Embed Size (px)
Citation preview
Critical Care
Rehabilitation Pathway (Standards)
South East Coast
Operational Delivery Networks Hosted by Medway Foundation Trust
Document control: This document will replace the Critical Care
Rehabilitation Pathway User Guide
Caroline Wilson 11/03/16 Presented to Network Leads
CW & MC 08/07/16 Agreed at Network Leads Meeting
Contents
Flowchart
Standards for Critical Care Rehabilitation Pathway Documents
Assessment Tools
• Hospital Anxiety Depression Scale
• Post Traumatic Stress Disorder Assessment Tool
• Barthel Activities of Daily Living Index
• RASS Score & CAM-ICU Score
• CPAx Assessment tool
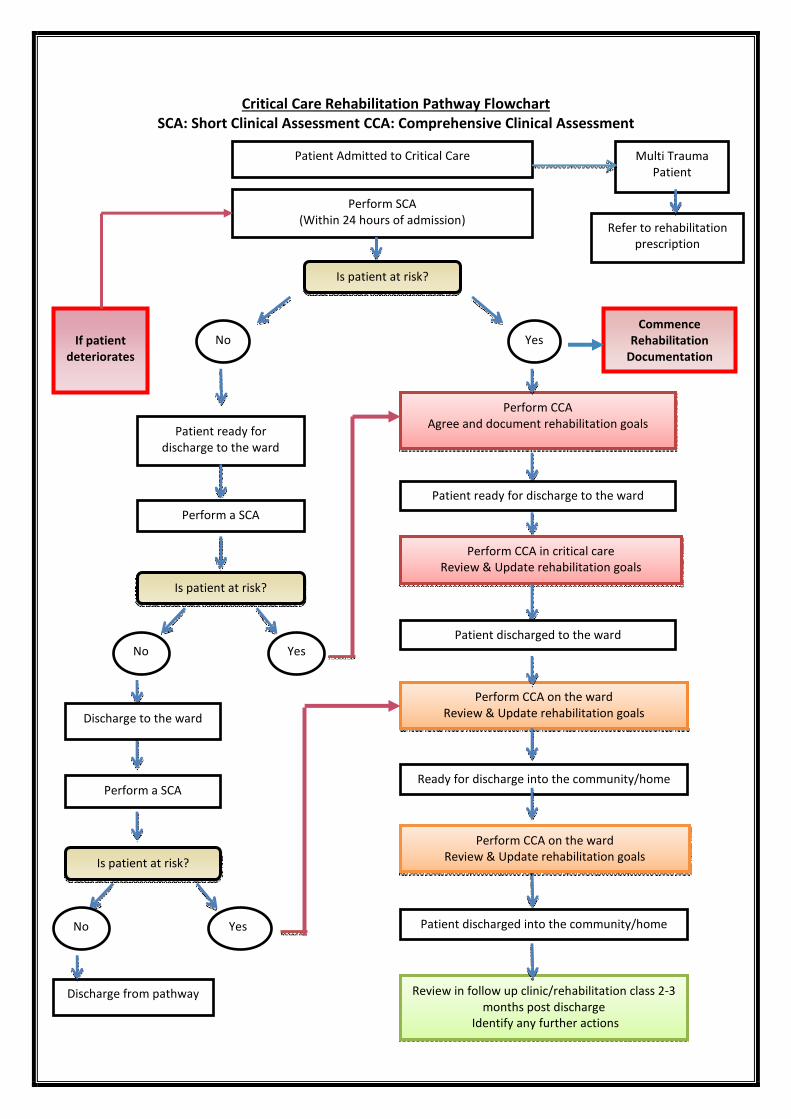
Critical Care Rehabilitation Pathway Flowchart
SCA: Short Clinical Assessment CCA: Comprehensive Clinical Assessment
Patient Admitted to Critical Care
Perform SCA
(Within 24 hours of admission)
Multi Trauma
Patient
Is patient at risk?
No Yes
Perform CCA
Agree and document rehabilitation goals
If patient
deteriorates
Patient ready for
discharge to the ward
Perform a SCA
Refer to rehabilitation
prescription
Patient ready for discharge to the ward
Perform CCA in critical care
Review & Update rehabilitation goals
Perform CCA on the ward
Review & Update rehabilitation goals
Ready for discharge into the community/home
Review in follow up clinic/rehabilitation class 2-3
months post discharge
Identify any further actions
Perform CCA on the ward
Review & Update rehabilitation goals
No
Discharge from pathway
Discharge to the ward
No Yes Patient discharged into the community/home
Patient discharged to the ward
Commence
Rehabilitation
Documentation
Yes
Perform a SCA
Is patient at risk?
Is patient at risk?
