Embed Size (px)
Citation preview

to poor neurological outcome andmortality.1 Signs of secondary neu-rological damage include brainswell ing (Figure 1), somnolence,abnormal motor function, andpupillary changes. Nevertheless, theonset and extent of secondary injuryare still difficult to detect. Intensiveneuromonitoring is therefore criticalin improving neurological prognosisin patients with TBI.
Changes in intracranial pressure(ICP), cerebral perfusion pressure(CPP), brain tissue partial pressure
Cover Article
This article has been designated for CE credit. A closed-book, multiple-choice examination fol-lows this article, which tests your knowledge ofthe following objectives:
1. Describe the interrelationships among intracranial pressure, cerebral perfusion pressure, brain tissue partial pressure of oxygen, blood pressure, and brain temperature
2. Identify aberrations in cerebral metabolites indicative of cerebral ischemia
3. Discuss common neuromonitoring parametersand the threshold values and appropriate nursing interventions associated with each
Sandy Cecil, RN , BAPatrick M . ChenSarah E. Callaway, RN , BSNSusan M . Rowland, RN , BSNDavid E. Adler, M DJefferson W. Chen, M D , PhD
CEContinuing Education
©2010 American Association of Critical-Care Nurses doi: 10.4037/ccn2010226
Traumatic brain injury(TBI) accounts for 1.4million reported injuriesand 52000 deaths eachyear in the United States.
TBI is the leading cause of death anddisability in patients from ages 1 to44 years.1 The main causes of TBIare motor vehicle crashes, falls, andassaults. Secondary neurologicaldamage, the damage that occurs inthe ensuing hours and days after theprimary injury, contributes markedly
www.ccnonline.org CriticalCareNurse Vol 31, No. 2, APRIL 2011 25
Traumatic brain injury accounts for nearly 1.4 million injuries and 52 000 deathsannually in the United States. Intensive bedside neuromonitoring is critical in pre-venting secondary ischemic and hypoxic injury common to patients with traumaticbrain injury in the days following trauma. Advancements in multimodal neuromon-itoring have allowed the evaluation of changes in markers of brain metabolism (eg,glucose, lactate, pyruvate, and glycerol) and other physiological parameters such asintracranial pressure, cerebral perfusion pressure, cerebral blood flow, partial pressureof oxygen in brain tissue, blood pressure, and brain temperature. This article high-lights the use of multimodal monitoring in the intensive care unit at a level I traumacenter in the Pacific Northwest. The trends in and significance of metabolic, physio-logical, and hemodynamic factors in traumatic brain injury are reviewed, the tech-nical aspects of the specific equipment used to monitor these parameters aredescribed, and how multimodal monitoring may guide therapy is demonstrated. Asa clinical practice, multimodal neuromonitoring shows great promise in improvingbedside therapy in patients with traumatic brain injury, ultimately leading toimproved neurological outcomes. (Critical Care Nurse. 2011;31:25-37)
Traumatic Brain InjuryAdvanced Multimodal Neuromonitoring From Theory to Clinical Practice
Figure 1 Traumatic brain injury canresult in frontal intraparenchymalhematomas with contusion edema andtraumatic subarachnoid hemorrhage.
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

of oxygen (PBTO2), blood pressure,brain temperature, and, recently,cerebral blood flow (CBF) are moni-tored in the intensive care unit (ICU).2
Cerebral microdialysis is a techniqueincreasingly used as a bedside methodfor measuring glucose, lactate, pyru-vate, and glycerol levels in the brainof patients with severe head trauma.3-5
Cerebral ischemia may be detectedon the basis of aberrations in cerebralmetabolites. Similarly, minimizingsecondary ischemic injury common inTBI may be possible with the manip-ulation of ICP, CPP, CBF, blood pres-sure, brain temperature, and PBTO2in brain parenchyma after acute braininjury.2,4-7
In this article, we describe the suc-cessful use of multimodal neuromon-itoring to guide therapy in our ICU.First, we provide an overview of thesignificance of changes in glucose,lactate, pyruvate, and glycerol levelsin traumatically injured brain andreview the importance and interrela-tionships between ICP, CPP, CBF,PBTO2, blood pressure, and braintemperature. We also describe thebackground and important clinical
aspects of specific current equipmentused in our ICU to measure all thechanges. Finally, we indicate thresh-old values that may change the treat-ment of patients with severe braininjury. Our emphasis is on cerebralmicrodialysis and CBF monitoring,
which are relatively new monitoringtechniques.
Metabolic and Cellular EnergyMetabolic Trends of Microdialysis Markers
Understanding the bioenergeticsof hypoxic and/or ischemic brain isimportant.4-7 As brain tissue becomeshypoxic, oxygen no longer functionsas the final electron carrier in theelectron transport chain. Nicoti-namide adenine dinucleotide hydro-gen therefore cannot deprotonate,and cells must rely on anaerobic respiration. Generation of adeno-sine triphosphate (ATP) is compro-mised; only 2 molecules of ATP are produced in contrast to the aer-obically generated 32 molecules(Figure 2). During ischemia, a lackof oxygen and glucose results inanaerobic respiration. In ischemic
Sandy Cecil is the supervisor/educator and charge nurse in a 10-bed neurological trauma,neurosurgical, surgical intensive care unit at Legacy Emanuel Medical Center in Portland,Oregon. Patrick M. Chen is an undergraduate biology student at Dartmouth College, Hanover, New Hampshire. Sarah E. Callaway is a charge nurse in the neurological trauma, neurosurgical, surgicalintensive care unit at Legacy Emanuel Medical Center. Susan M. Rowland is a relief charge nurse/preceptor coordinator at Legacy Emanuel Medical Center. David E. Adler is a neurosurgeon at Legacy Emanuel Medical Center. Jefferson W. Chen is the neurosurgical medical director at Legacy Emanuel Medical Center.
Corresponding author: Sandy Cecil, RN, 2801 N Gantenbein Ave, Portland, OR 97227 (e-mail: [email protected] [email protected]).
To purchase electronic or print reprints, contact The InnoVision Group, 101 Columbia, Aliso Viejo, CA 92656.Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected].
