueshould be further investigated using a different study designbecause it could not be covered under the scope of thecurrent study
To conclude the visual network highly connected inHCs is made less connected by disease be it MS orNMOSD However a higher degree of connections wasobserved in the ON groups (CIS-ON and NMOSD)compared with the nON group This suggests that thesystem responds to specific damage caused to the anteriorvisual pathway bringing connectivity closer to that ofa normal network regardless of disease type On the otherhand network segregation and integration and the effi-ciency of information transfer appear more affected bydisease type altered in the MS groups but not inNMOSD particularly in higher regions Therefore wesuggest that the response to damage is dependent on thetype of neurologic deficit within the limitations of theunderlying pathophysiology
Study fundingSupported by the National Multiple Sclerosis Society (researchgrant RG-1802-30165) and the Applebaum Foundation FPaul was supported by Deutsche Forschungsgemeinschaft(DFG Exc 257)
DisclosureY Backner I Ben-Shalom J Kuchling N Siebert M ScheelK Ruprecht A Brandt F Paul and N Levin report no dis-closures Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationOctober 11 2019 Accepted in final form January 10 2020
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 9
References1 Schoonheim MM Filippi M Functional plasticity in MS Friend or foe Neurology
2012791418ndash14192 Costello F Vision disturbances in multiple sclerosis Semin Neurol 201636185ndash1953 Abel AMcClelland C LeeMS Critical review typical and atypical optic neuritis Surv
Ophthalmol 201964770ndash7794 Chen JJ Pittock SJ Flanagan EP Lennon VA Bhatti MT Optic neuritis in the era of
biomarkers Surv Ophthalmol 20206512ndash175 Lennon VA Wingerchuk DM Kryzer TJ et al A serum autoantibody marker of neu-
romyelitis optica distinction from multiple sclerosis Lancet 20043642106ndash21126 Raz N Chokron S Ben-Hur T Levin N Temporal reorganization to overcome
monocular demyelination Neurology 201381702ndash7097 Raz N Dotan S Chokron S Ben‐Hur T Levin N Demyelination affects temporal
aspects of perception an optic neuritis study Ann Neurol 201271531ndash5388 Raz N Dotan S Benoliel T Chokron S Ben-Hur T Levin N Sustained motion
perception deficit following optic neuritis Behavioral and cortical evidence Neurology2011762103ndash2111
9 Benoliel T Raz N Ben-Hur T Levin N Cortical functional modifications followingoptic neuritis Mult Scler 201723220ndash227
10 Backner Y Kuchling JMassarwa S et al Anatomical wiring and functional networkingchanges in the visual system following optic neuritis JAMANeurol 201875287ndash295
11 Finke C Zimmermann H Pache F et al Association of visual impairment in neu-romyelitis optica spectrum disorder with visual network reorganization JAMANeurol201875296ndash303
12 Rubinov M Sporns O Complex network measures of brain connectivity uses andinterpretations Neuroimage 2010521059ndash1069
13 Fleischer V Radetz A Ciolac D et al Graph theoretical framework of brain networksin multiple sclerosis a review of concepts Neuroscience 201940335ndash53
14 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
15 Wingerchuk DM Banwell B Bennett JL et al International consensus diagnosticcriteria for neuromyelitis optica spectrum disorders Neurology 201585177ndash189
16 Kuchling J Backner Y Oertel FC et al Comparison of probabilistic tractography andtract-based spatial statistics for assessing optic radiation damage in patients withautoimmune inflammatory disorders of the central nervous system Neuroimage Clin201819538ndash550
17 Oertel FC Kuchling J Zimmermann H et al Microstructural visual system changes inAQP4-antibodyndashseropositive NMOSD Neurol Neuroimmunol Neuroinflamm 20174e334 doi 101212NXI0000000000000334
18 Association WM World Medical Association Declaration of Helsinki ethical prin-ciples for medical research involving human subjects JAMA 20133102191
19 Yushkevich PA Piven J Hazlett HC et al User-guided 3D active contour segmen-tation of anatomical structures significantly improved efficiency and reliabilityNeuroimage 2006311116ndash1128
20 Wang L Mruczek RE Arcaro MJ Kastner S Probabilistic maps of visual topographyin human cortex Cereb Cortex 2014253911ndash3931
21 Hindy NC Ng FY Turk-Browne NB Linking pattern completion in the hippo-campus to predictive coding in visual cortex Nat Neurosci 201619665
22 Cichy RM Khosla A Pantazis D Torralba A Oliva A Comparison of deep neuralnetworks to spatio-temporal cortical dynamics of human visual object recognitionreveals hierarchical correspondence Sci Rep 2016627755
23 Cichy RM Pantazis D Oliva A Similarity-based fusion of MEG and fMRI revealsspatio-temporal dynamics in human cortex during visual object recognition CerebCortex 2016263563ndash3579
24 Mackey WE Winawer J Curtis CE Visual field map clusters in human frontoparietalcortex Elife 20176e22974
25 Smith SM Jenkinson M Woolrich MW et al Advances in functional and structuralMR image analysis and implementation as FSL Neuroimage 200423S208ndashS219
26 Pool E-M Rehme AK Eickhoff SB Fink GR Grefkes C Functional resting-stateconnectivity of the humanmotor network differences between right-and left-handersNeuroimage 2015109298ndash306
27 Hardwick RM Rottschy C Miall RC Eickhoff SB A quantitative meta-analysis andreview of motor learning in the human brain Neuroimage 201367283ndash297
28 Rocca MA Meani A Riccitelli GC et al Abnormal adaptation over time of motornetwork recruitment in multiple sclerosis patients with fatigue Mult Scler J 2016221144ndash1153
29 Watts DJ Strogatz SH Collective dynamics of ldquosmall-worldrdquonetworks Nature 1998393440ndash442
30 Maslov S Sneppen K Specificity and stability in topology of protein networks Sci-ence 2002296910ndash913
31 Newman ME The structure and function of complex networks SIAM Rev 200345167ndash256
32 Latora V Marchiori M Efficient behavior of small-world networks Phys Rev Lett200187198701
33 Newman ME Modularity and community structure in networks Proc Natl Acad SciUSA 20061038577ndash8582
34 Zamvil SS Slavin AJ Does MOG Ig-posit ive AQP4-seronegative opti-cospinal inflammatory disease justify a diagnosis of NMO spectrumdisorder Neurol Neuroimmunol Neuroinflamm 20152e62 doi 101212NXI0000000000000062
35 Zekeridou A Lennon VA Aquaporin-4 autoimmunity Neurol NeuroimmunolNeuroinflamm 20152e110 doi 101212NXI0000000000000110
36 Toosy AT Hickman SJ Miszkiel KA et al Adaptive cortical plasticity in higher visualareas after acute optic neuritis Ann Neurol 200557622ndash633
37 Jenkins TM Toosy AT Ciccarelli O et al Neuroplasticity predicts outcome of opticneuritis independent of tissue damage Ann Neurol 20106799ndash113
38 Werring DJ Bullmore ET Toosy AT et al Recovery from optic neuritis is associatedwith a change in the distribution of cerebral response to visual stimulation a func-tional magnetic resonance imaging study J Neurol Neurosurg Psychiatry 200068441ndash449
39 Levin N Orlov T Dotan S Zohary E Normal and abnormal fMRI activation patternsin the visual cortex after recovery from optic neuritis Neuroimage 2006331161ndash1168
40 Cordani C Meani A Esposito F et al Imaging correlates of hand motor performancein multiple sclerosis a multiparametric structural and functional MRI study MultScler 20191352458518822145
41 Fling BW Martini DN Zeeboer E Hildebrand A Cameron M Neuroplasticity of thesensorimotor neural network associated with walking aid training in people withmultiple sclerosis Mult Scler Relat Disord 2019311ndash4
42 Tommasin S De Giglio L Ruggieri S et al Relation between functional connectivityand disability in multiple sclerosis a non-linear model J Neurol 20182652881ndash2892
43 Castellazzi G Debernard L Melzer TR et al Functional connectivity alterationsreveal complex mechanisms based on clinical and radiological status in mild relapsingremitting multiple sclerosis Front Neurol 20189690
44 Tewarie P Steenwijk MD Brookes MJ et al Explaining the heterogeneity of func-tional connectivity findings in multiple sclerosis an empirically informed modelingstudy Hum Brain Mapp 2018392541ndash2548
45 Rocca MA Savoldi F Valsasina P et al Cross-modal plasticity among sensory net-works in neuromyelitis optica spectrum disorders Mult Scler 201925968ndash979
46 Tewarie P Balk LJ Hillebrand A et al Structure‐function relationships in the visualsystem in multiple sclerosis an MEG and OCT study Ann Clin Transl Neurol 20174614ndash621
47 Liu Y Duan Y Huang J et al Multimodal quantitative MR imaging of the thalamus inmultiple sclerosis and neuromyelitis optica Radiology 2015277784ndash792
Appendix Authors
Name Location Contribution
YaelBacknerMSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Designed andconceptualized the studyanalyzed the data draftedthe figures and draftedthe manuscript forintellectual content
Ido Ben-ShalomBMedSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Analyzed the motornetwork data
JosephKuchlingMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
NadjaSiebert MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
MichaelScheel MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
KlemensRuprechtMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
AlexanderBrandt MD
CharitendashUniversitatsmedizinBerlin Germany Universityof California
Major role in dataacquisition
FriedemannPaul MD
CharitendashUniversitatsmedizinBerlin Germany
Supervised the study andrevised the manuscript forintellectual content
Netta LevinMD PhD
Hadassah-HebrewUniversity Medical CenterJerusalem Israel
Conceptualized anddesigned the studysupervised the studyand drafted themanuscript forintellectual content
