Embed Size (px)
Citation preview

Ches
t cl
inic
COVID-19 vaccine- related interstitial lung disease: a case studyJi Young Park ,1 Joo- Hee Kim ,1 In Jae Lee,2 Hwan Il Kim,1 Sunghoon Park,1 Yong Il Hwang,1 Seung Hun Jang,1 Ki- Suck Jung1
Case based discussion
To cite: Park JY, Kim J- H, Lee IJ, et al. Thorax Epub ahead of print: [please include Day Month Year]. doi:10.1136/thoraxjnl-2021-217609
1Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang, South Korea2Department of Radiology, Hallym University College of Medicine, Anyang, South Korea
Correspondence toDr Ji Young Park, Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Hallym University Sacred Heart Hospital, Hallym University College of Medicine, Anyang 14068, South Korea; evan007@ naver. com
Received 14 May 2021Accepted 11 July 2021
© Author(s) (or their employer(s)) 2021. No commercial re- use. See rights and permissions. Published by BMJ.
DR JI YOUNG PARKHerd immunity through extensive and rapid vaccina-tion rather than natural immunity acquired by infec-tion is necessary to control a global pandemic like COVID-19. The development of COVID-19 vaccines has been accelerated through government funding and the collaborative efforts of the medical–scien-tific institutions and the pharmaceutical industry.1 2 In South Korea, the ChAdOx1 nCoV-19 (Oxford/AstraZeneca) and BNT162b2 (Pfizer/BioNTech) vaccines have received emergency approval and are being used. Although the safety and efficacy of these vaccines were established through interim analysis in global clinical trials, long- term data and reports of rare adverse reactions remain inadequate.1 2 We report a case of interstitial lung disease (ILD) after COVID-19 vaccination and review the literature on influenza vaccine- related ILDs. This review is favour-able as influenza vaccines are widely administered annually among the elderly, and several vaccine- related ILDs have been reported.
DR HWAN IL KIMIn early April 2021, an 86- year- old man presented to the emergency department with a 1- day history of weakness, dyspnoea and fever. He had no cough, expectoration, nasal discharge or sore throat. One day before symptom onset, he had received a COVID-19 mRNA vaccine. He had hypertension, diabetes and chronic renal disease, which were well controlled with medications (atorvastatin, amlodipine, furo-semide, linagliptin, metformin and clopidogrel). He was a non- smoker with no history of cardiovas-cular, pulmonary, allergic or connective tissue disease (CTD). He took an influenza vaccine annually with no adverse events and had no history of adverse events with other vaccines or drugs. He denied any recent changes in his living environment and expo-sure to chemicals or organic particles. On admission, his body temperature was 38.2°C, and peripheral oxygen saturation was 80% on room air. He had no rash, oedema or clubbing, but bilateral crackles were found on auscultation. The partial pressure of oxygen in arterial blood (PaO2)/fraction of inspired oxygen ratio (FiO2) was maintained at 248 (50% FiO2; PaO2, 124.2 mm Hg; PaCO2, 21.2 mm Hg) with high- flow nasal cannula oxygen therapy. An electrocardiograph showed sinus tachycardia without ST changes. Blood investigations revealed the following: haemoglobin, 136 g/L; white cell count, 11.60×109/L (neutrophils, 82.8%; eosinophils, 4.1%; lymphocytes, 5.8%); platelets, 340×109/L; International Normalized Ratio (INR), 1.04; D- dimer, 0.55 µg/mL; blood urea nitrogen, 22.7 mg/dL; creatinine, 1.85 mg/dL;
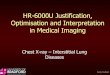
aspartate aminotransferase, 18 IU/L; and alanine aminotransferase, 11 IU/L. Chest radiograph revealed bilateral reticular opacities. Empirical antibiotics were administered for 3 days considering a diagnosis of pneumonia; however, the symptoms and chest radiograph findings worsened. Chest CT revealed bilateral diffuse ground- glass opacities (GGO) with focal consolidations, centrilobular micronodules and interlobular septal thickening (figure 1A,B). The C reactive protein level increased to 11.43 mg/dL. The brain natriuretic peptide level (88 pg/mL) was within the reference range, and serum procalcitonin (0.32 ng/mL) was slightly elevated.
