Embed Size (px)
Citation preview

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 1/24
1
I. PATIENT STATUS
PATIENT IDENTITY
Initial Name : Mrs. D
Sex : Female
Age : 48 years old
Nationally : Indonesia (Javanese)
Marital Status : Married
Religion : Islam
Occupation : Housewife
Educational Background : Elementary School
Address : Talang padang, Tanggamus
ANAMNESIS
Taken from : Autoanamnesis
Date : May 29th, 2014
Time : 14.00
Chief Complain : Shortness of breath since 2 month ago
Additional Complaint : The patient felt abdominal bloating and hard, liquid bowel movements
since 2 months ago, cough with phlegm, thrush, tongue dirty.
History of The Present Illness :
Patients present with shortness of breath since 2 months ago and became heavier since 1 week
ago. Patients complain of difficulty breathing while being crowded. Patients feel better when
you're in a sitting position or by using a high pillow. Shortness of breath arise every day and
compounded with moderate activity. Patients complain when it is relapse can reach 1-2 hours.
The patient also complained of cough with phlegm since 2 months ago. The patient admitted that
he had been undergoing treatment at the general hospital Pringsewu for 1 week. But in reference

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 2/24
2
to Abdul Moeloek Bandar Hospital. Patients also complain of poor appetite since 6 months ago.
Patients admitted to having obtained an ultrasound examination of the abdomen and liver
irritation.
The History of Illness :
(-) Small pox (-) Malaria (-) Kidney stone
(-) Chicken pox (-) Disentri (-) Hernia
(-) Difthery (+) Hepatitis (-) Prostat
(-) Pertusis (-) TifusAbdominalis (-) Melena
(-) Measles (-) Skirofula (+) Diabetic
(+) Influenza (-) Siphilis (-) Alergy
(-) Tonsilitis (-) Gonore (-) T u m o r
(-) Kholera (-) Hipertension. (-) Vaskular Disease
(-) Acute Rheumatoid Fever (-) Ventrikuli Ulcer (-) Operation(-) Pneumonia (-) Duodeni Ulcer
(-) Pleuritic (-) Gastritis
Family’s diseases History :
Patient didn’t know about his Family’s Disease History
Is there any family who suffer :
Patient said that one of the family members of the patient's husband has been sick TB and has
been dead several years ago
SYSTEM ANAMNESE
Note of Positive Complaints beside the title
Skin
(-) Boil (-) Hair (-) Night sweat
(-) Nail (-) Yellow /Werus (-) Cyanotic
(-) Others
Head
(-) Trauma (+) Headache
(-) Syncope (-) Pain of the sinus

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 3/24
3
Ear
(-) Pain (-) Tinitus
(-) Secret (-) Ear disorders
(-) Deafness
Nose
(-) Trauma (-) Clogging
(-) Pain (-) Nose disorders
(-) Sekret (-) common cold
(-) Epistaksis
Mouth
(-) Lip (+) Dirty Tongue
(-) Gums (-) Mouth disorders
(-) Membrane (+) Stomatitis
Throat
(+) Throat Pain (-) Voice Change
Neck
(-) Protruding (-) Neck Pain
Cor/ Lung
(+) Chest pain (+) Dyspneu
(-) Pulse (-) Hemoptoe
(-) Ortopneu (+) Cough
Abdomen (Gaster/ Intestine)
(-) Puffing (+) Acites
(-) Nausea (-) Hemoroid(-) Emesis (+) Diarrhea
(-) Hematemesis (-) Melena
(-) Disfagi (-) Pale colour of feses
(-) Colic (-) Black colour of feses
(-) Nodul

