Embed Size (px)
Citation preview

163www.allhealth.org
P ublic health – literally, thehealth of the public – is avast and complex enterprise
that defies simple definitions andboundaries. Compared to themedical system, which is primarilyconcerned with individual patientswhile they are ill or injured, thepublic health system seeks to keepcommunities and populationshealthy by educating them aboutphysical and mental health, andoperating programs to preventdisease, injury, and disability.1
Starting in 2001, Congress madenew financial investments in thepublic health infrastructure. In thelargest increases since World War II,2HHS distributed more than $7 billionto state and local govern-mentsbetween FY 2002 and FY 2006. Thegoal was to help them retool thepublic health system by hiring newpersonnel, improving laboratories,and broadly upgrading infra-structure, including informationtechnology that operates on a real-time basis.3 Still, as the devastationassociated with Hurricane Katrina in2005 made clear, the challengesremain enormous.
Following a visit to the Gulf Coast,Risa Lavizzo-Mourey, presidentand CEO of the Robert WoodJohnson Foundation, summed up amajor lesson from Katrina:
“…[M]ainstream America fails toregard huge numbers of our poorest,oldest, sickest, dispossessed, non-
KKEEYY FFAACCTTSS
Chapter 12:Public Health
Alliance for Health Reform
white people and their families asequal members of our society. If youhave any doubt… just think of thoseamazing pictures of the lost andforgotten of New Orleans huddledon rooftops, waving crude signs thatpleaded ‘Help Us,’ and calling outfor food and water that did notcome.”4
The collapse of critical infra-structure following Katrina under-scored the importance of building astronger and better coordinatedpublic health system thatencompasses many facets:sanitation, safe water and foodsupplies, control of infectiousdiseases, management of chronicdiseases, environmental riskreduction, access to health care,risk communication, andemergency preparedness.
This chapter describes the broadgoals, organization and financingof our public health system, anddiscusses current unmet andanticipated future challenges. Toget information about specificpublic health areas that are notcovered in this chapter, see the box,“Some Leading Public HealthResources.”
HOW DOES PUBLICHEALTH WORK?
Operating in the shadow ofmedicine, the public health systemis often invisible to the public.Funding for public health is modest
COVERING HEALTH ISSUES, 2006
FFoorr ssttoorryy iiddeeaass oonn ppuubblliicc hheeaalltthh,, sseeee ppaaggee 117711.. AA lliisstt ooffeexxppeerrttss aanndd wweebbssiitteess bbeeggiinnss oonn ppaaggee 117722..
Out of every $100 spent on healthin the U.S., only $3 is spent onpublic health by the government.a
The annual budget of the Centersfor Disease Control andPrevention (CDC) was $6.2 billionin 2006, compared to $28.6 billionfor the National Institutes ofHealth.b
The average lifespan increasedby 30 years during the 20thcentury. The CDC estimates that25 of those years were due topublic health improvements.c
Levels of lead in the blood arehigher for African-Americanchildren compared to white andHispanic children.d
Diabetes affects nearly 21 millionAmericans and is much morecommon among communities ofcolor than among whites.e
The growth in obesity prevalencein the U.S. is estimated toaccount for 27 percent of thegrowth in health spending overthe past 20 years.f
12

COVERING HEALTH ISSUES, 2006 CHAPTER 12
Alliance for Health Reform www.allhealth.org164
12
Some Leading Public Health ResourcesASTHMA
Information for Patients and the Public: http://www.nhlbi.nih.gov/health/public/lung/index.htm
Steps to a Healthier US: Prevention Report, Focus on Asthma, HHS Office of Disease Prevention and Health Promotion, Winter 2004:http://odphp.osophs.dhhs.gov/pubs/prevrpt/04Volume18/Issue2pr.htm
EPA Publications on Asthma and Indoor Environments,http://www.epa.gov/asthma/publications.html
BIOTERRORISMCDC: Bioterrorism Preparedness and Response, www.bt.cdc.gov
University of Minnesota Center for Infectious Disease Research and Policy,http://www.cidrap.umn.edu/index.html
CANCERCDC’s National Program of Cancer Registries, http://www.cdc.gov/cancer/npcr/
National Cancer Institute Surveillance, Epidemiology, and End Results (SEER), http://seer.cancer.gov
US Cancer Statistics, 2002, http://www.cdc.gov/cancer/npcr/uscs/index.htm
CHILDREN’S HEALTHBright Futures: Prevention and Health Promotion for Infants, Children, Adolescents, and Their Families(developed by HRSA’s Maternal and Child Health Bureau), http://brightfutures.aap.org/web/
EPA: Children’s Health Protection, http://yosemite.epa.gov/ochp/ochpweb.nsf/content/homepage.htm
DIABETESAmerican Diabetes Association, http://www.diabetes.org/home.jsp
National Diabetes Education Program, http://www.ndep.nih.gov/
EMERGENCY PREPAREDNESSFederal Emergency Management Agency, http://www.fema.gov
Public Health Emergency Response Guide for State, Local, and Tribal Health Directors http://www.bt.cdc.gov/planning/responseguide.asp
FOOD SAFETYCDC Food Safety Office, http://www.cdc.gov/foodsafety
The Food Safety Network, http://www.foodsafety.gov/~fsg/fsggov.html
HIV/AIDSHIV/AIDS Observance Days, http://www.omhrc.gov/hivaidsobservances/index.html
Kaiser Family Foundation HIV/AIDS Policy Research, Analysis, Media, and Public Health Partnershipshttp://www.kff.org/hivaids/index.cfm
CDC’s National Prevention Information Network, http://www.cdcnpin.org/scripts/index.asp
IMMUNIZATIONSNational Immunization Program, CDC http://www.cdc.gov/nip/
Mayo Clinic: How Vaccines Work , http://www.mayoclinic.com/health/vaccines/ID00023
INJURY PREVENTIONNational Center for Injury Prevention and Control, CDC, www.cdc.gov/ncipc/

by comparison to medicine, accounting for onlythree percent of the $1.9 trillion spent on health in2004.5 Yet over the last century, public health hasmade enormous contributions to society. During theearly 20th century, mortality in America fell by 40percent; clean water systems alone are credited withalmost half of the reduction in major cities. 6
In addition, public health agencies are well knownfor providing one-to-one or “personal health”services, which focus on prevention and earlydiagnosis. For example, cancer screening is availablefor people who can’t pay medical bills because theyare uninsured or underinsured. Immunizationcampaigns are often organized by public healthagencies, as are treatment services for infectiousdiseases, such as HIV/AIDS. Equally important are“population health” services that take the form ofsuch initiatives as driving safety (e.g., promotion of
seatbelt laws and airbags to prevent and minimizeinjury), tobacco control and SARS (Severe AcuteRespiratory Syndrome) prevention campaigns.7
The nation’s roadmap for meeting national publichealth goals is Healthy People 2010(www.healthypeople.gov). The initiative has beencoordinated for more than 25 years by the Office ofDisease Prevention and Health Promotion within theDept. of Health and Human Services (HHS), incollaboration with national organizations, state andlocal health departments, foundations, corporations,and many others in both the public and privatesectors.
State and local health departments use HealthyPeople to set their own targets,8 which are reported toand analyzed by the National Center for HealthStatistics at HHS’ Centers for Disease Control and
CHAPTER 12
www.allhealth.org Alliance for Health Reform
COVERING HEALTH ISSUES, 2006
165
12
Some Leading Public Health Resources (Cont.)OBESITY
Statistics Related to Overweight and Obesity, http://win.niddk.nih.gov/statistics/index.htmSurgeon General’s Call to Action to Prevent and Decrease Overweight and Obesityhttp://www.surgeongeneral.gov/topics/obesity/
PANDEMIC FLUPandemic Flu, www.pandemicflu.gov
Pandemic Influenza: National Vaccine Program Office, http://www.hhs.gov/nvpo/pandemics/
WHO Handbook for Journalists: Influenza Pandemic. December 2005http://www.pandemicflu.gov/rcommunication/
TOBACCOCDC’s Tobacco Information and Prevention Source (TIPS), http://www.cdc.gov/tobacco/
American Legacy Foundation (established by the Master Settlement Agreement),www.americanlegacy.org
Master Settlement Agreement: National Association of Attorneys General Tobacco Project,http://www.naag.org/issues/issue-tobacco.php
Smoking and Tobacco Control Monographs, National Cancer Institute,http://cancercontrol.cancer.gov/tcrb/monographs/
Special Reports: State Tobacco Settlement, November 2005.,http://www.tobaccofreekids.org/reports/settlements/
WOMEN’S HEALTHNational Women’s Health Information Center, HHS, www.4woman.gov
Minority Women’s Health, http://www.4woman.gov/minority/offices/
Women’s Health FastStats, http://www.cdc.gov/nchs/fastats/womens_health.htm

