Embed Size (px)
Citation preview

COVID-19The one we prepared for?
John Jay Shannon, MD
AMITA Health COVID Consortium
July 28, 2020

Disclosure
I have no financial or academic conflict of interest related to the subject being presented. The opinions are mine alone, and do not represent those of any of the departments or agencies of the State of Illinois.

Objectives
• Overview of the pandemic time course and IL experience with COVID-19
• Share reflections from 4 months of intense immersion
• Raise awareness of governmental players in pandemic response

Crimson Contagion
“The outbreak of the respiratory virus began in China and was quickly spread around the world by air travelers, who ran high fevers. In the United States, it was first detected in Chicago, and 47 days later, the World Health Organization declared a pandemic. By then it was too late: 110 million Americans were expected to become ill, leading to 7.7 million hospitalized and 586,000 dead.
That scenario, code-named “Crimson Contagion” and imagining an influenza pandemic, was simulated by the Trump administration’s Department of Health and Human Services in a series of exercises that ran from last January to August (2019).
The simulation’s sobering results — contained in a draft report dated October 2019 that has not previously been reported — drove home just how underfunded, underprepared and uncoordinated the federal government would be for a life-or-death battle with a virus for which no treatment existed……”
David E. Sanger, Eric Lipton, Eileen Sullivan and Michael Crowley. New York Times March 19, 2020

The course thus far: USA leads in world impact
https://coronavirus.jhu.edu/data/cumulative-cases; accessed July 28, 2020

New cases: rolling 7-day averages
https://coronavirus.jhu.edu/data/new-cases; accessed July 28, 2020

Summary of Tests, Cases, and Deaths-IL
URL: http://dph.illinois.gov/covid19/covid19-statistics

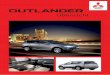
SARS CoV-2 positive test results this year: Illinois
1 2 0 0 0 1 3 81
937
3302
6651
9404 9539
13078
1737316749 16523
15689
10384
7499
50414447
4831
3347
0
2000
4000
6000
8000
10000
12000
14000
16000
18000
20000
Nu
mb
er o
f C
ases
COVID 19 Cases by Reporting Week
Source: IDPH Data team

9 |
Data shows cases increasing in all regions
Data from July 14 2020IDPH public

The shame and catastrophe of health inequities illustrated by COVID-19
• See Dr. Hill’s AMITA analysis of this subject, last consortium
• What are the forces driving these trends• Crowded housing/challenges with isolation and quarantine
• Reliance on public transportation
• Lack of paid time off inhibits a recommendation to quarantine
• Higher proportion of chronic disorders that drive risk for severe disease, driven by structural racism

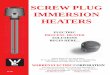
Demographics of CasesIL Census data: W 77%, AA 15%, Latinx 18%
URL: http://dph.illinois.gov/covid19/covid19-statistics

Trend in Numbers of Deaths

Demographics of DeathsIL Census data: W 77%, AA 15%, Latinx 18%
URL: http://dph.illinois.gov/covid19/covid19-statistics

Overall (all-cause) Mortality in IL, through June 2020• Significantly higher than in 2018 and 2019
• COVID a significant but not the only driver
• Analysis needed to explicate • Preventable and treatable
• Deaths of despair
• Deaths by violence

Long term care facilities
• >1000 of various types licensed in the state
• Difficult financial models-another Tale of Two Worlds
• Often understaffed, bigger challenges with • Resources
• Intellectual (e.g., infection prevention)
• supplies including personal protective equipment, testing
• Space and strategies for large-scale isolation
• Residents account for ~55% of COVID-related deaths in IL

Correctional health-the “other” congregate living


Outbreak of COVID-19 and Interventions in One of the Largest Jails in the United States: Cook County, IL, 2020Chad Zawitz, Sharon Welbel, Isaac Ghinai, Connie Mennella,Rebecca Levin, Usha Samala, Michelle Bryant Smith, Jane Gubser, Bridgette Jones, Kate Varela, Uzay Kirbiyik,Josh Rafinski, Anne Fitzgerald, Peter Orris, Alex Bahls, Stephanie R Black, Alison M Binder, Paige A Armstrongdoi: https://doi.org/10.1101/2020.07.12.20148494
Posted July 14, 2020.

My “folders” since March 21, 2020
Acute care hospitals Restore Illinois
Alternate Care Facilities Clinical trajectory/dispositions
Long-term care facilities Data
Correctional health Elective surgery
Clinical Homeless
Remdesivir IDPH
Ventilators IEMA
Reimbursement/licensure EMS
Illinois Hospital Association MetroSouth
McCormick Place Crisis Standards of Care
Visitation Face coverings/masks
and there are more…….

