Embed Size (px)
DESCRIPTION
Citation preview

Critical Thinking in Medicine
Eric S. Farbman, MD

Parkinson’s Disease:Bogus Treatments
Eric S. Farbman, MD

Hoaxes, Scams, Quackery
• Non-medical treatments without proven benefit
• Medical fraud
• Designed to enrich the promoter of the treatment more so than the patient
• In some cases, these can be dangerous to the health of the patient as well

Why Are People Vulnerable?
• Lack of suspicion—if it is on television, the internet, etc., then it must be true
• Overconfidence—some people believe that they are better equipped than scientists in determining whether something works
• Desperation—the sincere hope that something works when nothing else has
• Conspiracy—distrustful of the medical profession but attracted to “natural” methods

Why Do the Methods Seem to Work?• There is a poor grasp of innate probability
– In a group of 23 people, what are the odds that two share the same birthday?
• There is a belief that all effects must have deliberate causes
• There is a tendency towards selective memory
• There is the placebo effect
• There is a desire to please the individual
• There is the natural course of the disease

What is Quackery?
• It is the promotion of methods that have no evidence and lack a scientific rationale
• Malpractice usually involves negligence rather than fraud
• Some promoters are scam artists, some are blind “true believers”

Types of Hoax Treatments
• Vitamins/Supplements
• Procedures
• “Alternative medicine” practitioners

Supplements

Getting a Medication Approved• Since 1938, every medication has to go
through a New Drug Application (NDA) process before getting approval in the U.S.
• The goals of the NDA are:– Is the drug safe and effective for its proposed use,
and do the benefits outweigh the risks?– Is the labelling (package insert) appropriate, and
what should it contain?– Are the manufacturing methods adequate to
maintain the drug’s identity, strength, and purity?

Studies Required by the FDA
• First the sponsor must submit data showing that the drug is reasonably safe for use in small-scale clinical studies
• At this pre-clinical stage, the FDA will ask for:– A pharmacological profile of the drug– Determine acute toxicity in at least two species of
animals– Conduct short-term toxicity studies ranging from
two weeks to three months

Studies Required by the FDA:On the Road to Drug Approval
• Phase I: Develop drug’s safety profile– Normally subjects are healthy volunteers– Determines how drug is absorbed, distributed in
the body, metabolized, and excreted
• Phase II: Determine the drug’s safety and assess side effects– Given to volunteers who have the disease– Determine optimal dosage of the drug

Studies Required by the FDA:On the Road to Drug Approval
• Phase III: Verify the effectiveness of the drug against the condition that it targets– This also continues to investigate the safety of the
drug and record possible side effects and adverse reactions from long-term use.
– These studies are randomized, double-blind, placebo-controlled studies.
– Often have at least 1000 patients enrolled– If the medication is effective, the trial is deemed
successful—“pivotal”. Normally two pivotal trials are needed to ensure validity of the trials

Studies Required by the FDA:After Drug Approval
• Phase IV: Once the drug is on the market, the company must continue to perform observational studies to evaluate the drug’s safety during routine use.– The company may also monitor any usage of the
drug for un-approved indications.– Trials may be done based on those usages, but the
company CANNOT advertise “off-label” use


Studies Required forSupplement Approval

Health and Education Act of 1994• Defined a dietary supplement as:
– A product (other than tobacco) that is intended to supplement the diet
– Is intended for ingestion in pill, capsule, tablet, or liquid form
– Is not represented for use as a conventional food– Is labelled as a “dietary supplement”
• Nutritional support statements do not have to be approved by the FDA
• This law has made it very difficult for the FDA to ban dangerous dietary supplements.

“Legitimate” Supplements
• Vitamin E
• Gluathione
• Coenzyme Q10
• Vitamin B6
• Folic Acid
Which of these agents has a double-blind trial that supports its benefit in PD?