COVERING HEALTH ISSUES, 2006
Prevention (CDC). Quarterly data updates areavailable at http://wonder.cdc.gov/data2010/about.htm.9
Among the initiative’s 28 focus areas, some call forreductions in the prevalence of widespread chronicdiseases, such as cancer, diabetes and kidney disease.Other focus areas set targets for capacity-building,such as improvements in communications and publichealth infrastructure (see below). An overarchinggoal is to eliminate health disparities – aresponsibility that is shared with the medical system– through a strategy of public education campaignsthat can reduce individual risk factors, incombination with improvements in treatment ofchronic conditions.10
WHAT DOES PUBLIC HEALTHINFRASTRUCTURE INCLUDE?
The U.S. public health system is extensive. Itincludes:
- 2,864 local health departments; - 59 state, territorial and island nation health
departments;- Various federal agencies, particularly the CDC
and the Health Resources and ServicesAdministration (HRSA), which use much oftheir funding for state programs;
- Tribal health agencies, coordinated by the IndianHealth Service;
- More than 160,000 public and private laborato-ries;
- Hospitals and other private-sector healthcareproviders;
- Volunteer organizations, such as the AmericanRed Cross, the American Diabetes Association,the American Cancer Society and many others.11
When it comes to emergency response, local publichealth officials are always the first on the scene.These officials have multiple additionalresponsibilities, including monitoring of diseaseoutbreaks, environmental and restaurant healthinspections, oversight of delivery of preventiveservices such as immunizations and dozens of otheractivities.12
Under state constitutions, states have the primarylegal authority and responsibility for residents’public health and safety. The public health
department is a free-standing agency in half of thestates, and in all but one of those, the director is amember of the Governor’s cabinet. Other states havemultipurpose agencies that combine health, humanservices, environmental and other responsibilities.Every state and local jurisdiction approaches publichealth somewhat differently, depending oncommunity preferences, elected leadership priorities,geography, economic and business resources,regional health systems and other factors. 13
At the federal level, CDC is the lead agency.14 Whilea large proportion of the agency’s budget goes tostates,15 CDC also funds other partners, such as theAssociation of State and Territorial Health Officials,the Association of Public Health Laboratories, theNational Association of County and City HealthOfficials, the Council of State and TerritorialEpidemiologists,16 the Association of Schools ofPublic Health, and the Association of AmericanMedical Colleges,17 among others. Theseorganizations sponsor conferences, conveneworkgroups, develop and implement policies,conduct surveys and other research and providestandardized guidance and technical assistance.
The multi-disciplinary workforce numbers abouthalf a million federal, state, local and private sectorpersonnel.18 They include professional, technical,scientific, management, program administrators,researchers and support personnel, some of whommust be licensed and certified by state authorities orprofessional organizations.19 Public health nurses,administrators and environmental specialists are thelead occupational categories. Other key players arelaboratory personnel, inspectors, nutritionists,physicians, dentists, pharmacists, occupationalsafety specialists, engineers, biostatisticians, healtheducators, veterinarians and epidemiologists.20
HOW IS PUBLIC HEALTH FUNDED?
Only about three percent of the $1.9 trillion spent onhealth was used for population-based prevention andpublic health services in 2004.21 Because mostpublic health programs receive funding frommultiple sources, and many are run collaborativelywith several agencies (e.g., agencies dedicated tomental health and aging services), total spendingfigures on public health are hard to calculate.22
In addition to federal dollars, local governments
CHAPTER 12
Alliance for Health Reform www.allhealth.org166
12
contribute significantly to public health spending. Atthe state level, health departments depend heavily onfederal grant funds, and also receive some fundingfrom state taxes. At the local level, funding sourcesare diverse. For example, some counties andmunicipalities use property and sales taxes to fundprograms, and many charge fees for particularservices. Private foundations are also an importantsource of funding for research and for specialprojects in key areas such as health care for theuninsured, HIV/AIDS, alcoholism, obesity and drugabuse.23
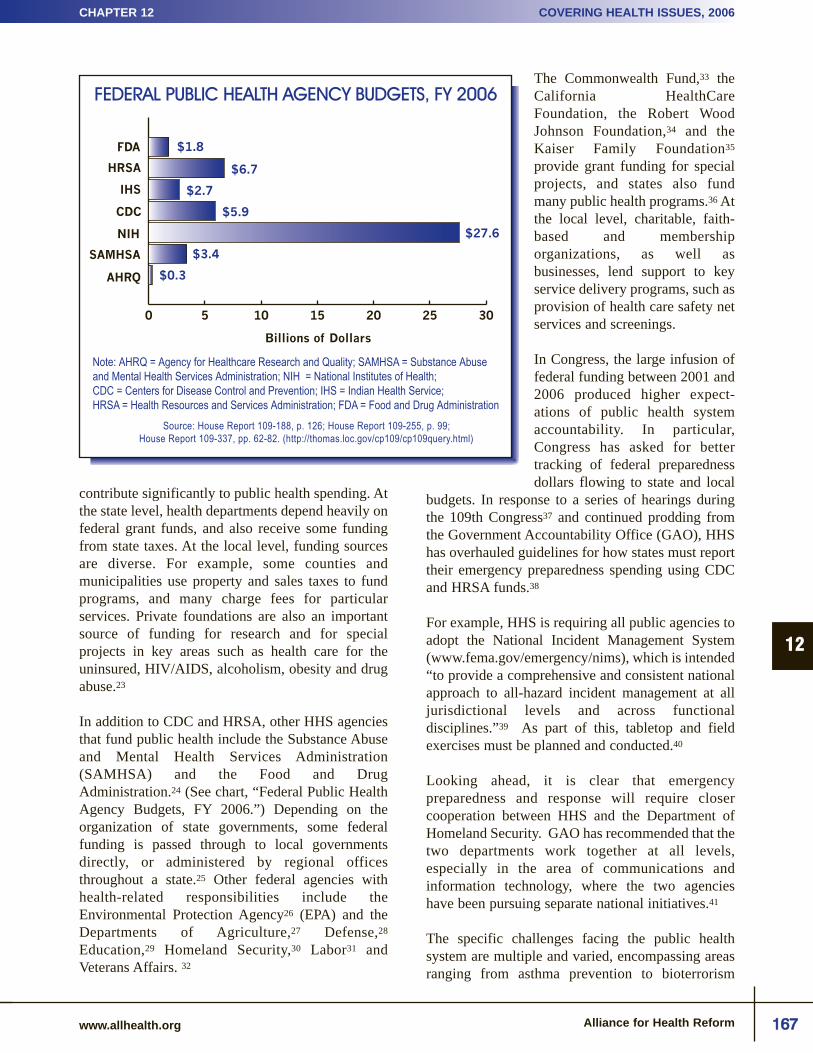
In addition to CDC and HRSA, other HHS agenciesthat fund public health include the Substance Abuseand Mental Health Services Administration(SAMHSA) and the Food and DrugAdministration.24 (See chart, “Federal Public HealthAgency Budgets, FY 2006.”) Depending on theorganization of state governments, some federalfunding is passed through to local governmentsdirectly, or administered by regional officesthroughout a state.25 Other federal agencies withhealth-related responsibilities include theEnvironmental Protection Agency26 (EPA) and theDepartments of Agriculture,27 Defense,28
Education,29 Homeland Security,30 Labor31 andVeterans Affairs. 32
The Commonwealth Fund,33 theCalifornia HealthCareFoundation, the Robert WoodJohnson Foundation,34 and theKaiser Family Foundation35
provide grant funding for specialprojects, and states also fundmany public health programs.36 Atthe local level, charitable, faith-based and membershiporganizations, as well asbusinesses, lend support to keyservice delivery programs, such asprovision of health care safety netservices and screenings.
In Congress, the large infusion offederal funding between 2001 and2006 produced higher expect-ations of public health systemaccountability. In particular,Congress has asked for bettertracking of federal preparednessdollars flowing to state and local
budgets. In response to a series of hearings duringthe 109th Congress37 and continued prodding fromthe Government Accountability Office (GAO), HHShas overhauled guidelines for how states must reporttheir emergency preparedness spending using CDCand HRSA funds.38
For example, HHS is requiring all public agencies toadopt the National Incident Management System(www.fema.gov/emergency/nims), which is intended“to provide a comprehensive and consistent nationalapproach to all-hazard incident management at alljurisdictional levels and across functionaldisciplines.”39 As part of this, tabletop and fieldexercises must be planned and conducted.40
Looking ahead, it is clear that emergencypreparedness and response will require closercooperation between HHS and the Department ofHomeland Security. GAO has recommended that thetwo departments work together at all levels,especially in the area of communications andinformation technology, where the two agencieshave been pursuing separate national initiatives.41
The specific challenges facing the public healthsystem are multiple and varied, encompassing areasranging from asthma prevention to bioterrorism
CHAPTER 12
www.allhealth.org Alliance for Health Reform
COVERING HEALTH ISSUES, 2006
167
12
FEDERAL PUBLIC HEALTH AGENCY BUDGETS, FY 2006
Source: House Report 109-188, p. 126; House Report 109-255, p. 99;House Report 109-337, pp. 62-82. (http://thomas.loc.gov/cp109/cp109query.html)
$1.8
Note: AHRQ = Agency for Healthcare Research and Quality; SAMHSA = Substance Abuseand Mental Health Services Administration; NIH = National Institutes of Health; CDC = Centers for Disease Control and Prevention; IHS = Indian Health Service; HRSA = Health Resources and Services Administration; FDA = Food and Drug Administration
Billions of Dollars
$6.7
$2.7
$5.9
$3.4
$0.3
0 5 10 15 20 25 30
FDA
HRSA
IHS
CDC
SAMHSA
AHRQ
NIH $27.6