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

Similarly global efficiency (figure 5C) shows change betweenthe HC and CIS-nON groups (035 and 025 respectively p =0008) Again no significant difference was found betweenthe NMOSD (031) and CIS-nON groups (p = 0093) butthe NMOSD group quantitatively shows higher efficiencyThe CIS-ON group once again shows no significant differ-ences (028) from any group but is between the NMOSD andCIS-nON groups in terms of global efficiency
Local efficiency showed similar results with differences foundbetween the CIS-nON group and the HC and NMOSDgroups though mostly in high-order regions particularly in thedorsal-lateral and parietal-frontal region subdivisions (lower-ventral V1v CIS-nONvsHCs only lower-dorsal V3d dorsal-lateral MST hMT V3a CIS-nON vs HCs only LO1 LO2V3b CIS-nON vs HCs and NMOSD frontal-parietal IPS3IPS4 IPS5 SPL1 vs HCs only IPS2 FEF vs HCs andNMOSD regions V3b IPS3 IPS5 have also shown significant
differences between HCs and CIS-ON) Details on local effi-ciency for each ROI can be seen in table e-3 (linkslwwcomNXIA207)
Motor network resultsDifferences between groups were found using the degreemetric in the motor putamen between the HC group whichwas most connected (054) and all patient groups (CIS-ON028 CIS-nON-motor 0225 CIS-nON-other 028 p lt 001for all) except for the NMOSD group (038 p = 01 aftermultiple comparison correction) No significant differenceswere found between any patient groups
In the pars opercularis (inferior frontal gyrusndashpars opercularis)differences were found between the CIS-nON-motor group(025) and the HC (057 p = 0004) and NMOSD (049p = 003) groups Density and global efficiency metrics alsoshow differences between the HC group and the CIS-nON-
Figure 4 Average degree of all 4 subject groups for selected regions of the 3 region subdivisions
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) hMT (dorsal-lateral subdivision) (B) VO1 (ventral-temporal subdivision) (C) FEF(frontal eye field parietal-frontal subdivision) Significantly different than HC CIS = clinically isolated syndrome HC = healthy control hMT = humanmiddletemporal region NMOSD = neuromyelitis optica spectrum disorder nON = nonoptic neuritis ON = optic neuritis
Figure 5 Segregation and integration metrics for all 4 subject groups
HCs in blue NMOSD in purple CIS-ON in red and CIS-nON in orange (A) Modularity (B) harmonizedmean of characteristic path length (C) global efficiencySignificantly different thanHC Significantly different thanNMOSD CIS = clinically isolated syndrome HC = healthy control NMOSD = neuromyelitis opticaspectrum disorder nON = nonoptic neuritis ON = optic neuritis
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 7
motor group (density HCs 012 CIS-nON-motor 007 p =0005 efficiencyHCs 014 CIS-nON-motor 009 p = 0001)Density also shows difference between the HC group and theCIS-ON group (011 p = 004) Other comparisons did notsurvive correction but surprisingly the general pattern remainshere similarly to the visual network HCs gt NMOSD gt CIS-ON CIS-nON-other gt CIS-nON-motor Results are pre-sented in figure e-3 (linkslwwcomNXIA207)
DiscussionIn this study we addressed visual cortical network patterns ininflammatory diseases following ON To that end we included2 prototypic autoimmune CNS diseases with distinct un-derlying pathophysiology MS and NMOSD3435 These dis-eases both share visual dysfunction caused by ON as clinicalcommonality Through these 2 disease types we haveattempted to discover whether changes to the visual systemfollowing ON are driven just by the specific neurologic visualdeficit or also by the underlying pathophysiology We usedgraph analysis methods to investigate topological and localchanges in resting-state visual networks of patients in those 2disease groups further dividing theMS group into patients withand without ON
Our main findings showed 2 distinct patterns of change in thevisual networks of the patient groups First the highly con-nected normal visual network is affected in all 3 diseasegroups showing reduced density and changes in topologyThese differences from HCs however are most pronouncedin the CIS-nON group The 2ON groups (NMOSD and CIS-ON) showed remarkably similar results in density and degreedistribution particularly in lower and dorsal-lateral regionsboth higher than those of patients with CIS-nON This sug-gests changes unique to the directly affected system (visualinput) We cautiously suggest that these changes may reflectan attempt to compensate for the damage incurred lastingeven when the underlying pathology has existed for yearsconsidering the relatively long disease durations displayed bythe NMOSD compared with the CIS-ON group
Second measures of network segregation and integration de-fining efficiency of information transfer and local structureshowed similarity between the MS-background groups (CIS-ON and CIS-nON) whereas the NMOSD group showedresults closer to those of the HCs This suggests that networksegregation and integration may be more affected by type ofunderlying pathophysiology rather than the specific neurologicdeficit
The question of whether cortical reorganization plays a role inrecovery from ON has long been discussed Early studies fo-cused mainly on cortical activity patterns in response to visualtasks presented to the affected eye Some studies have sug-gested that adaptive cortical plasticity following ON involvesincreased activity in higher visual areas assisting in overcoming
visual insult36ndash39 However later studies suggested that corticalactivation reflects the visual percept rather than demonstratesplasticity8 In recent years the importance of considering cor-tical networks rather than regional activity has emergedFunctional connectivity assessing the synchronized fluctua-tions in the fMRI signal between regions has shown sensitivityto neurologic damage and so it was suggested that connectivityrather than activity may play a role in clinical outcome How-ever as this is a cross-sectional study and no clinical measureswere included this remains hypothetical
InMS andNMOSDmuch emphasis has been given to changesin functional connectivity in sensorimotor networks Func-tional connectivity within the motor network was found toreflect motor function40 and to change in response to re-habilitative intervention41 in patients with MS Whether suchchanges reflect compensatory mechanisms or loss of function isstill a matter of debate4243 It has been suggested that theinterpretation of such observations depends on lesion load anddisease duration44
Our motor network results show no compensatory changes inthe subgroup of nON patients with motor symptoms On thecontrary specific clinical motor involvement resulted in re-duced connectivity within the motor cortex These results areparticularly prominent in view of the opposite results obtainedin the visual network where the relevant neurologic deficitseemed to be associated with elevated connectivity We suggestthat this may be the result of lesions located close to motorregions compared with the more peripheral damage sustainedthrough ON causing greater direct damage to the systemAnother piece of evidence supporting this suggestion is thedenser motor network seen in the NMOSD group who almostall had myelitis in addition to ON (19 of 23 patients) Thisfinding may be the motor networkrsquos equivalent of response todistant damage However because of the small numbers ofpatients included in the nonmotor subgroup and of patientswith nonmyelitis NMOSD these speculations should be takenwith caution
Although much attention has been given to the motor net-works in recent years the visual system has received less at-tention usually as a small part of a wider study4345 A studyfocusing on the visual system of patients with NMOSD andprevious ON has shown increase in the functional connectivityof the primary visual network compared with those withoutON11 These findings were also associated with greater retinaldamage and reduced visual acuity suggesting an attempt atcortical reorganization Similar findings were seen in our pre-vious work showing an increase in visual network connectivityin patients with CIS-ON compared with CIS-nON10 AMEGOCT study of the visual system in patients with MS has suc-ceeded in differentiating between patients with and withoutON based on a unique pattern of connectivity that specificallyinvolves the visual system46 These studies mostly focus on theneurologic deficit as the driving force behind the effects ob-served in MS and NMOSD connectivity and are congruent
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
with the general connectivity patterns presented in our currentstudy
However another cause for connectivity change may be thespecific type of disease Very few studies have tried to compareconnectivity between these 2 similar yet dissimilar diseasegroups Of these one has studied the functional and structuralconnectivity of the thalamus finding structural changes inboth diseases but functional disconnection only in MS47
Another study used a wide array of tests to differentiate be-tween the 2 disease types showing that the top 2 modalitiesuseful in this were white matter lesion load and functionalconnectivity48 In our results the white matter lesion elementappears negligible because both groups exhibit similar lesionnumber and volume and even lesion distribution was notlocalized in any of the groups And yet the segregation andintegration patterns of the functional visual network differedbetween MS and NMOSD with those of the latter moreclosely resembling that of HCs We suggest that this markeddifference may stem from differences in normal-appearingwhite matter Diffusion tensor imaging studies have showndiffusion abnormalities in both disease types but patientswith MS display widespread and more severe degree ofabnormality49ndash51 This may explain the difference in the seg-regation and integration properties of functional connectivitybetween the 2 groups
