Embed Size (px)
Citation preview

©2018 MFMER | slide-1
Corticosteroids in septic shock: Do we finally have an answer?Victoria Milano, PharmDPGY-1 Pharmacy Resident

©2018 MFMER | slide-2
Objectives• Review the pathophysiology of septic shock and
the mechanism of action of corticosteroids in septic shock
• Describe the recent clinical trials investigating the use of corticosteroids in septic shock
• Discuss the role of corticosteroids in septic shock based on current evidence

©2018 MFMER | slide-3
Sepsis and Septic Shock Definitions• Sepsis: life-threatening organ dysfunction
caused by a dysregulated host response to infection
• Septic shock: subset of sepsis with circulatory, cellular, and metabolic dysfunction associated with a higher risk of mortality
Singer M, et al. JAMA 2016; 315:801-810

©2018 MFMER | slide-4
Epidemiology• The mortality for patients with septic shock is
around 50%• Septic shock accounts for up to 10% of
admissions to intensive care units
Angus, D., et al. NEJM 2013; 369:840-851.Mayr, F., et al. Virulence. 2014;5:4-11.Rhodes A, et al. Crit Care Med 2017;45:486-552Walkey, A. et al. Crit Care Med. 41(6):1450-1457
020406080
100
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
Septic shockmortality (age-adjusted)Septic shockincidence

©2018 MFMER | slide-5
Anti-inflammatory
Septic Shock Pathophysiology
Gandhi N., The Hospitalist. 2012.
Proinflammatory
Hemodynamic alterations
Organ dysfunction
Coagulation disorders

©2018 MFMER | slide-6
Septic Shock PathophysiologyInfection
Plasma Plasma Plasma
Finfer, S. Crit Care Med. NEJM. 2013; 369:840-851
NO
Cytokines NOCytokines
Red blood cellOxygenTissueWhite blood cell

©2018 MFMER | slide-7
Septic Shock PathophysiologyInfection
Plasma Plasma Plasma
Finfer, S. Crit Care Med. NEJM. 2013; 369:840-851
Cortisol
Cortisol
Red blood cellOxygenTissueWhite blood cell

©2018 MFMER | slide-8
Critical Illness-Related Corticosteroid Insufficiency (CIRCI) in Septic Shock
Annane D, et al. Intensive Care Med 2017; 43:1781-1792
• Incidence of adrenal dysfunction may be as high as 50%
Dysregulation of HPA axis
Altered cortisol metabolism
Tissue resistance to
glucocorticoids

©2018 MFMER | slide-9
Identifying CIRCI
Give 250 mcg IV cosyntropin
Nonresponders:Change in cortisol level
≤9 mcg/dl
Responders: Change in cortisol level
>9 mcg/dl
Measure response at 30 and 60 minutes
Measure baseline cortisol

©2018 MFMER | slide-10
Corticosteroids in Septic Shock• Proinflammatory response
• Decreased production of cytokines• Decreased production of nitric oxide• Maintain endothelial integrity• Maintain vascular tone
• Subpopulation of patients with CIRCI

©2018 MFMER | slide-11
Poll-Everywhere Question• Which of the following is NOT a proposed
mechanism of corticosteroids in septic shock?• A) Counteract inflammatory cascade• B) Maintain vascular tone• C) Increase production of nitric oxide• D) Maintain endothelial integrity

©2018 MFMER | slide-12
History of Corticosteroids in Septic Shock
1950s-1980s
1950s-1980s
Dellinger et al. Crit Care Med. 2004; 32:858-873.Dellinger et al. Intensive Care Med. 2008; 34:17-60.Dellinger et al. Crit Care Med. 2013;41:580-637.Gandhi N., The Hospitalist. 2012.Rhodes et al. Intensive Care Med. 2017;43: 304-377.
19951950s-1980s 1995 2002 2004 2008 2018
2008/2012/2016
High-dose steroids
found to be beneficial
Two meta-analyses: high-dose steroids ineffective and
potentially harmful
Annane et al. trial
published
SSG: hydrocortisone
if requiring vasopressors
CORTICUS trial
published
SSG: hydrocortisone
if blood pressure
unresponsive to fluids and
vasopressors
ADRENAL and
APROCCHSS trials
published
SSG: surviving sepsis guidelines