DR SUNGHOON PARKThe results of COVID-19 PCR testing (Real- Q 2019- nCoV Detection kit; BioSewoom, Seoul, Korea) of nasopharyngeal swabs and sputum samples were negative, initially and after 3 days. Test results of the induced sputum samples were negative for other pathogens (seasonal respiratory virus multiplex PCR testing (Real- Q RV Detection kit, BioSewoom), bacterial culture, acid–fast bacillus smear, tubercu-losis PCR testing and respiratory bacterial multiplex PCR testing (Allplex PneumoBacter Assay; Seegene, Seoul, Korea)). He was seronegative for rheuma-toid factor and anticitrullinated peptide, antineutro-phil cytoplasmic, antinuclear, anti- dsDNA, anti- Sm, anti- U1RNP, anti- Scl-70, anti- Ro and anti- La anti-bodies. IgE, IgG, IgA and IgM concentrations were within the normal range, and 62 allergen- specific IgE antibodies using AdvanSure AlloScreen (LG Life Science, Seoul, Korea) were negative. Broncho-scopic bronchoalveolar lavage and lung biopsy could not be performed because of the patient’s refusal. COVID-19 vaccine- related ILD was diagnosed based on the clinical course, radiological features and labo-ratory results. We discontinued antibiotic therapy and initiated intravenous methylprednisolone at 1 mg/kg/day. His symptoms and chest radiography findings rapidly improved the following day. After 3 days, the steroid dose was reduced. Thirteen days later, he was discharged. Subsequently, the steroid dose was gradually tapered and discontinued with no relapse. The onset was acute after vaccination, and the clin-ical course was transient with rapid improvement by steroid treatment.
A SARS- CoV-2 serological antibody test performed 16 days after vaccination showed that both IgM and IgG were negative (STANDARD Q COVID-19 IgM/IgG Plus Test; SD Biosensor, Korea). The test was conducted to reconfirm whether the patient had a previously undiagnosed COVID-19 before vaccination and to rule out the hypothesis that a
1Park JY, et al. Thorax 2021;0:1–3. doi:10.1136/thoraxjnl-2021-217609
on Novem
ber 13, 2021 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thoraxjnl-2021-217609 on 6 August 2021. D
ownloaded from

Ches
t cl
inic
Case based discussion
past SARS- CoV-2 infection may have elicited a robust antibody response after vaccination. Moreover, high- dose steroids might prevent adequate antibody formation after vaccination. However, to date, there are no commercial antibody tests approved for the evaluation of immunity following COVID-19 vaccinations, including the tests we conducted.
DR YONG IL HWANGDrug- induced interstitial lung disease (DILD) has a wide spectrum of clinical presentation, from transient lung infiltration to acute respiratory distress syndrome, and is a diagnosis of exclusion. The ‘identification’ and ‘singularity’ criteria proposed by Camus et al3 were met, because other than the routine medications for hyper-tension and diabetes, COVID-19 mRNA vaccine was the only drug administered before the onset of ILD. The ‘temporal eligibility’ criteria were met as the patient had no respiratory symptoms or fever, and ILD with severe hypoxia occurred on the day after
vaccination. The rechallenge test is necessary only when no alter-native treatment is available; therefore, the patient was advised not to take the second dose of the vaccine. Lastly, the ‘exclusion of other conditions’ criterion was met as infections and CTDs were ruled out based on the radiological findings and microbiolog-ical and serological test results. Bronchoalveolar lavage and lung biopsy were not performed. However, their results are usually non- specific for the diagnosis of DILD.
DR SEUNG HUN JANG AND DR IN JAE LEEWe found 10 published case reports of influenza vaccine- associated ILD.4–12 The clinical characteristics of influenza vaccine- related ILD cases were similar to those of the current case in the following respects (figure 1c). Symptom onset was acute and occurred at a median of 2 days after vaccination, and fever appeared in most patients. In all cases where chest CT findings can be referred to, bilateral distribution and GGO were confirmed. All patients
Figure 1 (A) Clinical course and chest radiography findings of a patient with COVID-19 vaccine- related ILD. (B) Chest CT images obtained at 4 days (A) and 18 days after COVID-19 vaccination. (C) Data of 10 previously reported cases of influenza vaccine- related ILD. *One case each of chronic hypersensitive pneumonitis and idiopathic pulmonary fibrosis. #1, Johnston et al5; #2, Heinrichs et al6; #3, Kanemitsu et al7; #4, Bhurayanontachai8; #5, Umeda et al9; #6, Kumamoto et al10; #7, Watanabe et al11; #8, Hibino and Kondo12; #9, Hibino and Kondo12; #10, Numata et al.4 BAL, bronchoalveolar lavage; ED, emergency department; FiO2, fraction of inspired oxygen; HFNC, high- flow nasal cannula; ILD, interstitial lung disease; MPD, methylprednisolone; n, no; y, yes.