COVERING HEALTH ISSUES, 2006
preparedness and food safety, and from delivery ofHIV/AIDS prevention and treatments to preparationfor a possible pandemic flu outbreak. Following arebrief discussions of five high-profile topics in thefield – obesity, public health workforce issues, healthinformation technology, environmental health andpublic health services for the uninsured. For ideas onhow to further explore these and other areas, see thebox, “Some Leading Public Health Resources.”
ADDRESSING OBESITY IN THEPOPULATION
Arguably one of the biggest current public healthchallenges is the obesity epidemic – principallybecause of its connection to costly chronicconditions, including heart disease and diabetes – theconsequences of which can include kidney failureand limb amputations. In 1991, obesity prevalencerates were 15-19 percent in four states and above 20percent in none. But by 2004, prevalence rates were
20-24 percent in 33 states and above 25 percent innine states.42 Some economists think obesity hasaccounted for as much as 27 percent of the growth inhealth spending over the past 20 years – largelybecause it contributes to diabetes, hypertension andheart disease, among other costly chronicconditions.43 (See charts, “Obesity by State, 2005”and “Age Adjusted Incidence of Diabetes byRace/Ethnicity, 1997-2004.”)
The specific public health challenge is to identify themost effective interventions for improving nutritionand physical activity, and to develop strategies formaking these interventions affordable and availablein most communities – for example, in schoolcafeterias, worksites, playgrounds and grocerystores. These challenges are more difficult toimplement in some communities than others. Forexample, low-income working parents havetraditionally had to travel outside of theirneighborhoods to find a good selection of fresh fruits
CHAPTER 12
Alliance for Health Reform www.allhealth.org168
12
OBESITY BY STATE, 2005
Source: Centers for Disease Control and Prevention (www.cdc.gov/nccdphp/dnpa/obesity/trend/maps/index.htm)
(Percent of adults with a body mass index of 30+)
15% - 19% 20% - 24% 25% - 29% 30% - 34%

and vegetables in grocery stores. Thesefoods can also be more expensive thanfast food, and may require additionalpreparation. And for children in low-income communities, exerciseopportunities are often limited.44
In an effort to identify whatinterventions work, the CDC initiateda public-private partnership in the mid-1990’s to develop guidelines for aprogram known as “The CommunityGuide to Preventive Services”. Theguide reviews interventions that can beused in schools, at worksites, by healthcare systems and at a community-widelevel (www.thecommunityguide.org/obese).45
A complementary initiative is theNational Diabetes Education Program(NDEP), a joint effort of the CDC andthe National Institutes of Health(NIH). With more than 200 public andprivate organizations, NDEP supportscommunities, providers, and worksitesin educating individuals and families about pre-diabetes and diabetes prevention.46 NDEP uses anapproach in which scientists work directly withhealth educators and communications experts tocreate free and low-cost materials in severallanguages.47 The hope is that millions of people willlearn about and use NDEP’s meal planners,educational materials, and music CD’s and videosthat feature top artists promoting health messages(http://ndep.nih.gov/diabetes/pubs/ catalog.htm).48
PUBLIC HEALTH WORKFORCE
At the state level, economic recessions from 2001 to2003 prompted cuts in many state and local healthbudgets, including hiring freezes.49 Shortages ofpublic health personnel developed, and in 2004 wereas high as 20 percent in some states,50 withrecruitment being particularly difficult in rural andfrontier areas.51
One reason for shortages is the relatively modestsalaries made by many public health workforcepersonnel.52 Although wide variation exists acrossthe country and by position, in 2004, the nationalaverage salary of state and local public health
workers was only $42,000.53 Current shortages areespecially a pressing concern because the averageage of the public health workforce is now in the late40’s.54 Within the CDC, nearly half of the agency’sphysicians and biologists will be eligible forretirement by 2008.55
On a positive note, new undergraduate and graduateprograms in health sciences are training a morediverse generation of public health professionals.Since the mid-1990s, the proportion of racially andethnically diverse applicants for public healthschools has been increasing. In the fall of 2004, therewere more than 19,000 graduate students in thenation’s 36 accredited public health schools. One outof three is a member of a minority group, consistentwith the increasingly diverse population of the U.S.Since 1994, the number of applications receivedfrom members of minority groups has increased by87 percent, compared to a 54 percent increase inoverall applications.56
Some aspects of education are also becomingcheaper and more accessible. For example, dozens offree and low-cost continuing education courses areavailable online for practicing professionals.57 In a
CHAPTER 12
www.allhealth.org Alliance for Health Reform
COVERING HEALTH ISSUES, 2006
169
12
AGE-ADJUSTED INCIDENCE OF DIABETESBY RACE/ETHNICITY, 1997-2004
Source: Centers for Disease Control and Prevention (2005).(www.cdc.gov/diabetes/Statistics/incidence/table6.htm)
Hispanic
2000199919981997 2001
White
Rat
e P
er 1
000 P
opul
atio
n
4
6
8
10
12
9.2
7.4
4.6
2002
Black
2003 2004
9.6 9.710.3 10.4 10.5 10.5 10.5
7.78.2
9.5 9.6 9.8 9.59.9
4.7 4.95.4
6.06.5 6.5 6.6