A u t h ors
26 CriticalCareNurse Vol 31, No. 2, APRIL 2011 www.ccnonline.org
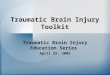
Figure 2 Flow chart of cellular metabolism. Under normal conditions, glucose isturned to pyruvate and nicotinamide adenine dinucleotide hydrogen (NADH+) in aer-obic glycolysis. These products are used in the Krebs cycle and electron transportchain to generate 32 molecules of ATP (left side). In ischemia and hypoxia, glucoseand oxygen levels are reduced. Lack of oxygen disables the electron transport chain,causing cells to begin anaerobic respiration (right side), in which pyruvate is con-verted to lactate. Only 2 molecules of ATP are produced, resulting in brain tissuedeath and the release of glycerol.
Normal conditions
Brain tissuedeath
Glucose
Pyruvate (2)NADH+ Lactate
Krebs cycle
Electron transport chain(oxygen as final carrier in chain)
Decreased blood flow=Decreased oxygen= Switch to anaerobic respiration
Ischemic and hypoxic conditions
32 ATP
2 ATP
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

and hypoxic states, glucose is con-verted primarily to lactate, resultingin decreased levels of pyruvate.4,8-10
These alterations in the Krebs cyclemake lactate and pyruvate excellentindicators of energy failure in thebrain. Because the levels of thesecompounds naturally fluctuate,detecting the changes in lactate levelsin relation to pyruvate levels, a rela-tionship known as the lactate topyruvate ratio (LPR), is desirable.Extensive research has shown thatthe LPR is a good indicator ofischemic and hypoxic conditions aswell as possible mitochondrial dam-age.5,7,8,11,12 Under anaerobic condi-tions, the PBTO2 and glucose leveldecrease while the LPR increases.8,9
Elevated glycerol levels also indi-cate failure in cellular bioenergetics.Glycerol levels increase when cellsdo not have sufficient energy tomaintain homeostasis.11,12 Becauseof a lack of ATP, calcium ion chan-nels can no longer be maintained,and cellular influx of calcium occurs.The influx activates phospholipases,causing the phospholipids withincellular membranes to be enzymati-cally cleaved, yielding abnormallyhigh glycerol levels.7
Microdialysis TechnologyMicrodialysis enables measure-
ment of the metabolic markers (glucose, pyruvate, lactate, and glyc-erol). The technique was firstdescribed in 1966, when Bito andcolleagues successfully placed dex-tran membrane-lined sacks in thecerebral hemispheres of dogs to col-lect amino acids. This technique wasrefined to its present-day form in the1970s by Tossman and Ungerstedt.7,11
Microdialysis involves a catheterwith a 10-mm semipermeable distal-
end membrane that is placed intothe brain parenchyma. The catheteris pumped with fluid isotonic to tis-sue interstitium. In short, the catheteracts as an artificial blood capillary12
(Figure 3). Through diffusion, mole-cules related to the production ofATP (glucose, pyruvate, lactate,glycerol) are collected from theinterstitial fluid and are analyzedhourly.3,7,13 The metabolites recoveredrepresent 70% of the true interstitialfluid concentrations.3
MicrodialysisWe use 2 devices to perform
cerebral microdialysis. The CMA600 (CMA Microdialysis, Solna,Sweden) is used for bedside analysisof metabolic indicators. This devicewas approved for use in the UnitedStates by the Food and Drug Admin-istration in 2005. A second type ofanalyzer is the ISCUSflex (CMAMicrodialysis), which was approved
by the Food and Drug Administra-tion in July 2009. At the time thisarticle was written, our facility wasthe only one involved in beta testsof the ISCUS in the United States.We have clinical experience withmore than 100 patients with bothanalyzers. The CMA 600 can beused to monitor up to 3 patientsand 4 reagents. In contrast, theISCUSflex can be used to monitorup to 8 patients simultaneously,with a total of 16 catheters and 5reagents. Calibration of both ana-lyzers is performed automaticallyevery 6 hours, and controls are runevery 24 hours.
The microdialysis catheter isplaced through a bolt or burr hole oris implanted during an open cran-iotomy. The catheter is then attachedto a microdialysis syringe filled withsterile perfusion fluid (artificialCSF) and placed in the CMA 106pump, which is precalibrated to
www.ccnonline.org CriticalCareNurse Vol 31, No. 2, APRIL 2011 27
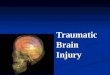
Figure 3 Microdialysis technique. The microdialysis catheter at the distal end actsas an artificial capillary. Extracellular substances diffuse from interstitial tissue toperfusion fluid inside the catheter membrane. Courtesy of CMA Microdialysis, Solna, Sweden.
Cell
Extracellular fluid
Bloo
d ca
pilla
ry
Mic
rodi
alys
is c
athe
ter
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

pump the perfusion fluid at a rate of0.3 µL/min. In TBI patients, thecatheter is ideally placed in the peri-contusional penumbra of the injury,and its position is verified by usingcomputed tomography.5 In addition,we place a second microdialysiscatheter in an area of undamagedtissue for comparison or reference.Each metabolite marker has a separatereagent for detection. The contentsof the buffer solution are mixed inthe reagent bottle.
We run samples every hour. Sam-ples can be run every 20 minutes, asindicated by changes in a patient’scondition. Increased attention to apatient’s catheters will decrease therisk of dislodgement of the micro-dialysis catheters. Of note, the Clini-cal Laboratory Improvement Actrequires control testing for thispoint-of-care device with low, normal,and abnormally high concentrationsas controls. Known concentrationsalong the linear range of each analyteare run every 24 hours during moni-toring and after a reagent change.8
Therapeutic Interventions forAbnormal Levels of Brain Metabolites
Normal brain glucose levels are30.6 (SD, 16.2) mg/dL (to convert tomillimoles per liter, multiply by0.0555).9,14 On the basis of the lowestlevel within the standard deviation(Table 1), the ischemic threshold forbrain glucose is 14.4 mg/dL. In ourpatients, strict adherence to tightglycemic control (blood glucose lev-els 80-110 mg/dL) often leads to dan-gerously low brain glucose levels thatcan be detected only with cerebralmicrodialysis.15 To avoid cerebralhypoglycemia, we adjusted our bloodglucose ranges to 110 to 180 mg/dL,
resulting in brain glucose levels of2.5 mg/dL or higher. This experi-ence suggests that preventing sys-temic hypoglycemia most likely iskey to preventing metabolic crisisand, ultimately, secondary braininjury.15 Therefore, earlier thanusual nutritional support as ameans of maintaining higher brainglucose levels may be important.