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 4/24
4
Urogenital
(-) Dysuria (-) Pyuria
(-) Stranguria (-) Kolik
(-) Polyuria (-) Oliguria
(-) Polakysuria (-) Anuria(-) Hematuria (-) Urine retention
(-) Kidney stone (-) Drip urine
(-) Wet the bed (-) Prostat
Katamenis
(-) Leukorhoe (-) Bleeding
(-) Other
Muscle and Neuron
(-) Anestesi (-) Hard to bite
(-) Parestesi (-) Ataksia
(-) Weak muscle (-) Hipo/hiper-estesi
(-) Afasia (-) Tick
(-) Amnesis (-) Vertigo
(-) Others (-) Disartri
(-) Convultion (-) Syncope
Extremities
(+) Edema (-) Deformitas
(-) Hinge pain (-) Cyanotic
Weight
Average weight (kg) : 50kg
Height (cm) : 155cm
Present Weight : 44kg
(if the patient doesn’t know certainly)
(-) steady
(+) down
(-) up

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 5/24
5
THE HISTORY OF LIFE
Birth place
(+) in home (-) matrinity (-) matrinity hospital
Helped by:
(+) Traditional matrinity (-) Doctor (-) Nurse (-) Others
Imunitation History (Unknown)
(-) Hepatitis (-) BCG (-) Campak (-) DPT (-) Polio Tetanus
Food History
Frequency/day : 3x/day
Amount/day : 1 place/eat (health)
Variation/day : Rice, vegetables, fish
Appetite : Decrease
Educational
(+) SD (-) SMP (-) SMA (-)SMK (-) Course Academy
Problem
Financial : low
Works : -
Family : normal
Others : -
Body Check Up
General Check Up
Height : 144 cm
Weight : 42 kg
Blood Pressure : 100/60 mmHg

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 6/24
6
Pulse : 104 x/minute
Temperature : 36,10C
Breath (Frequence&type) : 28 x/minute
Nutrition Condition : Normal,
Consciousness : Compos Mentis
Cyanotic : (-)
General Edema : pitting oedem
The way of walk : normal
Mobility : Passive
The age predicyion based on check up : 45 years old
Mentality Aspects
Behavior : Normal
Nature of Feeling : Normal
The thinking of process : Normal
Skin
Color : Olive
Keloid : (-)
Pigmentasi : (-)
Hair Growth : Normal
Arteries : Touchable
Touch temperature : Afrebris
Humid/dry : Dry
Sweat : Normal
Turgor : Normal
Icterus : Icteric
Fat Layers : Enough
Efloresensi : (-)
Edema : (+)
Others : (-)

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 7/24
7
Lymphatic Gland
Submandibula : no enlargement
Neck : no enlargement
Supraclavicula : no enlargement
Armpit : no enlargement
Head
Face Expression : Normal
Face Symmetric : Symmetric
Hair : Black
Temporal artery : Normal
Eye
Exopthalmus : (-)
Enopthalmus : (-)
Palpebra : edema (-)/(-)
Lens : Clear/Clear
Conjunctiva : Anemis +/+
Visus : Normal
Sklera : Icteric +/+
Ear
Deafnes : (-)
Foramen : (-)
Membrane tymphani : intact
Obstruction : (-)
Serumen : (-)
Bleeding : (-)
Liquid : (-)

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 8/24
8
Mouth
Lip : (-)
Tonsil : (-)
Palatal : Normal
Halibsts : No
Teeth : (-)
Trismus : (-)
Farings : Unhiperemis
Liquid Layers : (-)
Tongue : Dirty
Neck
JVP : Normal
Tiroid Gland : no enlargement
Limfe Gland : no enlargement
Chest
Shape : Simetric
Artery : Normal
Breast : Normal
Lung
Inspection : Left : simetric, no lession, normochest
Right : simetric, no lession, normochest
Palpation : Left : vokal fremitus decreased, pain (-)
Right : vokal fremitus decreased, pain (-)
Percussion : Left : flatness
Right : flatness
Auscultation : Left : vesiculer decrease, wheezing expiration (-), ronkhi (+)
Right : vesiculer decrease, wheezing expiration (-), ronkhi (+)