COVERING HEALTH ISSUES, 2006
related effort, several national organizations havedeveloped a set of core competencies to helpstandardize the practice of public health and improveskills in the workforce.58
Core competencies have also been developed for theuse of health information technology, also known as“informatics,”59 where a long-term strategy will beneeded to train and retrain workers in an increasinglyelectronic environment.60 The American MedicalInformatics Association (www.amia.org) isspearheading an initiative to train 10,000 new healthprofessionals in informatics by the year 2010.61
HEALTH INFORMATION TECHNOLOGY(HEALTH IT)
Among the many lessons learned from HurricaneKatrina was the important role that informationtechnology and “telehealth” solutions played soonafter the storm. In one example, a CDC alert aboutflood-related bacterial infections that was linked to adatabase of dermatology images allowed health careworkers to provide rapid and informed treatment.62
Veterans were among the few evacuees whosemedical records were immediately available onlineto providers giving services in new locations.63 Butin general, providers had no easy access to evacuees’medical records, since much of the informationabout prescription drugs that individuals weretaking, as well as other necessary supplies, wasdestroyed.
To address this, the HHS Office of the NationalCoordinator of Health Information Technology(ONCHIT) took the lead in a multi-agency effort toquickly recreate vital patient information. In slightlymore than a week, the Office worked withphysicians, pharmacists and benefit managers tocompile individuals’ medical data in a temporarydatabase that was made available to providersserving evacuees.64
Subsequently, in November 2005, HHS announcedthat a task force hosted by the Southern GovernorsAssociation would lead planning efforts for “a digitalhealth information recovery” in the Gulf States.65
The regional coordination of health informationnetworks (also known as Regional HealthInformation Organizations) was already an HHSpriority, but it gained new momentum after thestorm.66 To support the participation of state and
local public health agencies in those regionalnetworks, the Robert Wood Johnson Foundationprovided one-year “InformationLinks” grants to 21locations.67
HHS is convening work groups to advise on ways tospeed up health IT adoption and will issuerecommendations for electronic health records andfor biosurveillance, real-time tracking of informationthat can triangulate information from multiplesources to more accurately assess bioterrorism riskand emerging public health threats.68 Additionalrecommendations have been made by the e-HealthInitiative and Connecting for Health, two nationalcollaboratives with private-sector funding.69 Thenext few years are critically important for thedevelopment of new information security andprivacy standards that aim to allay fears that healthIT increases the risk of public exposure or misuse ofsensitive personal information.70
ENVIRONMENTAL HEALTH
The toxic post-Katrina floodwaters were a graphicexample of threats to human health during anenvironmental disaster. Environmental assessmentsof toxins such as heavy metals and petroleumproducts in New Orleans found varying levels ofcontamination across the city.71 Since the duration ofexposure to toxins is important to human health,there is disagreement among experts about the realmagnitude of danger posed to residents and returningevacuees over the long term.72
Lead exposure, which affects brain function inyoung children and contributes to high bloodpressure in adults, is a longstanding public healthchallenge. Unfortunately, the most recent CDC“biomonitoring” report concluded that whilechildren’s blood lead levels have been decreasingoverall, levels among African American children arestill higher than among whites.73 Lead is classifiedas a possible human carcinogen by the InternationalAgency for Research on Cancer.74
Using “safer substitutes” based on the“precautionary principle” – i.e., taking steps toreduce unnecessary risk – is increasingly well-established in environmental health riskassessments.75 For example, NIH has nearlyeliminated the production of radioactive waste on itscampus in Bethesda, Md., and operates a mercury-
CHAPTER 12
Alliance for Health Reform www.allhealth.org170
12

free hospital.76 Kaiser Permanente, Wal-Mart,Hewlett Packard, Microsoft, and many other majorcorporations have phased out the use of PVC plastic(polyvinyl chloride or vinyl), which releases dioxin,a known carcinogen.77
Environmental risks associated with chemical plantshave been monitored by EPA since the late 1980’s, 78
but the risk of terrorism has heightened concernsabout chemical plant security. DHS has identified3,400 facilities that “pose the greatest hazard tohuman life and health” if attacked, including 272sites where worst-case releases of toxic chemicalscould sicken or kill more than 50,000 people.79
Nonetheless, long-standing tensions over federal andstate regulation of industry toxins and industry self-regulation are likely to continue.80
PUBLIC HEALTH AND THE UNINSURED
Many people assume that the public health system isprimarily designed to provide medical care foruninsured people and other vulnerable populations.This is understandable, since public health agenciesspend considerable time and resources providingpersonal health services – e.g., immunizations,screening for tuberculosis and other infectiousdiseases, family planning and primary health care –as compared to community prevention efforts andpopulation-based services.81 Social justice andequity are core values of the field, and as long as theuninsured population continues to seek services,public health agencies and personnel will keep tryingto address basic needs by providing some medicalcare for individuals who lack other options.
CURRENT POLICY DEBATES
Public health is moving in new directions to respondto current and emerging challenges, but the field’sscope of responsibility and discontinuities in fundingcan make planning for the future a constantchallenge. Looming challenges include the need toreinforce the workforce, make better use ofinformation technology, expand efforts to improveenvironmental health and continue programs that tryto meet basic health needs of a rising number ofuninsured people. Because public health is subject tothe annual appropriations process, funding can varysignificantly from year to year, thus making the fateof programs and initiatives uncertain. And there aresome signals that Congress’ enthusiasm forproviding new money for public health in the form of
funding for emergency preparedness may be waning.For example, the FY 2006 appropriation for state andlocal bioterrorism and public health preparednesswas $824 million, down from $919 million in FY2005.82
Looking ahead, because lifestyle factors –particularly smoking, being sedentary, and beingoverweight – affect personal health and contribute toleading causes of death and disease, debate is sure tocontinue about the proper role of government andprivate organizations, such as health insurers andemployers, in shaping what individuals decide to eatand drink, and how they spend their personal time.
STORY IDEAS
Based on the scientific evidence, it is now gener-ally accepted that the same risk factors – espe-cially smoking, being sedentary and being over-weight – can contribute to leading causes ofdeath and disease such as heart disease andstroke. Conversely, healthy lifestyles reducehealthcare costs and improve the quality of life.Ask experts in your state what they think aboutthe extent to which government, and privateorganizations, should tell people what to eat anddrink, and how to spend their personal time.
Do school systems in your area rely on contractswith soft drink vendors and candy manufacturersto supplement their budgets? Are there efforts tochange that policy?
How do low-income communities develop safe,accessible places for children to play and adultsto walk or jog?
What environmental health risks flow from com-mercial or residential sources in your communi-ty? Is there an impact on tourism, for example?Do companies use a “safer substitutes” approachto assessing which materials and technologieswill have the fewest negative consequences forwater and land resources?
What medical services do public health pro-grams in your community deliver? What is thefocus of population health campaigns?
What emergency preparedness exercises areplanned in your state? What will they test? How
CHAPTER 12
www.allhealth.org Alliance for Health Reform
COVERING HEALTH ISSUES, 2006
171
12