The normal LPR is 23 (SD, 4).9
Normal glycerol levels are 184 to460 mg/dL (to convert to mil-limoles per liter, multiply by0.1086). An LPR near a thresholdvalue of 30, in conjunction with alow glucose level, requires interven-tion to prevent cellular energy fail-ure. Similarly, glycerol levels near921 mg/dL indicate cellular energyfailure9,14 (Table 1). Baseline LPR andglycerol levels are recorded andwatched for changes and trendstoward threshold ischemic values.Routine interventions to lower theLPR, by preventing anaerobic respi-ration that leads to abnormally ele-vated glycerol levels, includeincreasing glucose levels by adjust-ing insulin infusions for a permis-sive blood glucose level of 110 to180 mg/dL, elevating and adjustingthe patient’s head and position, andaugmenting CPP with vasopressors(Figure 4).
Intracranial MonitoringPhysiology of ICP and CPP
Elevated ICP is a common neu-rosurgical concern after traumabecause it impedes CBF and isassociated with ischemia andhypoxia.16 Common causes of ele-vated ICP include development ofmass lesions such as subduralhematoma, epidural hematoma,and intracerebral contusions.Additionally, cerebral edema andcommunicating and noncommuni-cating hydrocephalus are treatablecauses of increased ICP.17,18 ICP isthe target parameter for manytreatment algorithms. ICP is usedto calculate CPP, the pressure gra-dient for blood perfusion in thebrain measured in millimeters ofmercury and used to calculate CBF(CPP/cerebral vascular resistance).2,18
High ICP, a source of energyfailure, is associated with adecreased CPP and lower CBF, theunderlying cause of cellular energyfailure.19 Increased ICP and lowCPP often result in marked neuro-logical morbidity and poor out-come. The threshold values of ICP,CPP, and CBF, which vary markedlyaccording to body position, age,and body surface area, are widelydebated.16,18,20 Finally, ICP monitor-ing is accepted in the Brain Trauma
28 CriticalCareNurse Vol 31, No. 2, APRIL 2011 www.ccnonline.org
Table 1 Normal and threshold values of metabolic parameters important inneuromonitoring of patients with traumatic brain injury
Parameter
Glucose, mean (SD), mg/dL
Pyruvate, mean (SD), mg/dL
Lactate mean (SD), mg/dL
Lactate to pyruvate ratio
Glycerol, mg/dL
Threshold value
14.4
0.27 (fatal)
80.2 (fatal)
30
21
Normal levels
30.6 (16.2)
1.46 (0.33)
26.1 (8.1)
23 (4)
184-460
SI conversion factors: To convert glucose to mmol/L, multiply by 0.0555; pyruvate to µmol/L, multiply by113.56; lactate to mmol/L, multiply by 0.111; glycerol to mmol/L, multiply by 0.1086.
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

Foundation guidelines1 as the goldstandard for TBI monitoring toguide intervention.
Cerebral Pressure and PerfusionMonitoring Systems
Unlike microdialysis monitor-ing, intracerebral technology andmonitors vary in concept anddesign. Bedside physiologicalmonitors are used to measure ICPand calculate CPP. Pressure trans-duction varies between monitorsand involves different mechanisms,including catheter-tip strain gauge,external strain, and fiber optics.1
Pupillometers provide an alterna-tive method of evaluating ICP lev-els by giving quantitative evaluationof pupillary function.2,21
Camino ICP Monitor. TheCamino ICP monitor (IntegraNeuroSciences, Plainsboro, NJ)consists of a patented fiber-optictransducer-tipped pressure-temperature catheter that is placedvia a burr hole and can be used tomeasure ICP in the subdural,parenchymal, and ventricularspaces. The device measures ICPand brain temperature and dis-plays ICP waveforms and the cal-
can be used to measure ICP througha tunneled catheter, a bolted catheter,or an intraventricular approach.The ICP Express allows both contin-uous readings and CSF drainage viaventriculostomy. The ICP Expresscan be implanted in the subduralspace or the intraparenchymalspace and then secured to the skull.
The Codman microsensor tip is placed in sterile liquid to zero the sensor before implantation. Themicrosensor’s zero offset numberwill be displayed on the ICP Expressscreen. This offset number is specificto the transducer that was zeroed.Recording the zero offset referencenumber on the patient’s chart or onthe microsensor is important incase of a disconnection. This deviceis not compatible with magneticresonance imaging.
Ventriculostomy. A ventricu-lostomy catheter provides a methodfor monitoring ICP while simultane-ously reducing ICP through thera-peutic CSF drainage. Using aventriculostomy is particularly help-ful in treating obstructive hydro-cephalus.23 If an excessive amount ofCSF accumulates in the ventriclesafter TBI, the fluid can be externally
culated CPP. The Camino catheterhas a miniaturized transducer at thedistal end. The device has no fluid-filled system, thus eliminating theproblems associated with an exter-nal transducer, pressure dome, andpressure tubing. The monitor pro-vides continuous information anddoes not require recalibration.22
The fiber-optic catheter, with itsintegrated transducer, is insertedthrough a burr hole space in thesubdural, parenchymal, and ven-tricular spaces. The transducermust be zeroed before insertionand disconnected from the pream-plification connector when apatient is moved. A red mark willindicate correct placement in thebrain parenchyma. The subduraland ventricular catheters do nothave a red line, rather they havegraduated lines to calculate thedepth of the catheter.22 Thecatheter is visible on computedtomography and is not compatiblewith magnetic resonance imaging.
CODMAN ICP Express. TheCODMAN ICP Express (Codman &Shurtleff Inc, Raynham, Massachu-setts) is also used for measuring ICPand calculating CPP. The ICP Express
www.ccnonline.org CriticalCareNurse Vol 31, No. 2, APRIL 2011 29
Figure 4 Flow chart of metabolic related therapy integrates the possible responses to low blood glucose, elevated lactate to pyruvate ratio, and glucose (left). Normothermic treatment is used to reduce brain metabolic demand (right).
Low bloodglucose
Enteral feedingInsulin Insulin infusion
Acetaminophenor ibuprofen
Elevated braintemperature
Adjust headposition Vasopressors
Return aerobicrespiration and
glucose
Elevated lactate to pyruvate
ratio and/or high glycerol
Adjust capillaryblood glucose
Cooling blanketsor ice packs
Invasive coolingIcycath
CoolGuard
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

drained through a ventricularcatheter secured to the head.