2 Park JY, et al. Thorax 2021;0:1–3. doi:10.1136/thoraxjnl-2021-217609
on Novem
ber 13, 2021 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thoraxjnl-2021-217609 on 6 August 2021. D
ownloaded from

Ches
t cl
inic
Case based discussion
recovered, and most responded well to steroid therapy. Interest-ingly, 8 of 10 patients were Asian, underlying ILD in two cases. Although publication bias is a significant limitation, these might be risk factors for influenza vaccine- related ILD. There was a vaccine safety committee’s report of acute deterioration of underlying ILD after influenza vaccinations from the Japanese Ministry of Health, Labour and Welfare (19 cases from 22.8 million doses of H1N1 vaccine in 2009–2010, Japan).9 However, the evaluation of risk factors for adverse reactions should be analysed through prospec-tive studies that can proactively evaluate every vaccinated indi-vidual and not through case series or reports from passive safety surveillance. Moreover, for rare adverse reactions and delayed- onset events, large healthcare databases with standardised defini-tions and appropriate statistic models are necessary (active safety surveillance).
Between 14 December 2020 and 6 June 2021, 905.89 million people received at least one dose of the COVID-19 vaccine world-wide.13 We reviewed the WHO global pharmacovigilance database (through VigiAccess, summary statistics from VigiBase) to iden-tify individual cases of suspected COVID-19 vaccine- related ILD. Eighty- four cases of ILD (single diagnosis code) had been reported until 6 June 2021. Additional cases of COVID-19 vaccine- related adverse events registered included 135 cases of pneumonitis, 88 of acute respiratory distress syndrome, 9 of pulmonary alveolar haemorrhage, 9 of organising pneumonia, 6 of hypersensitivity pneumonitis, 4 of alveolitis, 2 of eosinophilic pneumonia and 1 case each of acute interstitial pneumonitis, immune- mediated lung disease and pulmonary vasculitis. However, a significant limitation of this database is that the information came from various sources, and the causal relationship between a suspected adverse effect and the drug is inconsistent.
DR JOO-HEE KIMVarious candidate vaccines against COVID-19, such as inactivated vaccines, viral vector vaccines, nucleic acid (DNA or mRNA- based) vaccines and protein subunit vaccines, are in different stages of development and clinical trials. Two mRNA- based vaccines being used worldwide under an emergency authorisation, BNT162b2 and mRNA-1273 (Moderna), showed 95% and 94.1% efficacy, respectively, in the primary analysis of phase II/III trials.1 2 Both vaccines showed similar reactogenicity profiles. The most common local reaction was pain at the injection site (BNT162b2, 71%; mRNA-1273, 74% among older participants after the first dose), which resolved within 2–3 days. Redness and swelling at the injec-tion site were infrequent (approximately 6%). Systemic reactions were more common in young individuals and after the second dose than the first dose. With both vaccines, fatigue was reported by approximately one- third of the elderly subjects after the first dose. Fever occurred in 16% and 17.4% of young individuals after the second dose of the BNT162b2 and mRNA-1273, respectively. The rate of treatment- related serious adverse events was 0.02% (4/21621) and 0.04% (6/15181) with BNT162b2 and mRNA-1273, respectively. No vaccine- related ILD was reported in either clinical trial.1 2
DR KI-SUCK JUNG AND DR JI YOUNG PARKThe safety of the mRNA- based vaccines currently in use has been confirmed through phase II/III trials. However, extremely rare or late- onset adverse events might be identified only after the vaccine has been widely administered to the general population. After the national vaccination programme, anaphylaxis and thrombotic events have been reported, although further analysis is necessary
to determine their relevance.14 15 In countries such as South Korea, where vaccine availability is limited, elderly subjects are being prioritised for vaccination after healthcare workers. However, older adults usually have pre- existing comorbidities and are less tolerable of adverse events. A comprehensive review with a long- term follow- up about the safety of COVID-19 vaccines in older adults is lacking. This report suggests that healthcare professionals monitoring the adverse events should be vigilant for COVID-19 vaccine- related ILD, for a prompt diagnosis and timely treatment. Although vaccine- related ILD should be listed as an adverse reac-tion of the COVID-19 vaccine, we emphasise that the risk:benefit ratio remains firmly in favour of vaccination.