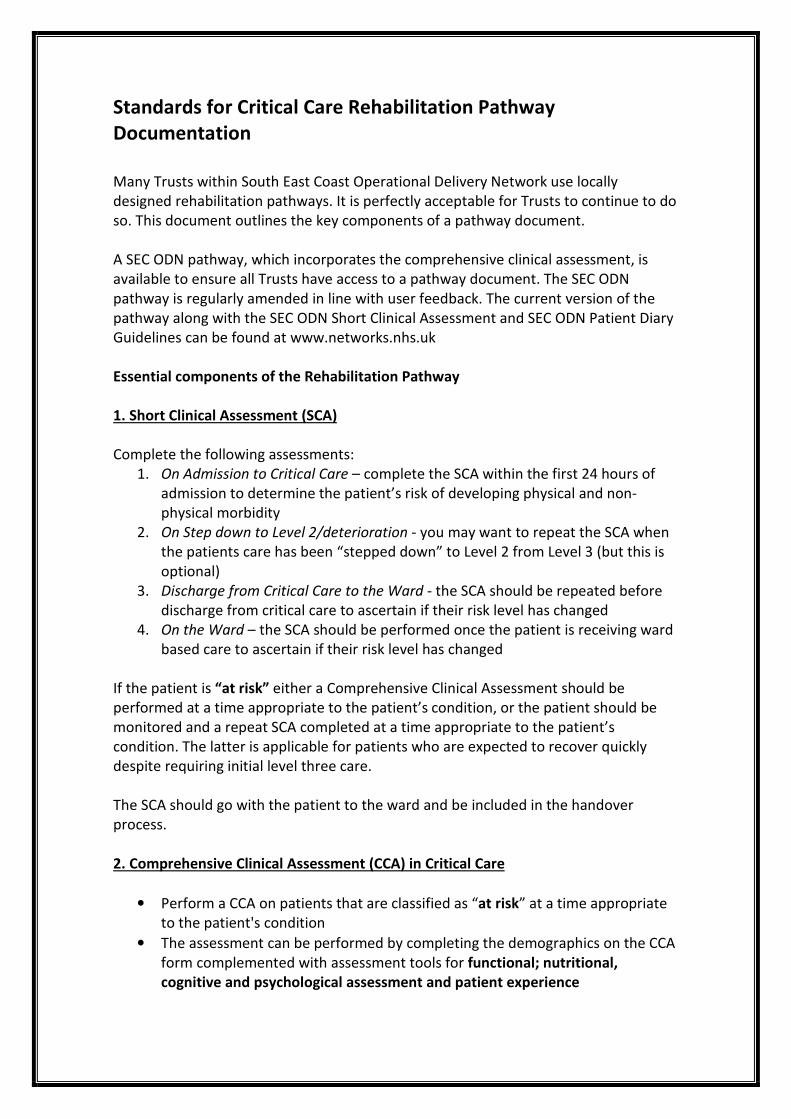
Standards for Critical Care Rehabilitation Pathway
Documentation
Many Trusts within South East Coast Operational Delivery Network use locally
designed rehabilitation pathways. It is perfectly acceptable for Trusts to continue to do
so. This document outlines the key components of a pathway document.
A SEC ODN pathway, which incorporates the comprehensive clinical assessment, is
available to ensure all Trusts have access to a pathway document. The SEC ODN
pathway is regularly amended in line with user feedback. The current version of the
pathway along with the SEC ODN Short Clinical Assessment and SEC ODN Patient Diary
Guidelines can be found at www.networks.nhs.uk
Essential components of the Rehabilitation Pathway
1. Short Clinical Assessment (SCA)
Complete the following assessments:
1. On Admission to Critical Care – complete the SCA within the first 24 hours of
admission to determine the patient’s risk of developing physical and non-
physical morbidity
2. On Step down to Level 2/deterioration - you may want to repeat the SCA when
the patients care has been “stepped down” to Level 2 from Level 3 (but this is
optional)
3. Discharge from Critical Care to the Ward - the SCA should be repeated before
discharge from critical care to ascertain if their risk level has changed
4. On the Ward – the SCA should be performed once the patient is receiving ward
based care to ascertain if their risk level has changed
If the patient is “at risk” either a Comprehensive Clinical Assessment should be
performed at a time appropriate to the patient’s condition, or the patient should be
monitored and a repeat SCA completed at a time appropriate to the patient’s
condition. The latter is applicable for patients who are expected to recover quickly
despite requiring initial level three care.
The SCA should go with the patient to the ward and be included in the handover
process.
2. Comprehensive Clinical Assessment (CCA) in Critical Care
• Perform a CCA on patients that are classified as “at risk” at a time appropriate
to the patient's condition
• The assessment can be performed by completing the demographics on the CCA
form complemented with assessment tools for functional; nutritional,
cognitive and psychological assessment and patient experience
• A functional assessment should be performed by the physiotherapist in order
to focus the physiotherapy goals to facilitate the patient’s rehabilitation
• Identify specific rehabilitation goals not already specified in the nursing,
physiotherapy or medical care plan
• Short and medium term rehabilitation goals should be agreed, whenever
possible, with the patient, and ideally involving the patient's family and/or
carer. The goals are to be documented within the pathway along with progress
notes and any referrals that have been made to facilitate the patient's full
recovery
• Reassess the patient when the clinical condition is indicated
The SEC ODN pathway contains examples of assessment tools; they are not mandatory
for use and can be replaced by your own assessment/tools as long as they are
validated tools. Assessment tools are to be used to direct and support clinical
assessment as appropriate.
Stages of the Rehabilitation Pathway
Whilst in Critical Care
Rehabilitation should include measures to prevent avoidable physical and non-physical
morbidity and to facilitate recovery from identified physical and non-physical
morbidity related to the patient's episode of critical illness.
Referral Considerations:
Dietician
Pharmacist
Speech and Language Therapist
Occupational Therapist
Patient diaries should be completed for patients in line with Trust guidelines and all
patients should receive both written and spoken information about their critical care
stay.
On discharge from Critical Care
A CCA and functional assessment should be performed and the patient’s short and
medium term rehabilitation goals should be reassessed with the patient, ideally
involving the patient’s family and/or carer. The goals are documented within the
pathway along with progress notes and any referrals that have been made to facilitate
the patient's full recovery.
An individualised rehabilitation manual plan should be available and given to the
patient, at the point in their pathway appropriate to their rehabilitation needs, offering
them a structured and supported rehabilitation programme for at least 6 weeks
following their discharge from critical care. The manual may contain general advice,
techniques to overcome cognitive dysfunctions and a programme of exercise.
It may be appropriate to return and discuss the patient diary at this point; however,
not all patients will be “ready” for this. Some patients may wish to continue their diary
whilst on the ward.
Information must be given to the patient and their family and/or carer about
transition from critical care to the ward environment.
Referral Considerations:
Dietician
Pharmacist
Speech and Language Therapist
Occupation Therapist
Rehabilitation Lead
Ensure that a formal structured handover of patient care is in line with “Acutely ill
patients in hospital” (NICE CG50). This should include the formal handover of the
individualised, structured rehabilitation programme.