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 9/24
9
Cor
Inspection : Ictus cordis not visible
Palpation : Ictus Cordis no palpable
Percussion : difficult to essess
Auscultation : Heart Sound 1 & 2 Regular
Artery
Temporalic artery : No aberration
Caritic artery : No aberration
Brachial artery : No aberration
Radial artery : No aberration
Femoral artery : No aberration
Poplitea artery : No aberration
Posterior tibialis artery : No aberration
Stomach
Inspection : convex
Palpation : Stomach Wall : undulation (-), pain (+)
Heart : Hepatomegali (+)
Limfe : Splenomegali (+)
Kidney : Ballotement (-)
Percussion : Shifting Dullness (+)
Auscultation : Intestine Sounds (+)
Genital (no indication)
Movement Joint
Arm Right Left
Muscle Normal Normal
Tones Normal Normal
Mass Normal Normal

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 10/24
10
Joint Normal Normal
Movement Normal Normal
Strength Normal Normal
Heel and Leg
Wound/injury : not found
Varices : (-)
Muscle (tones&mass) : Normal
Joint : Normal
Movement : Normal
Strength/Power : Normal
Edema : (+) (pitting edema)
Others : (-)
Reflexs
Right Left
Tendon Reflex Normal Normal
Bisep Normal Normal
Trisep Normal Normal
Pattela Normal Normal
Achiles Normal Normal
Cremaster Normal Normal
Skin Reflex Normal Normal
Patologic Reflex Not Found Not Found
Laboratory
Routine Blood
- Hb : 7,0 gr/dl
- Leukosit : 19400/ mikroliter
- LED : 110 mm/jam

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 11/24
11
- Trombosit : 316.000
- Diff. Count
o Basofil : 0%
o Eosinofil : 2%
o Stem : 0%
o Segment : 86%
o Limfosit : 6%
o Monosit : 6%
USG
Impression : Hepatomegaly, according hepatoma picture
Ascites and bilateral pleural effusion
Ren, spleen, bladder and uterus normal
Resume
Patient came to hospital and told
Patients present with shortness of breath since 2 months ago and became heavier since 1 week
ago. Patients complain of difficulty breathing while doing activity. Patients feel better when in a
sitting position or by using a high pillow. Shortness of breath arise every day and compounded
with moderate activity. Patients complain when it is relapse can reach 1-2 hours. The patient also
complained of cough with sputum since 2 months ago. Patients also complain of poor appetite
since 6 months ago. Patients admitted to having obtained an ultrasound examination of the
abdomen and liver irritation. Ultrasound examination : Hepatomegaly, according hepatoma
picture, ascites and bilateral pleural effusion, dan ren, spleen, bladder and uterus normal.
Radiology chest X-Ray : meniscus sign that blunts the costophrenic angle on the PA projection.
Working Diagnose
- PE with Hepatoma
Basic Diagnose
Anamnesis

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 12/24
12
- shortness of breath Smoking history
Physics Examination
- flatness percussion
- Rhonki (+)
Support Radiology
- Chest X-Ray : meniscus sign that blunts the costophrenic angle on the PA projection
Ultrasound
- Hepatomegaly, according hepatoma picture, ascites and bilateral pleural effusion
Differential Diagnose
- TB
-
Cor abnormality
Basic Differential Diagnose
Anamnesis
- Shortness of breath
- Recurrent Dyspneu
- Chough with sputum
- Member of family has been diagnosed TB
Physics Examination
- Symetrics
- Flatness percussion
- Rhonki (+)
Support Examination
- Chest X ray : meniscus sign that blunts the costophrenic angle
Support Check Up
- Laboratory
o Ureum Creatinin
o Electrolite
o GDS