Acknowledgements We have described data retrieved from VigiBase, which collects data from various sources, and the degree of association between a certain drug and reported adverse event might vary, depending on the case. Our report does not represent the opinion of the Uppsala Monitoring Centre or the WHO.
Contributors JYP, HIK and SP treated the patient and collected the data for the manuscript. IL reviewed the radiology of the case. J- HK, YIH and SHJ contributed to analysis and interpretation. JYP and KJ oversaw the conception, writing, formatting and editing. All authors reviewed and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not- for- profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non- commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
ORCID iDsJi Young Park http:// orcid. org/ 0000- 0002- 6533- 4656Joo- Hee Kim http:// orcid. org/ 0000- 0002- 1572- 5149
REFERENCES 1 Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT162b2 mRNA
Covid-19 vaccine. N Engl J Med 2020;383:2603–15. 2 Baden LR, El Sahly HM, Essink B, et al. Efficacy and safety of the mRNA-1273 SARS-
CoV-2 vaccine. N Engl J Med 2021;384:403–16. 3 Camus P, Fanton A, Bonniaud P, et al. Interstitial lung disease induced by drugs and
radiation. Respiration 2004;71:301–26. 4 Numata T, Hida N, Yazaki K, et al. Seasonal influenza vaccine- induced pneumonitis
presenting with multiple pulmonary nodules. Intern Med 2018;57:707–11. 5 Johnston SD, Kempston A, Robinson TJ. Pneumonitis secondary to the influenza
vaccine. Postgrad Med J 1998;74:541–2. 6 Heinrichs D, Sennekamp J, Kirsten A, et al. Allergische alveolitis nACh
Grippeschutzimpfung. Pneumologie 2009;63:508–11. 7 Kanemitsu Y, Kita H, Fuseya Y, et al. [Interstitial pneumonitis caused by seasonal
influenza vaccine]. Nihon Kokyuki Gakkai Zasshi 2010;48:739–42. 8 Bhurayanontachai R. Possible life- threatening adverse reaction to monovalent H1N1
vaccine. Crit Care 2010;14:422. 9 Umeda Y, Morikawa M, Anzai M, et al. Acute exacerbation of idiopathic pulmonary
fibrosis after pandemic influenza A (H1N1) vaccination. Intern Med 2010;49:2333–6. 10 Kumamoto T, Mitsuyama H, Hamasaki T. [Case report; Drug induced lung injury caused
by 2009 pandemic H1N1 vaccine]. Nihon Naika Gakkai Zasshi 2011;100:3034–7. 11 Watanabe S, Waseda Y, Takato H, et al. Influenza vaccine- induced interstitial lung
disease. Eur Respir J 2013;41:474–7. 12 Hibino M, Kondo T. Interstitial pneumonia associated with the influenza vaccine: a
report of two cases. Intern Med 2017;56:197–201. 13 Our World In Data. Coronavirus (COVID-19) vaccinations, 2021. Available: https://
ourworldindata. org/ covid- vaccinations 14 Smadja DM, Yue Q- Y, Chocron R, et al. Vaccination against COVID-19: insight from
arterial and venous thrombosis occurrence using data from VigiBase. Eur Respir J 2021;58. doi:10.1183/13993003.00956-2021. [Epub ahead of print: 01 Jul 2021].
15 Gee J, Marquez P, Su J, et al. First month of COVID-19 vaccine safety monitoring - United States, December 14, 2020- January 13, 2021. MMWR Morb Mortal Wkly Rep 2021;70:283–8.
3Park JY, et al. Thorax 2021;0:1–3. doi:10.1136/thoraxjnl-2021-217609
on Novem
ber 13, 2021 by guest. Protected by copyright.
http://thorax.bmj.com
/T
horax: first published as 10.1136/thoraxjnl-2021-217609 on 6 August 2021. D
ownloaded from