©2018 MFMER | slide-13
Hydrocortisone and FludrocortisoneSteroid Hydrocortisone Fludrocortisone
Anti-Inflammatory Activity
1 10
Mineralocorticoid Activity
1 125
Duration (T1/2 hr) 8-12 8-12How supplied Injection and tablet Tablet
Adverse effects Hyperglycemia, neuropathy, myopathy,
delirium, immunosuppression
Edema, hypokalemia

©2018 MFMER | slide-14
Annane TrialAdult ICU patients requiring mechanical ventilation
within 8°of onset of septic shock19 ICUs in France
Hydrocortisone + Fludrocortisone50 mg IV every 6 hours
50 µg PO daily for 7 days
Hydrocortisone Placebo + Fludrocortisone Placebo
7 days
n=150 n=149
Annane, et al. JAMA 2002;288:862-871.
Nonrespondersn=114
Respondersn=36
Nonrespondersn=115
Respondersn=34

©2018 MFMER | slide-15
Annane OutcomesOutcome Steroids Placebo OR/HR P-value
All Patients28-Day mortality 82 (55%) 91 (61%) 0.65 (0.39-1.07) 0.091-Year mortality 102 (68%) 112 (75%) 0.62 (0.36-1.05) 0.08Vasopressor withdrawal 7 days 9 days 1.54 (1.10-2.16) 0.01
Nonresponders28-Day mortality 60 (53%) 73 (63%) 0.54 (0.31-0.97) 0.04
1-Year mortality 77 (68%) 88 (77%) 0.57 (0.31-1.04) 0.07
Vasopressor withdrawal 7 days 10 days 1.91 (1.29-2.84) 0.001Responders
28-Day mortality 22 (61%) 18 (53%) 0.97 (0.32-2.99) 0.961-Year mortality 25 (69%) 24 (71%) 0.70 (0.20-2.40) 0.57Vasopressor withdrawal 9 days 7 days 0.49
Annane, et al. JAMA 2002;288:862-871.

©2018 MFMER | slide-16
CORTICUSAdult ICU patients within 72° of onset of septic shock
52 ICUs
Hydrocortisone50 mg IV Q6H for 5d, then Q12H for
days 6-8, then Q24H for days 9-11, then stopped
Placebo
n=251 n=248
Sprung, et al. NEJM 2008;358:111-24.
Nonrespondersn=125
Respondersn=118
Nonrespondersn=108
Respondersn=136

©2018 MFMER | slide-17
CORTICUS Trial Outcomes
Nonresponders28-Day mortality 49 (39%) 39 (36%) 1.09 (0.77-1.52) 0.69
1-Year mortality 73 (59%) 60 (57%) 1.03 (0.83-1.29) 0.89
Time to shock reversal 3.9 days 6.0 days 0.06
Outcome Steroid Placebo RR P-valueAll Patients
28-Day mortality 86 (34%) 78 (32%) 1.09 (0.84-1.41) 0.511-Year mortality 137 (57%) 127 (54%) 1.05 (0.89-1.23) 0.58Time to shock reversal 3.3 days 5.8 days <0.001
Responders28-Day mortality 34 (29%) 39 (29%) 1.00 (0.68-1.49) 1.001-Year mortality 61 (55%) 67 (53%) 1.03 (0.82-1.31) 0.80Time to shock reversal 2.8 days 5.8 days <0.001
Sprung, et al. NEJM 2008;358:111-24.

©2018 MFMER | slide-18
Baseline CharacteristicsBaseline Characteristics Annane, et al. CORTICUS
Steroids Placebo Steroid PlaceboMedicalEmergencyElective
89 (59%)50 (37%)
6 (4%)
90 (60%)55 (37%)
4 (3%)
80 (32%)138 (55%)31 (12%)
93 (38%)132 (54%)
21 (9%)Mean arterial pressure 54±10 55±9
Systolic blood pressure 94±23 95±27
SAPS II score 60±19 57±19 50±18 49±17DopamineDobutamineEpinephrineNorepinephrine
136 (91%)53 (35%)41 (27%)46 (31%)
137 (92%)51 (34%)31 (21%)48 (32%)
27 (11%)
35 (14%)224 (89%)
29 (12%)
22 (9%)231 (93%)
Annane, et al. JAMA 2002;288:862-871. Sprung, et al. NEJM 2008;358:111-24.