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 13/24
13
o Lipid Profile
o Uric Acid
o Albumin
- Rivalta test
- Sitology
Treatment Plan
(1) General Treatment
- Bed Rest
- Nutrition (high calory, high protein)
(2) Special Treatment
-
Medicamentosa
o IVFD RL : D5 gtt X/minute
o Cetirizin ½ tab 2x1
o Ranitidin 2x1 amp
o Ciprofloxacine 200mg/12 jam
o Dexamethasone 3x1 amp
o Curcuma 3x1 tab
o Antasid tab 3x1
- Non Medicamentosa
o Therapeutic thoracentesis
o Activity adjustment
o Go to doctor immedietly if appear any symptoms
Prognose
Quo ad Vitam : Dubia ad bonam
Quo ad Functonam : Dubia
Quo ad Sanationam : Dubia ad malam

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 14/24
14
II. REFERENCE
A. Definition
Pleural effusion means the collection of large amounts of free fluid in the pleural space.The
effusion is analogous to edema fluid in the tissues and can be called “edema of the pleural
cavity.” The causes of the effusion are the same as the causes of edema in other tissues,
including (1) blockage of lymphatic drainage from the pleural cavity; (2) cardiac failure, which
causes excessively high peripheral and pulmonary capillary pressures, leading to excessive
transudation of fluid into the pleural cavity (3) greatly reduced plasma colloid osmotic pressure,
thus allowing excessive transudation of fluid; and (4) infection or any other cause of
inflammation of the surfaces of the pleural cavity, which breaks down the capillary membranes
and allows rapid dumping of both plasma proteins and fluid into the cavity.
The pleural space lies between the lung and the chest wall and normally contains a very thin
layer of fluid, which serves as a coupling system. A pleural effusion is present when there is an
excess quantity of fluid in the pleural space. Pleural effusions seen in patients with increased
pulmonary venous pressure represent another reservoir for edema fluid, one that may
compromise respiratory function less than would having the same fluid in the lung parenchyma.
B.
Etiology
Pleural fluid accumulates when pleural fluid formation exceeds pleural fluid absorption.
Normally, fluid enters the pleural space from the capillaries in the parietal pleura and is removed
via the lymphatics in the parietal pleura. Fluid also can enter the pleural space from the
interstitial spaces of the lung via the visceral pleura or from the peritoneal cavity via small holes
in the diaphragm. The lymphatics have the capacity to absorb 20 times more fluid than is formed
normally. Accordingly, a pleural effusion may develop when there is excess pleural fluid
formation (from the interstitial spaces of the lung, the parietal pleura, or the peritoneal cavity) or
when there is decreased fluid removal by the lymphatics.

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 15/24
15
C. Radiological Investigations
Most pleural effusions are detected on plain chest radiography, although lateral (and specifically
lateral decubitus) radiographs increase sensitivity. About 200 ml of pleural fluid must be present
before any change is evident on the plain posteroanterior (PA) chest radiograph. The classical
appearance of pleural effusion is easily recognised. However, loculated fluid may appear
atypically and encysted fluid within the lung fissure may give the appearance of an
intraparenchymal mass.
D. Pleural fluid diagnostic tests
When a patient is found to have a pleural effusion, an effort should be made to determine the
cause. The first step is to determine whether the effusion is a transudate or an exudate. A
transudative pleural effusion occurs when systemic factors that influence the formation and
absorption of pleural fluid are altered. The leading causes of transudative pleural effusions in the
United States are left-ventricular failure and cirrhosis. An exudative pleural effusion occurs
when local factors that influence the formation and absorption of pleural fluid are altered. The
leading causes of exudative pleural effusions are bacterial pneumonia, malignancy, viral
infection, and pulmonary embolism. The primary reason for making this differentiation is that
additional diagnostic procedures are indicated with exudative effusions to define the cause of the
local disease. Transudative and exudative pleural effusions are distinguished by measuring the
lactate dehydrogenase (LDH) and protein levels in the pleural fluid. Exudative pleural effusions
meet at least one ofthe following criteria, whereas transudative pleural effusions meet none:
1. Pleural fluid protein/serum protein >0.5
2. Pleural fluid LDH/serum LDH >0.6
3. Pleural fluid LDH more than two-thirds normal upper limit for serum
These criteria misidentify ~25% of transudates as exudates. If one or more of the exudative
criteria are met and the patient is clinically thought to have a condition producing a transudative
effusion, the difference between the protein levels in the serum and the pleural fluid should be
measured. If this gradient is >31 g/L (3.1 g/dL), the exudative categorization by these criteria can
be ignored because almost all such patients have a transudative pleural effusion. If a patient has
an exudative pleural effusion, the following testson the pleural fluid should be obtained:

