Embed Size (px)
Citation preview

Brief Communication
Cross-cultural adaptation and validation of the Korean fibromyalgia impact
questionnaire in women patients with fibromyalgia for clinical research
Sang-Cheol Bae1 & Ji-Hyun Lee21Department of Internal Medicine, Division of Rheumatology, Hanyang University College of Medicine, TheHospital for Rheumatic Diseases, Seoul (E-mail: [email protected]); 2Department of Internal Medicine,Maryknoll Hospital, Busan, Korea
Accepted in revised form 1 May 2003
Abstract
Our aim was to translate and cross-culturally adapt the fibromyalgia impact questionnaire into Korean(KFIQ), and then evaluate its reliability and validity. The FIQ was translated into Korean by threetranslators and then independently translated back into English by three different translators. A total of 62women patients with fibromyalgia (FM) were studied for the psychometric properties of the KFIQ. Themean age of the patients was 47.1 (25–73) years, and all were female. The mean KFIQ score was 48.3 (17–91), and the mean Korean health assessment questionnaire (KHAQ) score was 0.4 (0–1.7). The test–retestreliability of the KFIQ yielded an intraclass correlation coefficient of 0.85 (0.53–0.96). For the constructvalidity, the Spearman rank correlations of KFIQ with patient global assessments using visual analog scale(pain, 0.58; morning stiffness, 0.45; fatigue, 0.48; depression, 0.43; anxiety, 0.56; global well-being, 0.46;disease severity, 0.49; impact on life, 0.51), KHAQ (0.44), and tender points (0.60) were high and statis-tically significant. The KFIQ might be a reliable and valid instrument for measuring health status andphysical functioning in Korean women patients with FM, but needs further study.
Key words: Fibromyalgia, Fibromyalgia impact questionnaire, Korean, Reliability, Validity
Introduction
Fibromyalgia (FM) is a common disorder char-acterized by widespread musculoskeletal pain,stiffness, paresthesia, nonrestorative sleep, easyfatigability, and multiple tender points which aresymmetrically distributed, and affects predomi-nantly women [1].
Since physical, laboratory, and radiologic ex-aminations produce no significant findings in pa-tients with FM, it is necessary to develop anobjective index to assess the characteristics ofthe disorder. Parts of the health assessment ques-tionnaire (HAQ) and arthritis impact mea-surement scales (AIMS), which were developed forrheumatoid arthritis, have been used to evalu-
ate physical functioning in FM [2, 3], butthese measures were not designed specifically forFM.
The fibromyalgia impact questionnaire (FIQ) isa self completed measure developed specifically forFM by Burckhardt et al. [4]. Authors demon-strated that the FIQ had sufficient evidence of re-liability and validity to warrant further testing inboth research and clinical setting [4]. The originalFIQ has been translated to Swedish, Hebrew,German, and Turkish [5–8], but no Korean ver-sion exists. The aim of this study was to assess thecultural appropriateness of FIQ for Korean pop-ulations, translate the questionnaire, and study itspsychometric properties in research and clinicalapplications.
Quality of Life Research 13: 857–861, 2004.� 2004 Kluwer Academic Publishers. Printed in the Netherlands.
857

Materials and methods
Subjects
Two groups of women patients were consecutivelyselected and studied, one of 20 subjects only forcomprehensibility testing and another of 62 sub-jects for psychometric testing. Both groups werepatients with FM attending an outpatient clinic atthe Hospital for Rheumatic Diseases, HanyangUniversity, Seoul and Maryknoll Hospital, Busan,Korea. All patients met the 1990 American Collegeof Rheumatology criteria for FM [1] and gavewritten informed consent.
The FIQ [4]
The FIQ was originally composed of 10 subscalesincluding 19 items, but recently a ‘climb stairs’item was added to the physical functioning sub-scale, and thus the current FIQ comprises 10subscales including 20 items (11 items make onephysical functioning subscale). The time referentof all FIQ items is past 1 week.