The use of graph-based analysis has enabled us to explore boththese driving forces of connectivity alterations the specificneurologic deficit and the disease type itself that appear to beassociated with different types of change Another advantageof this method is its ability to examine connectivity not only ina holistic manner In a work from 2015 the advantage ofgraph-based analysis inMS was presented Although emphasiswas on cognitive changes it was suggested that graph theoryshould be used to overcome the simplistic and incompleteinterpretations of previous methods52 Work on functionalconnectivity of the visual network in MS over the years hasmainly examined the network as a single entity using in-dependent component analysis1053 or seed-region analysis54
However the introduction of graph theory methods12 hasopened new possibilities in studying the affected network InMS the different works report both decreased global con-nectivity attributed to disease course and adaptation patternswith increased local connectivity and modularity13 Our cur-rent findings highlighting reorganization in dorsal-lateralregions known to be involved in dynamic perception pro-cesses are consistent with our previous works that emphasizedpersistent motion perception impairment following ON78
Based on our previous works in the field we suggest that thedorsal stream-specific increase in connectivity in our currentstudy may be part of a recovery process involving functionalmodifications Because bothON groups exhibit such a patternthis supports the notion that the neurologic deficit elicits thesechanges As this is a cross-sectional study this remains onlya suggestion
This study has several limitations First graph theorymethods are often used on larger subject groups Howeverthe significance of the results and their consistency with ourprevious findings convince us that our current findings aretrue Second the differences in age in all groups and indisease duration between the disease groups are problem-atic but these measures were factored into the variousanalyses and had no significant influence on the resultsThird our assumptions regarding the existence of com-pensatory mechanisms are based on the patterns emergingand former findings of our research Further light could havebeen shed on the matter had behavioral measures beenincluded as well as a longitudinal design It should be fur-ther noted that this study analyzed only functional con-nections within the visual system without the addedinformation that could have been gleaned from the com-plementing structural connectome limiting the ability todisentangle compensatory changes from structural damageFurthermore although the differences between groups mayindeed be interpreted as reorganizational changes of thevisual network in response to damage they may also reflectdifferential level of damage between individuals This issueshould be further investigated using a different study designbecause it could not be covered under the scope of thecurrent study
To conclude the visual network highly connected inHCs is made less connected by disease be it MS orNMOSD However a higher degree of connections wasobserved in the ON groups (CIS-ON and NMOSD)compared with the nON group This suggests that thesystem responds to specific damage caused to the anteriorvisual pathway bringing connectivity closer to that ofa normal network regardless of disease type On the otherhand network segregation and integration and the effi-ciency of information transfer appear more affected bydisease type altered in the MS groups but not inNMOSD particularly in higher regions Therefore wesuggest that the response to damage is dependent on thetype of neurologic deficit within the limitations of theunderlying pathophysiology
Study fundingSupported by the National Multiple Sclerosis Society (researchgrant RG-1802-30165) and the Applebaum Foundation FPaul was supported by Deutsche Forschungsgemeinschaft(DFG Exc 257)
DisclosureY Backner I Ben-Shalom J Kuchling N Siebert M ScheelK Ruprecht A Brandt F Paul and N Levin report no dis-closures Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationOctober 11 2019 Accepted in final form January 10 2020
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 9
References1 Schoonheim MM Filippi M Functional plasticity in MS Friend or foe Neurology
2012791418ndash14192 Costello F Vision disturbances in multiple sclerosis Semin Neurol 201636185ndash1953 Abel AMcClelland C LeeMS Critical review typical and atypical optic neuritis Surv
Ophthalmol 201964770ndash7794 Chen JJ Pittock SJ Flanagan EP Lennon VA Bhatti MT Optic neuritis in the era of
biomarkers Surv Ophthalmol 20206512ndash175 Lennon VA Wingerchuk DM Kryzer TJ et al A serum autoantibody marker of neu-
romyelitis optica distinction from multiple sclerosis Lancet 20043642106ndash21126 Raz N Chokron S Ben-Hur T Levin N Temporal reorganization to overcome
monocular demyelination Neurology 201381702ndash7097 Raz N Dotan S Chokron S Ben‐Hur T Levin N Demyelination affects temporal
aspects of perception an optic neuritis study Ann Neurol 201271531ndash5388 Raz N Dotan S Benoliel T Chokron S Ben-Hur T Levin N Sustained motion
perception deficit following optic neuritis Behavioral and cortical evidence Neurology2011762103ndash2111
9 Benoliel T Raz N Ben-Hur T Levin N Cortical functional modifications followingoptic neuritis Mult Scler 201723220ndash227
10 Backner Y Kuchling JMassarwa S et al Anatomical wiring and functional networkingchanges in the visual system following optic neuritis JAMANeurol 201875287ndash295
11 Finke C Zimmermann H Pache F et al Association of visual impairment in neu-romyelitis optica spectrum disorder with visual network reorganization JAMANeurol201875296ndash303
12 Rubinov M Sporns O Complex network measures of brain connectivity uses andinterpretations Neuroimage 2010521059ndash1069
13 Fleischer V Radetz A Ciolac D et al Graph theoretical framework of brain networksin multiple sclerosis a review of concepts Neuroscience 201940335ndash53
14 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
15 Wingerchuk DM Banwell B Bennett JL et al International consensus diagnosticcriteria for neuromyelitis optica spectrum disorders Neurology 201585177ndash189
16 Kuchling J Backner Y Oertel FC et al Comparison of probabilistic tractography andtract-based spatial statistics for assessing optic radiation damage in patients withautoimmune inflammatory disorders of the central nervous system Neuroimage Clin201819538ndash550
17 Oertel FC Kuchling J Zimmermann H et al Microstructural visual system changes inAQP4-antibodyndashseropositive NMOSD Neurol Neuroimmunol Neuroinflamm 20174e334 doi 101212NXI0000000000000334
18 Association WM World Medical Association Declaration of Helsinki ethical prin-ciples for medical research involving human subjects JAMA 20133102191
19 Yushkevich PA Piven J Hazlett HC et al User-guided 3D active contour segmen-tation of anatomical structures significantly improved efficiency and reliabilityNeuroimage 2006311116ndash1128
20 Wang L Mruczek RE Arcaro MJ Kastner S Probabilistic maps of visual topographyin human cortex Cereb Cortex 2014253911ndash3931
21 Hindy NC Ng FY Turk-Browne NB Linking pattern completion in the hippo-campus to predictive coding in visual cortex Nat Neurosci 201619665
22 Cichy RM Khosla A Pantazis D Torralba A Oliva A Comparison of deep neuralnetworks to spatio-temporal cortical dynamics of human visual object recognitionreveals hierarchical correspondence Sci Rep 2016627755
23 Cichy RM Pantazis D Oliva A Similarity-based fusion of MEG and fMRI revealsspatio-temporal dynamics in human cortex during visual object recognition CerebCortex 2016263563ndash3579
24 Mackey WE Winawer J Curtis CE Visual field map clusters in human frontoparietalcortex Elife 20176e22974
25 Smith SM Jenkinson M Woolrich MW et al Advances in functional and structuralMR image analysis and implementation as FSL Neuroimage 200423S208ndashS219
26 Pool E-M Rehme AK Eickhoff SB Fink GR Grefkes C Functional resting-stateconnectivity of the humanmotor network differences between right-and left-handersNeuroimage 2015109298ndash306
27 Hardwick RM Rottschy C Miall RC Eickhoff SB A quantitative meta-analysis andreview of motor learning in the human brain Neuroimage 201367283ndash297
28 Rocca MA Meani A Riccitelli GC et al Abnormal adaptation over time of motornetwork recruitment in multiple sclerosis patients with fatigue Mult Scler J 2016221144ndash1153
29 Watts DJ Strogatz SH Collective dynamics of ldquosmall-worldrdquonetworks Nature 1998393440ndash442
30 Maslov S Sneppen K Specificity and stability in topology of protein networks Sci-ence 2002296910ndash913
31 Newman ME The structure and function of complex networks SIAM Rev 200345167ndash256
32 Latora V Marchiori M Efficient behavior of small-world networks Phys Rev Lett200187198701
33 Newman ME Modularity and community structure in networks Proc Natl Acad SciUSA 20061038577ndash8582
34 Zamvil SS Slavin AJ Does MOG Ig-posit ive AQP4-seronegative opti-cospinal inflammatory disease justify a diagnosis of NMO spectrumdisorder Neurol Neuroimmunol Neuroinflamm 20152e62 doi 101212NXI0000000000000062