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 16/24
16
description of the appearance of the fluid, glucose level, differential cell count, microbiologic
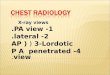
studies, and cytology.
Figure 1 Approach to the diagnosis of pleural effusions. CHF, congestive heart failure; CT, computedtomography; LDH, lactate dehydrogenase;PE, pulmonary embolism; TB, tuberculosis; PF, pleural fluid.
E. Differential Diagnoses of Pleural Effusions
Transudative Pleural Ef fusions
1. Congestive heart failure
2. Cirrhosis
3. Pulmonary embolization
4. Nephrotic syndrome
5. Peritoneal dialysis
6. Superior vena cava obstruction
7. Myxedema
8. Urinothorax

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 17/24
17
Exudative Pleural Ef fusions
1. Neoplastic diseases
a. Metastatic disease
b. Mesothelioma
2. Infectious diseases
a. Bacterial infections
b. Tuberculosis
c. Fungal infections
d. Viral infections
e. Parasitic infections
3. Pulmonary embolization
4. Gastrointestinal disease
a. Esophageal perforation
b. Pancreatic disease
c. Intraabdominal abscesses
d. Diaphragmatic hernia
e. After abdominal surgery
f. Endoscopic variceal sclerotherapy
g. After liver transplant
5. Collagen vascular diseases
a. Rheumatoid pleuritis
b. Systemic lupus erythematosus
c. Drug-induced lupus
d. Immunoblastic lymphadenopathy
e. Sjögren’s syndrome
f. Granulomatosis with polyangiitis
(Wegener’s)
g. Churg-Strauss syndrome
6. Post-coronary artery bypass surgery
7. Asbestos exposure
8. Sarcoidosis
9. Uremia
10. Meigs’ syndrome
11. Yellow nail syndrome
12. Drug-induced pleural disease
a. Nitrofurantoin
b. Dantrolene
c. Methysergide
d. Bromocriptine
e. Procarbazine
f. Amiodarone
g. Dasatinib
13. Trapped lung
14. Radiation therapy
15. Post-cardiac injury syndrome
16. Hemothorax
17. Iatrogenic injury
18. Ovarian hyperstimulation syndrome
19. Pericardial disease
20. Chylothorax