COVERING HEALTH ISSUES, 2006
will the outcomes be used to plan for real-worlddisasters such as a major storm?
EXPERTS AND WEBSITES
Analysts/Advocates
Alden, Errol, Executive Director, AmericanAcademy of Pediatrics, 847/228-5005
Anderson, Gerard, Director, Center for HealthFinance and Management, Johns HopkinsUniversity, 410/955-3241
Barbera , Joseph, Co-Director, Institute for Crisis,Disaster and Risk Management, GeorgeWashington University, 202/994-8424
Benjamin, Georges, Executive Director, AmericanPublic Health Association, 202/777-2742
Blewett, Lynn, Associate Professor, School ofPublic Health, University of Minnesota , 612/626-4739
Boufford, Jo Ivey, Professor of Health Policy andPublic Service, New York University, 212/998-7410
Cassel, Christine, President, American Board ofInternal Medicine, 215/446-3500
Collins, Sarah, Assistant Vice President, TheCommonwealth Fund, 212/606-3838
Epstein, Daniel, Press Officer, Pan AmericanHealth Organization, 202/974-3000
Fischer , Julie, Senior Associate, Chemical &Biological Weapons Nonproliferation, StimsonCtr, 202/223-5956
Fisher, Barbara Loe, Co-Founder and President,National Vaccine Information Center, 703/938-3783
Gostin , Lawrence, Associate Dean, Law Center,Georgetown University, 202/662-9373
Hamburg, Margaret, Senior Scientist, NuclearThreat Initiative, 202/296-4810
Heldring , Margaret, President, America'sHealthTogether, 202/966-1138
Helms, Robert, Director of Health Policy Studies,American Enterprise Institute, 202/862-5877
Hinman, Alan, Senior Public Health Scientist,Public Health Informatics Institute, 404/687-5636
Jarris, Paul, Executive Director, Association ofState and Territorial Health Officials, 202/371-9090
Koplan, Jeffrey, Vice President for AcademicHealth Affairs, Robert W. Woodruff HealthSciences Center, Emory University, 404/778-2444
Kremer, Michael, Gates Professor of DevelopingSocieties, Harvard University, 617/495-9145
Levi, Jeffrey, Executive Director, Trust forAmerica's Health, 202/223-9870
Libbey, Patrick, Executive Director, NationalAssociation of County and City Health Officials,202/783-5550
Lurie, Nicole, Director, Center for PopulationHealth and Health Disparities, RANDCorporation, 703/413-1100 x5127
Markel, Howard, Director, Center for the Historyof Medicine, University of Michigan, 734/647-6914
Marks, James, Senior Vice President, Director ofHealth Group, Robert Wood Johnson Foundation,609/627-5796
Morrison, Stephen, Executive Director, HIV/AIDSTask Force and Director, Africa Program, Centerfor Strategic and International Studies, 202/775-3276
Myers, Matt, President and CEO, Campaign forTobacco Free Kids, 202/296-5469
O'Toole, Tara, Chief Executive Officer andDirector, Center for Biosecurity, University ofPittsburgh, 443/573-3304
Osterholm, Mike, Director, Center for InfectiousDisease Research and Policy, University ofMinnesota, 612/626-6770
Rowland, Diane, Executive Vice President, KaiserFamily Foundation, 202/347-5270
Ryan, Elaine, Deputy Executive Director, NationalAssociation of State Medicaid Directors, 202/682-0100
Salinsky, Eileen, Principal Research Associate,National Health Policy Forum, 202/872-0238
Scheppach, Ray, Executive Director, NationalGovernors Association, 202/624-5300
Tallon, James, President, United Hospital Fund,212/494-0700
CHAPTER 12
Alliance for Health Reform www.allhealth.org172
12

Turnock, Bernard J., Clinical Professor,Community Health Sciences, University ofIllinois at Chicago, 312/413-0107
Wilson, Joy Johnson, Federal Affairs Counsel,National Conference of State Legislatures,202/624-5400
Government
Baylor, Norman, Director, Office of Vaccines,Food and Drug Administration, 301/827-5105
Beall, Jack, Director, National Disaster MedicalSystem, Department of Health and HumanServices, 202/646-4315
Collins, Janet, Director, National Center forChronic Disease Prevention and HealthPromotion, Centers for Disease Control andPrevention, 770/488-5401
Crosse, Marcia, Director, Health Care,Government Accountability Office, 202/512-3407
Curie, Charles, Administrator, Substance Abuseand Mental Health Services Administration,240/276-2000
Fauci, Anthony, Director, National Institute ofAllergy and Infection Diseases, National Institutesof Health, 301/496-2263
Gellin, Bruce, Director, National Vaccine ProgramOffice, Department of Health and HumanServices, 202/690-5566
Gerberding, Julie Louise, Director, Centers forDisease Control and Prevention, 404/639-7000
Lister, Sarah, Expert in Public Health andEpidemiology, Congressional Research Service,202/707-7320
Nabel, Gary, Director, Vaccine Research Center,National Institutes of Health, 301/496-1852
Phillips , Sally, Director, BioterrorismPreparedness Research , Agency for HealthcareResearch and Quality, 301/427-1571
Stakeholders
Bocchino, Carmella, Senior Vice President,Medical Affairs, America's Health InsurancePlans, 202/778-3200
Burch, Christine, Executive Director, NationalAssociation of Public Hospitals, 202/585-0100
Doyle, Arnold G., Director of Public Policy,Roche Pharmaceuticals, 973/235-5000
Gonzalez, Rose, Director, Department ofGovernment Affairs, American NursesAssociation, 301/628-5000
Marone, Barbara, Federal Affairs Director,American College of Emergency Physicians,202/728-0610 x3017
Mitchell, Alicia, Vice President, Media Relations,American Hospital Association, 202/626-2339
Smith, Rick, Senior Vice President for Policy andStrategic Communications, PhRMA, 202/835-3400
Spatz, Ian, Vice President, Public Policy, Merck &Company, Inc., 202/638-4170
Yeater, Dianne, Senior Associate for DisasterHealth Services, American Red Cross, 202/303-8613
Websites
America's HealthTogetherwww.healthtogether.org
American Academy of Pediatricswww.aap.org
American Enterprise Insititutewww.aei.org
American Public Health Associationwww.apha.org
American Red Crosswww.redcross.org
Association of State and Territorial HealthOfficialswww.astho.org
Bloomberg School of Public Health, JohnsHopkins Universitywww.jhsph.edu
Bright Futureshttp://brightfutures.aap.org/web
Campaign for Tobacco Free Kidswww.tobaccofreekids.org
CDC: Emergency Preparedness and Response www.bt.cdc.gov
Center for Biosecurity, University of Pittsburghwww.upmc-biosecurity.org
CHAPTER 12
www.allhealth.org Alliance for Health Reform
COVERING HEALTH ISSUES, 2006
173
12

Alliance for Health Reform www.allhealth.org
COVERING HEALTH ISSUES, 2006 CHAPTER 1
174
12
Center for Civilian Biodefense Studies, JohnsHopkins Universitywww.hopkins-biodefense.org
Center for Infectious Disease Research and Policy,University of Minnesotawww.cidrap.umn.edu
Center for the Law and Public's Health,Georgetown University Law Centerwww.law.georgetown.edu
Center for the Study of Bioterrorism andEmerging Infectionswww.bioterrorism.slu.edu
Centers for Disease Control and Preventionwww.cdc.gov
Chemical & Biological WeaponsNonproliferation, Stimson Ctrwww.stimson.org/cwc
Department of Health and Human Serviceswww.dhhs.gov
Federal Emergency Management Agencywww.fema.gov
George Washington University Institute for Crisis,Disaster and Risk Management www.gwu.edu/~icdrm/index.html
The Global Alliance for Vaccines andImmunizationwww.vaccinealliance.org
Government Accountability Officewww.gao.gov
Health Affairswww.healthaffairs.org
Institute of Medicinewww.iom.edu
Kaiser Family Foundation HIV/AIDS PolicyResearch, Analysis, Media, and Public HealthPartnershipswww.kff.org/hivaids/index.cfm
Nat. Institute of Allergy and Infection Diseases,NIHwww.niaid.nih.gov
Nat. Vaccine Program Office, DHHSwww.hhs.gov/nvpo
National Academy of Scienceswww.nas.edu
National Association of County and City HealthOfficialswww.naccho.org
National Association of Public Hospitalswww.naph.org
National Cancer Institute Surveillance,Epidemiology, and End Results http://seer.cancer.gov
National Center for Chronic Disease Preventionand Health Promotion www.cdc.gov/nccdphp
National Diabetes Education Program www.ndep.nih.gov
National Disaster Medical System, DHSwww.oep-ndms.dhhs.gov
National Governors Associationwww.nga.org
National Institute of Allergy and InfectiousDiseaseswww3.niaid.nih.gov
National Vaccine Information Centerwww.909shot.com
The National Vaccine Program Officewww.hhs.gov/nvpo
National Women's Health Information Centerwww.4women.gov
Office of Homeland Securitywww.whitehouse.gov/homeland
Office of the Surgeon Generalwww.surgeongeneral.gov
Pan American Health Organizationwww.paho.org
Public Health Informatics Institutewww.phii.org
Robert W. Woodruff Health Sciences Center,Emory Universitywww.whsc.emory.edu
Robert Wood Johnson Foundationwww.rwjf.org
Substance Abuse and Mental Health ServiceAdministrationwww.samhsa.gov
Trust for America's Healthwww.healthyamericans.org