©2018 MFMER | slide-19
ComparisonStudy Annane, et al. CORTICUS
Results Decreased 28-day mortality No 28-day mortality differenceSimilarities Quicker time to shock reversal Quicker time to shock reversal
Differences • SBP <90 mmHg despite fluid replacement and vasopressors
• Addition of fludrocortisone• Abrupt stop of steroids after 7d• Enrolled earlier• Met power• Higher SAPS II scores
• Hypotensive OR receiving vasopressors at time of enrollment
• Tapered over 11d• Enrolled later• Did not meet power• Lower SAPS II scores
Annane, et al. JAMA 2002;288:862-871. Sprung, et al. NEJM 2008;358:111-24.

©2018 MFMER | slide-20
Poll-Everywhere Question• What finding was consistent between the
Annane and CORTICUS trials?
• A) Quicker time to shock reversal
• B) Decreased 28-day mortality
• C) Decreased 1-year mortality
• D) Increased time to vasopressor withdrawal

©2018 MFMER | slide-21
Surviving Sepsis Guidelines• “We suggest against using IV hydrocortisone to
treat septic shock patients if adequate fluid resuscitation and vasopressor therapy are able to restore hemodynamic stability. If this is not achievable, we suggest IV hydrocortisone at a dose of 200 mg per day.” (weak recommendation, low quality of evidence)
Rhodes A, et al. Crit Care Med 2017; 45:486-552

©2018 MFMER | slide-22
APROCCHSS (Hydrocortisone plus Fludrocortisone for Adults with Septic Shock)
Annane D, et al. NEJM 2018; 378:809-818
Adult ICU patients within 24° of onset of septic shock
34 ICUs
Hydrocortisone + Fludrocortisone
Drotrecogin alfa (activated)
Hydrocortisone + Fludrocortisone + Drotrecogin alfa
(activated)Placebos
n=614 n=627
Primary outcome = 90-day all-cause mortality
Hydrocortisone + Fludrocortisone
50 mg IV every 6 hours50 µg PO daily for 7 days
Hydrocortisone Placebo + Fludrocortisone Placebo
7 days

©2018 MFMER | slide-23
Population• Indisputable or probable septic shock for less
than 24 hours• SOFA score of ≥3 for at least two organs for at
least 6 hours• Receipt of vasopressor therapy for at least 6
hours to maintain a SBP ≥90 mmHg or MAP ≥65 mmHg
• Dose of ≥0.25 mcg/kg/min or ≥1 mg/hr
Annane D, et al. NEJM 2018; 378:809-818

©2018 MFMER | slide-24
Baseline Characteristics Hydrocortisone +Fludrocortisone
Placebo
Male 65.5% 67.7%Age 66±14 66±15Admission from medical ward 82.4% 81%
SAPS II 56±19 56±19SOFA score 12±3 11±3Infection source
PulmonaryUrinary TractAbdomen
60.7% 16.6%12.1%
58%18.8%10.9%
EpinephrineDose (mcg/kg/min)
NorepinephrineDose (mcg/kg/min)
8.6%2.31±6.62
87%1.02±1.61
9.3%1.74±2.41
88%1.14±1.16
Annane D, et al. NEJM 2018; 378:809-818

©2018 MFMER | slide-25
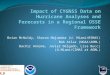
Mortality
4334 35
474939 41
53
0
10
20
30
40
50
60
90 days 28 days ICUdischarge
180 days
Hydrocortisone +Fludrocortisone
Placebo
P=0.04
P=0.04
Annane D, et al. NEJM 2018; 378:809-818
% o
f Pat
ient
s
P=0.03
P=0.06