35 Zekeridou A Lennon VA Aquaporin-4 autoimmunity Neurol NeuroimmunolNeuroinflamm 20152e110 doi 101212NXI0000000000000110
36 Toosy AT Hickman SJ Miszkiel KA et al Adaptive cortical plasticity in higher visualareas after acute optic neuritis Ann Neurol 200557622ndash633
37 Jenkins TM Toosy AT Ciccarelli O et al Neuroplasticity predicts outcome of opticneuritis independent of tissue damage Ann Neurol 20106799ndash113
38 Werring DJ Bullmore ET Toosy AT et al Recovery from optic neuritis is associatedwith a change in the distribution of cerebral response to visual stimulation a func-tional magnetic resonance imaging study J Neurol Neurosurg Psychiatry 200068441ndash449
39 Levin N Orlov T Dotan S Zohary E Normal and abnormal fMRI activation patternsin the visual cortex after recovery from optic neuritis Neuroimage 2006331161ndash1168
40 Cordani C Meani A Esposito F et al Imaging correlates of hand motor performancein multiple sclerosis a multiparametric structural and functional MRI study MultScler 20191352458518822145
41 Fling BW Martini DN Zeeboer E Hildebrand A Cameron M Neuroplasticity of thesensorimotor neural network associated with walking aid training in people withmultiple sclerosis Mult Scler Relat Disord 2019311ndash4
42 Tommasin S De Giglio L Ruggieri S et al Relation between functional connectivityand disability in multiple sclerosis a non-linear model J Neurol 20182652881ndash2892
43 Castellazzi G Debernard L Melzer TR et al Functional connectivity alterationsreveal complex mechanisms based on clinical and radiological status in mild relapsingremitting multiple sclerosis Front Neurol 20189690
44 Tewarie P Steenwijk MD Brookes MJ et al Explaining the heterogeneity of func-tional connectivity findings in multiple sclerosis an empirically informed modelingstudy Hum Brain Mapp 2018392541ndash2548
45 Rocca MA Savoldi F Valsasina P et al Cross-modal plasticity among sensory net-works in neuromyelitis optica spectrum disorders Mult Scler 201925968ndash979
46 Tewarie P Balk LJ Hillebrand A et al Structure‐function relationships in the visualsystem in multiple sclerosis an MEG and OCT study Ann Clin Transl Neurol 20174614ndash621
47 Liu Y Duan Y Huang J et al Multimodal quantitative MR imaging of the thalamus inmultiple sclerosis and neuromyelitis optica Radiology 2015277784ndash792
Appendix Authors
Name Location Contribution
YaelBacknerMSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Designed andconceptualized the studyanalyzed the data draftedthe figures and draftedthe manuscript forintellectual content
Ido Ben-ShalomBMedSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Analyzed the motornetwork data
JosephKuchlingMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
NadjaSiebert MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
MichaelScheel MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
KlemensRuprechtMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
AlexanderBrandt MD
CharitendashUniversitatsmedizinBerlin Germany Universityof California
Major role in dataacquisition
FriedemannPaul MD
CharitendashUniversitatsmedizinBerlin Germany
Supervised the study andrevised the manuscript forintellectual content
Netta LevinMD PhD
Hadassah-HebrewUniversity Medical CenterJerusalem Israel
Conceptualized anddesigned the studysupervised the studyand drafted themanuscript forintellectual content
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

motor group (density HCs 012 CIS-nON-motor 007 p =0005 efficiencyHCs 014 CIS-nON-motor 009 p = 0001)Density also shows difference between the HC group and theCIS-ON group (011 p = 004) Other comparisons did notsurvive correction but surprisingly the general pattern remainshere similarly to the visual network HCs gt NMOSD gt CIS-ON CIS-nON-other gt CIS-nON-motor Results are pre-sented in figure e-3 (linkslwwcomNXIA207)
DiscussionIn this study we addressed visual cortical network patterns ininflammatory diseases following ON To that end we included2 prototypic autoimmune CNS diseases with distinct un-derlying pathophysiology MS and NMOSD3435 These dis-eases both share visual dysfunction caused by ON as clinicalcommonality Through these 2 disease types we haveattempted to discover whether changes to the visual systemfollowing ON are driven just by the specific neurologic visualdeficit or also by the underlying pathophysiology We usedgraph analysis methods to investigate topological and localchanges in resting-state visual networks of patients in those 2disease groups further dividing theMS group into patients withand without ON
Our main findings showed 2 distinct patterns of change in thevisual networks of the patient groups First the highly con-nected normal visual network is affected in all 3 diseasegroups showing reduced density and changes in topologyThese differences from HCs however are most pronouncedin the CIS-nON group The 2ON groups (NMOSD and CIS-ON) showed remarkably similar results in density and degreedistribution particularly in lower and dorsal-lateral regionsboth higher than those of patients with CIS-nON This sug-gests changes unique to the directly affected system (visualinput) We cautiously suggest that these changes may reflectan attempt to compensate for the damage incurred lastingeven when the underlying pathology has existed for yearsconsidering the relatively long disease durations displayed bythe NMOSD compared with the CIS-ON group
Second measures of network segregation and integration de-fining efficiency of information transfer and local structureshowed similarity between the MS-background groups (CIS-ON and CIS-nON) whereas the NMOSD group showedresults closer to those of the HCs This suggests that networksegregation and integration may be more affected by type ofunderlying pathophysiology rather than the specific neurologicdeficit
The question of whether cortical reorganization plays a role inrecovery from ON has long been discussed Early studies fo-cused mainly on cortical activity patterns in response to visualtasks presented to the affected eye Some studies have sug-gested that adaptive cortical plasticity following ON involvesincreased activity in higher visual areas assisting in overcoming
visual insult36ndash39 However later studies suggested that corticalactivation reflects the visual percept rather than demonstratesplasticity8 In recent years the importance of considering cor-tical networks rather than regional activity has emergedFunctional connectivity assessing the synchronized fluctua-tions in the fMRI signal between regions has shown sensitivityto neurologic damage and so it was suggested that connectivityrather than activity may play a role in clinical outcome How-ever as this is a cross-sectional study and no clinical measureswere included this remains hypothetical
InMS andNMOSDmuch emphasis has been given to changesin functional connectivity in sensorimotor networks Func-tional connectivity within the motor network was found toreflect motor function40 and to change in response to re-habilitative intervention41 in patients with MS Whether suchchanges reflect compensatory mechanisms or loss of function isstill a matter of debate4243 It has been suggested that theinterpretation of such observations depends on lesion load anddisease duration44
Our motor network results show no compensatory changes inthe subgroup of nON patients with motor symptoms On thecontrary specific clinical motor involvement resulted in re-duced connectivity within the motor cortex These results areparticularly prominent in view of the opposite results obtainedin the visual network where the relevant neurologic deficitseemed to be associated with elevated connectivity We suggestthat this may be the result of lesions located close to motorregions compared with the more peripheral damage sustainedthrough ON causing greater direct damage to the systemAnother piece of evidence supporting this suggestion is thedenser motor network seen in the NMOSD group who almostall had myelitis in addition to ON (19 of 23 patients) Thisfinding may be the motor networkrsquos equivalent of response todistant damage However because of the small numbers ofpatients included in the nonmotor subgroup and of patientswith nonmyelitis NMOSD these speculations should be takenwith caution
Although much attention has been given to the motor net-works in recent years the visual system has received less at-tention usually as a small part of a wider study4345 A studyfocusing on the visual system of patients with NMOSD andprevious ON has shown increase in the functional connectivityof the primary visual network compared with those withoutON11 These findings were also associated with greater retinaldamage and reduced visual acuity suggesting an attempt atcortical reorganization Similar findings were seen in our pre-vious work showing an increase in visual network connectivityin patients with CIS-ON compared with CIS-nON10 AMEGOCT study of the visual system in patients with MS has suc-ceeded in differentiating between patients with and withoutON based on a unique pattern of connectivity that specificallyinvolves the visual system46 These studies mostly focus on theneurologic deficit as the driving force behind the effects ob-served in MS and NMOSD connectivity and are congruent
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
with the general connectivity patterns presented in our currentstudy
However another cause for connectivity change may be thespecific type of disease Very few studies have tried to compareconnectivity between these 2 similar yet dissimilar diseasegroups Of these one has studied the functional and structuralconnectivity of the thalamus finding structural changes inboth diseases but functional disconnection only in MS47