(1) One physical functioning subscale: The first 11items – ‘do shopping’, ‘do laundry with a washerand dryer’, ‘prepare meals’, ‘wash dishes/cookingutensils by hand’, ‘vacuum a rug’, ‘make beds’,‘walk several blocks’, ‘visit friends or relative’, ‘doyard work’, ‘drive a car’, ‘climb stairs’ – constituteone physical functioning subscale. Each item israted on a 4-point Likert-type scale (always: 0,most: 1, occasionally: 2, never: 3). The 11 items areadded together and divided by the number of validscores to yield one score for physical functioningsubscale. An average raw score between 0 and 3 isobtained and multiplied by 3.33 to normalize thisscore to 10 (range, 0–10).
(2) Two ‘feel good’ and ‘work missed’ subscales:The next two items refer to the number of days (0–7) in the past 1 week when the subjects felt welland how often they missed work because of FMsymptoms. Raw scores can range from 0 to 7 andthe score for the latter question is reversed. Tonormalize these scores to 10, the scores are mul-tiplied by 1.43 (range, 0–10).
(3) Seven other subscales: The last seven items –on work difficulty, pain, fatigue, morning tired-ness, stiffness, anxiety, and depression – are mea-sured using a 0–10 anchored visual analog scale
(VAS), 10 indicating the worst possible condition.The nine items (12 through 20) make 9 subscalesrespectively.
The FIQ is scored such that a higher score in-dicates a greater impairment. The total FIQ scorecan range from 0 to 100. This is achieved bysumming raw scores for each of the 10 subscales.For example, a score of ‘6’ on 5 subscales and ‘4’on the remaining 5 subscales would yield anoverall FIQ score of 50 which represents themidpoint of the total score possible. If one or morequestions are missed, we multiple the final sum-mary score by 10/x (i.e. if one question is missed,we multiply by 10/9 ¼ 1.111).
Translation of the FIQ
The translation of the fibromyalgia impact ques-tionnaire into the Korean (KFIQ) followedguidelines proposed by Guillemin et al. [9], andwas performed by three translators (bilingual,their mother tongue is Korean) and then inde-pendently translated back into English by threedifferent translators (bilingual, their mother ton-gue is English) with committee review.
Comprehensibility
Twenty patients with FM were asked to rate eachquestion with regard to whether they understoodand were familiar with it (comprehensibility) on a4-point scale (poor, 1; moderate, 2; good, 3; verygood, 4). We regarded questions as comprehensi-ble when patients answered with ‘3’ or ‘4’ [10].
Reliability
Reliability was tested by test–retest reliability. Thetest–retest was performed with a 1-week interval in20 patients among 62 subjects who agreed tocomplete the questionnaire twice.
Construct validity
Construct validity was assessed by comparing theresponse on the FIQ and other measures: (1) FMsymptoms by VAS, (2) Korean health assessmentquestionnaire (KHAQ) [10], and (3) tender pointcount (TPC).
858

For the severity of FM symptoms, VAS wasused by patients to rate current levels of pain,morning stiffness, fatigue, depression, anxiety,global well-being, disease severity, and impact ofFM on life, which were done separately in additionto the FIQ. Items were scored 0–10, 10 indicatingthe worst possible condition.
The HAQ is a self-administered instrument formeasuring physical disability in patients withrheumatoid arthritis, but it has been used amongpatients with other rheumatic diseases. It consistsof 20 items in 8 groups of functional limitations ofthe lower and upper extremities. The HAQ hasbeen translated into Korean (KHAQ) [10]. TheKHAQ evaluates only physical functioning, butthe KFIQ present additional information such asdepression, anxiety, etc.
For the TPC, a count of 18 tender points at 9symmetrical sites [1] was performed by thumbpalpation of physicians. Definite tenderness wasconsidered to be present if some involuntary ver-bal or facial expression of pain occurred or a winceor withdrawal was observed. The amount ofmanual pressure applied over a tender point wasabout 4 kg/cm2 (tested periodically against a dol-orimeter).