©2018 MFMER | slide-26
Secondary OutcomesOutcome to 90-days Hydrocortisone +
Fludrocortisone(n=614)
Placebo
(n=627)
Pvalue
Vasopressor-free days 54±39 47±40 0.007
Ventilator-free days 45±39 40±39 0.04Organ-failure free days 51±39 45±40 0.006Discharge from ICU 382 (62.3%) 359 (57.4%) 0.08Discharge from hospital 334 (54.5%) 310 (49.6%) 0.09Mortality from any cause
NonrespondersResponders
101/198 (51%)61/184 (33%)
115/228 (50%)67/170 (39%)
0.910.22
Annane D, et al. NEJM 2018; 378:809-818

©2018 MFMER | slide-27
Adverse EventsAdverse Events
(≥1 event)Hydrocortisone + Fludrocortisone
Placebo Pvalue
By day 180Serious event 53.1% 58.0% 0.08
Serious bleeding event 20.7% 19.0% 0.46Episode of superinfection 31.1% 28.4% 0.30
By day 7Episode of blood glucose ≥150 89.1% 83.1% 0.002No. of days with ≥1 episode of blood glucose ≥150 mg/dl
4.3±2.5 3.4±2.5 <0.001
Annane D, et al. NEJM 2018; 378:809-818

©2018 MFMER | slide-28
ADRENAL(Adjunctive Glucocorticoid Therapy in Patients with Septic Shock)
Adult ICU patients requiring mechanical ventilation within 24° of
onset of septic shock69 ICUs (Australia, UK, New Zealand,
Saudi Arabia, Denmark)
HydrocortisoneContinuous IV infusion of 200 mg over 24 hours for 7 days or until
ICU discharge/death
PlaceboContinuous IV infusion over 24
hours for 7 days or until ICU discharge/death
Primary outcome = 90-day all-cause mortality
Venkatesh B, et al. NEJM 2018; 378:797-808
n=1853 n=1860

©2018 MFMER | slide-29
Population• Documented or strong clinical suspicion of
infection• Fulfilled two or more SIRS criteria• Treated with vasopressors or inotropic agents
for ≥4 hours up to and at the time of randomization
Venkatesh B, et al. NEJM 2018; 378:797-808
SIRS=systemic inflammatory response syndrome

©2018 MFMER | slide-30
Baseline CharacteristicsHydrocortisone Placebo
Male 60.4% 61.3%Age 62.3±14.9 62.7±15.2Admission type
MedicalSurgical
68.8%31.2%
68.2%31.8%
APACHE II Score 24 (19-29) 23 (18-29)Mean arterial pressure-mmHg 72.5±8.2 72.2±8.3Infection source
PulmonaryAbdomen
33.8% 25.9%
36.5%25.2%
NorepinephrineVasopressinEpinephrine
98.4%15.1%7.2%
97.9%17.3%6.1%
Venkatesh B, et al. NEJM 2018; 378:797-808

©2018 MFMER | slide-31
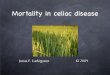
Mortality
2822
2924
0
5
10
15
20
25
30
35
90 days 28 days
HydrocortisonePlacebo
P=0.50
P=0.13
% o
f Pat
ient
s
Venkatesh B, et al. NEJM 2018; 378:797-808

©2018 MFMER | slide-32
Subgroup AnalysisSubgroup Hydrocortisone Placebo OR P value
Catecholamine Dose ≤15 mcg/min>15 mcg/min
224/968 (23%)281/849 (33%)
228/995 (23%)291/805 (36%)
1.02 (0.82-1.26)0.86 (0.70-1.05)
0.25
APACHE II Score≥25<25
326/840 (39%)184/990 (19%)
297/785 (38%)229/1039 (22%)
1.01 (0.83-1.24)0.82 (0.66-1.02)
0.17
Time from shockonset to randomization<6 hr6 to <12 hr12 to <18 hr≥18 hr
110/352 (31%)127/511 (25%)119/437 (27%)154/525 (29%)
96/344 (28%)153/486 (32%)106/423 (25%)167/566 (30%)
1.16 (0.83-1.61)0.71 (0.54-0.94)1.13 (0.83-1.54)0.99 (0.76-1.29)
0.08
Venkatesh B, et al. NEJM 2018; 378:797-808