Another study used a wide array of tests to differentiate be-tween the 2 disease types showing that the top 2 modalitiesuseful in this were white matter lesion load and functionalconnectivity48 In our results the white matter lesion elementappears negligible because both groups exhibit similar lesionnumber and volume and even lesion distribution was notlocalized in any of the groups And yet the segregation andintegration patterns of the functional visual network differedbetween MS and NMOSD with those of the latter moreclosely resembling that of HCs We suggest that this markeddifference may stem from differences in normal-appearingwhite matter Diffusion tensor imaging studies have showndiffusion abnormalities in both disease types but patientswith MS display widespread and more severe degree ofabnormality49ndash51 This may explain the difference in the seg-regation and integration properties of functional connectivitybetween the 2 groups
The use of graph-based analysis has enabled us to explore boththese driving forces of connectivity alterations the specificneurologic deficit and the disease type itself that appear to beassociated with different types of change Another advantageof this method is its ability to examine connectivity not only ina holistic manner In a work from 2015 the advantage ofgraph-based analysis inMS was presented Although emphasiswas on cognitive changes it was suggested that graph theoryshould be used to overcome the simplistic and incompleteinterpretations of previous methods52 Work on functionalconnectivity of the visual network in MS over the years hasmainly examined the network as a single entity using in-dependent component analysis1053 or seed-region analysis54
However the introduction of graph theory methods12 hasopened new possibilities in studying the affected network InMS the different works report both decreased global con-nectivity attributed to disease course and adaptation patternswith increased local connectivity and modularity13 Our cur-rent findings highlighting reorganization in dorsal-lateralregions known to be involved in dynamic perception pro-cesses are consistent with our previous works that emphasizedpersistent motion perception impairment following ON78
Based on our previous works in the field we suggest that thedorsal stream-specific increase in connectivity in our currentstudy may be part of a recovery process involving functionalmodifications Because bothON groups exhibit such a patternthis supports the notion that the neurologic deficit elicits thesechanges As this is a cross-sectional study this remains onlya suggestion
This study has several limitations First graph theorymethods are often used on larger subject groups Howeverthe significance of the results and their consistency with ourprevious findings convince us that our current findings aretrue Second the differences in age in all groups and indisease duration between the disease groups are problem-atic but these measures were factored into the variousanalyses and had no significant influence on the resultsThird our assumptions regarding the existence of com-pensatory mechanisms are based on the patterns emergingand former findings of our research Further light could havebeen shed on the matter had behavioral measures beenincluded as well as a longitudinal design It should be fur-ther noted that this study analyzed only functional con-nections within the visual system without the addedinformation that could have been gleaned from the com-plementing structural connectome limiting the ability todisentangle compensatory changes from structural damageFurthermore although the differences between groups mayindeed be interpreted as reorganizational changes of thevisual network in response to damage they may also reflectdifferential level of damage between individuals This issueshould be further investigated using a different study designbecause it could not be covered under the scope of thecurrent study
To conclude the visual network highly connected inHCs is made less connected by disease be it MS orNMOSD However a higher degree of connections wasobserved in the ON groups (CIS-ON and NMOSD)compared with the nON group This suggests that thesystem responds to specific damage caused to the anteriorvisual pathway bringing connectivity closer to that ofa normal network regardless of disease type On the otherhand network segregation and integration and the effi-ciency of information transfer appear more affected bydisease type altered in the MS groups but not inNMOSD particularly in higher regions Therefore wesuggest that the response to damage is dependent on thetype of neurologic deficit within the limitations of theunderlying pathophysiology
Study fundingSupported by the National Multiple Sclerosis Society (researchgrant RG-1802-30165) and the Applebaum Foundation FPaul was supported by Deutsche Forschungsgemeinschaft(DFG Exc 257)
DisclosureY Backner I Ben-Shalom J Kuchling N Siebert M ScheelK Ruprecht A Brandt F Paul and N Levin report no dis-closures Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationOctober 11 2019 Accepted in final form January 10 2020
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 9
References1 Schoonheim MM Filippi M Functional plasticity in MS Friend or foe Neurology
2012791418ndash14192 Costello F Vision disturbances in multiple sclerosis Semin Neurol 201636185ndash1953 Abel AMcClelland C LeeMS Critical review typical and atypical optic neuritis Surv
Ophthalmol 201964770ndash7794 Chen JJ Pittock SJ Flanagan EP Lennon VA Bhatti MT Optic neuritis in the era of
biomarkers Surv Ophthalmol 20206512ndash175 Lennon VA Wingerchuk DM Kryzer TJ et al A serum autoantibody marker of neu-
romyelitis optica distinction from multiple sclerosis Lancet 20043642106ndash21126 Raz N Chokron S Ben-Hur T Levin N Temporal reorganization to overcome
monocular demyelination Neurology 201381702ndash7097 Raz N Dotan S Chokron S Ben‐Hur T Levin N Demyelination affects temporal
aspects of perception an optic neuritis study Ann Neurol 201271531ndash5388 Raz N Dotan S Benoliel T Chokron S Ben-Hur T Levin N Sustained motion
perception deficit following optic neuritis Behavioral and cortical evidence Neurology2011762103ndash2111
9 Benoliel T Raz N Ben-Hur T Levin N Cortical functional modifications followingoptic neuritis Mult Scler 201723220ndash227
10 Backner Y Kuchling JMassarwa S et al Anatomical wiring and functional networkingchanges in the visual system following optic neuritis JAMANeurol 201875287ndash295
11 Finke C Zimmermann H Pache F et al Association of visual impairment in neu-romyelitis optica spectrum disorder with visual network reorganization JAMANeurol201875296ndash303
12 Rubinov M Sporns O Complex network measures of brain connectivity uses andinterpretations Neuroimage 2010521059ndash1069
13 Fleischer V Radetz A Ciolac D et al Graph theoretical framework of brain networksin multiple sclerosis a review of concepts Neuroscience 201940335ndash53
14 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
15 Wingerchuk DM Banwell B Bennett JL et al International consensus diagnosticcriteria for neuromyelitis optica spectrum disorders Neurology 201585177ndash189
16 Kuchling J Backner Y Oertel FC et al Comparison of probabilistic tractography andtract-based spatial statistics for assessing optic radiation damage in patients withautoimmune inflammatory disorders of the central nervous system Neuroimage Clin201819538ndash550
17 Oertel FC Kuchling J Zimmermann H et al Microstructural visual system changes inAQP4-antibodyndashseropositive NMOSD Neurol Neuroimmunol Neuroinflamm 20174e334 doi 101212NXI0000000000000334
18 Association WM World Medical Association Declaration of Helsinki ethical prin-ciples for medical research involving human subjects JAMA 20133102191
19 Yushkevich PA Piven J Hazlett HC et al User-guided 3D active contour segmen-tation of anatomical structures significantly improved efficiency and reliabilityNeuroimage 2006311116ndash1128
20 Wang L Mruczek RE Arcaro MJ Kastner S Probabilistic maps of visual topographyin human cortex Cereb Cortex 2014253911ndash3931
21 Hindy NC Ng FY Turk-Browne NB Linking pattern completion in the hippo-campus to predictive coding in visual cortex Nat Neurosci 201619665
22 Cichy RM Khosla A Pantazis D Torralba A Oliva A Comparison of deep neuralnetworks to spatio-temporal cortical dynamics of human visual object recognitionreveals hierarchical correspondence Sci Rep 2016627755
23 Cichy RM Pantazis D Oliva A Similarity-based fusion of MEG and fMRI revealsspatio-temporal dynamics in human cortex during visual object recognition CerebCortex 2016263563ndash3579
24 Mackey WE Winawer J Curtis CE Visual field map clusters in human frontoparietalcortex Elife 20176e22974
25 Smith SM Jenkinson M Woolrich MW et al Advances in functional and structuralMR image analysis and implementation as FSL Neuroimage 200423S208ndashS219
26 Pool E-M Rehme AK Eickhoff SB Fink GR Grefkes C Functional resting-stateconnectivity of the humanmotor network differences between right-and left-handersNeuroimage 2015109298ndash306
27 Hardwick RM Rottschy C Miall RC Eickhoff SB A quantitative meta-analysis andreview of motor learning in the human brain Neuroimage 201367283ndash297
28 Rocca MA Meani A Riccitelli GC et al Abnormal adaptation over time of motornetwork recruitment in multiple sclerosis patients with fatigue Mult Scler J 2016221144ndash1153
29 Watts DJ Strogatz SH Collective dynamics of ldquosmall-worldrdquonetworks Nature 1998393440ndash442
30 Maslov S Sneppen K Specificity and stability in topology of protein networks Sci-ence 2002296910ndash913