ICP monitoring via a ventriculardrain is accomplished by using atransducer system.2 Ventricu-lostomies are leveled at the tragusand open to drainage at the pre-scribed centimeters of water theneurosurgeon orders. Documentingthe amount of CSF drained hourly isimportant. Troubleshooting meas-ures if drainage stops include lower-ing the ventriculostomy, flushingaway from the head in case of clotin the tubing, and flushing 0.1 mLof preservative-free normal salinetoward the head. The stopcock tothe transducer must be turned inthe direction of flow for continuousICP monitoring or for drainage ofCSF. During repositioning of thepatient, the stopcock is turned to theoff position to prevent overdrainageof CSF.
Pupillometry. The pupil checkwith a flashlight has always been astandard subjective measurementof pupil reactivity and status of thenervous system and brain. Nowchanges in constriction and dilata-tion of pupils to light can be quanti-tatively assessed. The NeuropticsForeSite pupillometer (Medtronic,Minneapolis, Minnesota) is a non-invasive, battery-operated, hand-held device that uses light stimulusand rapid live photography to meas-ure maximum and minimum aper-ture and constriction velocity ofpupils.2 Although the pupillometeris a relatively new device, preliminarytesting suggests that constrictionvelocities less than 0.8 mm/s indicateincreased brain volume and veloci-ties less than 0.6 mm/s suggest ele-vated and problematic ICP. Similarly,pupil reactivity less than 10% after
light stimulus suggests elevated ICPand should be considered in con-junction with the results of othermonitoring systems for ICP.21 Wehave found that using the pupil-lometer is an easy and quickadjunct to assessing neurologicalchanges of patients with TBI.
In order to use the pupillometer,the head rest of the device must befitted correctly. The head rest is dis-posable and should be changed foreach patient. Awake patients areinstructed to look straight aheadand focus their untested eye on adistant object. Manually and gentlyholding the patient’s eye open maybe necessary. The green pupilboundary circle must be centeredon the pupil for measurement. Exactmeasurement of each pupil andconstriction is then obtained. Thismeasurement is more reliable andconsistent than the subjective assess-ment of a health care provider.21
ICP monitoring and cathetershave become the standard of carefor measuring ICP.5 Baseline normalICP levels range from 0 to 10 mmHg; treatment threshold values areusually 20 to 25 mm Hg.1,16,18,24,25 IdealCPP is approximately 60 mm Hg;the treatment threshold value isabout 50 mm Hg1,24,25 (Table 2).Current TBI guidelines includefirst- and second-tier interventions
to reduce ICP if it increases beyondthe threshold value. First-tier inter-ventions may involve draining CSF,increasing PaO2 and PaCO2 levels,administering diuretics, or elevatingthe head of the bed to an optimal30º angle. Second-tier interventionsinvolve administering medications,such as mannitol, furosemide (toreduce intravascular volume),hypertonic saline, or barbiturates,to reduce ICP. Patients who do notrespond to these therapeutic inter-ventions require computed tomog-raphy and, possibly, craniotomy orcraniectomy.1,24,25 Finally, a brief trialof hyperventilation may be used asa temporary measure to controlhigh ICP1 (Figure 5).
Cerebral Blood FlowCBF is a complex and essential
variable in determining whether thebrain experiences posttraumaticsecondary damage. Acute braintrauma causes a decrease in CBFwhile increasing the demand forblood and oxygen.2,26 Many variablesaffect blood flow in the brain, includ-ing metabolic regulation, PaCO2,PaO2, and autoregulation.18,26
Increases in CPP can increase CBFduring ischemic conditions. Autoreg-ulation of this change in CPP andCBF includes vasodilatation andvasoconstriction (Figure 6). The
30 CriticalCareNurse Vol 31, No. 2, APRIL 2011 www.ccnonline.org
Table 2 Normal and threshold values of hemodynamic parameters importantin neuromonitoring of patients with traumatic brain injury
Parameter
Intracranial pressure, mm Hg
Cerebral perfusion pressure, mm Hg
Mean arterial pressure, mm Hg
Cerebral blood flow, mL/100 g per minute
Threshold value
20-25
50
15
Normal levels
0-10
>60
Augmented to keepcerebral perfusion
pressure >60 mm Hg
18-35
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

vasodilatation cascade occurs whenCPP decreases, cyclically increasingvasodilatation. In response, ICPand cerebral vascular resistanceincrease, aggravating brain edema.In contrast, the vasoconstrictioncascade occurs when CPP increases,causing constriction of vessels toreduce cerebral blood volume andCBF. If autoregulation is ineffective,CBF is determined by blood pres-sure. Hypotension may then causeischemia. Similarly, hypertensionmay cause hyperemia.26-28
CBF Monitoring SystemsDirect measurement of CBF is
relatively new in neurointensive care.Accordingly, real-time perfusion
per 100 grams per minute) with anattached probe. The probe is mini-mally invasive and includes aheated distal thermister and a prox-imal thermister to track baselinetemperature. The monitor andprobe measure tissue perfusion bymeasuring the ability of the tissue tocarry heat through thermal conduc-tion, represented as the K value bythermal convection from bloodflow. The monitoring system calcu-lates tissue perfusion by calculatingthermal convection and total dissi-pated initial power. The probe canbe viewed on computed tomogra-phy and radiography. It is not com-patible with magnetic resonanceimaging.30
measuring devices and technologyare still being developed and refined.Monitoring CBF could play animportant role in neurological care,because the brain depends on con-tinuous blood flow to supply glucoseand oxygen. Regional CBF is consid-ered an important upstream moni-toring parameter indicative oftissue viability.29
Hemedex System. The HemedexCBF monitoring system (Codman &Shurtleff, Inc) is approved by theFood and Drug Administration forthe bedside monitoring of tissueblood flow and circulation. Withthis device, CBF is measured by cal-culating real-time tissue perfusion at the capillary level (in milliliters
www.ccnonline.org CriticalCareNurse Vol 31, No. 2, APRIL 2011 31
Figure 5 Flow chart of hemodynamic related therapy integrates the possible responses to elevated ICP, low CPP, and low or highbrain oxygen level.