During ward based care
A CCA and functional assessment should be performed and the patient’s current
rehabilitation needs and goals identified with the patient, ideally involving the
patient's family and/or carer. The goals are documented within the pathway along
with progress notes and any referrals that have been made to facilitate the patient’s
full recovery. The patients’ rehabilitation goals should be documented to inform all
staff involved with their care.
Review the possibility of retuning and discussing the patient diary.
Give the patient their rehabilitation manual if appropriate.
Give the patient written and spoken information about their critical care stay.
Referral Considerations:
Dietician
Pharmacist
Speech and Language – swallow assessment
Community Occupation Therapist
Clinical psychology
Before Discharge to home
A CCA and functional assessment should be performed and based on this assessment
the patients rehabilitation goals in their individualised manual are reviewed updated
and new goals agreed with the patient.
Review the possibility of returning and discussing the patient diary.
Give the patient their rehabilitation manual if appropriate.
Give the patient a copy of their critical care discharge summary.
Give the patient written and spoken information about discharge arrangements and
any referrals for ongoing care and general guidance on what to expect at home
(including returning to work, driving and local support services).
Ensure all discharge documents are completed and forwarded to the appropriate
discharge services.
Check the information booklet(s) have been given to the patient or family.
Give the patient and family the opportunity to provide feedback about their
experience of Critical Care and Critical Care rehabilitation.
Referral Considerations:
Social Worker – social assessment
Community Physiotherapist
Community Occupational Therapist
District Nurse
Dietician
Clinical Psychology
Follow up 2/3 months after discharge from hospital
The location of the follow up assessment will be influenced by the Trusts' provision for
rehabilitation. The assessment should ideally be face to face in the hospital or
community setting, performed by an appropriately skilled healthcare professional who
is familiar with the patients critical care problems and rehabilitation pathway.
At the follow up the patient is assessed, combining the comprehensive clinical
assessment and other functional assessment tools as per Trust policy, to determine
on-going health and social care needs.
In Trusts where a rehabilitation class is available, provision must be made to ensure
the follow up of patients who do not attend the class.
Give the patient and family the opportunity to provide feedback about their
experience of Critical Care and Critical Care rehabilitation.
Tools to help with Assessment These tools are to assist with the assessment of the patients; they are not diagnostic
tools but merely give an indication of potential problems. They then can provide a
baseline on which to formulate the rehabilitation goals.
HADS The higher the score in the assessment the greater the indication the patient may be
suffering with some form of depression and/or anxiety.
PTSD The higher the score in the assessment the greater the indication the patient may be
suffering with some form of Post-Traumatic Stress Disorder
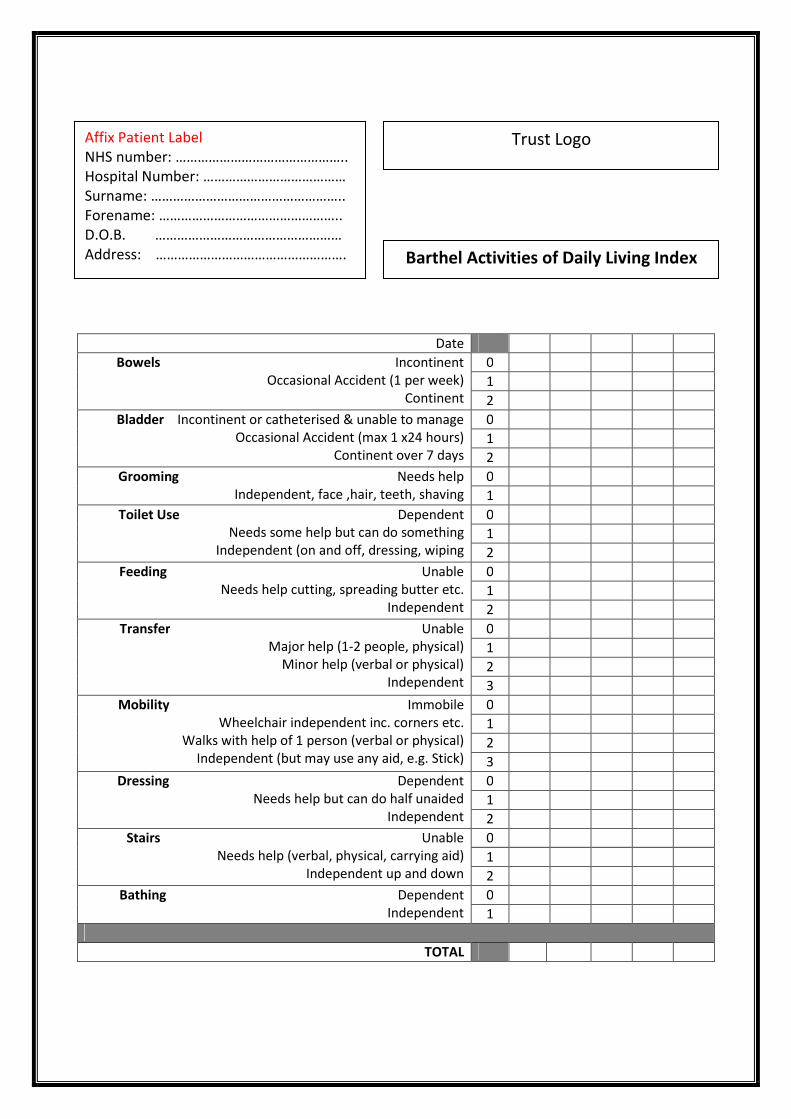
Barthel Activities of Daily Living Index This tool helps you assess patients’ ability to perform the activities of daily living. The
higher the score the more independent the patient and low scores highlights areas
that can be improved.