31 Newman ME The structure and function of complex networks SIAM Rev 200345167ndash256
32 Latora V Marchiori M Efficient behavior of small-world networks Phys Rev Lett200187198701
33 Newman ME Modularity and community structure in networks Proc Natl Acad SciUSA 20061038577ndash8582
34 Zamvil SS Slavin AJ Does MOG Ig-posit ive AQP4-seronegative opti-cospinal inflammatory disease justify a diagnosis of NMO spectrumdisorder Neurol Neuroimmunol Neuroinflamm 20152e62 doi 101212NXI0000000000000062
35 Zekeridou A Lennon VA Aquaporin-4 autoimmunity Neurol NeuroimmunolNeuroinflamm 20152e110 doi 101212NXI0000000000000110
36 Toosy AT Hickman SJ Miszkiel KA et al Adaptive cortical plasticity in higher visualareas after acute optic neuritis Ann Neurol 200557622ndash633
37 Jenkins TM Toosy AT Ciccarelli O et al Neuroplasticity predicts outcome of opticneuritis independent of tissue damage Ann Neurol 20106799ndash113
38 Werring DJ Bullmore ET Toosy AT et al Recovery from optic neuritis is associatedwith a change in the distribution of cerebral response to visual stimulation a func-tional magnetic resonance imaging study J Neurol Neurosurg Psychiatry 200068441ndash449
39 Levin N Orlov T Dotan S Zohary E Normal and abnormal fMRI activation patternsin the visual cortex after recovery from optic neuritis Neuroimage 2006331161ndash1168
40 Cordani C Meani A Esposito F et al Imaging correlates of hand motor performancein multiple sclerosis a multiparametric structural and functional MRI study MultScler 20191352458518822145
41 Fling BW Martini DN Zeeboer E Hildebrand A Cameron M Neuroplasticity of thesensorimotor neural network associated with walking aid training in people withmultiple sclerosis Mult Scler Relat Disord 2019311ndash4
42 Tommasin S De Giglio L Ruggieri S et al Relation between functional connectivityand disability in multiple sclerosis a non-linear model J Neurol 20182652881ndash2892
43 Castellazzi G Debernard L Melzer TR et al Functional connectivity alterationsreveal complex mechanisms based on clinical and radiological status in mild relapsingremitting multiple sclerosis Front Neurol 20189690
44 Tewarie P Steenwijk MD Brookes MJ et al Explaining the heterogeneity of func-tional connectivity findings in multiple sclerosis an empirically informed modelingstudy Hum Brain Mapp 2018392541ndash2548
45 Rocca MA Savoldi F Valsasina P et al Cross-modal plasticity among sensory net-works in neuromyelitis optica spectrum disorders Mult Scler 201925968ndash979
46 Tewarie P Balk LJ Hillebrand A et al Structure‐function relationships in the visualsystem in multiple sclerosis an MEG and OCT study Ann Clin Transl Neurol 20174614ndash621
47 Liu Y Duan Y Huang J et al Multimodal quantitative MR imaging of the thalamus inmultiple sclerosis and neuromyelitis optica Radiology 2015277784ndash792
Appendix Authors
Name Location Contribution
YaelBacknerMSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Designed andconceptualized the studyanalyzed the data draftedthe figures and draftedthe manuscript forintellectual content
Ido Ben-ShalomBMedSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Analyzed the motornetwork data
JosephKuchlingMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
NadjaSiebert MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
MichaelScheel MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
KlemensRuprechtMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
AlexanderBrandt MD
CharitendashUniversitatsmedizinBerlin Germany Universityof California
Major role in dataacquisition
FriedemannPaul MD
CharitendashUniversitatsmedizinBerlin Germany
Supervised the study andrevised the manuscript forintellectual content
Netta LevinMD PhD
Hadassah-HebrewUniversity Medical CenterJerusalem Israel
Conceptualized anddesigned the studysupervised the studyand drafted themanuscript forintellectual content
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

with the general connectivity patterns presented in our currentstudy
However another cause for connectivity change may be thespecific type of disease Very few studies have tried to compareconnectivity between these 2 similar yet dissimilar diseasegroups Of these one has studied the functional and structuralconnectivity of the thalamus finding structural changes inboth diseases but functional disconnection only in MS47
Another study used a wide array of tests to differentiate be-tween the 2 disease types showing that the top 2 modalitiesuseful in this were white matter lesion load and functionalconnectivity48 In our results the white matter lesion elementappears negligible because both groups exhibit similar lesionnumber and volume and even lesion distribution was notlocalized in any of the groups And yet the segregation andintegration patterns of the functional visual network differedbetween MS and NMOSD with those of the latter moreclosely resembling that of HCs We suggest that this markeddifference may stem from differences in normal-appearingwhite matter Diffusion tensor imaging studies have showndiffusion abnormalities in both disease types but patientswith MS display widespread and more severe degree ofabnormality49ndash51 This may explain the difference in the seg-regation and integration properties of functional connectivitybetween the 2 groups
The use of graph-based analysis has enabled us to explore boththese driving forces of connectivity alterations the specificneurologic deficit and the disease type itself that appear to beassociated with different types of change Another advantageof this method is its ability to examine connectivity not only ina holistic manner In a work from 2015 the advantage ofgraph-based analysis inMS was presented Although emphasiswas on cognitive changes it was suggested that graph theoryshould be used to overcome the simplistic and incompleteinterpretations of previous methods52 Work on functionalconnectivity of the visual network in MS over the years hasmainly examined the network as a single entity using in-dependent component analysis1053 or seed-region analysis54
However the introduction of graph theory methods12 hasopened new possibilities in studying the affected network InMS the different works report both decreased global con-nectivity attributed to disease course and adaptation patternswith increased local connectivity and modularity13 Our cur-rent findings highlighting reorganization in dorsal-lateralregions known to be involved in dynamic perception pro-cesses are consistent with our previous works that emphasizedpersistent motion perception impairment following ON78
Based on our previous works in the field we suggest that thedorsal stream-specific increase in connectivity in our currentstudy may be part of a recovery process involving functionalmodifications Because bothON groups exhibit such a patternthis supports the notion that the neurologic deficit elicits thesechanges As this is a cross-sectional study this remains onlya suggestion
This study has several limitations First graph theorymethods are often used on larger subject groups Howeverthe significance of the results and their consistency with ourprevious findings convince us that our current findings aretrue Second the differences in age in all groups and indisease duration between the disease groups are problem-atic but these measures were factored into the variousanalyses and had no significant influence on the resultsThird our assumptions regarding the existence of com-pensatory mechanisms are based on the patterns emergingand former findings of our research Further light could havebeen shed on the matter had behavioral measures beenincluded as well as a longitudinal design It should be fur-ther noted that this study analyzed only functional con-nections within the visual system without the addedinformation that could have been gleaned from the com-plementing structural connectome limiting the ability todisentangle compensatory changes from structural damageFurthermore although the differences between groups mayindeed be interpreted as reorganizational changes of thevisual network in response to damage they may also reflectdifferential level of damage between individuals This issueshould be further investigated using a different study designbecause it could not be covered under the scope of thecurrent study
To conclude the visual network highly connected inHCs is made less connected by disease be it MS orNMOSD However a higher degree of connections wasobserved in the ON groups (CIS-ON and NMOSD)compared with the nON group This suggests that thesystem responds to specific damage caused to the anteriorvisual pathway bringing connectivity closer to that ofa normal network regardless of disease type On the otherhand network segregation and integration and the effi-ciency of information transfer appear more affected bydisease type altered in the MS groups but not inNMOSD particularly in higher regions Therefore wesuggest that the response to damage is dependent on thetype of neurologic deficit within the limitations of theunderlying pathophysiology
Study fundingSupported by the National Multiple Sclerosis Society (researchgrant RG-1802-30165) and the Applebaum Foundation FPaul was supported by Deutsche Forschungsgemeinschaft(DFG Exc 257)
DisclosureY Backner I Ben-Shalom J Kuchling N Siebert M ScheelK Ruprecht A Brandt F Paul and N Levin report no dis-closures Go to NeurologyorgNN for full disclosures
Publication historyReceived by Neurology Neuroimmunology amp NeuroinflammationOctober 11 2019 Accepted in final form January 10 2020
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 9