Abbreviations: CPP, cerebral perfusion pressure; CSF, cerebral spinal fluid; CT, computed tomography; ICP, intracranial pressure; PBTO2, brain tissue partial pressure ofoxygen.
Low cerebral blood flow
Brainoxygen(PBTO2)
Adjust blood pressure
MaximizeCPP
Low blood pressure: phenylephrine, norepinephrine, vasopressins,
dopamineCT scan
Mannitolhypotonic
saline
Barbiturates vs craniotomy/craniectomy30° anglehead
Diuretics
+ PaO2+ PCO2
Drain CSF
High blood pressure: metoprolol, nicardipine, enalapril,
nitroglycerin, sodium nitroprusside
Reduce ICP tomaximize CPPand cerebral blood flow
ElevatedICP, low
CPP
Medication,sedation, anti-
inflammatorycoolingdevices
Reduce ICP
Increase CPP
Treathypovolemia,hypotension,
hypoxia
Hyperventi-lation
Increasebody
tempera-ture
anesthesia,sedatives
Increasedemand
Reducedelivery
High PBTO2“luxury perfusion”
Low PBTO2
Reduceincreaseddemand
IncreaseddeliveryTier 2Tier 1
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

The probe is inserted through aburr hole or is placed 2 to 2.5 cmbelow the dura into brain whitematter (Figure 7). The probe issecured via fixation disc or a single-or double-lumen bolt. In patientswith TBI, the probe is placed eitherin noninjured brain white matteripsilateral or contralateral to theinjury or in the ischemic penumbrasurrounding injured brain tissue.For comparison, a probe can beplaced in uninjured brain tissue.Once the probe is placed by a neu-rosurgeon, a nurse attaches theprobe to an umbilical cord andmonitor to begin calibration. Theproper K value for white brain mat-ter is 4.9 to 5.8 mW/cm per degreeCelsius. The probe can be retractedor advanced accordingly if the Kvalue is not within range.
The monitor provides CBFparameters within a temperaturerange of 25ºC to 39.5ºC. Cooling thepatient should be considered if braintemperature is greater than 38.5ºC.
The monitor does not run onbattery power, so the probe must be
disconnected from the umbilical cordbefore the patient is transported toother departments for proceduresor tests. The probe should be securedto the patient’s head dressing to pre-vent dislodging the probe. If theprobe is used in conjunction with amicrodialysis catheter, the 2 cathetersmust be separated by 2.0 mm foraccurate results.
TranscranialDoppler Sonog-raphy. Althoughwe do not rou-tinely use tran-scranial Dopplersonography forpatients who donot have ananeurysm, thistechnique isbeing investi-gated in patientswith TBI. Withthis technique, aprobe with alow-frequencyultrasonic signalis used on thin
areas of cranium to measure veloc-ity and direction of blood flow inthe intracranial arteries.31,32
Although most commonly used todetect vasospasm after cerebralaneurysms, Doppler imaging can beused to detect posttraumatic cere-bral hemodynamic changes andcomplications such as hyperemia,
32 CriticalCareNurse Vol 31, No. 2, APRIL 2011 www.ccnonline.org
Figure 6 Vasodilatation (left) and vasoconstriction (right) cascades protect the brain. The dynamics of cerebral blood flow arebest encompassed by the patterns of intact autoregulation. The vasodilatation cascade occurs when cerebral perfusion pressure(CPP) decreases, leading to increases in cerebral blood volume (CBV) and intracranial pressure (ICP), which can lead to edema. IfCPP increases, vasoconstriction occurs, reducing CBV and decreasing edema by decreasing ICP.
Edema+CSF
Reduceedema
– Blood viscosity
Hyperemia
Hypocapnia
+ Blood viscosity
Hypoxia
Hypercapnia– CPP + CPP
+ ICP – ICP+ CBV – CBV
+ Vasodi-latation
+ Vasocon-striction
Figure 7 Hemedex catheter. Probe can be tunneled or bolted.Probe is embedded 2 to 2.5 cm below the dura.Courtesy Hemedex Inc, Cambridge, Massachusetts.
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

vasospasm, decreased CBF, andintracranial hypertension.31,32 Tran-scranial Doppler sonography pro-vides a real-time assessment ofchanges in flow velocity that reflectchanges in CBF when cardiac out-put and blood pressure remainconstant.32-34
Blood Pressure Mean arterial pressure (MAP)
and ICP are important in calculat-ing CPP (CPP=ICP–MAP). CPP isdirectly proportional to CBF. Drasticdecreases in CPP result in decreasedCBF. Autoregulation (Figure 6) pro-tects the brain from variation inblood pressure. When autoregula-tion is functional, large changes inMAP do not lead to significantchanges in CBF.35 If autoregulationis impaired, uncontrolled bloodpressure directly causes changes inICP, CPP, and CBF. In patients withimpaired autoregulation, reducingblood pressure reduces CBF andaggravates ischemia. In contrast, inpatients with impaired cerebralautoregulation, hypertension cancause increases in ICP and CBF.35
Blood pressure is measured byusing a cuff or an arterial catheter.
Normal CBF is 18 to 35 mL/100 gper minute.30 The threshold value is15 mL/100 g per minute36 (Table 2).Because of the synergistic relation-ship between CBF and arterial bloodpressure, both parameters must beconsidered in therapeutic decisionmaking.26 MAP is monitored at leasthourly; the goal is to maintain anoptimal MAP to achieve a CPPgreater than 60 mm Hg (Table 2).MAP can be controlled by using flu-ids and vasoactive agents. Medica-tions that decrease MAP includemetoprolol, nicardipine, enalapril,
such as near-infrared spectroscopyand more invasive fiber-opticcatheter technology1; however, adirect monitoring system hasrecently been introduced.
The Licox PBTO2 monitoring sys-tem (Integra NeuroSciences, Plains-boro, New Jersey) measures PO2 andtemperature in the brain. PO2 is anestablished marker of cerebralischemia and secondary brain injury.The triple-lumen introducer kit,with a 7-mm–long oxygen-sensingarea at the distal tip, measuresregional oxygenation, with separateprobes to measure ICP and temper-ature. The most recent device pro-vides the option to bolt or tunnelthe catheter and has a sensor thatmeasures temperature and oxygenintegrated into the same catheter.The Licox catheter uses Clark-typeelectrode technology to measurePO2 in blood of tissue.38
The catheter is placed 25 to 35 mm into the brain. The oxygensensor is located in the white matterof the brain, preferably in thepenumbra of the injured area. Thecatheter is inserted via the triple- ordouble-lumen bolt. The optimallocation for normal brain measure-ments is uninjured brain. Setupand calibration are minimal. Afterthe brain has adjusted to the newcatheter, an oxygen challenge testshould be performed by setting theventilator fraction of inspired oxy-gen at 100% for 2 to 5 minutes. PBTO2should increase. A neurosurgeoncan adjust the probe as needed.