www.allhealth.org Alliance for Health Reform
CHAPTER 12 COVERING HEALTH ISSUES, 2006
175
12
ENDNOTESa California Health Care Foundation (2006). “US Health Care Spending Quick Reference Guide.”
(http://www.chcf.org/documents/insurance/QuickReferenceGuide06.pdf). Retrieved on July 5, 2006.
b Dept. of Health and Human Services (2006). “FY 2007 Budget in Brief.” February.(http://www.hhs.gov/budget/07budget/overview.html). Retrieved on July 5, 2006.
c CDC (1999). “Ten Great Public Health Achievements —United States, 1900-1999.” MMWR Weekly, 48(12), April 2.(http://www.cdc.gov/mmwr/preview/mmwrhtml/00056796.htm). Retrieved on July 5, 2006.
d CDC and Dept. of Health and Human Services (2005). “Third National Report on Human Exposure to Environmental Chemicals.”July, p. 38. (http://www.cdc.gov/exposurereport/). Retrieved on July 5, 2006.
e CDC (2005). “National Diabetes Fact Sheet.” October 26. (http://www.cdc.gov/diabetes/pubs/pdf/ndfs_2005.pdf). Retrieved onJuly 5, 2006.
f Thorpe, Kenneth (2006). “What Accounts for the Rise in Health Care Spending?” PowerPoint Presentation at the 13th PrincetonConference, May 24. (http://council.brandeis.edu/pubs/Prince13/thorpe_princetonfinal5-06.pdf). Retrieved on July 7, 2006;Thorpe, Kenneth et al. (2004). “The Impact of Obesity on Rising Medical Spending.” Health Affairs, Web Exclusive W-4, October20, p. 484-485. (www.healthaffairs.org). Retrieved on July 6, 2006.
1 Dept. of Health and Human Services (1999). “Public Health in America Statement.” Public Health Functions Project, December.(http://www.health.gov/phfunctions). Retrieved on July 3, 2006.
2 Lumpkin, John R. and Margaret S. Richards (2002). “Transforming the Public Health Information Infrastructure.” Health Affairs,21(6), December, p. 45. (http://content.healthaffairs.org/cgi/reprint/21/6/45). Retrieved on July 3, 2006.
3 Dept. of Health and Human Services (2006). “Budget in Brief: Fiscal Year 2007.” February, p. 102, 104.(http://www.hhs.gov/budget/07budget/2007BudgetInBrief.pdf). Retrieved on July 5, 2006.
4 Robert Wood Johnson Foundation (2005). “2005 Annual Report: President’s Message.” p. 3.(http://www.rwjf.org/files/publications/annual/2005/RWJF_AR05_presidents_message.pdf). Retrieved on July 3, 2006.
5 California Health Care Foundation (2006). “US Health Care Spending Quick Reference Guide.”(http://www.chcf.org/documents/insurance/QuickReferenceGuide06.pdf). Retrieved on July 3, 2006.
6 Cutler, David and Grant Miller (2004). “The Role of Public Health Improvements in Health Advances: The 20th Century UnitedStates.” National Bureau of Economic Research, February.(http://post.economics.harvard.edu/faculty/dcutler/papers/cutler_miller_cities.pdf). Retrieved on July 3, 2006.
7 Schneider, Mary-Jane. Introduction to Public Health. Boston: Jones and Bartlett, 2006, p. 12-13.
8 Dept. of Health and Human Services (2000). "Healthy People 2010: Understanding and Improving Health." November, Forewordand p. 2, 4. (www.healthypeople.gov/Document/pdf/uih/2010uih.pdf) Retrieved on July 3, 2006.
9 CDC (2004). “DATA 2010…the Healthy People 2010 Database.” July. (http://wonder.cdc.gov/data2010/about.htm). Retrieved onJuly 3, 2006.
10 Dept. of Health and Human Services (2000). "Healthy People 2010: Understanding and Improving Health." November, p. 2, 16-17. (www.healthypeople.gov/Document/pdf/uih/2010uih.pdf). Retrieved on July 3, 2006).
11 Lister, Sarah A. “An Overview of the U.S. Public Health System in the Context of Emergency Preparedness.” CRS Report forCongress RL31719. March, p. 3. (http://www.fas.org/sgp/crs/homesec/RL31719.pdf). Also see Turnock, Bernard J. Public Health:What It Is and How It Works, Third Edition. Boston: Jones and Bartlett, 2004, p. 223-273.
12 National Association of County and City Officials (2001). “Local Public Health Agency Infrastructure: A Chartbook.” October, p.1. (http://archive.naccho.org/documents/chartbook.html). Retrieved on July 3, 2006.
U.S. Army Medical Research Institute ofInfectious Diseaseswww.usamriid.army.mil
U.S. Dept. of Defense; Nuclear, Biological, andChemical
www.nbc-med.org
Vaccine Research Center, NIHwww.vrc.nih.gov

