Embed Size (px)
Citation preview

CRP Health Policy & Researchwww.crphealthpolicy.com
A SummAry of Key CAnAdiAn
PoliCy doCumentS in mentAl HeAltH

IntroductionPurpose The British Columbia Nurses’ Union (BCNU) recently launched a Mental Health Strategy. One of this project’s goals is to begin a discussion that will lead to an improved mental health system for patients, families, and the broader community.
The aim of this project is to develop a focused position statement that is informed by the academic literature, key policy documents, and the membership of the BCNU. This paper represents a summary of key Canadian policy documents in Mental Health of the last decade. It is designed to summarize data to be used in conjunction with a review of the academic literature, which has already been prepared for BCNU.
Background CRP has been contracted by the BCNU to create two products to date. First, a document reviewing the literature on Mental Health Systems was conducted to find relevant academic literature on the issue of mental health system reform. This document represents the completion of the second project. It reviews key policy documents in mental health of the last decade. These documents have been collapsed for their relevant recommendations, and summarized to help readers understand expert perspectives on mental health system reform.
These documents are expected to provide a rubric for a workshop for the BCNU’s membership to help inform the final position statement, at the discretion of the initiative’s steering committee.
Canadian Mental Health Policy Psychological health has recently emerged as a social and political priority. Many Canadians are impacted by untreated mental health illness in their workplaces, their homes, and their communities. Although we can identify the issues around us – there is a lack of services available to refer people in need. The inadequacy of care has been identified by many community groups, and there is an identifiable consensus to call to action. Its time that organizations start to contribute to a system wide change that will support people struggling with mental illness in the very communities we work and our members live.
This report reviews twelve recent publications recommending changes to the mental health system. From these reports three main themes were identified: collaboration, staffing, and the continuum of care. Each of them will be explained and their synthesized recommendations presented to provide a condensed account of these reports.
This Document This document has collapsed twelve relevant policy documents on mental health in Canada, with a specific focus on BC, into three over-arching themes listed above. This document provides two-page spreads summarizing these themes both visually and with text. Each theme page includes a breakdown of relevant points of the theme, and a section focussing on rural communities. These summaries start on page three. The document also contains two visualized summaries of the text. A grid indicating which documents were summarized, and which recommendations they are related to, is presented on the facing page. Near the end of the document is a word cloud, and is accompanied by an explanaition of its use. Some examples of effective programs are also provided. A complete list of the policy documents summarized is available on the final page of this document.
BC T
ertia
ry M
enta
l Hea
lth...
Inqu
est:
Touc
hing
the
Dea
th...
Still
Wai
ting:
Firs
t-H
and.
..Ps
ycho
soci
al H
ealth
& S
afet
y...
Lost
in th
e Sh
adow
s: H
ow a
...Im
prov
ing
Hea
lth S
ervi
ces f
or...
Nat
iona
l Gui
delin
es fo
r Sen
iors
'..C
hang
ing
Dire
ctio
ns, C
hang
ing.
.M
enta
l Hea
lth C
omiss
ion.
..Va
ncou
ver's
Men
tal H
ealth
...Im
prov
ing
heal
th o
utco
mes
...Sh
ared
Men
tal H
ealth
Car
e...
Theme 1 - Collaboration
Coordinated access to tertiary care
Intergrated, locally delivered services
Program Leadership and Accountability
Provincial Collaboration
Increase access to knowledge about the LTC system for phycisians and families
Create and improve transition services (Acute - LTC - Community - Forensic)
Engage employers as tools for prevention and supporting staying at work
Improve information sharing protocols between key agency partners
Specialized care for Seniors with Mental Illness
Theme 2 - StaffingSpecialty training for Clinicians and Staff
Sufficient staffing, with appropriate expertise
Expertise in Child and Youth Mental health services
Policy for employees/employers about Mental Health
Enhanced urgent care for Mental Health
Theme 3 - Continuum of Care
Innovative service delivery
Prioritize Long Term Care (LTC) of elderly and cognitively impaired persons
Standardize care between facilities to promote continuity
Specialized services for individuals with aggression needed
Need for leadership to ensure continuum of care
Better referal system between services
Low threshold mental health treatment programs
Add Long-term and secure mental health treatment beds

Theme 1: CollaborationWorking Together to Achieve our Goals The mental health care system in Canada has long been fragmented. People have been unable to access the care they need due to a lack of appropriate services in their area. We also see the fragmentation of services providers, as highlighted in recent reports. For example, the Vancouver Police Department notes that forensic and public health systems are interdependent but are not formally working together to provide appropriate services at appropriate times. The challenges identified most commonly were:
• Limited availability of acute care• Limited availability of long-term care• Community support for people both transitioning from medical care or the forensic system• Population level prevention to care for people within the community
before they are in need of acute care • Partnerships, collaboration, and knowledge exchange – the ability of
service providers and clients to work together
Despite the long list of challenges, there are several opportunities that can be addressed in the short term, and other initiatives that will require long-term, sustainable support (financial/HR). Arguably a system restructuring would be most desirable, however there are several changes that will make the current system much more efficient and effective.
Aside from any discussion of collaboration, the most consistent consideration seen across all policy documents is that of insufficient funding, and insufficient staff. We must acknowledge that no other intervention will be effective without first seeing a significantly increased level of funding for mental health systems.
Collaboration in Forensics Recent evidence from VPD call centers show that calls involving mental health are on the rise. Police Officers are faced with situations where neither the forensic nor the health systems have the resources to help resolve the situation. The lack of emergency mental health services means that many people are inappropriately placed within the forensic system.
Communication Systems Working together may not be as difficult as it may seem, and better communication could be the initial and most important step. Many reports indicate that practitioners often feel that they cannot report relevant clinical information to other service providers because of confidentiality laws. These perceptions, whether true or untrue, should be examined and information sharing should be promoted. Efforts should be undertaken to ensure that the information technology (IT) is in place to communicate data as well. Unfortunately, IT systems in place today are fractured and often don’t have the capacity to share data between different services.
Community Development A realistic and effective first step to collaboration is education for all stakeholders on issues of mental health conditions, confidentiality, and effective communication –including conflict resolution. The second and most effective strategy will be to bring all community members to the same table. Together we can develop strategies that will effectively address the variety of concerns and recent recommendations made. The community is currently in need of a leader to initiate this alliance.
Alliances between Acute Services & Others The health care system is structurally under-resourced, and as such, cannot meet rising mental health demands. Acute care is limited, and the lack of long-term care beds results in many people being pushed back into the community before they are ready to be reintroduced. Expansion of acute care services is recommended to improve the ability of acute services to work in concert with both community and tertiary services.
Rural & Remote Communities Rural communities are also in need of an effective mental health strategy; with even fewer services available to them it will be essential to develop different approaches. It would be appropriate to create a committee of people with rural experience to look at opportunities and challenges for collaboration in rural areas.
Rural Communities Acute Health
Community Key Areas
Empowering Communities The community includes both community services and family support. Families and community members need education and awareness to cope with mental illness and to reduce stigma. The reduction of stigma through community health promotion efforts will help to improve health-seeking behaviours before mental illness becomes a critical care or forensic issue.

Theme 2: People Make the SystemHaving Sufficient, Well Supported staff Staffing within the field of mental health is another weakness within the current system. Many of the recent reports were essentially case studies of critical incidents, and in many cases, addressing staffing issues may have prevented these incidents from occurring. Predominantly, it is primary care that suffers when appropriate staffing levels and supports are not in place. However, there are many lessons to be learned and many potential solutions that can be implemented going forward. The following section outlines key areas in which staffing can be strengthened.
Meeting Client Needs with Sufficient Staff Staffing levels need to increase overall, throughout the health care system. For example, one report specifically recommends increasing nursing levels to .59 hours of RN/patient/day and 3.06 hours of nursing/patient/day in long term care facilities. Multi-disciplinary teams were recommended often, and staffing levels need to expand to accommodate this. Some specialized areas of practice that were highlighted and should be considered are: geriatrics, concurrent disorders and managing violent patients. Smaller facilities may feel as though hiring more staff with different specializations is not justified, but this limits the ability to support challenging clients. More non-clinical staff are also recommended to fulfill the appropriate staffing levels for community support services, such as housing programs.
Providing Appropriate Support Staff should have clearly defined reporting channels to various supervisors so they know their concerns, or the concerns of their clients, are being noted and dealt with. Proper supervision ensures that staff are working with clients in appropriate ways and not taking on more than they have the capacity for. A good supervisory strategy also means that workplace roles and responsibilities are clearly
defined, which is a key principle for promoting psychological health and safety.
In addition to supervision, proper supports for staff struggling with mental health challenges should be in place. Having clear policies around leave and accommodations, as well as collaborative return-to-work processes, have been shown to reduce burnout and staff turnover.
Best Skills for the Best Results Working with clients with mental illness requires a specialized set of knowledge. Care providers must know how to assess patients during intake processes, identify conditions that present in complex ways (such as delirium in elderly patients), manage behavioural issues and much more. Training also allows staff to feel confident in their roles and can also reduce incidents of injury on the job. However, due to budget cutbacks across the province, staff training programs have been reduced. In some settings, new models of care are implemented without consideration for the
context of the health care setting. If a new model is sufficiently out of place, or if sufficient resources are not provided for the implementation of a model, staff may become resistant to its implementation. These issues may exacerbate problems with adherence to evidence based practices. As LPNs become increasingly involved in mental health, it is becoming increasingly important for a post-basic training program in mental health to be developed for them.
In all cases, training and other education should be an ongoing process to ensure consistency of practice within the workplace.
Keeping Care Safe In many of the incidents described in these reports, clients fell through the cracks when staff felt that their case loads were too high. When staff do not have enough time to spend with every client, critical issues or treatment needs may be missed, leading to situations that are dangerous for all parties involved, such as an attack by a violent patient. Having a manageable workload is also crucial for employee’s own mental health. To avoid this, it is recommended that staff and management communicate clearly and frequently about workload and capacity issues without fear of reprimand. This may require a culture change within the workplace to encourage fault-free reporting.
Staffing Levels
Staff Supervision & Support Staff Training
Workload Management
Rural & Remote Communities
Staffing in Remote Environments All of these staff related issues are exacerbated in rural and remote communities. The main challenge that these communities face is attracting enough staff to practice in these areas. In order to operate the programming that people with mental illness in these communities require, care providers have been forced to expand their scope of practice, sometimes beyond their capacity. Additionally, less experienced staff are often sent to work in remote communities without much training or any supervision, having to take on the workload of many staff members. This was the case in one report, where these staffing issues led, in part, to a young client’s suicide.

Theme 3: The Continuum of Care
Access &Entry Placement Maintenance
& Exit
Management
Urgent Care A key consideration brought forward by many policy documents is the availability of urgent and emergency care. In the Vancouver context, it is recommended that an urgent care facility be built, potentially attached to a hospital or the Burnaby Centre, which could handle the high number of emergency mental health and addictions cases. Throughout the system, all services and sub-services should consider how clients might gain urgent access to their programs, and define this process clearly for other service providers.
Assertive Approaches Clients with mental illness do not always seek care, for a wide variety of reasons. Assertive tactics to engage clients in care should be undertaken. Centralized intake services can be a part of this, however they must be well funded, resourced, and empowered. Mental health and addictions screenings should be incorporated system wide.
Reviewing Performance A review of access issues in the mental health system should be undertaken. Particular attention should be paid to indirect barriers, such as travel costs.
Enhancing Clients’ Flow Through the System The final theme identified in the review can be described as the continuum of care. From a systems perspective, this is an issue of integration, both laterally and vertically (further explained below). From a client centred point of view, this is a question of creating a seamless experience for both the patient and the service provider. Chiefly, this theme calls for an elimination of onerous work on the part of the client, and elimination of key bottlenecks and wait lists. Services are encouraged to take an assertive approach, making sure they actively seek to provide services to clients, rather than requiring clients to actively seek services from providers.
Appropriate Resources The process of planning care is often under-resourced. It is recommended that dedicated teams, possibly integrated with centralized intake, be created to effectively coordinate placement. Such teams must be well resourced.
Meeting Population Level Needs In general, decisions to place clients in one level of care and not another are based on the availability of services, rather than individual clinical need. To address this problem, standardized algorithms for determining patient needs should be developed. The service mix in each area should then
be appropriate for population needs.
Apparent Gaps Several key populations are seen as dramatically underserved by the current system. Services for the following populations should be expanded: Dementia, Refractory Psychosis, Dual Diagnosis, Youth-Adult Transition Ages (16-24), and Violent Patients. Violent patients may also need legislation changes allowing them to be placed in appropriate services against their will. Underlying causes of violence, such as untreated dementia, poor fit in LTC, and insufficient staffing must be addressed in order to keep patients and staff safe.
Empowering Communities While the concept of deinstitutionalization is a laudable goal, the ability of individuals with mental health issues to thrive in communities has been taken for granted. Appropriate community supports and programming must be in place for clients on their way out of the system, or moving to less acute levels of care. Such supports shouldn’t be limited to formal programs - employers should be supported with accommodations for individuals with mental illnesses in the workplace. Families caring for loved ones with mental illness should have access to financial assistance and respite care.
Long Term Care Many reports cite the issue of Long Term Care (LTC) availability. A long wait-list in LTC means backlogs throughout the system, from entry points to urgent care. LTC capacity must be expanded.
Communication Communication of client information is perceived as a major issue, particularly when moving between services. Clarity should be established on what information confidentiality laws prohibit the sharing of, and clinicians should be empowered to share client data.
Integrated Management Most BC Health Authorities utilize a matrix model of management. In this model, managers are responsible for their areas, and reporting structures do not necessarily intersect further up the chain of command. While this improves community engagement and involvement, it is also seen as fracturing services. It is recommended that matrix approaches be modified by adding a single point reporting structure. Mental health services should be overseen at the highest levels. At minimum there should be an Assistant Deputy Minister. Lower level managers should build trust and effective communication within their team and between teams. Longer tenures of managers may have the effect of building more trust.
Lateral Integration Creating better flow between access, placements, maintenance and exit from the system can be seen as a matter of vertical integration. Equally important is the concept of lateral integration. This concept refers to integration between various types of services at each step for the patient. For example, Assertive Community Outreach teams provide lateral integration in that they have nurses, social workers, psychiatrists, and others working on the same team, readily available to clients.
Housing & Primary Care The most significant issues of integration
are access to physical primary health services and housing. These two important domains should be integrated into the mental health system.
Rural & Remote Communities Connecting services between different geographical locations is also considered an issue of lateral integration. Rural and remote communities make this somewhat difficult, often with differing management structures, resources and clinical practices. As mentioned before, services should have a single point of reporting for their management systems. Efforts should be undertaken to reduce barriers in clients moving between areas if different specialties are needed. Integrated data systems may provide a good start to this.

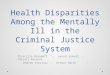
The Word Cloud A word cloud is a visual representation of a statistical analysis of the individual words contained in a body of text. During the process of summarizing the key policy documents, the team created a composite set of notes detailing all relevant information that was to be included in this report. Using the web based tool “Tagul Clouds,” this text was analyzed to produce this word cloud. Words that appear more frequently in text are represented as larger, while less frequently occuring words are presented as smaller.
At a glance, we can see words like Staff, Staffing, Manage, Workplace, and Team, indicating that labour issues are key considerations of the documents. Similarly, we can see the words Depression, Senior, Older, Suicide, and Addiction, which may give us a clue as to some of the target populations addressed by the reports.
It would be erroneous to say that there are only negative things within the mental health system. Indeed, there are many examples of effective approaches that should be lauded for their successes, and for their integration of the recommendations made by the policy documents of the previous decade. Three have been selected for discussion here, to help provide a background for this document.
Where it Has Worked
Mental Health Emergency Services (MHES) Commonly referred to by the call sign of the police vehicle associated with it (in Vancouver, Car 87) this service integrates mental health with police services. A nurse, often an RPN, accompanies a police officer with additional training on emergency calls that are believed to involve mental health issues. The service is an ideal example of lateral service integration and appropriate training for the problem that the program is meant to address. It is criticized, however, as being largely insufficient for the problem it is attempting to address. What’s more, if effective services were available to the mental health population, it is likely that mental health crises would be less common, and less police intervention would be required.
Assertive Community Treatment (ACT) The ACT model of delivering services is becoming widely regarded as the state-of-the-art in mental health care delivery. It employs highly interdisciplinary teams including counsellors, nurses, social workers, psychiatrists and others to help meet the needs of clients. Housing and physical primary care are built into this model, and so clients can be stabilized in as many domains of their lives as possible. A high service-provider-to-client ratio ensures that staff have sufficient time and support to effectively provide care. ACT is very favourably reviewed in economic terms. It is believed that due to its ability to stabilize volatile clients, savings are then incurred on account of reduced visits to emergency departments and less involvement in the criminal justice system. The model is sometimes criticized as being highly rigid, and as such not appropriate for all clients. For example, clients who are already stable may not experience a high level of benefit over more traditional service models.
The Housing First Philosophy Housing First is not a service delivery model so much as it is a philosophical orientation towards providing services. It suggests that before we begin to address issues of mental health, we must first provide stable, supportive housing to individuals. This is profoundly different from the current approach, which generally requires individuals to be somewhat mentally stable before they are admitted to social housing programs. The integration of this philosophy into care models has had documented positive effects, and is seen as a priority in the development of new mental health care systems.
87

References
BC Ministry of Health. (2013). Improving Health Services for Individuals with Severe Addiction and Mental Illness. Victoria.
Canadian Coalition for Seniors Mental Health. (2006). National Guidelines for Senior's Mental Health - The Assessment and Treatment of Depression. Toronto.
Canadian Psychiatric Association and the College of Family Physicians of Canada. (1996). Shared Mental Health Care in Canada: A Position Paper. Mississuaga & Ottawa.
Coroner of Ontario. (2005). Inquest: Touching the Death of Ezz-El-Dine El-Roubi and Pedro Lopez (Jury Rec-ommendations). Toronto.
Mental Health Comission. (2012). Psychological Health & Safety. Ottawa.
Mental Health Commission of Canada. (2012). Changing Directions, Changing Lives: The Mental Health Strategy for Canada. Ottawa.
Mental Health Commission of Canada. Collaborative Mental Health Care: Milestones and historical perspec-tive of its development in Canada. Ottawa.
Provincial Health Services Authority (BC). (2013). BC Tertiary Mental Health Services. Vancouver.
Regional Mental Health & Addictions Program (VCH & PHC). (2013). Improving Health Outcomes, Housing and Safety: Addressing the needs of individuals with severe addiction and mental illness. Vancouver.
Representative for Children & Youth. (2014). Lost in the Shadows: How a Lack of Help Meant a Loss of Hope for One First Nations Girl. Victoria.
Representative for Children & Youth. (2013). Still Waiting: First-hand Experiences with Youth Mental Health Services in BC. Victoria.
Vancouver Police Department. (2013). Vancouver’s Mental Health Crisis: An Update Report. Vancouver.