©2018 MFMER | slide-33
Secondary OutcomesOutcome Hydrocortisone
(n=1853)Placebo(n=1860)
P value
Blood transfusion 683 (37%) 773 (41.7%) 0.004Recurrence of mechanical ventilation
180 (9.8%) 154 (8.3%) 0.11
Median time in daysResolution of shock 3 (2-5) 4 (2-9) <0.001Discharge from the ICU 10 (5-30) 12 (6-42) <0.001Cessation from initial mechanical ventilation
6 (3-18) 7 (3-24) <0.001
Mean number of daysAlive and out of the ICU 58.2±34.8 56.0±35.4 0.047Alive and free from RRT 42.6±39.1 40.4±38.5 0.29
Venkatesh B, et al. NEJM 2018; 378:797-808

©2018 MFMER | slide-34
Adverse EventsAdverse Events Hydrocortisone
(N=1835)Placebo(N=1829)
Hyperglycemia 6 3Hypernatremia 3 0Myopathy 3 0Total adverse events 27 6
Venkatesh B, et al. NEJM 2018; 378:797-808

©2018 MFMER | slide-35
ComparisonAPROCCHSS ADRENAL
Results Decreased 90-day mortality No 90-day mortality differenceSimilarities Quicker time to shock reversal Quicker time to shock reversalDifferences • Receiving vasopressors ≥6h
• Hydrocortisone boluses + fludrocortisone
• Majority of medical admissions• 28% renal-replacement therapy• Pulmonary, UTI, abdominal
source most common• Patients sicker
• Receiving vasopressors ≥4h• Continuous IV hydrocortisone• Majority of medical admissions,
many surgical admissions• 13% renal-replacement therapy• Pulmonary, abdominal, UTI
source most common• Patients not as sick
Suffredini, A. NEJM 2018; 378:860-861.Annane D, et al. NEJM 2018; 378:809-818Venkatesh B, et al. NEJM 2018; 378:797-808

©2018 MFMER | slide-36
Comparison of all Four Trials
Study # of Pts
Mortality Treatment Start
(hours)
Mortality Benefit
Shock Reversal
(days)Annane, et al. 299 58% ≤8 6% 2CORTICUS 499 33% ≤72 None 3
APROCCHSS 1241 46% ≤24 6.1% 2ADRENAL 3800 28% ≤24 None 1
Annane, et al. JAMA 2002;288:862-871. Sprung, et al. NEJM 2008;358:111-24.Annane D, et al. NEJM 2018; 378:809-818Venkatesh B, et al. NEJM 2018; 378:797-808

©2018 MFMER | slide-37
Summary• The data still shows conflicting evidence if
corticosteroids have a mortality benefit• Corticosteroids improve time to shock reversal• Hyperglycemia is the most significant adverse
event consistently shown in trials

©2018 MFMER | slide-38
Case• LM is a 68-year-old male with new onset septic
shock from a community acquired pneumonia. He is requiring high doses of vasopressors despite adequate fluid resuscitation and is still not maintaining goal MAP. He has respiratory, liver, and renal failure. Would you use hydrocortisone in this patient?

©2018 MFMER | slide-39
Poll-Everywhere Question• Would you use hydrocortisone in this patient?
• A) Yes• B) No

©2018 MFMER | slide-40
Recommendations• Patients with adequate fluid resuscitation
requiring high dose vasopressors with higher SOFA/SAPS II scores (SOFA >10, SAPS II >55) regardless of MAP within 24h of septic shock
• Would recommend hydrocortisone 200 mg IV for 7 days
• Septic shock patients beyond 24 hours, not requiring vasopressors, with lower scores
• Would not recommend hydrocortisone

©2018 MFMER | slide-41
Remaining Questions• Taper vs. abruptly stop corticosteroids• Duration of corticosteroids • Bolus vs. continuous infusion• When to start corticosteroids• Should fludrocortisone be added to
hydrocortisone

©2018 MFMER | slide-42
• Questions?