Although measuring ICP andCPP is key in patients with TBI,monitoring cerebral oxygenationcan indicate hypoxic events earlierthan monitoring ICP and CPP canand thus may improve neurological
nitroglycerin, and nitropresside. Sub-optimal MAP can be increased byusing phenylephrine, norepinephrine,vasopressin, or dopamine. Maintain-ing optimal CPP in order to maximizeCBF may also require interventionsthat decrease ICP (Figure 5).
Brain Tissue OxygenationMechanisms
Maintaining appropriate oxygenflow to satisfy the metabolic demandsof the brain is critical to ensuringgood neurological outcome. Thisconcept is emphasized more generallyin the overall physiological resuscita-tion of injured patients.1,17 Establish-ing a patent airway and restoringcirculating blood volume and oxy-genation are all attempts to maintainnormal oxygenation of brain tissue.
The principal cause of secondarybrain damage and poor neurologicaloutcome is cerebral hypoxia triggeredduring the ischemic cascade.17,37 Sys-temic hypoxia, hypotension, andintracranial hypertension can lead tooxygen deprivation. If autoregulationis functional, low PO2 can be resolvedby vasodilatation. When autoregula-tion is impaired, low oxygen flow eas-ily disrupts brain metabolism.17,28 Theeffects of manipulations of ICP, CPP,and PCO2 on PBTO2 have been reviewedextensively, stressing that high ICPand low CPP correlate with low PBTO2and poor neurological outcome.37
Monitoring SystemsThe Brain Trauma Foundation
recommends oxygen monitoringbecause a significant number ofpatients with TBI have hypoxemiaand hypotension. As with ICP tech-nology, various techniques for PBTO2monitoring have been developed.Examples include indirect systems
NtoJuTth
www.ccnonline.org CriticalCareNurse Vol 31, No. 2, APRIL 2011 33
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

outcome. The goal PBTO2 value isgreater than 20 mm Hg; the ideal is30 mm Hg. Lower values may indi-cate impending hypoxia.1 A PBTO2of 55 mm Hg suggests a thresholdvalue defined as “luxury perfusion.”39
In order to improve PBTO2 duringischemic conditions, CBF can bemaximized by decreasing ICP viabarbiturates, CSF drainage, and/orcraniotomy. If the decreased PBTO2is due to lower oxygen delivery,increasing CPP and avoiding hypoten-sion, hypovolemia, and hypoxia willbe important. Common interven-tions to improve cerebral oxygendelivery include administration ofisotonic solutions, vasopressors,and blood transfusions and increasesin the fraction of inspired oxygen.Because pain, shivering, agitation,and fever further increase cerebralmetabolism, sedatives, anti -inflammatory agents, and coolingdevices are used. In contrast, PBTO2may reach luxury perfusion levelsbecause of hyperemia or excessivecerebral blood flow, which increasesICP. High PBTO2 and hyperemia canbe temporarily reduced with care-fully guided prophylactic hyperven-tilation, although this interventionmay cause secondary injury. If hyper-ventilation is used, brain oxygena-tion should be monitored with eithera tissue oxygenation monitor or ajugular bulb catheter. Decreasingbody temperature and inducingheavy sedation can further decreasethe demand of the brain tissue andin turn increase PBTO2
1 (Figure 5).
Brain Temperature andHypothermiaReduction of Brain Temperature
In humans, brain temperatureis an important marker of brain
Monitoring Brain TemperatureMonitoring brain temperature
is relatively easy because it is anintegral part of multiple systems. In our ICU, the Camino bolt systemand the Hemedex and Licox systemscan all be used to monitor braintemperature.
Brain hyperthermia, a tempera-ture of 38.5ºC or greater, can be pre-vented by multiple methods. Ofnote, brain hyperthermia must bemonitored simultaneously withbody temperature to ensure thatcooling interventions are adequatelyaffecting the temperature of theinjured brain tissue. Administrationof antipyretics such as acetamino-phen or ibuprofen is a common ini-tial therapeutic intervention. Passivecooling measures such as coolingblankets and/or ice packs can beused.43 Invasive cooling measuresare considered if the noninvasivemethods are ineffective. We use theThermogard XP system (Zoll Med-ical Corporation, Chelmsford, Mas-sachusetts), an intravascular,multilumen catheter. We preventhyperthermia in patients with TBIby starting use of the ThermogardXP system if brain temperature isgreater than 38.5ºC. The Hemedexmonitor for CBF functions withinthe temperature ranges of 25ºC to39.5ºC.1 The goal of using the Ther-mogard XP system is to reducebrain temperature to a normother-mic range of 36ºC to 37ºC. Ourhyperthermia orders require fre-quent laboratory tests for levels ofpotassium, phosphates, and magne-sium; prothrombin and partialthromboplastin times, and plateletcounts to prevent coagulopathies.43
Treatment with the Thermogardmay cause shivering, a normal
metabolism and cellular injury. Ininitial studies on ischemic brain inanimals, slight changes in braintemperature accounted for fluctua-tions in histological changes in braintissue. Normothermia and moder-ate hypothermia in rats (33ºC)resulted in a marked decrease inbrain glutamate levels, the metabo-lite uncontrollably released duringtissue energy failure. Although low-ering brain temperature in humanswith TBI is still debated and scien-tifically unproved, the interventionis a neuroprotective strategy that intheory reduces the metabolic demandof the brain, possibly decreasingsecondary neuronal injury andimproving behavioral outcomes.40-42
The mechanisms of moderatehypothermia (32ºC-33ºC) and nor-mothermia (36ºC-37ºC) on postis-chemic tissue, although complex,are multifunctional. At the cellularlevel, hypothermia and reductionof brain temperature in general canblock excitatory neurotransmitters.Prevention of toxic calcium overloadallows continued proper amino acidfolding by replacing ubiquitin andresults in improved oxygen deliveryand CBF and depresses the immuneresponse. Increased brain tempera-ture has been associated with longerICU stays and thus extended inten-sive care, as well as higher mortal-ity.42 Finally, smaller nonrandomand class 2 clinical studies haveindicated the successful use ofhypothermia in neuroprotection.42
Similarly the Brain Trauma Founda-tion1 has recommended that inducedhypothermia within the first 48hours of injury may reduce mortal-ity, further stressing the importanceand merit of temperature monitor-ing in TBI.