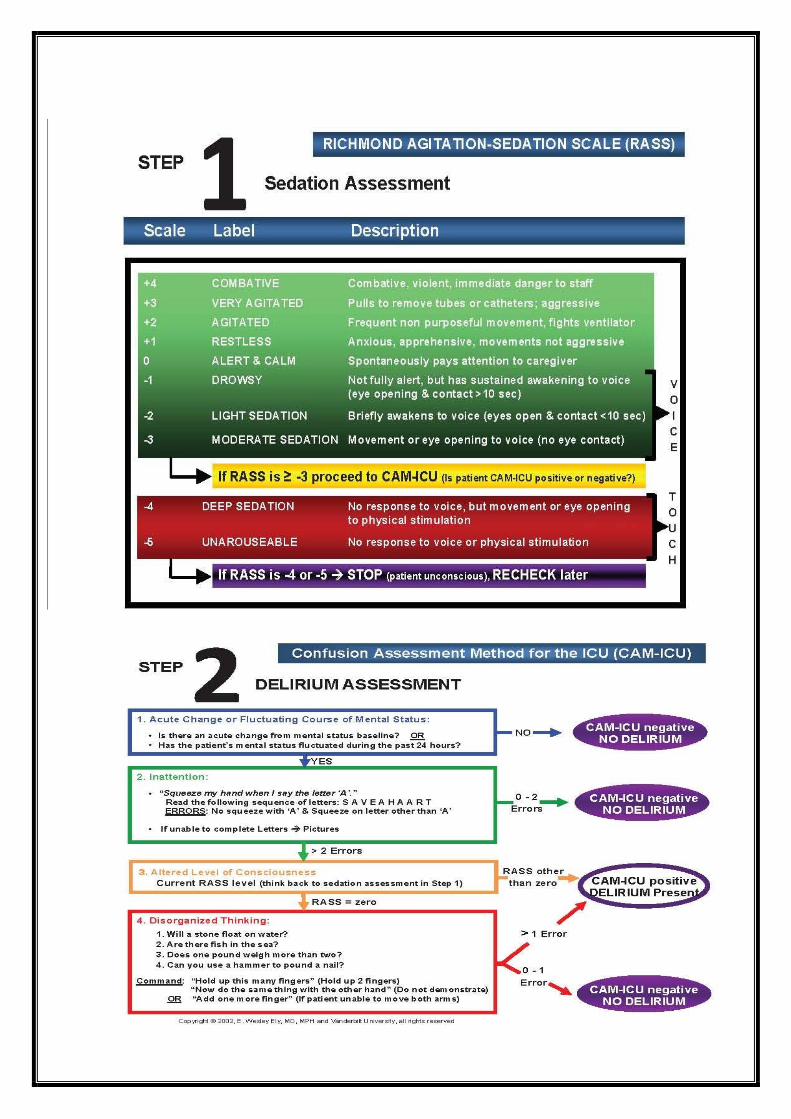
RASS SCORE & CAM – ICU SCORE This tool is to assist in the monitoring of delirium for ICU patients. The Confusion
Assessment Method for the ICU (CAM-ICU) and the Intensive Care Delirium Screening
Checklist (ICDSC) are well validated delirium assessment tools. For further information
please refer to www.icudelirium.org
CPAx Physiotherapy Assessment Tool The Chelsea Critical Care assessment tool. A tool to measure physical morbidity in the
general adult critical care patient.
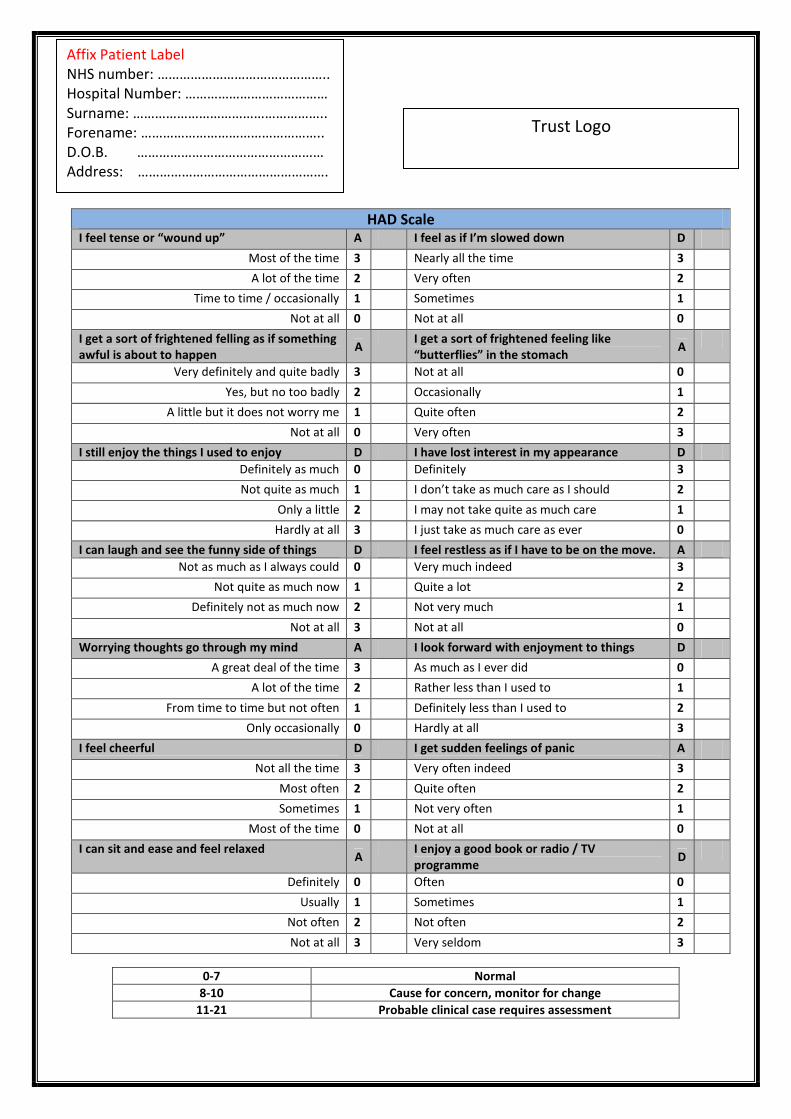
HAD Scale I feel tense or “wound up” A I feel as if I’m slowed down D
Most of the time 3 Nearly all the time 3 A lot of the time 2 Very often 2
Time to time / occasionally 1 Sometimes 1 Not at all 0 Not at all 0
I get a sort of frightened felling as if something
awful is about to happen A
I get a sort of frightened feeling like
“butterflies” in the stomach A
Very definitely and quite badly 3 Not at all 0 Yes, but no too badly 2 Occasionally 1
A little but it does not worry me 1 Quite often 2 Not at all 0 Very often 3
I still enjoy the things I used to enjoy D I have lost interest in my appearance D
Definitely as much 0 Definitely 3 Not quite as much 1 I don’t take as much care as I should 2
Only a little 2 I may not take quite as much care 1 Hardly at all 3 I just take as much care as ever 0
I can laugh and see the funny side of things D I feel restless as if I have to be on the move. A
Not as much as I always could 0 Very much indeed 3 Not quite as much now 1 Quite a lot 2
Definitely not as much now 2 Not very much 1 Not at all 3 Not at all 0
Worrying thoughts go through my mind A I look forward with enjoyment to things D A great deal of the time 3 As much as I ever did 0
A lot of the time 2 Rather less than I used to 1 From time to time but not often 1 Definitely less than I used to 2