Alliance for Health Reform www.allhealth.org
COVERING HEALTH ISSUES, 2006 CHAPTER 1
176
12
13 Beitsch, Leslie M. et al. (2006) “Structure and Functions of State Public Health Agencies.” American Journal of Public Health.96(1), p. 168-169. (http://www.ajph.org/cgi/content/abstract/96/1/167). Retrieved on July 3, 2006.
14 CDC. “About CDC: Our Story.” (http://www.cdc.gov/about/ourstory.htm). Retrieved on July 3, 2006.
15 Dept. of Health and Human Services (2006). “Budget in Brief: Fiscal Year 2007.” February, p. 21-22, 30, 32, 33, 41, 42.(http://www.hhs.gov/budget/07budget/2007BudgetInBrief.pdf). Retrieved on July 5, 2006; ExpectMore.gov (2006). “CDC: Stateand Local Preparedness Grants Assessment.” January. (http://www.whitehouse.gov/omb/expectmore/detail.10001052.2005.html).Retrieved on July 10, 2006.
16 CDC (2006). “Our National Partners.” National Enviornmental Public Health Tracking Program, Quarterly Tracker, 1(2), Winter.(http://www.cdc.gov/nceh/tracking/qtrack/2006_winter/partners.htm). Retrieved on July 5, 2006.
17 ASPH, ATPM and AAMC (2006). “CDC Cooperative Agreement Funding Opportunities.” (http://www.cdc-cafunding.org/).Retrieved on July 5, 2006.
18 Gebbie, Kristine (2000). “Public Health Work Force: Enumeration 2000.” Center for Health Policy, Columbia University School ofNursing, December, p. 11. (http://www.nursing.hs.columbia.edu/institutes-centers/chphsr/enum2000.pdf). Retrieved on July 3,2006; Turnock, Bernard J. Public Health: Career Choices That Make a Difference. Boston: Jones and Bartlett, 2006, p. 20.
19 Turnock, Bernard J. Public Health: Career Choices That Make a Difference. Boston: Jones and Bartlett, 2006, p. 20.
20 Turnock, Bernard J. Public Health: Career Choices That Make a Difference. Boston: Jones and Bartlett, 2006, p. 35-36.
21 California HealthCare Foundation (2006). “US Health Care Spending Quick Reference Guide.”(http://www.chcf.org/documents/insurance/QuickReferenceGuide06.pdf). Retrieved on July 3, 2006.
22 Lister, Sarah A. “An Overview of the U.S. Public Health System in the Context of Emergency Preparedness.” CRS Report forCongress RL31719. March, p. 13. (http://www.fas.org/sgp/crs/homesec/RL31719.pdf). Retrieved on July 3, 2006.
23 Schneider, Mary-Jane. Introduction to Public Health. Boston: Jones and Bartlett, 2006, p. 36-45.
24 Dept. of Health and Human Services (2006). “HHS: What We Do.” March. (http://www.hhs.gov/about/whatwedo.html/). RetrievedJuly 5, 2006.
25 Dept. of Health and Human Services (2006). “Budget in Brief: Fiscal Year 2007.” February, p. 21-22, 30, 32, 33, 41, 42.(http://www.hhs.gov/budget/07budget/2007BudgetInBrief.pdf). Retrieved on July 5, 2006.
26 Environmental Protection Agency (2006). “EPA: About EPA.” June. (http://www.epa.gov/epahome/aboutepa.htm). Retrieved onJuly 5, 2006.
27 Dept. of Agriculture (2005). “About USDA.” February.(http://www.usda.gov/wps/portal/!ut/p/_s.7_0_A/7_0_1OB?navtype=MA&navid=ABOUT_USDA). Retrieved on July 5, 2006.
28 Department of Defense (2006). “DoD 101: An Introductory Overview of the Department of Defense.” May.(http://www.defenselink.mil/pubs/dod101/dod101_for_2002.html). Retrieved on July 5, 2006.
29 Dept. of Education (2002). “An Overview of the U.S. Department of Education.” June.(http://www.ed.gov/about/overview/focus/whattoc.html?src=ln). Retrieved on July 6, 2006.
30 Dept. of Homeland Security. “Emergencies and Disasters: Preparing America.” (http://www.dhs.gov/dhspublic/theme_home2.jsp).Retrieved on July 6, 2006.
31 Dept.of Labor. "About DOL: General Information." (www.dol.gov). Retrieved on July 6, 2006.
32 Dept. of Veterans Affairs (2006). “About VA Home.” (http://www.va.gov/about_va/). May. Retrieved on July 6, 2006.
33 The Commonwealth Fund (2006). “About Us.” (http://www.cmwf.org/aboutus/aboutus.htm). Retrieved on July 7, 2006.
34 Robert Wood Johnson Foundation (2006). “Our Mission.” (http://www.rwjf.org/about/mission.jhtml). Retrieved on July 6, 2006.
35 Kaiser Family Foundation (2006). “About the Kaiser Family Foundation.” (http://www.kff.org/about/index.cfm). Retrieved on July6, 2006.
36 California Healthcare Foundation (2006). “About CHCF.” (http://www.chcf.org/aboutchcf/). Retrieved on July 6, 2006.

www.allhealth.org Alliance for Health Reform
37 Government Printing Office (2006). “Terrorism: Emergency Preparedness.” J-109-46, Hearing before the Subcommittee onTerrorism, Technology and Homeland Security of the Committee on the Judiciary, Oct. 26.(http://a257.g.akamaitech.net/7/257/2422/19jan20061300/www.access.gpo.gov/congress/senate/pdf/109hrg/25378.pdf). Retrievedon July 5, 2006.
38 Lister, Sarah A. “An Overview of the U.S. Public Health System in the Context of Emergency Preparedness.” CRS Report forCongress RL31719. March, p. 22-24, 26, 29. (http://www.fas.org/sgp/crs/homesec/RL31719.pdf). Retrieved on July 3, 2006.
39 Chertoff, Michael (2005). Letter to Governors from The NIMS Integration Center, US Department of Homeland Security. October4. (http://www.fema.gov/pdf/emergency/nims/letter_to_the_governors.pdf). Retrieved on July 3, 2006.
40 Lister, Sarah A. “An Overview of the U.S. Public Health System in the Context of Emergency Preparedness.” CRS Report forCongress RL31719. March, p. 26, 29. (http://www.fas.org/sgp/crs/homesec/RL31719.pdf). Retrieved on July 3, 2006.
41 Government Accountability Office (2005). “Information Technology: Federal Agencies Face Challenges in ImplementingInitiatives to Improve Public Health Infrastructure.” Highlights, June. (http://www.gao.gov/highlights/d05308high.pdf). Retrievedon July 3, 2006.
42 Centers for Disease Control (2006). “Overweight and Obesity: Obesity Trends: U.S. Obesity Trends 1985–2004.” March.(http://www.cdc.gov/nccdphp/dnpa/obesity/trend/maps/index.htm). Retrieved on July 1, 2006.
43 Thorpe, Kenneth (2006). “What Accounts for the Rise in Health Care Spending?” PowerPoint Presentation at the 13th PrincetonConference, May 24. (http://council.brandeis.edu/pubs/Prince13/thorpe_princetonfinal5-06.pdf). Retrieved on July 7, 2006;Thorpe, Kenneth et al. (2004). “The Impact of Obesity on Rising Medical Spending.” Health Affairs, Web Exclusive W-4, October20, p. 484-485. (www.healthaffairs.org). Retrieved on July 6, 2006.
44 National Conference of State Legislatures (2004). “Access to Healthy Food to Be New Focus of NCSL Project.” Press release,NCSL News, February 14. (http://www.ncsl.org/programs/press/2005/pr050214.htm). Retrieved on July 6, 2006.
45 CDC (2006). “Guide to Community Preventive Services: Obesity.” May. (http://www.thecommunityguide.org). Retrieved on July3, 2006.
46 NIH and CDC (2006). “National Diabetes Education Program.” February. (http://www.cdc.gov/diabetes/ndep/index.htm).Retrieved on July 3, 2006; see also: (http://www.ndep.nih.gov/).
47 National Diabetes Education Program. “NDEP Overview Brochure: Changing the Way Diabetes Is Treated.”(http://ndep.nih.gov/diabetes/pubs/NDEP_Overview_Brochure.pdf). Retrieved on July 5, 2006.
48 National Diabetes Education Program. "NDEP's Publications Catalog." (http://ndep.nih.gov/diabetes/pubs/catalog.htm) Retrievedon July 3, 2006.
49 Boyd, Donald and Victoria Wachino (2004). “Is the State Fiscal Crisis Over? A 2004 State Budget Update.” Kaiser Commissionon Medicaid and the Uninsured, January, p. 2, 7. (http://www.kff.org/medicaid/7003.cfm). Retrieved on July 3, 2006.
50 Association of State and Territorial Health Officials (2004). “State Public Health Employee Worker Shortage Report: A CivilService Recruitment and Retention Crisis.” p. 2. (http://www.astho.org/pubs/Workforce-Survey-Report-2.pdf ). Retrieved on July3, 2006.
51 Schur, Claudia L. (2004). “Rural Public Health Infrastructure” in Bridging the Health Divide: The Rural Public Health ResearchAgenda. University of Pittsburgh Center for Rural Health Practice, April, p. 9.(http://www.upb.pitt.edu/crhp/Bridging%20the%20Health%20Divide.pdf). Retrieved on July 3, 2006.
52 Association of State and Territorial Health Officials (2004). “State Public Health Employee Worker Shortage Report: A CivilService Recruitment and Retention Crisis.” p.10. (http://www.astho.org/pubs/Workforce-Survey-Report-2.pdf ). Retrieved on July3, 2006.
53 Turnock, Bernard J. Public Health: Career Choices That Make a Difference. Boston: Jones and Bartlett, 2006, p. 40, citingBureau of the Census Federal, State, and Local Governments, Public Employment and Payroll Data. Public Employment Dataavailable at www.census.gov/govs/www/apes.html
54 Association of State and Territorial Health Officials (2004). “State Public Health Employee Worker Shortage Report: A CivilService Recruitment and Retention Crisis.” p. 2. (http://www.astho.org/pubs/Workforce-Survey-Report-2.pdf ). Retrieved on July3, 2006.
55 Partnership for Public Service (2003). “Homeland Insecurity: Building the Expertise to Defend America from Bioterrorism.” July,p. 18. (http://www.ourpublicservice.org/usr_doc/Homeland_Insecurity_-Building_the_Expertise_to_Defend_America_from_Bioterrorism.pdf). Retrieved on July 3, 2006.
CHAPTER 12 COVERING HEALTH ISSUES, 2006
177
12