Statistics
Test–retest reliability was tested using intraclasscorrelation coefficients. Spearman rank correlationcoefficients were calculated between the KFIQscore and (1) FM symptoms by VAS, (2) KHAQ,and (3) TPC. Data were analyzed on a personalcomputer using the standard statistical software(SAS V8.1).
Results
Comprehensibility
The comprehensibility of the KFIQ was assessedby 20 patients. Patient ratings of each question inKFIQ were high, with 82–100% of the patientsrating the comprehensibility of each question as‘good’ or ‘very good’. The least-comprehensiblequestion was ‘walk several blocks’ (comprehensi-bility was 82%).
Demographic and clinical characteristicsof the subjects
A total of 62 patients with FM were entered in thepsychometric study. All patients were female. Theage of the patients (mean ± SD) was 47.1 ± 11.6(range 25–73) years. The socioeconomic charac-teristics of the 62 patients are shown in Table 1.
The KFIQ score was 48.3 ± 13.0 (17–91). Themean and SDs of the each components of the FIQare shown in Table 2. The KHAQ score was0.42 ± 0.41 (0–1.7). The VAS, KHAQ, and TPCscores are shown in Table 3.
Table 1. Demographic characteristics of 62 women with FM
Age, mean (SD) years 47.1 (11.6)
Education, mean (SD) years 10.4 (3.7)
Marital status (%)
Married 84
Divorced 11
Never married 5
Employment (%)
Full time 18
Part time 8
None 74
Family income (SD) · 104 won/month 169 (103) [1408 (858)]*
Disease duration, mean (SD) years 4.8 (5.6)
*Numbers in brackets are US dollars according to current
exchange rate.
Table 2. Means, SDs, and Test–retest reliability of the KFIQ
items (n = 62)
KFIQ item (scale range) Mean SD R*
N = 20
Physical functioning (0–10) 1.6 1.6 0.80
Feel good (0–10) 6.5 3.0 0.64
Work missed (0–10) 1.0 2.2 0.85
Ability to do the job (0–10) 1.0 2.4 0.95
Pain (0–10) 6.2 2.2 0.76
Fatigue (0–10) 7.0 2.0 0.67
Morning tiredness (0–10) 7.1 1.7 0.96
Stiffness (0–10) 6.4 2.5 0.87
Anxiety (0–10) 6.2 2.3 0.53
Depression (0–10) 6.0 2.3 0.63
Total (0–100) 48.3 13.0 0.85
*R is the intraclass correlation coefficient, which means test–
retest reliability.
859
Response rate
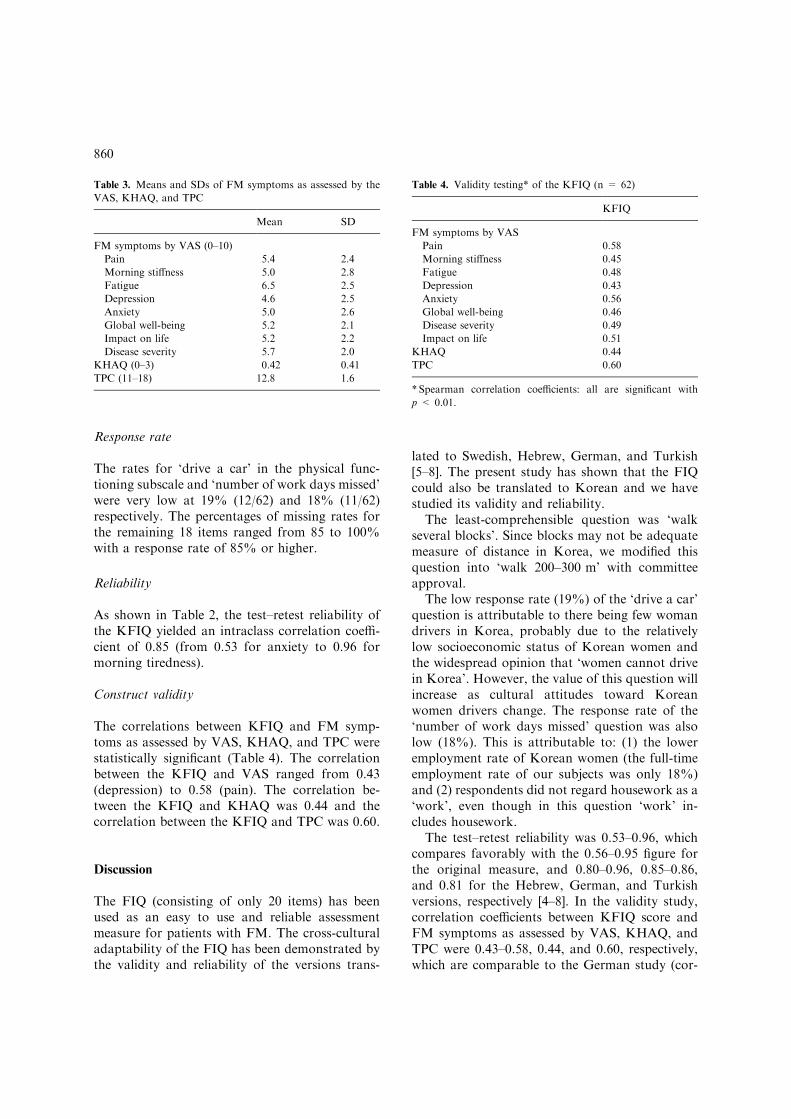
The rates for ‘drive a car’ in the physical func-tioning subscale and ‘number of work days missed’were very low at 19% (12/62) and 18% (11/62)respectively. The percentages of missing rates forthe remaining 18 items ranged from 85 to 100%with a response rate of 85% or higher.
Reliability
As shown in Table 2, the test–retest reliability ofthe KFIQ yielded an intraclass correlation coeffi-cient of 0.85 (from 0.53 for anxiety to 0.96 formorning tiredness).
Construct validity