Only occasionally 0 Hardly at all 3 I feel cheerful D I get sudden feelings of panic A
Not all the time 3 Very often indeed 3 Most often 2 Quite often 2 Sometimes 1 Not very often 1
Most of the time 0 Not at all 0 I can sit and ease and feel relaxed
A I enjoy a good book or radio / TV
programme D
Definitely 0 Often 0 Usually 1 Sometimes 1
Not often 2 Not often 2 Not at all 3 Very seldom 3
0-7 Normal
8-10 Cause for concern, monitor for change
11-21 Probable clinical case requires assessment
Affix Patient Label
NHS number: ………………………………………..
Hospital Number: …………………………………
Surname: ……………………………………………..
Forename: …………………………………………..
D.O.B. ……………………………………………
Address: …………………………………………….
………………………………………………………………
Trust Logo
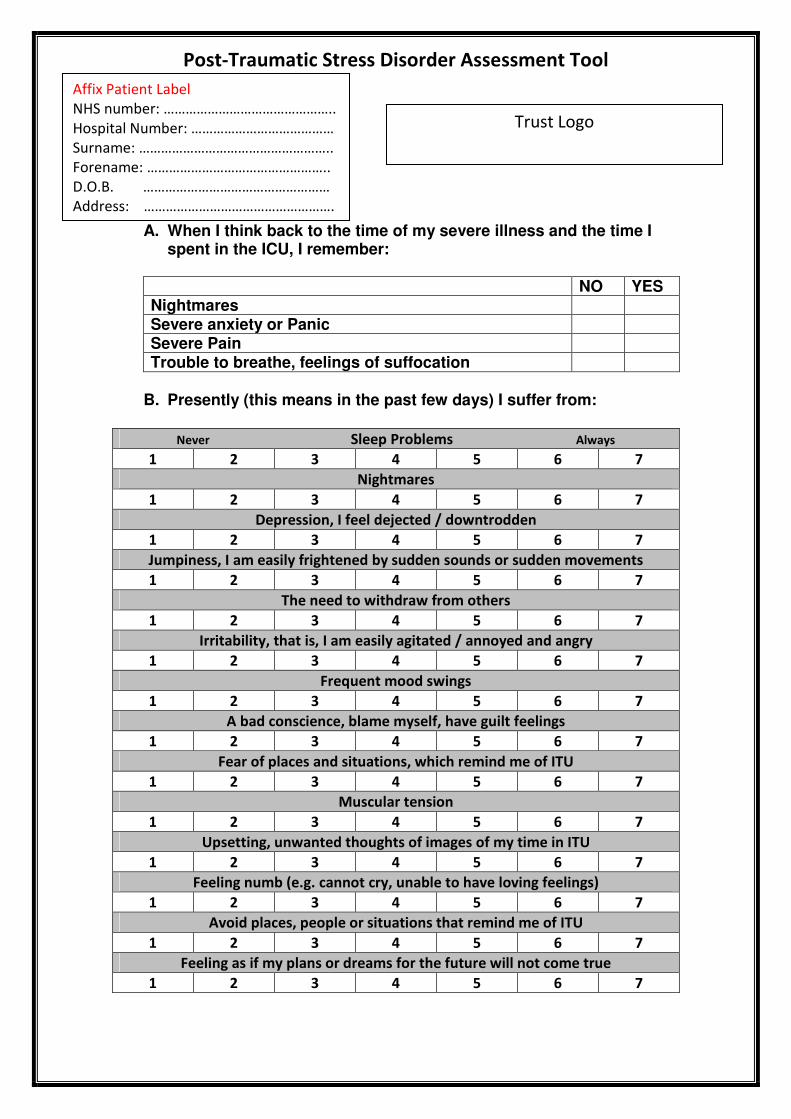
Post-Traumatic Stress Disorder Assessment Tool
A. When I think back to the time of my severe illness and the time I spent in the ICU, I remember:
NO YES Nightmares Severe anxiety or Panic Severe Pain Trouble to breathe, feelings of suffocation
B. Presently (this means in the past few days) I suffer from:
Never Sleep Problems Always
1 2 3 4 5 6 7
Nightmares
1 2 3 4 5 6 7
Depression, I feel dejected / downtrodden
1 2 3 4 5 6 7
Jumpiness, I am easily frightened by sudden sounds or sudden movements
1 2 3 4 5 6 7
The need to withdraw from others
1 2 3 4 5 6 7
Irritability, that is, I am easily agitated / annoyed and angry
1 2 3 4 5 6 7
Frequent mood swings
1 2 3 4 5 6 7
A bad conscience, blame myself, have guilt feelings
1 2 3 4 5 6 7
Fear of places and situations, which remind me of ITU
1 2 3 4 5 6 7
Muscular tension
1 2 3 4 5 6 7
Upsetting, unwanted thoughts of images of my time in ITU
1 2 3 4 5 6 7
Feeling numb (e.g. cannot cry, unable to have loving feelings)
1 2 3 4 5 6 7
Avoid places, people or situations that remind me of ITU
1 2 3 4 5 6 7
Feeling as if my plans or dreams for the future will not come true
1 2 3 4 5 6 7
Affix Patient Label
NHS number: ………………………………………..