References1 Schoonheim MM Filippi M Functional plasticity in MS Friend or foe Neurology
2012791418ndash14192 Costello F Vision disturbances in multiple sclerosis Semin Neurol 201636185ndash1953 Abel AMcClelland C LeeMS Critical review typical and atypical optic neuritis Surv
Ophthalmol 201964770ndash7794 Chen JJ Pittock SJ Flanagan EP Lennon VA Bhatti MT Optic neuritis in the era of
biomarkers Surv Ophthalmol 20206512ndash175 Lennon VA Wingerchuk DM Kryzer TJ et al A serum autoantibody marker of neu-
romyelitis optica distinction from multiple sclerosis Lancet 20043642106ndash21126 Raz N Chokron S Ben-Hur T Levin N Temporal reorganization to overcome
monocular demyelination Neurology 201381702ndash7097 Raz N Dotan S Chokron S Ben‐Hur T Levin N Demyelination affects temporal
aspects of perception an optic neuritis study Ann Neurol 201271531ndash5388 Raz N Dotan S Benoliel T Chokron S Ben-Hur T Levin N Sustained motion
perception deficit following optic neuritis Behavioral and cortical evidence Neurology2011762103ndash2111
9 Benoliel T Raz N Ben-Hur T Levin N Cortical functional modifications followingoptic neuritis Mult Scler 201723220ndash227
10 Backner Y Kuchling JMassarwa S et al Anatomical wiring and functional networkingchanges in the visual system following optic neuritis JAMANeurol 201875287ndash295
11 Finke C Zimmermann H Pache F et al Association of visual impairment in neu-romyelitis optica spectrum disorder with visual network reorganization JAMANeurol201875296ndash303
12 Rubinov M Sporns O Complex network measures of brain connectivity uses andinterpretations Neuroimage 2010521059ndash1069
13 Fleischer V Radetz A Ciolac D et al Graph theoretical framework of brain networksin multiple sclerosis a review of concepts Neuroscience 201940335ndash53
14 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
15 Wingerchuk DM Banwell B Bennett JL et al International consensus diagnosticcriteria for neuromyelitis optica spectrum disorders Neurology 201585177ndash189
16 Kuchling J Backner Y Oertel FC et al Comparison of probabilistic tractography andtract-based spatial statistics for assessing optic radiation damage in patients withautoimmune inflammatory disorders of the central nervous system Neuroimage Clin201819538ndash550
17 Oertel FC Kuchling J Zimmermann H et al Microstructural visual system changes inAQP4-antibodyndashseropositive NMOSD Neurol Neuroimmunol Neuroinflamm 20174e334 doi 101212NXI0000000000000334
18 Association WM World Medical Association Declaration of Helsinki ethical prin-ciples for medical research involving human subjects JAMA 20133102191
19 Yushkevich PA Piven J Hazlett HC et al User-guided 3D active contour segmen-tation of anatomical structures significantly improved efficiency and reliabilityNeuroimage 2006311116ndash1128
20 Wang L Mruczek RE Arcaro MJ Kastner S Probabilistic maps of visual topographyin human cortex Cereb Cortex 2014253911ndash3931
21 Hindy NC Ng FY Turk-Browne NB Linking pattern completion in the hippo-campus to predictive coding in visual cortex Nat Neurosci 201619665
22 Cichy RM Khosla A Pantazis D Torralba A Oliva A Comparison of deep neuralnetworks to spatio-temporal cortical dynamics of human visual object recognitionreveals hierarchical correspondence Sci Rep 2016627755
23 Cichy RM Pantazis D Oliva A Similarity-based fusion of MEG and fMRI revealsspatio-temporal dynamics in human cortex during visual object recognition CerebCortex 2016263563ndash3579
24 Mackey WE Winawer J Curtis CE Visual field map clusters in human frontoparietalcortex Elife 20176e22974
25 Smith SM Jenkinson M Woolrich MW et al Advances in functional and structuralMR image analysis and implementation as FSL Neuroimage 200423S208ndashS219
26 Pool E-M Rehme AK Eickhoff SB Fink GR Grefkes C Functional resting-stateconnectivity of the humanmotor network differences between right-and left-handersNeuroimage 2015109298ndash306
27 Hardwick RM Rottschy C Miall RC Eickhoff SB A quantitative meta-analysis andreview of motor learning in the human brain Neuroimage 201367283ndash297
28 Rocca MA Meani A Riccitelli GC et al Abnormal adaptation over time of motornetwork recruitment in multiple sclerosis patients with fatigue Mult Scler J 2016221144ndash1153
29 Watts DJ Strogatz SH Collective dynamics of ldquosmall-worldrdquonetworks Nature 1998393440ndash442
30 Maslov S Sneppen K Specificity and stability in topology of protein networks Sci-ence 2002296910ndash913
31 Newman ME The structure and function of complex networks SIAM Rev 200345167ndash256
32 Latora V Marchiori M Efficient behavior of small-world networks Phys Rev Lett200187198701
33 Newman ME Modularity and community structure in networks Proc Natl Acad SciUSA 20061038577ndash8582
34 Zamvil SS Slavin AJ Does MOG Ig-posit ive AQP4-seronegative opti-cospinal inflammatory disease justify a diagnosis of NMO spectrumdisorder Neurol Neuroimmunol Neuroinflamm 20152e62 doi 101212NXI0000000000000062
35 Zekeridou A Lennon VA Aquaporin-4 autoimmunity Neurol NeuroimmunolNeuroinflamm 20152e110 doi 101212NXI0000000000000110
36 Toosy AT Hickman SJ Miszkiel KA et al Adaptive cortical plasticity in higher visualareas after acute optic neuritis Ann Neurol 200557622ndash633
37 Jenkins TM Toosy AT Ciccarelli O et al Neuroplasticity predicts outcome of opticneuritis independent of tissue damage Ann Neurol 20106799ndash113
38 Werring DJ Bullmore ET Toosy AT et al Recovery from optic neuritis is associatedwith a change in the distribution of cerebral response to visual stimulation a func-tional magnetic resonance imaging study J Neurol Neurosurg Psychiatry 200068441ndash449
39 Levin N Orlov T Dotan S Zohary E Normal and abnormal fMRI activation patternsin the visual cortex after recovery from optic neuritis Neuroimage 2006331161ndash1168
40 Cordani C Meani A Esposito F et al Imaging correlates of hand motor performancein multiple sclerosis a multiparametric structural and functional MRI study MultScler 20191352458518822145
41 Fling BW Martini DN Zeeboer E Hildebrand A Cameron M Neuroplasticity of thesensorimotor neural network associated with walking aid training in people withmultiple sclerosis Mult Scler Relat Disord 2019311ndash4
42 Tommasin S De Giglio L Ruggieri S et al Relation between functional connectivityand disability in multiple sclerosis a non-linear model J Neurol 20182652881ndash2892
43 Castellazzi G Debernard L Melzer TR et al Functional connectivity alterationsreveal complex mechanisms based on clinical and radiological status in mild relapsingremitting multiple sclerosis Front Neurol 20189690
44 Tewarie P Steenwijk MD Brookes MJ et al Explaining the heterogeneity of func-tional connectivity findings in multiple sclerosis an empirically informed modelingstudy Hum Brain Mapp 2018392541ndash2548
45 Rocca MA Savoldi F Valsasina P et al Cross-modal plasticity among sensory net-works in neuromyelitis optica spectrum disorders Mult Scler 201925968ndash979
46 Tewarie P Balk LJ Hillebrand A et al Structure‐function relationships in the visualsystem in multiple sclerosis an MEG and OCT study Ann Clin Transl Neurol 20174614ndash621
47 Liu Y Duan Y Huang J et al Multimodal quantitative MR imaging of the thalamus inmultiple sclerosis and neuromyelitis optica Radiology 2015277784ndash792
Appendix Authors
Name Location Contribution
YaelBacknerMSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Designed andconceptualized the studyanalyzed the data draftedthe figures and draftedthe manuscript forintellectual content
Ido Ben-ShalomBMedSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Analyzed the motornetwork data
JosephKuchlingMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
NadjaSiebert MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
MichaelScheel MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
KlemensRuprechtMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
AlexanderBrandt MD
CharitendashUniversitatsmedizinBerlin Germany Universityof California
Major role in dataacquisition
FriedemannPaul MD
CharitendashUniversitatsmedizinBerlin Germany
Supervised the study andrevised the manuscript forintellectual content
Netta LevinMD PhD
Hadassah-HebrewUniversity Medical CenterJerusalem Israel
Conceptualized anddesigned the studysupervised the studyand drafted themanuscript forintellectual content
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

References1 Schoonheim MM Filippi M Functional plasticity in MS Friend or foe Neurology
2012791418ndash14192 Costello F Vision disturbances in multiple sclerosis Semin Neurol 201636185ndash1953 Abel AMcClelland C LeeMS Critical review typical and atypical optic neuritis Surv
Ophthalmol 201964770ndash7794 Chen JJ Pittock SJ Flanagan EP Lennon VA Bhatti MT Optic neuritis in the era of
biomarkers Surv Ophthalmol 20206512ndash175 Lennon VA Wingerchuk DM Kryzer TJ et al A serum autoantibody marker of neu-
romyelitis optica distinction from multiple sclerosis Lancet 20043642106ndash21126 Raz N Chokron S Ben-Hur T Levin N Temporal reorganization to overcome
monocular demyelination Neurology 201381702ndash7097 Raz N Dotan S Chokron S Ben‐Hur T Levin N Demyelination affects temporal
aspects of perception an optic neuritis study Ann Neurol 201271531ndash5388 Raz N Dotan S Benoliel T Chokron S Ben-Hur T Levin N Sustained motion
perception deficit following optic neuritis Behavioral and cortical evidence Neurology2011762103ndash2111
9 Benoliel T Raz N Ben-Hur T Levin N Cortical functional modifications followingoptic neuritis Mult Scler 201723220ndash227
10 Backner Y Kuchling JMassarwa S et al Anatomical wiring and functional networkingchanges in the visual system following optic neuritis JAMANeurol 201875287ndash295