What the heck is an Alternate Care Facility?
• Specifically designed for catastrophes: weather, pandemic, etc.
• Sites for care when the existing healthcare system cannot meet need, whatever the reason
• IL ACF strategy driven by early assessments by IEMA, based on pandemic modeling and gap analysis

Forecasting models-Based on empiric observations/lived data-rough projections for resource planning-e.g., IHME
Mechanistic models-Based on simulations based on presumed effects of transmissions and mitigation-constrained by knowledge of virus and public health dynamics-rough projections for resource planning
Homdahl I, Buckee C. DOI:10.1056/NEJMp2016822

Mechanistic models informing Governor Pritzker-Argonne National Laboratory (focus on Chicago)-Northwestern University-University of Chicago-University of Illinois at Urbana Champaign
“The most timely information we have (case number, positivity rates) is the least reliable while the most reliable data (hospitalizations, deaths)is the least timely .”
Await less biased or confounded data sources, e.g., sentinel surveillance

Health system “surge”: we should all be proud, Illinoisans grateful

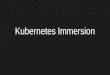
Hospital Resources – Med/Surg Beds

Hospital Resources – ICU

Hospital Resources
URL: http://dph.illinois.gov/covid19/hospitalization-utilization

Clinical trajectory
Illinois (~6000 pts, through May 2020)
• Discharged home independent 50-55%
• Discharged home, need assistance 10-15%
• Discharged to skilled nursing 10-15%
• Died 12-15%
CDC (data through 06/29/20)
• Proportion admitted to ICU 24-36%
• Proportion of admits that die 2-28%
• ALOS (without ICU) ~5 days
• ALOS (with ICU) ~14 days


The LNO is the receiving unit's expert on the sending organization's capabilities and limitations.
The LNO advises the receiving headquarters commander and staff on the optimum employment of the sending organization's capabilities.

Who does what in a pandemic and how is it organized? I
• Federal: President of the United States• Health and Human Services
• Centers for Disease Control and Prevention• Office of the Assistant Secretary for Preparedness and Response (ASPR)• Centers for Medicare and Medicaid Services
• Homeland Security• Federal Emergency Management Agency
• State: Governor of Illinois• Emergency Management Agency (IEMA)• Department of Public Health (IDPH)
• 97 local health departments• 11 Emergency Management Regions, with 61 Medical Directors
• Healthcare and Family Services (IL HFS)

The power of the feds
July 23, 2020
_____________________________
Date
/s/
_____________________________
Alex M. Azar II
Renewal of Determination That A Public Health Emergency ExistsAs a result of the continued consequences of Coronavirus Disease 2019 (COVID-19) pandemic, on this date and after consultation with public health officials as necessary, I, Alex M. Azar II, Secretary of Health and Human Services, pursuant to the authority vested in me under section 319 of the Public Health Service Act, do hereby rene

Who does what in a pandemic and how is it organized? II
• Relationship of IDPH with Regional health ecosystem• Regulatory oversight
• “Guidance”
• Light hand with actual clinical coordination
• Limited insight into health system operations
• Responsibility (uniquely from the systems and hospitals themselves) to preserve surge capacity

Lumpers vs. splitters: we have a map for every need

Restore Illinois-4 consolidated regions Illinois Regional COVID-19 Resurgence Criteria
May 5, 2020 June 15, 2020
Resurgence criteria (from Phase 4 back to Phase 3)
-test positivity rate-admits with COVID-like illness-med/surg bed availability-ICU bed availability


Why We’re Losing the Battle With Covid-19*
“Hospital beds were filling up, hospital floors reconfigured and surge units readied. Doctors and nurses, in Harris County (TX) …. have begun a worrying and familiar census-taking of ventilators and personal protective equipment. And the same stories that played out in Wuhan and Lombardy and Seattle and New York were beginning anew. …..(t)he root of this catastrophe, doctors, scientists and health historians say, is our failure to fully incorporate public health into our understanding of what it means to be a functioning society. Until we do that, we will be unable to effectively respond to crises like this one — let alone prevent them.”
Jeneen InterlandiNew York Times MagazineJuly 14, 2020
*article title

Lessons I am still learning
• Heavy the head that wears the crown.
• We are a country of GDIs.
• We need to pay more attention to public health:• Fund it AND• Recognize that tabletops are not “exercises in fantasy”.
• “Space, staff, smarts, stuff”-we need to be acting more like regional ecosystems-including small hospitals to referral hospitals, long-term care facilities, and correctional health in one soup
• We may need to rethink reliance on J-I-T and a global economy in this particular dimension of the economy
• Humility (e.g., as a pulmonologist who thought he knew what masks do and do not do)
• Gratitude for the dedication and resilience of front-line caregivers

Thanks and happy to answer questions