Hospital Number: …………………………………
Surname: ……………………………………………..
Forename: …………………………………………..
D.O.B. ……………………………………………
Address: …………………………………………….
Trust Logo
Date
Bowels Incontinent
Occasional Accident (1 per week)
Continent
0
1
2
Bladder Incontinent or catheterised & unable to manage
Occasional Accident (max 1 x24 hours)
Continent over 7 days
0
1
2
Grooming Needs help
Independent, face ,hair, teeth, shaving
0
1
Toilet Use Dependent
Needs some help but can do something
Independent (on and off, dressing, wiping
0
1
2
Feeding Unable
Needs help cutting, spreading butter etc.
Independent
0
1
2
Transfer Unable
Major help (1-2 people, physical)
Minor help (verbal or physical)
Independent
0
1
2
3
Mobility Immobile
Wheelchair independent inc. corners etc.
Walks with help of 1 person (verbal or physical)
Independent (but may use any aid, e.g. Stick)
0
1
2
3
Dressing Dependent
Needs help but can do half unaided
Independent
0
1
2
Stairs Unable
Needs help (verbal, physical, carrying aid)
Independent up and down
0
1
2
Bathing Dependent
Independent
0
1
TOTAL
Affix Patient Label
NHS number: ………………………………………..
Hospital Number: …………………………………
Surname: ……………………………………………..
Forename: …………………………………………..
D.O.B. ……………………………………………
Address: …………………………………………….
Trust Logo
Barthel Activities of Daily Living Index
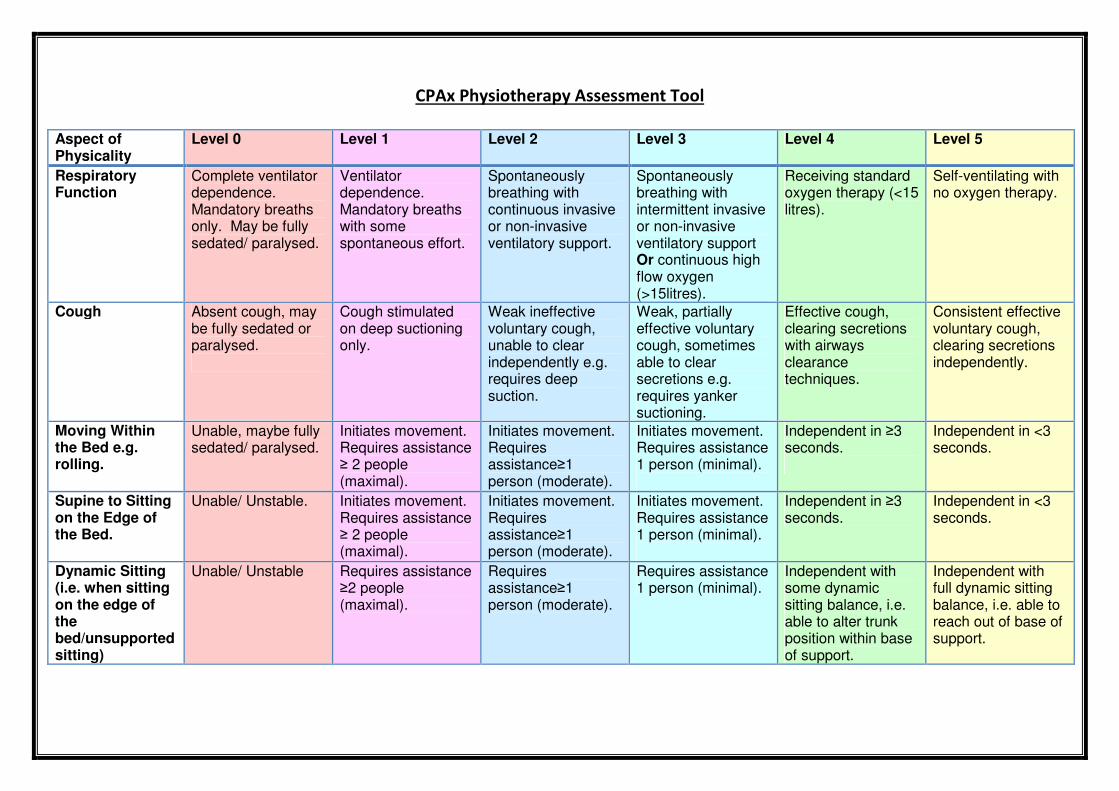
CPAx Physiotherapy Assessment Tool
Aspect of Physicality
Level 0 Level 1 Level 2 Level 3 Level 4 Level 5
Respiratory Function
Complete ventilator dependence. Mandatory breaths only. May be fully sedated/ paralysed.
Ventilator dependence. Mandatory breaths with some spontaneous effort.
Spontaneously breathing with continuous invasive or non-invasive ventilatory support.
Spontaneously breathing with intermittent invasive or non-invasive ventilatory support Or continuous high flow oxygen (>15litres).
Receiving standard oxygen therapy (<15 litres).
Self-ventilating with no oxygen therapy.
Cough Absent cough, may be fully sedated or paralysed.
Cough stimulated on deep suctioning only.
Weak ineffective voluntary cough, unable to clear independently e.g. requires deep suction.