34 CriticalCareNurse Vol 31, No. 2, APRIL 2011 www.ccnonline.org
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

thermoregulatory response to hypo -thermia. Shivering increases oxygenconsumption in skeletal muscles,diverting valuable oxygen away fromthe injured brain. Refractory shiver-ing may require deep sedation and/or the administration of paralyticagents to facilitate the induction andmaintenance of hypothermia andminimize oxygen consumption.43-45
ConclusionAdvancements in neuromonitor-
ing have improved the bedside careof patients with TBI. These develop-ments have provided the possibilityof true multimodal monitoring foreffective therapy. As described inthis article, we have taken steps toturn this possibility into a routinestandard of practice. Neuromonitor-ing traditionally has been used as amethod of detecting problems asthe problems emerge. Yet, many ofthese technologies can be used todetect problems before the problemsbecome major, thus creating theopportunity for more timely inter-ventions. The nursing staff in ourICU realize that caring for patientswith complex brain injuries requiresvigilant monitoring of multipleparameters in hopes of preventingsecondary injury. In addition to theconventional placement of a ven-triculostomy in a patient with TBI,we routinely use microdialysis toevaluate metabolic changes (glucose,pyruvate, lactate, glycerol) and vari-ous monitoring systems to assess
ICP, CPP, CBF, blood pressure, andbrain temperature. Figure 8 showsplacement of the devices in a typicalpatient in our ICU. In this article,we have detailed our practice byexplaining the background of theparameters monitored in TBIpatients, the technical aspects ofeach machine or device used, andrelated therapeutic interventions.Our use of multimodal monitoringto provide comprehensive care hasgreat potential to improve the out-comes of our patients who havemarked neurological injury. CCN
AcknowledgmentsThis manuscript would not have been possiblewithout the editorial guidance of Christine SmithSchulman, RN, CNS, CCRN, the clinical nurse special-ist at Legacy Emanuel Medical Center. In addi-tion, we thank Dan Jones, RN, and KimberlySkaale, RN, staff nurses in ICU East at LegacyEmanuel Medical Center, for their review of themanuscript.
Financial DisclosuresNone reported.
References1. Brain Trauma Foundation; American Asso-
ciation of Neurological Surgeons; Congressof Neurological Surgeons; Joint Section on
Neurotrauma and Critical Care, AANS/CNS;Bratton SL, Chestnut RM, Ghajar J, et al.Guidelines for the management of severehead injury [published correction appearsin J Neurotrauma. 2008;25(3):276-278] .J Neurotrauma. 2007;24 (suppl 1):S1-S106.
2. Bader M. Gizmos and gadgets for the neu-roscience intensive care unit. J Neurosci Nurs.2006;38(4):248-260.
3. Bellander B, Cantais E, Enblad P, et al.Consensus meeting on microdialysis inneurointensive care. Intensive Care Med.2004;30(12): 2166-2169.
4. Goodman JC, Robertson CS. Microdialysis:is it prime time? Curr Opin Crit Care. 2009;15(2):110-117.
5. Presciutti M, Schmidt JM, Alexander S.Neuromonitoring in intensive care: focuson microdialysis and its nursing implica-tions. J Neurosci Nurs. 2009;41(3):131-139.
6. Persson L, Hillered L. Chemical monitoringof neurosurgical intensive care patients usingintracerebral microdialysis. J Neurosurg.1992;76:72-80.
7. Tisdall MM, Smith M. Cerebral microdialy-sis: research technique or clinical tool. Br JAnaesth. 2008;97(1):18-25.
8. Hillered L, Vespa P, Hovda D. Translationalneurochemical research in acute humanbrain injury: the current status and poten-tial future for cerebral microdialysis. J Neu-rotrauma. 2005;22:3-41.
9. Johnston AJ, Gupta AK. Advanced monitor-ing in the neurology intensive care unit: micro -dialysis. Curr Opin Crit Care. 2002;8:121-127.
10. Zauner A, Daugherty WP, Bullock MR,Warner DS. Brain oxygenation and energymetabolism, I: biological function andpathophysiology. Neurosurgery. 2002;51(2):289-301.
11. Peerdeman SM, Girbes AR, Vandertop WP.Cerebral microdialysis as a new tool forneurometabolic monitoring. Intensive CareMed. 2000;26:662-669.
12. Ungerstedt U, Rostami E. Microdialysis inneurointensive care. Curr Pharm Des. 2004;10(18):2145-2152.
13. Peerdeman S, Tulder MW, Vandertop W.Cerebral microdialysis as a monitoringmethod in subarachnoid hemorrhagepatients, and correlation with clinicalevents. J Neurol. 2003;250:797-805.
Figure 8 Placement of multimodal catheters and monitoring probes. Computedtomography scans of 24-year-old woman with severe traumatic brain injury showplacement of catheter for microdialysis and probes for monitoring brain tissue partialpressure of oxygen, blood flow, and intracranial pressure.
Microdialysis
HemedexHemedexLicox
To learn more about traumatic brain injury,read “Functional and Cognitive Recovery ofPatients With Traumatic Brain Injury: Pre-diction Tree Model Versus General Model”in Critical Care Nurse, 2009;29(4):12-22. Available at www.ccnonline.org.
Now that you’ve read the article, create or contributeto an online discussion about this topic using eLetters.Just visit www.ccnonline.org and click “Respond toThis Article” in either the full-text or PDF view ofthe article.
www.ccnonline.org CriticalCareNurse Vol 31, No. 2, APRIL 2011 35
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from

14. Reinstrup P, Stahl N, Mellergard P, Uski T,Ungerstedt U, Nordstrom CH. Intracerebralmicrodialysis in clinical practice: baselinevalues for chemical markers during wake-fulness, anesthesia, and neurosurgery. Neu-rosurgery. 2000;47:701-709.