CoEnzyme Q10

CoEnzyme Q10
• Eighty people in study
• Randomized to placebo, 300mg/day, 300mg twice/day, 300mg 4x/day
• Followed for 16 months or until the patient needed treatment with levodopa
• Primary variable was a change in UPDRS
• Statistically signifcant benefits seen at highest dose, trending towards benefit at lower doses

Why Is CoQ10 Thought to Work?
• Causes of Parkinson’s Disease are not known
• Thought to be at least partially due to oxidation (“rusting”) of the brain
• CoQ10 is a potent anti-oxidant
• So, what about other anti-oxidants?

Vitamin E• One of the few supplements to have a well-
designed negative trial
• Original selegiline trials had four arms– Selegiline/Placebo– Selegiline/Vitamin E– Placebo/Vitamin E– Placebo/Placebo
• No effect on progression of PD by itself
• No enhancement of selegiline in combination

Glutathione
• 9 patients with early, untreated PD were given IV gluathione 600mg twice/day for 30 days
• All improved significantly after therapy as measured by CURS– Evaluates rigidity, tremor, speech, facial
expression, bradykinesia, gait, postural stability
• After 30 days of therapy were completed, the therapeutic effect lasted an additional 2 months

Problems with Gluathione Study
• Very small sample size
• No control group—no placebo arm
• Original study done in 1996; where are the follow-up studies?
Per
cen
tage
of
Pat
ien
ts *
†‡
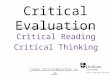
TREAT RLS US1
TREAT RLS 12
TREAT RLS 23
n=187 n=193 n=146 n=137 n=131 n=134
73%
53%60%
41%
57%
40%
0
20
40
60
80
100
Ropinirole (n=464)
Placebo (n=464)
n=187 n=193 n=146 n=137 n=131 n=134


Less Reputable Supplements




Other Treatments
• Prakotin– I’m not sure what it is– It shows up on some websites– The word “prakotin” does not show up in the
medline database



Low Dose Naltrexone
• Naltrexone was approved by the FDA in 1984
• Dose was 50mg for the purpose of helping heroin or opium addicts– Works by blocking opioid receptors
• Supposedly a smaller dose (4.5mg) enhances the body’s immune system and its response to many diseases including Parkinson’s disease

Low Dose Naltrexone (cont’d)
• There is nothing in the literature to support its use in neurological disease
• There is virtually nothing in the literature to support its use in anything
• Any benefits reported for Parkinson disease are purely anecdotal

LDN in the Medical Literature


“Medical” Procedures

Chelation
• A chelator is an organic compound that forms stable bonds with metal atoms.
• They often are used for acute metal toxicity
• Often times they have serious side effects

Chelating Agents
• Dimercaprol– Given intramuscularly– Used for arsenic, lead, mercury, cadmium poisoning– Side effects: Headache, nausea, vomiting
• Penicillamine– Treatment for copper poisoning and Wilson’s disease– Side effects: Aplastic anemia, lupus, hemolytic anemia

Chelating Agents (cont’d)• Edetate (EDTA)
– Possible chelator of many things– Usually used for lead poisoning– Side effect: nephrotoxicity
• Deferoxamine– Used for acute iron intoxication– Does not cross blood brain barrier– Side effects: skin reactions, neurotoxicity (i.e.
retinal degeneration), hepatic and renal dysfunction, severe coagulopathies, hypotensive shock

Chelation Therapy• There are no trials that show any benefit in PD
• Even if we assume that excess iron is part of the pathology, there is no chelator that can effectively cross into the brain to remove this iron without side effects
• There are well-designed trials for other conditions which have yielded negative results
• Using chelation instead of proven treatments (i.e. CABG) can have fatal consequences


Hyperbaric Medicine
• The delivery of pressurized oxygen to the body
• Useful (and approved) for treating– Decompression sickness (“The Bends”)– Carbon Monoxide Poisoning– Cyanide poisoning– Burns– Necrotizing soft tissue infections

Hyperbaric Medicine in PD
• 2 abstracts/articles from various International Congresses on Hyperbaric Medicine
• One article (originally in Russian literature)
• All supposedly show benefit

Hyperbaric in PD: Abstract 1• 72 y.o. male diagnosed with idiopathic PD
• Started on sinemet 10/100 three times/day
• Eighteen months after diagnosis, he started on hyperbaric oxygenation and had great results. He was also able to come off of his sinemet
• Problems:– Dose of sinemet is insufficient– Disease is probably mild at time of treatment– Scale used to rate improvement is not validated

Hyperbaric in PD: Abstract 2
• Fifteen patients (8 men, 7 women)– Etiology of PD:
• 7 idiopathic
• 4 vasculopathic
• 3 post-encephalic
• 1 other kind
– No controls– Nothing said about medication changes– Difficult to know what to make of results

Hyperbaric in PD: Russian article• 64 patients (29 men, 35 women)• Duration of illness ranged from 1 – 15 years• Etiology
– Atherosclerosis of cerebral vessels in 49 patients
– This combined with arterial hypertension in 6
– History of encephalitis in 8
– Closed head trauma in 1
• Results:– “Good treatment results were noted in 18…”
– “Therapeutic effect was considered satisfactory in 26…”
– No measurement scales of any kind were used!

Other Devices with No FDA Approved Indications



“Alternative Medicine” Practitioners

Acupuncture
• One study on alternative medicine use in PD shows that 10% of patients will try acupuncture
• An open-label trial of 25 patients with idiopathic PD were followed for 6 months– No significant improvement in treatment measures– 2.4 worsening on UPDRS motor scores– 16% improvement in quality of life scale– 29% improvement on depression scale

Acupuncture (cont’d)
• Because of this, a randomized, controlled double-blind study was done.
• 14 patients were enrolled
• There were no statistically significant changes in the outcomes measured
• In the patients who received true acupuncture, there was a trend towards improvement in the quality of life scale

Acupuncture (cont’d)• One study compared two groups, differing the
number of treatments between them• There were no differences on the Parkinson
motor scales, quality of life scales, or psychiatric symptoms measurements
• A recent meta-analysis of all acupuncture in PD was published– “Evidence for acupuncture…is not convincing.”– Sample sizes are too small to draw conclusions– No evidence for acupuncture vs. placebo
adjustments or acupuncture + drugs vs. drugs only

Chiropractic
“What are the principal functions of the spine?
To support the head To support the ribs To support the chiropractor.”
BJ Palmer, 1952,Questions and Answers about Chiropractic

Chiropractic Principles• Many chiropractors are against
– childhood vaccinations– medications in general
• There are chiropractors who claim that their adjustments can fix– ear infections– asthma– just about everything
• Many chiropractor recommend supplements which they themselves sell

Evidence-Based Analysis of Some Chiropractic Practices
• Full spine X-rays– There is no evidence to support the use of this– This is a large radiation exposure– The films are usually of poor quality
• Spinal manipulations– There is some evidence for benefit of lower spinal
manipulations; it is transient and similar to PT– There is no evidence for any other adjustments– There is no evidence for any benefit in children

What About Chiropractic with PD?
• If you do a web search, there will be over 3000 hits
• Many chiropractor websites talk about the scientific evidence of “upper cervical” adjustments in the treatment of PD
• They are all referring to the same article

The Articles

Examining the Literature• What do PD and MS have in common?
– Answer: They are both treated by neurologists.– Not much else that I can see
• Diagnostic tests used in this trial included paraspinal digital infrared imaging and laser-aligned radiography– Neither technique is supported by any medical literature– In 2000 after reviewing more than 2500 articles, the
AAN concluded that paraspinal imaging is “unacceptable as a clinical tool” for diagnosing low back pain or neuromuscular disease

Other Problems
• Patients were questioned for a history of head trauma (retrospective bias)
• There were no PD scales used in the analysis of how the patients did. It was based on subjective reports of patients and changes on the erroneous tests mentioned before
• Apparently all of the patients also had subluxations that were corrected

What is a Subluxation?• The definition varies even between chiropractors
The medical definition of a subluxation is where the bony surfaces of a joint no longer face each other exactly but remain partially aligned. This condition would not be amenable to chiropractic.
• In general, they are thought to cause “nerve interference” and are the cause of the problems
• Even though they are supposedly visible on x-rays, radiologists never mention them

So, Is the Chiropractor Doing Anything to Help in PD?
• The study listed above did not have a control group to control for placebo effect
• There is a study unrelated to chiropractic looking at the benefit of massage therapy
• 7 patients received eight 1-hr sessions of whole body massage over eight weeks
• Patients reported enjoying the massage and also reported benefits on quality of life surveys

Unfortunately, some physicians become quacks as well

Which Alternative Medicine Treatments Should Be Used?
• The terms conventional medicine and alternative medicine should not be used
• We should look at treatments as proven, experimental, or questionable
• From a 1998 JAMA editorial:“There is no alternative medicine. There is only scientifically
proven, evidence-based medicine supported by solid data or unproven medicine, for which scientific evidence is lacking. Whether a therapeutic practice is "Eastern" or "Western," is unconventional or mainstream…is irrelevant.”

ReferencesBorromeil A, et al. OTI (HBOT) efficiency in decompensated-complicated PD. In: Oriani G, Wattel F. Proceedings of the Twelfth International Congress on Hyperbaric Medicine, 1998.Cristian A, Katz M, Cutrone E, Walker RH. Evaluation of acupuncture in the treatment of PD: A double-blind pilot study. Movement Disorders
20(9): 1185-1188, 2005.Elster E. Eighty-one patients with MS and PD undergoing upper cervical chiropractic care to correct vertebral subluxation: A retrospective analysis. J Vertebral Subluxation Res 6:1-9, 2004.Elster E. Upper cervical chiropractic management of a patient with PD: A case report. Journal of Manipulative and Physiological Therapeutics 23(8): 573-577, 2000.Eng ML, Lyons KE, Greene MS, Pahwa R. Open-label trial regarding the use of acupuncture and Yin Tui Na in PD Outpatients: A pilot study
on efficacy, tolerability, and quality of life. Journal of Alternative and Complementary Medicine 12(4): 395-399, 2006.Fontanarosa PB, Lundberg GD. Alternative medicine meets science. JAMA 280:1618-1619, 1998.Hoggard ML, Johnson KE, Shirachi DY. Hyperbaric oxygen treatment of a PD patient: A case study. In: Cramer FS. Proceedings of the Fourteenth International Congress on Hyperbaric Medicine, 2003: 206-209.Lee MS, Shin B, Kong JC, Ernst E. Effectiveness of acupuncture for Parkinson disease: A systematic review. Movement Disorders 23(11):
1505-1515, 2008.Kaur D, Andersen JK. Ironing out PD: is therapeutic treatment with iron chelators a real possibility? Aging Cell 1: 17-21, 2002.Neretin VYa, Lobov MA, Kotov SV, Cheskidova GF, Molchanova GS. Hyperbaric oxygenation in comprehensive treatment of parkinsonism.
Neuroscience & Behavioral Physiology 20(6): 490-492, 1990.Parkinson Study Group. Effects of tocopherol and deprenyl on the progression of disability in early PD. New Engl J Med, 328: 176-183, 1993.Paterson C, Allen JA, Browning M, Barlow G, Ewings P. A pilot study of therapeutic massage for people with PD: The added value of user
involvement. Complementary Therapies in Clinical Practice 11: 161-171, 2005.Rajendran PR, Thompson RE, Reich SG. The use of alternative therapies by patients with Parkinson’s disease. Neurology 57: 790-794, 2001.Sechi G, et al. Reduced intravenous glutathione in the treatment of early PD. Prog Neuropsychopharmacol Biol Psychiatry 20: 1159-1170, 1996.Shulman LM, et al. Acupuncture therapy for the symptoms of PD. Movement Disorders 17(4): 799-802, 2002.Shults CW, et al. Effects of coenzyme Q10 in early PD: Evidence of slowing of the functional decline. Arch Neurol 59: 1541-1550, 2002.Smith JP, et al. Low-dose naltrexone therapy improves active Crohn’s disease. American Journal of Gastroenterology 102: 820-828, 2007.Weber C, Ernst ME. Antioxidants, supplements, and Parkinson’s disease. Annals of Pharmacotherapy 40: 935-938, 2006.Webpage: http://www.quackwatch.org

Questions?