Weak, partially effective voluntary cough, sometimes able to clear secretions e.g. requires yanker suctioning.
Effective cough, clearing secretions with airways clearance techniques.
Consistent effective voluntary cough, clearing secretions independently.
Moving Within the Bed e.g. rolling.
Unable, maybe fully sedated/ paralysed.
Initiates movement. Requires assistance ≥ 2 people (maximal).
Initiates movement. Requires assistance≥1 person (moderate).
Initiates movement. Requires assistance 1 person (minimal).
Independent in ≥3 seconds.
Independent in <3 seconds.
Supine to Sitting on the Edge of the Bed.
Unable/ Unstable. Initiates movement. Requires assistance ≥ 2 people (maximal).
Initiates movement. Requires assistance≥1 person (moderate).
Initiates movement. Requires assistance 1 person (minimal).
Independent in ≥3 seconds.
Independent in <3 seconds.
Dynamic Sitting (i.e. when sitting on the edge of the bed/unsupported sitting)
Unable/ Unstable Requires assistance ≥2 people (maximal).
Requires assistance≥1 person (moderate).
Requires assistance 1 person (minimal).
Independent with some dynamic sitting balance, i.e. able to alter trunk position within base of support.
Independent with full dynamic sitting balance, i.e. able to reach out of base of support.
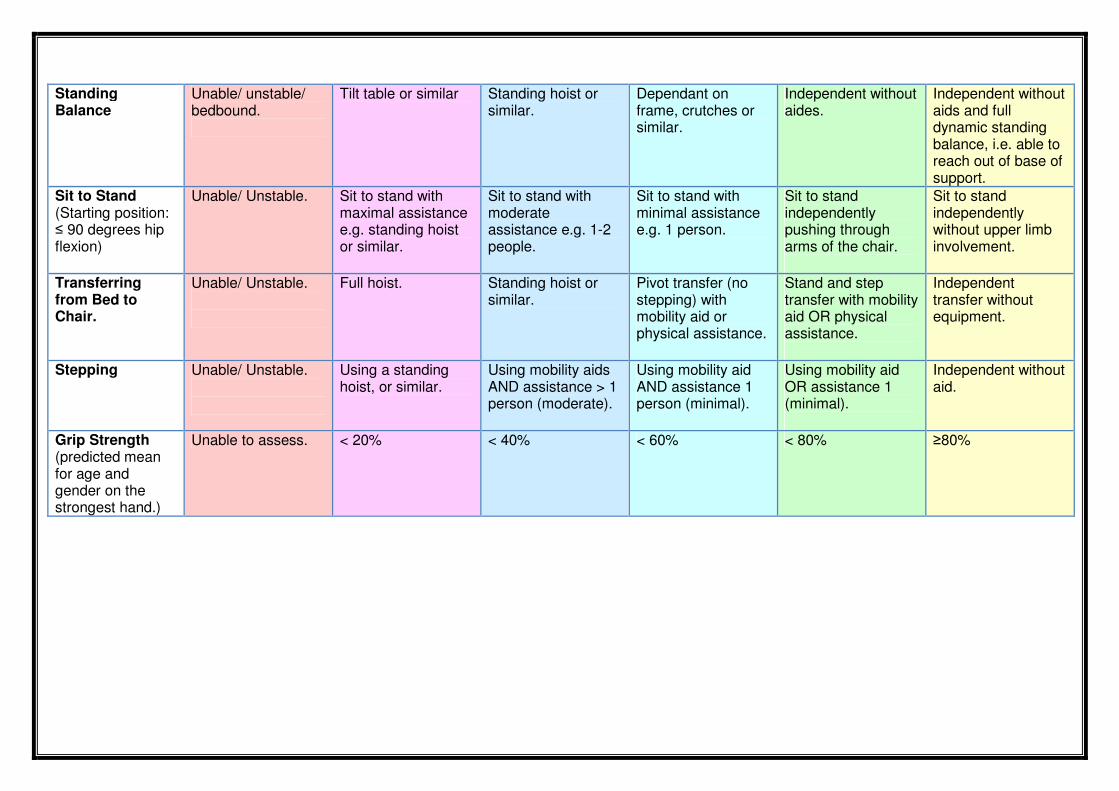
Standing Balance
Unable/ unstable/ bedbound.
Tilt table or similar Standing hoist or similar.
Dependant on frame, crutches or similar.
Independent without aides.
Independent without aids and full dynamic standing balance, i.e. able to reach out of base of support.
Sit to Stand (Starting position: ≤ 90 degrees hip flexion)
Unable/ Unstable. Sit to stand with maximal assistance e.g. standing hoist or similar.
Sit to stand with moderate assistance e.g. 1-2 people.
Sit to stand with minimal assistance e.g. 1 person.
Sit to stand independently pushing through arms of the chair.
Sit to stand independently without upper limb involvement.
Transferring from Bed to Chair.
Unable/ Unstable.
Full hoist. Standing hoist or similar.
Pivot transfer (no stepping) with mobility aid or physical assistance.
Stand and step transfer with mobility aid OR physical assistance.
Independent transfer without equipment.
Stepping Unable/ Unstable.
Using a standing hoist, or similar.
Using mobility aids AND assistance > 1 person (moderate).
Using mobility aid AND assistance 1 person (minimal).
Using mobility aid OR assistance 1 (minimal).
Independent without aid.
Grip Strength (predicted mean for age and gender on the strongest hand.)