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 18/24
18
1. Effusion due to heart failure
The most common cause of pleural effusion is left-ventricular failure. The effusion occurs
because the increased amounts of fluid in the lung interstitial spaces exit in part across the
visceral pleura; this overwhelms the capacity of the lymphatics in the parietal pleura to
remove fluid. In patients with heart failure, a diagnostic thoracentesis should be performed
if the effusions are not bilateral and comparable in size, if the patient is febrile, or if the
patient has pleuritic chest pain to verify that the patient has a transudative effusion.
Otherwise the patient’s heart failure is treated. If the effusion persists despite therapy, a
diagnostic thoracentesis should be performed. A pleural fluid N-terminal pro-brain
natriuretic peptide (NT-proBNP) >1500 pg/mL is virtually diagnostic of an effusion
secondary to congestive heart failure.
2. Hepatic hydrothorax
Pleural effusions occur in ~5% of patients with cirrhosis and ascites. The predominant
mechanism is the direct movement of peritoneal fluid through small openings in the
diaphragm into the pleural space. The effusion is usually right-sided and frequently is
large enough to produce severe dyspnea.
3. Parapneumonic effusion
Parapneumonic effusions are associated with bacterial pneumonia, lung abscess, or
bronchiectasis and are probably the most common cause of exudative pleural effusion in
the United States. Empyema refers to a grossly purulent effusion. Patients with aerobic
bacterial pneumonia and pleural effusion present with an acute febrile illness consisting of
chest pain, sputum production, and leukocytosis. Patients with anaerobic infections present
with a subacute illness with weight loss, a brisk leukocytosis, mild anemia, and a history
of some factor that predisposes them to aspiration. The possibility of a parapneumonic
effusion should be considered whenever a patient with bacterial pneumonia is initially
evaluated. The presence of free pleural fluid can be demonstrated with a lateral decubitus
radiograph, computed tomography (CT) of the chest, or ultrasound. If the free fluid
separates the lung from the chest wall by >10 mm, a therapeutic thoracentesis should be
performed. Factors indicating the likely need for a procedure more invasive than a
thoracentesis (in increasing order of importance) include the following:
Loculated pleural fluid

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 19/24
19
Pleural fluid pH <7.20
Pleural fluid glucose <3.3 mmol/L (<60 mg/dL)
Positive Gram stain or culture of the pleural fluid
Presence of gross pus in the pleural space
If the fluid recurs after the initial therapeutic thoracentesis and if any of these
characteristics are present, a repeat thoracentesis should be performed. If the fluid cannot
be completely removed with the therapeutic thoracentesis, consideration should be given
to inserting a chest tube and instilling a fibrinolytic agent (e.g., tissue plasminogen
activator, 10 mg) or performing a thoracoscopy with the breakdown of adhesions.
Decortication should be considered when these measures are ineffective.
4. Effusion secondary to malignancy
Malignant pleural effusions secondary to metastatic disease are the second most common
type of exudative pleural effusion. The three tumors that cause ~75% of all malignant
pleural effusions are lung carcinoma, breast carcinoma, and lymphoma. Most patients
complain of dyspnea, which is frequently out of proportion to the size of the effusion. The
pleural fluid is an exudate, and its glucose level may be reduced if the tumor burden in the
pleural space is high. The diagnosis usually is made via cytology of the pleural fluid. If the
initial cytologic examination is negative, thoracoscopy is the best next procedure if
malignancy is strongly suspected. At the time of thoracoscopy, a procedure such as pleural
abrasion should be performed to effect a pleurodesis. An alternative to thoracoscopy is
CT- or ultrasound-guided needle biopsy of pleural thickening or nodules. Patients with a
malignant pleural effusion are treated symptomatically for the most part, since the
presence of the effusion indicates disseminated disease and most malignancies associated
with pleural effusion are not curable with chemotherapy. The only symptom that can be
attributed to the effusion itself is dyspnea. If the patient’s lifestyle is compromised by
dyspnea and if the dyspnea is relieved with a therapeutic thoracentesis, one of the
following procedures should be considered: (1) insertion of a small indwelling catheter or
(2) tube thoracostomy with the instillation of a sclerosing agent such as doxycycline, 500
mg.