Alliance for Health Reform www.allhealth.org
56 Association of Schools of Public Health (2005). “2004 Annual Data Report.” June, p. 1, 6-7.(http://www.asph.org/userfiles/ADR2004.pdf). Retrieved on July 3, 2006.
57 For example, see the Public Health Foundation’s TrainingFinder Real-time Affiliate Integrated Network (TRAIN) at www.train.org.
58 Council on Linkages between Academia and Public Health Practice (2001). “Core Competencies Without Skill Levels.” April.(http://www.trainingfinder.org/competencies/list_nolevels.htm). Retrieved on July 3, 2006.
59 National Committee on Vital and Health Statistics (2001) “A National Agenda for Public Health Informatics.” June.(http://www.ncvhs.hhs.gov/010627p3.pdf). Retrieved on July 3, 2006.
60 American Health Information Management Association (2006). “Building the Work Force for Health Information Transformation.”p. 3. (http://www.ahima.org/emerging_issues/Workforce_web.pdf). Retrieved on July 5, 2006.
61 American Medical Informatics Association (2006). “AMIA 10x10: 10,000 Trained by 2010.” July. (http://www.amia.org/10x10).Retrieved on July 5, 2006.
62 Jones, Jennifer (2005). “Shock to the System: Katrina Highlights Holes in Emergency Health Care System.” Government HealthIT, December 5. (http://www.govhealthit.com/article91600-12-05-05-Print). Retrieved on July 5, 2006.
63 Baker, ML (2005). “Electronic Health Data Helping Katrina Victims.” Ziff Davis CIO Insight. September 15.(http://www.cioinsight.com/article2/0,1540,1859142,00.asp). Retrieved on July 5, 2006.
64 Ferris, Nancy (2005). “health IT to Help with Care for Katrina Victims.” Government Health IT, September 9.(http://www.govhealthit.com/article90700-09-09-05-Web). Retrieved on July 5, 2006; Broder, Caroline (2005). “Effort Under Wayto Provide Medication Data on Katrina Evacuees.” Healthcare IT News, September 16.(http://www.healthcareitnews.com/printStory.cms?id=3662). Retrieved on July 1, 2006.
65 Dept. of Health and Human Services (2005). “HHS Enters Into Agreements to Support Digital Health Recovery for the Gulf Coast:Partnerships Will Accelerate Electronic Health Records in Gulf States.” Press release, November 17.(http://www.hhs.gov/news/press/2005pres/20051117.html). Retrieved on July 5, 2006.
66 California HealthCare Foundation (2005). “Care Delivery: Health Officials Seek to Expand RHIOs.” iHealthBeat, June 10.(http://www.ihealthbeat.org/index.cfm?Action=dspItem&itemID=112023). Retrieved on July 5, 2006; Robinson, Bryan (2005).“RHIO Resistance: CIOs Are Slow to Enlist in Regional Health Info Organizations Pending More Progress on Local Systems,Finances.” Government Health IT, November 14. (http://www.govhealthit.com/article91429). Retrieved on July 5, 2006.
67 Robert Wood Johnson Foundation (2005). “Public Health Agencies to Explore Use of Information Technology to Improve Health.”Press Release, December 14. (http://www.rwjf.org/newsroom/newsreleasesdetail.jsp?id=10386). Retrieved on July 5, 2006.
68 Powner, David A. (2006). “Health Information Technology: HHS Is Continuing Efforts to Define a National Strategy.” Testimonybefore the Subcommittee on Federal Workforce and Agency Organization, Committee on Government Reform, House ofRepresentatives. Government Accountability Office, March 15, p. 7-8, 11-12. (http://www.gao.gov/new.items/d06346t.pdf).Retrieved on July 5, 2006; Access Intelligence, LLC (2006). “DHS Plans Award Soon for National Biosurveillance Info System.”Defense Daily’s TR2: Terror Response Technology Report, May 17, p. 1.(http://www.investorideas.com/Companies/WDT/Media/TR2_0517.pdf). Retrieved on July 10, 2006.
69 Association of State and Territorial Health Officials (2005). “Public Health, Health Care and Health Information Technology: ANew Opportunity for Public Health Agencies.” Public Health Informatics Update, July.(http://www.astho.org/pubs/healthinformationtechnologyupdateJuly2005.pdf). Retrieved on July 5, 2006.
70 Connecting for Health (2005). “Linking Health Care Information: Proposed Methods for Improving Care and Protecting Privacy.”February, p. 1, 4. (http://www.connectingforhealth.org/assets/reports/linking_report_2_2005.pdf). Retrieved on July 6, 2006.
71 Environmental Protection Agency (2006). “Response to 2005 Hurricanes: Sampling of Residual Sediment in Flood ImpactedAreas.” June. (http://www.epa.gov/katrina/testresults/sediments/residual_zip.html). Retrieved on July 6, 2006.
72 PBS (2005). “Environmental Impact of Katrina.” Online News Hour with Jim Lehrer, November 8.(http://www.pbs.org/newshour/bb/science/july-dec05/neworleans_11-08.html). Retrieved on July 5, 2006.
73 CDC and Dept. of Health and Human Services (2005). “Third National Report on Human Exposure to Environmental Chemicals.”July, p. 38. (http://www.cdc.gov/exposurereport/). Retrieved on July 5, 2006.
74 CDC and Dept. of Health and Human Services (2005). “Third National Report on Human Exposure to Environmental Chemicals.”July, p. 40. (http://www.cdc.gov/exposurereport/). Retrieved on July 5, 2006.
75 Wikipedia (2006). “Precautionary Principle.” June. (http://en.wikipedia.org/wiki/Precautionary_principle). Retrieved on July 5,2006.
COVERING HEALTH ISSUES, 2006 CHAPTER 1
178
12

www.allhealth.org Alliance for Health Reform
76 Maryland Department of the Environment (2002-2006). “National Institutes of Health.”(www.mde.state.md.us/BusinessInfoCenter/PollutionPrevention/P2/profiles/nih.asp). Retrieved on July 5, 2006.
77 Rauber, Chris. “Bay Area Companies Join Forces to Phase Out PVC Plastics.” East Bay Business Times, December 7.(http://www.bizjournals.com/eastbay/stories/2005/12/05/daily25.html). Retrieved on July 5, 2006.
78 Environmental Protection Agency (2006). “Toxics Release Inventory (TRI) Program.” June. (http://www.epa.gov/tri/). RetrievedJuly 5, 2006.
79 Government Accountability Office (2006). “Homeland Security: DHS Is Taking Steps to Enhance Security at Chemical Facilities,but Additional Authority is Needed.” GAO-06-150, January, p.22. (http://www.gao.gov/new.items/d06150.pdf). Retrieved on July5, 2006.
80 New York Times (2006). “Worse Than Nothing.” Editorial, June 14.(http://select.nytimes.com/gst/abstract.html?res=F60C1FF638550C778DDDAF0894DE404482). Retrieved on July 5, 2006.
81 Turnock, Bernard J. Public Health: What It Is and How It Works, Third Edition. Boston: Jones and Bartlett, 2004, p. 275.
82 Dept. of Health and Human Services (2006). “Budget in Brief: Fiscal Year 2007.” February, p. 104.(http://www.hhs.gov/budget/07budget/2007BudgetInBrief.pdf). Retrieved on July 5, 2006.
CHAPTER 12 COVERING HEALTH ISSUES, 2006
179
12
Alliance for Health Reform www.allhealth.org
COVERING HEALTH ISSUES, 2006 CHAPTER 1
180
12