The correlations between KFIQ and FM symp-toms as assessed by VAS, KHAQ, and TPC werestatistically significant (Table 4). The correlationbetween the KFIQ and VAS ranged from 0.43(depression) to 0.58 (pain). The correlation be-tween the KFIQ and KHAQ was 0.44 and thecorrelation between the KFIQ and TPC was 0.60.
Discussion
The FIQ (consisting of only 20 items) has beenused as an easy to use and reliable assessmentmeasure for patients with FM. The cross-culturaladaptability of the FIQ has been demonstrated bythe validity and reliability of the versions trans-
lated to Swedish, Hebrew, German, and Turkish[5–8]. The present study has shown that the FIQcould also be translated to Korean and we havestudied its validity and reliability.
The least-comprehensible question was ‘walkseveral blocks’. Since blocks may not be adequatemeasure of distance in Korea, we modified thisquestion into ‘walk 200–300 m’ with committeeapproval.
The low response rate (19%) of the ‘drive a car’question is attributable to there being few womandrivers in Korea, probably due to the relativelylow socioeconomic status of Korean women andthe widespread opinion that ‘women cannot drivein Korea’. However, the value of this question willincrease as cultural attitudes toward Koreanwomen drivers change. The response rate of the‘number of work days missed’ question was alsolow (18%). This is attributable to: (1) the loweremployment rate of Korean women (the full-timeemployment rate of our subjects was only 18%)and (2) respondents did not regard housework as a‘work’, even though in this question ‘work’ in-cludes housework.
The test–retest reliability was 0.53–0.96, whichcompares favorably with the 0.56–0.95 figure forthe original measure, and 0.80–0.96, 0.85–0.86,and 0.81 for the Hebrew, German, and Turkishversions, respectively [4–8]. In the validity study,correlation coefficients between KFIQ score andFM symptoms as assessed by VAS, KHAQ, andTPC were 0.43–0.58, 0.44, and 0.60, respectively,which are comparable to the German study (cor-
Table 3. Means and SDs of FM symptoms as assessed by the
VAS, KHAQ, and TPC
Mean SD
FM symptoms by VAS (0–10)
Pain 5.4 2.4
Morning stiffness 5.0 2.8
Fatigue 6.5 2.5
Depression 4.6 2.5
Anxiety 5.0 2.6
Global well-being 5.2 2.1
Impact on life 5.2 2.2
Disease severity 5.7 2.0
KHAQ (0–3) 0.42 0.41
TPC (11–18) 12.8 1.6
Table 4. Validity testing* of the KFIQ (n = 62)
KFIQ
FM symptoms by VAS
Pain 0.58
Morning stiffness 0.45
Fatigue 0.48
Depression 0.43
Anxiety 0.56
Global well-being 0.46
Disease severity 0.49
Impact on life 0.51
KHAQ 0.44
TPC 0.60
* Spearman correlation coefficients: all are significant with
p < 0.01.
860

relation coefficients between German FIQ andpain VAS, HAQ, and TPC values were 0.65, 0.61,and 0.58, respectively) [7]. The low correlationbetween the KHAQ and the KFIQ might be ex-plained by that the KHAQ evaluates only physicalfunctioning.
The results of the present study suggest that theKFIQ might be a reliable and valid instrument formeasuring health status and physical functioningin Korean women patients with FM, but theKFIQ needs more work in the future.
Acknowledgements
This work was supported by a grant from theKorea Health 21 R&D Project, Ministry of Health& Welfare, Republic of Korea (01-PJ1-PG1-01CH10-0007). We greatly thank Dr Robert M.Bennett, Oregon Health Sciences University,Portland, OR for Permission to translate the FIQinto Korean, Eun-Joo Kwak for her data man-agement and statistical analyses, and thoughtfulcomments of anonymous reviewers which madeour paper more strengthen.
References
1. Wolfe F, Smythe HA, Yunus MB, et al. The American
College of Rheumatology 1990 criteria for the classification
of fibromyalgia. Report of the Multicenter Criteria Com-
mittee. Arthritis Rheum 1990; 33: 160–172.
2. Ramey DR, Fries JF, Singh G. The Health Assessment
Questionnaire 1995 – Status and Review. Quality of Life
and Pharmacoeconomics in Clinical Trials. 2nd ed., Phil-
adelphia: Lippincott-Raren Publishers, 1996, pp. 227–
233.
3. Meenan RF, Gertman PM, Mason JH. Measuring health
status in arthritis. The arthritis impact measurement scales.
Arthritis Rheum 1980; 23: 146–152.
4. Burckhardt CS, Clark SR, Bennett RM. The fibromyalgia
impact questionnaire: Development and validation. J
Rheumatol 1991; 18: 728–733.
5. Hedin PJ, Hamne M, Burckhardt CS, Engstrom-Laurent
A. The fibromyalgia impact questionnaire, a Swedish
translation of new tool for evaluation of the fibromyalgia
patient. Scand J Rheumatol 1995; 24: 69–75.
6. Buskila A, Neumann L. Assessing functional disability and
health status of women with fibromyalgia: Validation of a
Hebrew version of the fibromyalgia impact questionnaire. J
Rheumatol 1996; 23: 903–906.
7. Offenbalcher M, Waltz M, Schoeps P. Validation of a
German version of the fibromyalgia impact questionnaire
(FIQ-G). J Rheumatol 2000; 27: 1984–1988.
8. Sarmer S, Ergin S, Yavuzer G. The validity and reliability
of the Turkish version of the fibromyalgia impact ques-
tionnaire. Rheumatol Int 2000; 20: 9–12.
9. Guillemin F, Bombardier C, Beaton D. Cross-cultural
adaptation of health related quality of life measures: Lit-
erature review and proposed guidelines. J Clin Epidemiol
1993; 46: 1417–1432.
10. Bae SC, Cook EF, Kim SY. Psychometric evaluation of a
Korean health assessment questionnaire for clinical re-
search. J Rheumatol 1998; 25: 1975–1979.
Address for correspondence: Sang-Cheol Bae, The Hospital for
Rheumatic Diseases, Hanyang University Medical Center,
Seoul 133-792, South Korea
Phone: +82-2-2290-9203; Fax: +82-2-2298-8231
E-mail: [email protected]
861