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 20/24
20
5. Mesothelioma
Malignant mesotheliomas are primary tumors that arise from the mesothelial cells that line
the pleural cavities; most are related to asbestos exposure. Patients with mesothelioma
present with chest pain and shortness of breath. The chest radiograph reveals a pleural
effusion, generalized pleural thickening, and a shrunken hemithorax. Thoracoscopy or
open pleural biopsy is usually necessary to establish the diagnosis. Chest pain should be
treated with opiates, and shortness of breath with oxygen and/or opiates.
6. Effusion secondary to pulmonary embolization
The diagnosis most commonly overlooked in the differential diagnosis of a patient with an
undiagnosed pleural effusion is pulmonary embolism. Dyspnea is the most common
symptom. The pleural fluid is almost always an exudate. The diagnosis is established by
spiral CT scan or pulmonary arteriography. Treatment of a patient with a pleural effusion
secondary to pulmonary embolism is the same as it is for any patient with pulmonary
emboli. If the pleural effusion increases in size after anticoagulation, the patient probably
has recurrent emboli or another complication, such as a hemothorax or a pleural infection.
7. Tuberculous pleuritis
In many parts of the world, the most common cause of an exudative pleural effusion is
tuberculosis (TB). Tuberculous pleural effusions usually are associated with primary TB
and are thought to be due primarily to a hypersensitivity reaction to tuberculous protein in
the pleural space. Patients with tuberculous pleuritis present with fever, weight loss,
dyspnea, and/or pleuritic chest pain. The pleural fluid is an exudate with predominantly
small lymphocytes. The diagnosis is established by demonstrating high levels of TB
markers in the pleural fluid (adenosine deaminase >40 IU/L or interferon γ >140 pg/mL).
Alternatively, the diagnosis can be established by culture of the pleural fluid, needle
biopsy of the pleura, or thoracoscopy. The recommended treatments of pleural and
pulmonary TB are identical.
8. Effusion secondary to viral infection
Viral infections are probably responsible for a sizable percentage of undiagnosed
exudative pleural effusions. In many series, no diagnosis is established for ~20% of
exudative effusions, and these effusions resolve spontaneously with no long-term residua.
The importance of these effusions is that one should not be too aggressive in trying to

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 21/24
21
establish a diagnosis for the undiagnosed effusion, particularly if the patient is improving
clinically.
9. Chylothorax
A chylothorax occurs when the thoracic duct is disrupted and chyle accumulates in the
pleural space. The most common cause of chylothorax is trauma (most frequently thoracic
surgery), but it also may result from tumors in the mediastinum. Patients with chylothorax
present with dyspnea, and a large pleural effusion is present on the chest radiograph.
Thoracentesis reveals milky fluid, and biochemical analysis reveals a triglyceride level
that exceeds 1.2 mmol/L (110 mg/dL). Patients with chylothorax and no obvious trauma
should have a lymphangiogram and a mediastinal CT scan to assess the mediastinum for
lymph nodes. The treatment of choice for most chylothoraxes is insertion of a chest tube
plus the administration of octreotide. If these modalities fail, a pleuroperitoneal shunt
should be placed unless the patient has chylous ascites. An alternative treatment is ligation
of the thoracic duct. Patients with chylothoraxes should not undergo prolonged tube
thoracostomy with chest tube drainage because this will lead to malnutrition and
immunologic incompetence.
10.
Hemothorax
When a diagnostic thoracentesis reveals bloody pleural fluid, a hematocrit should be
obtained on the pleural fluid. If the hematocrit is more than one-half of that in the
peripheral blood, the patient is considered to have a hemothorax. Most hemothoraxes are
the result of trauma; other causes include rupture of a blood vessel or tumor. Most
patients with hemothorax should be treated with tube thoracostomy, which allows
continuous quantification of bleeding. If the bleeding emanates from a laceration of the
pleura, apposition of the two pleural surfaces is likely to stop the bleeding. If the pleural
hemorrhage exceeds 200 mL/h, consideration should be given to thoracoscopy or
thoracotomy.
11. Miscellaneous causes of pleural effusion.
There are many other causes of pleural effusion. Key features of some of these conditions
are as follows: If the pleural fluid amylase level is elevated, the diagnosis of esophageal
rupture or pancreatic disease is likely. If the patient is febrile, has predominantly
polymorphonuclear cells in the pleural fluid, and has no pulmonary parenchymal

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 22/24
22
abnormalities, an intraabdominal abscess should be considered. The diagnosis of an
asbestos pleural effusion is one of exclusion. Benign ovarian tumors can produce ascites
and a pleural effusion (Meigs’ syndrome), as can the ovarian hyperstimulation syndrome.
Several drugs can cause pleural effusion; the associated fluid is usually eosinophilic.
Pleural effusions commonly occur after coronary artery bypass surgery. Effusions
occurring within the first weeks are typically left-sided and bloody, with large numbers of
eosinophils, and respond to one or two therapeutic thoracenteses. Effusions occurring
after the first few weeks are typically left-sided and clear yellow, with predominantly
small lymphocytes, and tend to recur. Other medical manipulations that induce pleural
effusions include abdominal surgery; radiation therapy; liver, lung, or heart
transplantation; and the intravascular insertion of central lines.
F. Therapy
1. Medicamentosa
Pharmacologic management of pleural effusion depends on the condition’s etiology. For
example, medical management includes nitrates and diuretics for congestive heart failure
and pulmonary edema, antibiotics for parapneumonic effusion and empyema, and
anticoagulation for pulmonary embolism. In patients with parapneumonic effusions,
empyemas, and effusions associated with esophageal perforation and intra-abdominal
abscesses, antibiotics should be administered early when these conditions are suspected.
Antibiotic selection should be based on the suspected causative microorganisms and the
overall clinical picture. Considerations include the patient's age, comorbidities, duration of
the illness, setting (community vs nursing home), and local organism sensitivities. Various
effective single agents and combination antimicrobial therapies exist. Coverage should
generally include anaerobic organisms. Options may include clindamycin, extended-
spectrum penicillins, and imipenem. Depending on the patient's clinical condition,
infectious disease consultation may be appropriate. Particular attention must be given to
potential drug interactions, adverse effects, and preexisting conditions.
2. Therapeutic Thoracentesis
Therapeutic thoracentesis to remove larger amounts of pleural fluid is used to alleviate
dyspnea and to prevent ongoing inflammation and fibrosis in parapneumonic effusions. In

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 23/24
23
addition to the precautions listed previously for diagnostic thoracentesis, note 3 additional
considerations when performing therapeutic thoracentesis.
First, to avoid producing a pneumothorax during the removal of large quantities of fluid,
remove fluid during therapeutic thoracentesis with a catheter, rather than with a sharp
needle, introduced into the pleural space. Various specially designed thoracentesis trays
are available for introducing small catheters into the pleural space. Alternatively, newer
systems using spring-loaded, blunt-tip needles that avoid lung puncture are also available.
Second, monitor oxygenation closely during and after thoracentesis because arterial
oxygen tension paradoxically might worsen after pleural fluid drainage due to shifts in
perfusion and ventilation in the reexpanding lung. Consider use of empiric supplementaloxygen during the procedure.
Third, remove only moderate amounts of pleural fluid to avoid reexpansion pulmonary
edema and to avoid causing a pneumothorax. Removal of 400-500 mL of pleural fluid is
often sufficient to alleviate shortness of breath. The recommended limit is 1000-1500 mL
in a single thoracentesis procedure.
3. Tube Thoracostomy
Although small, freely flowing parapneumonic effusions can be drained by therapeutic
thoracentesis, most larger effusions and complicated parapneumonic effusions or
empyemas require drainage by tube thoracostomy.
Traditionally, large-bore chest tubes (20-36F) have been used to drain thick pleural fluid
and to break up loculations in empyemas. However, such tubes are not always well
tolerated by patients and are difficult to direct correctly into the pleural space. However,
small-bore tubes (7-14F) inserted at the bedside or under radiographic guidance have been
shown to provide adequate drainage, even when empyema is present. These tubes cause
less discomfort and are more likely to be placed successfully within a pocket of pleural
fluid. Using 20-cm water suction and flushing the tube with normal saline every 6-8 hours
may prevent occlusion of small-bore catheters.

8/10/2019 CR Pleural Effusion Ec Hepatoma
http://slidepdf.com/reader/full/cr-pleural-effusion-ec-hepatoma 24/24