15. Oddo M, Schmidt JM, Carrera E, et al.Impact of tight glycemic control of cerebralglucose metabolism after severe braininjury: a microdialysis study. Crit Care Med.2008;36(12):3233-3238.
16. Chang JJ, Youn TS, Benson D, et al. Physio-logic and functional outcome correlates ofbrain tissue hypoxia in traumatic braininjury. Crit Care Med. 2009;37(1):283-290.
17. Meixensberger J, Jaeger M, Väth A, Dings J,Kunze E, Roosen K. Brain tissue oxygenguided treatment supplementing ICP/CPPtherapy after traumatic brain injury. J Neu-rol Neurosurg Psychiatry. 2003;74(6):760-764.
18. Steiner LA, Andrews PJ. Monitoring theinjured brain: ICP and CBF. Br J Anaesth.2006;97(1):26-38.
19. Reinert M, Barth A, Rothen HU, Schaller B,Takala J, Seiler RW. Effects of cerebral per-fusion pressure and increased fraction ofinspired oxygen on brain tissue, oxygen,lactate and glucose in patients with severehead injury. Acta Neurochir (Wein).2003;145(5):341-349.
20. Carter BG, Butt W, Taylor A. ICP and CPP:excellent predictors of long term outcomein severely brain injured children. ChildsNerv Syst. 2008;24(2):245-251.
21. Taylor WR, Chen JW, Meltzer H, et al.Quantitative pupillometry, a new technol-ogy: normative data and preliminary obser-vations of patients with acute head injury. J Neurosurg. 2003;98(1):205-213.
22. Camino User Manual. Plainsboro, NJ: Inte-gra NeuroSciences; 2004.
23. Jenkinson MD, Hayhurst C, Al-Jumaily M,Kandasamy J, Clark S, Mallucci CL. Therole of endoscopic third ventriculostomy inadult patients with hydrocephalus. J Neuro-surg. 2009;110(5):861-866.
24. Chesnut R. The implications of the guide-lines for the management of severe headinjury for the practicing neurosurgeon.Surg Neurol. 1998;50:87-193.
25. Wolfe T, Torbey M. Management of intracra-nial pressure. Curr Neurol Neurosci Rep. 2009;9:477-485.
26. Shardlow E, Jackson A. Cerebral blood flowand intracranial pressure. Anesth IntensiveCare Med. 2008;9:222-225.
27. Gwinnutt CL, Saha B. Cerebral blood flowand intracranial pressure. Anesth IntensiveCare Med. 2005;6:153-156.
28. Walters FJ. Intracranial pressure and cere-bral blood flow. Update Anaesth. 1998;8.http://www.nda.ox.ac.uk/wfsa/html/u08/u08_013.htm. Accessed May 30, 2010.
29. Vajkoczy P, Schomacher M, Czabanka M,Horn P. Monitoring cerebral blood flow inneurosurgical intensive care. Eur Neurol Dis.2007;7:6-10. http://www.touchneurology.com/articles/monitoring-cerebral-blood-flow-neurosurgical-intensive-care?page=0%2C4. Accessed June 7, 2010.
30. HEMEDEX Pocket Reference Guide. Rayn-ham, MA: Codman & Shurtleff Inc; 2008.
31. Doberstein C, Martin NA. TranscranialDoppler ultrasonography in head injury.In: Narayan RK, Wilberger JE, PovlishockJT, eds. Neurotrauma. New York, NY:McGraw-Hill Co; 1996:539-552.
32. Saqqur M, Zygun D, Demchuk A. Role oftranscranial Doppler in neurocritical care.Crit Care Med. 2007;35:216-223.
33. Molina CA, Barreto AD, Taivgoulis G, et al.Transcranial ultrasound in clinical sono-brombolysis (TUCSON) trial. Ann Neurol.2009;66(1):28-38.
34. Czosnyka M, Brady K, Reinhard M,Smielewski P, Steiner LA. Monitoring ofcerebrovascular autoregulation: facts, mythsand missing links. Neurocrit Care. 2009;10(3):373-386.
35. Phan N, Rosenthal G, Manley G. Bedsideassessment of cerebral pressure autoregula-tion and vasoreactivity in severe traumaticbrain injury: insight in arterial vs. venouscontrol [abstract]. J Neurotrauma. 2009;26(8):A66. Abstract 255.
36. Botteri M, Bandera E, Minelli C, LatronicoN. Cerebral blood flow thresholds for cere-bral ischemia in traumatic brain injury: asystematic review. Crit Care Med. 2008;36:3089-3092.
37. Narotam PK, Burjonrappa SC, Raynor SC,Rao M, Taylon C. Cerebral oxygenation inmajor pediatric trauma: its relevance totrauma severity and outcome. J PediatrSurg. 2006;41(3):505-513.
38. Licox IMC Complete Neuromonitoring:Directions for Use (Model IP2.P). Plains-boro, NJ: Integra NeuroSciences; 2004.
39. Wilensky EM, Bloom S, Leicter D, et al.Brain tissue oxygen practice guidelinesusing the LICOX CMP monitoring system2005. J Neurosci Nurs. 2005;37:278-288.
40. Gallangher C, Tyson R, Sutherland G. Dif-ferential neuronal and glial metabolicresponse during hypothermia in an experi-mental animal model. Neurosurgery. 2009;64:555-561.
41. Zhao H, Steinberg G, Sapolsky R. Generalversus specific actions of mild-moderatehypothermia in attenuating cerebralischemic damage. J Cereb Blood Flow Metab.2007;27:1879-1894.
42. Sahuquillo J, Mena MP, Vilalta A, Poca MA.Moderate hypothermia in management ofsevere traumatic brain injury: a good ideaproved ineffective? Curr Pharm Design.2004;10:2193-2204.
43. Weinberg AD. Hypothermia. Ann EmergMed. 1993;22:370-377.
44. Diller K, Zhu L. Hypothermia therapy forbrain injury. Annu Rev Biomed Eng. 2009;11:135-162.
45. Buggy DJ, Crossley A. Thermoregulation,mild preoperative hypothermia and post-anesthetic shivering. Br J Anaesth. 2000;84:615-628.
36 CriticalCareNurse Vol 31, No. 2, APRIL 2011 www.ccnonline.org
by Fred Ferron on April 25, 2011ccn.aacnjournals.orgDownloaded from