11 Finke C Zimmermann H Pache F et al Association of visual impairment in neu-romyelitis optica spectrum disorder with visual network reorganization JAMANeurol201875296ndash303
12 Rubinov M Sporns O Complex network measures of brain connectivity uses andinterpretations Neuroimage 2010521059ndash1069
13 Fleischer V Radetz A Ciolac D et al Graph theoretical framework of brain networksin multiple sclerosis a review of concepts Neuroscience 201940335ndash53
14 Polman CH Reingold SC Banwell B et al Diagnostic criteria for multiple sclerosis2010 revisions to the McDonald criteria Ann Neurol 201169292ndash302
15 Wingerchuk DM Banwell B Bennett JL et al International consensus diagnosticcriteria for neuromyelitis optica spectrum disorders Neurology 201585177ndash189
16 Kuchling J Backner Y Oertel FC et al Comparison of probabilistic tractography andtract-based spatial statistics for assessing optic radiation damage in patients withautoimmune inflammatory disorders of the central nervous system Neuroimage Clin201819538ndash550
17 Oertel FC Kuchling J Zimmermann H et al Microstructural visual system changes inAQP4-antibodyndashseropositive NMOSD Neurol Neuroimmunol Neuroinflamm 20174e334 doi 101212NXI0000000000000334
18 Association WM World Medical Association Declaration of Helsinki ethical prin-ciples for medical research involving human subjects JAMA 20133102191
19 Yushkevich PA Piven J Hazlett HC et al User-guided 3D active contour segmen-tation of anatomical structures significantly improved efficiency and reliabilityNeuroimage 2006311116ndash1128
20 Wang L Mruczek RE Arcaro MJ Kastner S Probabilistic maps of visual topographyin human cortex Cereb Cortex 2014253911ndash3931
21 Hindy NC Ng FY Turk-Browne NB Linking pattern completion in the hippo-campus to predictive coding in visual cortex Nat Neurosci 201619665
22 Cichy RM Khosla A Pantazis D Torralba A Oliva A Comparison of deep neuralnetworks to spatio-temporal cortical dynamics of human visual object recognitionreveals hierarchical correspondence Sci Rep 2016627755
23 Cichy RM Pantazis D Oliva A Similarity-based fusion of MEG and fMRI revealsspatio-temporal dynamics in human cortex during visual object recognition CerebCortex 2016263563ndash3579
24 Mackey WE Winawer J Curtis CE Visual field map clusters in human frontoparietalcortex Elife 20176e22974
25 Smith SM Jenkinson M Woolrich MW et al Advances in functional and structuralMR image analysis and implementation as FSL Neuroimage 200423S208ndashS219
26 Pool E-M Rehme AK Eickhoff SB Fink GR Grefkes C Functional resting-stateconnectivity of the humanmotor network differences between right-and left-handersNeuroimage 2015109298ndash306
27 Hardwick RM Rottschy C Miall RC Eickhoff SB A quantitative meta-analysis andreview of motor learning in the human brain Neuroimage 201367283ndash297
28 Rocca MA Meani A Riccitelli GC et al Abnormal adaptation over time of motornetwork recruitment in multiple sclerosis patients with fatigue Mult Scler J 2016221144ndash1153
29 Watts DJ Strogatz SH Collective dynamics of ldquosmall-worldrdquonetworks Nature 1998393440ndash442
30 Maslov S Sneppen K Specificity and stability in topology of protein networks Sci-ence 2002296910ndash913
31 Newman ME The structure and function of complex networks SIAM Rev 200345167ndash256
32 Latora V Marchiori M Efficient behavior of small-world networks Phys Rev Lett200187198701
33 Newman ME Modularity and community structure in networks Proc Natl Acad SciUSA 20061038577ndash8582
34 Zamvil SS Slavin AJ Does MOG Ig-posit ive AQP4-seronegative opti-cospinal inflammatory disease justify a diagnosis of NMO spectrumdisorder Neurol Neuroimmunol Neuroinflamm 20152e62 doi 101212NXI0000000000000062
35 Zekeridou A Lennon VA Aquaporin-4 autoimmunity Neurol NeuroimmunolNeuroinflamm 20152e110 doi 101212NXI0000000000000110
36 Toosy AT Hickman SJ Miszkiel KA et al Adaptive cortical plasticity in higher visualareas after acute optic neuritis Ann Neurol 200557622ndash633
37 Jenkins TM Toosy AT Ciccarelli O et al Neuroplasticity predicts outcome of opticneuritis independent of tissue damage Ann Neurol 20106799ndash113
38 Werring DJ Bullmore ET Toosy AT et al Recovery from optic neuritis is associatedwith a change in the distribution of cerebral response to visual stimulation a func-tional magnetic resonance imaging study J Neurol Neurosurg Psychiatry 200068441ndash449
39 Levin N Orlov T Dotan S Zohary E Normal and abnormal fMRI activation patternsin the visual cortex after recovery from optic neuritis Neuroimage 2006331161ndash1168
40 Cordani C Meani A Esposito F et al Imaging correlates of hand motor performancein multiple sclerosis a multiparametric structural and functional MRI study MultScler 20191352458518822145
41 Fling BW Martini DN Zeeboer E Hildebrand A Cameron M Neuroplasticity of thesensorimotor neural network associated with walking aid training in people withmultiple sclerosis Mult Scler Relat Disord 2019311ndash4
42 Tommasin S De Giglio L Ruggieri S et al Relation between functional connectivityand disability in multiple sclerosis a non-linear model J Neurol 20182652881ndash2892
43 Castellazzi G Debernard L Melzer TR et al Functional connectivity alterationsreveal complex mechanisms based on clinical and radiological status in mild relapsingremitting multiple sclerosis Front Neurol 20189690
44 Tewarie P Steenwijk MD Brookes MJ et al Explaining the heterogeneity of func-tional connectivity findings in multiple sclerosis an empirically informed modelingstudy Hum Brain Mapp 2018392541ndash2548
45 Rocca MA Savoldi F Valsasina P et al Cross-modal plasticity among sensory net-works in neuromyelitis optica spectrum disorders Mult Scler 201925968ndash979
46 Tewarie P Balk LJ Hillebrand A et al Structure‐function relationships in the visualsystem in multiple sclerosis an MEG and OCT study Ann Clin Transl Neurol 20174614ndash621
47 Liu Y Duan Y Huang J et al Multimodal quantitative MR imaging of the thalamus inmultiple sclerosis and neuromyelitis optica Radiology 2015277784ndash792
Appendix Authors
Name Location Contribution
YaelBacknerMSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Designed andconceptualized the studyanalyzed the data draftedthe figures and draftedthe manuscript forintellectual content
Ido Ben-ShalomBMedSc
Hadassah-HebrewUniversity MedicalCenter JerusalemIsrael
Analyzed the motornetwork data
JosephKuchlingMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
NadjaSiebert MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
MichaelScheel MD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition
KlemensRuprechtMD
CharitendashUniversitatsmedizinBerlin Germany
Major role in dataacquisition and revised themanuscript for intellectualcontent
AlexanderBrandt MD
CharitendashUniversitatsmedizinBerlin Germany Universityof California
Major role in dataacquisition
FriedemannPaul MD
CharitendashUniversitatsmedizinBerlin Germany
Supervised the study andrevised the manuscript forintellectual content
Netta LevinMD PhD
Hadassah-HebrewUniversity Medical CenterJerusalem Israel
Conceptualized anddesigned the studysupervised the studyand drafted themanuscript forintellectual content
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 NeurologyorgNN
48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

48 Eshaghi A Riyahi-Alam S Saeedi R et al Classification algorithms with multi-modaldata fusion could accurately distinguish neuromyelitis optica from multiple sclerosisNeuroimage Clin 20157306ndash314
49 Kim SH Kwak K Hyun JW et al Diffusion tensor imaging of normal‐appearing whitematter in patients with neuromyelitis optica spectrum disorder and multiple sclerosisEur J Neurol 201724966ndash973
50 Matthews L Kolind S Brazier A et al Imaging surrogates of disease activity in neuro-myelitis optica allow distinction from multiple sclerosis PLoS One 201510e0137715
51 Pache F Zimmermann H Finke C et al Brain parenchymal damage in neuromyelitisoptica spectrum disordermdasha multimodal MRI study Eur Radiol 2016264413ndash4422
52 Schoonheim MM Meijer KA Geurts JJ Network collapse and cognitive impairmentin multiple sclerosis Front Neurol 2015682
53 Gallo A Esposito F Sacco R et al Visual resting-state network in relapsing-remitting MS with and without previous optic neuritis Neurology 2012791458ndash1465
54 Rocca MA Valsasina P Leavitt VM et al Functional network connectivity abnor-malities in multiple sclerosis correlations with disability and cognitive impairmentMult Scler 201824459ndash471
55 Xia M Wang J He Y BrainNet Viewer a network visualization tool for human brainconnectomics PLoS One 20138e68910
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 7 Number 3 | May 2020 11
DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

DOI 101212NXI000000000000068720207 Neurol Neuroimmunol Neuroinflamm
Yael Backner Ido Ben-Shalom Joseph Kuchling et al Cortical topological network changes following optic neuritis
This information is current as of March 2 2020
ServicesUpdated Information amp
httpnnneurologyorgcontent73e687fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent73e687fullhtmlref-list-1
This article cites 54 articles 6 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionplasticityPlasticity
httpnnneurologyorgcgicollectionoptic_neuritisOptic neuritis see Neuro-ophthalmologyOptic Nerve
httpnnneurologyorgcgicollectionmultiple_sclerosisMultiple sclerosis
httpnnneurologyorgcgicollectionfmrifMRI
httpnnneurologyorgcgicollectiondevics_syndromeDevics syndromefollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2020 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm