Embed Size (px)
Citation preview
Hospital & Physician Reimbursement Guide for ICD ImplantsJuly 2016
CRHF ECONOMICS & HEALTH POLICY
Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 1/22
HOSPITAL & PHYSICIAN REIMBURSEMENT GUIDE FOR ICD IMPLANTSThis guide has been developed to help you understand Medicare coverage and payment for implantable cardioverter defibrillator (ICD) and cardiac resynchronization therapy with implantable cardioverter defibrillator (CRT-D).
These coding suggestions and coverage guidelines do not replace seeking coding advice from the payer and/or your coding staff. The ultimate responsibility for correct coding lies with the provider of services. Please contact your local payer for interpretation of the appropriate codes to use for specific procedures. Medtronic makes no guarantee that the use of this information will prevent differences of opinion or disputes with Medicare or other third party payers as to the correct form of billing or the amount that will be paid to providers of service.
Table of ContentsOverview . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2
Coverage for ICD Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4
Coding for ICD Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
Inpatient Hospital MS-DRGs for ICD Therapy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Medicare Implant Registry . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Frequently Asked Questions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20
CPT copyright 2015 American Medical Association. All rights reserved. CPT is a registered trademark of the American Medical Association. Applicable FARS/DFARS restrictions apply to government use. Fee schedules, relative value units, conversion factors and/or related components are not assigned by the AMA, are not part of CPT, and the AMA is not recommending their use. The AMA does not directly or indirectly practice medicine or dispense medical services. The AMA assumes no liability for the data contained or not contained herein.
2/22Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Overview
OVERVIEWThe implantable automatic defibrillator is an electronic device designed to detect and treat life-threatening tachyarrhythmias. The device consists of a pulse generator and electrodes for sensing and defibrillating. When the device senses an arrhythmia, it sends an electrical signal through the leads to terminate the arrhythmia and restore normal heart rhythm.
On January 27, 2005 Medicare expanded their covered indications which resulted in the addition of two different patient classifications, Primary Prevention and Secondary Prevention.
Secondary PreventionICDs are used for “secondary prevention” in individuals with known arrhythmias and also in those who have survived an episode of sudden cardiac arrest.
The history of Medicare coverage for implantable automatic defibrillators1:
§ January 24, 1986: Coverage to treat life-threatening ventricular tachyarrhythmias.
§ July 1, 1999: Expanded coverage for additional types of cardiac patients.
§ October 1, 2003: Expanded coverage for patients with a documented prior myocardial infarction (MI).
§ January 27, 2005: Expanded coverage based on the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT)
Primary PreventionICDs are also used for “primary prevention” for individuals who have a high risk of life-threatening arrhythmias due to a variety of risk factors.
MADIT-II and SCD-HeFT PatientsMADIT-II and SCD-HeFT were two clinical trials that studied the impact of ICD therapy on specific patient populations. Both trials demonstrated decreased risk of death from sudden cardiac arrest for patients who receive an ICD. MADIT-II patients have survived a previous myocardial infarction (MI) and have impairment of the left ventricle, but no prior history of an arrhythmia. MADIT-II and SCD-HeFT patient populations overlap. The SCD-HeFT population is broader, for example, a prior MI is a MADIT-II indication, but may or may not be present in a SCD-HeFT patient. Both populations may include abnormalities in QRS duration.
Patient Population Summary
MADIT-II SCD-HeFTPrior MI Ischemic or nonischemic cardiomyopathy
Ejection Fraction ≤ 30% NYHA Class II or III
Ejection Fraction ≤ 35%
Overview
3/22 Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Overview
Medicare ICD RegistryWith the expanded coverage in 2005, Medicare also introduced the requirement of an ICD registry to collect information about primary prevention patients. An implant registry is currently maintained by the American College of Cardiology’s National Cardiovascular Data Registry (ACC-NCDR®). Hospitals must enter Primary prevention patient data in the registry as a condition for Medicare coverage, with some exceptions. Hospitals may choose to enter all of their ICD and CRT-D patients into the registry. The existence of the ACC-NCDR registry, which was launched on April 3, 2006, subsequently expanded Medicare coverage to patients diagnosed with:§ Nonischemic dilated cardiomyopathy (NIDCM) > 3 months and < 9 months, and§ NYHA Class II or III heart failure, and§ Measured LVEF ≤ 35% if they participated in the ACC-NCDR ICD registry
For further clarification, visit the Medicare website: https://www.cms.gov/Medicare/Medicare-General-Information/MedicareApprovedFacilitie/ICDregistry.html or visit the National Cardiovascular Data Registry website: http://ncdr.com.
Q0
In the above paragraph CMS (Medicare) requires both Hospital Outpatient and Physician claims to indicate that the patient data has been entered into the Registry by appending the Q0 modifier to the implant procedure code. The definition of the Q0 modifier is: Investigational clinical service provided in a clinical research study that is in an approved clinical research study.
As discussed on Page 2, Primary Prevention patients have indications under MADIT-II and SCD-HeFT, which should be reflected by diagnosis codes on the claim. The claim should reflect the primary prevention diagnosis code that supports primary prevention and must include the Q0 modifier with the implant CPT code; this is applicable for Hospital Outpatient and Physician claims.
Additional Medicare Implant Registry information is available on page 19.
Cardiac Resynchronization Therapy with DefibrillatorCardiac resynchronization therapy with defibrillator (CRT-D) combines the benefits of defibrillation with synchronous biventricular pacing capabilities. CRT-D is used in individuals who qualify for an ICD and who also have indications for CRT.
Medicare does not have a national coverage determination specifically for CRT-D therapy. As CRT-D combines the benefits of defibrillation with synchronous biventricular pacing capabilities, it is important that the patient first and foremost meets the national coverage indications for an ICD. To determine if the biventricular pacing capabilities are warranted, the current indications for biventricular pacing and supporting literature should be considered. Please contact your local payer’s medical director for more specific information regarding the coverage policies for your area.
4/22Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coverage for ICD Therapy
COVERAGE FOR ICD THERAPY
Medicare CoverageThe Medicare coverage policy for ICD implants occurring on or after January 27, 2005 is printed verbatim; however, it is reformatted for easier readability. Note that in this policy, coverage has been extended to the SCD-HeFT2 population.
The Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT),2 a landmark clinical trial in heart failure (HF) and cardiology, compares the efficacy of implantable cardioverter defibrillators (ICDs), amiodarone, and placebo in treating 2,521 patients with an ejection fraction of 35% or lower and NYHA Functional Class II or III symptoms. Patients within NYHA Class II have symptoms with ordinary exertion, while NYHA Class III patients have symptoms with less than normal exertion. The National Institutes of Health’s National Heart, Lung, and Blood Institute conducted the SCD-HeFT clinical study as an independent trial, with funding from Medtronic, Inc. and Wyeth Ayerst. The study found that ICDs provided a 23% relative reduction in all-cause mortality as compared to the placebo. This mortality benefit was observed in patients who were already optimally managed on drug therapy. Amiodarone had no significant effect on all-cause mortality. Patients with SCD-HeFT indications have not experienced a sudden cardiac arrest (SCA), and hence their treatment with ICD therapy is considered to be a “primary prevention” measure.
The Multicenter Automatic Defibrillator Implantation Trial II (MADIT-II)3 studied the benefit of ICD therapy in patients with a prior myocardial infarction (MI), a left ventricular ejection fraction (LVEF) of 30% or lower, and who were in NYHA Functional Class I, II, or III at the time of enrollment. NYHA Class I patients have symptoms with greater than normal exertion. The study demonstrated a 31% relative reduction in mortality in patients who had ICDs, compared to those in the optimized medical therapy group.
Medicare Coverage Policy20.4 IMPLANTABLE AUTOMATIC DEFIBRILLATORS, Medicare National Coverage Determinations Manual (Chapter 1, Part I (Sections 10-80.12) Coverage Determinations)*
A. General The implantable automatic defibrillator is an electronic device designed to detect and treat life-threatening tachyarrhythmias. The device consists of a pulse generator and electrodes for sensing and defibrillating.
B. Covered Indications 1. Documented episode of cardiac arrest due to ventricular fibrillation (VF), not due to a transient
or reversible cause (effective July 1, 1991).
2. Documented sustained ventricular tachyarrhythmia (VT), either spontaneous or induced by an electrophysiology (EP) study, not associated with an acute myocardial infarction (MI) and not due to a transient or reversible cause (effective July 1, 1999).
3. Documented familial or inherited conditions with a high risk of life-threatening VT, such as Long QT syndrome or hypertrophic cardiomyopathy (effective July 1, 1999).
Additional indications effective for services performed on or after October 1, 2003: 4. Coronary artery disease with a documented prior MI, a measured left ventricular ejection fraction (LVEF)
≤ 0.35, and inducible, sustained VT or VF at EP study. (The MI must have occurred more than 40 days prior to defibrillator insertion. The EP test must be performed more than 4 weeks after the qualifying MI.)
5. Documented prior MI and a measured LVEF ≤ 0.30 and a QRS duration of > 120 milliseconds (the QRS
* The coverage policy is available at http://www.cms.gov/medicare-coverage-database/details/ncd-details.aspx?NCDId=110&ncdver=3&IsPopup=y&NCAId=102&NcaName=Implantable+Defibrillators+-+Clinical+Trials&bc=AAAAAAAAIAAA&.
Coverage for IC
D
Therapy
5/22 Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coverage for ICD Therapy
restriction does not apply to services performed on or after January 27, 2005). Patients must not have: a. New York Heart Association (NYHA) Classification IV; b. Cardiogenic shock or symptomatic hypotension while in a stable baseline rhythm; c. Had a coronary artery bypass graft (CABG) or percutaneous transluminal coronary angioplasty (PTCA)
within past 3 months; d. Had an enzyme positive MI within past month (Effective for services on or after January 27, 2005, patients
must not have an acute MI in the past 40 days); e. Clinical symptoms or findings that would make them a candidate for coronary revascularization; or f. Any disease, other than cardiac disease (e.g., cancer, uremia, liver failure), associated with a likelihood of
survival less than 1 year.
Additional indications effective for services performed on or after January 27, 2005:
6. Patients with ischemic dilated cardiomyopathy (IDCM), documented prior MI, NYHA Class II and III heart failure, and measured LVEF ≤ 35%;
7. Patients with nonischemic dilated cardiomyopathy (NIDCM) > 9 months, NYHA Class II and III heart failure, and measured LVEF ≤ 35%;
8. Patients who meet all current Centers for Medicare & Medicaid Services (CMS) coverage requirements for a cardiac resynchronization therapy (CRT) device and have NYHA Class IV heart failure;
All indications must meet the following criteria: a. Patients must not have irreversible brain damage from preexisting cerebral disease; b. MIs must be documented and defined according to the consensus document of the Joint European
Society of Cardiology/American College of Cardiology Committee for the Redefinition of Myocardial Infarction4;
Indications 3-8 (primary prevention of sudden cardiac death) must also meet the following criteria: a. Patients must be able to give informed consent; b. Patients must not have: § Cardiogenic shock or symptomatic hypotension while in a stable baseline rhythm; § Had a CABG or PTCA within the past 3 months; § Had an acute MI within the past 40 days; § Clinical symptoms or findings that would make them a candidate for coronary revascularization; § Any disease, other than cardiac disease (e.g., cancer, uremia, liver failure), associated with a likelihood of
survival less than 1 year; c. Ejection fractions must be measured by angiography, radionuclide scanning, or echocardiography; d. The beneficiary receiving the defibrillator implantation for primary prevention is enrolled in either a Food and
Drug Administration (FDA) approved category B investigational device exemption (IDE) clinical trial (42 CFR §405.201), a trial under the CMS Clinical Trial Policy (National Coverage Determination (NCD) Manual §310.1), or a qualifying data collection system including approved clinical trials and registries. Initially, an implantable cardiac defibrillator (ICD) database will be maintained using a data submission mechanism that is already in use by Medicare participating hospitals to submit data to the Iowa Foundation for Medical Care (IFMC) – a Quality Improvement Organization (QIO) contractor – for determination of reasonable and necessary and quality improvement. Initial hypothesis and data elements are specified in this decision (Appendix VI) and are the minimum necessary to ensure that the device is reasonable and necessary. Data collection will be completed using the ICDA (ICD Abstraction Tool) and transmitted via QNet (Quality Network Exchange) to the IFMC who will collect and maintain the database. Additional stakeholder-developed data collection systems to augment or replace the initial QNet system, addressing at a minimum the hypotheses specified in this decision, must meet the following basic criteria:
§ Written protocol on file; § Institutional review board review and approval; § Scientific review and approval by two or more qualified individuals who are not part of the research team; § Certification that investigators have not been disqualified.
6/22Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coverage for ICD Therapy
For purposes of this coverage decision, CMS will determine whether specific registries or clinical trials meet these criteria.
e. [Was not included in the original publication.] f. Providers must be able to justify the medical necessity of devices other than single lead devices. This
justification should be available in the patient’s medical record.
9. Patients with NIDCM > 3 months, NYHA Class II or III heart failure, and measured LVEF ≤ 35%, only if the following additional criteria are also met: a. Patients must be able to give informed consent; b. Patients must not have:
• Cardiogenic shock or symptomatic hypotension while in a stable baseline rhythm; • Had a CABG or PTCA within the past 3 months; • Had an acute MI within the past 40 days; • Clinical symptoms or findings that would make them a candidate for coronary revascularization; • Irreversible brain damage from preexisting cerebral disease; • Any disease, other than cardiac disease (e.g., cancer, uremia, liver failure), associated with a
likelihood of survival less than 1 year; c. Ejection fractions must be measured by angiography, radionuclide scanning, or echocardiography;d. MIs must be documented and defined according to the consensus document of the Joint European Society
of Cardiology/American College of Cardiology Committee for the Redefinition of Myocardial Infarction4;e. The beneficiary receiving the defibrillator implantation for this indication is enrolled in either an FDA-
approved category B IDE clinical trial (42 CFR §405.201), a trial under the CMS Clinical Trial Policy (NCD Manual §310.1), or a prospective data collection system meeting the following basic criteria:
• Written protocol on file; • Institutional Review Board review and approval; • Scientific review and approval by two or more qualified individuals who are not part of the research team; • Certification that investigators have not been disqualified.
For purposes of this coverage decision, CMS will determine whether specific registries or clinical trials meet these criteria.
f. Providers must be able to justify the medical necessity of devices other than single lead devices. This justification should be available in the patient’s medical record.
C. Other Indications
All other indications for implantable automatic defibrillators not currently covered in accordance with this decision will continue to be covered under Category B IDE trials (42 CFR §405.201) and the CMS routine clinical trials policy (NCD §310.1).
Please see the following page for a Medicare ICD/CRT-D coverage overview chart.
7/22 Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coverage for ICD Therapy
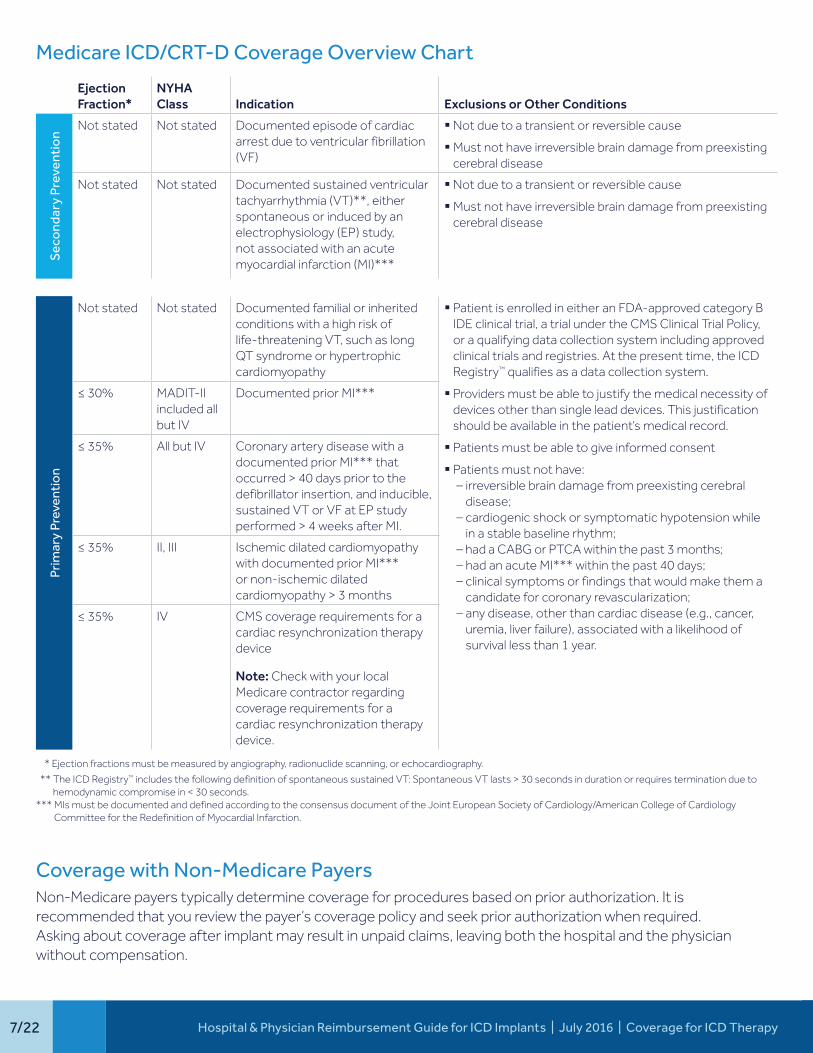
Medicare ICD/CRT-D Coverage Overview Chart
Ejection Fraction*
NYHA Class Indication Exclusions or Other Conditions
Sec
ond
ary
Prev
enti
on
Not stated Not stated Documented episode of cardiac arrest due to ventricular fibrillation (VF)
§ Not due to a transient or reversible cause
§ Must not have irreversible brain damage from preexisting cerebral disease
Not stated Not stated Documented sustained ventricular tachyarrhythmia (VT)**, either spontaneous or induced by an electrophysiology (EP) study, not associated with an acute myocardial infarction (MI)***
§ Not due to a transient or reversible cause
§ Must not have irreversible brain damage from preexisting cerebral disease
Prim
ary
Prev
enti
on
Not stated Not stated Documented familial or inherited conditions with a high risk of life-threatening VT, such as long QT syndrome or hypertrophic cardiomyopathy
§ Patient is enrolled in either an FDA-approved category B IDE clinical trial, a trial under the CMS Clinical Trial Policy, or a qualifying data collection system including approved clinical trials and registries. At the present time, the ICD Registry™ qualifies as a data collection system.
§ Providers must be able to justify the medical necessity of devices other than single lead devices. This justification should be available in the patient’s medical record.
§ Patients must be able to give informed consent
§ Patients must not have:– irreversible brain damage from preexisting cerebral
disease;– cardiogenic shock or symptomatic hypotension while
in a stable baseline rhythm;– had a CABG or PTCA within the past 3 months;– had an acute MI*** within the past 40 days;– clinical symptoms or findings that would make them a
candidate for coronary revascularization;– any disease, other than cardiac disease (e.g., cancer,
uremia, liver failure), associated with a likelihood of survival less than 1 year.
≤ 30% MADIT-II included all but IV
Documented prior MI***
≤ 35% All but IV Coronary artery disease with a documented prior MI*** that occurred > 40 days prior to the defibrillator insertion, and inducible, sustained VT or VF at EP study performed > 4 weeks after MI.
≤ 35% II, III Ischemic dilated cardiomyopathy with documented prior MI*** or non-ischemic dilated cardiomyopathy > 3 months
≤ 35% IV CMS coverage requirements for a cardiac resynchronization therapy device
Note: Check with your local Medicare contractor regarding coverage requirements for a cardiac resynchronization therapy device.
* Ejection fractions must be measured by angiography, radionuclide scanning, or echocardiography.
** The ICD Registry™ includes the following definition of spontaneous sustained VT: Spontaneous VT lasts > 30 seconds in duration or requires termination due to hemodynamic compromise in < 30 seconds.
*** MIs must be documented and defined according to the consensus document of the Joint European Society of Cardiology/American College of Cardiology Committee for the Redefinition of Myocardial Infarction.
Coverage with Non-Medicare PayersNon-Medicare payers typically determine coverage for procedures based on prior authorization. It is recommended that you review the payer’s coverage policy and seek prior authorization when required. Asking about coverage after implant may result in unpaid claims, leaving both the hospital and the physician without compensation.
8/22Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coding for ICD Therapy
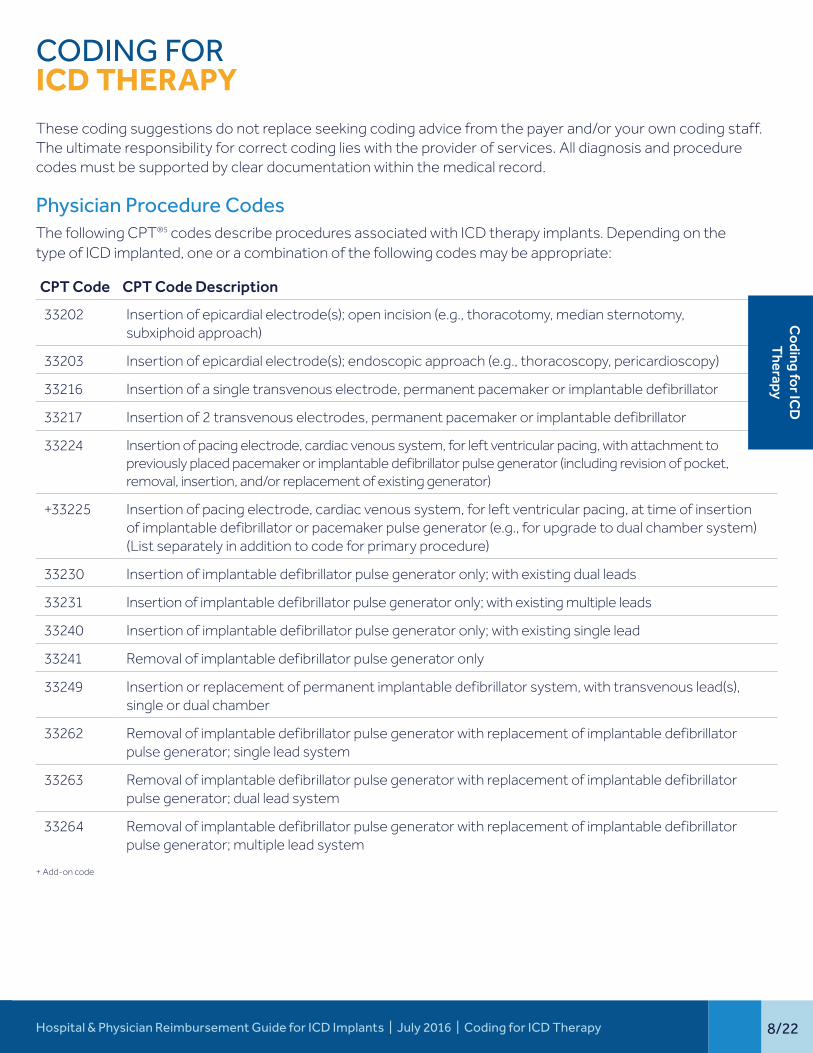
CODING FOR ICD THERAPYThese coding suggestions do not replace seeking coding advice from the payer and/or your own coding staff. The ultimate responsibility for correct coding lies with the provider of services. All diagnosis and procedure codes must be supported by clear documentation within the medical record.
Physician Procedure Codes The following CPT®5 codes describe procedures associated with ICD therapy implants. Depending on the type of ICD implanted, one or a combination of the following codes may be appropriate:
CPT Code CPT Code Description
33202 Insertion of epicardial electrode(s); open incision (e.g., thoracotomy, median sternotomy, subxiphoid approach)
33203 Insertion of epicardial electrode(s); endoscopic approach (e.g., thoracoscopy, pericardioscopy)
33216 Insertion of a single transvenous electrode, permanent pacemaker or implantable defibrillator
33217 Insertion of 2 transvenous electrodes, permanent pacemaker or implantable defibrillator
33224 Insertion of pacing electrode, cardiac venous system, for left ventricular pacing, with attachment to previously placed pacemaker or implantable defibrillator pulse generator (including revision of pocket, removal, insertion, and/or replacement of existing generator)
+33225 Insertion of pacing electrode, cardiac venous system, for left ventricular pacing, at time of insertion of implantable defibrillator or pacemaker pulse generator (e.g., for upgrade to dual chamber system) (List separately in addition to code for primary procedure)
33230 Insertion of implantable defibrillator pulse generator only; with existing dual leads
33231 Insertion of implantable defibrillator pulse generator only; with existing multiple leads
33240 Insertion of implantable defibrillator pulse generator only; with existing single lead
33241 Removal of implantable defibrillator pulse generator only
33249 Insertion or replacement of permanent implantable defibrillator system, with transvenous lead(s), single or dual chamber
33262 Removal of implantable defibrillator pulse generator with replacement of implantable defibrillator pulse generator; single lead system
33263 Removal of implantable defibrillator pulse generator with replacement of implantable defibrillator pulse generator; dual lead system
33264 Removal of implantable defibrillator pulse generator with replacement of implantable defibrillator pulse generator; multiple lead system
+ Add-on code
Coding for IC
D
Therapy
9/22 Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coding for ICD Therapy
Physician Specialty6 The previous page includes various procedure codes associated with ICD implants. Only certain physician specialties are allowed to bill and be reimbursed based on information entered in the Internet-based Provider Enrollment, Chain and Ownership System (PECOS). Physicians self-designate their Medicare physician specialty on the Medicare enrollment application or PECOS. This specialty code is then associated with the claims submitted by that physician. When important information changes occur, revisions must be communicated via paper or the applicable fields updated in the PECOS system.6 Selected Physician Specialty codes are:§ 06 Cardiology § 11 Internal Medicine § 21 Cardiac Electrophysiology
Registry RequirementsPer CMS, Providers (e.g., hospitals and physicians) are required to report the 8-digit number assigned by the National Library of Medicine for dates of service on or after January 1, 2014.7 The clinical trial number allows CMS to track Medicare payments for various reasons. Based on information posted on https://clinicaltrials.gov/ct2/show/NCT01999140 the 8-digit number applicable for an Implantable Cardioverter Defibrillator/ICD Registry is NCT 01999140. Additional coding requirements include: § ICD-10-CM Diagnosis code Z00.6: Encounter for examination for normal comparison and control in clinical
research program. This diagnosis code can be reported in either the primary or secondary positions.§ Q0 Modifier, if applicable
Hospital Inpatient Procedure CodesFY 2016 Implantable Defibrillator and Cardiac Resynchronization Defibrillator ICD-10-PCS (Procedure Coding System) options are available at this web site address: http://www.medtronic.com/wcm/groups/mdtcom_sg/@mdt/@crdm/documents/documents/icd-10-icd-proc-code-10-7-15.pdf
10/22Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coding for ICD Therapy
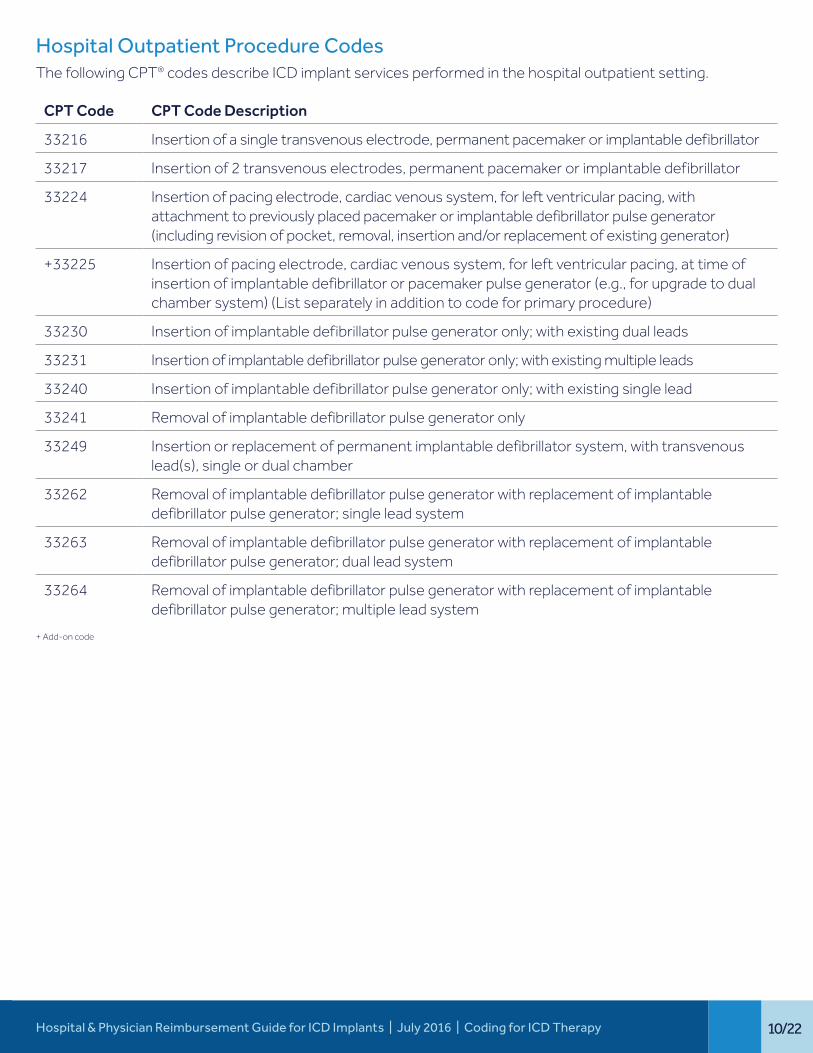
Hospital Outpatient Procedure CodesThe following CPT® codes describe ICD implant services performed in the hospital outpatient setting.
CPT Code CPT Code Description
33216 Insertion of a single transvenous electrode, permanent pacemaker or implantable defibrillator
33217 Insertion of 2 transvenous electrodes, permanent pacemaker or implantable defibrillator
33224 Insertion of pacing electrode, cardiac venous system, for left ventricular pacing, with attachment to previously placed pacemaker or implantable defibrillator pulse generator (including revision of pocket, removal, insertion and/or replacement of existing generator)
+33225 Insertion of pacing electrode, cardiac venous system, for left ventricular pacing, at time of insertion of implantable defibrillator or pacemaker pulse generator (e.g., for upgrade to dual chamber system) (List separately in addition to code for primary procedure)
33230 Insertion of implantable defibrillator pulse generator only; with existing dual leads
33231 Insertion of implantable defibrillator pulse generator only; with existing multiple leads
33240 Insertion of implantable defibrillator pulse generator only; with existing single lead
33241 Removal of implantable defibrillator pulse generator only
33249 Insertion or replacement of permanent implantable defibrillator system, with transvenous lead(s), single or dual chamber
33262 Removal of implantable defibrillator pulse generator with replacement of implantable defibrillator pulse generator; single lead system
33263 Removal of implantable defibrillator pulse generator with replacement of implantable defibrillator pulse generator; dual lead system
33264 Removal of implantable defibrillator pulse generator with replacement of implantable defibrillator pulse generator; multiple lead system
+ Add-on code
11/22 Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coding for ICD Therapy
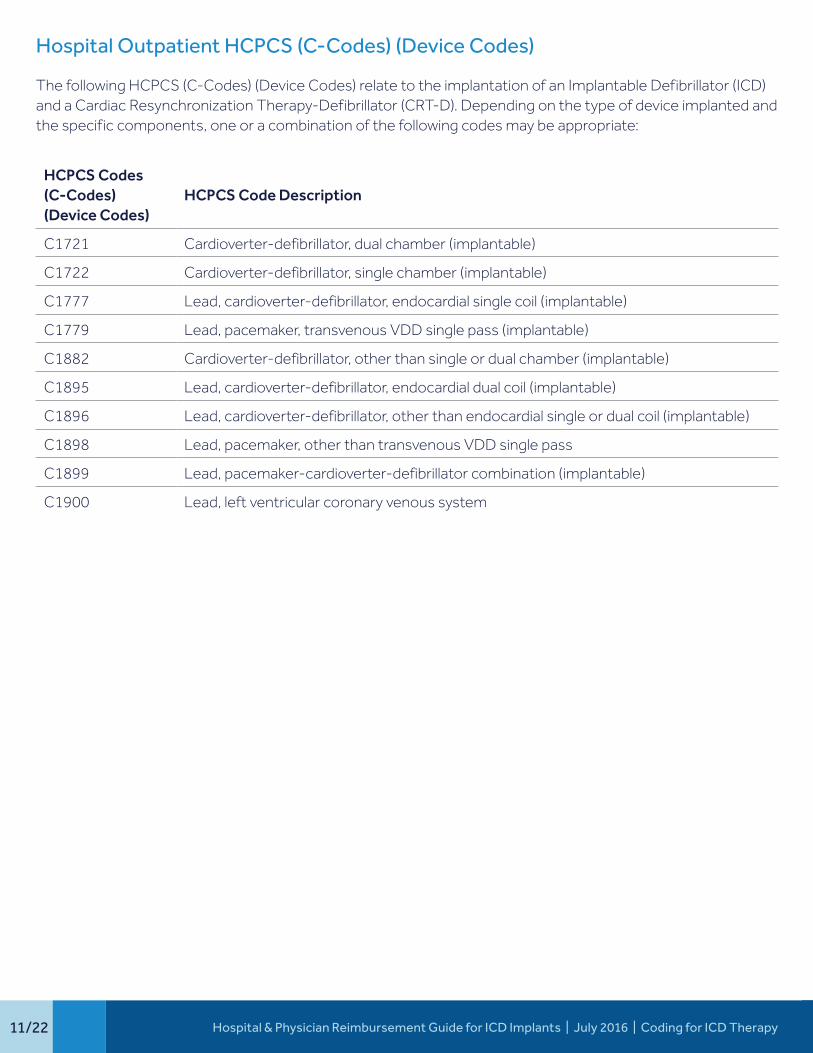
Hospital Outpatient HCPCS (C-Codes) (Device Codes)
The following HCPCS (C-Codes) (Device Codes) relate to the implantation of an Implantable Defibrillator (ICD) and a Cardiac Resynchronization Therapy-Defibrillator (CRT-D). Depending on the type of device implanted and the specific components, one or a combination of the following codes may be appropriate:
HCPCS Codes (C-Codes) (Device Codes)
HCPCS Code Description
C1721 Cardioverter-defibrillator, dual chamber (implantable)
C1722 Cardioverter-defibrillator, single chamber (implantable)
C1777 Lead, cardioverter-defibrillator, endocardial single coil (implantable)
C1779 Lead, pacemaker, transvenous VDD single pass (implantable)
C1882 Cardioverter-defibrillator, other than single or dual chamber (implantable)
C1895 Lead, cardioverter-defibrillator, endocardial dual coil (implantable)
C1896 Lead, cardioverter-defibrillator, other than endocardial single or dual coil (implantable)
C1898 Lead, pacemaker, other than transvenous VDD single pass
C1899 Lead, pacemaker-cardioverter-defibrillator combination (implantable)
C1900 Lead, left ventricular coronary venous system
12/22Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coding for ICD Therapy
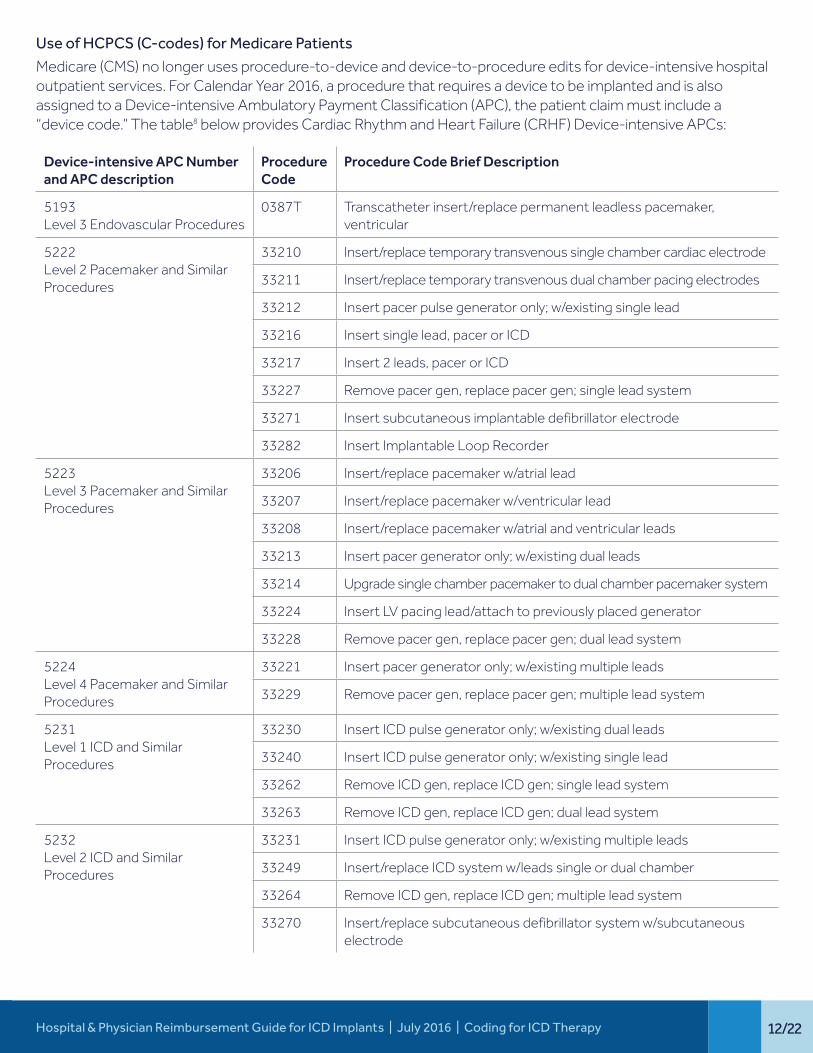
Use of HCPCS (C-codes) for Medicare Patients
Medicare (CMS) no longer uses procedure-to-device and device-to-procedure edits for device-intensive hospital outpatient services. For Calendar Year 2016, a procedure that requires a device to be implanted and is also assigned to a Device-intensive Ambulatory Payment Classification (APC), the patient claim must include a “device code.” The table8 below provides Cardiac Rhythm and Heart Failure (CRHF) Device-intensive APCs:
Device-intensive APC Number and APC description
Procedure Code
Procedure Code Brief Description
5193 Level 3 Endovascular Procedures
0387T Transcatheter insert/replace permanent leadless pacemaker, ventricular
5222 Level 2 Pacemaker and Similar Procedures
33210 Insert/replace temporary transvenous single chamber cardiac electrode
33211 Insert/replace temporary transvenous dual chamber pacing electrodes
33212 Insert pacer pulse generator only; w/existing single lead
33216 Insert single lead, pacer or ICD
33217 Insert 2 leads, pacer or ICD
33227 Remove pacer gen, replace pacer gen; single lead system
33271 Insert subcutaneous implantable defibrillator electrode
33282 Insert Implantable Loop Recorder
5223 Level 3 Pacemaker and Similar Procedures
33206 Insert/replace pacemaker w/atrial lead
33207 Insert/replace pacemaker w/ventricular lead
33208 Insert/replace pacemaker w/atrial and ventricular leads
33213 Insert pacer generator only; w/existing dual leads
33214 Upgrade single chamber pacemaker to dual chamber pacemaker system
33224 Insert LV pacing lead/attach to previously placed generator
33228 Remove pacer gen, replace pacer gen; dual lead system
5224 Level 4 Pacemaker and Similar Procedures
33221 Insert pacer generator only; w/existing multiple leads
33229 Remove pacer gen, replace pacer gen; multiple lead system
5231 Level 1 ICD and Similar Procedures
33230 Insert ICD pulse generator only; w/existing dual leads
33240 Insert ICD pulse generator only; w/existing single lead
33262 Remove ICD gen, replace ICD gen; single lead system
33263 Remove ICD gen, replace ICD gen; dual lead system
5232 Level 2 ICD and Similar Procedures
33231 Insert ICD pulse generator only; w/existing multiple leads
33249 Insert/replace ICD system w/leads single or dual chamber
33264 Remove ICD gen, replace ICD gen; multiple lead system
33270 Insert/replace subcutaneous defibrillator system w/subcutaneous electrode
13/22 Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coding for ICD Therapy
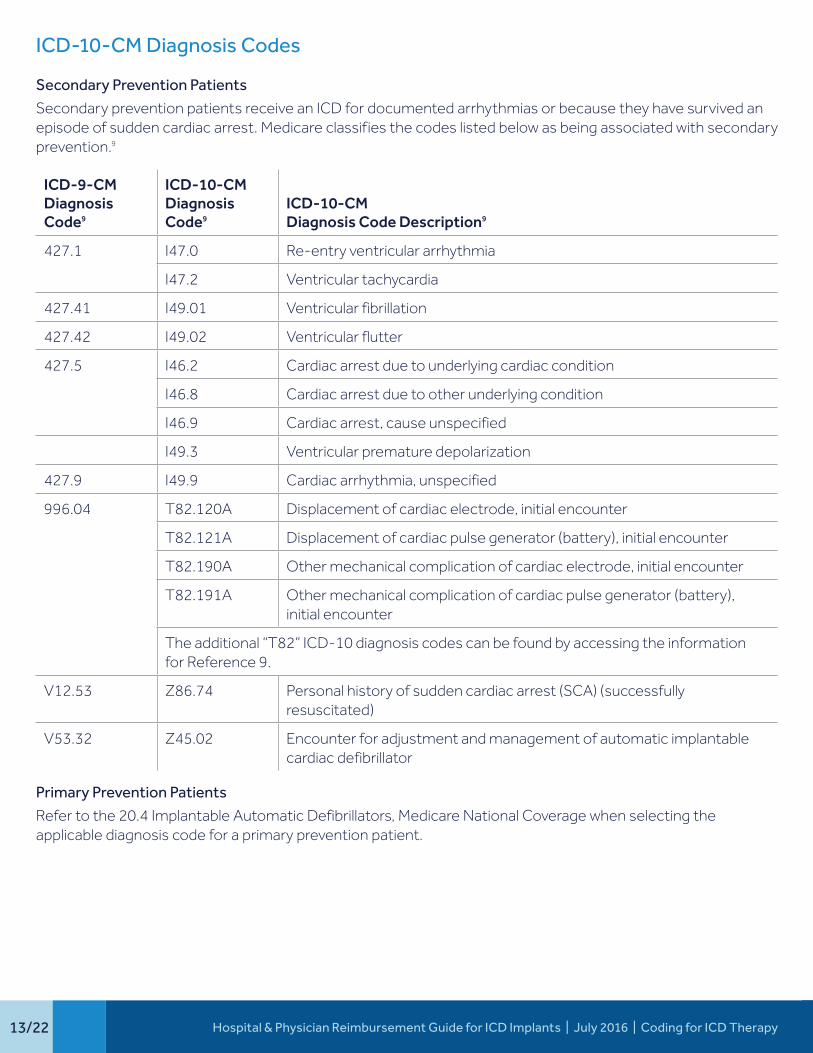
ICD-10-CM Diagnosis Codes
Secondary Prevention Patients
Secondary prevention patients receive an ICD for documented arrhythmias or because they have survived an episode of sudden cardiac arrest. Medicare classifies the codes listed below as being associated with secondary prevention.9
ICD-9-CMDiagnosis Code9
ICD-10-CMDiagnosis Code9
ICD-10-CM Diagnosis Code Description9
427.1 I47.0 Re-entry ventricular arrhythmia
I47.2 Ventricular tachycardia
427.41 I49.01 Ventricular fibrillation
427.42 I49.02 Ventricular flutter
427.5 I46.2 Cardiac arrest due to underlying cardiac condition
I46.8 Cardiac arrest due to other underlying condition
I46.9 Cardiac arrest, cause unspecified
I49.3 Ventricular premature depolarization
427.9 I49.9 Cardiac arrhythmia, unspecified
996.04 T82.120A Displacement of cardiac electrode, initial encounter
T82.121A Displacement of cardiac pulse generator (battery), initial encounter
T82.190A Other mechanical complication of cardiac electrode, initial encounter
T82.191A Other mechanical complication of cardiac pulse generator (battery), initial encounter
The additional “T82” ICD-10 diagnosis codes can be found by accessing the information for Reference 9.
V12.53 Z86.74 Personal history of sudden cardiac arrest (SCA) (successfully resuscitated)
V53.32 Z45.02 Encounter for adjustment and management of automatic implantable cardiac defibrillator
Primary Prevention Patients
Refer to the 20.4 Implantable Automatic Defibrillators, Medicare National Coverage when selecting the applicable diagnosis code for a primary prevention patient.
14/22Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coding for ICD Therapy
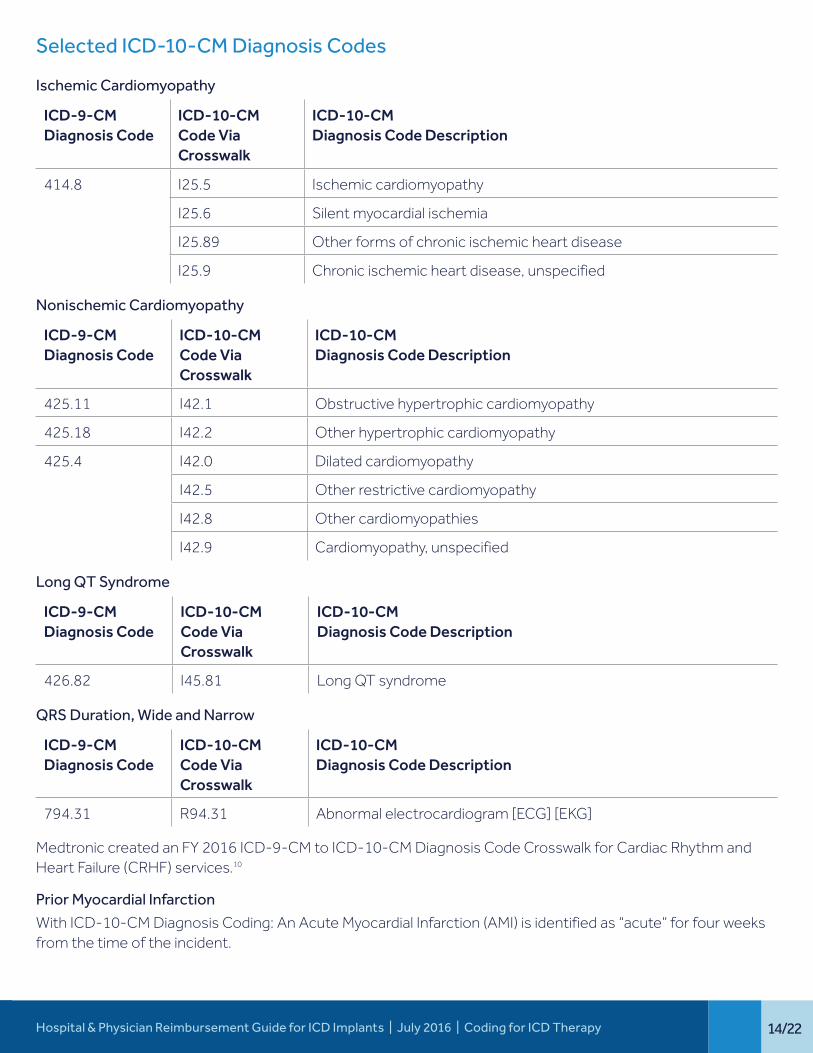
Selected ICD-10-CM Diagnosis Codes
Ischemic Cardiomyopathy
ICD-9-CMDiagnosis Code
ICD-10-CM Code Via Crosswalk
ICD-10-CM Diagnosis Code Description
414.8 I25.5 Ischemic cardiomyopathy
I25.6 Silent myocardial ischemia
I25.89 Other forms of chronic ischemic heart disease
I25.9 Chronic ischemic heart disease, unspecified
Nonischemic Cardiomyopathy
ICD-9-CMDiagnosis Code
ICD-10-CM Code Via Crosswalk
ICD-10-CM Diagnosis Code Description
425.11 I42.1 Obstructive hypertrophic cardiomyopathy
425.18 I42.2 Other hypertrophic cardiomyopathy
425.4 I42.0 Dilated cardiomyopathy
I42.5 Other restrictive cardiomyopathy
I42.8 Other cardiomyopathies
I42.9 Cardiomyopathy, unspecified
Long QT Syndrome
ICD-9-CMDiagnosis Code
ICD-10-CM Code Via Crosswalk
ICD-10-CM Diagnosis Code Description
426.82 I45.81 Long QT syndrome
QRS Duration, Wide and Narrow
ICD-9-CMDiagnosis Code
ICD-10-CM Code Via Crosswalk
ICD-10-CM Diagnosis Code Description
794.31 R94.31 Abnormal electrocardiogram [ECG] [EKG]
Medtronic created an FY 2016 ICD-9-CM to ICD-10-CM Diagnosis Code Crosswalk for Cardiac Rhythm and Heart Failure (CRHF) services.10
Prior Myocardial Infarction
With ICD-10-CM Diagnosis Coding: An Acute Myocardial Infarction (AMI) is identified as “acute” for four weeks from the time of the incident.
15/22
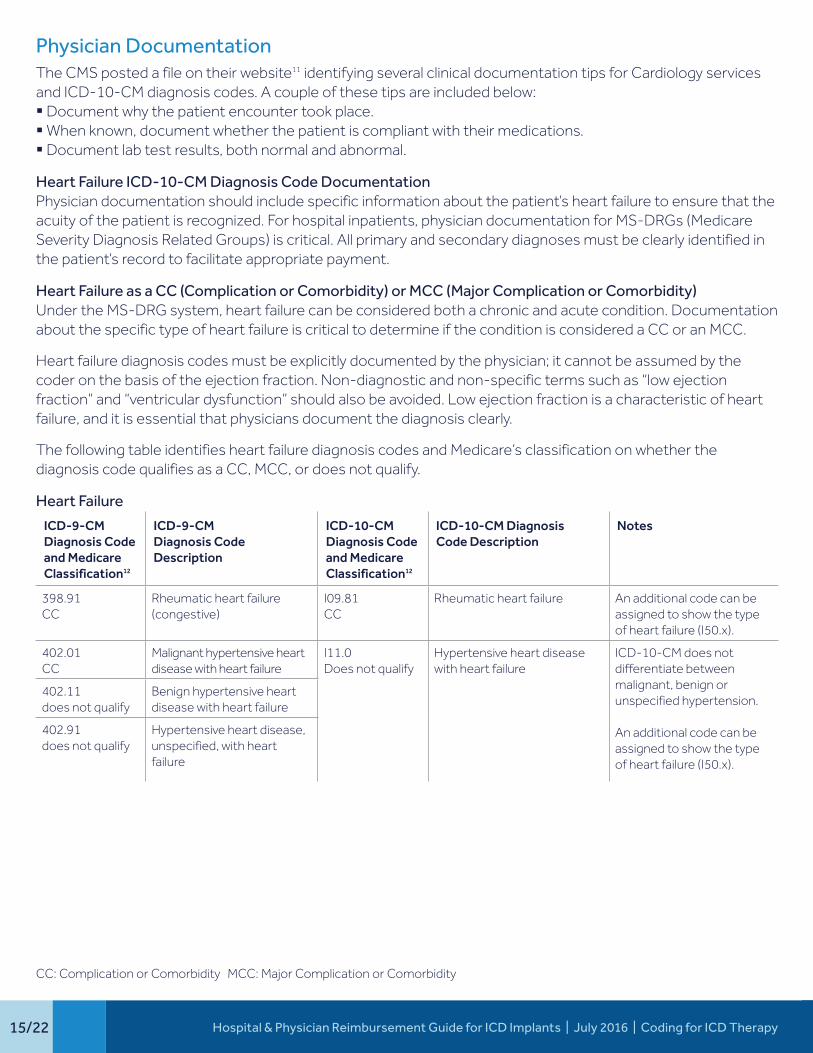
Physician DocumentationThe CMS posted a file on their website11 identifying several clinical documentation tips for Cardiology services and ICD-10-CM diagnosis codes. A couple of these tips are included below: § Document why the patient encounter took place. § When known, document whether the patient is compliant with their medications. § Document lab test results, both normal and abnormal.
Heart Failure ICD-10-CM Diagnosis Code Documentation Physician documentation should include specific information about the patient’s heart failure to ensure that the acuity of the patient is recognized. For hospital inpatients, physician documentation for MS-DRGs (Medicare Severity Diagnosis Related Groups) is critical. All primary and secondary diagnoses must be clearly identified in the patient’s record to facilitate appropriate payment.
Heart Failure as a CC (Complication or Comorbidity) or MCC (Major Complication or Comorbidity)Under the MS-DRG system, heart failure can be considered both a chronic and acute condition. Documentation about the specific type of heart failure is critical to determine if the condition is considered a CC or an MCC.
Heart failure diagnosis codes must be explicitly documented by the physician; it cannot be assumed by the coder on the basis of the ejection fraction. Non-diagnostic and non-specific terms such as “low ejection fraction” and “ventricular dysfunction” should also be avoided. Low ejection fraction is a characteristic of heart failure, and it is essential that physicians document the diagnosis clearly.
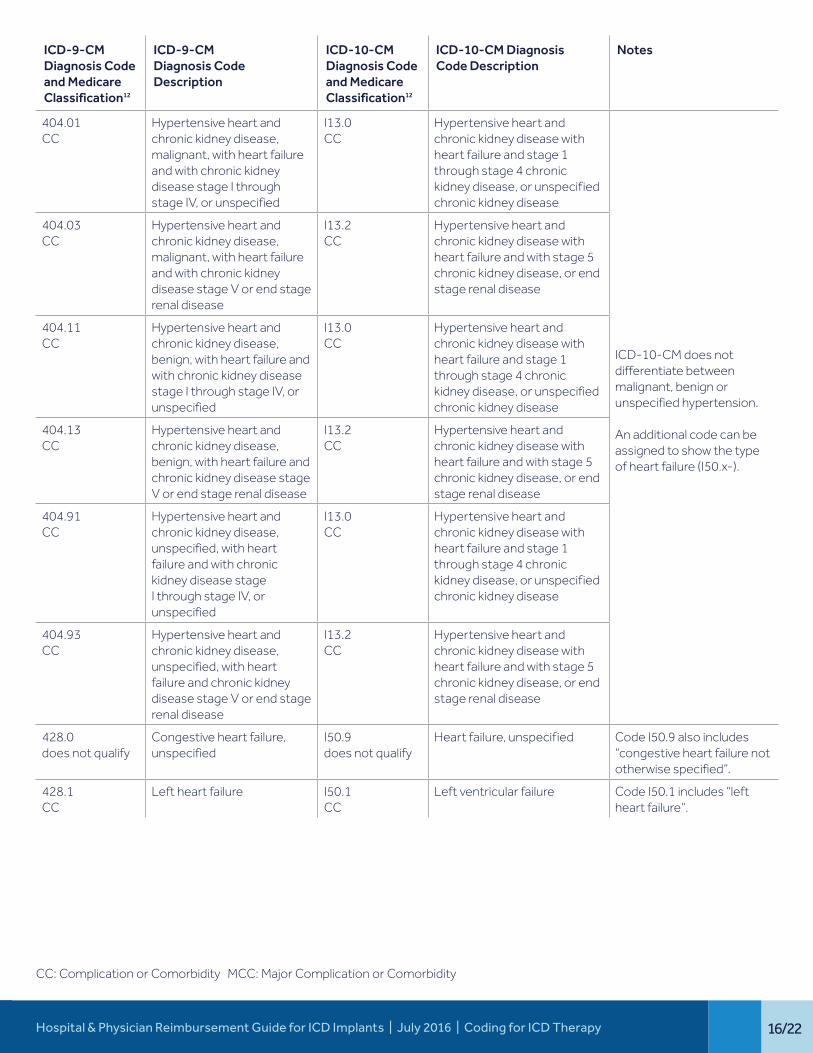
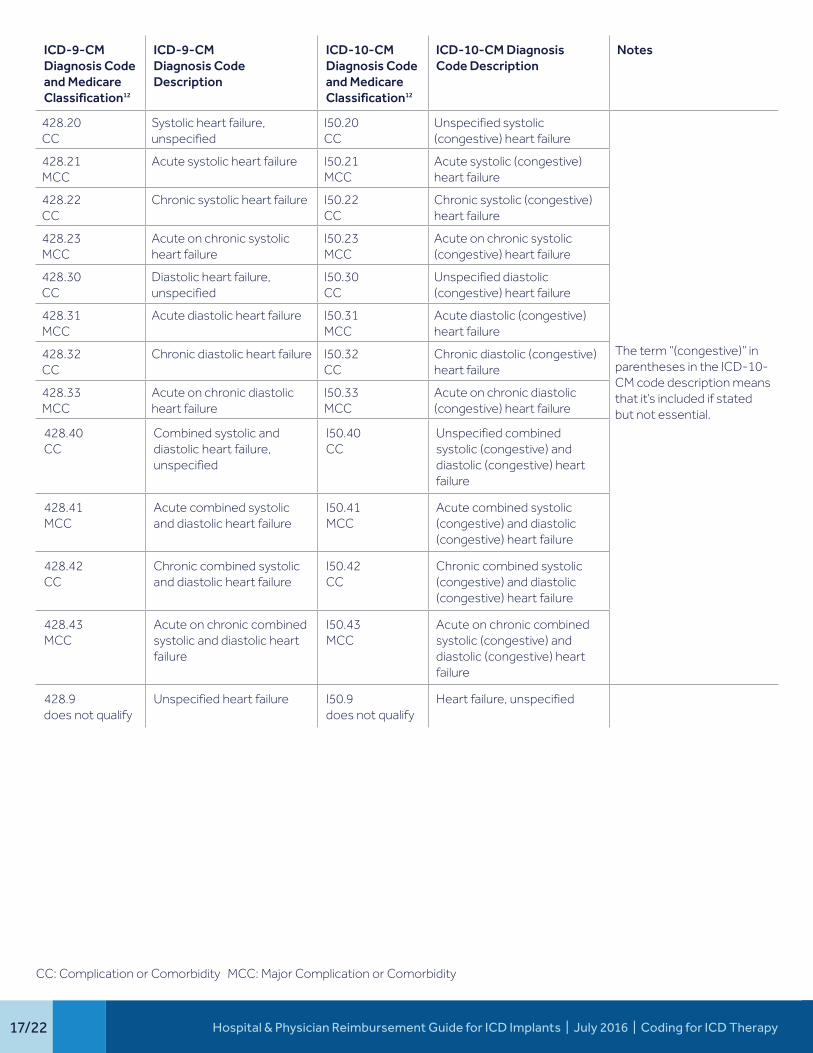
The following table identifies heart failure diagnosis codes and Medicare’s classification on whether the diagnosis code qualifies as a CC, MCC, or does not qualify.
Heart Failure
ICD-9-CMDiagnosis Code and Medicare Classification12
ICD-9-CMDiagnosis Code Description
ICD-10-CMDiagnosis Code and Medicare Classification12
ICD-10-CM Diagnosis Code Description
Notes
398.91CC
Rheumatic heart failure (congestive)
I09.81CC
Rheumatic heart failure An additional code can be assigned to show the type of heart failure (I50.x).
402.01 CC
Malignant hypertensive heart disease with heart failure
I11.0Does not qualify
Hypertensive heart disease with heart failure
ICD-10-CM does not differentiate between malignant, benign or unspecified hypertension.
An additional code can be assigned to show the type of heart failure (I50.x).
402.11 does not qualify
Benign hypertensive heart disease with heart failure
402.91 does not qualify
Hypertensive heart disease, unspecified, with heart failure
CC: Complication or Comorbidity MCC: Major Complication or Comorbidity
Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coding for ICD Therapy
16/22
CC: Complication or Comorbidity MCC: Major Complication or Comorbidity
ICD-9-CMDiagnosis Code and Medicare Classification12
ICD-9-CMDiagnosis Code Description
ICD-10-CMDiagnosis Code and Medicare Classification12
ICD-10-CM Diagnosis Code Description
Notes
404.01CC
Hypertensive heart and chronic kidney disease, malignant, with heart failure and with chronic kidney disease stage I through stage IV, or unspecified
I13.0CC
Hypertensive heart and chronic kidney disease with heart failure and stage 1 through stage 4 chronic kidney disease, or unspecified chronic kidney disease
ICD-10-CM does not differentiate between malignant, benign or unspecified hypertension.
An additional code can be assigned to show the type of heart failure (I50.x-).
404.03CC
Hypertensive heart and chronic kidney disease, malignant, with heart failure and with chronic kidney disease stage V or end stage renal disease
I13.2CC
Hypertensive heart and chronic kidney disease with heart failure and with stage 5 chronic kidney disease, or end stage renal disease
404.11CC
Hypertensive heart and chronic kidney disease, benign, with heart failure and with chronic kidney disease stage I through stage IV, or unspecified
I13.0CC
Hypertensive heart and chronic kidney disease with heart failure and stage 1 through stage 4 chronic kidney disease, or unspecified chronic kidney disease
404.13CC
Hypertensive heart and chronic kidney disease, benign, with heart failure and chronic kidney disease stage V or end stage renal disease
I13.2CC
Hypertensive heart and chronic kidney disease with heart failure and with stage 5 chronic kidney disease, or end stage renal disease
404.91CC
Hypertensive heart and chronic kidney disease, unspecified, with heart failure and with chronic kidney disease stage I through stage IV, or unspecified
I13.0CC
Hypertensive heart and chronic kidney disease with heart failure and stage 1 through stage 4 chronic kidney disease, or unspecified chronic kidney disease
404.93CC
Hypertensive heart and chronic kidney disease, unspecified, with heart failure and chronic kidney disease stage V or end stage renal disease
I13.2CC
Hypertensive heart and chronic kidney disease with heart failure and with stage 5 chronic kidney disease, or end stage renal disease
428.0does not qualify
Congestive heart failure, unspecified
I50.9does not qualify
Heart failure, unspecified Code I50.9 also includes “congestive heart failure not otherwise specified”.
428.1CC
Left heart failure I50.1CC
Left ventricular failure Code I50.1 includes “left heart failure”.
Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coding for ICD Therapy
17/22
ICD-9-CMDiagnosis Code and Medicare Classification12
ICD-9-CMDiagnosis Code Description
ICD-10-CMDiagnosis Code and Medicare Classification12
ICD-10-CM Diagnosis Code Description
Notes
428.20CC
Systolic heart failure, unspecified
I50.20CC
Unspecified systolic (congestive) heart failure
The term “(congestive)” in parentheses in the ICD-10-CM code description means that it’s included if stated but not essential.
428.21MCC
Acute systolic heart failure I50.21MCC
Acute systolic (congestive) heart failure
428.22CC
Chronic systolic heart failure I50.22CC
Chronic systolic (congestive) heart failure
428.23 MCC
Acute on chronic systolic heart failure
I50.23MCC
Acute on chronic systolic (congestive) heart failure
428.30 CC
Diastolic heart failure, unspecified
I50.30CC
Unspecified diastolic (congestive) heart failure
428.31MCC
Acute diastolic heart failure I50.31MCC
Acute diastolic (congestive) heart failure
428.32CC
Chronic diastolic heart failure I50.32CC
Chronic diastolic (congestive) heart failure
428.33 MCC
Acute on chronic diastolic heart failure
I50.33MCC
Acute on chronic diastolic (congestive) heart failure
428.40 CC
Combined systolic and diastolic heart failure, unspecified
I50.40 CC
Unspecified combined systolic (congestive) and diastolic (congestive) heart failure
428.41 MCC
Acute combined systolic and diastolic heart failure
I50.41 MCC
Acute combined systolic (congestive) and diastolic (congestive) heart failure
428.42 CC
Chronic combined systolic and diastolic heart failure
I50.42 CC
Chronic combined systolic (congestive) and diastolic (congestive) heart failure
428.43 MCC
Acute on chronic combined systolic and diastolic heart failure
I50.43 MCC
Acute on chronic combined systolic (congestive) and diastolic (congestive) heart failure
428.9 does not qualify
Unspecified heart failure I50.9 does not qualify
Heart failure, unspecified
CC: Complication or Comorbidity MCC: Major Complication or Comorbidity
Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Coding for ICD Therapy
18/22
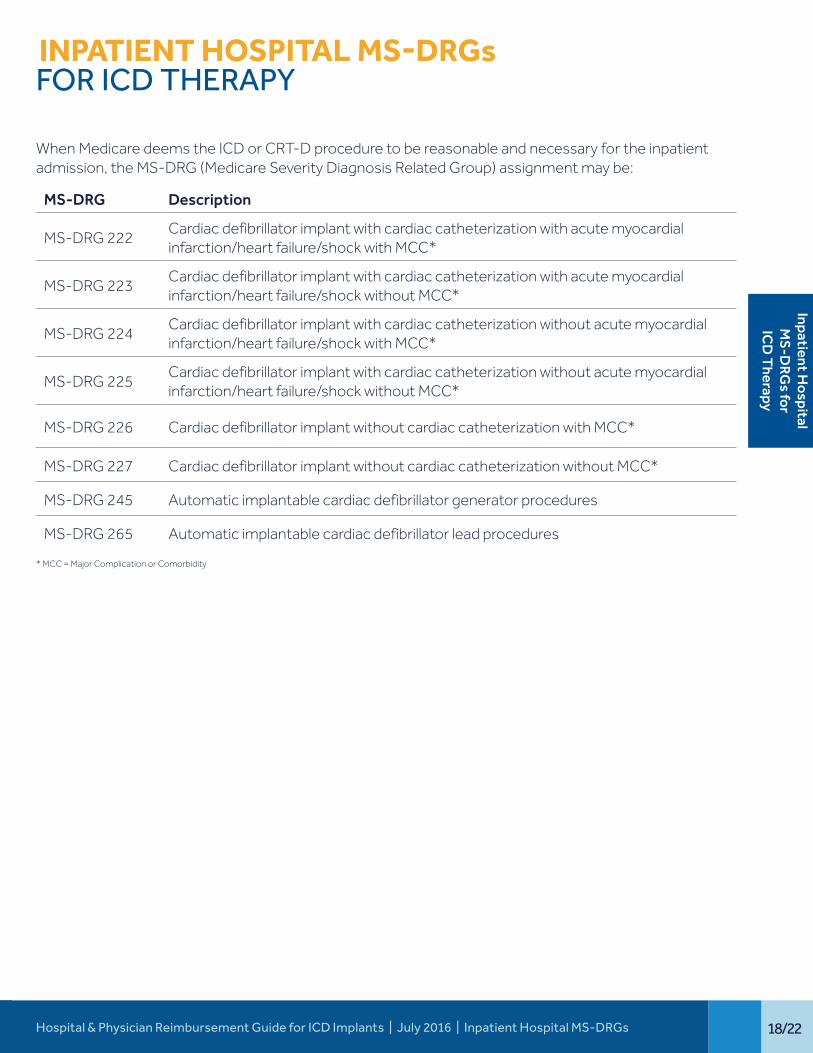
INPATIENT HOSPITAL MS-DRGs FOR ICD THERAPY
When Medicare deems the ICD or CRT-D procedure to be reasonable and necessary for the inpatient admission, the MS-DRG (Medicare Severity Diagnosis Related Group) assignment may be:
MS-DRG Description
MS-DRG 222Cardiac defibrillator implant with cardiac catheterization with acute myocardial infarction/heart failure/shock with MCC*
MS-DRG 223Cardiac defibrillator implant with cardiac catheterization with acute myocardial infarction/heart failure/shock without MCC*
MS-DRG 224Cardiac defibrillator implant with cardiac catheterization without acute myocardial infarction/heart failure/shock with MCC*
MS-DRG 225Cardiac defibrillator implant with cardiac catheterization without acute myocardial infarction/heart failure/shock without MCC*
MS-DRG 226 Cardiac defibrillator implant without cardiac catheterization with MCC*
MS-DRG 227 Cardiac defibrillator implant without cardiac catheterization without MCC*
MS-DRG 245 Automatic implantable cardiac defibrillator generator procedures
MS-DRG 265 Automatic implantable cardiac defibrillator lead procedures
* MCC = Major Complication or Comorbidity
Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Inpatient Hospital MS-DRGs
Inpatient Hospital
MS
-DRG
s for IC
D T
herapy
19/22 Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Medicare ICD Implant Registry
MEDICARE ICD IMPLANT REGISTRY
NCDR® ICD Registry™ participation is mandatory to obtain Medicare coverage for both inpatient and outpatient ICD services for primary prevention patients.
The Implantable Automatic Defibrillators Medicare National Coverage Determination (20.4) allows other trials/registries to submit information about their data collection to the CMS to determine if the data collection requirement is satisfied. CMS will then determine whether trials/registries meet these criteria.
Medicare patients enrolled in either an FDA-approved Category B Investigational Device Exemption (IDE) clinical trial or a trial receiving coverage under the Medicare Routine Costs in Clinical Trials policy do not need to have their data submitted to this registry.
The ICD Registry is a collaboration between the American College of Cardiology Foundation® and the Heart Rhythm SocietySM, and is formally referred to as the American College of Cardiology’s National Cardiovascular Data Registry’s (ACC-NCDR) ICD Registry™. The purpose of the registry is to meet Medicare’s data requirements.
This registry collects:a) Patient demographics, provider and facility characteristicsb) Device type and characteristics for ICD implantationc) Atrial, ventricular, defibrillator and left-heart lead datad) Adverse event ratese) Compliance with ACC/AHA/HRS clinical guidelines recommendationsf) Data necessary for meeting the CMS requirements for hospitals that perform ICD implantation procedures
Hospitals can choose to enter only Medicare primary prevention patients or all ICD patients that would include primary and secondary patients for both Medicare and non-Medicare patients. It is also very important to remember that for primary prevention implants, Medicare requires the Q0 modifier to be appended to the applicable ICD procedure code for both the physician and the hospital if the patient is an Outpatient.9
Unique Device Identifier (UDI): The Global Unique Device Identification Database (GUDID) serves as reference catalog for devices with an identifier. This database is available at: http://www.fda.gov/medicaldevices/deviceregulationandguidance/uniquedeviceidentification/globaludidatabasegudid/default.htm
The identifier (UDI) is sent to the FDA by the manufacturing company. The registry data collection form (V2.2) currently includes a UDI question but this is not a required data field at this time. Presently, there is no anticipated timeline as to when the UDI will be required.
Per CMS, Providers (e.g., hospitals and physicians) are required to report the 8-digit number assigned by the National Library of Medicine for dates of service on or after January 1, 2014.7 The clinical trial number allows CMS to track Medicare payments for various reasons. Based on information posted on https://clinicaltrials.gov/ct2/show/NCT01999140 the 8-digit number applicable for an Implantable Cardioverter Defibrillator/ICD Registry is NCT 01999140. Additional coding requirements include: § ICD-10-CM Diagnosis code Z00.6: Encounter for examination for normal comparison and control in clinical
research program. This diagnosis code can be reported in either the primary or secondary positions.§ Q0 Modifier, if applicable
More information can be found at http://ncdr.com or by calling the American College of Cardiology at 1-800-257-4737 to speak with an NCDR team member.
Med
icar
e Im
plan
t Re
gist
ry
20/22Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Frequently Asked Questions
FREQUENTLY ASKED QUESTIONS
Does Medicare grant prior authorization for services?
No. Traditional (Fee-for-Service) Medicare does not typically require or grant prior authorization for services; however, some Medicare Advantage Plans do require prior authorizations. Please contact your local Medicare contractor when you have questions on Medicare coverage. Medicare’s website address is: http://www.cms.gov.
How do non-Medicare payers determine coverage for ICD implants?
Non-Medicare payers typically determine coverage through the prior authorization process. Contact the patient’s payer to determine how you should proceed.
Have there been any written changes to Medicare’s covered indications since January 27, 2005?
No, the National Coverage Determination (NCD) has not changed. However, as mentioned on page 3, patients with nonischemic dilated cardiomyopathy (NICDM) > 3 months, NYHA Class II and III heart failure, and measured LVEF ≤ 35% will be covered as a result of the ACC-NCDR registry.
Does Medicare cover ICD therapy for the treatment of atrial fibrillation in patients who do not have a corresponding ventricular indication?
No. As of October 1, 2003, Medicare coverage is not available for ICD therapy for the treatment of atrial fibrillation in patients who do not have a corresponding ventricular indication, unless the patients are receiving ICD therapy under category B IDE trial (42 CFR §405.201) or the CMS routine clinical trials policy (CIM 30-1, NCD 130.1).
Are there national CMS QRS requirements for NYHA Class IV heart failure CRT-D patients?
No, but Medicare local contractors my develop local coverage decisions or coding/billing articles for cardiac resynchronization therapy defibrillators (CDT-D). Some of these local coverage decisions (LCDs) may require a strict adherence for FDA labeling (e.g., patients must have a QRS duration > 120 ms or 130 ms, etc.) in order for coverage to be granted. Contact your local Medicare contractor for more information regarding these and other policy requirements. Local Medicare coverage can be researched at: http://www.cms.gov/medicare-coverage-database/overview-and-quick-search.aspx.
Who must report the Q0 (zero) modifier?
Physicians must report the Q0 modifier on Medicare claims submitted on or after April 1, 2005 for primary prevention patients. The Q0 modifier should be appended to the primary procedure code describing the service. This modifier is also applicable to Medicare Hospital Outpatient claims (OPPS) and has been since April 1, 2005. The Q0 modifier is not required for secondary prevention diagnosis codes.9
What are the documentation requirements for replacing ICDs?
The Medicare NCD does not discuss coverage criteria for replacing an ICD generator. The Department of Justice Resolution Model released to hospitals on August 30, 2012 includes information regarding device replacements on pages 8-9.13
Frequently Asked
Questions
21/22 Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 | Frequently Asked Questions
What are the four NYHA (New York Heart Association) functional classifications? The NYHA functional capacity is an estimation of a patient’s limitation during physical activity as shown below.
NYHA I: No limitation of physical activity. Ordinary physician activity does not cause undue fatigue, palpitation, dyspnea (shortness of breath).
NYHA II: Slight limitation of physical activity. Comfortable at rest. Ordinary physical activity results in fatigue, palpitation, dyspnea (shortness of breath).
NYHA III: Marked limitation of physical activity. Comfortable at rest. Less than ordinary activity causes fatigue, palpitation, or dyspnea.
NYHA IV: Unable to carry on any physical activity without discomfort. Symptoms of heart failure at rest. If any physical activity is undertaken, discomfort increases.
Source: http://www.heart.org/HEARTORG/Conditions/HeartFailure/AboutHeartFailure/Classes-of-Heart-Failure_UCM_306328_Article.jsp
Do secondary diagnosis codes make a difference in DRG assignment?
Yes. With the MS-DRG payment structure, secondary diagnoses codes can affect the DRG assignment. The secondary diagnosis will determine if the patient has a major complication or comorbidity (MCC).
Can certain CC or MCC codes be excluded for MS-DRG assignment in particular situations?
Yes. Eight ICD-10 MCC diagnosis codes are only valid if the patient is discharged alive. This list includes14:
I46.2 I46.8 I46.9 I49.01 R09.2 R57.0 R57.1 R57.8
Cardiac arrest due to underlying cardiac condition
Cardiac arrest due to other underlying condition
Cardiac arrest, cause unspecified
Ventricular fibrillation
Respiratory arrest
Cardiogenic shock
Hypovolemic shock
Other shock

Hospital & Physician Reimbursement Guide for ICD Implants | July 2016 22/22

References1 The history of Medicare coverage for implantable automatic defibrillators can be found at: http://
www.cms.gov/medicare-coverage-database/details/ncd-details.aspx?NCDId=110&ncdver=3&bc=BAAAgAAAAAAA&.
2 Bardy GH, Lee KL, Mark DB, et al, for the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT) Investigators. Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure [published correction appears in N Engl J Med. May 19, 2005;352(20):2146]. N Engl J Med. January 20, 2005;352(3):225-237.
3 Moss AJ, Zareba W, Hall WJ, et al, for the Multicenter Automatic Defibrillator Implantation Trial II Investigators. Prophylactic implantation of a defibrillator in patients with myocardial infarction and reduced ejection fraction. N Engl J Med. March 21, 2002;346(12):877-883.
4 Alpert JS, Thygesen K, Antman E, Bassand JP. Myocardial infarction redefined – a consensus document of The Joint European Society of Cardiology/American College of Cardiology Committee for the redefinition of myocardial infarction. J Am Coll Cardiol. September 2000;36(3):959-969.
Criteria for acute, evolving, or recent MI: Either one of the following criteria satisfies the diagnosis for an acute, evolving, or recent MI:
1) Typical rise and gradual fall (troponin) or more rapid rise and fall (CK-MB) of biochemical markers of myocardial necrosis with at least one of the following: a) Ischemic symptoms b) Development of pathologic Q waves on the ECG c) ECG changes indicative of ischemia (ST segment elevation or depression) or d) Coronary artery intervention (e.g., coronary angioplasty)
2) Pathologic findings of an acute MI Criteria for established MI: Any one of the following criteria satisfies the diagnosis for established MI: 1) Development of new pathologic Q waves on serial ECGs. The patient may or may not remember
previous symptoms. Biochemical markers of myocardial necrosis may have normalized, depending on the length of time that has passed since the infarct developed.
2) Pathologic findings of a healed or healing MI. 5 CPT copyright 2015 American Medical Association. All rights reserved. CPT is a registered trademark
of the American Medical Association.6 Pub 100-04 Medicare Claims Processing (CMS), Transmittal 2098 dated November 19, 2010 with the
subject of New Physician Specialty Codes for Cardiac Electrophysiology and Sports Medicine is at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R2098CP.pdf The PECOS FAQs ICN 909015 dated December 2015 is at: https://www.cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNProducts/Downloads/Internet-Based-PECOS-FAQs-Fact-Sheet-ICN909015.pdf
7 Pub 100-04 Medicare Claims Processing (CMS) Transmittal 2955 dated May 14, 2014 with the subject of Mandatory Reporting of an 8-Digit Clinical Trial Number on Claims can be found at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Transmittals/Downloads/R2955CP.pdf
8 The Device-intensive APC information is available on pages 70421-70422 of the Final CMS Hospital Outpatient Prospective Payment System rule published in the November 13, 2015 Federal Register available at: https://www.gpo.gov/fdsys/pkg/FR-2015-11-13/pdf/2015-27943.pdf
9 Pub 100-04 Medicare Claims Processing Manual (CMS), Chapter 32 – Billing Requirements for Special Services, Section 270.2 - Billing Requirements for Patients Enrolled in a Data Collection is available at: https://www.cms.gov/Regulations-and-Guidance/Guidance/Manuals/Downloads/clm104c32.pdf.
10 Medtronic FY 2016 ICD-9-CM to ICD-10-CM Diagnosis Code Crosswalk for Cardiac Rhythm and Heart Failure services can be found at: http://www.medtronic.com/wcm/groups/mdtcom_sg/@mdt/@crdm/documents/documents/icd9-2-icd10-diag-crhf-10-7-15.pdf
11 The ICD-10-Clinical Concepts for Cardiology file can be found at: https://www.cms.gov/Medicare/Coding/ICD10/Downloads/ICD10ClinicalConceptsCardiology1.pdf
12 Medicare’s MCC (Table 6I) and CC (Table 6J) for the selected fiscal year are available at: https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/index.html
13 Department of Justice ICD Investigation Medical Review Guidelines/Resolution Model, Section 3, pages 8-9.
14 Appendix C - Complications or Comorbidities Exclusion list included in the ICD-10-CM/PCS MS-DRG v33 Definitions Manual is available on the CMS website at: https://www.cms.gov/ICD10Manual/version33-fullcode-cms/fullcode_cms/P0375.html
medtronic.com
UC201500767a EN ©2016 Medtronic. Minneapolis, MN. All Rights Reserved. Printed in USA. 07/2016
Medtronic710 Medtronic Parkway Minneapolis, MN 55432-5604 USA Tel: 763.514.4000 Fax: 763.514.4879
Toll-free: 1.800.328.2518(24-hour technical support for physicians and medical professionals)
FOR ADDITIONAL INFORMATION PLEASE CONTACT
CRHF ECONOMICS & HEALTH POLICY
Visit our website: www.Medtronic.com/crdmreimbursementEmail us: [email protected] our coding hotline: 1.866.877.4102





