Unable to assess. < 20% < 40% < 60% < 80% ≥80%
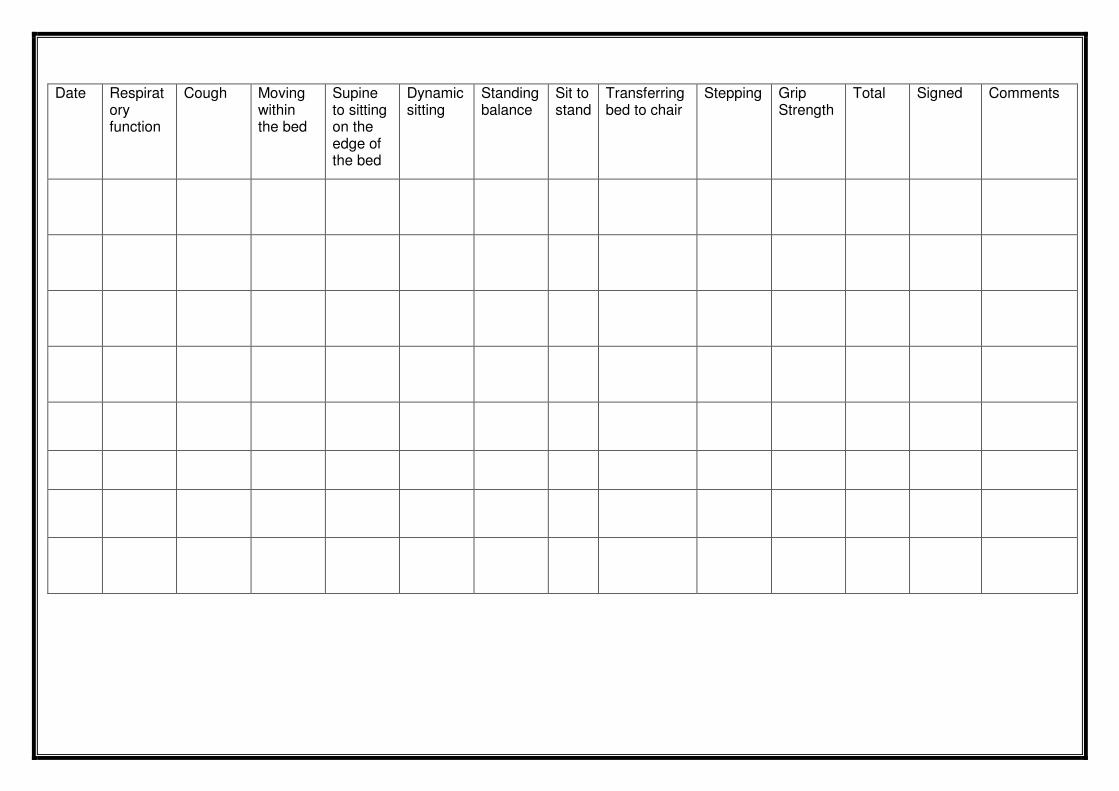
Date Respiratory function
Cough Moving within the bed
Supine to sitting on the edge of the bed
Dynamic sitting
Standing balance
Sit to stand
Transferring bed to chair
Stepping Grip Strength
Total Signed Comments
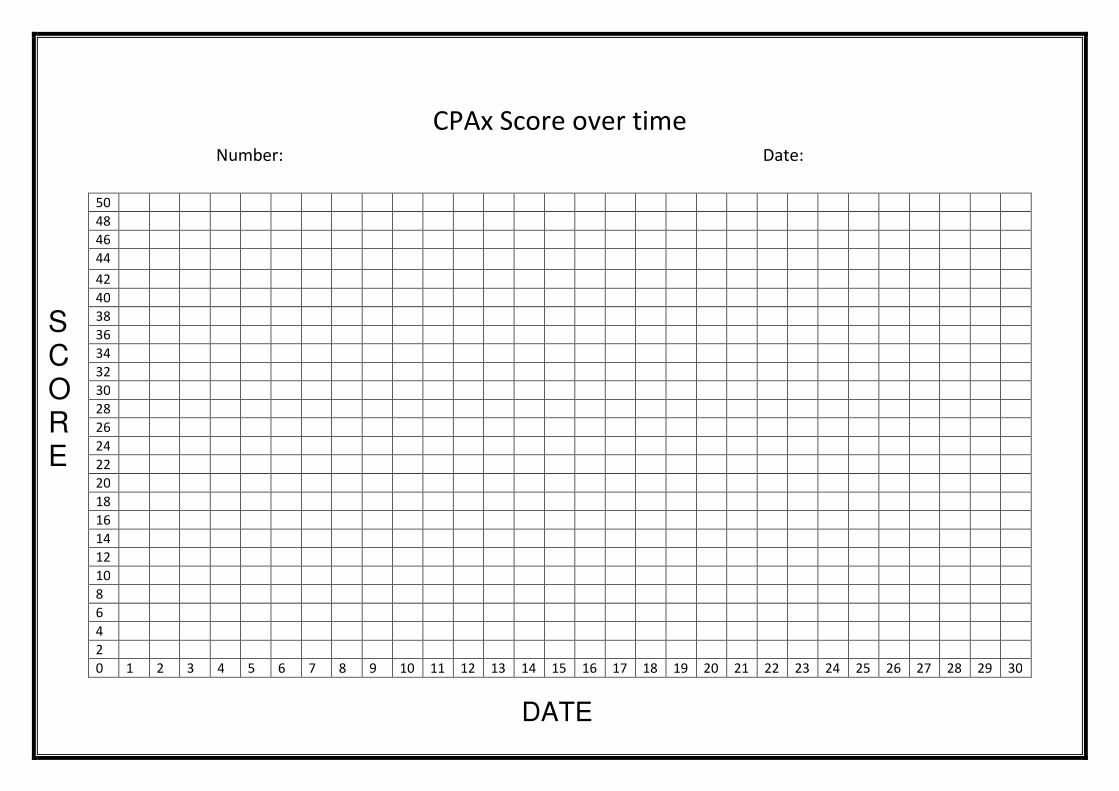
CPAx Score over time
Number: Date:
50
48
46
44
42
40
38
36
34
32
30
28
26
24
22
20
18
16
14
12
10
8
6
4
2
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30
DATE
SCORE





























